Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Body Mass Index Enhances the Associations Between Plasma Glucose and Mortality in Patients with Acute Coronary Syndrome
Authors Wen J, He L, Du X, Ma CS
Received 20 April 2022
Accepted for publication 28 July 2022
Published 31 August 2022 Volume 2022:15 Pages 2675—2682
DOI https://doi.org/10.2147/DMSO.S370118
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ming-Hui Zou
Jing Wen,1,2 Liu He,1 Xin Du,1 Chang-Sheng Ma1
1Department of Cardiology, Capital Medical University Affiliated Anzhen Hospital; National Clinical Research Center for Cardiovascular Diseases, Beijing, People’s Republic of China; 2Department of Geriatrics, Beijing Fengtai Hospital, Beijing, People’s Republic of China
Correspondence: Chang-Sheng Ma; Xin Du, Department of Cardiology, Beijing Anzhen Hospital, Capital Medical University, No. 2 Beijing Anzhen Road, Chaoyang District, Beijing, 100029, People’s Republic of China, Tel +86-10-84005363, Fax +86-10-84005361, Email [email protected]; [email protected]
Background: It is uncertain whether the effect of hyperglycemia on mortality among patients with acute coronary syndrome (ACS) could be adjusted by other modifiable risk factors. Greater body mass index (BMI) might enhance the effect of fasting blood glucose (FPG) on cardiovascular mortality in patients with ACS.
Methods: We retrospectively enrolled patients admitted for ACS from 2008 to 2017 in Beijing and divided them into three BMI groups (normal weight ≤ 25 kg/m2, overweight 25– 29.9 kg/m2, obese ≥ 30 kg/m2). The relationships between the blood glucose levels and all-cause or cardiovascular mortalities and their heterogeneities across the groups were analyzed using Cox regression models.
Results: A total of 8,086 patients were enrolled, with 746 all-cause and 496 cardiovascular mortalities recorded during the follow-up period. Each 1 mmol/L increase in FPG was associated with an increased risk of all-cause mortality across all groups (adjusted hazard ratio [HR] 1.06, 95% confidence interval [CI] 1.02– 1.09 for normal weight patients; adjusted HR: 1.09, 95% CI: 1.05– 1.13 for overweight patients; adjusted HR: 1.12, 95% CI: 1.03– 1.22 for obese patients), and was associated with an increased risk of cardiovascular mortality among overweight (adjusted HR: 1.10, 95% CI: 1.05– 1.14) and obese patients (adjusted HR: 1.15, 95% CI: 1.04– 1.26), which was greater (p for heterogeneity = 0.006) than the association in the normal weight group (adjusted HR: 1.03, 95% CI: 0.99– 1.08). Similar results were found among 2,537 patients with ACS diagnosed with diabetes.
Conclusion: Greater BMI enhances the effect of FPG on cardiovascular mortality among patients with ACS.
Keywords: acute coronary syndrome, mortality, fasting plasma glucose, body mass index
Background
Abnormal glucometabolic disorders were strongly associated with poor prognoses in patients with acute coronary syndrome (ACS),1–4 such as greater infarct size, higher risk of congestive heart failure, and cardiogenic shock.5 Among patients with ACS who did not know whether they had diabetes mellitus (DM), the relative risk of in-hospital mortality was 3.9 times higher in those with a fasting plasma glucose (FPG) greater than or equal to 6.1 mmol/L compared with those with an FPG lower than 6.1 mmol/L. Among patients with ACS and established DM, those with an FPG greater than or equal to 10 mmol/L had a 70% increase in the relative risk of in-hospital mortality compared with patients with a well-controlled FPG (3.9–6.1 mmol/L).5 Obesity is associated with an increased risk of insulin resistance and type 2 DM, and obesity alone or combined with hyperglycemia accelerates adverse changes in cardiovascular disease risk factors.6,7 However, evidence is still lacking on whether being overweight or obese will aggravate the adverse effects of abnormal blood glucose on the prognosis of patients with ACS. This study investigated whether effect modification might exist in the associations between FPG or glycosylated hemoglobin type A1c (HbA1c) in patients with ACS with all-cause or cardiovascular mortalities across different body mass index (BMI) groups.
Methods
Study Population
We invited 18 hospitals from Beijing, including seven secondary hospitals (providing general medical services to about 400 thousand of the local population) and 11 tertiary hospitals (typically having the greatest number of beds and providing the most comprehensive medical services) to participate in this study. From these hospitals, patients admitted with a discharge diagnosis of ACS8 from January 1, 2008, to December 31, 2017, and aged ≥18 years were included. Those who had severe non-cardiac comorbidities with a life expectancy of <12 months or died within 10 minutes after hospitalization were excluded. A total of 12,640 admitted patients with ACS were identified, including those with unstable angina pectoris, non-ST-segment elevation myocardial infarction, and ST-segment elevation myocardial infarction. There were 4,347 patients lacking FPG data and 207 whose BMI was less than 18.5 kg/m2 that were excluded. Ultimately, 8,086 patients were enrolled in this study.
