Back to Journals » Clinical Interventions in Aging » Volume 21
FIB-4 Index, Systemic Inflammation, and Troponin Trajectory After Endovascular Thrombectomy in Older Patients with Large-Vessel Occlusion Stroke
Authors Chen W, Tan Y, Bai X, Wang T, Jiao L, Zhang L, Li H
Received 23 February 2026
Accepted for publication 7 May 2026
Published 16 May 2026 Volume 2026:21 601412
DOI https://doi.org/10.2147/CIA.S601412
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Wenjie Chen,1 Yahang Tan,1 Xuesong Bai,2 Tao Wang,2 Liqun Jiao,2 Liyong Zhang,3 Hong Li1
1Department of Cardiology, Beijing Chaoyang Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Department of Neurosurgery, Xuanwu Hospital, Capital Medical University, Beijing, People’s Republic of China; 3Department of Neurosurgery, Liaocheng People’s Hospital, Shandong First Medical University, Liaocheng, Shandong, People’s Republic of China
Correspondence: Liyong Zhang; Email [email protected] Hong Li, Email [email protected]
Background: Stroke–heart syndrome affects prognosis after large-vessel occlusion acute ischemic stroke (LVO-AIS). The Fibrosis-4 (FIB-4) index may reflect metabolic vulnerability, but its association with post-stroke myocardial injury and the modifying role of systemic inflammation remain unclear.
Methods: This retrospective single-center cohort included 448 consecutive patients aged ≥ 60 years with anterior-circulation LVO-AIS treated with endovascular thrombectomy. Cardiac troponin I was measured at admission and 48 hours after admission. Troponin trajectory was classified as no myocardial injury, non-dynamic myocardial injury, or dynamic myocardial injury. Ordinal logistic regression assessed associations of FIB-4 and C-reactive protein (CRP) with troponin trajectory. Binary logistic regression assessed 90-day mortality.
Results: Among 448 patients, 255 had no myocardial injury, 35 had non-dynamic myocardial injury, and 158 had dynamic myocardial injury. In fully adjusted models, intermediate and high FIB-4 were associated with more severe troponin trajectory compared with low FIB-4 [odds ratio (OR) 2.04, 95% confidence interval (CI) 1.18– 3.59; and OR 3.14, 95% CI 1.59– 6.30, respectively]. Elevated CRP was also associated with more severe troponin trajectory (OR 2.91, 95% CI 1.86– 4.59). The association between high FIB-4 and troponin trajectory differed by CRP status (P for interaction = 0.019), being significant among patients with CRP ≥ 5 mg/L (OR 3.40, 95% CI 1.49– 7.76). Dynamic myocardial injury was associated with 90-day mortality (OR 5.08, 95% CI 2.43– 11.21).
Conclusion: Higher FIB-4 and elevated CRP were associated with more severe troponin trajectory. Systemic inflammation may modify the FIB-4–myocardial injury association, and dynamic myocardial injury identified patients at increased mortality risk.
Keywords: acute ischemic stroke, endovascular thrombectomy, fib-4 index, stroke-heart syndrome, C-reactive protein
Introduction
Despite successful reperfusion with endovascular thrombectomy (EVT), a substantial proportion of older patients with large-vessel occlusion acute ischemic stroke (LVO-AIS) experience poor outcomes.1 Cardiac complications after stroke, recently conceptualized as stroke–heart syndrome (SHS), represent an important contributor to post-stroke morbidity and mortality.2,3 Among these complications, myocardial injury is common but clinically heterogeneous. Isolated troponin elevation after acute ischemic stroke may reflect chronic structural heart disease, renal dysfunction, pre-existing myocardial injury, or acute stroke-triggered myocardial injury. Therefore, serial troponin assessment and dynamic changes over time may provide more clinically meaningful information than a single measurement by helping distinguish stable or chronic myocardial injury from acute evolving injury.2,4 Recent studies in patients receiving reperfusion therapy have further shown that dynamic troponin changes may provide prognostic or complication-related information beyond admission troponin elevation, including after intravenous thrombolysis and mechanical thrombectomy.5,6
The Fibrosis-4 (FIB-4) index, originally developed as a non-invasive marker of liver fibrosis, has increasingly been recognized as a composite indicator of systemic vulnerability and cardiovascular risk.7–9 Prior studies have linked higher FIB-4 to adverse outcomes in ischemic stroke patients receiving reperfusion therapy and in patients with cardiovascular disease.8 Its components—age, aminotransferase levels, and platelet count—capture overlapping domains of metabolic dysfunction, hepatic stress, inflammation, and hemostatic disturbance. In acute stroke, such vulnerability may be particularly relevant because autonomic imbalance, systemic inflammation, endothelial dysfunction, and thromboinflammatory activation may converge to promote myocardial injury.10–12 C-reactive protein (CRP), a widely used marker of systemic inflammation, has also been associated with poor outcomes after EVT-treated stroke.13,14 Because inflammation may amplify the cardiovascular consequences of metabolic vulnerability, CRP may modify the association between FIB-4 and post-stroke myocardial injury.
However, the relationship between FIB-4, systemic inflammation, troponin trajectory, and clinical outcomes in older patients with LVO-AIS undergoing EVT remains insufficiently defined. Therefore, we conducted this retrospective single-center cohort study in older patients with anterior-circulation LVO-AIS undergoing EVT to: (1) investigate the associations of FIB-4 and CRP with troponin trajectory; (2) assess whether systemic inflammation modifies the association between FIB-4 and troponin trajectory; and (3) explore the prognostic association between troponin trajectory and 90-day mortality.
Materials and Methods
Study Design and Population
This retrospective single-center cohort study analyzed data from consecutive older patients with anterior-circulation LVO-AIS treated with EVT at Beijing Chaoyang Hospital between January 2023 and January 2026.
The inclusion criteria were as follows: (1) age ≥60 years; (2) pre-stroke modified Rankin Scale (mRS) score ≤2; (3) occlusion of the intracranial internal carotid artery (ICA) or middle cerebral artery (M1/M2 segments) confirmed by digital subtraction angiography (DSA), CT angiography, or MR angiography; (4) EVT initiation within 6 hours of symptom onset, or within 6–24 hours in patients meeting DAWN/DEFUSE-3 eligibility criteria;1,15 and (5) availability of serial cardiac troponin I (cTnI) measurements at admission and 48 hours after admission.
