Back to Journals » Breast Cancer: Targets and Therapy » Volume 14
Factors Predicting Positive Sentinel Lymph Node Biopsy in Clinically Node-Negative Breast Cancer
Authors Alsumai TS ![]() , Alhazzaa N, Alshamrani A, Assiri S, Alhefdhi A
, Alhazzaa N, Alshamrani A, Assiri S, Alhefdhi A ![]()
Received 1 May 2022
Accepted for publication 22 September 2022
Published 11 October 2022 Volume 2022:14 Pages 323—334
DOI https://doi.org/10.2147/BCTT.S373005
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Pranela Rameshwar
Thuraya S Alsumai,1 Norah Alhazzaa,1 Abdullah Alshamrani,2 Sarah Assiri,1 Amal Alhefdhi1,3
1Department of Surgery, Section of Breast & Endocrine Surgery, King Faisal Specialist Hospital & Research Center, Riyadh, Saudi Arabia; 2Department of Surgery, Security Forces Hospital, Riyadh, Saudi Arabia; 3Faculty of Medicine, Alfaisal University, Riyadh, Saudi Arabia
Correspondence: Thuraya S Alsumai, Department of Surgery, King Faisal Specialist Hospital & Research Center, Riyadh, Saudi Arabia, Tel +966 565433996, Email [email protected]
Purpose: Sentinel lymph node (SLN) biopsy (SLNB) is the standard tool to stage the axilla of breast cancer patients. This study aimed to identify the predictors of positive SLNB in patients with clinically node-negative breast cancer.
Patients and Methods: A retrospective, single-institution cohort of patients with early-stage breast cancer without clinically identifiable axillary lymphadenopathy was chosen from January 2010 to December 2018. Logistic regression was used to identify possible predictors of positive SLNB.
Results: Four hundred and seventy patients were identified; their mean age was 50± 11 years. Most patients had the following characteristics: invasive ductal carcinoma (n=382, 81.3%), unilateral tumor (n=461, 98.1%), unifocal disease (n=351, 74.7%), intermediate grade (n=276, 59.0%), and estrogen and progesterone receptor positivity with human epidermal growth factor receptor 2 negativity (n=305, 64.9%). The mean size of the breast mass was 2.3± 1.5 cm. SLNB was positive in 128 (27.2%) cases. The mean number of SLNs was 2± 1.2. Axillary lymph node dissection was performed in 109 patients. The mean number of lymph nodes removed was 15± 6. In 66 (60.6%) of the 109 patients with metastatic axillary nodes, only the SLNs were found to be positive. The number of SLNs, tumor size, tumor grade, receptor status, prominent axillary lymph nodes, and lymphovascular invasion predicted positive SLNB (P = 0.01, 0.03, 0.03, and 0.04 and < 0.001 and < 0.001, respectively).
Conclusion: Our results suggest that a number of histopathological and radiological characteristics of breast cancer can predict SLNB positivity in clinically node-negative breast cancer patients.
Keywords: axillary metastasis, lymphatic metastasis, axillary lymph node dissection, hormonal receptors
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Zhang has been published for this article.
Introduction
The evolution of the surgical management of breast cancer began in the late 1800s through the efforts of Halstead.1 Halstead described the importance of integrating axillary lymph node (ALN) dissection (ALND) with mastectomy for the treatment of breast cancer.1–3 ALND used to be performed as a routine procedure in all patients with breast cancer undergoing mastectomy to control the spread of breast cancer. However, over the last two decades, ALND has largely been replaced by the less invasive method of sentinel lymph node (SLN) biopsy (SLNB). As a result, ALND rates have decreased in patients with early-stage breast cancer.4,5
The SLN is the first regional lymph node (LN) to which cancer spreads, thereby reflecting the status of the remaining LNs in the basin.6 SLNB was first described in a 1960 paper by Gould et al,6 who proposed that SLNB eliminates the need to perform ALND for lymphatic staging. This concept has been proven to be especially important in breast cancer surgery, as it allows the patient to avoid routine ALND.6 In SLNB of the axilla, breast cancer metastasis is tracked by injection of a lymphatic blue dye or a radiolabeled colloid in the peri-areolar area. This is followed by intraoperative visualization of the dyed LN or detection by a gamma probe. After frozen sectioning, the SLN is histologically examined for presence of metastasis.6 SLNB is currently considered the standard of care.7 Other intraoperative methods of SLN detection have been proposed such as intraoperative electrical lymph scoring (ELS) and has shown high sensitivity.8 A number of studies have shown that SLNB is an accurate reflector of the cancer status of axillary LNs.2,4,7 Furthermore, SLNB plays an essential role in the control and local spread of cancer in the axilla.9
Similar to ALND, SLNB presents a number of possible risks and complications. These include upper limb lymphedema,7 movement impairment, and pain or paresthesia,10 all of which negatively affect the quality of life of patients with breast cancer.7 These complications are less likely to occur in patients undergoing SLNB than in those undergoing full ALND; however, they are not wholly eliminated.9 A post-SLNB rate of upper limb lymphedema of nearly 7% in the first 6 to 36 months has been reported.11 Furthermore, upper limb range motion impairment or stiffness has been described in 3.5% of the patients, shoulder and arm pain in 8.1%, and numbness in up to 10%.12
Due to the widespread establishment of breast cancer screening programs in many countries, there have been increasing rates of screening-detected breast cancers, which are usually detected in the early stages with no axillary involvement.13–15 This has prompted an interest in ALN staging and surgery. Studying the factors influencing SLNB positivity has also been a subject of interest in the efforts to identify methods to reduce the need for axillary surgery. Several studies have concluded that there is a high association between patient’s clinical, pathological, and radiological factors, an SLNB positivity. To the best of our knowledge, there are no similar studies conducted in our population of breast cancer patients.