Data were collected through chart reviews by trained staff. The patients’ demographic characteristics, disease history, physical examinations, laboratory examinations, echocardiographs, in-hospital treatments, and medications at discharge were recorded using well-designed case report forms as the baseline information. The first results of the FPG, HbA1c, and other laboratory tests after admission were included in the analysis. The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki. Ethical approvals were acquired from Beijing Anzhen Hospital. Informed consent was waived because this study is a retrospective study. The study was conducted with patient information strictly confidential.
Clinical Outcomes
The database was linked to the Chinese National Mortality Surveillance System in Beijing to obtain all patients’ in- and out-of-hospital survival information since admission. All-cause deaths were classified into cardiovascular and non-cardiovascular deaths. Cardiovascular deaths were defined as dying from myocardial infarction, cardiogenic shock, cardiac rupture, malignant arrhythmias, stroke, pulmonary embolism, and other causes of cardiovascular death.
Statistical Analysis
Continuous variables were presented as mean ± standard deviation (SD), normally distributed variables were compared by ANOVA, and non-normally distributed variables were compared by non-parametric tests. Categorical variables were expressed as numbers (percentages) and compared using chi-square tests among the different BMI groups (normal weight: BMI 18.5–24.9 kg/m2; overweight: BMI 25–29.9 kg/m2; obesity: BMI ≥ 30 kg/m2).
Cox regression analyses were used to estimate the adjusted hazard ratios (HR) and their 95% confidence intervals (CI) per 1 mmol/L increase of baseline FPG or different baseline HBA1c levels (normoglycemia: not diagnosed with diabetes and HbA1c < 5.7%; prediabetes: not diagnosed with diabetes and HbA1c 5.7%–6.4%; undiagnosed DM: not diagnosed with diabetes but HbA1c ≥ 6.5%; known DM group: diagnosed with diabetes) with all-cause or cardiovascular mortalities, adjusted for sex, age, Hb, creatinine clearance, left ventricular ejection fraction less than 40%, or history of congestive heart failure, DM, smoking, coronary heart disease, systolic blood pressure greater than 140/90 mmHg, or history of hypertension, ischemic stroke, aspirin or platelet P2Y12 receptor antagonist use, Angiotensin-converting enzyme inhibitor (ACEI) or Angiotensin II receptor blocker (ARB) therapies. The heterogeneity tests were conducted to explore the interaction effects of FPG or HbA1c levels on the risk of all-cause or cardiovascular mortalities across the different BMI groups. All statistical analyses were performed using SAS software, version 9.4 (SAS Institute, Cary, NC, USA). Two‐sided p values < 0.05 were deemed significant.
Results
Participant Characteristics
A total of 8,086 patients with ACS were enrolled in this study, with a median follow-up time to death or the end of follow-up of 4.1 years (interquartile range, 2.3–5.8 years). Seven hundred forty-six all-cause deaths and four hundred ninety-six cardiovascular deaths occurred during follow-up. The mean age was 63.1 ± 11.9 years for all patients, 5,515 (68%) were men, and 2,537 (31%) were diagnosed with DM. Among the normal weight (n = 3,770), overweight (n = 3,488), and obesity groups (n = 828), the mean FPG levels were 6.7 ± 2.8 mmol/L, 6.8 ± 2.8 mmol/L, and 6.9 ± 2.7 mmol/L (p < 0.05), the mean HbA1c levels were 6.7 ± 1.6%, 6.8 ± 1.6%, and 6.8 ± 1.5% (p < 0.05), and 30.8%, 31.5%, and 33.5% of the patients had a history of a DM diagnosis (p > 0.05), respectively. There were no significant differences among the three groups concerning proportions of men, current smoking, alcohol consumption, and prevalence of coronary heart disease, heart failure, DM, transient ischemic attack, and atrial fibrillation. However, with the increase of BMI across the groups, the proportion of patients with a history of hypertension and hyperlipidemia increased (p < 0.05) (Table 1).