The exclusion criteria were as follows: (1) active malignancy or severe infection at admission, to avoid confounding effects on inflammatory biomarkers; (2) concurrent acute coronary syndrome or acute myocardial infarction, to distinguish stroke-associated myocardial injury from primary type 1 myocardial infarction; (3) acute liver injury, defined as alanine aminotransferase (ALT) or aspartate aminotransferase (AST) >3 times the upper limit of normal at admission, to specifically investigate the impact of subclinical metabolic vulnerability rather than overt hepatic injury; (4) known chronic kidney disease or severe renal insufficiency, defined as serum creatinine >2.0 mg/dL, estimated glomerular filtration rate <30 mL/min/1.73 m2, or maintenance dialysis, given that impaired renal clearance can lead to non-specific troponin elevation; and (5) missing data for key variables, including components of the FIB-4 index, baseline C-reactive protein (CRP), serial cTnI measurements, or 90-day follow-up.
The study was approved by the Ethics Committee of Beijing Chaoyang Hospital, Capital Medical University. The requirement for written informed consent was waived because of the retrospective nature of the study.
Clinical and Procedural Data Collection
Baseline demographic and clinical variables were extracted from prospectively maintained stroke registries and complemented by manual review of the electronic medical record. We recorded age, sex, vascular risk factors and comorbidities, including hypertension, diabetes mellitus, hyperlipidemia, coronary artery disease, atrial fibrillation, prior stroke, and smoking history. Stroke severity at baseline was quantified using the National Institutes of Health Stroke Scale (NIHSS). Baseline infarct core was estimated using the Alberta Stroke Program Early CT Score (ASPECTS) on non-contrast CT.16
Baseline medication use was extracted from the updated electronic medical record system and manually verified through review of admission records, prior outpatient prescriptions, medication reconciliation notes, and discharge summaries when available. Baseline medication use was defined as documented active or regular use within 30 days before the index stroke admission. Medications newly initiated after admission, medications administered only during emergency treatment or the periprocedural period, and loading doses given for the index EVT procedure were not considered baseline medication use. For all included patients, baseline medication status could be determined from the available medical records. Medication variables included antihypertensive, antidiabetic, lipid-lowering, anticoagulant, and antiplatelet therapies. Antihypertensive therapy included angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, calcium-channel blockers, beta-blockers, diuretics, or other blood pressure–lowering agents. Antidiabetic therapy included insulin and oral or injectable glucose-lowering medications. Lipid-lowering therapy included statins, ezetimibe, fibrates, proprotein convertase subtilisin/kexin type 9 inhibitors, or other lipid-lowering agents. Anticoagulant therapy included warfarin or direct oral anticoagulants. Antiplatelet therapy included aspirin, clopidogrel, ticagrelor, cilostazol, or other antiplatelet agents.
The cause of stroke was adjudicated according to the TOAST classification and grouped as cardioembolism, large-artery atherosclerosis, or other causes.17,18 The occlusion location was defined on baseline angiographic imaging and categorized as ICA, M1, or M2 segment occlusion.19 Procedural data included the first-line thrombectomy strategy, categorized as no device pass, aspiration, stent retriever, or combined approach, and final reperfusion graded by the modified Thrombolysis in Cerebral Infarction (mTICI) score.20 Successful reperfusion was defined as mTICI 2b–3.21,22
Periprocedural complications, including symptomatic intracranial hemorrhage (sICH) and malignant cerebral edema, were also recorded. sICH was diagnosed according to the Heidelberg Bleeding Classification.23–25 Malignant cerebral edema was defined as hypodense parenchymal involvement in at least 50% of the middle cerebral artery territory with regional brain swelling or cerebral herniation, and a midline shift ≥5 mm at the septum pellucidum or pineal gland with effacement of the basal cisterns.26
FIB-4 Index and CRP
The FIB-4 index was calculated using age, aspartate aminotransferase (AST), alanine aminotransferase (ALT), and platelet count according to the following formula: FIB-4= Age(years)×AST(U/L)/(Platelet count [10^9/L]×√ALT [U/L]). Baseline laboratory tests were obtained at admission before EVT. Based on established cut-offs from prior studies, patients were categorized into three groups: low (<1.30), intermediate (1.30–2.67), and high (>2.67).27 Systemic inflammation was assessed using serum CRP (mg/L) measured at admission. CRP was dichotomized as low (<5.0 mg/L) versus high (≥5.0 mg/L) based on a recent study in EVT-treated stroke patients, which demonstrated that CRP ≥5.0 mg/L independently predicts poor outcomes.14
Definition of Troponin Trajectory
Serum cTnI levels were measured at admission and 48 hours after admission using a standard high-sensitivity assay. The institutional upper reference limit was 0.034 ng/mL. Based on the dynamic evolution of cTnI, patients were classified into three ordinal troponin trajectory categories:
No myocardial injury: all cTnI measurements remained ≤ the upper reference limit.
Non-dynamic myocardial injury: at least one cTnI measurement was > the upper reference limit, but without a significant rising pattern. This category included patients with stable elevation, defined as a relative change <20%, or a falling pattern, defined as a decrease ≥20% from admission to 48 hours, reflecting chronic myocardial injury or resolving acute injury preceding the index stroke.
Dynamic myocardial injury: at least one cTnI measurement was > the upper reference limit, with a rising pattern defined as a ≥20% increase from admission to 48 hours. This pattern was considered consistent with acute evolving myocardial injury potentially triggered by the index stroke.
The 20% relative change threshold was adopted from the Fourth Universal Definition of Myocardial Infarction to distinguish acute from chronic myocardial injury.2
Outcome Measures
The primary clinical outcome was all-cause mortality at 90 days after stroke onset. Vital status at 90 days was ascertained through outpatient visits, structured telephone interviews, or review of medical records and death certificates.
Statistical Analysis
Patients with missing data for FIB-4 calculation, baseline CRP, serial cTnI measurements, or 90-day follow-up were excluded. Baseline characteristics were summarized according to troponin trajectory groups and FIB-4 categories. Continuous variables are presented as median with interquartile range and were compared using the Kruskal–Wallis test. Categorical variables are presented as counts and percentages and were compared using Pearson’s chi-square test or Fisher’s exact test, as appropriate.
To investigate the association of FIB-4 and CRP with troponin trajectory, ordinal logistic regression models were fitted, with troponin trajectory as the ordinal outcome. The proportional odds assumption was assessed using the Brant test and was not materially violated in the primary ordinal logistic regression models. Model 1 was unadjusted. Model 2 was adjusted for age, sex, hypertension, diabetes mellitus, hyperlipidemia, coronary artery disease, atrial fibrillation, smoking history, prior stroke, and prior medications, including antihypertensive, antidiabetic, lipid-lowering, anticoagulant, and antiplatelet therapy. Model 3 was further adjusted for NIHSS score, ASPECTS, occlusion site, TOAST classification, first-line thrombectomy technique, and final mTICI score. FIB-4 and CRP were modeled separately in the primary analyses.
Restricted cubic spline models were fitted using three knots placed at the 10th, 50th, and 90th percentiles, with the median value as the reference, to visualize potential non-linear associations.