The aim of this study is to identify all positive SLNBs in our population of patients with clinically node-negative breast cancer and to investigate the association between positive SLNB and patients’ clinical, histopathological, and radiological characteristics.
Materials and Methods
Study Design
This study involves a retrospective single-institution cohort that included all patients with early-stage breast cancer without clinically identifiable axillary lymphadenopathy at the King Faisal Specialist Hospital and Research Center in Riyadh, Saudi Arabia. Patients were selected from January 2010 through December 2018, and the estimated sample size was 300 patients. Categorical variables included family history; Tru-cut pathology; tumor grade, receptor status; laterality; radiological location and focality; presence of prominent axillary LNs (defined as enlarged axillary LNs in size on ultrasonography without other suspicious ultrasonographic features for metastasis such as absent fatty hilum, increased cortical thickness, and increased vascularity)16,17; ultrasound-guided axillary LN biopsy; surgery type; SLNB status; macro and micrometastasis; ALND status; surgical pathology; tumor focality in final pathology; lymphovascular invasion; locoregional recurrence; and recurrence type. Continuous variables included age at diagnosis, radiological tumor size, total SLNs, positive SLNs, negative SLNs¸ total ALND nodes, positive ALND nodes, and size in final pathology.
Data Collection Method
Data were retrospectively collected from the patients’ electronic medical records. All patients who were treated outside King Faisal Specialist Hospital were excluded. All patients with locally advanced and metastatic breast cancer were excluded. All patients who had clinically positive lymph nodes, or FNA-proven axillary lymph node metastasis were excluded. Missing data were extracted from patients’ paper charts. Radiological images were reviewed by expert breast radiologists; pathology slides were reviewed by expert breast cancer pathologists. Data collection was performed by all investigators.
Statistical Analysis
Data were imported into and analyzed using SPSS version 23 for Windows (IBM Corp., Armonk, NY, USA). Descriptive statistics (for continuous variables) and frequency tables (for categorical variables) were used to summarize the predictors of positive SLNB. Simple logistic regressions (involving one outcome variable and one predictor) were first performed to investigate the relationship between the outcome variable (SLNB) and each of the predictors. A multiple logistic regression analysis (involving one outcome variable and multiple predictors) was also performed to investigate the relationship between the outcome variable and each of the predictors.
Wald chi-square tests for type III analysis were used to determine whether the effects of the predictors were statistically significant. The Hosmer–Lemeshow goodness-of-fit test was used to determine the model adequacy (P > 0.05 indicates good model fit).18 Odds ratio (OR) estimates and corresponding 95% confidence intervals (CIs) were used to quantify the strength of the predictor effects. For all tests, significance was set at P < 0.05.
Ethical Considerations
All project procedures and reporting were performed in accordance with the standards of the ethics committee of the Research Advisory Council (RAC) of King Faisal Specialist Hospital and Research Center (RAC approval number #2191286). All patient data were collected as part of routine medical practice. Patient information and data were kept confidential and secure at all times. The investigators followed international and King Faisal Specialist Hospital guidelines on retrospective studies.
This study was eligible for waiver of consent because of its retrospective nature, in which no harm is posed to study participants. Absence of harm is defined as the probability and magnitude of damage or discomfort not greater than ordinarily encountered in daily life, or during the performance of routine physical or psychological tests, with no effect on the course of disease management.
Results
The study included 470 patients with early-stage breast cancer, of whom 342 (72.8%) had a negative SLNB and 128 (27.2%) had a positive SLNB. The mean age at diagnosis was 50.5. The majority of patients had unilateral cancer (98.1%). The most frequent pathology included invasive ductal carcinoma (IDC) or IDC plus ductal carcinoma in situ (DCIS) (81.3%), grade II (59%), estrogen receptor (ER)-positive, progesterone receptor (PR)-positive, and human epidermal growth factor receptor 2 (HER2)-negative breast cancer (64.9%) regardless of their SLNB status.
