Back to Journals » International Journal of Women's Health » Volume 18
Global Patterns and Temporal Trends in Modifiable Risk Factors Among Women of Childbearing Age, 1990–2021: A Systematic Analysis from the Global Burden of Disease Study
Authors Xu Q ![]() , Zhang H, Chen B
, Zhang H, Chen B ![]() , Xie Z, Lin Q, Zhao Y, She G, Zhong F, Li J
, Xie Z, Lin Q, Zhao Y, She G, Zhong F, Li J
Received 29 January 2026
Accepted for publication 4 May 2026
Published 17 May 2026 Volume 2026:18 599831
DOI https://doi.org/10.2147/IJWH.S599831
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Qian Xu,1,2,* Huabin Zhang,1,2,* Bin Chen,3 Zhaomin Xie,2 Queran Lin,4 Yuqing Zhao,1,2 Gaoli She,2 Fei Zhong,2 Jie Li1– 3
1School of Medicine, South China University of Technology, Guangzhou, Guangdong, People’s Republic of China; 2Global Health Research Center, Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Sciences, Southern Medical University, Guangzhou, Guangdong, People’s Republic of China; 3School of Public Health, Southern Medical University, Guangzhou, Guangdong, People’s Republic of China; 4Department of Primary Care and Public Health, School of Public Health, Faculty of Medicine, Imperial College London, WHO Collaborating Centre for Public Health Education and Training, London, UK
*These authors contributed equally to this work
Correspondence: Jie Li, Global Health Research Center, Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Sciences, Southern Medical University, Guangzhou, Guangdong, People’s Republic of China, Tel +86-020-83525975, Email [email protected] Fei Zhong, Global Health Research Center, Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Sciences, Southern Medical University, Guangzhou, Guangdong, People’s Republic of China, Email [email protected]
Objective: Women of childbearing age (WCBA, 15– 49 years) are a key population for public health prevention, yet evidence on long-term trends in modifiable risk factors and their attributable burden remains limited. We aimed to assess global patterns and temporal changes in major modifiable risk factors among WCBA.
Methods: Using data from the Global Burden of Disease (GBD) 2021, we analysed summary exposure values, deaths, and disability-adjusted life years (DALYs) attributable to 83 modifiable risk factors across metabolic, behavioural, and environmental/occupational domains.
Results: In 2021, 1.10 million deaths and 108.0 million DALYs among WCBA were attributable to modifiable risk factors, representing 34.83% of total deaths and 26.52% of total DALYs. The leading Level 3 risk factors for DALYs were unsafe sex (4.89%), iron deficiency (3.36%), high body mass index (BMI) (3.19%), and high fasting plasma glucose (FPG) (2.48%). Between 1990 and 2021, environmental and occupational risk exposures generally declined over time, whereas metabolic risk exposures—particularly high BMI (EAPC 1.83%) and high FPG (EAPC 1.59%)—showed sustained increases across most regions. Risk profiles varied across sociodemographic index (SDI) levels, with reproductive and nutritional risks predominating in lower-SDI settings and metabolic or behavioural risks more prominent in higher-SDI settings.
Conclusion: Modifiable risk factors account for a substantial proportion of disease burden among WCBA. The coexistence of rising metabolic risks and persistent reproductive and nutritional challenges calls for targeted strategies—strengthening reproductive health and nutrition programmes in lower-SDI settings, and prioritising obesity prevention and metabolic screening in higher-SDI regions.
Keywords: women of childbearing age, modifiable risk factors, global burden of disease, disability-adjusted life years, temporal trends, public health prevention
Introduction
Women of childbearing age (WCBA), defined as females aged 15–49 years, constitute a key population for public health prevention.1,2 WCBA represent a distinct group characterized by overlapping nutritional, metabolic, and reproductive vulnerabilities.3,4 Health risks during this life stage contribute substantially to morbidity, mortality, and adverse reproductive outcomes, with implications for both women’s current health, pregnancy outcomes, and population health more broadly.1,2,5 In addition, ongoing demographic transition and changing fertility patterns worldwide have further increased the importance of monitoring risk factors in this population, as shifts in the timing and context of childbearing may alter both exposure profiles and the public health consequences of these risks.6,7 Despite improvements in healthcare coverage in many regions,8,9 WCBA continue to face a wide range of preventable health risks,10,11 underscoring the need for population-level evidence to inform effective prevention strategies.12
Over recent decades, socioeconomic development, urbanisation, and lifestyle changes have reshaped the risk profile of WCBA worldwide.3 The burden attributable to metabolic risk factors has increased markedly, driven in part by rising levels of high body mass index (BMI) and dysglycaemia, alongside growing challenges related to mental health.13–15 At the same time, environmental exposures such as air and water pollution remain important contributors to health risk in many low- and middle-income settings.16 These concurrent trends indicate an increasingly complex mix of traditional and emerging risk factors affecting WCBA, highlighting the importance of comprehensive assessment across multiple risk domains.