To assess whether systemic inflammation modified the association between FIB-4 and troponin trajectory, CRP-stratified analyses were performed using CRP <5 mg/L and CRP ≥5 mg/L. In these analyses, high FIB-4 was compared with low/intermediate FIB-4. A parsimonious adjustment model was used to reduce overfitting due to limited subgroup sample size. Interaction was tested using the likelihood ratio test comparing models with and without the interaction term between FIB-4 category and CRP group.
Binary logistic regression was used to evaluate the association between troponin trajectory and 90-day mortality. P for trend was calculated by modeling troponin trajectory as an ordinal variable. Exploratory subgroup analyses were performed according to major comorbidities and baseline medication use, including hypertension, diabetes mellitus, hyperlipidemia, coronary artery disease, atrial fibrillation, prior stroke, and antihypertensive, antidiabetic, lipid-lowering, anticoagulant, and antiplatelet therapies. In these analyses, high FIB-4 was compared with low/intermediate FIB-4. Because of limited subgroup sample sizes and sparse outcome distributions in some strata, a parsimonious ordinal logistic regression model was used, adjusted for age, sex, and NIHSS score. Interaction P values were calculated by including multiplicative interaction terms between high FIB-4 and subgroup variables. Crude logistic regression analyses were further performed to examine the association between high FIB-4 and 90-day mortality within each troponin trajectory group. Multivariable adjustment was not performed in these stratified mortality analyses because of the limited number of deaths and sparse event distributions within some trajectory strata.
A two-sided P value <0.05 was considered statistically significant. Analyses were performed using R software, version 4.3.2.
Results
Baseline Characteristics
Five patients with acute myocardial infarction, ten with concurrent severe infections, fifteen with active malignancy, three with acute liver injury, and thirteen with missing liver function indicators were excluded. In the revised single-center cohort, 448 consecutive patients with anterior-circulation LVO-AIS treated with EVT at Beijing Chaoyang Hospital were included in the final analysis (Figure 1). All patients completed 90-day follow-up. Of these, 255 patients had no myocardial injury, 35 had non-dynamic myocardial injury, and 158 had dynamic myocardial injury.
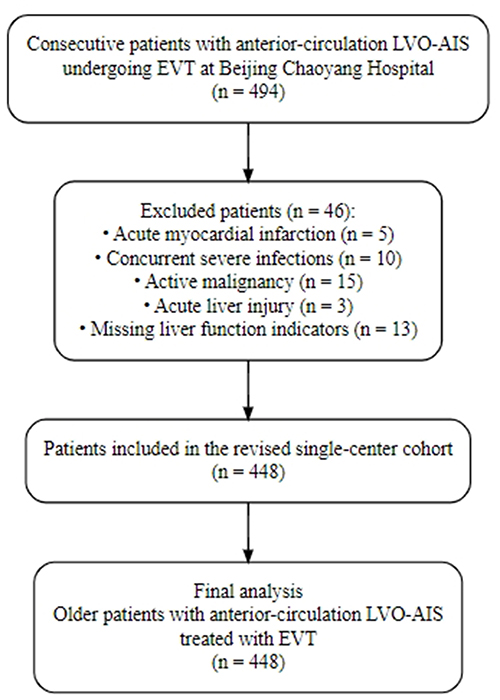 |
Figure 1 Study flowchart showing patient selection. |
Baseline characteristics according to troponin trajectory are presented in Table 1. Patients with dynamic myocardial injury were older and had higher prevalences of hypertension, diabetes mellitus, hyperlipidemia, and coronary artery disease. Baseline medication use was also summarized across troponin trajectory groups. Lipid-lowering therapy and antiplatelet therapy differed significantly among the groups, whereas antihypertensive, antidiabetic, and anticoagulant therapies did not. NIHSS scores were highest in the dynamic injury group, whereas ASPECTS were lower in patients with myocardial injury. The distribution of TOAST classification and successful reperfusion differed significantly across groups, whereas occlusion site and first-line thrombectomy technique did not. FIB-4 and CRP levels differed significantly across troponin trajectory groups.
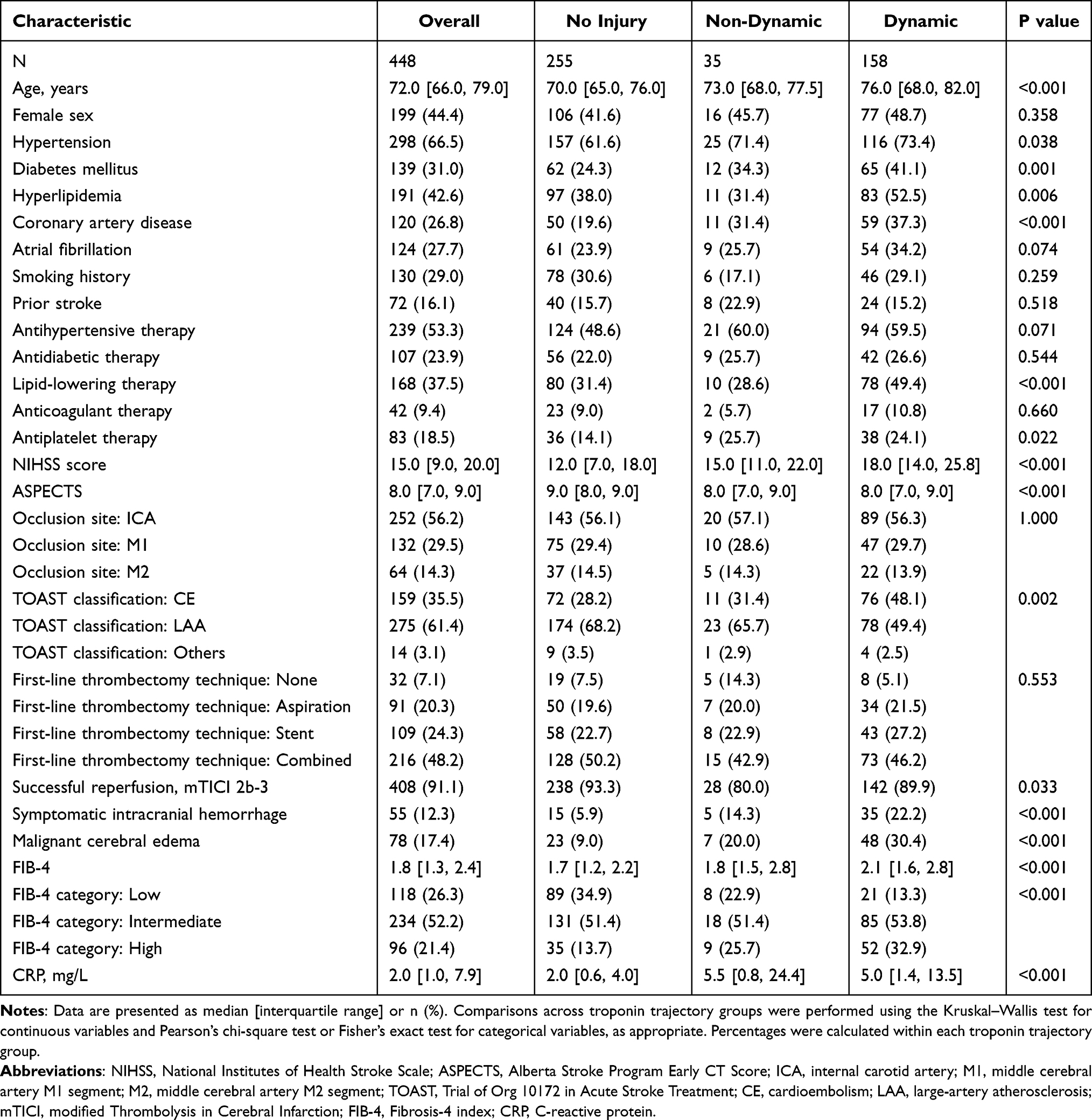 |
Table 1 Patient Demographics and Baseline Characteristics According to Troponin Trajectory |
Baseline characteristics according to FIB-4 category are shown in Supplementary Table S1. Patients with higher FIB-4 categories were older and had higher prevalences of atrial fibrillation and anticoagulant therapy use. NIHSS scores and CRP levels increased across FIB-4 categories, whereas ASPECTS decreased. The distribution of troponin trajectory differed significantly across FIB-4 categories, with dynamic myocardial injury observed in 17.8%, 36.3%, and 54.2% of patients in the low, intermediate, and high FIB-4 groups, respectively.