Across different radiological modalities, most patients had unifocal (74.7%), upper outer quadrant (UOQ) location (51.5%). The mean radiological size was similar between SLNB-negative and -positive patients (2.31 cm for SLNB-negative patients and 2.34 cm for SLNB-positive patients). Among SLNB-positive patients, 41.4% had prominent ALNs on ultrasonography, whereas only 24.9% of SLNB-negative patients did. Simple mastectomy was the most common type of surgery (46%). All subjects had undergone SLNB. The average number of total SLNs was 2. Among the SLNB-positive patients, 85.2% had macrometastasis, and all had undergone ALND. None of the SLNB-negative patients and none of the SLNB-positive patients with micrometastasis had undergone ALND.
Unifocal tumors (77.4%) with IDC or IDC plus DCIS (81.5%) were the most common findings in final pathology for both SLNB results. The average tumor size in final pathology was 2.3 cm. The majority of patients (92.8%) did not have recurrence. Of the 34 patients (7.2%) who had recurrence, nearly two-thirds had distant metastasis (61.8%). Table 1 shows the categorical clinical and radiopathological characteristics of the patient population based on the SLNB result, and Table 2 shows the continuous characteristics based on the SLNB result.
 |
Table 1 Clinical and Radiopathological Characteristics of Early Breast Cancer Patients Based on SLNB Result (Categorical Variables) (n = 470) |
 |
Table 2 Clinical and Radiopathological Characteristics of Early Breast Cancer Patients Based on SLNB Result (Continuous Variables) (n = 470) |
Simple and multiple logistic regression analyses were first performed to investigate the relationship between the outcome variable (SLNB) and each of the predictors. Some predictors (ie, Tru-cut pathology, receptor status, radiological location, surgery, and surgical pathology) were recoded to combine categories with only small samples.
