Back to Journals » Breast Cancer: Targets and Therapy » Volume 18
From Axillary Lymph Node Dissection to Sentinel Node Biopsy in Breast Cancer: A 23-Year Population-Based Large-Sample Study with Long-Term Survival Outcomes
Authors Mangone L ![]() , Marinelli F
, Marinelli F ![]() , Bisceglia I
, Bisceglia I ![]() , Braghiroli MB, Neri A, Morabito F, Pinto C, Ragazzi M, Ferrari G, Coiro S, Cenini E
, Braghiroli MB, Neri A, Morabito F, Pinto C, Ragazzi M, Ferrari G, Coiro S, Cenini E
Received 31 October 2025
Accepted for publication 4 February 2026
Published 17 April 2026 Volume 2026:18 573154
DOI https://doi.org/10.2147/BCTT.S573154
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Harikrishna Nakshatri
Lucia Mangone,1 Francesco Marinelli,1 Isabella Bisceglia,1 Maria Barbara Braghiroli,1 Antonino Neri,2 Fortunato Morabito,3 Carmine Pinto,4 Moira Ragazzi,5 Guglielmo Ferrari,3 Saverio Coiro,6 Eugenio Cenini6
1Epidemiology Unit, Azienda USL-IRCCS di Reggio Emilia, Reggio Emilia, Italy; 2Scientific Directorate, Azienda USL-IRCCS di Reggio Emilia, Reggio Emilia, Italy; 3Associazione “Vittorio Lodini per la Ricerca in Chirurgia” di Reggio Emilia, Reggio Emilia, Italy; 4Medical Oncology Unit, Azienda USL-IRCCS di Reggio Emilia, Reggio Emilia, Italy; 5Pathology Unit, Azienda USL-IRCCS di Reggio Emilia, Reggio Emilia, Italy; 6Breast Surgery Unit, Azienda USL-IRCCS di Reggio Emilia, Reggio Emilia, Italy
Correspondence: Lucia Mangone, Epidemiology Unit, Azienda USL-IRCCS di Reggio Emilia, Via Giovanni Amendola, 2, Reggio Emilia, 42123, Italy, Email [email protected]
Purpose: Axillary surgery in breast cancer has progressively evolved over the past decades toward less invasive approaches.
Patients and Methods: This population-based study analyzed 10,955 women diagnosed with invasive breast cancer between 2000 and 2022 in Reggio Emilia, Italy, to assess long-term trends in axillary management.
Results: A marked decline in axillary lymph node dissection (ALND) was observed—from 47.9% in 2000– 2004 to 18.1% in 2017– 2022—with a parallel increase in sentinel lymph node biopsy (SLNB) from 43.8% to 74.7%. The shift was particularly pronounced in stage I tumors, where ALND dropped from 44.7% to 2.9%. Overall survival at 15 years was significantly higher in the SLNB group (78%) compared to the ALND group (72%). These results align with major clinical trials (e.g. ACOSOG Z0011, SINODAR-ONE), confirming their applicability in unselected populations. Although ALND remained more frequent in patients with larger tumors or undergoing mastectomy, its role has substantially diminished.
Conclusion: Our findings reinforce the safety and effectiveness of conservative axillary approaches and reflect their successful implementation in real-world practice. Further research should address the impact of these trends on quality of life and incorporate additional data on radiotherapy and tumor biology to guide future surgical decision-making.
Keywords: breast cancer, axillary lymph node dissection, sentinel lymph node biopsy, population-based study, surgical de-escalation
Introduction
Breast cancer is the leading cause of cancer-related death among women worldwide.1 While incidence continues to rise in certain regions, survival rates have steadily improved due to the early detection of small tumours through screening programs and the advent of effective systemic therapies, even for biologically aggressive disease types.2
The increasing detection of smaller breast tumours underscores the need for an appropriate surgical approach, particularly with regard to accurate axillary staging.3 Historically, axillary lymph node dissection (ALND) was a cornerstone of breast cancer surgery. However, over the past decades, the management of the axilla has shifted toward a more conservative approach.4,5
Although ALND provides precise staging of axillary lymph node involvement, it is also associated with significant morbidity, including lymphedema, sensory neuropathy, restricted shoulder mobility, and chronic pain—all of which can negatively affect quality of life.6,7 As a result, sentinel lymph node biopsy (SLNB) has largely replaced ALND for staging purposes in early breast cancer.8,9
Complete axillary dissection remains the standard surgical option only for selected patients, such as those with biopsy-proven axillary metastases or in specific cases with SLN involvement. However, even the need for axillary staging itself is now being questioned in some low-risk settings, as no definitive survival benefit has been demonstrated.
Widespread use of mammographic screening has led to the diagnosis of small, early-stage tumours in the majority of patients.10,11 Among those with positive SLNs, only a minority harbor additional metastases in non-sentinel lymph nodes.12–14 Furthermore, the majority of SLN-positive patients who forgo ALND still receive adjuvant systemic therapy and/or endocrine treatment and have a low risk of locoregional recurrence.15,16
The American College of Surgeons Oncology Group (ACOSOG) Z0011 randomised clinical trial challenged the traditional role of ALND. It demonstrated that, among women with one or two metastatic sentinel lymph nodes undergoing breast-conserving surgery with whole-breast radiotherapy, omitting ALND did not adversely affect axillary recurrence, disease-free survival, or overall survival.17,18 These findings support the notion that sentinel node status now functions more as a prognostic marker than a strict surgical indication.19
As a result, ALND has been progressively abandoned in patients with clinically node-negative disease. Both the NSABP B-32 trial5 and the study by Veronesi et al8 confirmed that SLNB does not increase the risk of recurrence nor compromise survival. On the contrary, sparing the axilla can lead to improved patient outcomes by reducing treatment-related morbidity.
Consequently, in cases of sentinel lymph node micrometastases, ALND should be avoided,20,21 as it has no impact on survival and SLNB alone offers adequate locoregional control.22 Even in patients with macrometastases, the benefit of ALND remains unproven, and its use should be carefully weighed against potential harm.18,23–25
This study aims to evaluate, in a population-based setting, how the use of ALND has evolved over 23 years and to assess its impact on breast cancer survival in comparison to SLNB.
Materials and Methods
Data Sources
The data for this study were obtained from the Reggio Emilia Cancer Registry (RE-CR), which covers a population of approximately 532,000 residents. The RE-CR is recognized as a high-quality registry, with a microscopic confirmation rate of 98.8% for breast cancers and a death certificate-only (DCO) rate of less than 0.1%.26 This study includes all malignant breast tumours registered in the RE-CR from 2000 to 2022. The procedures for conducting epidemiological analyses using RE-CR data were approved by the Reggio Emilia Ethics Committee (Protocol No. 2014/0019740 of 04/08/2014).