Exploratory post hoc pairwise comparisons for variables with significant overall differences are provided in Supplementary Tables S2 and S3.
Association of FIB-4 and CRP with Troponin Trajectory
Higher FIB-4 category was associated with more severe troponin trajectory in ordinal logistic regression analyses (Table 2). In the fully adjusted model, both the intermediate and high FIB-4 groups were associated with higher odds of more severe troponin trajectory compared with the low FIB-4 group [intermediate vs. low: OR 2.04, 95% CI 1.18–3.59; P = 0.011; high vs. low: OR 3.14, 95% CI 1.59–6.30; P = 0.001].
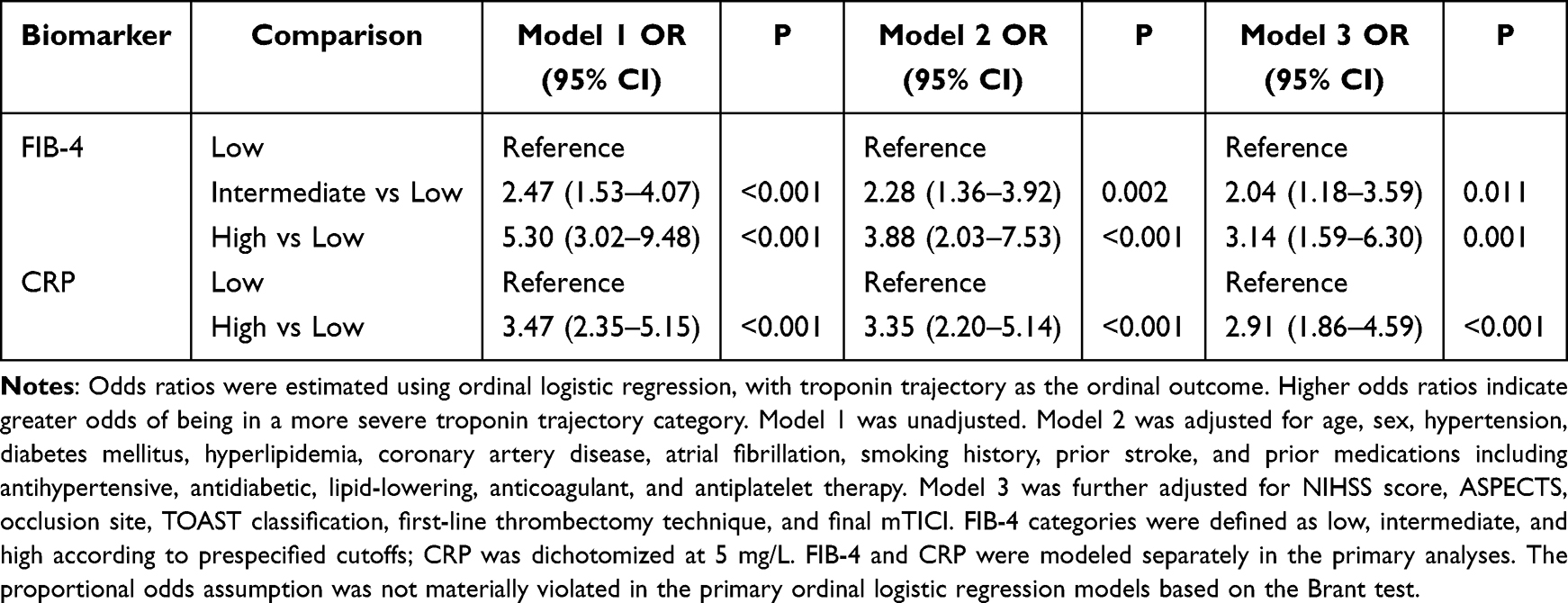 |
Table 2 Association of FIB-4 and CRP with Troponin Trajectory |
Elevated CRP was also associated with more severe troponin trajectory. In the fully adjusted model, CRP ≥5 mg/L was associated with higher odds of more severe troponin trajectory [OR 2.91, 95% CI 1.86–4.59; P < 0.001]. Restricted cubic spline models were fitted using three knots placed at the 10th, 50th, and 90th percentiles, with the median value as the reference. P values for overall association and non-linearity are presented in Figure 2.
