Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
From China’s Multicenter Prospective Cohort: Right Ventricular Afterload and Prognosis in Hospitalized Patients with Acute Exacerbation of COPD
Authors Gao A ![]() , Liu X
, Liu X ![]() , Jiao X, Ding Y, Gao Z, Gao Y, Zhang J, Yang J, Yang S
, Jiao X, Ding Y, Gao Z, Gao Y, Zhang J, Yang J, Yang S ![]() , Yang Y
, Yang Y
Received 14 March 2026
Accepted for publication 9 June 2026
Published 17 June 2026 Volume 2026:21 605642
DOI https://doi.org/10.2147/COPD.S605642
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Zijing Zhou
Aili Gao,1– 3 Xia Liu,4 Xiaojing Jiao,1,2 Yuan Ding,1,2 Zehan Gao,1,2 Yuan Gao,1,2 Junwei Zhang,1,2 Junwei Yang,1,2 Suqiao Yang,1,2,5 Yuanhua Yang1,2
1Department of Respiratory and Critical Care Medicine, Beijing Institute of Respiratory Medicine and Beijing Chao-Yang Hospital, Capital Medical University, Beijing, 100020, People’s Republic of China; 2Beijing Key Laboratory of Multimodal Intelligent Diagnosis and Treatment System for Respiratory Diseases, Beijing, 100020, People’s Republic of China; 3Department of Respiratory and Critical Care Medicine, Beijing Shunyi District Hospital, Beijing, 101300, People’s Republic of China; 4Department of Respiratory and Critical Care Medicine, Capital Medical University Daxing Teaching Hospital, Capital Medical University, Beijing, 102600, People’s Republic of China; 5Evidence-based Medicine Center, Beijing Chao-Yang Hospital, Capital Medical University, Beijing, 100020, People’s Republic of China
Correspondence: Suqiao Yang, Department of Respiratory and Critical Care Medicine, Beijing Institute of Respiratory Medicine and Beijing Chao-Yang Hospital, Capital Medical University, Beijing, 100020, People’s Republic of China, Email [email protected] Yuanhua Yang, Department of Respiratory and Critical Care Medicine, Beijing Institute of Respiratory Medicine and Beijing Chao-Yang Hospital, Capital Medical University, Beijing, 100020, People’s Republic of China, Tel +86-10-85231437, Fax +86-10-65005099, Email [email protected]
Purpose: The relationship between increased right ventricular (RV) afterload (moderate-to-high suspicion of pulmonary hypertension indicated by echocardiography) and the prognosis of patients hospitalized with acute exacerbation of chronic obstructive pulmonary disease (AECOPD) is not yet well understood.
Patients and Methods: This prospective cohort study was conducted in 11 hospitals from 2017 to 2020, involving patients hospitalized with AECOPD. Echocardiography was performed within 48 hours of admission. Patients were classified into two groups: those with increased RV afterload (n=237) and those with normal RV afterload (n=415). Hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated using Cox regression analysis to evaluate the impact of RV afterload on patient outcomes. Kaplan-Meier survival curves were employed to assess the association between RV afterload and 3-year all-cause mortality.
Results: Kaplan-Meier survival curves demonstrated that the 3-year all-cause mortality rates were 22.8% in AECOPD patients with increased RV afterload and 9.5% in those with normal RV afterload. Cox regression analysis indicated that increased RV afterload is an independent predictor of poor prognosis in hospitalized AECOPD patients, significantly increasing the risk of 3-year all-cause mortality (HR=2.172, 95% CI: 1.384– 3.411; P< 0.001). Additionally, elevated brain natriuretic peptide (BNP) or n-terminal pro-brain natriuretic peptide (NT-proBNP) (HR=2.694, 95% CI: 1.724– 4.209; P< 0.001), and lower body mass index (BMI) (HR=0.880, 95% CI: 0.833– 0.930; P< 0.001) were independent risk factors for mortality.
Conclusion: Increased RV afterload is associated with a significant increase in the risk of 3-year all-cause mortality in patients hospitalized with AECOPD, posing a 2.2-fold higher risk compared to those with normal RV afterload. It also stands as an independent risk factor for mortality. Elevated BNP or NT-proBNP levels and reduced BMI are additional independent risk factors of mortality. Early detection of these three risk factors could play a role in stratifying high-risk patients, guiding clinical decision-making, and improving patient outcomes in AECOPD.
Plain Language Summary: In this study, we focused on individuals hospitalized for AECOPD. We investigated the association between moderate-to-high suspicion of pulmonary hypertension on echocardiography and their prognosis. Our results can help identify those at high risk of mortality. Echocardiography is a noninvasive and widely available tool, yet its validation in large real-world cohorts remains limited. Moreover, many people are hospitalized for AECOPD, and our findings apply to the much larger population seen in primary care and routine clinical practice.
Keywords: respiratory diseases, echocardiography, mortality, n-terminal pro-brain natriuretic peptide/brain natriuretic peptide, body mass index
Introduction
Chronic obstructive pulmonary disease (COPD) is a common cause of death worldwide, characterized by persistent and typically progressive airflow obstruction.1 Acute exacerbation of COPD (AECOPD), defined as an acute worsening of respiratory symptoms such as dyspnea, cough, and/or sputum production within 14 days in patients with COPD, significantly impact health outcomes. AECOPD not only represents a major source of mortality worldwide, but also imposes a significant economic burden and has a rising prevalence.2 Particularly in China, COPD ranks as the third leading cause of death and significantly compromises the quality of life of patients.3
Cardiovascular disease, as one of the most significant comorbidities and complications in patients with COPD, contributes to right heart failure and an increased risk of death.4 Studies have demonstrated that a concurrent diagnosis of heart failure greatly worsens prognosis for patients with COPD.5 Increased right ventricular (RV) afterload, which may arise from various causes, is known to heighten the risk of cardiovascular events and adversely affect the prognosis of these patients. In recent years, the function of the RV has garnered increasing attention. Echocardiography has emerged as a reliable method for assessing structural and functional changes of the heart in COPD patients.6
Despite acknowledging the impact of increased RV afterload on cardiovascular health in COPD patients, its long-term prognostic significance in hospitalized patients with AECOPD—more than two years after discharge—remains uncertain, as previous studies have focused on stable COPD pulmonary hypertension rather than acute RV afterload changes during AECOPD. Therefore, this study was conducted to investigate the potential relationship between increased RV afterload and the long-term prognosis in these hospitalized AECOPD patients, aiming to fill the gap in existing research and seek to explore whether echocardiographic screening can provide valuable insights for clinical management, especially regarding risk stratification and monitoring in AECOPD patients.