In this study we use the hospital’s internal database, established in 1996 and recently confirmed (Resolution no. 0413 of 15/09/2025): the first author of this work is the Director of the Cancer Registry and is also responsible for data access.
The RE-CR integrates data from multiple sources, including histology reports, hospital discharge records, mortality data, primary care physician reports, and laboratory information.
Information regarding stage at diagnosis, type of surgery (quadrantectomy or mastectomy), SLN biopsy, presence of lymph node micrometastases, and ALND dissection was extracted from the medical records. Regarding the details of the surgical techniques used, in our Department of Surgical Oncology, sentinel lymph node biopsy (SLNB) was performed throughout the study period using Technetium-99m, following a standardized protocol. Axillary lymph node dissection (ALND), when performed, included Berg levels I and II, with extension to level III in case of disease involvement detected during preoperative evaluation or macroscopic disease identified intraoperatively. In 97% of cases, staging was based on pathological assessment; in the remaining 3%, clinical stage was used. Staging was performed according to the 8th edition of the TNM classification system.27 Cases were stratified by age into three groups: <50 years, 50–69 years (which corresponds to the target age group for mammographic screening in Italy), and ≥70 years.
The analyses were conducted across five periods. The first period, the longest, encompasses three intervals (2000–2004, 2005–2009, 2010–2013), corresponding to the era when the ALND was routinely performed. The second period (2014–2016) reflects the implementation of international guidelines recommending the omission of ALND in patients with micrometastatic disease.20 The third period (2017–2022) coincides with the initiation of the SINODAR-ONE trial,28 during which ALND was also avoided in patients with macrometastatic sentinel lymph nodes (pN+).
Statistical Methods
Descriptive analyses were performed to examine patient characteristics, including age at diagnosis, type of surgery, disease stage, SLN and ALN removal, and presence of micrometastases. These variables were stratified by the five predefined periods.
The distribution of ALND and SLND was also reported separately for patients with stage I disease across the five periods. Logistic regression was used to estimate odds ratios (ORs) with corresponding 95% confidence intervals (CIs) to evaluate the association between ALND on potential predictors such as age at diagnosis, disease stage, and period of diagnosis. A separate logistic regression analysis was conducted specifically for patients with stage I to assess the association of ALND with age at diagnosis, type of surgery, period of diagnosis, and tumor size (T). Overall survival was analyzed using the Kaplan-Meier method, with stratification by type of axillary surgery (ALND versus SLNB). Trends over time were evaluated by calculating the annual per cent change (APC) in age‑standardised rates using Joinpoint Regression analysis. A two-sided P-value <0.05 was considered statistically significant. All statistical analyses were performed using STATA version 16.1.
Results
Between 2000 and 2022, a total of 10,955 patients with infiltrating breast cancer were identified as residents of the province of Reggio Emilia at the time of diagnosis (Table 1). The majority of tumours (43%) were diagnosed in women aged 50–69 years, followed by 36.5% in those aged ≥70 years, and 20.6% in women under 50 years of age. Most patients (63%) underwent quadrantectomy, 24.7% underwent mastectomy, and 12.1% did not undergo surgery. Across the entire period, 49% of cases were diagnosed at stage I, 30.6% at stage II, 10.6% at stage III, and 4.7% at stage IV.
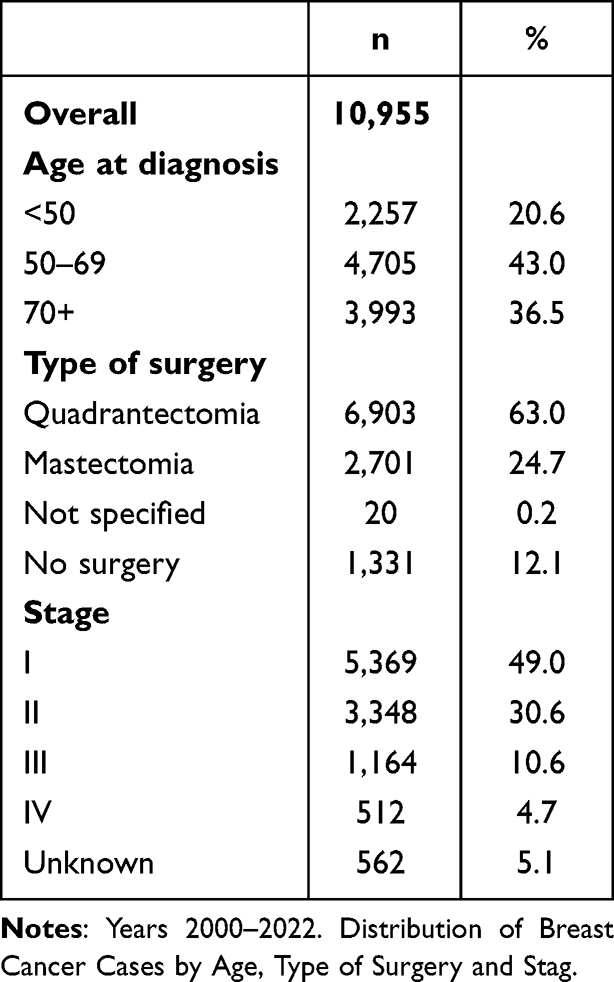 |
Table 1 Reggio Emilia Cancer Registry |
When stratified by period (Table 2), a progressive increase in the proportion of stage I tumours was observed, from 42.4% in 2000–2004 to 53.2% in 2017–2022. Concurrently, a decrease in metastatic (stage IV) cases was noted (from 5.8% to 3.8%). Surgical procedures remained largely stable over time: quadrantectomy accounted for 64.2% of procedures in 2000–2004 and 64.4% in 2017–2022, while mastectomy rates were 23.7% and 25.3%, respectively. The number of recorded micrometastases increased from zero to 105 cases over time. In parallel with the rise in early-stage diagnoses, there was an increase in node negative (N0) tumours (from 56.6% to 66.5%) and a decrease in pN1 (20% to 13.6%) and N2 (5.8% to 3.5%) tumours, while the proportion of N3 cases remained stable (0.7%).