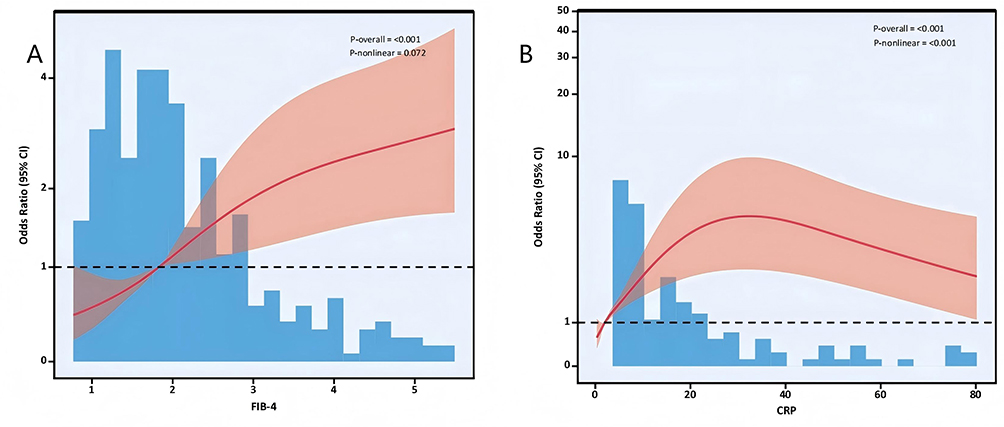 |
Figure 2 Restricted cubic spline analyses of the associations of FIB-4 and CRP with troponin trajectory. (A) Restricted cubic spline analysis of the association between FIB-4 and troponin trajectory. (B) Restricted cubic spline analysis of the association between CRP and troponin trajectory. The solid curve represents the estimated odds ratio for being in a more severe troponin trajectory category, and the shaded area represents the 95% confidence interval. |
CRP-Stratified Association Between High FIB-4 and Troponin Trajectory
In CRP-stratified analyses, the association between high FIB-4 and more severe troponin trajectory differed significantly by CRP status (P for interaction = 0.019; Table 3). Among patients with CRP ≥5 mg/L, high FIB-4 was associated with more severe troponin trajectory in the adjusted model [OR 3.40, 95% CI 1.49–7.76; P = 0.004]. Among patients with CRP <5 mg/L, the association was not statistically significant [OR 0.69, 95% CI 0.30–1.58;P = 0.379].
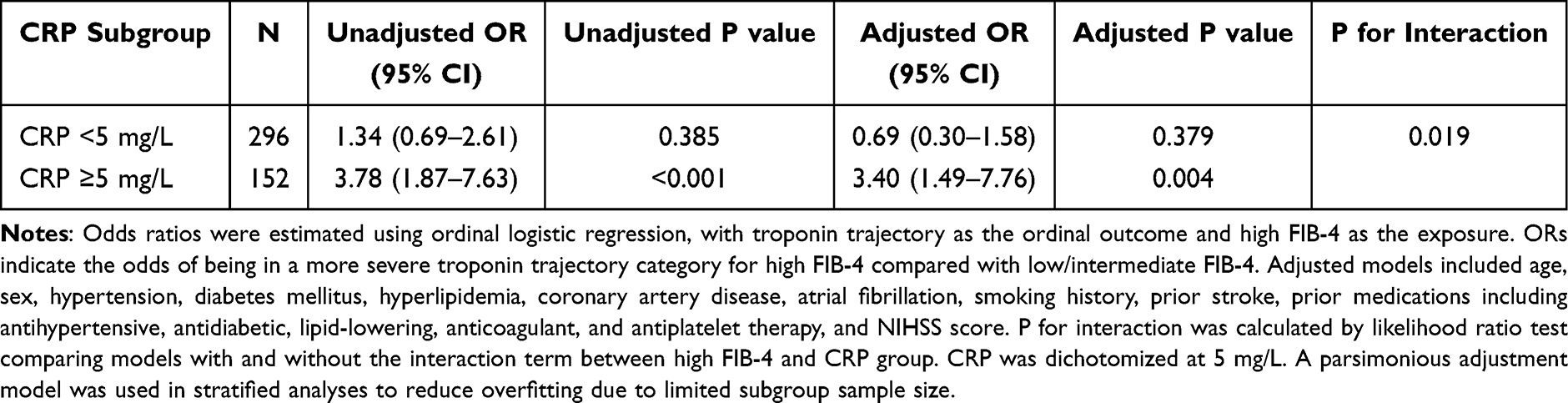 |
Table 3 Association Between High FIB-4 and Troponin Trajectory Stratified by CRP Status |
Association Between Troponin Trajectory and 90-Day Mortality
Overall, 67 of 448 patients died within 90 days. Mortality rates increased across troponin trajectory groups: 5.1% in the no myocardial injury group, 14.3% in the non-dynamic myocardial injury group, and 31.0% in the dynamic myocardial injury group (Table 4).
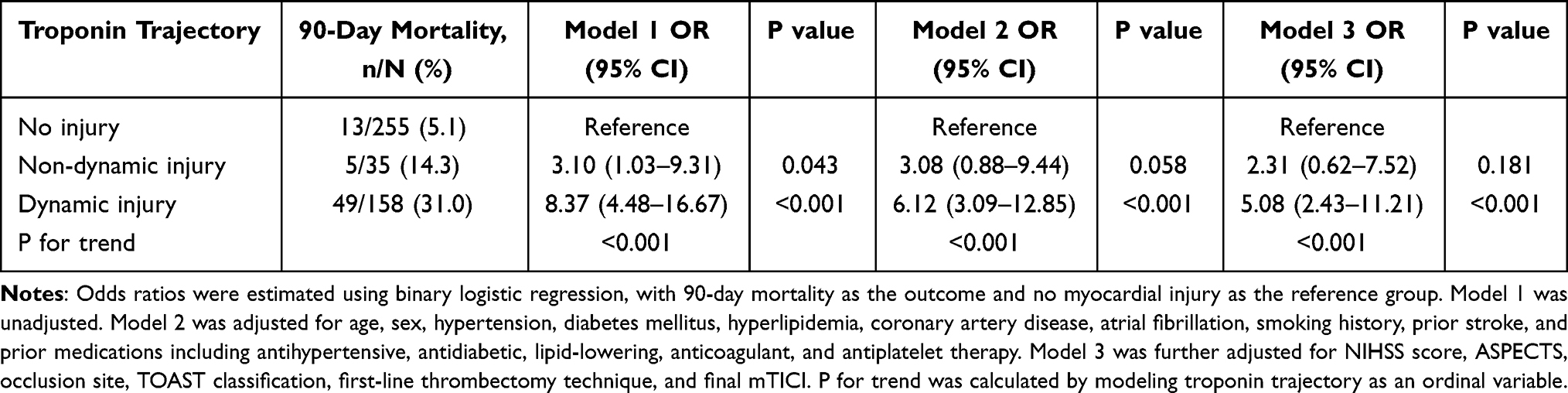 |
Table 4 Association Between Troponin Trajectory and 90-Day Mortality |
Compared with no myocardial injury, dynamic myocardial injury was associated with higher odds of 90-day mortality in the unadjusted model [OR 8.37, 95% CI 4.48–16.67; P < 0.001], Model 2 [OR 6.12, 95% CI 3.09–12.85; P < 0.001], and Model 3 [OR 5.08, 95% CI 2.43–11.21; P < 0.001]. Non-dynamic myocardial injury was not significantly associated with 90-day mortality in Model 3 [OR 2.31, 95% CI 0.62–7.52; P = 0.181]. The trend across troponin trajectory categories was significant in all models (all P for trend <0.001).