Materials and Methods
Patients
Patients were collected from the registry for the period from April 11, 2017, to November 1, 2020. In total, 652 hospitalized patients with AECOPD were included in this study (Figure 1).
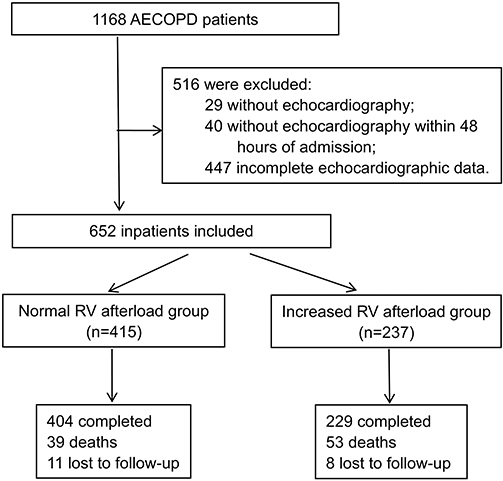 |
Figure 1 Flowchart of the study population. |
The inclusion criteria were as follows: 1) Age of 40 years or older; 2) Diagnosis of COPD based on the 2016 Global Initiative for Chronic Obstructive Lung Disease (GOLD) Guidelines,7 as confirmed by a senior physician, Diagnosis required post-bronchodilator pulmonary function tests showing a forced expiratory volume in the first second (FEV1) to forced vital capacity (FVC) ratio of less than 0.7; 3) Hospitalization specifically for AECOPD; 4) Echocardiography conducted within 48 hours after admission.
The exclusion criteria were as follows: 1) Inability to provide written informed consent; 2) Presence of active malignant tumors; 3) Pneumothorax present on admission; 4) Life expectancy of less than 6 months.
For the purpose of this post-hoc analysis, we applied an additional exclusion criterion: absence of complete data for RV afterload assessment [i.e., missing tricuspid regurgitation velocity (TRV), right ventricular to left ventricular basal diameter ratio (RV/LV ratio), main pulmonary artery (PA) diameter, or inferior vena cava (IVC) diameter with inspiratory collapse rate].
Study Design
The data of this study were collected from a national multicenter prospective registry study, supported by the National Key Research and Development Program of China (Clinical Trials.gov ID: NCT03185377). This study adheres to the ethical guidelines of the Declaration of Helsinki.
Increased RV afterload was identified based on echocardiographic criteria indicative of a moderate or high probability of pulmonary hypertension (PH). This was determined if at least one of the following echocardiographic findings was present:8 (1) Peak TRV at least 2.9 m/s. (2) Peak TRV of 2.8 m/s or less, accompanied by at least two of the following items: ① RV/LV ratio greater than 1.0; ② the diameter of the main PA exceeding 25 mm; ③ IVC diameter greater than 21mm with an inspiratory collapse rate less than 50% (with a sniff).
Left ventricular (LV) hypertrophy was defined as a maximal end-diastolic wall thickness greater than 11mm,9 and RV hypertrophy was defined as an RV wall thickness greater than 5 mm.10
Data Collection and Assessments
A comprehensive medical history was obtained for each patient, detailing the time of diagnosis of COPD, smoking index (calculated as cigarettes per day multiplied by the number of smoking years), body mass index (BMI). Additionally, comorbid conditions were recorded, including hypertension, coronary atherosclerotic heart disease (CHD), chronic atrial fibrillation, history of myocardial infarction, diabetes, cerebral infarction, cerebral hemorrhage, nephrotic syndrome, chronic nephritis, asthma, bronchiectasis, sleep apnea hypopnea syndrome (SAHA), pulmonary thromboembolism (PTE), and deep vein thrombosis (DVT). Diagnostic assessments involved parameters obtained from chest computer tomography (CT), electrocardiography (ECG), echocardiography, and pulmonary function tests.
Echocardiography was performed within 48 hours of admission as part of routine clinical practice, assessing parameters when technically feasible such as ejection fraction (EF), left ventricular end-diastolic diameter (LVEDD), right ventricular basal diameter, main PA inner diameter, RV/LV basal diameter ratio, tricuspid annular plane systolic excursion (TAPSE), TRV, IVC diameter, inspiratory collapse with a sniff, and ventricular wall motion amplitude and thickness.
Spirometry results encompassed forced expiratory volume in one second (FEV1), FEV1 percentage of predicted, forced vital capacity (FVC), FEV1/FVC ratio, and GOLD stages of COPD severity. The GOLD stages were defined based on post-bronchodilator FEV1 percentage of predicted values, categorizing severity into mild (GOLD 1, FEV1≥80%), moderate (GOLD 2, 50% ≤ FEV1 < 80%), severe (GOLD 3, 30% ≤ FEV1 < 50%), and very severe (GOLD 4, FEV1 < 30%).
Laboratory tests conducted within 24 hours of admission included measurements of white blood cell count (WBC), hematocrit (HCT), hemoglobin (Hb), platelet count (PLT), D-dimer, alanine aminotransferase (ALT), aspartate aminotransferase (AST), serum creatinine (Scr), total cholesterol (TC), triglycerides (TG), blood glucose (GLU), and either n-terminal pro-brain natriuretic peptide (NT-proBNP) or brain natriuretic peptide (BNP).
Resting arterial blood gas analysis was performed, recording of partial pressure of oxygen (PaO2), partial pressure of carbon dioxide (PaCO2), potential of hydrogen (PH), and fraction of inspiration oxygen (FiO2).
Outcomes
The primary outcome of the study was all-cause mortality. Patients were monitored at intervals of 3, 6, 12, 24, 30, and 36 months post-discharge to assess symptoms, rehospitalization rates, and overall prognosis. These follow-up assessments were conducted either during outpatient visits or through telephone interviews.
All data collected during the study were meticulously recorded and subsequently verified by dedicated investigators to ensure reliability. Resting echocardiography, a critical component of the assessment, was performed by trained sonographers who were intentionally blinded to the patients’ group assignments to maintain the objectivity of the results. Additionally, researchers at each participating center received standardized training prior to the study commencement, which was aimed at guaranteeing consistency and accuracy across all data collection points. This rigorous approach to training and data handling was designed to uphold the integrity of the study findings.
Statistical Analysis
Sample size calculation: Based on pilot data, the mortality rate was 26% in the increased RV afterload group and 13% in the control group. Assuming a two-sided α of 0.05 and a power of 80%, the estimated sample size was 142 patients per group. After accounting for a 10% anticipated loss to follow-up, the final sample size was set at 158 patients per group, yielding a total of 316 patients.
Statistical analyses were conducted using IBM SPSS version 27.0 (64-bit). The distribution of the data was initially assessed using the Shapiro–Wilk test to determine normality. Data that followed a normal distribution were expressed as mean ± Standard Deviation (SD), whereas non-normally distributed variables were reported using the median and interquartile range (IQR; 25th-75th percentile). Categorical variables were presented as frequencies and percentages.