Although previous studies have quantified mortality and disease burden among women, evidence remains limited on long-term patterns of exposure to, and disease burden attributable to, a broad spectrum of modifiable risk factors among WCBA.2,17,18 Existing research has often focused on individual diseases, single risk factors, or specific countries, limiting comparability and the ability to prioritise prevention efforts across populations.3,19 In particular, few studies have systematically examined how risk exposures and their relative contributions to disease burden have changed over time across diverse geographic and sociodemographic contexts using a consistent analytical framework. This gap is especially important because risk profiles during the childbearing years may have intergenerational consequences through effects on conception, pregnancy, fetal growth, and later offspring health.
The Global Burden of Disease (GBD) 2021 study offers an opportunity to address these gaps by providing harmonised estimates of exposure and attributable burden for a wide range of modifiable risk factors across countries and over time.13 Compared with prior single-risk or single-country studies, the GBD comparative risk assessment framework enables consistent cross-country, cross-risk, and longitudinal comparisons using standardized definitions and modeling procedures. Using GBD 2021 data, this study aimed to identify the leading modifiable risk factors contributing to mortality and disability-adjusted life years (DALYs) among WCBA and to characterise global, regional, and national trends in risk exposure from 1990 to 2021. By clarifying the evolving distribution of major risk factors, this analysis seeks to support prioritisation of prevention strategies and evidence-based public health planning for women of childbearing age.
Methods
Study Population and Data Sources
This study focused on WCBA, defined by the WHO as females aged 15 to 49 years, a group undergoing physiological changes associated with reproductive function.18 Data were derived from the GBD 2021 study, coordinated by the Institute for Health Metrics and Evaluation (IHME) at the University of Washington. GBD 2021 provides systematically compiled estimates for 204 countries and territories across 23 age groups and includes data on 88 risk factors, 155 health outcomes, and 631 risk–outcome pairs.13 All data used in this analysis were publicly available through the GBD Results Tool (http://ghdx.healthdata.org/gbd-results-tool).
Comparative Risk Assessment Framework
Risk factor estimation followed the GBD comparative risk assessment (CRA) framework, which quantifies the attributable burden.13 This process includes seven key steps:
- Estimating risk exposure: Using 51,337 data sources—including surveys, surveillance systems, and remote sensing—exposure levels were modeled by location, age, sex, and year through Bayesian meta-regression methods (eg, ST-GPR and DisMod-MR 2.1).13
- Estimating relative risks (RRs): Associations between 88 risk factors and 155 health outcomes were quantified based on 3359 data sources through systematic reviews, meta-analyses, and meta-regression. For 211 risk–outcome pairs, the Burden of Proof Risk Function (BPRF) was applied to model non-linear dose–response relationships and account for study heterogeneity, while traditional meta-regression was used for the remaining 420 pairs.13
- Defining the theoretical minimum risk exposure level (TMREL): The TMREL represents the exposure level associated with the lowest possible risk, based on epidemiological evidence or predefined thresholds.
- Calculating population attributable fractions (PAFs): The PAF reflects the proportion of risk-attributable burden that could be avoided if exposure were reduced to the TMREL.
- Computing summary exposure values (SEVs): SEVs reflect the risk-weighted prevalence of exposure on a scale from 0 (no excess risk) to 100 (highest possible risk).
- Adjusting for mediation and interactions: Mediation and overlapping effects among risk factors were accounted for to prevent overestimation.
- Estimating attributable burden: The attributable deaths and DALYs were calculated by multiplying the PAF by the total disease burden for each outcome.
Risk Factor Classification
GBD 2021 categorized 88 risk factors hierarchically across five levels. Level 0 comprises all risk factors, Level 1 includes three broad categories (environmental/occupational, behavioral, and metabolic risks), and Levels 2 to 4 consist of increasingly specific risk factors or clusters. This study excluded five risk factors—suboptimal breastfeeding, non-exclusive breastfeeding, discontinued breastfeeding, child stunting, and zinc deficiency—due to their irrelevance to WCBA, resulting in a final analysis of 83 risk factors. These exclusions were made because these risks are not directly estimated within the GBD Study for the WCBA population.
Key Variables and Definitions
SEV quantifies population-level exposure to a risk factor by integrating prevalence and risk magnitude. It ranges from 0 to 100, where higher values indicate higher exposure or risk severity. SEVs were computed using age-, sex-, location-, and time-specific exposure estimates weighted by associated RRs.13
Sociodemographic Index (SDI) is a composite indicator of development, incorporating total fertility rate under age 25, mean education among individuals aged ≥15 years, and lag-distributed income per capita.20 Countries were categorized into five SDI quintiles: low, low-middle, middle, high-middle, and high. SDI was used to evaluate geographic disparities in risk exposures and burden.
Estimation of Attributable Burden
The burden attributable to each risk factor was estimated in terms of deaths and DALYs. For each risk–outcome pair, the PAF was first calculated and then multiplied by the total burden of the corresponding health outcome.