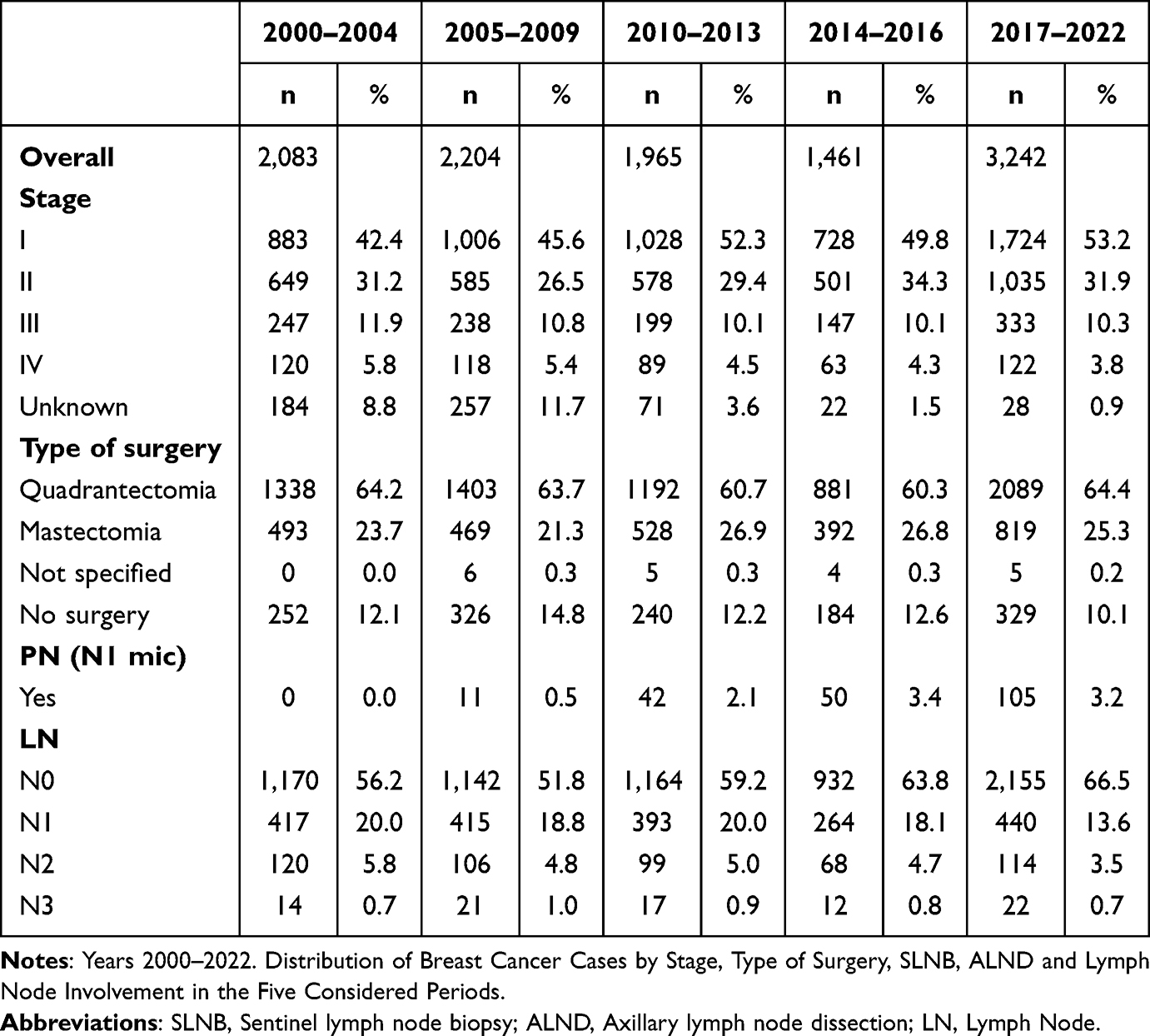 |
Table 2 Reggio Emilia Cancer Registry |
SLNB increased markedly from 43.8% in 2000–2004 to 74.7% in 2017–2022, whereas ALND declined from 47.9% to 18.1% during the same period (Table 3). Focusing on stage I, ALND was dramatically reduced from 29.3% in 2000–2004 to 1% in 2017–2022. Conversely, the proportion of the SLNB increased from 64.8% to 91.7% over the same timeframe.
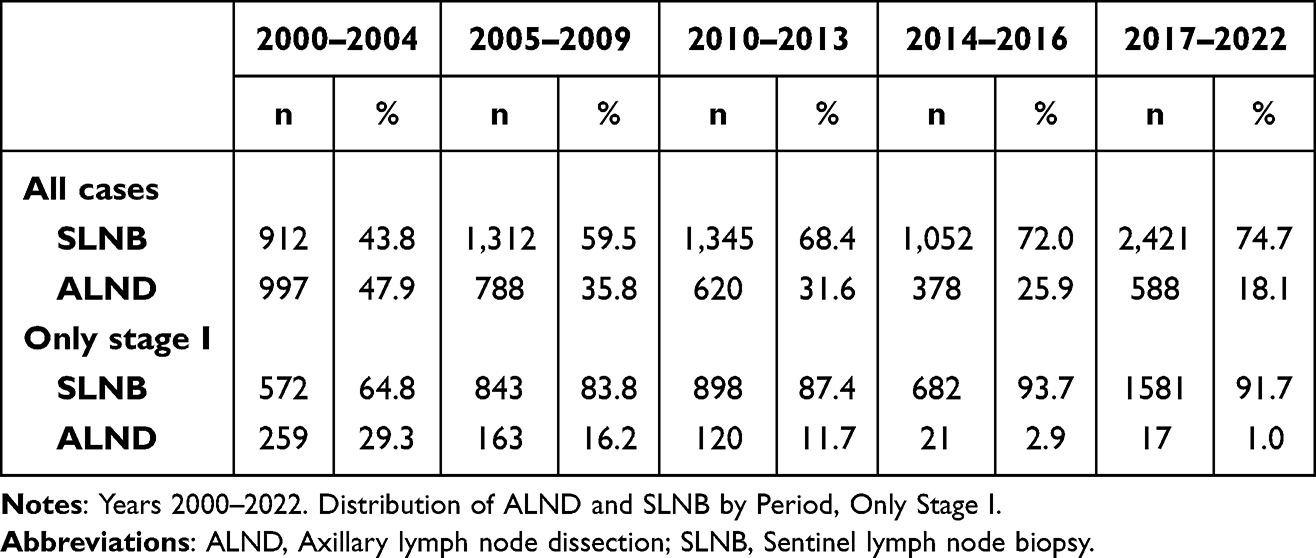 |
Table 3 Reggio Emilia Cancer Registry |
Multivariate analysis (Table 4A) showed that the likelihood of undergoing ALND significantly decreased with increasing age: women aged 50–69 years had an OR of 0.83 (95% CI 0.73–0.95) and those aged ≥70 years had an OR of 0.38 (95% CI 0.33–0.44). Conversely, the likelihood of ALND increased substantially with stage: stage II (OR 12.36; 95% CI 10.93; 13.98) and stage III (OR 54.12; 95% CI 44.85; 65.32). Across periods, the odds of undergoing ALND declined markedly, particularly in 2014–2016 (OR 0.21; 95% CI 0.18; 0.26) and even more so in 2017–2022 (OR 0.12; 95% CI 0.10; 0.14). In stage I subgroup (Table 4B), the probability of receiving ALND was significantly higher among women undergoing mastectomy (OR 3.59; 95% CI 2.81; 4.57), and among those with tumours measuring 11–20 mm (OR 1.65; 95% CI 1.14; 2.40). Conversely, the probability of ALND significantly decreased over time with a 98% reduction in 2017–2022 (OR 0.02; 95% CI 0.01; 0.03).