The independent samples t-test was used for continuous variables that were normally distributed, while the chi-square (χ2) test was applied to categorical variables to compare characteristics between the two groups. In case of non-normally distributed data, nonparametric tests such as the Mann–Whitney U-test were utilized.
Survival analyses were conducted using Kaplan-Meier curves, and group differences were evaluated with the Log rank test. To further explore the association between various indicators and clinical outcomes in patients with AECOPD, both univariate and multivariate Cox regression analyses were performed, with adjustments made for potential confounding factors. Results were presented as hazard ratios [HR, 95% CI (confidence interval), P].
Missing outcome data were completely random and accounted for less than 5%. Therefore, no imputation was performed in this analysis. For all statistical test, a two-sided p-value of less than 0.05 was considered to indicate statistical significance.
Results
A total of 1168 patients with AECOPD were enrolled from 2017 to 2020. Of these, 652 participants met the inclusion criteria and were included in the final study population for follow-up analysis (Figure 1).
The patients were divided into two groups based on echocardiographic findings: those with increased RV afterload (n=237) and those with normal RV afterload (n=415).
Compared with included patients, those excluded (n=516, 44.2%) were generally similar in baseline characteristics and core clinical variables. (Supplementary Table S1).
Baseline Characteristics
The baseline characteristics of the cohort were summarized in Table 1. The study population consisted of 652 patients with a median age of 69 years, of whom 506 (77.6%) were male. Hypertension, CHD and diabetes were the most prevalent comorbidities in both the increased RV afterload group and the normal RV afterload group. Notable differences in baseline characteristics between these two groups were identified, including variations in age, BMI, chronic atrial fibrillation, diabetes, cerebral infarction, asthma, PTE, and DVT, all reaching statistical significance (P<0.05; Table 1).
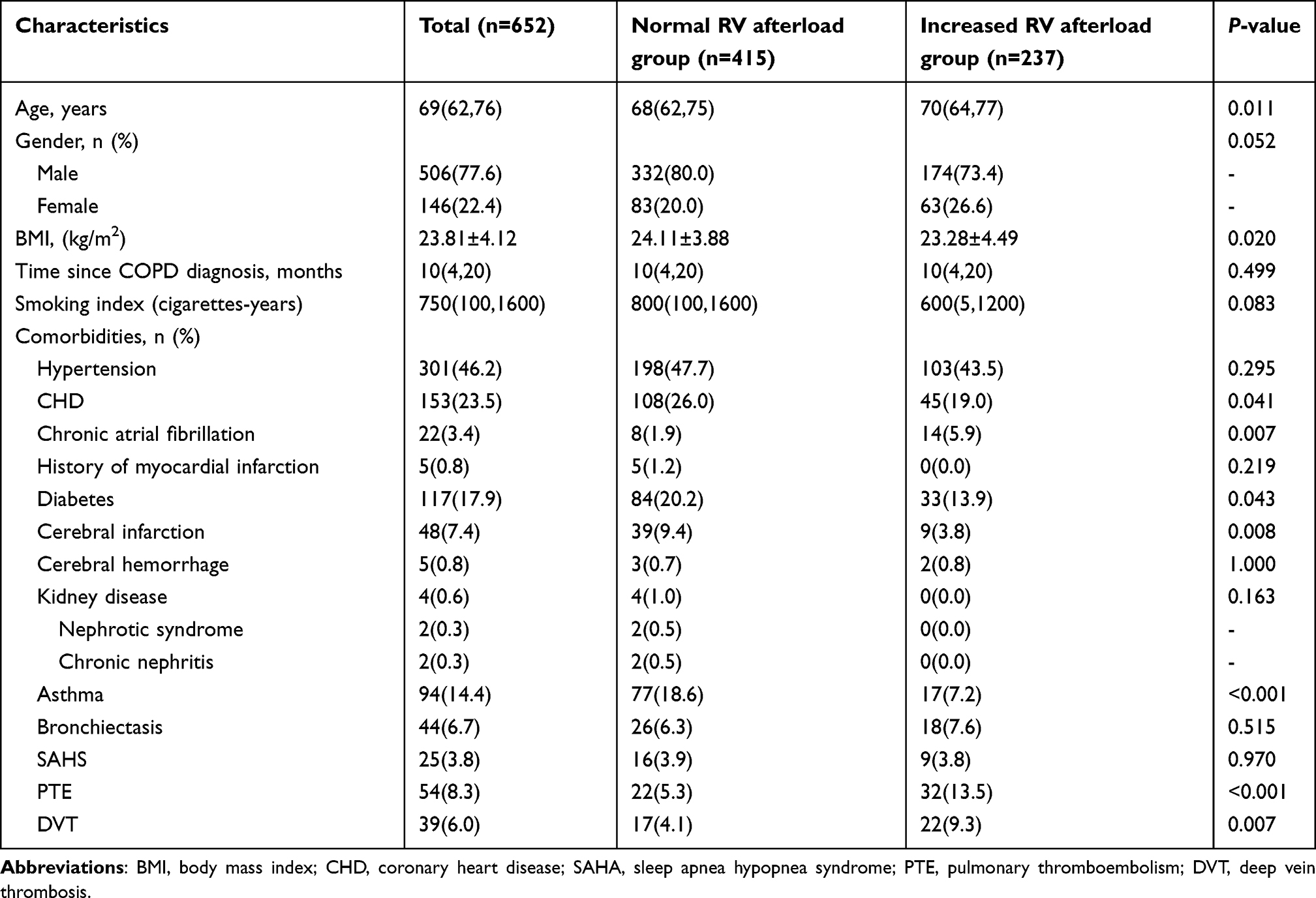 |
Table 1 Baseline Characteristics of the Study Population |
The most frequently reported symptom among all patients was sputum (90.3%), followed by dyspnea (73.5%) and chest distress (48.8%). A comparative analysis of symptoms and clinical signs indicated statistically significant differences between the groups in the prevalence of fever, moist crackles, and edema in the lower extremities. Notably, bilateral lower limb edema was the most common presentation in the increased RV afterload group, affecting 27% of these patients, which was significantly higher than the incidence of either unilateral left or right lower limb edema (Table 2).