Supplementary Analyses
In exploratory subgroup analyses, P values for interaction were <0.05 for hyperlipidemia, CAD, antidiabetic therapy, lipid-lowering therapy, and antiplatelet therapy (Supplementary Table S4). The P value for interaction was 0.052 for diabetes mellitus.
In crude analyses, high FIB-4 was associated with higher odds of 90-day mortality in the overall cohort [OR 4.90, 95% CI 2.83–8.49; P < 0.001; Supplementary Table S5]. In analyses stratified by troponin trajectory, this association was significant in the dynamic myocardial injury group [OR 4.12, 95% CI 2.01–8.46; P < 0.001], but not in the no myocardial injury group [OR 1.97, 95% CI 0.51–7.54; P = 0.323] or the non-dynamic myocardial injury group [OR 6.00, 95% CI 0.81–44.35; P = 0.079]. The interaction between FIB-4 category and troponin trajectory was not statistically significant (P for interaction = 0.539).
Discussion
In this retrospective single-center cohort study of older patients with anterior-circulation LVO-AIS undergoing EVT, we found that higher FIB-4 and elevated CRP were independently associated with more severe troponin trajectory. In CRP-stratified analyses, the association between high FIB-4 and troponin trajectory was evident among patients with elevated CRP but not among those with low CRP, suggesting that systemic inflammation may modify the relationship between metabolic vulnerability and stroke-associated myocardial injury. We also found that dynamic myocardial injury was independently associated with increased 90-day mortality.
Several pathophysiological pathways may explain the association between elevated FIB-4 and post-stroke myocardial injury. Although FIB-4 was originally developed as a non-invasive marker of liver fibrosis, accumulating evidence suggests that it may also reflect systemic vulnerability and cardiovascular risk.7–11,27 In older patients with acute stroke, the components of FIB-4—age, aminotransferase levels, and platelet count—may capture overlapping domains of biological aging, metabolic dysfunction, hepatic stress, inflammation, and hemostatic disturbance. Endothelial oxidative stress, neuroinflammation, and blood–brain barrier disruption may further increase myocardial susceptibility to acute stress.28–30 In addition, liver dysfunction and platelet abnormalities are closely related to hemostatic dysregulation and immune-metabolic alterations, which may contribute to thromboinflammatory activation and cardiovascular instability.31,32 In the setting of AIS, autonomic dysregulation, catecholamine surge, endothelial dysfunction, and systemic inflammatory responses may converge to promote myocardial injury as part of SHS.29,30,33 Therefore, elevated FIB-4 in this context should be interpreted less as a specific indicator of overt liver fibrosis and more as a composite marker of reduced physiological reserve.
Our findings complement and extend previous studies on inflammatory markers and outcomes after stroke. Prior studies have shown that systemic inflammatory indices, including neutrophil-based markers, CRP, and composite immune-inflammatory scores, are associated with stroke severity and adverse outcomes after reperfusion therapy.12–14,34,35 CRP has also been linked to cardiac dysfunction and troponin elevation in ischemic stroke, supporting the biological plausibility of an inflammation-related pathway in post-stroke myocardial injury.36,37 Compared with studies focusing mainly on neurological outcomes or single biomarker measurements, our study examined troponin trajectory as an ordinal marker of myocardial injury evolution after stroke. By distinguishing no myocardial injury, non-dynamic myocardial injury, and dynamic myocardial injury, this approach may better capture clinically relevant heterogeneity in post-stroke cardiac involvement. The significant association between elevated CRP and more severe troponin trajectory further supports the role of systemic inflammation in stroke-associated myocardial injury.
A key finding of this study is the interaction between high FIB-4 and elevated CRP. One plausible interpretation is that FIB-4 reflects baseline metabolic or physiological vulnerability, whereas CRP reflects acute systemic inflammatory activation.7,38 Among patients with low CRP, high FIB-4 was not significantly associated with worse troponin trajectory, suggesting that chronic vulnerability alone may be insufficient to trigger evolving myocardial injury. In contrast, among patients with elevated CRP, high FIB-4 was associated with substantially higher odds of more severe troponin trajectory. This finding suggests that systemic inflammation may amplify the cardiovascular consequences of metabolic vulnerability in the acute stroke setting. Because this interaction was exploratory, it should be validated in larger cohorts.
The observed association between FIB-4 and troponin trajectory should also be interpreted against the background of pre-existing vascular disease and baseline treatment. Common comorbidities such as hypertension, diabetes mellitus, hyperlipidemia, coronary artery disease, atrial fibrillation, and prior stroke may increase myocardial susceptibility through chronic inflammation, endothelial dysfunction, atherosclerotic burden, and reduced cardiovascular reserve. Baseline medications may reflect the burden and treatment intensity of these conditions, while also potentially influencing inflammatory or thrombotic pathways. After incorporating these comorbidities and medication variables into the multivariable models, the main associations remained evident. Exploratory subgroup analyses suggested possible heterogeneity across selected comorbidity and medication strata, but these findings should be considered hypothesis-generating because of limited subgroup sample sizes.
The association between dynamic myocardial injury and 90-day mortality highlights the prognostic importance of serial troponin assessment after stroke. Previous studies have shown that troponin elevation after acute ischemic stroke is associated with poor outcomes, and recent evidence suggests that rising troponin patterns may provide additional prognostic information.2,4–6,39 Isolated troponin elevation may represent chronic structural heart disease, renal dysfunction, pre-existing myocardial injury, or resolving injury preceding the index stroke. In contrast, a rising troponin pattern after admission may better reflect acute evolving myocardial injury in the context of stroke–heart syndrome. In our cohort, dynamic myocardial injury was independently associated with markedly increased odds of 90-day mortality after adjustment for vascular risk factors, baseline medication use, stroke severity, infarct extent, stroke subtype, procedural characteristics, and final reperfusion status. These findings suggest that troponin trajectory may help identify patients with systemic decompensation and high short-term mortality risk after EVT.
From a clinical perspective, FIB-4 and CRP are inexpensive and widely available biomarkers that can be obtained from routine admission laboratory tests. Their combined interpretation may help identify older patients with LVO-AIS who are metabolically vulnerable and exposed to heightened inflammatory stress. For patients with high FIB-4 and elevated CRP, clinicians may consider closer cardiac surveillance, repeated troponin assessment, electrocardiographic monitoring, and multidisciplinary evaluation when clinically indicated. However, our findings do not establish that biomarker-guided interventions improve outcomes, and prospective studies are needed before these markers can be incorporated into standardized management pathways.