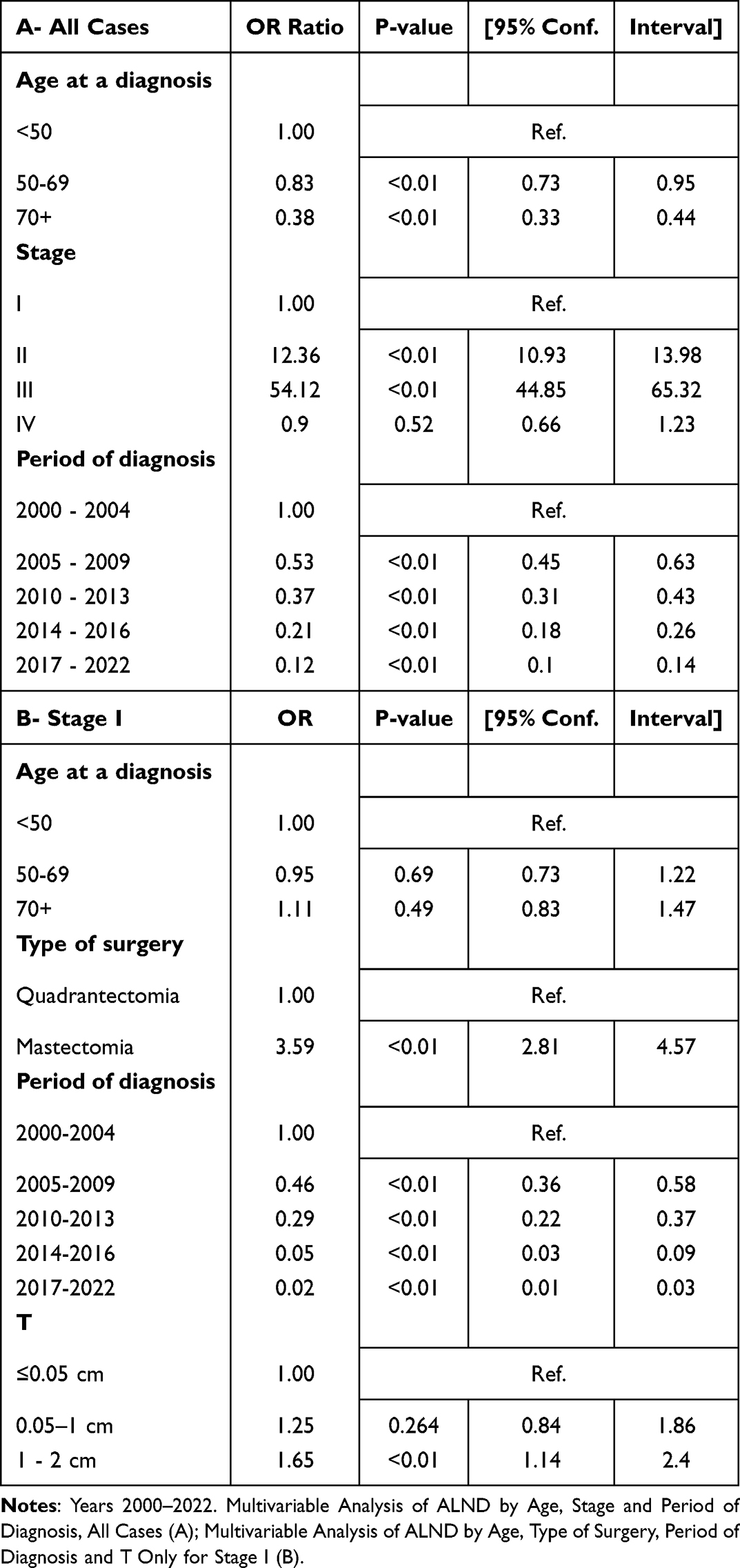 |
Table 4 Reggio Emilia Cancer Registry |
Overall survival among women with stage I breast cancer was higher for those who underwent SLNB compared to ALND (Figure 1). This survival benefit became statistically significant at 15 years of follow-up (78% for SLNB versus 72% for ALND). Finally, the epidemiological trends in breast cancer over the study period (Figure 2) showed a slight increase in incidence (APC 0.2; 95% CI 0.0; 0.3), and a significant decrease in mortality (APC −1.7; 95% CI −2.2; −1.1).