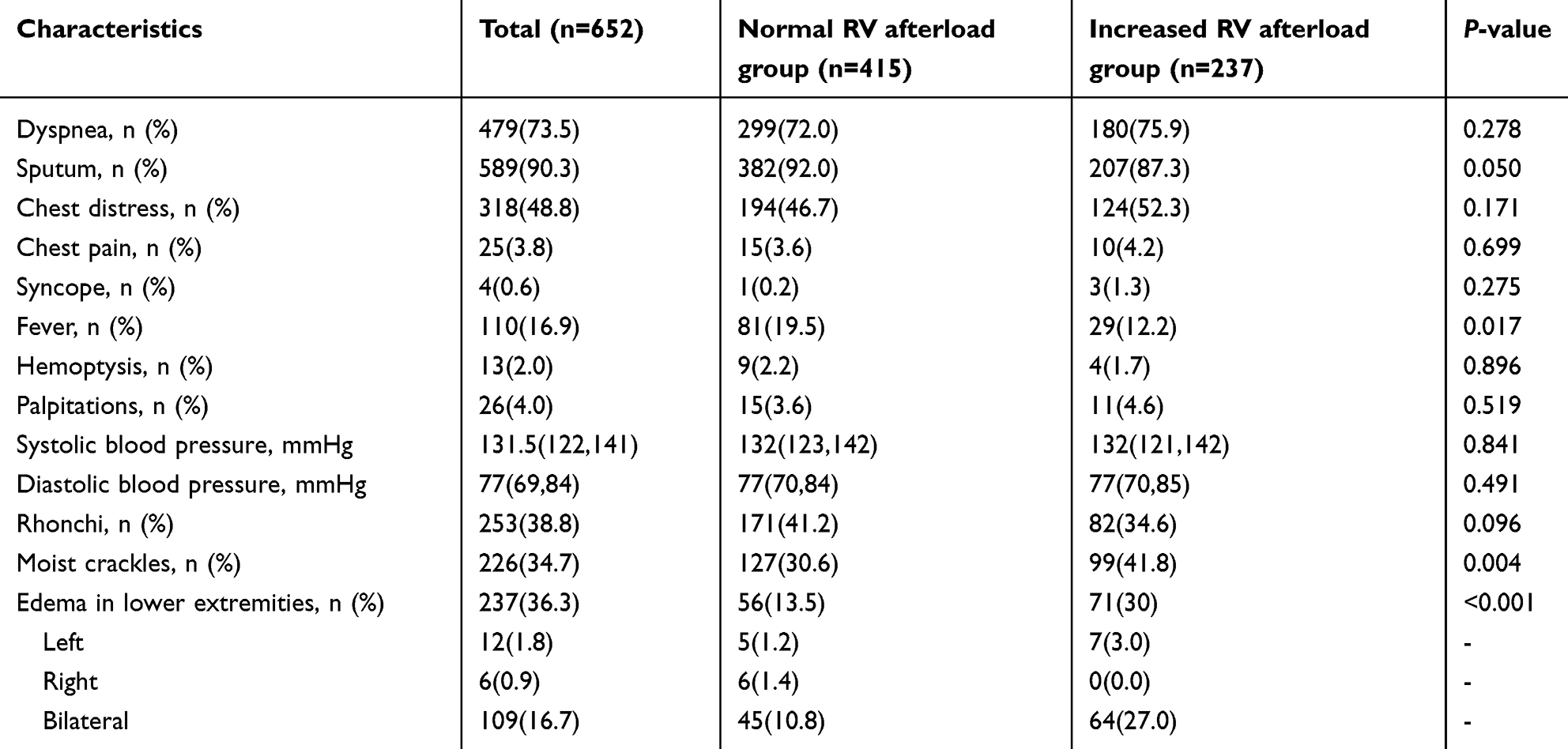 |
Table 2 Clinical Manifestations of the Study Population |
In the analysis of echocardiographic parameters, patients in the increased RV afterload group demonstrated significantly higher instances of TAPSE values less than 18 mm and greater RV wall thickness when compared to those in the normal RV afterload group. These differences were statistically significant (P<0.05, Table 3).
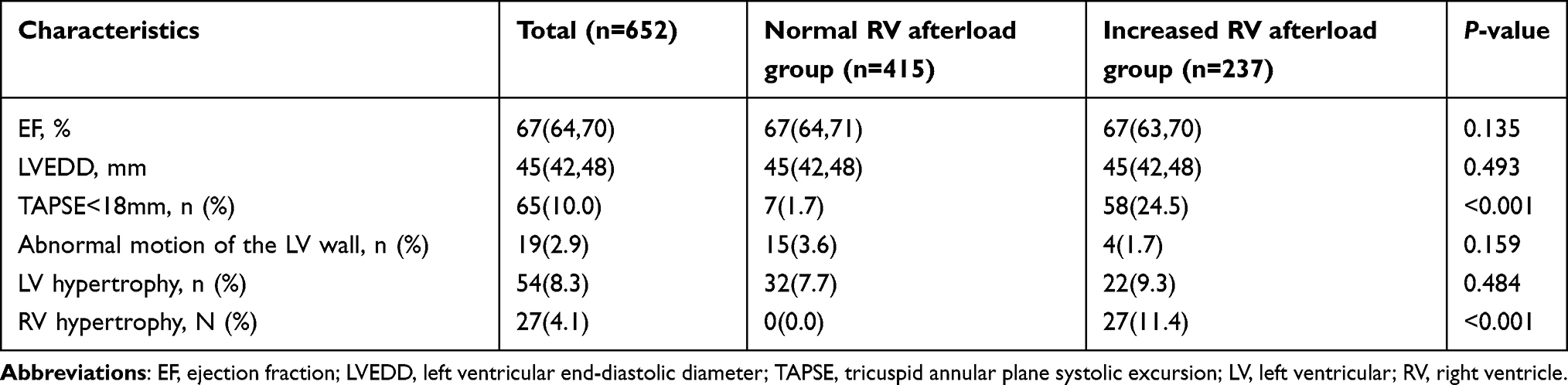 |
Table 3 Echocardiographic Data of the Study Population |
Compared to the normal RV afterload group, patients in the increased RV afterload group exhibited decreased levels of WBC, PLT, TG, GLU, PaO2 and FEV1. Conversely, levels of D-dimer, NT-proBNP/BNP and PaCO2 were significantly elevated in this group (P<0.05). There were no significant differences in the levels of other laboratory indicators (P<0.05) as shown in Table 4.