The results of the simple logistic regression analysis indicated a statistically significant relationship between a positive SLNB and a higher number of total SLNs (OR = 1.29; 95% CI, 1.1–1.5; P = 0.002), larger size in final pathology (OR = 1.22; 95% CI, 1.06–1.41; P = 0.005), grade I cancer (OR = 2.06; 95% CI, 1.06–3.98; P = 0.029), ER-positive/PR-positive/HER2-negative status (OR = 2.01; 95% CI, 1.27–3.19; P = 0.003), unifocality on radiology (OR = 0.46; 95% CI, 0.24–0.88; P = 0.01), prominent ALNs (OR = 2.13; 95% CI, 1.39–3.28; P = 0.001), unifocality in final pathology (OR = 0.52; 95% CI, 0.28–0.96; P = 0.02), and lymphovascular invasion (OR = 3.93; 95% CI, 2.43–6.344; P < 0.001). The results are shown in Table 3.
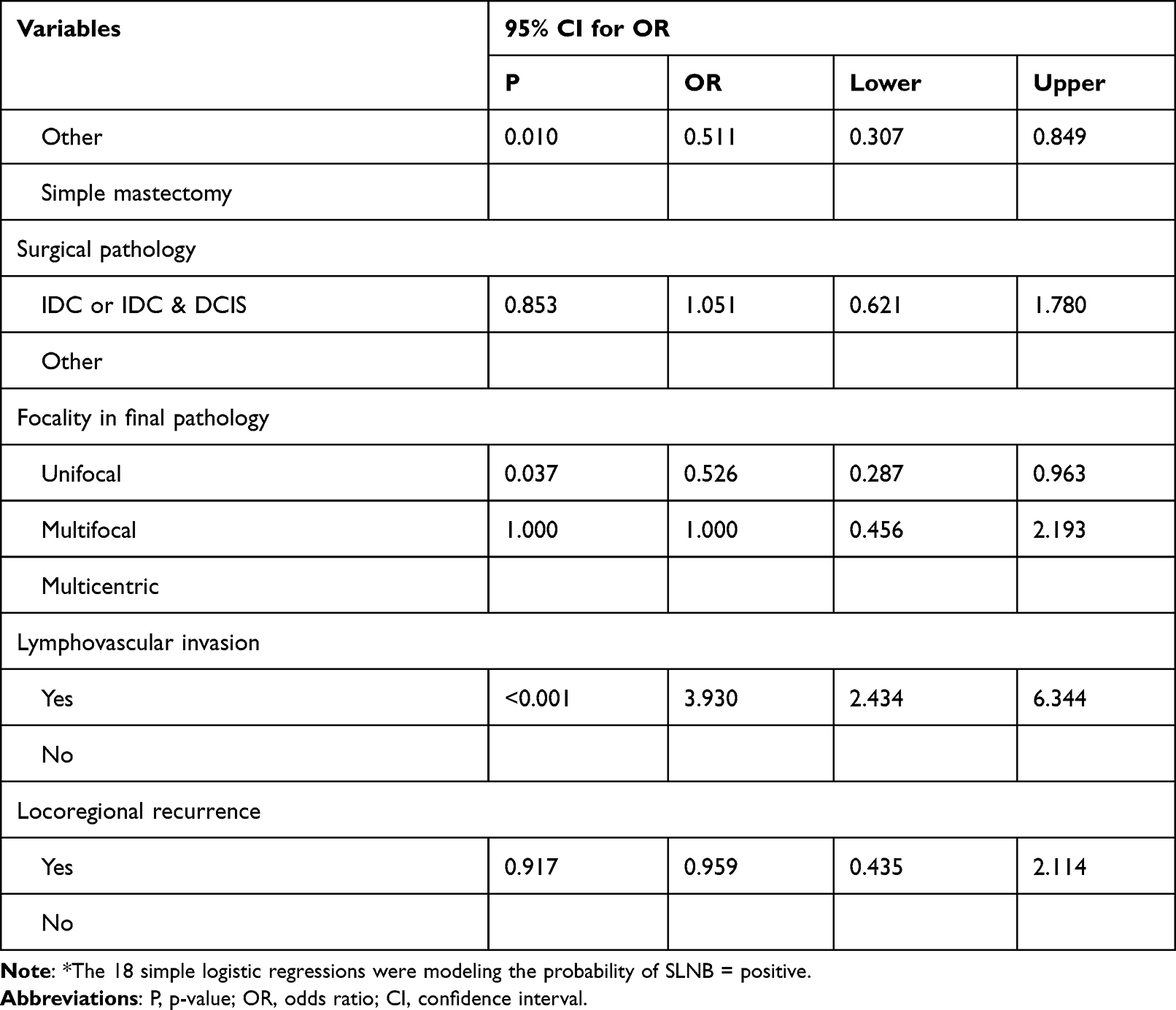 |
Table 3 Relationship Between SLNB Positivity and Early Breast Cancer Patients’ Clinical and Radiopathological Characteristics (Simple Regression Analysis*) |
For the multiple logistic regression analysis, the results of the Hosmer–Lemeshow goodness-of-fit test indicated that the model was adequate (χ2(8) = 7.285, P = 0.506). The results indicated that there was a statistically significant relationship between a positive SLNB and a higher number of total SLNs (OR = 1.27; 95% CI, 1.05–1.54; P = 0.01), larger size in final pathology (OR = 1.26; 95% CI, 1.01–1.56; P = 0.03), grade I cancers (OR = 2.42; 95% CI, 1.01–5.79; P = 0.03), ER-positive/PR-positive/HER2-negative status (OR = 1.83; 95% CI, 1.02–3.30; P = 0.04), prominent ALNs (OR = 3.37; 95% CI, 1.82–6.24; P < 0.001), and lymphovascular invasion (OR = 3.13; 95% CI, 1.79–5.47; P < 0.001). The results are shown in Table 4.
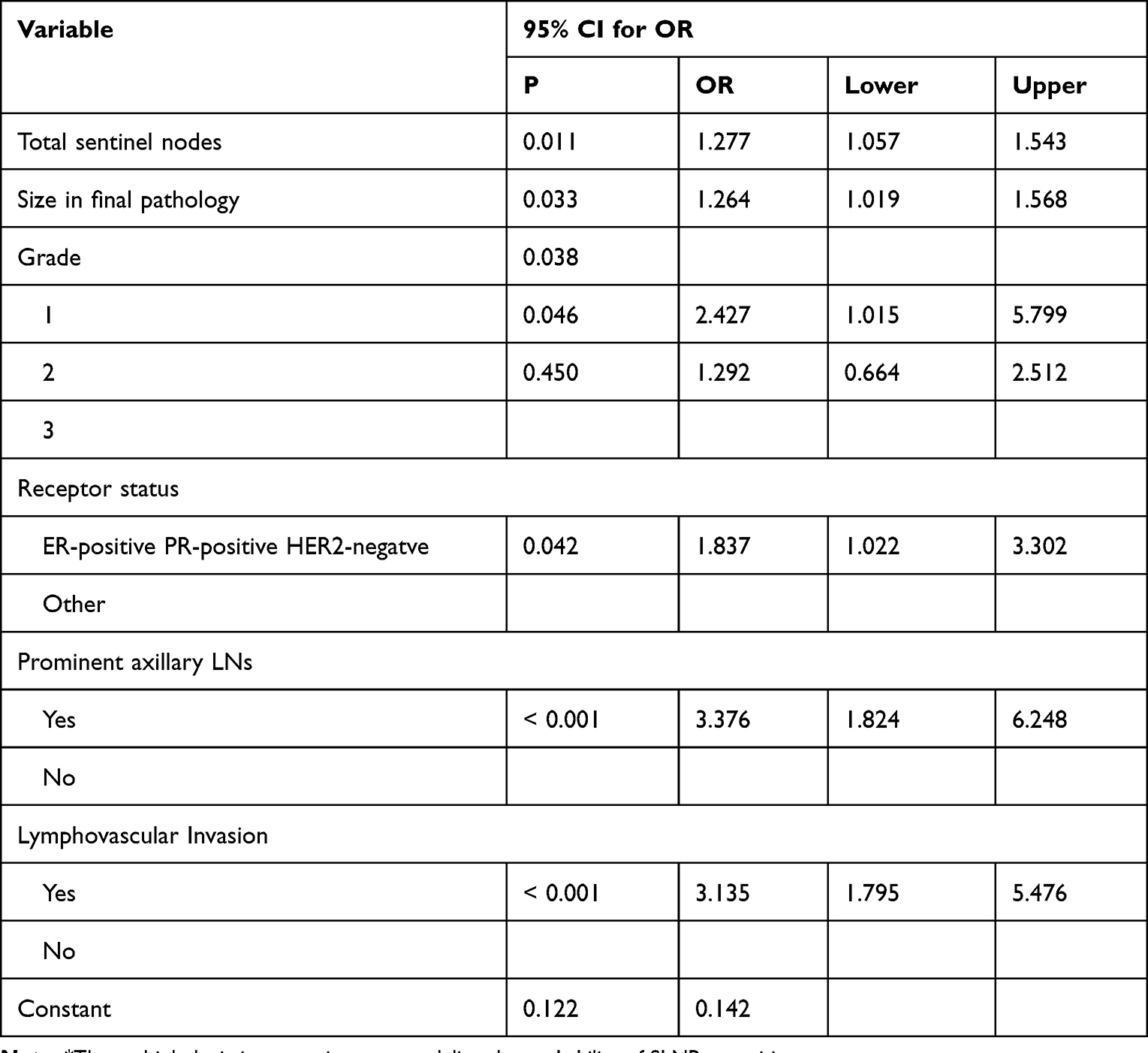 |
Table 4 Relationship Between SLNB Positivity and Early Breast Cancer Patients’ Clinical and Radiopathological Characteristics (Multiple Regression Analysis*) |
Discussion
Breast cancer is one of the most frequently diagnosed cancers in women and is a leading cause of cancer-related death worldwide.19,20 ALND, a highly invasive procedure, was previously performed on all breast cancer patients to assess the extent of axillary disease spread until it was replaced by the less invasive SLNB. Both procedures are associated with significant morbidity, such as upper limb lymphedema, paresthesia, stiffness, and weakness.21 Noninvasive methods for predicting the positivity of SLNs, especially in patients with clinically negative LNs, have been reported in the