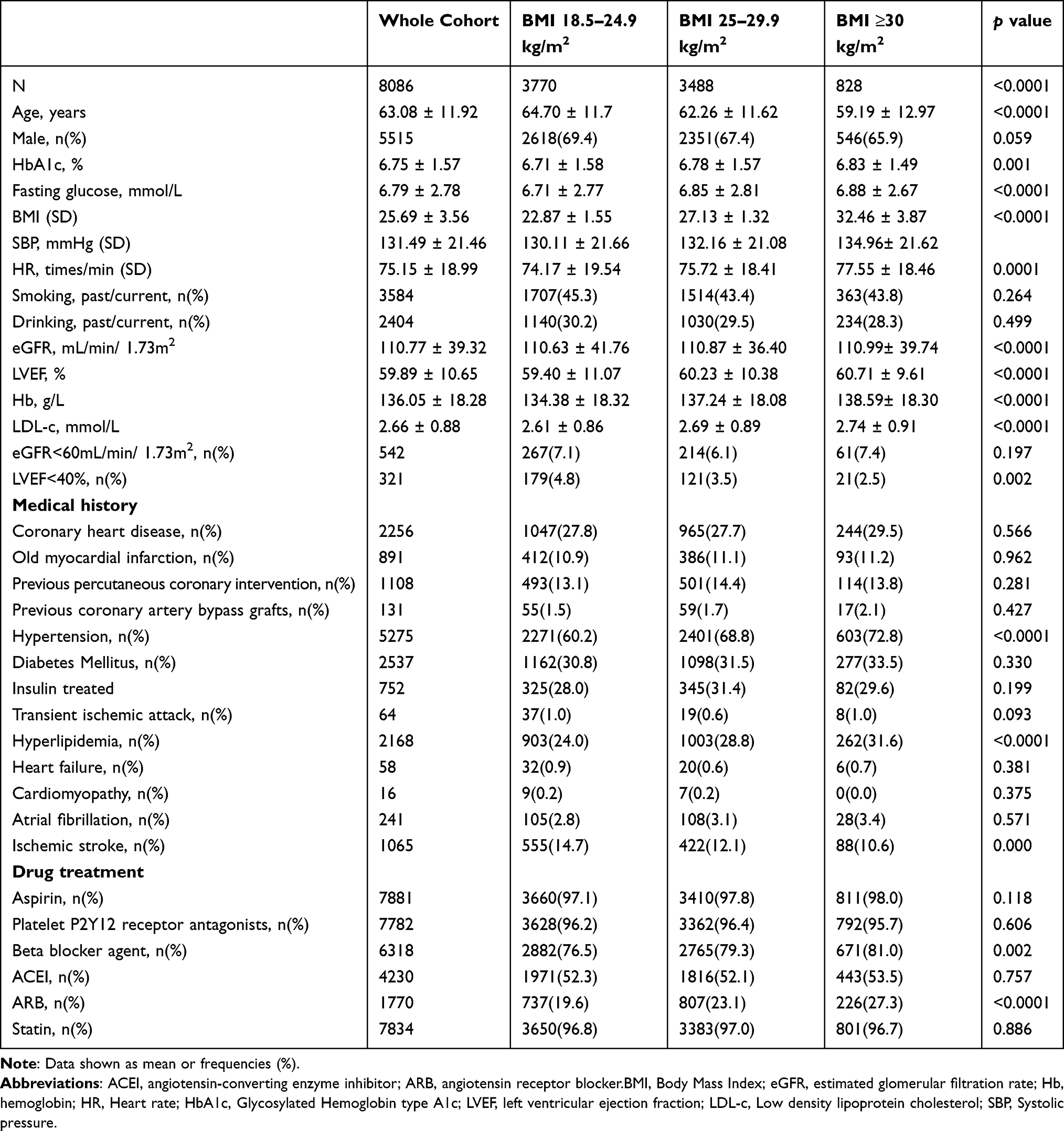 |
Table 1 Characteristics of Patients by BMI Groups |
The all-cause mortality rates were 223.5, 145.7, and 149.1 per 1,000 person-years among the normal weight, overweight, and obese patients without DM, while the mortality rates were 341.2, 300.4, and 288.4 per 1,000 person-years among the normal weight, overweight, and obese patients with DM, respectively. The cardiovascular mortality rates were 148.1, 100.4, and 106.5 per 1,000 person-years among the normal weight, overweight, and obese patients without DM, and 203.9, 210.5, and 204.7 per 1,000 person-years among the normal weight, overweight, and obese patients with DM.
Association of Fasting Blood Glucose with Mortality Across the Body Mass Index Groups
From the Cox regression models, each 1 mmol/L FPG increase was significantly associated with a greater risk of cardiovascular mortality (HR [95% CI]: 1.03 [0.99–1.08] in the normal weight group but not significant, 1.10 [1.05–1.14] in the overweight group, and 1.15 [1.04–1.26] in the obese group) and with greater risk of all-cause mortality (HR [95% CI]: 1.06 [1.02–1.09] in the normal weight group, 1.09 [1.05–1.13] in the overweight group, and 1.12 [1.03–1.22] in the obese group) after adjustment for confounders. For cardiovascular mortality in patients with diagnosed DM (HR [95% CI] 0.98 [0.93–1.05] in the normal weight group, 1.08 [1.02–1.13] in the overweight group, 1.18 [1.05–1.33] in the obese group); but for all-cause mortality: HR [95% CI] 1.04 [0.99–1.08] in the normal weight group, 1.08 [1.03–1.13] in the overweight group, and 1.14 [1.03–1.26] in the obese group). And for cardiovascular mortality in patients without diagnosed DM (HR [95% CI] 1.13 [1.06–1.20] in the normal weight group, 1.12 [1.05–1.19] in the overweight group, and 1.17 [0.94–1.45] in the obese group; but for all-cause mortality: HR [95% CI] 1.12 [1.05–1.18] in the normal weight group, 1.09 [1.03–1.16] in the overweight group, and 1.09 [0.90–1.32] in the obese group). The results of the heterogeneity tests show that the interaction effects of FPG on all-cause mortality were not statistically significant across the BMI groups; however, the interaction effects of FPG on cardiovascular mortality were statistically significant among all patients with ACS and those diagnosed with DM (Table 2, Figure 1 and 2).