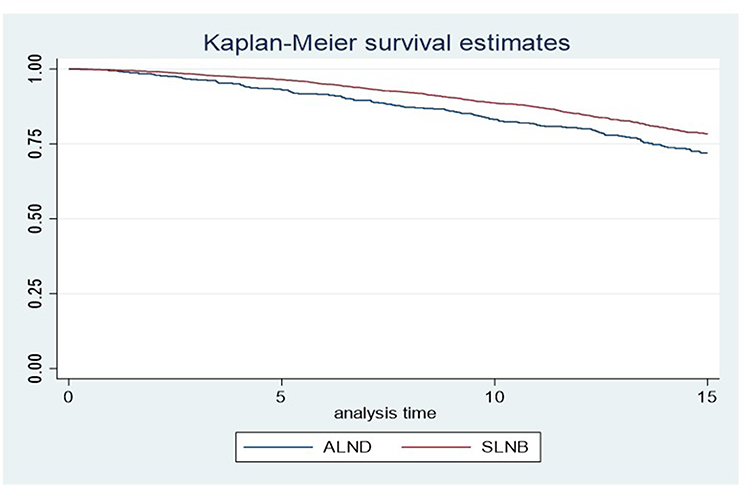 |
Figure 1 Reggio Emilia Cancer Registry. Years 2000–2022. Kaplan-Meier survival estimates by ALND and SLNB. |
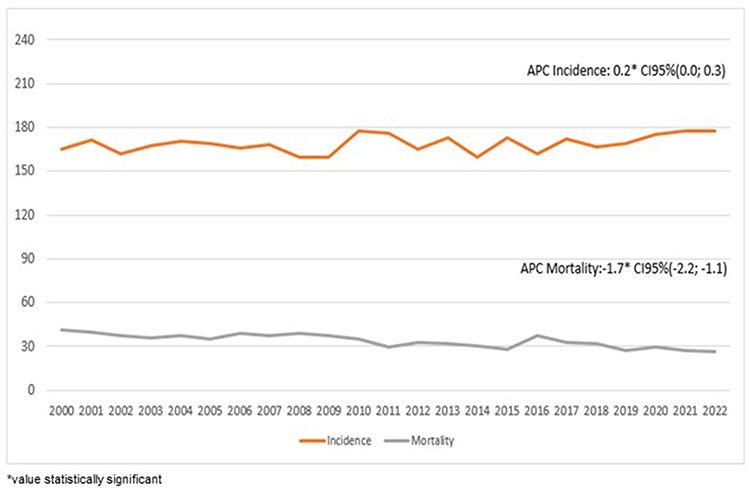 |
Figure 2 Reggio Emilia Cancer Registry. Years 2000–2022. Incidence and mortality trend and APC (Annual Percentage Change). |
Discussion
Axilla management in breast cancer has changed significantly over the past two decades, reflecting a broader shift in surgical oncology toward more conservative, evidence-based approaches. This population-based study illustrates that evolution in detail, documenting how clinical trial results and international guidelines have influenced everyday practice in a cohort of nearly 11,000 women diagnosed between 2000 and 2022.
The most striking change was the significant reduction in ALND, particularly in patients with stage I disease. This reflects a widespread adoption of recommendations from pivotal studies such as Galimberti et al20 and SINODAR-ONE,28 which promoted the safety of omitting ALND in patients with limited nodal involvement. In parallel, SLNB increased, solidifying its role as the standard axillary staging procedure.
Breast cancer is increasingly common in Western countries, with rising incidence observed particularly among younger women.29,30 Breast cancer early detection, adherence to screening programs and treatment, have improved patient outcomes.31–33
Survival has improved substantially due to widespread screening programs enabling earlier diagnosis and the availability of more effective therapies.31–33
Improvements in survival rates are most evident in areas with good adherence to mammography screening, as evidenced in our previous studies with an increase in stage I cancers (42.4% to 53.2% between 2000 and 2022) and a decrease in metastatic cancers (from 5.5% to 3.8%).11,34 Similarly, node-negative tumors (pN0) increased from 56.2% to 66.5%, while pN1 and pN2 disease decreased from 20% to 13.6% and from 5.8% to 3.5%, respectively. Interestingly, pN3 rates remained stable at 0.7%, suggesting that while early detection has improved, a small subset of aggressive tumors still present with advanced nodal involvement.
Notably, surgical treatment of the primary tumor remained relatively constant throughout the study period, with quadrantectomy consistently accounting for about 64% of procedures and mastectomy around 25%. In stage I patients, multivariate analysis showed that mastectomy was associated with a significantly higher probability of undergoing ALND (OR 3.59; 95% CI: 2.81–4.57), as was tumor size between 11–20 mm (OR 1.65; 95% CI: 1.14–2.40). However, the decision to perform a mastectomy is influenced by multiple clinical and pathological factors, such as the discrepancy between tumor size and breast volume, anatomical location, the presence of multifocal or multicentric disease, previous ipsilateral quadrantectomy, and cases in which radiotherapy is contraindicated or refused by the patient.
From an expert perspective, the strength of this study lies in its ability to track these changes over time in a non-selective cohort. Unlike clinical trials, which often include selected patient populations, this registry captures the full spectrum of clinical practice and patient variability. The fact that ALND was nearly eliminated in stage I disease—falling to just 17 cases among 581 patients (1%) in the final study period—is a powerful indicator of how thoroughly evidence has shaped surgical practice in the real world.
Importantly, this de-escalation did not negatively impact outcomes. On the contrary, overall survival among stage I patients was slightly better in those treated with SLNB than ALND, with a statistically significant advantage emerging at 15 years (78% versus 72%).
What We Know from the Literature
The gradual reduction of axillary surgery for small breast cancers began in the mid-1980s,35 with SLNB progressively introduced in the 1990s. SLNB has since become the gold standard for axillary staging in women with early-stage breast cancer and clinically negative lymph nodes, significantly improving quality of life by reducing surgical morbidity.36 The improvement could be the result of a combination of multiple factors: on the one hand, SLNB causes less post-surgical trauma and is advantageous for post-operative recovery, but it is also necessary to take into account the progress of adjuvant therapy in the treatment of breast cancer.Seminal trials such as the Krag study5 demonstrated that SLNB does not compromise survival: 8-year overall survival was 90.3% in the SLNB group compared to 91.8% in the ALND group, with no significant increase in recurrence (8 versus 14 cases, respectively). Similarly, the Veronesi study8 showed no increase in the risk of local recurrence or distant metastases in patients with the SLNB approach.
Although our study does not assess the risk of distant recurrence, 5- and 10-year overall survival was consistently higher in the SLNB group, and the difference becomes statistically significant at 15 years. In the presence of micrometastases, prior studies reported no significant difference in disease-free survival at 5 years (84.4% ALND versus 87.8% SLNB) and 10 years (76.8% ALND versus 74.9% SLNB).21 In our registry, micrometastases were only recorded in the most recent years, and the sample size was too limited for meaningful analysis.
Two randomized clinical trials have shown that SLNB is not inferior to ALND in terms of overall survival.23,37 Still, it is also true that these were clinical trials with selected patients.38 In contrast, our registry-based study includes all diagnosed cases, offering a real-world perspective. Interestingly, while ALND rates in N1 patients increased up to 2016, a decline has been observed since 2017, likely reflecting guideline updates and the influence of the SINODAR-ONE trial.28
A recent population-based study reported that the rate of ALND decreased from 47.1% in 2012 to 17.6% in 2021,39 closely mirroring our findings (47.9% in 2000–2004 versus 18.1% in 2017–2022). When analyzing stage I specifically, ALND fell from 29.3% to 1%, reinforcing that ALND should be nearly abandoned in small tumours. Nonetheless, 17 women with stage I disease still underwent ALND in our recent period, most with T1c tumours.