Statistical Analysis
This study extracted SEV, estimated deaths, and DALYs attributable to risk factors for WCBA from the GBD 2021 results tool, including 95% uncertainty intervals (UIs). The 95% UIs were generated using advanced Bayesian methods, integrating multiple data sources and accounting for uncertainties from measurement errors, study design variations, and potential biases. Posterior distributions were sampled 500 times, with UIs defined by the 2.5th and 97.5th percentiles. In contrast, 95% confidence intervals (CIs) were used only for the age-standardized rates (ASRs) and estimated annual percentage change (EAPC) values. The 95% UIs and 95% CIs were applied to different types of estimates and were not used for direct inferential comparison. ASRs with 95% CIs were calculated using the GBD 2021 world standard population to adjust for age structure differences, ensuring comparability across studies.20
A descriptive analysis examined SEV, estimated deaths, and DALYs by risk factor level, SDI, GBD 21 regions, and 204 countries and territories from 1990 to 2021. Temporal trends in age-standardized SEVs and DALYs were assessed using the EAPC with a 95% CI, calculated from a log-linear regression model:

where x is the calendar year and β represents the annual change in log-transformed ASRs. A positive EAPC with a 95% CI excluding zero indicates a significant upward trend, while a negative value indicates a decline.17,21 As a sensitivity analysis, we compared the EAPC from log-linear regression with the average annual percentage change (AAPC) derived from joinpoint regression for the three major risk categories at the global level, using Joinpoint Regression Program (version 5.2.0.0, April 2024; Statistical Research and Applications Branch, National Cancer Institute).
Spearman’s rank correlation was used to explore associations between SEV, age-standardized DALY rate (ASDR), and SDI. Gaussian process regression with a LOESS smoother was applied to estimate expected SEV and ASDR values across SDI levels.21 All analyses and visualizations were conducted using R (version 4.2.2).
Results
Global Exposure to Risk Factors Among WCBA
In 2021, among Level 2 risk factors, the highest global SEVs among WCBA were observed for high LDL cholesterol (44.71), air pollution (40.92), and dietary risks (33.99). At the Level 3 hierarchy, dietary risks showed particularly high exposure levels, especially diets low in milk (SEV 88.37) and low in omega-6 polyunsaturated fatty acids (77.75).
From 2010 to 2021, metabolic risks were the only Level 1 category showing an increase in age-standardised SEVs, with an EAPC of 1.69%. Within Level 2 metabolic risks, nearly all exposures increased, except for kidney dysfunction. High BMI and high FPG showed the fastest increases, with EAPCs of 1.89% and 1.57%, respectively. In contrast, most environmental and occupational risks declined, with air pollution showing the largest reduction (EAPC −1.42%). Among behavioural risks, drug use increased most rapidly (EAPC 3.16%), whereas tobacco exposure declined most sharply (EAPC −1.71%). Among specific risk factors, high BMI and diets high in sugar-sweetened beverages showed the steepest increases in exposure, with EAPCs of 1.83% and 1.79%, respectively (Table 1).
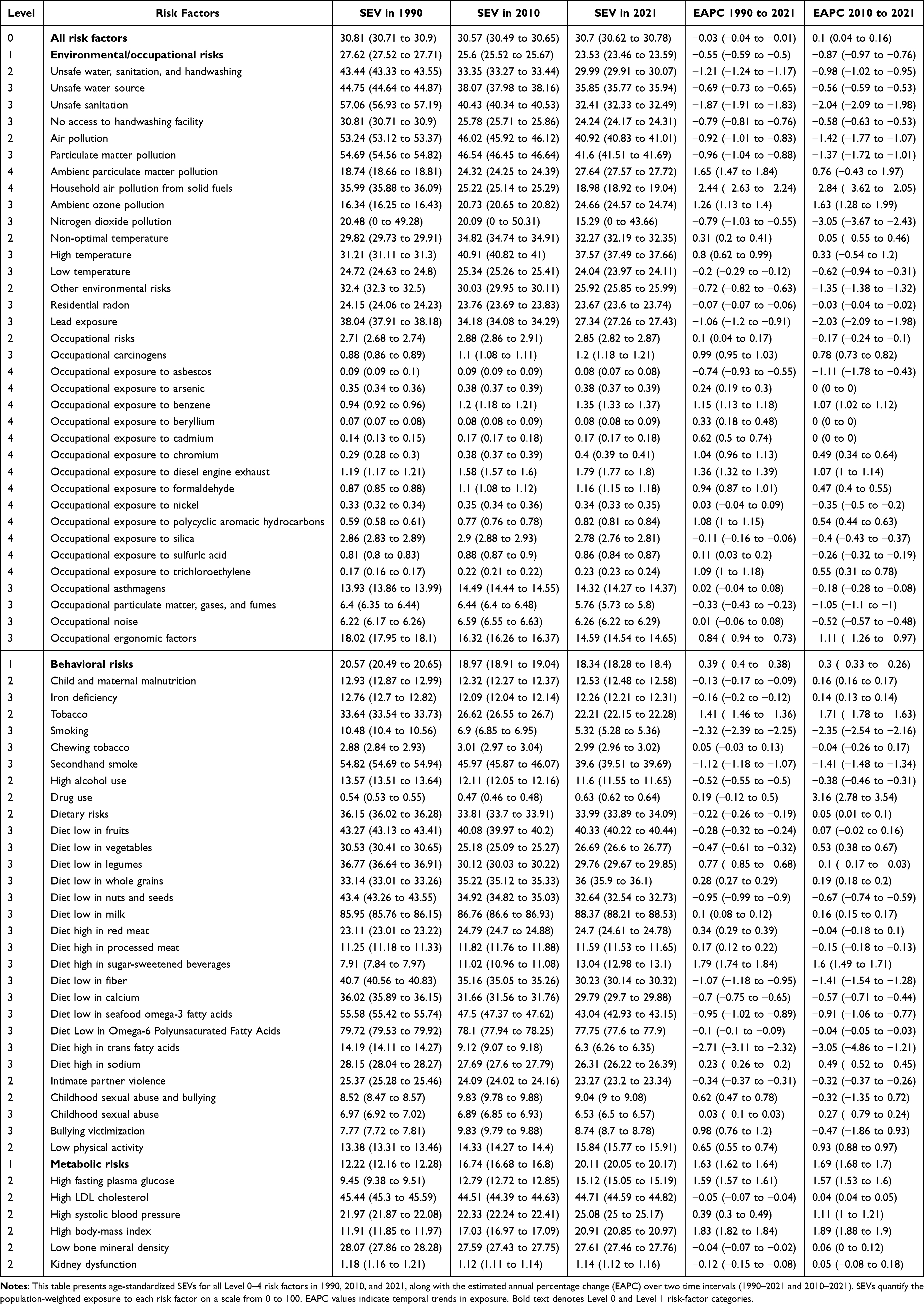 |
Table 1 Summary Exposure Values and Temporal Trends of Major Risk Factors Among Women of Childbearing Age, 1990–2021 |
The joinpoint regression-derived AAPC estimates were highly consistent with the EAPC estimates for environmental/occupational, behavioural, and metabolic risks, supporting the robustness of the overall temporal patterns (Table S1).