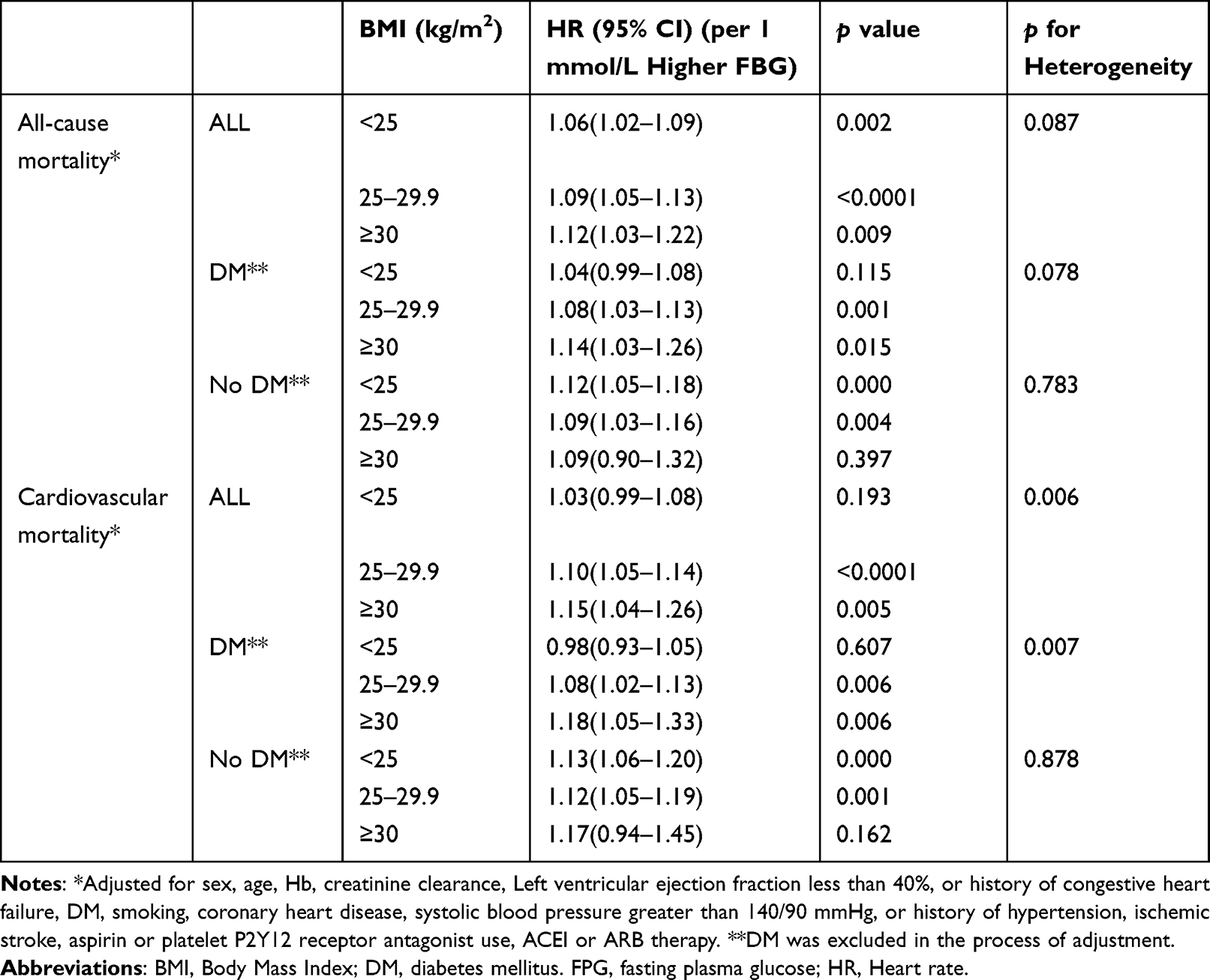 |
Table 2 Associations of FPG with All-Cause Mortality or Cardiovascular Mortality Across Different BMI Groups |
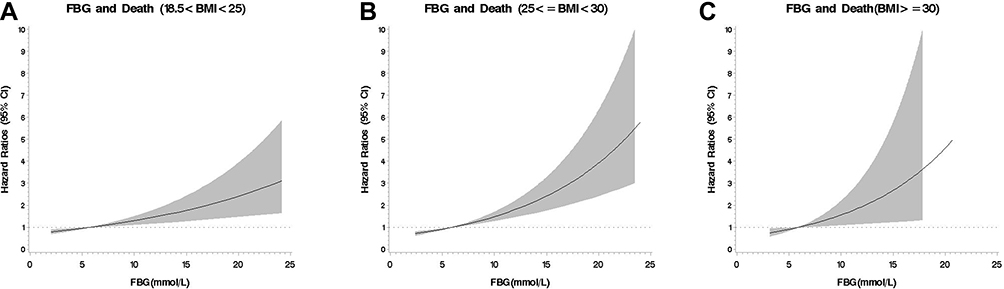 |
Figure 1 Fasting plasma glucose and all-cause death in three groups. (A) Fasting plasma glucose and all-cause death in the normal weight group (B) Fasting plasma glucose and all-cause death in the overweight group (C) Fasting plasma glucose and all-cause death in the obese group. |
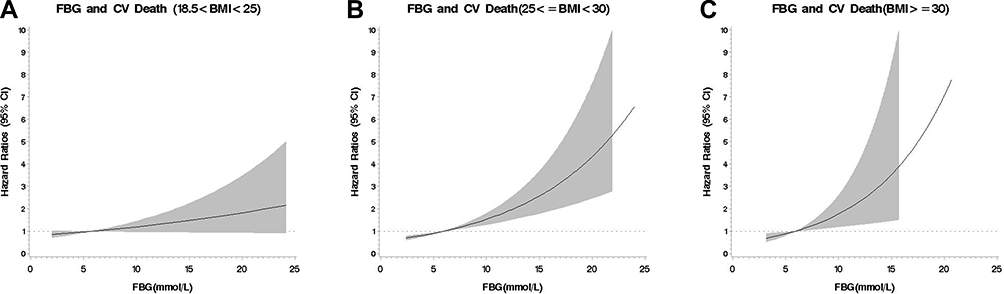 |
Figure 2 Fasting plasma glucose and cardiovascular death in three groups. (A) Fasting plasma glucose and cardiovascular death in the normal weight group (B) Fasting plasma glucose and cardiovascular death in the overweight group (C) Fasting plasma glucose and cardiovascular death in the obese group. |
Association of Glycosylated Hemoglobin Type A1c with Mortality Across the Body Mass Index Groups
In the normoglycemia group (HbA1c < 5.7%), prediabetes (HbA1c 5.7–6.4%), undiagnosed DM (with HbA1c ≥ 6.5%), and diagnosed DM were not significantly associated with a higher risk of all-cause or cardiovascular mortalities after adjustment for confounders in the normal weight group (for all-cause mortality: HR [95% CI] 1.26 [0.80–1.97], 1.54 [0.87–2.72], and 1.51 [0.99–2.31]; for cardiovascular mortality: HR [95% CI] 1.57 [0.86–2.87], 1.78 [0.84–3.78], and 1.70 [0.95–3.02]), in the overweight group (for all-cause mortality: HR [95% CI] 0.84 [0.46–1.53], 1.02 [0.51–2.02], and 1.51 [0.88–2.59]; for cardiovascular mortality: HR [95% CI] 1.07 [0.48–2.39], 1.29 [0.53–3.16], and 1.92 [0.93–3.74]), or in the obese group (for all-cause mortality: HR [95% CI] 1.16 [0.32–4.18], 1.20 [0.33–4.39], and 0.59 [0.18–2.00]; for cardiovascular mortality: HR [95% CI] 1.40 [0.33–6.00], 1.16 [0.26–5.21], and 0.72 [0.18–2.86]). The heterogeneity tests across the three BMI groups were not statistically significant (all p > 0.05) (Table 3).
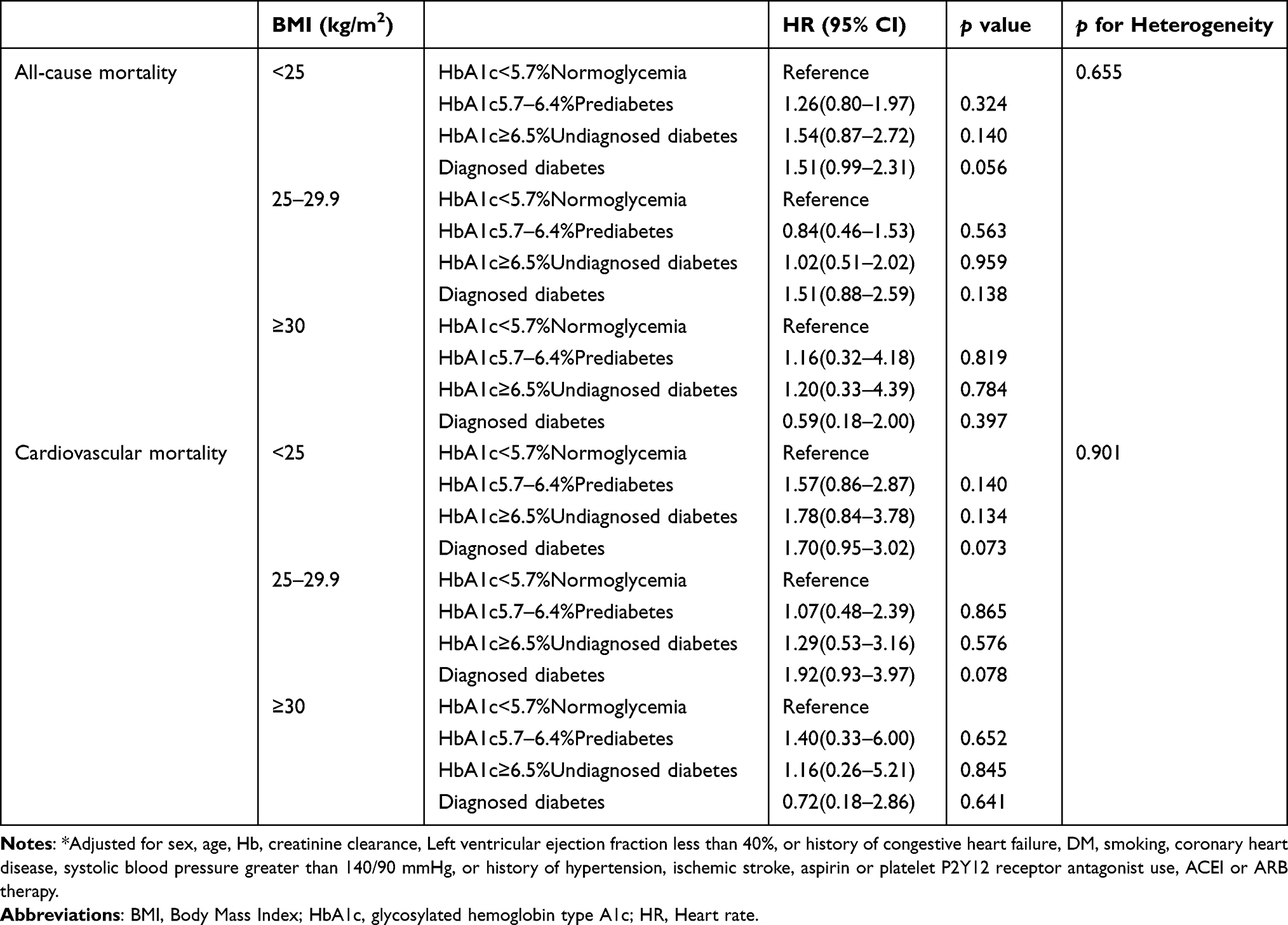 |
Table 3 Associations of HbA1c with All-Cause and Cardiovascular Mortality Across Different BMI Groups * |