In that same study,39 the odds of receiving ALND increase in T2 (OR 1.10; 95% CI 1.03; 1.17) and even more in T3 (OR 2.290; 95% CI 1.15; 4.99) compared to T1.
Weiss et al40 analyzing over 12,000 mastectomy patients with positive sentinel lymph node between 2006 and 2014, reported a modest increase in SLND (34% to 37%) and a major decrease in ALND (47% to 23%): SLND was more commonly used in older women with comorbidities, small, well-differentiated tumours, and hormone receptor-positive disease.
In patients with 1–2 positive sentinel lymph nodes undergoing mastectomy between 2005 and 2015, axillary radiotherapy (RT) has emerged as a valid alternative to ALND without compromising the outcome.41 A more recent trial42 showed that 49% of patients were treated with RT plus axillary RT and only 13% received ALND, with no differences in regional recurrences or disease-free survival between the two groups.
Data from the Netherlands Cancer Registry43 examined 1,090 T1-T2 N0 patients and showed a wide variation in axillary management: observation alone (20%), ALND (40%), regional RT (30%), or ALND + RT (10%). The corresponding 5-year overall survival rates were 79%, 87.9%, 87.2%, and 87.9%, respectively, suggesting that observation alone may be insufficient in some cases.
In our study, we did not collect data on RT, but among N1 patients in the most recent period, 58.4% underwent ALND while 41.6% underwent SLNB.
Finally, between 2012 and 2017, the proportion of ALND in mastectomy patients declined from 81.3% to 68%.44 The likelihood of receiving ALND remained higher in young women and in those with larger high-grade tumors. However, at an international level, the debate is still open: while more recent evidence, such as the results from the SINODAR-ONE and SENOMAC trials, has begun to challenge the necessity of axillary lymph node dissection (ALND) in certain mastectomy cohorts, international guidelines still reflect a lack of total consensus. In many clinical settings, ALND remains the standard of care for these patients to ensure local control. Our finding that ALND rates remain high underscores the cautious “real-world” transition in surgical practice. We believe this highlights the importance of our epidemiological review in documenting how clinicians navigate these guideline disputes in daily practice.
Strengths and Limitations
A key strength of this study is its population-based design with a long observation period and complete case capture. The analysis included all women diagnosed with breast cancer in the Reggio Emilia province over 23 years, without any selection criteria. This real-world setting reinforces the external validity of the findings and provides a rare opportunity to evaluate the true impact of clinical guidelines and trial results on daily clinical practice. The results echo those of landmark clinical trials, but in an unselected, non-trial population, highlighting the widespread penetration of evidence into routine care.
However, some limitations should be acknowledged. First, this is a single-center study, which may limit generalizability beyond northern Italy, despite standardized protocols. Second, data on adjuvant therapies such as radiotherapy, chemotherapy, endocrine therapy, and targeted therapy as well as biological variables were not available, which may influence both treatment decisions and outcomes. Finally, survival analyses were not fully adjusted for potential confounders, so the observed benefit of SLNB over ALND should be interpreted with caution.
Conclusion
This large, population-based study of nearly 11,000 women with breast cancer confirms a substantial and progressive reduction in axillary node dissection over 23 years of observation, particularly in stage I disease, where SLNB is now the standard of care. Crucially, this shift in practice did not result in worse outcomes: women with stage I tumours who underwent SLNB alone had consistently better survival compared to those treated with ALND, with the difference becoming statistically significant after 15 years of follow-up.
These results validate the safety and efficacy of de-escalated axillary approaches in early-stage breast cancer and confirm that evidence from clinical trials has meaningfully shaped real-world practice. While axillary dissection persists in selected cases, ongoing refinement of indications is warranted. Future studies should aim to incorporate data on radiotherapy, tumor biology, and—most importantly—quality of life and long-term functional outcomes, which are central to modern, patient-centered oncologic care.
Institutional Review Board Statement
This population-based cohort study utilised data from the Reggio Emilia Cancer Registry, which was approved by the Provincial Ethics Committee of Reggio Emilia (ref. no. 2014/0019740 of 4 August 2014). Notwithstanding the absence of consent, the Ethics Committee authorised the processing of personal data, including data suitable for revealing the state of the health of deceased or unreachable patients, to conduct the study.
According to Italian legislation*population-based cancer registries collect pseudonymised personal data for surveillance purposes that do not need the collection of explicit individual consent, without any direct or indirect intervention on patients, therefore the approval of a research ethics committee was not required.
*Presidente del Consiglio dei Ministri. Decreto del Presidente del Consiglio dei Ministri, 3/3/2017,41 Identificazione dei sistemi di sorveglianza e dei registri di mortalità, di tumori e di altre patologie. 17A03142, GU Serie Generale n.109 del 12-05-2017. Available at: https://www.gazzettaufficiale.it/eli/id/2017/05/12/17A03142/sg last access: February 4, 2025.
Data Sharing Statement
The data presented in this study are available upon request from the corresponding author. Due to ethical and privacy issues, the data are not publicly available; requests for data must be approved by the Ethics Committee after the presentation of a study protocol.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was partially supported by the Italian Ministry of Health - Ricerca Corrente Annual Programme 2026.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Łukasiewicz S, Czeczelewski M, Forma A, et al. Breast cancer-epidemiology, risk factors, classification, prognostic markers, and current treatment strategies-an updated review. Cancers. 2021;13(17):4287. PMID: 34503097; PMCID: PMC8428369. doi:10.3390/cancers13174287
2. Duffy SW, Tabár L, Yen AM, et al. Mammography screening reduces rates of advanced and fatal breast cancers: results in 549,091 women. Cancer. 2020;126(13):2971–11. PMID: 32390151; PMCID: PMC7318598. doi:10.1002/cncr.32859