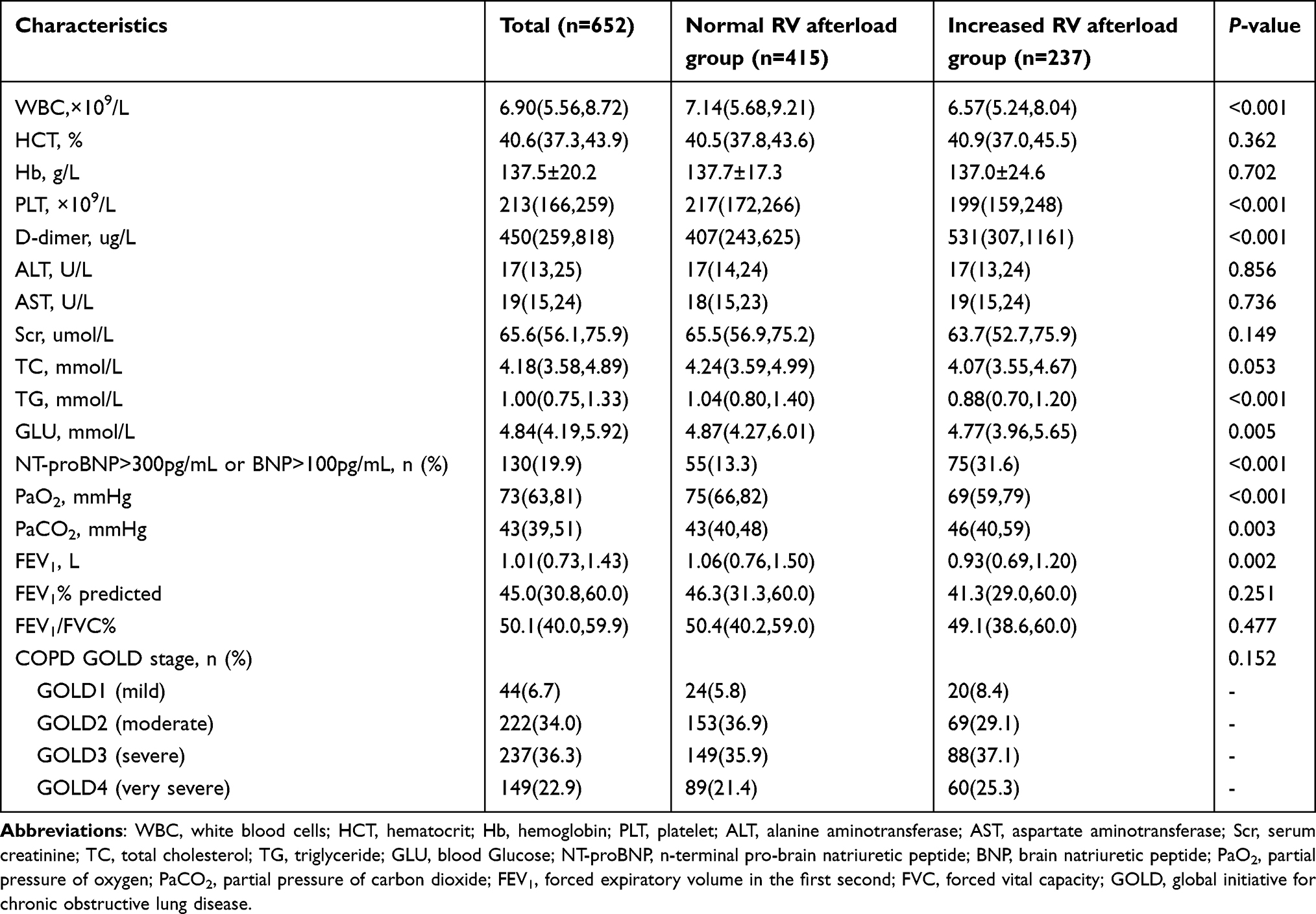 |
Table 4 Laboratory and Pulmonary Function Tests of the Study Population |
Additionally, the distribution of GOLD stages did not differ significantly between the two groups (P=0.152; Table 4).
Comparison of Survival Curves Between the Increased RV Afterload Group and the Normal RV Afterload Group
The survival of patients in the increased RV afterload group progressively declined over time, with survival rates at 12 months, 24 months, and 36 months recorded at 91.5%, 84.6%, and 77.2%, respectively. In contrast, the normal RV afterload group maintained higher survival rates of 96.1%, 95.9%, and 90.5% at the corresponding time intervals. Kaplan-Meier and log-rank analyses were employed to evaluate these trends, confirming that the survival curves for the increased RV afterload group were significantly worse than those for the normal RV afterload group (P<0.001, Figure 2).
 |
Figure 2 Kaplan-Meier survival curves for increased RV afterload group were 91.5%, 84.6% and 77.2% in 12-month, 24-month and 36-month, respectively, compared with 96.1%, 95.9% and 90.5% in the normal RV afterload group (Log Rank test, P<0.001). |
Analysis of Risk Factors Related to 3-Year All-Cause Mortality in Patients with AECOPD
Univariable Cox regression analyses for all candidate variables are presented in Supplementary Table S2. Based on clinical relevance, five variables (age, BMI, PTE, increased RV afterload, and NT-proBNP/BNP) were entered into the multivariable Cox model (Table 5). The proportional hazards assumption was tested using time-dependent covariates; no violation was detected (Age P=0.998, BMI P=0.146, PTE P=0.256, RV afterload P=0.098, NT-proBNP/BNP P=0.386); events per variable=18.4 (92 deaths/ 5 covariates). The results from the multivariate analysis indicated that increased RV afterload, elevated level of BNP or NT-proBNP, and decreased BMI were independent risk factors for 3-year all-cause mortality. Notably, the risk of mortality for patients with increased RV afterload was more than double that of patients with normal RV afterload, highlighting its significant impact on prognosis (Table 5).
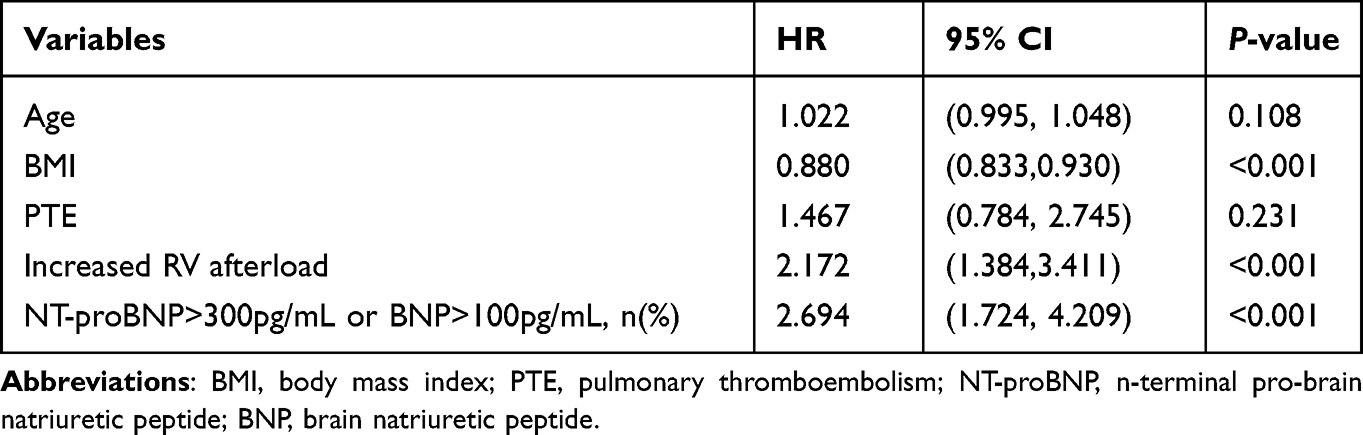 |
Table 5 Prognostic Factors for All-cause Mortality in the Hospitalized AECOPD Patients |
A sensitivity analysis excluding patients with PTE yielded consistent results (HR 2.307, 95% CI 1.436–3.707, P<0.001), compared with the main analysis (HR 2.172, 95% CI 1.384–3.411, P=0.001)
Discussion
Our study demonstrated that AECOPD patients with increased RV afterload had a significantly lower survival rate and a 2.2-fold higher risk of 3-year all-cause mortality compared to those with normal RV afterload. Factors independently associated with an increased risk of 3-year mortality in hospitalized AECOPD patients included increased RV afterload, elevated levels of BNP or NT-proBNP, and decreased BMI.