Discussion
In the current study, higher FPG levels were associated with increased risks for all-cause and cardiovascular mortalities among patients with ACS after adjusting for confounders. Greater BMI enhanced the adjusted associations between FPG and cardiovascular mortality. However, compared with the normoglycemia group, prediabetes, undiagnosed (with HbA1c ≥ 6.5%), and diagnosed DM were not significantly associated with all-cause or cardiovascular mortalities in each BMI group.
Previous epidemiological studies have shown that approximately 25% to 50% of patients with acute myocardial infarction (AMI) have hyperglycemia,9 and abnormal glucometabolic disorders were strongly associated with a higher risk of cardiovascular complications.5 Obesity alone increases the absolute risk for DM and vascular disease,10 while, combined with hyperglycemia, it accelerates adverse changes in the risk profile of cardiovascular disease at an even faster speed.6,7 Previous studies have reported that higher BMI might modify the association between HbA1c and cardiovascular outcomes in patients with type 2 DM.11,12 In our study, cardiovascular mortality risks increased with higher FPG levels. The associations between FPG and cardiovascular mortality were stronger among patients with ACS and higher BMI, which indicated that being overweight or obese might modify the effect of abnormal glucometabolic disorders on adverse cardiovascular prognoses.
Several mechanisms may explain the relationship between metabolic disorders and adverse cardiovascular events. First, abnormal glucose metabolism can disrupt normal endothelial function, accelerate atherosclerotic plaque formation, and contribute to plaque rupture and subsequent thrombosis, which will increase the risk of macrovascular disease, and may also lead to infarct expansion by several maladaptive metabolic pathways.13 A study population consisted of 2450 patients with obstructive acute myocardial infarction (obs-AMI) and 239 with non-obstructive acute myocardial infarction confirm the