Several limitations should be acknowledged. First, this was a retrospective single-center study, which may limit causal inference and generalizability to other populations and treatment settings. Second, FIB-4 and CRP were measured at admission, and acute stroke itself may influence aminotransferase levels, platelet count, and inflammatory biomarkers. Therefore, FIB-4 in this context should be interpreted as a composite marker of systemic vulnerability rather than as a specific marker of chronic liver fibrosis. Third, troponin was measured at two predefined time points only, and more frequent sampling might have provided a more detailed characterization of myocardial injury evolution. Fourth, cardiac imaging, electrocardiographic monitoring data, and adjudicated cardiac causes of death were not systematically available, limiting mechanistic interpretation of myocardial injury. Fifth, although we adjusted for major comorbidities, baseline medication use, stroke severity, procedural variables, and final reperfusion status, residual confounding from unmeasured factors cannot be excluded. Finally, the subgroup and interaction analyses were exploratory and should be interpreted cautiously because of limited sample size and sparse events in some strata. External validation in larger multicenter cohorts is warranted.
Conclusions
In older patients with anterior-circulation LVO-AIS undergoing EVT, higher FIB-4 and elevated CRP were associated with more severe troponin trajectory, and elevated CRP modified the association between high FIB-4 and myocardial injury trajectory. Dynamic myocardial injury was further associated with increased 90-day mortality. These findings suggest that combined assessment of FIB-4, CRP, and serial troponin may help characterize metabolic-inflammatory vulnerability and cardiac risk after EVT. External validation in larger prospective cohorts is warranted.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding authors, Dr. Hong Li, upon reasonable request and subject to institutional and ethical restrictions regarding patient confidentiality.
Institutional Review Board Statement
The study was approved by the Ethics Committee of Beijing Chaoyang Hospital, Capital Medical University. The requirement for written informed consent was waived by the Ethics Committee because this was a retrospective observational study using existing medical records, involved no direct patient contact or intervention, and posed minimal risk to participants. All patient data were anonymized or de-identified before analysis and handled confidentially. The study was conducted in accordance with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by Noncommunicable Chronic Diseases-National Science and Technology Major Project, grant number 2024ZD0526800/2024ZD0526806.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Nogueira RG, Jadhav AP, Haussen DC, et al. Thrombectomy 6 to 24 hours after stroke with a mismatch between deficit and infarct. N Engl J Med. 2018;378(1):11–12. doi:10.1056/NEJMoa1706442
2. Rosso M, Ramaswamy S, Mulatu Y, et al. Rising cardiac troponin: a prognostic biomarker for mortality after acute ischemic stroke. J Am Heart Assoc. 2024;13(4):e032922. doi:10.1161/JAHA.123.032922
3. Ma S, Li J, Kong Q, et al. Impact of acute myocardial injury on short- and long-term outcomes in patients with primary intracerebral hemorrhage. J Am Heart Assoc. 2025;14(3):e037053. doi:10.1161/JAHA.124.037053
4. Jiang C, Xiong X, Chen C, et al. Elevated baseline high-sensitivity cardiac troponin T associates with early neurological deterioration after thrombectomy for acute ischemic stroke. Am J Cardiol. 2025;256:1–7. doi:10.1016/j.amjcard.2025.07.016
5. Cheng Z, Zhan Z, Huang X, et al. Troponin elevation on admission along with dynamic changes and their association with hemorrhagic transformation after thrombolysis. Front Aging Neurosci. 2021;13:758678. doi:10.3389/fnagi.2021.758678
6. Chen F, Bai X, Wang X, et al. Impact of high-sensitivity troponin elevation and dynamic changes on 90-day mortality in patients with acute ischemic stroke after mechanical thrombectomy: results from an observational cohort. J Neurointerv Surg. 2023;15(11):1142–1147. doi:10.1136/jnis-2022-019682
7. Devesa A, Delgado V, Valkovic L, et al. Multiorgan imaging for interorgan crosstalk in cardiometabolic diseases. Circ Res. 2025;136(11):1454–1475. doi:10.1161/CIRCRESAHA.125.325517
8. Gao W, She J, Wu X, et al. Association of liver fibrosis-4 index with functional outcomes in Chinese patients with acute ischemic stroke undergoing mechanical thrombectomy. Sci Rep. 2025;15(1):13086. doi:10.1038/s41598-025-98426-w
9. Bixler D, Zhong Y, Ly KN, et al. Mortality among patients with chronic hepatitis B infection: the chronic hepatitis cohort study (CHeCS). Clin Infect Dis. 2019;68(6):956–963. doi:10.1093/cid/ciy598
10. Çadırci E, Sorgun MH, Bozkurt KU, et al. Is the FIB-4 score a prognostic factor in acute ischemic stroke patients receiving intravenous thrombolytic therapy? J Clin Neurosci. 2025;136:111251. doi:10.1016/j.jocn.2025.111251
11. Norata D, Lattanzi S, Broggi S, et al. Liver fibrosis-4 score predicts outcome of patients with ischemic stroke undergoing intravenous thrombolysis. Front Neurol. 2023;14:1103063. doi:10.3389/fneur.2023.1103063
12. Rao Z, Zhang Y, Zhu C. Association of systemic immune-inflammation index with severity in acute ischemic stroke patients: a cross-sectional study. Front Neurol. 16:1553730. 2025. doi:10.3389/fneur.2025.1553730
13. Bian J, Guo S, Huang T, et al. CRP as a potential predictor of outcome in acute ischemic stroke. Biomed Rep. 2023;18(2):17. doi:10.3892/br.2023.1599
14. Finck T, Sperl P, Hernandez-Petzsche M, et al. Inflammation in stroke: initial CRP levels can predict poor outcomes in endovascularly treated stroke patients. Front Neurol. 2023;14:1167549. doi:10.3389/fneur.2023.1167549
15. Albers GW, Marks MP, Kemp S, et al. Thrombectomy for stroke at 6 to 16 hours with selection by perfusion imaging. N Engl J Med. 2018;378(8):708–718. doi:10.1056/NEJMoa1713973
16. Barber PA, Demchuk AM, Zhang J, Buchan AM. Validity and reliability of a quantitative computed tomography score in predicting outcome of hyperacute stroke before thrombolytic therapy. Lancet. 2000;355(9216):1670–1674. doi:10.1016/S0140-6736(00)02237-6
17. Adams HP Jr, Bendixen BH, Kappelle LJ, et al. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST Stroke. 1993;24(1):35–41. doi:10.1161/01.STR.24.1.35