literature. A 2017 study by Dong et al investigated the use of noninvasive, preoperative T2-weighted fat-suppression and diffusion-weighted magnetic resonance imaging to predict SLN status. Their result showed that characterizing intratumoral heterogeneity may indicate positive nodal status; however, further validation studies are needed to replicate their findings.22
In the present study, we attempted to identify noninvasive predictors of positive SLNs in our cohort by investigating patients’ clinical, histopathological, and radiological characteristics. Several previous studies have examined different predictors of SLNB positivity; however, to our knowledge, ours is the first national study on this topic. Based on the evaluation of 470 patients with node-negative invasive breast cancer who underwent SLNB in our center over an 8-year period, we identified six independent predictors of SLN positivity by multivariate analysis. These included a higher number of total SLNs, larger tumor size in final pathology, grade I cancers, ER-positive/PR-positive/HER2-negative status, prominent ALNs on preoperative imaging, and lymphovascular invasion. Although tumor unifocality in radiology and in final pathology were associated with positive SLNB in the univariate analysis, they were not retained in the multivariate analysis.
Several previous publications have identified tumor size to be the strongest predictive factor of the risk of SLN positivity23,24 and to be associated with a higher probability of detection of metastatic disease after ALND;25–29 our results are consistent with the literature showing that patients with a larger tumor size in final pathology are more likely to be SLNB-positive. With a one-unit increase in tumor size in final pathology, the likelihood of being SLNB-positive increases by 26.4% (OR = 1.264; 95% CI, 1.019–1.568). In previous studies, angiolymphatic invasion has been shown to be a powerful predictor of the presence of invasion in SLNs.30 Similarly, our results showed that patients who had lymphovascular invasion would be more likely to be SLNB-positive than patients who did not have lymphovascular invasion (OR = 3.135; 95% CI, 1.795–5.476).