A previous study11 suggested that the cardiac function and structure were similar between patients with recent AECOPD (30 days post-exacerbation) and patients with stable COPD (for at least three months). Our study, however, focused exclusively on patients admitted with acute exacerbations, indicating that the cardiac changes we observed might be transient, appearing within the initial one-month hospitalization period. Interestingly, in the group with increased RV afterload, mortality rates did not differ significantly between patients with and without RV wall thickness (χ2=0.000, P=0.985). Given that RV wall thickness typically indicates chronic RV afterload, this finding indirectly suggests that the elevated mortality risk associated with increased RV pressure may not solely result from chronic RV afterload. Other contributing factors, such as transient increases in afterload, may also play a role. However, this condition was often overlooked by clinicians. Our study highlighted that increased RV afterload in hospitalized AECOPD patients led to a poor prognosis, with the risk of death more than doubling, even in cases of short-term afterload elevation.
RV afterload may contribute to significant changes in RV morphology and function, characterized by two compensatory mechanisms: adaptive remodeling, which involves hypertrophy and increased myocardial contractility, while maintaining chamber volume and function, and maladaptive remodling, which results in overstretching of RV cardiomyocytes and dilatation, eventually may lead to exhaustion of compensatory mechanisms, increased cardiac volumes, and heart failure.12,13 This distinction is crucial as most patients with COPD exhibit some degree of RV dysfunction,14 which is associated with a higher risk of major cardiovascular events even in mild stages of the disease.15 The significant alter on the size, thickness, wall motion, and both systolic and diastolic functions of the ventricles and atria caused by COPD markedly affects patients’ quality of life and prognosis.16 Our study further demonstrated that the survival time of AECOPD patients with increased RV afterload group was relatively shorter compared to those with normal RV afterload.
Moreover, in our study, we found that elevated levels of BNP/NT-proBNP were closely related to the prognosis of patients with AECOPD, serving as an independent risk factor for mortality. High levels of these biomarkers should be promptly addressed to mitigate poor outcomes.
Supporting our observations, Mohammed et al17 highlighted the predictive value of BNP for cardiac functions in COPD patients, noting that the significantly high level of BNP might be associated with increased ventricular overload and the stimulation secretion from left and right ventricular muscle; further, plasma BNP level was positively correlated with heart function classification grade in patients with COPD;18 similarly, Su et al19 indicated that NT-proBNP levels, which increase with cardiac burden, effectively reflect the severity of pulmonary hypoxia, inflammation, and cardiovascular stress, especially during acute exacerbations compared to stable phase.20 These findings align with our result demonstrating that BNP/NT-proBNP, as cardiac biomarkers, play a crucial role in predicting long-term health outcomes in AECOPD patients, with elevated NT-proBNP levels linked to an increased all-cause mortality risk.21,22 As these biomarkers are primarily synthesized by cardiomyocytes in response to increased RV afterload, they served as valuable clinical indicators, providing a simple, reliable, and easily accessible tool for reflecting RV afterload and monitoring disease progression in AECOPD patients.
In addition, our findings indicated that lower BMI is associated with poor prognosis and acts as an independent risk factor for mortality in patients with AECOPD. This aligns with the results of a prospective cohort study,23 which followed Chinese adults over an average of 10.1 years and found that a low BMI (<18.5 kg·m−2) significantly increased the risk for COPD. Additionally, extensive research24–27 has consistently showed that low BMI in patients with COPD is often associated with adverse outcomes, including increased mortality rates, more frequent exacerbation, and decreased lung function. These findings are further supported by Wada et al,28 who identified potential mechanisms linking low BMI with higher COPD mortality, such as accelerated lung aging from chronic smoke exposure and reduced physiological reserves in underweight patients. Additionally, underweight patients may exhibit lower resistance and are more prone to experience complications or comorbidities. Taeyun Kim et al29 further elucidated that a decrease in BMI was associated with an increased risk of all-cause mortality in a dose-dependent manner in COPD patients over a three-year follow-up period. This association extended beyond pulmonary disease, as a lower BMI correlates with a higher risk of mortality in patients with acute and chronic heart failure.30,31 Collectively, these studies underscore the critical need of regular BMI monitoring and comprehensive nutritional interventions in this vulnerable population.
Our study demonstrated that increased RV afterload does not correlate directly with the severity of COPD as assessed by GOLD stages. This finding suggests that higher GOLD grades do not necessarily imply greater RV afterload. Due to the variability and heterogeneity of COPD’s clinical manifestations, the severity of the disease may not consistently align with the level of PH.32 For example, a prospective French multicenter cohort study revealed that a small subgroup of COPD patients with severe PH only exhibited moderate airway obstruction.33
Of note, the prevalence of PTE was significantly higher in the increased RV afterload group (13.5% vs. 5.3%). Since PTE can independently elevate RV afterload and increase mortality risk, it could theoretically act as a confounder. However, in our multivariable Cox regression analysis, PTE was not independently associated with the outcome (p>0.05), and adjusting for PTE did not materially alter the association between increased RV afterload and mortality. Thus, PTE did not serve as an independent confounder in this study.
Our study possesses several notable strengths. The relatively long follow-up period and the use of a multicenter database enhance the generalizability of our findings. Additionally, echocardiography’s widespread applicability allows it to be readily implemented in most hospital settings. Echocardiography plays a crucial role in screening for suspected PH and demonstrates high discriminative value in routine clinical practice.34 It is utilized to assess structural and functional changes in the heart in patients with AECOPD, providing non-invasive, rapid, and reliable parameters. This facilitates early monitoring and identification of abnormalities, which could potentially enable timely interventions and be associated with improved patient prognosis.