3. Czajka ML, Pfeifer C. Breast Cancer Surgery. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025. PMID: 31971717.
4. Gill G. Sentinel-lymph-node-based management or routine axillary clearance? One-year outcomes of sentinel node biopsy versus axillary clearance (SNAC): a randomized controlled surgical trial. Ann Surg Oncol. 2009;16(2):266–275. doi:10.1245/s10434-008-0229-z
5. Krag DN, Anderson SJ, Julian TB, et al. Sentinel-lymph-node resection compared with conventional axillary-lymph-node dissection in clinically node-negative patients with breast cancer: overall survival findings from the NSABP B-32 randomised phase 3 trial. Lancet Oncol. 2010;11(10):927–933. PMID: 20863759; PMCID: PMC3041644. doi:10.1016/S1470-2045(10)70207-2
6. Mansel RE, Fallowfield L, Kissin M, et al. Randomized multicenter trial of sentinel node biopsy versus standard axillary treatment in operable breast cancer: the ALMANAC trial. J Natl Cancer Inst. 2006;98(9):599–609. Erratum in: J Natl Cancer Inst. 2006 Jun 21;98 (12):876. PMID: 16670385. doi:10.1093/jnci/djj158
7. Lucci A, McCall LM, Beitsch PD, et al. Surgical complications associated with sentinel lymph node dissection (SLND) plus axillary lymph node dissection compared with SLND alone in the American College of Surgeons Oncology Group Trial Z0011. J Clin Oncol. 2007;25(24):3657–3663. PMID: 17485711. doi:10.1200/JCO.2006.07.4062
8. Veronesi U, Viale G, Paganelli G, et al. Sentinel lymph node biopsy in breast cancer: ten-year results of a randomized controlled study. Ann Surg. 2010;251(4):595–600. PMID: 20195151. doi:10.1097/SLA.0b013e3181c0e92a
9. Canavese G, Bruzzi P, Catturich A, et al. Sentinel lymph node biopsy versus axillary dissection in node-negative early-stage breast cancer: 15-Year follow-up update of a randomized clinical trial. Ann Surg Oncol. 2016;23(8):2494–2500. PMID: 26975739. doi:10.1245/s10434-016-5177-4
10. Bleyer A, Welch HG. Effect of three decades of screening mammography on breast-cancer incidence. N Engl J Med. 2012;367(21):1998–2005. doi:10.1056/nejmoa1206809
11. Mangone L, Marinelli F, Bisceglia I, et al. Five-year relative survival by stage of breast and colon cancers in northern Italy. Front Oncol. 2022;12:982461. doi:10.3389/fonc.2022.982461
12. Kim T, Giuliano AE, Lyman GH. Lymphatic mapping and sentinel lymph node biopsy in early-stage breast carcinoma: a metaanalysis. Cancer. 2006;106(1):4–16. doi:10.1002/cncr.21568
13. Krag DN, Anderson SJ, Julian TB, et al. Technical outcomes of sentinel-lymph-node resection and conventional axillary-lymph-node dissection in patients with clinically node-negative breast cancer: results from the NSABP B-32 randomised phase III trial. Lancet Oncol. 2007;8(10):881–888. PMID: 17851130. doi:10.1016/S1470-2045(07)70278-4
14. Goyal A, Douglas-Jones A, Newcombe RG, et al. Predictors of non-sentinel lymph node metastasis in breast cancer patients. Eur J Cancer. 2004;40(11):1731–1737. doi:10.1016/j.ejca.2004.04.006
15. Hwang RF, Gonzalez-Angulo AM, Yi M, et al. Low locoregional failure rates in selected breast cancer patients with tumor-positive sentinel lymph nodes who do not undergo completion axillary dissection. Cancer. 2007;110(4):723–730. PMID: 17587208. doi:10.1002/cncr.22847
16. Bilimoria KY, Bentrem DJ, Hansen NM, et al. Comparison of sentinel lymph node biopsy alone and completion axillary lymph node dissection for node-positive breast cancer. J Clin Oncol. 2009;27(18):2946–2953. PMID: 19364968. doi:10.1200/JCO.2008.19.5750
17. Giuliano AE, McCall L, Beitsch P, et al. Locoregional recurrence after sentinel lymph node dissection with or without axillary dissection in patients with sentinel lymph node metastases: the American College of Surgeons Oncology Group Z0011 randomized trial. Ann Surg. 2010;252(3):426–432. PMID: 20739842; PMCID: PMC5593421. doi:10.1097/SLA.0b013e3181f08f32
18. Giuliano AE, Ballman KV, McCall L, et al. Effect of axillary dissection vs no axillary dissection on 10-Year overall survival among women with invasive breast cancer and sentinel node metastasis: the ACOSOG Z0011 (Alliance) randomized clinical trial. JAMA. 2017;318(10):918–926. PMID: 28898379; PMCID: PMC5672806. doi:10.1001/jama.2017.11470
19. Corso G, Galimberti V, Veronesi P. De-escalation treatment of axilla in breast cancer. Clin Transl Oncol. 2020;22(3):445–446. PMID: 31073973. doi:10.1007/s12094-019-02129-4
20. Galimberti V, Cole BF, Zurrida S, et al. Axillary dissection versus no axillary dissection in patients with sentinel-node micrometastases (IBCSG 23-01): a phase 3 randomised controlled trial. Lancet Oncol. 2013;14(4):297–305. Erratum in: Lancet Oncol. 2013 Jun;14(7): e254. PMID: 23491275; PMCID: PMC3935346. doi:10.1016/S1470-2045(13)70035-4
21. Galimberti V, Cole BF, Viale G, et al. Axillary dissection versus no axillary dissection in patients with breast cancer and sentinel-node micrometastases (IBCSG 23-01): 10-year follow-up of a randomised, controlled phase 3 trial. Lancet Oncol. 2018;19(10):1385–1393. PMID: 30196031. doi:10.1016/S1470-2045(18)30380-2
22. Solá M, Alberro JA, Fraile M, et al. Complete axillary lymph node dissection versus clinical follow-up in breast cancer patients with sentinel node micrometastasis: final results from the multicenter clinical trial AATRM 048/13/2000. Ann Surg Oncol. 2013;20(1):120–127. PMID: 22956062. doi:10.1245/s10434-012-2569-y
23. Donker M, van Tienhoven G, Straver ME, et al. Radiotherapy or surgery of the axilla after a positive sentinel node in breast cancer (EORTC 10981-22023 AMAROS): a randomised, multicentre, open-label, phase 3 non-inferiority trial. Lancet Oncol. 2014;15(12):1303–1310. PMID: 25439688; PMCID: PMC4291166. doi:10.1016/S1470-2045(14)70460-7
24. Sávolt Á, Péley G, Polgár C, et al. Eight-year follow up result of the OTOASOR trial: the optimal treatment of the axilla - surgery or radiotherapy after positive sentinel lymph node biopsy in early-stage breast cancer: a randomized, single centre, phase III, non-inferiority trial. Eur J Surg Oncol. 2017;43(4):672–679. PMID: 28139362. doi:10.1016/j.ejso.2016.12.011
25. Morigi C, Peradze N, Galimberti V, et al. Feasibility and surgical impact of Z0011 trial criteria in a single-Institution practice. Breast J. 2020;26(7):1330–1336. PMID: 32506628. doi:10.1111/tbj.13851
26. Mangone L, Borciani E, Michiara M, et al. I Tumori Nelle Province dell’Area Vasta Emilia Nord: Piacenza, Parma, Reggio Emilia e Modena: Anni 2013–2014; Associazione Italiana Registri Tumori; 2015; Modena, Italy.
