Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Family Functioning is Associated with Post-Stroke Depression in First-Ever Stroke Survivors: A Longitudinal Study
Authors Wang X, Hu CX, Lin MQ, Liu SY, Zhu FY, Wan LH
Received 13 October 2022
Accepted for publication 8 December 2022
Published 29 December 2022 Volume 2022:18 Pages 3045—3054
DOI https://doi.org/10.2147/NDT.S393331
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Taro Kishi
Xiao Wang,1,* Cai-Xia Hu,2,* Man-Qiu Lin,2 Shu-Ying Liu,2 Fen-Yan Zhu,3 Li-Hong Wan1
1School of Nursing, Sun Yat-sen University, Guangzhou, People’s Republic of China; 2Department of Neurology, Guangdong Provincial Hospital of Traditional Chinese Medicine, Guangzhou, People’s Republic of China; 3Department of Neurology, The Third Affiliated Hospital of Sun Yat-sen University, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Li-Hong Wan, School of Nursing, Sun Yat-sen University, 74 Zhongshan Road II, Guangzhou, 510080, People’s Republic of China, Tel +86 18926179419, Fax +86 020-87333043, Email [email protected]
Background: Post-stroke depression (PSD) can aggravate the mortality and recurrence rate in stroke patients. The relationship between family functioning and PSD at different phases after a first-ever stroke is unclear. The purpose of this longitudinal study was to investigate the patterns and relationship of family functioning and PSD at acute hospitalization and 6 months post-discharge in first-ever stroke survivors.
Methods: This is a longitudinal study conducted in Guangzhou, China. Family functioning and depression were measured by the Short Form Family Assessment Device (SF-FAD) and Self-Rating Depression Scale (SDS) at baseline and 6 months post-discharge. Multiple linear regression analysis was used to explore the relationship between family functioning and PSD.
Results: The prevalence of PSD at acute hospitalization and 6 months post-discharge was 32.9% and 20.0%, respectively. SDS scores decreased significantly from baseline to 6 months post-discharge, while SF-FAD scores did not change significantly during this period. The Pearson correlation coefficient showed that SF-FAD scores were positively associated with SDS scores at the two time points (r1 = 0.341, r2 = 0.510, P < 0.05). Multiple linear regression analyses indicated that SF-FAD scores could predict PSD at baseline (unstandardized coefficient: 7.010, P < 0.05) and 6 months post-discharge (unstandardized coefficient: 9.672, P < 0.001).
Conclusion: This study found that first-ever stroke survivors had good family functioning at baseline and 6 months post-discharge. The findings in this study verified that poor family functioning is positively associated with PSD at different phases post-stroke. Good family functioning is an important protective factor against PSD.
Keywords: family functioning, depression, stroke
Introduction
The socio-economic burden of stroke in China is sharply increasing, and the number of stroke patients in China ranks first worldwide, with approximately 17.04 million people over the age 40 have experienced strokes.1 Additionally, Chinese residents over the age of 25 have the highest lifetime risk of stroke in the world, which means about two-fifths of Chinese people have a stroke risk in their lifetime.2 Stroke is the leading cause of death and disability in China, which is characterized by high prevalence, mortality, and disability rates, posing a serious threat to the health of the Chinese population.1 The weighted prevalence of stroke in Chinese people over age 40 years is increasing with time, reaching 2.58% in 2019.3 In 2019, there were 3.94 million new cases of stroke, and stroke caused 2.19 million deaths and 45.9 million disability-adjusted life years (DALYs) in China.4
Stroke severely impairs the physical condition of patients, with studies showing that 10.4% of stroke patients experienced severe disability within 1 month after a stroke.5 Stroke survivors can also develop psychological disorders. Post-stroke depression (PSD) was the most common neuropsychiatric complication after a stroke, and about one-third of stroke patients experience post-stroke depression.6 The most common risk factors for PSD were stroke severity, cognitive deficits and physical impairment.7 Current studies found that 35.2% to 87% stroke patients had cognitive deficits, and there is a strong correlation between cognitive deficits and PSD.8 The Edelkraut study found that there is a higher incidence of depression in stroke patients with aphasia.9 The Williams and Demeyere study found that cognitive deficits in spatial attention, executive function, memory, number and language processing, and praxis could exacerbate depressive symptoms at 6 months post-stroke.10 Depression seriously threatens the recovery and health outcomes for stroke patients. Stroke survivors with depression are more likely to have less effective rehabilitation post-stroke, higher all-cause mortality, suicidal ideation and stroke recurrence.11–14 The stroke recurrence of patients with PSD was 1.48 times higher than that in those without PSD.14
Psychotherapy plays a significant role in the treatment of PSD, and social support is considered the most meaningful factor against PSD.15 In China, the family is the most basic social unit for individuals, and family relationships are an integral part of social support, especially for elder adults.16 Family functioning refers to the family’s ability to meet the basic needs of family members and personal growth needs, as well as the ability to cope with difficult circumstances.17 Family plays an important role in regulating an individual’s mental health, and one Chilean study conducted with 6206 families found that good family functioning is associated with fewer health problems in the family, especially a reduction of psychological and mental disorders.18 A Chinese study of different family structures found that it is family functioning rather than family structure that can significantly affect an individual’s psychological well-being.19 Family care is directly related to the quality of life of stroke patients at home.20
Current study suggest an association between family functioning and depression in patients with major depressive disorder, and patients with healthy family functioning have shorter duration of depression.21 Nan found that family care is beneficial in preventing depression in patients with chronic diseases, and patients with higher satisfaction with home support have lower depression levels.22 One cross-sectional study of stroke patients in the acute phase found that family functioning is negatively associated with PSD.23 Stroke patients remain at high risk of depression within 6 months post-stroke,24 but there is a lack of longitudinal studies exploring the relationship between family functioning and PSD in different phases after stroke.