association of hyperglycemic obs-AMI with elevated inflammatory markers and larger infarct sizes.14 Admission stress-hyperglycemia (aHGL) was identified as a strong predictor of adverse short- and long-term outcomes in both obstructive coronary arteries and non-obstructive coronary arteries, regardless of diabetes. aHGL should be considered a high-risk prognostic marker in all AMI patients.15 In hyperglycemic patients with STEMI, optimal peri-procedural glycemic control by reducing oxidative stress and inflammation may improve the outcome after PCI.16
Second, obesity might increase adverse cardiovascular events both directly and indirectly. The direct effects are mediated by obesity-induced structural and functional adaptations of the cardiovascular system to accommodate excess body weight, as well as by adipokine effects on inflammation and vascular homeostasis, leading to a proinflammatory and prothrombotic milieu. Almost all cardiovascular diseases could increase in frequency in obesity, including hypertension, coronary heart disease, heart failure, and atrial fibrillation.17 The indirect effects are mediated through the risk of metabolic syndromes such as insulin resistance, dyslipidemia, and hypertension.18 A meta-analysis that included 65 studies, which involved 516,325 participants, demonstrated that insulin resistance was a better predictor of cardiovascular disease events than fasting glucose or insulin levels in adults without DM.19 Obesity is a major driving force for insulin resistance in adipose tissue, which triggers low-grade inflammation in adipocytes and contributes to impaired glucose metabolism in skeletal muscle and the liver and low insulin secretion from pancreatic β cells, which all promote hyperglycemia. Insulin resistance alone or combined with hyperglycemia promotes adverse changes in cardiovascular disease risk factors, including atherogenic dyslipidemia and blood pressure elevation.20 Greater obesity might enhance the effect of abnormal glucometabolic disorders on adverse cardiovascular prognoses among patients with ACS.