Global Burden Attributable to Risk Factors
In 2021, an estimated 1.10 million deaths and 108.0 million DALYs among WCBA were attributable to risk factors, accounting for 34.83% of total deaths and 26.52% of total DALYs in this population.
At the Level 2 category, unsafe sex was the leading contributor to mortality, with 326,051 attributable deaths, followed by dietary risks (201,280 deaths), high systolic blood pressure (149,159), air pollution (145,818), and high BMI (123,004). In terms of DALYs, unsafe sex contributed 19.84 million DALYs, followed by child and maternal malnutrition (17.81 million), high BMI (13.00 million), dietary risks (11.77 million), and occupational risks (10.14 million) (Figure 1 and Table S2). The disease outcomes associated with these risks varied; unsafe sex was predominantly linked to HIV/AIDS and neoplasms, whereas high BMI was associated with multiple conditions, including diabetes, cardiovascular diseases, respiratory disorders, and selected cancers.
 |
Figure 1 Global deaths and DALYs attributable to major risk factors among WCBA in 2021. (A) Global attributable deaths from major Level 2 risk factors among women of childbearing age (WCBA) in 2021; (B) global attributable disability-adjusted life years (DALYs). Risk factors are ranked by total attributable burden. |
Temporal Trends in Leading Level 3 Risk Factors
Between 1990 and 2021, the composition of the top 25 Level 3 risk factors contributing to DALYs among WCBA changed substantially. In 1990, iron deficiency ranked first, followed by unsafe sex and particulate matter pollution. By 2021, unsafe sex became the leading contributor, accounting for 4.89% of total DALYs, followed by iron deficiency (3.36%), high BMI (3.19%), and high FPG (2.48%).
Among the top 25 risk factors, high BMI showed the largest relative increase in attributable DALYs (+150.2%), followed by high FPG (+135.24%). In contrast, the burden attributable to iron deficiency remained relatively stable over time, while particulate matter pollution declined substantially. Notably, only a small number of risk factors showed increasing trends in age-standardised DALY rates, including low birthweight and short gestation (EAPC 1.44%), high BMI (EAPC 1.14%), high FPG (EAPC 0.93%), and bullying victimisation (EAPC 0.74%). Among these, low birthweight and short gestation showed the steepest increase in age-standardised DALY rates (Figures 2 and S1).
 |
Figure 2 Temporal trends in age-standardised DALY rates for selected Level 3 risk factors among WCBA, 1990–2021. Risk factors are ordered by DALYs in descending order for 1990 and 2021. Lines connecting the same risk factor across time indicate rank changes: solid lines represent an increase or no change, while dashed lines indicate a decline. Colors indicate risk categories, with red representing environmental and occupational risks, blue representing behavioural risks, and green representing metabolic risks. EAPC values are presented numerically in the rightmost column. Pale shading for the rank-26 rows indicates risk factors outside the top 25 in one year that are included to preserve rank-transition continuity. Abbreviations: WCBA, women of childbearing age; DALYs, disability-adjusted life years; EAPC, estimated annual percentage change; LBW and short gestation, low birthweight and short gestation. |
Regional Variation in Risk Profiles
Marked heterogeneity in leading risk factors was observed across regions in 2021. High BMI was the leading Level 3 risk factor in 10 regions, including East Asia, Western Europe, and Latin America, whereas unsafe sex ranked first in four sub-Saharan African regions. Iron deficiency was the predominant risk in Central and South Asia. Drug use was the leading risk factor in High-income North America, smoking in Central Europe, and high FPG in the High-income Asia Pacific region (Figure 3 and Table S3).