18. Ay H, Benner T, Arsava EM, et al. A computerized algorithm for etiologic classification of ischemic stroke: the causative classification of stroke system. Stroke. 2007;38(11):2979–2984. doi:10.1161/STROKEAHA.107.490896
19. Goyal M, Menon BK, van Zwam WH, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet. 2016;387(10029):1723–1731. doi:10.1016/S0140-6736(16)00163-X
20. Zaidat OO, Yoo AJ, Khatri P, et al. Recommendations on angiographic revascularization grading standards for acute ischemic stroke: a consensus statement. Stroke. 2013;44(9):2650–2663. doi:10.1161/STROKEAHA.113.001972
21. Saver JL, Goyal M, Bonafe A, et al. Solitaire with the intention for thrombectomy as primary endovascular treatment for acute ischemic stroke trial: protocol for a randomized, controlled, multicenter study. Int J Stroke. 2015;10(3):439–448. doi:10.1111/ijs.12459
22. Winkelmeier L, Faizy TD, Brekenfeld C, et al. Comparison of thrombolysis in cerebral infarction 2b and 3 reperfusion in endovascular therapy for large ischemic anterior circulation strokes. J Neurointerv Surg. 2024;16(11):1076–1082. doi:10.1136/jnis-2023-020724
23. Li Z, Hao J, Wen C, et al. Predictive factors for very poor outcomes after endovascular thrombectomy in anterior circulation large vessel occlusion: a multicentre retrospective study in China. BMJ Open. 2025;15(10):e101244. doi:10.1136/bmjopen-2025-101244
24. Berger C, Fiorelli M, Steiner T, et al. Hemorrhagic transformation of ischemic brain tissue: asymptomatic or symptomatic? Stroke. 2001;32(6):1330–1335. doi:10.1161/01.STR.32.6.1330
25. von Kummer R, Broderick JP, Campbell BC, et al. The heidelberg bleeding classification: classification of bleeding events after ischemic stroke and reperfusion therapy. Stroke. 2015;46(10):2981–2986. doi:10.1161/STROKEAHA.115.010049
26. Beez T, Munoz-Bendix C, Steiger HJ, et al. Decompressive craniectomy for acute ischemic stroke. Crit Care. 2019;23(1):209. doi:10.1186/s13054-019-2490-x
27. Gorur M, Satar S, Acehan S, et al. FIB-4, a surrogate marker of liver fibrosis, predicts mortality and adverse events after acute myocardial infarction. Intern Emerg Med. 2025. doi:10.1007/s11739-025-04094-z
28. Craige SM, Kaur G, Bond JM, et al. Endothelial reactive oxygen species: key players in cardiovascular health and disease. Antioxid Redox Signal. 2025;42(16–18):905–932. doi:10.1089/ars.2024.0706
29. Levinson S, Pulli B, Heit JJ. Neuroinflammation and acute ischemic stroke: impact on translational research and clinical care. Front Surg. 12:1501359. 2025. doi:10.3389/fsurg.2025.1501359
30. Bernardo-Castro S, Sousa JA, Brás A, et al. Pathophysiology of blood-brain barrier permeability throughout the different stages of ischemic stroke and its implication on hemorrhagic transformation and recovery. Front Neurol. 2020;11:594672. doi:10.3389/fneur.2020.594672
31. Lisman T, Caldwell SH, Burroughs AK, et al. Hemostasis and thrombosis in patients with liver disease: the ups and downs. J Hepatol. 2010;53(2):362–371. doi:10.1016/j.jhep.2010.01.042
32. Li X, Zhang Q, Wang Z, et al. Immune and metabolic alterations in liver fibrosis: a disruption of oxygen homeostasis? Front Mol Biosci. 2022;8:802251. doi:10.3389/fmolb.2021.802251
33. Scheitz JF, Sposato LA, Schulz-Menger J, et al. Stroke-heart syndrome: recent advances and challenges. J Am Heart Assoc. 2022;11(17):e026528. doi:10.1161/JAHA.122.026528
34. Aierken K, Ma L, Zhu Y, et al. The association between the systemic immune-inflammation index and in-hospital mortality among acute ischemic stroke with atrial fibrillation patients undergoing intravenous thrombolysis. Front Cardiovasc Med. 2025;12:1541762. doi:10.3389/fcvm.2025.1541762
35. Jiang J, Tan C, Zhou W, et al. Plasma C-Reactive protein level and outcome of acute ischemic stroke patients treated by intravenous thrombolysis: a systematic review and meta-analysis. Eur Neurol. 2021;84(3):145–150. doi:10.1159/000514099
36. Jia M, Shi Y, Wang Y, et al. High-Sensitivity C-Reactive protein and ischemic stroke in patients with nonalcoholic fatty liver disease: a prospective study. J Healthc Eng. 2022;2022:9711712. doi:10.1155/2022/9711712
37. Montellano FA, Kluter EJ, Rücker V, et al. Cardiac dysfunction and high-sensitive C-reactive protein are associated with troponin T elevation in ischemic stroke: insights from the SICFAIL study. BMC Neurol. 2022;22(1):511. doi:10.1186/s12883-022-03017-1
38. McCracken C, Raisi-Estabragh Z, Veldsman M, et al. Multi-organ imaging demonstrates the heart-brain-liver axis in UK Biobank participants. Nat Commun. 2022;13(1):7839. doi:10.1038/s41467-022-35321-2
39. Loggini A, Bonin Pinto C, Von Hagn H, et al. Prognostic value of cardiac troponin I in acute ischemic stroke patients treated with reperfusion therapy: a multicenter retrospective cohort study. Int J Neurosci. 2025;135(15):1–8. doi:10.1080/00207454.2023.2279506
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Lymphocyte to Monocyte Ratio is Independently Associated with Futile Recanalization in Acute Ischemic Stroke After Endovascular Therapy
Guan J, Wang Q, Zhao Q
Neuropsychiatric Disease and Treatment 2023, 19:2585-2596
Published Date: 28 November 2023
The Effects of Remimazolam versus Propofol on Endovascular Thrombectomy for Acute Ischemic Stroke: Study Protocol for a Randomized Controlled Trial
Fu L, Zhou R, Jiang W, Lan L, Chen X, Cao Y, Xia L, Zhou Y, Han J, Zhou D, Zhang X
Vascular Health and Risk Management 2024, 20:533-539
Published Date: 3 December 2024
The Role of Fibrinogen in Mediating NGAL-Associated Neuronal Damage in Acute Ischemic Stroke: A Moderated Mediation Analysis
Zhao N, Chen Y, Lu Z, Han L, Song Y, Ding J, Zhu D, Guan Y
Journal of Inflammation Research 2024, 17:10557-10570
Published Date: 6 December 2024
Nomogram-Based Prediction of 3-Month Unfavorable Outcome and Early Neurological Deterioration After Endovascular Thrombectomy in Acute Ischemic Stroke
Wu Y, Han J, Cheng Y, Wei M, Liu F, Chen C, Tan Y, Ma W, Yu J, Han J, Luo G, Huo K
Therapeutics and Clinical Risk Management 2025, 21:239-256
Published Date: 27 February 2025
Safety and Clinical Outcomes of Endovascular Thrombectomy in Very Elderly Patients (≥80 Years) with Acute Ischemic Stroke: A Prospective Multicenter Cohort Study in Vietnam
Ngo TKT, Tran TC, Nguyen TH
Clinical Interventions in Aging 2026, 21:610832
Published Date: 9 June 2026