The main advantage of this observational study is (I) a large number of patients and events; (II) the patients’ treatments in the Beijing hospitals reflects the actual situation of clinical practice, and the quality of FPG and HbA1c analyses is guaranteed; (III) follow-up data collection is based on the Chinese National Mortality Surveillance System with high quality and coverage.
Our study had several limitations. First, all participants were from China; future studies should enroll participants of other ethnic groups. Second, our study did not collect data on central obesity assessed by waist circumference. Several studies have shown that central obesity assessed by waist circumference or waist-to-hip ratio was an important risk factor for long-term mortality among patients with AMI21,22 or coronary heart disease at baseline.23 Third, although we adjusted for some common comorbidities, including hypertension, old myocardial infarction, ischemic stroke, and DM, we could not adjust the severity of the disease further because the ACS registry did not collect relevant data. In addition, some patients may have been admitted with undiagnosed DM or impaired glucose tolerance but were enrolled in the DM-free group.
Conclusion
This large observational study of patients with ACS in clinical practice showed a gradual increase in the risk of cardiovascular mortality with elevated FPG values. With an increase in BMI, cardiovascular mortality was more strongly influenced by FPG. This means that strict control of plasma glucose is critical in obese and overweight patients with ACS. Keeping blood glucose and body weight well-controlled might be more effective in improving patients with ACS prognoses than only keeping blood glucose under control.
Abbreviations
ACS, acute coronary syndrome; BMI, body mass index; FPG, fasting plasma glucose; HbA1c, glycosylated hemoglobin type A1c; DM, diabetes mellitus; OMI, old myocardial infarction; HR, hazard ratio; CI, confidence interval; STEMI, ST-segment elevation myocardial infarction; ACEI, angiotensin converting enzyme inhibitors; ARB, angiotensin receptor blocker; AMI, acute myocardial infarction; CHD, coronary heart disease; UAP, unstable angina pectoris.
Funding
This work was supported by the National Key Research and Development Program of China (2020YFC2004803), the National Natural Science Foundation of China (82103904) and grant from Beijing Municipal Commission of Science and Technology (D171100006817001).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Avanzini F, Mafrici A, Riva E., et al. A multicenter observational study on the management of hyperglycemia in patients with acute coronary syndrome. Nutr Metab Cardiovasc Dis. 2015;25(10):916–923. doi:10.1016/j.numecd.2015.07.007
2. Lee TF, Burt MG, Heilbronn LK, et al. Relative hyperglycemia is associated with complications following an acute myocardial infarction: a post hoc analysis of HI-5 data. Cardiovasc Diabetol. 2017;16(1):157. doi:10.1186/s12933-017-0642-3
3. Gu J, Pan JA, Fan YQ, et al. Prognostic impact of HbA1c variability on long-term outcomes in patients with heart failure and type 2 diabetes mellitus. Cardiovasc Diabetol. 2018;17(1):96. doi:10.1186/s12933-018-0739-3
4. Zheng J, Cheng J, Wang T, et al. Does HbA1c level have clinical implications in diabetic patients undergoing coronary artery bypass grafting? A systematic review and meta-analysis. Int J Endocrinol. 2017;2017:1537213. doi:10.1155/2017/1537213
5. Kosiborod M. Hyperglycemia in acute coronary syndromes from mechanisms to prognostic implications. Endocrinol Metab Clin North Am. 2018;47(1):185–202. doi:10.1016/j.ecl.2017.11.002
6. Koliaki C, Liatis S, Kokkinos A. Obesity and cardiovascular disease: revisiting an old relationship. Metabolism. 2019;92:98–107. doi:10.1016/j.metabol.2018.10.011
7. Laakso M, Kuusisto J. Insulin resistance and hyperglycaemia in cardiovascular disease development. Nat Rev Endocrinol. 2014;10(5):293–302. doi:10.1038/nrendo.2014.29
8. Collet J-P, Thiele H, Barbato E, et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021;42(14):1289–1367. doi:10.1093/eurheartj/ehaa575
9. Mansour AA, Wanoose HL. Acute phase hyperglycemia among patients hospitalized with acute coronary syndrome: prevalence and prognostic significance. Oman Med J. 2011;26(2):85–90. doi:10.5001/omj.2011.22
10. Bhupathiraju SN, Hu FB. Epidemiology of Obesity and Diabetes and Their Cardiovascular Complications. Circ Res. 2016;118(11):1723–1735. doi:10.1161/CIRCRESAHA.115.306825