 |
Figure 3 Leading Level 3 risk factors for DALYs among WCBA by GBD region and SDI quintile in 2021. For each GBD region and SDI quintile, Level 3 risk factors are ranked by attributable DALYs from left (highest) to right (tenth). Risks are color-coded based on the EAPC in age-standardized DALY rates from 1990 to 2021. Abbreviations: WCBA, women of childbearing age; DALYs, disability-adjusted life years; GBD, Global Burden of Disease; EAPC, estimated annual percentage change; Bullying, bullying victimization; Low fruit intake, diet low in fruits; Sexual violence against children, childhood sexual abuse; Low vegetable intake, diet low in vegetables; Low whole grains, diet low in whole grains; High BMI, high body mass index; High FPG, high fasting plasma glucose; High LDL, high LDL cholesterol; High SBP, high systolic blood pressure; Partner violence, intimate partner violence; LBW & short gestation, low birthweight and short gestation; Ergonomic risks, occupational ergonomic factors; PM pollution, particulate matter pollution; SDI, Sociodemographic Index. |
Geographic variation was also evident in exposure trends. High FPG was the fastest-growing risk in seven regions, while high BMI showed the largest increases in five regions, particularly in East and South Asia. Occupational ergonomic risks increased most rapidly in several Latin American regions, and drug use rose sharply in High-income North America and Central Europe. At the national level, high BMI was the leading Level 3 risk factor in 94 countries, followed by unsafe sex in 46 countries, smoking in 21 countries, and iron deficiency in 16 countries (Figure S2). For exposure, dietary risks—especially low milk consumption—ranked first in 142 countries (Figure S3).
Risk Factor Exposure and Burden by SDI
Risk factor profiles differed substantially across SDI quintiles. In 2021, unsafe sex, iron deficiency, and particulate matter pollution dominated in low-SDI regions; iron deficiency, unsafe sex, and high BMI in low-middle SDI regions; and high BMI, high FPG, and high alcohol use in high-middle and high-SDI regions. Drug use emerged as a leading contributor in high-SDI settings (Figures 3 and S4).
Across SDI levels, SEVs for metabolic and behavioural risks increased with rising SDI, whereas environmental and occupational exposures declined. Despite increasing exposure to metabolic and behavioural risks, age-standardised DALY rates for all three major risk categories generally decreased with higher SDI. Over time, from 1990 to 2021, SEVs for environmental and occupational risks declined across most SDI quintiles, whereas metabolic SEVs increased steadily at all SDI levels, particularly in high-SDI regions. Behavioural SEVs remained relatively stable or declined slightly, while their associated DALY rates decreased across all quintiles. In contrast, age-standardised DALY rates for metabolic risks showed modest overall declines but increased in high-SDI regions, indicating a divergence between exposure and burden (Figures 4 and S5).
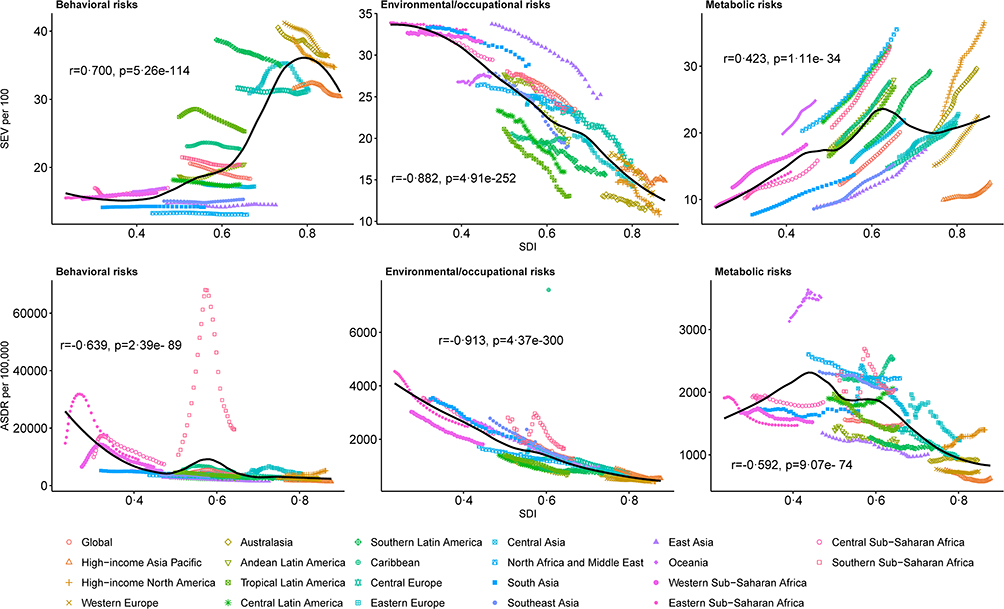 |
Figure 4 Risk factor exposure and attributable burden among WCBA across SDI levels in 2021. This figure displays the association between sociodemographic index (SDI) and risk factor exposure (SEVs) as well as age-standardised DALY rates for behavioural, metabolic, and environmental/occupational risk categories among WCBA in 2021. Solid lines represent expected values based on SDI, and points represent observed regional estimates. |
Discussion
In this comprehensive analysis of 83 modifiable risk factors among WCBA across 204 countries, we observed a clear transition in the global risk profile over the past three decades. While traditional environmental and nutritional risks have declined or stabilised, metabolic risks have emerged as increasingly dominant contributors to disease burden. At the same time, reproductive and behavioural risks remain substantial, particularly in lower-SDI settings. Together, these findings reflect a complex and evolving risk landscape shaped by demographic, socioeconomic, and lifestyle transitions.