We acknowledge that echocardiography is operator-dependent, and potential measurement variability across different hospitals could affect the results. To address this, we implemented uniform training and developed a standard operating manual to minimize heterogeneity across study sites. These measures help ensure the reliability of our echocardiographic parameters.
Although right heart catheterization (RHC) remains the gold standard for diagnosing PH, it is not routinely recommended for COPD patients due to its invasive nature. Moreover, during acute exacerbations of COPD, infection, cardiac insufficiency, or PTE can transiently increase right heart load, making RHC potentially inappropriate for all patients. Instead, echocardiographic parameters effectively capture changes in RV morphology and function, serving as a non-invasive, convenient, and valuable screening tool for COPD prognosis.35 Our study shows that early echocardiographic assessment of RV afterload may aid risk stratification in AECOPD patients. Intensified monitoring in those with elevated RV afterload may help identify patients at higher risk of long-term mortality, potentially adding a hemodynamic prognostic indicator, However, external validation in other populations and prospective studies are needed before clinical implementation.
Our study has certain limitations. First, restricting the analysis to patients with complete echocardiography data may introduce selection bias and limit the strength of our findings. Second, echocardiography was not performed during the follow-up period, raising the possibility that RV afterload observed during AECOPD may have normalized by the time of follow-up. This suggests that transient increases in RV afterload during acute exacerbations could still contribute to poor prognosis. Third, our study was observational with baseline differences between groups (eg., age and comorbidities). Although multivariable adjustment, residual confounding cannot be ruled out. Also, given the observational design, our findings should be interpreted as hypothesis-generating rather than causal. Fourth, since the research was conducted in a single country, our findings have limited general applicability.
Conclusion
Our study has established that increased RV afterload during hospitalization in patients with AECOPD correlates with a significantly elevated rate of 3-year all-cause mortality. This condition also serves as an independent risk factor for long-term mortality, adding incremental hemodynamic value. Additionally, our findings indicate that elevated levels of BNP or NT-proBNP, alongside with low BMI, are independent risk factors for mortality in hospitalized patients with AECOPD. Our analysis underscores the potential importance of early detection and management of these risk factors may be associated with improved long-term prognosis of hospitalized patients with AECOPD. RV afterload assessed by admission echocardiography may aid in identifying high-risk patients, guiding closer monitoring of right heart function alongside managing cardiac stress and nutritional deficiencies.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author (Yuanhua Yang) upon reasonable request.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki, and has been approved by the ethics committee of Beijing Chao-Yang Hospital, Capital Medical University (Approval Number: 2017-3-14-3). In addition, Written informed consent was obtained from all recruited participants.
Acknowledgments
Thanks to participating multiple hospitals: Beijing Chao-Yang Hospital, Beijing Daxing District People’s Hospital, The Second Hospital of Hebei Medical University, Beijing Fangshan District Liangxiang Hospital, Tongji Hospital, Shanxi Bethune Hospital, Fuwai Hospital, Beijing Sixth Hospital, The First Affiliated Hospital of Nanchang University, Shenzhen People’s Hospital, Peking University International Hospital.
We thank Fuwai Hospital, the lead center of the multicenter project under which this study was conducted. The authors have a research collaboration with Fuwai Hospital but no employment, affiliation, or financial relationship.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
S. Yang is supported by the Beijing High-Level Innovation and Entrepreneurship Talent Support Program-Healthcare Platform young top talent projects (G202521115), National Research Program for Prevention and Management of Pulmonary Embolism and Deep Venous Thrombosis (Y096). Y. Yang is supported by the Clinical research and transformation research (2022-NHLHCRF-LX-01), the National Key Research and Development Program (2023YFC2507202). The funders played no role in the design, conduct, data collection, analysis or interpretation of the study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2023 report) [EB/OL]. Available from: http://goldcopd.org/2023-gold-report-2/.
2. Boehm A, Pizzini A, Sonnweber T, et al. Assessing global COPD awareness with Google trends. Eur Respir J. 2019;53(6):1900351. doi:10.1183/13993003.00351-2019
3. Zhu B, Wang Y, Ming J, Chen W, Zhang L. Disease burden of COPD in China: a systematic review. Int J Chron Obstruct Pulmon Dis. 2018;13:1353–12. doi:10.2147/COPD.S161555
4. Almagro P, Boixeda R, Diez-Manglano J, Gómez-Antúnez M, López-García F, Recio J. Insights into chronic obstructive pulmonary disease as critical risk factor for cardiovascular disease. Int J Chron Obstruct Pulmon Dis. 2020;15:755–764. doi:10.2147/COPD.S238214
5. Cuthbert JJ, Kearsley JW, Kazmi S, et al. The impact of heart failure and chronic obstructive pulmonary disease on mortality in patients presenting with breathlessness. Clin Res Cardiol. 2019;108(2):185–193. doi:10.1007/s00392-018-1342-z
6. Kabir MA, Haque SD, Baker DA, et al. Study on association between echocardiographic findings in COPD patients with severity of COPD. Mediscope. 2020;7(1):44–50. doi:10.3329/mediscope.v7i1.47139
7. Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2016 report). Available from: https://goldcopd.org/past-gold-reports/. Accessed March 10, 2017.
8. Humbert M, Kovacs G, Hoeper MM, et al. 2022 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J. 2022;43(38):3618–3731. doi:10.1093/eurheartj/ehac237
9. Movahed MR, Ramaraj R, Manrique C, Hashemzadeh M. Left ventricular hypertrophy is independently associated with all-cause mortality. Ame J Cardiovascu Dis. 2022;12(1):38–41.
10. Bhattacharya PT, Shams P, Ellison MB. Right ventricular hypertrophy. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024.
11. Pereira MBDCM, Castello-Simões V, Heubel AD, et al. Comparing cardiac function and structure and their relationship with exercise capacity between patients with stable COPD and recent acute exacerbation: a cross-sectional study. J Bras Pneumol. 2022;48(5):e20220098.
12. Llucià-Valldeperas A, de Man FS, Bogaard HJ. Adaptation and maladaptation of the right ventricle in pulmonary vascular diseases. Clin Chest Med. 2021;42(1):179–194. doi:10.1016/j.ccm.2020.11.010
13. Rako ZA, Kremer N, Yogeswaran A, et al. Adaptive versus maladaptive right ventricular remodeling. ESC Heart Fail. 2023;10(2):762–775.