The ER, PR, and HER2 statuses are important factors in breast cancer management and are also important indicators for the efficacy of endocrine and targeted therapies in hormone-dependent breast tumors. The predictive value of hormone receptors has been a controversial area in the literature. Although there are published data linking ER- and PR-positive status with ALN metastases,31,32 other studies have indicated no significant association between hormone receptor status and nodal metastases.33–36 Our multivariate analysis showed that patients with ER-positive/PR-positive/HER2-negative tumors have a 83.7% higher likelihood of SLNB positivity (OR = 1.837; 95% CI, 1.022–3.302) than patients with other subtypes. We believe the association of ER, PR, and HER2 statuses with SLNB positivity warrants further exploration.
The primary imaging modality used for the investigation of ALN disease is axillary ultrasonography. It is routinely performed for our breast cancer patients and is interpreted by expert breast radiologists. If axillary ultrasonography revealed pathological nodes, they were sampled using fine-needle aspiration (FNA). Axillary ultrasonography has demonstrated excellent (76%) sensitivity for the detection of clinically significant ALNs in a large series.37 We defined prominent ALNs as those that did not meet the ultrasonographic criteria to be pathological or those whose pre-operative FNA biopsy results indicated that they were negative for metastasis. Our study identified a significant association between prominent ALNs on preoperative imaging and SLNB positivity (OR = 3.376; 95% CI, 1.824–6.248). This finding is similar to those of many previously published reports on the clinical significance of axillary ultrasonography.38–40
It has been noted in the literature that the diagnosis of breast cancer at a younger age (ie, younger than 40 years) is usually associated with more aggressive tumor types and less favorable outcomes. In a few studies, younger age at diagnosis was a predictive factor for SLNB positivity.21,26,30,34 In our study, age was not significantly associated with SNLB positivity. This could be attributed to the trend toward older age at diagnosis in our patient population.
There are potential limitations in the present study. These include its retrospective nature and its sample size, which makes it prone to confounding factors; however, we believe that this has not greatly influenced the study’s results because our patients were relatively similar in terms of clinical and tumor characteristics.
Conclusion
In summary, a higher number of SLNs, larger tumor size, grade I cancer, ER-positive/PR-positive/HER2-negative status, prominent ALNs on preoperative imaging, and lymphovascular invasion emerged as independent predictors of SLN positivity in clinically node-negative breast cancer patients. Although the prognostic implications of minimal ALN involvement remain an area of continuing research, we believe that our findings can contribute to creating future reliable predictive models of SLN positivity in early-stage breast cancer, which in turn can significantly contribute to therapeutic decisions.
Abbreviations
LN, lymph node; SLN, sentinel lymph node; SLNB, sentinel lymph node biopsy; ALN, axillary lymph node; ALND, axillary lymph node dissection; OR, odds ratio; CI, confidence interval; RAC, Research Advisory Council; IDC, invasive ductal cancer; DCIS, ductal carcinoma in situ; ER, estrogen receptor; PR, progesterone receptor; HER2, human epidermal growth factor receptor 2; UOQ, upper outer quadrant; FNA, fine-needle aspiration.
Data Sharing Statement
The data that supports the findings of this research are not publicly available due to institutional restrictions; however, data will be available upon reasonable request to the corresponding author.
Acknowledgments
The authors of this study wish to acknowledge the help provided by Ms Samia Al Hashem and Ms Areej Alfattan in data management and performing preliminary analyses for this project.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Halsted WS. I. The results of operations for the cure of cancer of the breast performed at the Johns Hopkins Hospital from June, 1889, to January, 1894. Ann Surg. 1894;20(5):497–555. doi:10.1097/00000658-189407000-00075
2. Giuliano AE, Jones RC, Brennan M, Statman R. Sentinel lymphadenectomy in breast cancer. J Clin Oncol. 1997;15(6):2345–2350. doi:10.1200/JCO.1997.15.6.2345
3. Chintamani. The paradigm shifts in the management of breast cancer—have we finally arrived? Indian J Surg. 2013;75(6):419–423. doi:10.1007/s12262-013-1022-1
4. Kelley MC, Hansen N, McMasters KM. Lymphatic mapping and sentinel lymphadenectomy for breast cancer. Am J Surg. 2004;188(1):49–61. doi:10.1016/j.amjsurg.2003.10.028