The increasing dominance of metabolic risks likely reflects global lifestyle changes associated with urbanisation, including higher intake of energy-dense foods, reduced physical activity, and sedentary behaviours.22,23 Importantly, high BMI and dysglycaemia increased consistently across most regions and SDI levels, and were among the few risk factors with rising age-standardised DALY rates. Given that these exposures accumulate during the reproductive years, they may have implications not only for chronic disease risk but also for pregnancy outcomes and intergenerational health.3,17,24–26 These patterns highlight the need for earlier, prevention-oriented strategies targeting metabolic health before and during the reproductive period.
At the same time, the continued prominence of unsafe sex and iron deficiency underscores persistent inequities in access to essential health services and adequate nutrition, particularly in low- and low-middle SDI settings. Unsafe sex remained the leading contributor to DALYs globally, largely driven by HIV/AIDS and related conditions,27–29 while iron deficiency continued to reflect sustained nutritional vulnerability linked to menstruation and pregnancy.30–32 The coexistence of these risks with rising metabolic exposures suggests that many regions are experiencing a dual burden, requiring integrated approaches that address both traditional and emerging health challenges.
Behavioural risks showed mixed trends. While tobacco exposure declined markedly and alcohol use decreased in many regions, drug use increased rapidly, and low physical activity became more prevalent. These divergent patterns suggest that existing public health strategies have been effective for some established risks but less so for emerging or context-specific behaviours. Addressing these risks will require adaptive, multi-sectoral interventions that combine regulation, health promotion, and broader social policies.
Substantial heterogeneity across SDI levels further highlights the need for context-specific strategies.33,34 In lower-SDI regions, reproductive and nutritional risks remain dominant contributors to disease burden, whereas in higher-SDI settings, metabolic and behavioural risks play a more prominent role. Although age-standardised DALY rates generally decline with increasing SDI, the continued rise in metabolic exposures—particularly in high-SDI regions—suggests that current health systems are insufficiently focused on prevention, especially during early adulthood and the preconception period.22,23,35
From a policy perspective, these findings support a shift toward integrated, life-course approaches to prevention in WCBA. In lower-SDI settings, strengthening sexual and reproductive health services and scaling up nutrition programmes remain critical. In higher-SDI regions, prioritising obesity prevention, improving dietary quality, and implementing early screening for metabolic risk factors are essential. Across all settings, integrating maternal health, non-communicable disease prevention, and behavioural risk reduction may provide the greatest opportunity to reduce long-term disease burden.
Several limitations should be considered when interpreting these findings. First, this analysis is based on estimates from the GBD 2021 study and depends on the availability and quality of underlying data, with greater uncertainty in low-income and conflict-affected regions and potential variation in national-level data quality. Second, as an ecological analysis based on country-level modeled estimates, the findings should not be interpreted at the individual level and may mask important within-country disparities by socioeconomic position, ethnicity, or urban-rural residence. Third, only risk factors included within the GBD framework were analysed, and some relevant social and contextual determinants of health were not captured. Fourth, incomplete coverage of the full 15–49 years age range for certain risk factors may have resulted in minor misclassification or underestimation. Last, estimates for 2020 and 2021 may have been influenced by pandemic-related disruptions to data collection, healthcare access, and risk-factor trajectories and should therefore be interpreted with caution.
Conclusions
In conclusion, a substantial proportion of disease burden among WCBA is attributable to a limited number of modifiable risk factors, with a marked shift towards metabolic risks alongside persistent reproductive and nutritional challenges. These findings highlight the need for context-specific prevention strategies: strengthening sexual and reproductive health services and nutritional interventions in low- and middle-SDI settings, while prioritising obesity prevention, healthy diet promotion, and early metabolic screening in higher-SDI regions. Future research should aim to validate these findings using independent cohort and surveillance data and to further elucidate causal pathways linking evolving risk exposures to health outcomes in this population.
Data Sharing Statement
All data used in this study are publicly available from GBD Results Tool at https://ghdx.healthdata.org/gbd-results-tool. For further information regarding access to GBD data, readers may contact the GBD Secretariat ([email protected]). Analytical code supporting the findings of this study is available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study used publicly available, aggregated, and anonymized secondary data from the Global Burden of Disease 2021 study. No direct contact with participants was involved, and no identifiable personal information was accessed. According to items 1 and 2 of Article 32 of the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects issued in China on February 18, 2023, studies using legally obtained public data or anonymized information data may be exempt from ethical review, provided that they do not cause harm to humans and do not involve sensitive personal information or commercial interests. Therefore, this study was exempt from ethical approval, and the requirement for informed consent was waived by the Institutional Review Board of Guangdong Provincial People’s Hospital (No. KY2026-400-01).