14. Nasir SA, Singh S, Fotedar M, Chaudhari SK, Sethi KK. Echocardiographic evaluation of right ventricular function and its role in the prognosis of chronic obstructive pulmonary disease. J Cardiovascu Echography. 2020;30(3):125–130. doi:10.4103/jcecho.jcecho_10_20
15. Armentaro G, Pelaia C, Cassano V, et al. Association between right ventricular dysfunction and adverse cardiac events in mild COPD patients. Eur J Clin Invest. 2023;53(2):e13887. doi:10.1111/eci.13887
16. Celeski M, Segreti A, Polito D, et al. Traditional and advanced echocardiographic evaluation in chronic obstructive pulmonary disease: the forgotten relation. Am J Cardiol. 2024;217:102–118.
17. Mohammed RA, Mohamed LA, Abdelsalam EM, et al. Assessment of cardiac dysfunction in patients with chronic obstructive pulmonary disease (COPD): a cross-sectional study. Cureus. 2023;15(5):e39629.
18. Guo HJ, Jiang F, Chen C, Shi JY, Zhao YW. Plasma brain natriuretic peptide, platelet parameters, and cardiopulmonary function in chronic obstructive pulmonary disease. World J Clin Cases. 2021;9(36):11165–11172.
19. Su X, Lei T, Yu H, et al. NT-proBNP in different patient groups of COPD: a systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2023;18:811–825. doi:10.2147/COPD.S396663
20. Tian F, Song W, Wang L, et al. NT-pro BNP in AECOPD-PH: old biomarker, new insights-based on a large retrospective case-controlled study. Respir Res. 2021;22(1):321. doi:10.1186/s12931-021-01917-3
21. Pavasini R, Tavazzi G, Biscaglia S, et al. Amino terminal pro brain natriuretic peptide predicts all-cause mortality in patients with chronic obstructive pulmonary disease: systematic review and meta-analysis. Chron Respir Dis. 2017;14(2):117–126. doi:10.1177/1479972316674393
22. Li H, Zeng Z, Cheng J, et al. Prognostic role of NT-proBNP for in-hospital and 1-year mortality in patients with acute exacerbations of COPD. Int J Chron Obstruct Pulmon Dis. 2020;15:57–67. doi:10.2147/COPD.S231808
23. Li J, Zhu L, Wei YX, et al. Association between adiposity measures and COPD risk in Chinese adults. Eur Respir J. 2020;55(4):1901899. doi:10.1183/13993003.01899-2019
24. Shin SH, Kwon SO, Kim V, et al. Association of body mass index and COPD exacerbation among patients with chronic bronchitis. Respir Res. 2022;23(1):52. doi:10.1186/s12931-022-01957-3
25. Kim EK, Singh D, Park JH, et al. Impact of body mass index change on the prognosis of chronic obstructive pulmonary disease. Respiration. 2020;99(11):943–953. doi:10.1159/000511022
26. Baig MMA, Hashmat N, Adnan M, Rahat T. The relationship of dyspnea and disease severity with anthropometric indicators of malnutrition among patients with chronic obstructive pulmonary disease. Pak J Med Sci. 2018;34(6):1408–1411. doi:10.12669/pjms.346.15769
27. Sun Y, Milne S, Jaw JE, et al. BMI is associated with FEV1 decline in chronic obstructive pulmonary disease: a meta-analysis of clinical trials. Respir Res. 2019;20(1):236. doi:10.1186/s12931-019-1209-5
28. Wada H, Ikeda A, Maruyama K, et al. Low BMI and weight loss aggravate COPD mortality in men, findings from a large prospective cohort: the JACC study. Sci Rep. 2021;11:1531.
29. Kim T, Shin SH, Kim H, et al. Longitudinal BMI change and outcomes in chronic obstructive pulmonary disease: a nationwide population-based cohort study. Respir Res. 2024;25(1):150. doi:10.1186/s12931-024-02788-0
30. Hwang I-C, Choi H-M, Yoon YE, et al. Body mass index, muscle mass, and all-cause mortality in patients with acute heart failure: the obesity paradox revisited. Int J Heart Failure. 2022;4(2):95–109. doi:10.36628/ijhf.2022.0007
31. Nguyen HTT, Ha TTT, Tran HB, et al. Relationship between BMI and prognosis of chronic heart failure outpatients in Vietnam: a single-center study. Front Nutr. 2023;10:1251601. doi:10.3389/fnut.2023.1251601
32. García AR, Piccari L. Emerging phenotypes of pulmonary hypertension associated with COPD: a field guide. Curr Opin Pulm Med. 2022;28(5):343–351.
33. Dauriat G, Reynaud-Gaubert M, Cottin V, et al. Severe pulmonary hypertension associated with chronic obstructive pulmonary disease: a prospective French multicenter cohort. J Heart Lung Transplant. 2021;40(9):1009–1018. doi:10.1016/j.healun.2021.04.021
34. Rezende CF, Mancuzo EV, Nunes MDCP, Orrêa RA. Acurácia do Ecocardiograma Transtorácico como Método de Triagem na Prática Clínica da Investigação da Hipertensão Pulmonar. Arq Bras Cardiol. 2023;120(7):e20220461. doi:10.36660/abc.20220461
35. Aurangabadkar GM, Lanjewar AV, Jadhav US, Ali SN, Wagh PB. Evaluation of pulmonary hypertension in chronic obstructive pulmonary disease. Cureus. 2022;14(2):e21828. doi:10.7759/cureus.21828
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Body Mass Index Enhances the Associations Between Plasma Glucose and Mortality in Patients with Acute Coronary Syndrome
Wen J, He L, Du X, Ma CS
Diabetes, Metabolic Syndrome and Obesity 2022, 15:2675-2682
Published Date: 31 August 2022
Obesity Paradox in Heart Failure with Mildly Reduced Ejection Fraction
Reinhardt M, Schupp T, Abumayyaleh M, Lau F, Schmitt A, Abel N, Akin M, Rusnak J, Akin I, Behnes M
Pragmatic and Observational Research 2024, 15:31-43
Published Date: 5 March 2024
Can the ADO Index Be Used as a Predictor of Mortality from COVID-19 in Patients with COPD?
Yazar EE, Gunluoglu G, Arpinar Yigitbas B, Calikoglu M, Gulbas G, Yılmaz Demirci N, Sarioglu N, Bozkus F, Hoca NT, Ogan N, Tural Onur S, Turan MO, Kosar F, Akpinar EE, Mete B, Ozturk C
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:851-858
Published Date: 4 April 2024
Comparison of Tools for Nutrition Assessment in Stable Subjects with Chronic Obstructive Pulmonary Disease: Which is the Best Mortality Predictor in Real Clinical Practice?
Nishimura K, Kusunose M, Shibayama A, Nakayasu K
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:593903
Published Date: 16 April 2026