5. Veronesi U, Paganelli G, Galimberti V, et al. Sentinel-node biopsy to avoid axillary dissection in breast cancer with clinically negative lymph-nodes. Lancet. 1997;349(9069):1864–1867. doi:10.1016/S0140-6736(97)01004-0
6. Gould EA, Winship T, Philbin PH, Kerr HH. Observations on a “sentinel node” in cancer of the parotid. Cancer. 1960;13:77–78. doi:10.1002/1097-0142(196001/02)13:1<77::aid-cncr2820130114>3.0.co;2-d
7. Veronesi U, Paganelli G, Viale G, et al. A randomized comparison of sentinel-node biopsy with routine axillary dissection in breast cancer. N Engl J Med. 2003;349(6):546–553. doi:10.1056/NEJMoa012782
8. Mahdavi R, Yousefpour N, Abbasvandi F, et al. Intraoperative pathologically-calibrated diagnosis of lymph nodes involved by breast cancer cells based on electrical impedance spectroscopy; a prospective diagnostic human model study. Int J Surg. 2021;96:106166. doi:10.1016/j.ijsu.2021.106166
9. Gipponi M, Bassetti C, Canavese G, et al. Sentinel lymph node as a new marker for therapeutic planning in breast cancer patients. J Surg Oncol. 2004;85(3):102–111. doi:10.1002/jso.20022
10. Deutsch M, Land S, Begovic M, Sharif S. The incidence of arm edema in women with breast cancer randomized on the National Surgical Adjuvant Breast and Bowel Project study B-04 to radical mastectomy versus total mastectomy and radiotherapy versus total mastectomy alone. Int J Radiat Oncol Biol Phys. 2008;70(4):1020–1024. doi:10.1016/j.ijrobp.2007.07.2376
11. Bromham N, Schmidt-Hansen M, Astin M, Hasler E, Reed MW. Axillary treatment for operable primary breast cancer. Cochrane Database Syst Rev. 2017;1:CD004561. doi:10.1002/14651858.CD004561.pub3
12. McLaughlin SA, Wright MJ, Morris KT, et al. Prevalence of lymphedema in women with breast cancer 5 years after sentinel lymph node biopsy or axillary dissection: objective measurements. J Clin Oncol. 2008;26(32):5213–5219. doi:10.1200/JCO.2008.16.3725
13. Humphrey LL, Helfand M, Chan BK, Woolf SH. Breast cancer screening: a summary of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med. 2002;137(5Part 1):347–360. doi:10.7326/0003-4819-137-5_part_1-200209030-00012
14. Iwamoto T, Kumamaru H, Miyata H, et al. Distinct breast cancer characteristics between screen- and self-detected breast cancers recorded in the Japanese Breast Cancer Registry. Breast Cancer Res Treat. 2016;156(3):485–494. doi:10.1007/s10549-016-3770-7
15. Niraula S, Biswanger N, Hu P, Lambert P, Decker K. Incidence, characteristics, and outcomes of interval breast cancers compared with screening-detected breast cancers. JAMA Netw Open. 2020;3(9):e2018179. doi:10.1001/jamanetworkopen.2020.18179
16. Vassallo P, Wernecke K, Roos N, Peters PE. Differentiation of benign from malignant superficial lymphadenopathy: the role of high-resolution US. Radiology. 1992;183(1):215–220. doi:10.1148/radiology.183.1.1549675
17. Choi YJ, Ko EY, Han BK, Shin JH, Kang SS, Hahn SY. High-resolution ultrasonographic features of axillary lymph node metastasis in patients with breast cancer. Breast. 2009;18(2):119–122. doi:10.1016/j.breast.2009.02.004
18. Agresti A. Categorical Data Analysis. Hoboken, NJ: John Wiley & Sons, Inc; 2003.
19. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
20. Alotaibi RM, Rezk HR, Juliana CI, Guure C. Breast cancer mortality in Saudi Arabia: modelling observed and unobserved factors. PLoS One. 2018;13(10):e0206148. doi:10.1371/journal.pone.0206148
21. Pavlista D, Duskova M, Novotny J, et al. Komplikace disekce axily pro karcinom prsu [Complications of axillary dissection in breast carcinoma]. Ceska Gynekol. 2002;67(6):333–337. Czech.
22. Dong Y, Feng Q, Yang W, et al. Preoperative prediction of sentinel lymph node metastasis in breast cancer based on radiomics of T2-weighted fat-suppression and diffusion-weighted MRI. Eur Radiol. 2018;28(2):582–591. doi:10.1007/s00330-017-5005-7
23. Viale G, Zurrida S, Maiorano E, et al. Predicting the status of axillary sentinel lymph nodes in 4351 patients with invasive breast carcinoma treated in a single institution. Cancer. 2005;103(3):492–500. doi:10.1002/cncr.20809
24. Minami S, Sakimura C, Irie J, Tokai Y, Okubo H, Ohno T. Predictive factors among clinicopathological characteristics for sentinel lymph node metastasis in T1-T2 breast cancer. Cancer Manag Res. 2021;13:215–223. doi:10.2147/CMAR.S284922
25. Olivotto IA, Jackson JS, Mates D, et al. Prediction of axillary lymph node involvement of women with invasive breast carcinoma: a multivariate analysis. Cancer. 1998;83(5):948–955. doi:10.1002/(SICI)1097-0142(19980901)83:5<948::AID-CNCR21>3.0.CO;2-U
26. Harden SP, Neal AJ, Al-Nasiri N, Ashley S, Querci Della Rovere G. Predicting axillary lymph node metastases in patients with T1 infiltrating ductal carcinoma of the breast. Breast. 2001;10(2):155–159. doi:10.1054/brst.2000.0220
27. Tan LG, Tan YY, Heng D, Chan MY. Predictors of axillary lymph node metastases in women with early breast cancer in Singapore. Singapore Med J. 2005;46(12):693–697.