27. Sobin L, Gospodarowicz M, Wittekind C. TNM Classification of Malignant Tumours.
28. Tinterri C, Gentile D, Gatzemeier W, et al. Preservation of axillary lymph nodes compared with complete dissection in T1-2 breast cancer patients presenting one or two metastatic sentinel lymph nodes: the SINODAR-ONE multicenter randomized clinical trial. Ann Surg Oncol. 2022;29(9):5732–5744. PMID: 35552930. doi:10.1245/s10434-022-11866-w
29. Fernandes U, Guidi G, Martins D, et al. Breast cancer in young women: a rising threat: a 5-year follow-up comparative study. Porto Biomed J. 2023;8(3):e213. PMID: 37362019; PMCID: PMC10289488. doi:10.1097/j.pbj.0000000000000213
30. Hassaine Y, Jacquet E, Seigneurin A, et al. Evolution of breast cancer incidence in young women in a French registry from 1990 to 2018: towards a change in screening strategy? Breast Cancer Res. 2022;24(1):87. PMID: 36471434; PMCID: PMC9724405. doi:10.1186/s13058-022-01581-5
31. Ginsburg O, Yip CH, Brooks A, et al. Breast cancer early detection: a phased approach to implementation. Cancer. 2020;126(Suppl 10):2379–2393. PMID: 32348566; PMCID: PMC7237065. doi:10.1002/cncr.32887
32. Yu J, Mu Q, Fung M, et al. Challenges and opportunities in metastatic breast cancer treatments: nano-drug combinations delivered preferentially to metastatic cells may enhance therapeutic response. Pharmacol Ther. 2022;236:108108. PMID: 34999182; PMCID: PMC9256851. doi:10.1016/j.pharmthera.2022.108108
33. Miller KD, Nogueira L, Devasia T, et al. Cancer treatment and survivorship statistics, 2022. CA Cancer J Clin. 2022;72(5):409–436. PMID: 35736631. doi:10.3322/caac.21731
34. Mangone L, Bisceglia I, Michiara M, et al. Breast cancer in Italy: stage and region distribution. Breast Cancer. 2022;14:125–131. PMID: 35515355; PMCID: PMC9064450. doi:10.2147/BCTT.S360244
35. Bromham N, Schmidt-Hansen M, Astin M, et al. Axillary treatment for operable primary breast cancer. Cochrane Database Syst Rev. 2017;1(1):CD004561. doi:10.1002/14651858.CD004561.pub3
36. Magnoni F, Galimberti V, Corso G, et al. Axillary surgery in breast cancer: an updated historical perspective. Semin Oncol. 2020;47(6):341–352. PMID: 33131896. doi:10.1053/j.seminoncol.2020.09.001
37. Giuliano AE, Hunt KK, Ballman KV, et al. Axillary dissection vs no axillary dissection in women with invasive breast cancer and sentinel node metastasis: a randomized clinical trial. JAMA. 2011;305(6):569–575. PMID: 21304082; PMCID: PMC5389857. doi:10.1001/jama.2011.90
38. McGuire KP. Axillary dissection - the bell tolls for thee. N Engl J Med. 2024;390(13):1231–1232. PMID: 38598579. doi:10.1056/NEJMe2401805
39. Wang T, Jones T, Thomas SM, et al. Trends in axillary lymph node dissection after mastectomy among patients with limited nodal burden. JAMA Network Open. 2025;8(2):e2459692. PMID: 39946126; PMCID: PMC11826356. doi:10.1001/jamanetworkopen.2024.59692
40. Weiss A, Lin H, Babiera GV, et al. Evolution in practice patterns of axillary management following mastectomy in patients with 1-2 positive sentinel nodes. Breast Cancer Res Treat. 2019;176(2):435–444. PMID: 31025270. doi:10.1007/s10549-019-05243-7
41. Moossdorff M, Nakhlis F, Hu J, et al. The potential impact of AMAROS on the management of the axilla in patients with clinical T1-2N0 breast cancer undergoing primary total mastectomy. Ann Surg Oncol. 2018;25(9):2612–2619. PMID: 29855827. doi:10.1245/s10434-018-6519-1
42. Kantor O, Means J, Grossmith S, et al. Optimizing axillary management in clinical T1-2N0 mastectomy patients with positive sentinel lymph nodes. Ann Surg Oncol. 2022;29(2):972–980. PMID: 34467507. doi:10.1245/s10434-021-10726-3
43. De Wild SR, van Roozendaal LM, De Wilt JHW, et al. De-escalation of axillary treatment in the event of a positive sentinel lymph node biopsy in cT1-2 N0 breast cancer treated with mastectomy: nationwide registry study (BOOG 2013-07). Br J Surg. 2024;111(4):znae077. PMID: 38597154; PMCID: PMC11004788. doi:10.1093/bjs/znae077
44. Leonard LD, de Araujo TB, Quinn C, et al. De-implementation of axillary dissection in women undergoing mastectomy for breast cancer. Ann Surg Oncol. 2023;30(9):5692–5702. PMID: 37326811. doi:10.1245/s10434-023-13698-8
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Is Routine Intraoperative Frozen Section Analysis of Sentinel Lymph Nodes Necessary in Every Early-Stage Breast Cancer?
Lerttiendamrong B, Treeratanapun N, Vacharathit V, Tantiphlachiva K, Vongwattanakit P, Manasnayakorn S, Vongsaisuwon M
Breast Cancer: Targets and Therapy 2022, 14:281-290
Published Date: 19 September 2022
Factors Predicting Positive Sentinel Lymph Node Biopsy in Clinically Node-Negative Breast Cancer
Alsumai TS, Alhazzaa N, Alshamrani A, Assiri S, Alhefdhi A
Breast Cancer: Targets and Therapy 2022, 14:323-334
Published Date: 11 October 2022