Acknowledgments
We acknowledge the Global Burden of Disease Study team for providing access to the dataset used in this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
JL was supported by National Natural Science Foundation of China (82473620), National Science and Technology Major Project (2025ZD0549500 and 2024ZD0532700), Guangzhou Science and Technology Program (2025A03J4433), and Start-up Funding of Guangdong Provincial People’s Hospital. The funding sources do not have any role in the design, interpretation of the study, or the decision to publish the results.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Temmerman M, Khosla R, Bhutta ZA, Bustreo F. Towards a new global strategy for women’s, children’s and adolescents’ health. BMJ. 2015;351:h4414. doi:10.1136/bmj.h4414
2. Huang D, Lai H, Shi X, et al. Global temporal trends and projections of acute hepatitis E incidence among women of childbearing age: age-period-cohort analysis 2021. J Infect. 2024;89(4):106250. doi:10.1016/j.jinf.2024.106250
3. Gaillard R, Jaddoe VWV. Maternal cardiovascular disorders before and during pregnancy and offspring cardiovascular risk across the life course. Nat Rev Cardiol. 2023;20(9):617–13. doi:10.1038/s41569-023-00869-z
4. Stephenson J, Heslehurst N, Hall J, et al. Before the beginning: nutrition and lifestyle in the preconception period and its importance for future health. Lancet. 2018;391(10132):1830–1841. doi:10.1016/s0140-6736(18)30311-8
5. Campbell J, Cometto G, Rasanathan K, et al. Improving the resilience and workforce of health systems for women’s, children’s, and adolescents’ health. BMJ. 2015;351:h4148. doi:10.1136/bmj.h4148
6. Fauser B, Adamson GD, Boivin J, et al. Declining global fertility rates and the implications for family planning and family building: an IFFS consensus document based on a narrative review of the literature. Hum Reprod Update. 2024;30(2):153–173. doi:10.1093/humupd/dmad028
7. Mills M, Rindfuss RR, McDonald P, te Velde E. Why do people postpone parenthood? Reasons and social policy incentives. Hum Reprod Update. 2011;17(6):848–860. doi:10.1093/humupd/dmr026
8. Sanghera J, Gentile L, Guerras-Delgado I, et al. Human rights in the new global strategy. BMJ. 2015;351:h4184. doi:10.1136/bmj.h4184
9. Ojong SA, Temmerman M, Khosla R, Bustreo F. Women’s health and rights in the twenty-first century. Nat Med. 2024;30(6):1547–1555. doi:10.1038/s41591-024-03036-0
10. McDougall L, Sharma A, Franz-Vasdeki J, et al. Prioritising women’s, children’s, and adolescents’ health in the post-2015 world. BMJ. 2015;351:h4327. doi:10.1136/bmj.h4327
11. Zarocostas J. World’s health systems must be strengthened to meet women’s needs, says WHO. BMJ. 2009;339(nov11 1):b4685. doi:10.1136/bmj.b4685
12. UN. Two billion women without access to social protection. Women UN Updated October 17. Available from: https://news.un.org/en/story/2024/10/1155701.
13. GBD 2021 Risk Factors Collaborators. Global burden and strength of evidence for 88 risk factors in 204 countries and 811 subnational locations, 1990-2021: a systematic analysis for the global burden of disease study 2021. Lancet. 2024;403(10440):2162–2203. doi:10.1016/s0140-6736(24)00933-4
14. Zhou J, Zhang Y, Teng Y, et al. Association between preconception body mass index and fertility in adult female: a systematic review and meta-analysis. Obes Rev. 2024;25(10):e13804. doi:10.1111/obr.13804
15. Dai F, Cai Y, Chen M, Dai Y. Global trends of depressive disorders among women of reproductive age from 1990 to 2021: a systematic analysis of burden, sociodemographic disparities, and health workforce correlations. BMC Psychiatry. 2025;25(1):263. doi:10.1186/s12888-025-06697-4
16. GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet. 2020;396(10258):1223–1249. doi:10.1016/s0140-6736(20)30752-2
17. Sun P, Yu C, Yin L, et al. Global, regional, and national burden of female cancers in women of child-bearing age, 1990-2021: analysis of data from the global burden of disease study 2021. EClinicalMedicine. 2024;74:102713. doi:10.1016/j.eclinm.2024.102713
18. Cao F, Li DP, Wu GC, et al. Global, regional and national temporal trends in prevalence for musculoskeletal disorders in women of childbearing age, 1990-2019: an age-period-cohort analysis based on the global burden of disease study 2019. Ann Rheum Dis. 2024;83(1):121–132. doi:10.1136/ard-2023-224530
19. Vogel B, Acevedo M, Appelman Y, et al. The Lancet women and cardiovascular disease Commission: reducing the global burden by 2030. Lancet. 2021;397(10292):2385–2438. doi:10.1016/s0140-6736(21)00684-x
20. GBD 2021 Diseases and Injuries Collaborators. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the global burden of disease study 2021. Lancet. 2024;403(10440):2133–2161. doi:10.1016/s0140-6736(24)00757-8
21. Lv B, Lan JX, Si YF, et al. Epidemiological trends of subarachnoid hemorrhage at global, regional, and national level: a trend analysis study from 1990 to 2021. Mil Med Res. 2024;11(1):46. doi:10.1186/s40779-024-00551-6