28. Kohrt HE, Olshen RA, Bermas HR, et al. New models and online calculator for predicting non-sentinel lymph node status in sentinel lymph node positive breast cancer patients. BMC Cancer. 2008;8:66. doi:10.1186/1471-2407-8-66
29. Sopik V, Narod SA. The relationship between tumour size, nodal status and distant metastases: on the origins of breast cancer. Breast Cancer Res Treat. 2018;170(3):647–656. doi:10.1007/s10549-018-4796-9
30. Fein DA, Fowble BL, Hanlon AL, et al. Identification of women with T1-T2 breast cancer at low risk of positive axillary nodes. J Surg Oncol. 1997;65(1):34–39. doi:10.1002/(sici)1096-9098(199705)65:1<34::aid-jso7>3.0.co;2-p
31. Barth A, Craig PH, Silverstein MJ. Predictors of axillary lymph node metastases in patients with T1 breast carcinoma. Cancer. 1997;79(10):1918–1922. doi:10.1002/(SICI)1097-0142(19970515)79:10<1918::AID-CNCR12>3.0.CO;2-Y
32. Gann PH, Colilla SA, Gapstur SM, Winchester DJ, Winchester DP. Factors associated with axillary lymph node metastasis from breast carcinoma: descriptive and predictive analyses. Cancer. 1999;86(8):1511–1519. doi:10.1002/(sici)1097-0142(19991015)86:8<511::aid-cncr18>3.0.co;2-d
33. Chua B, Ung O, Taylor R, Boyages J. Frequency and predictors of axillary lymph node metastases in invasive breast cancer. ANZ J Surg. 2001;71(12):723–728. doi:10.1046/j.1445-1433.2001.02266.x
34. Ding J, Jiang L, Wu W. Predictive value of clinicopathological characteristics for sentinel lymph node metastasis in early breast cancer. Med Sci Monit. 2017;23:4102–4108. doi:10.12659/msm.902795
35. Gajdos C, Tartter PI, Bleiweiss IJ. Lymphatic invasion, tumor size, and age are independent predictors of axillary lymph node metastases in women with T1 breast cancers. Ann Surg. 1999;230(5):692–696. doi:10.1097/00000658-199911000-00012
36. Yoshihara E, Smeets A, Laenen A, et al. Predictors of axillary lymph node metastases in early breast cancer and their applicability in clinical practice. Breast. 2013;22(3):357–361. doi:10.1016/j.breast.2012.09.003
37. Tucker NS, Cyr AE, Ademuyiwa FO, et al. Axillary ultrasound accurately excludes clinically significant lymph node disease in patients with early stage breast cancer. Ann Surg. 2016;264(6):1098–1102. doi:10.1097/SLA.0000000000001549
38. Sato K, Tamaki K, Tsuda H, et al. Utility of axillary ultrasound examination to select breast cancer patients suited for optimal sentinel node biopsy. Am J Surg. 2004;187(6):679–683. doi:10.1016/j.amjsurg.2003.10.012
39. Ramjeesingh R, Quan ML, Gardner S, Holloway CM. Prediction of involvement of sentinel and nonsentinel lymph nodes in a Canadian population with breast cancer. Can J Surg. 2009;52(1):23–30.
40. Susini T, Nori J, Olivieri S, et al. Predicting the status of axillary lymph nodes in breast cancer: a multiparameter approach including axillary ultrasound scanning. Breast. 2009;18(2):103–108. doi:10.1016/j.breast.2009.02.001
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Is Routine Intraoperative Frozen Section Analysis of Sentinel Lymph Nodes Necessary in Every Early-Stage Breast Cancer?
Lerttiendamrong B, Treeratanapun N, Vacharathit V, Tantiphlachiva K, Vongwattanakit P, Manasnayakorn S, Vongsaisuwon M
Breast Cancer: Targets and Therapy 2022, 14:281-290
Published Date: 19 September 2022
From Axillary Lymph Node Dissection to Sentinel Node Biopsy in Breast Cancer: A 23-Year Population-Based Large-Sample Study with Long-Term Survival Outcomes
Mangone L, Marinelli F, Bisceglia I, Braghiroli MB, Neri A, Morabito F, Pinto C, Ragazzi M, Ferrari G, Coiro S, Cenini E
Breast Cancer: Targets and Therapy 2026, 18:573154
Published Date: 17 April 2026