11. Li W, Katzmarzyk PT, Horswell R, et al. HbA1c and all-cause mortality risk among patients with type 2 diabetes. Int J Cardiol. 2016;202:490–496. doi:10.1016/j.ijcard.2015.09.070
12. van Munster SN, van der Graaf Y, de Valk HW, et al. Effect modification in the association between glycated haemoglobin and cardiovascular disease and mortality in patients with type 2 diabetes. Diabetes Obes Metab. 2017;19(3):320–328. doi:10.1111/dom.12820
13. Liu L, Chen X, Liu Y, et al. The association between fasting plasma glucose and all- cause and cause- specific mortality by gender: the rural Chinese cohort study. Diabetes Metab Res Rev. 2019;35(4):e3129. doi:10.1002/dmrr.3129
14. Paolisso P, Foà A, Bergamaschi L, et al. Impact of admission hyperglycemia on short and long-term prognosis in acute myocardial infarction: MINOCA versus MIOCA. Cardiovasc Diabetol. 2021;20(1):192. doi:10.1186/s12933-021-01384-6
15. Paolisso P, Foà A, Bergamaschi L, et al. Hyperglycemia, inflammatory response and infarct size in obstructive acute myocardial infarction and MINOCA. Cardiovasc Diabetol. 2021;20(1):33. doi:10.1186/s12933-021-01222-9
16. Marfella R, Sasso FC, Siniscalchi M, et al. Peri-procedural tight glycemic control during early percutaneous coronary intervention is associated with a lower rate of in-stent restenosis in patients with acute ST-elevation myocardial infarction. J Clin Endocrinol Metab. 2012;97(8):2862–2871. doi:10.1210/jc.2012-1364
17. Lavie CJ, Pandey A, Lau DH, et al. Obesity and atrial fibrillation prevalence, pathogenesis, and prognosis: effects of weight loss and exercise. J Am Coll Cardiol. 2017;70(16):2022–2035. doi:10.1016/j.jacc.2017.09.002
18. Kachur S, Lavie CJ, de Schutter A, et al. Obesity and cardiovascular diseases. Minerva Med. 2017;108(3):212–228. doi:10.23736/S0026-4806.17.05022-4
19. Gast KB, Tjeerdema N, Stijnen T, et al. Insulin resistance and risk of incident cardiovascular events in adults without diabetes: meta-analysis. PLoS One. 2012;7(12):e52036. doi:10.1371/journal.pone.0052036
20. Koliaki C, Liatis S, Obesity KA. Cardiovascular disease: revisiting an old relationship. Metabolism. 2019;92:98–107.
21. Kawashiri MA, Nakanishi C, Tsubokawa T, et al. Impact of enhanced production of endogenous heme oxygenase-1 by pitavastatin on survival and functional activities of bone marrow-derived mesenchymal stem cells. J Cardiovasc Pharmacol. 2015;65(6):601–606. doi:10.1097/FJC.0000000000000231
22. Berglund L, Riserus U, Hambraeus K. Repeated measures of body mass index and waist circumference in the assessment of mortality risk in patients with myocardial infarction. Ups J Med Sci. 2019;124(1):78–82. doi:10.1080/03009734.2018.1494644
23. Coutinho T, Goel K, Corrêa de Sá D, et al. Central obesity and survival in subjects with coronary artery disease: a systematic review of the literature and collaborative analysis with individual subject data. J Am Coll Cardiol. 2011;57(19):1877–1886. doi:10.1016/j.jacc.2010.11.058
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association Between Plasma Ceramides and One-Year Mortality in Patients with Acute Coronary Syndrome: Insight from the PEACP Study
Li F, Li D, Yu J, Jia Y, Wen J, Li W, Tong Y, Wu J, Wan Z, Cao Y, Zhang Q, Zeng R
Clinical Interventions in Aging 2023, 18:571-584
Published Date: 6 April 2023
Obesity Paradox in Heart Failure with Mildly Reduced Ejection Fraction
Reinhardt M, Schupp T, Abumayyaleh M, Lau F, Schmitt A, Abel N, Akin M, Rusnak J, Akin I, Behnes M
Pragmatic and Observational Research 2024, 15:31-43
Published Date: 5 March 2024
Can the ADO Index Be Used as a Predictor of Mortality from COVID-19 in Patients with COPD?
Yazar EE, Gunluoglu G, Arpinar Yigitbas B, Calikoglu M, Gulbas G, Yılmaz Demirci N, Sarioglu N, Bozkus F, Hoca NT, Ogan N, Tural Onur S, Turan MO, Kosar F, Akpinar EE, Mete B, Ozturk C
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:851-858
Published Date: 4 April 2024
Effect of Maternal Pre-Pregnancy Body Mass Index on Longitudinal Fetal Growth and Mediating Role of Maternal Fasting Plasma Glucose: A Retrospective Cohort Study
Chen Q, He Z, Wang Y, Yang X, Liu N, Zhang S, Ma L, Shi X, Jia X, Yang Y, Sun Y, He Y
Diabetes, Metabolic Syndrome and Obesity 2024, 17:1911-1921
Published Date: 2 May 2024
Impact of Anemia and Acquired Anemia on in-Hospital Mortality of Acute Coronary Syndrome Patients

Yakut I, Dervis E
International Journal of General Medicine 2024, 17:6431-6442
Published Date: 24 December 2024