22. GBD 2013 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990-2013: a systematic analysis for the global burden of disease study 2013. Lancet. 2015;386(10010):2287–2323. doi:10.1016/s0140-6736(15)00128-2
23. GBD 2015 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990-2015: a systematic analysis for the global burden of disease study 2015. Lancet. 2016;388(10053):1659–1724. doi:10.1016/s0140-6736(16)31679-8
24. Huang X, Wu Y, Ni Y, Xu H, He Y. Global, regional, and national burden of type 2 diabetes mellitus caused by high BMI from 1990 to 2021, and forecasts to 2045: analysis from the global burden of disease study 2021. Front Public Health. 2025;13:1515797. doi:10.3389/fpubh.2025.1515797
25. Sun Y, Shen Z, Zhan Y, et al. Effects of pre-pregnancy body mass index and gestational weight gain on maternal and infant complications. BMC Pregnancy Childbirth. 2020;20(1):390. doi:10.1186/s12884-020-03071-y
26. Huang C, Li J, Qin G, et al. Maternal hypertensive disorder of pregnancy and offspring early-onset cardiovascular disease in childhood, adolescence, and young adulthood: a national population-based cohort study. PLoS Med. 2021;18(9):e1003805. doi:10.1371/journal.pmed.1003805
27. GBD 2019 Tuberculosis Collaborators. Global, regional, and national sex differences in the global burden of tuberculosis by HIV status, 1990-2019: results from the global burden of disease study 2019. Lancet Infect Dis. 2022;22(2):222–241. doi:10.1016/s1473-3099(21)00449-7
28. Ramjee G, Daniels B. Women and HIV in Sub-Saharan Africa. AIDS Res Ther. 2013;10(1):30. doi:10.1186/1742-6405-10-30
29. Li J, Xie DD, Cui HL, et al. Trends in the burden and determinants of HIV in the Asia-Pacific region (1990-2019): an age-period-cohort analysis of the 2019 global burden of disease study. J Med Virol. 2024;96(6):e29724. doi:10.1002/jmv.29724
30. Han X, Ding S, Lu J, Li Y. Global, regional, and national burdens of common micronutrient deficiencies from 1990 to 2019: a secondary trend analysis based on the global burden of disease 2019 study. EClinicalMedicine. 2022;44:101299. doi:10.1016/j.eclinm.2022.101299
31. Munro MG, Mast AE, Powers JM, et al. The relationship between heavy menstrual bleeding, iron deficiency, and iron deficiency anemia. Am J Obstet Gynecol. 2023;229(1):1–9. doi:10.1016/j.ajog.2023.01.017
32. Stevens GA, Finucane MM, De-Regil LM, et al. Global, regional, and national trends in haemoglobin concentration and prevalence of total and severe anaemia in children and pregnant and non-pregnant women for 1995-2011: a systematic analysis of population-representative data. Lancet Glob Health. 2013;1(1):e16–25. doi:10.1016/s2214-109x(13)70001-9
33. Peacock A, Leung J, Larney S, et al. Global statistics on alcohol, tobacco and illicit drug use: 2017 status report. Addiction. 2018;113(10):1905–1926. doi:10.1111/add.14234
34. GBD 2019 Universal Health Coverage Collaborators. Measuring universal health coverage based on an index of effective coverage of health services in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet. 2020;396(10258):1250–1284. doi:10.1016/s0140-6736(20)30750-9
35. Garvey WT, Mechanick JI, Brett EM, et al. American association of clinical endocrinologists and American college of endocrinology comprehensive clinical practice guidelines for medical care of patients with obesity. Endocr Pract. 2016;22 Suppl 3:1–203. doi:10.4158/ep161365.Gl
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Global Spatiotemporal Trends and Modifiable Risk Factors for Female Infertility: An Age-Period-Cohort Using Global Burden of Disease Study 2021 and Mendelian Randomization Analysis
Zhou Y, Peng D
International Journal of Women's Health 2025, 17:2929-2945
Published Date: 5 September 2025
Impact of Tobacco Exposure on Low Back Pain-Related Disability-Adjusted Life Years in China: Trends From 1990–2021 and Projections for the Next 15 years Using ARIMA Modeling
Song S, Feng S, Lu H, Li B
Journal of Pain Research 2025, 18:5303-5320
Published Date: 8 October 2025
Global, Regional, and National Burden of Alopecia Areata in Children and Adolescents Aged 0-19 years from 1990 to 2021 and Projection to 2040
Lu H, Li J, Ma K, Li L, Wang S, Wang T, Zhang B
Clinical, Cosmetic and Investigational Dermatology 2026, 19:582775
Published Date: 6 February 2026
Global, Regional, and National Burden of Adolescent Polycystic Ovary Syndrome from 1990 to 2021, with Projections of Disease Burden to 2041: A Systematic Analysis Based on the Global Burden of Disease Study 2021
Cao X, Yu Z, Wu S
International Journal of Women's Health 2026, 18:587430
Published Date: 13 March 2026
Epidemiological Trends and Projections of PM2.5-Attributable COPD Burden in China Over 1990–2035
Li M, Wang L, Amhare AF, Song Y, Wan P, Shi S, Qiao L, Guo Y
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:565060
Published Date: 16 March 2026