Therefore, the purposes of this study were to explore the development of family functioning and PSD from acute hospitalization to 6 months post-discharge, as well as the association between family functioning and PSD at the two time points in this population.
Methods
Study Design and Participants
This was a longitudinal study conducted over a period of 6 months. Convenience sampling was used in this study. Stroke survivors were recruited from the inpatient department of neurology of a hospital in Guangzhou, China. The inclusion criteria included the following: (1) hospitalized within one month after first-ever ischemic stroke, and (2) having clear consciousness to be able to read the questionnaires. The exclusion criteria were as follows: (1) history of depression; (2) Wernicke aphasia, or (3) accompanying diseases such as heart or liver disease, renal insufficiency, or malignant tumors.
Questionnaire Instruments and Variables
Sociodemographic and Disease-Related Characteristics
Sociodemographic and disease-related information consisted of gender, age, education, marriage, job, family history of stroke, smoking, the diagnosis of diabetes, hyperlipidemia, and disability post-stroke. Disability post-stroke was assessed by the Modified Rankin Scale (mRS) with good validity and reliability.25 The total scores ranged from 0 (no disability) to 5 (severe disability requiring ongoing care). A score of ≥3 represents post-stroke disability.
Short Form Family Assessment Device
Family functioning was assessed by the Short Form Family Assessment Device (SF-FAD). The SF-FAD was simplified by Wang based on the Family Assessment Device.26,27 The SF-FAD contains six sub-scales, including problem solving, communication, affective responsiveness, affective involvement, behavior control and general functioning. SF-FAD contains 24 items, and each item has four responses “much like my home”, “like my home”, “not like my home”, or “not like my home at all” corresponding to a score of 1 to 4. The total SF-FAD score is equal to the total score of all entries/number of entries, and the total SF-FAD score ranges from 1 to 4. A higher SF-FAD and sub-scales score represents poorer family functioning, and a score lower than 2 indicates good family functioning. Cronbach’s alpha for the SF-FAD is 0.899.26
Self-Rating Depression Scale
Depression was measured using the Self-Rating Depression Scale (SDS). This scale was developed by Zung to assess depression in terms of psychotic emotional symptoms, corporality disorders, psychomotor disorders and depressed psychological disorders.28 The SDS consists of 20 items and the total score ranges from 20 to 80. Higher SDS scores indicate more severe depressive symptoms. The depression severity index is calculated from the cumulative score of 20 items out of 80 (maximum total score). The index ranges from 0.25 to 1.00. The higher the index, the more severe the depression, with an index ≥0.5 indicating depression.
Data Collection
For patients who met the study inclusion criteria, the investigator explained the purpose, significance, requirements of the study, and the principles of privacy protection. Patients were informed that they had the right to decide to participate in or refuse this study, and they could withdraw from the study at any time for any reason, which would not negatively affect their treatment. Data collection began after patients voluntarily participated and signed an informed consent form. Sociodemographic and disease-related characteristics were collected during acute hospitalization (T1), and family functioning and PSD were assessed using the SF-FAD and SDS at the two time points (T1, at acute hospitalization and T2, 6 months post-discharge). Baseline data were collected at T1, including sociodemographic and disease-related characteristics, SF-FAD and SDS. The investigators collected baseline data with participants face-to-face in the ward. Prior to the time point of 6 months post-discharge, the investigators contacted participants in advance by telephone to determine the follow-up time. Participants needed to complete the SF-FAD and SDS at T2. Follow-up data were collected during participants’ outpatient review. If the patient could not return to the hospital, telephone interviews or electronic questionnaires were used to collect information. One hundred and one participants were recruited at baseline and completed the baseline measurement (Figure 1). Eighty-five participants completed follow-up measurement at T2. Sixteen participants were excluded in this study because they did not complete follow-up assessment at T2 (three of whom had a recurrence of stroke and 13 refused follow-up or lost communication).
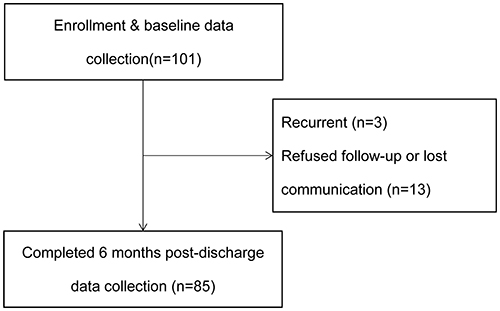 |
Figure 1 Flow chart of participants. |
Statistical Analysis
Descriptive statistical analyses were performed to describe sociodemographic and disease-related characteristics, family functioning and PSD. Paired t-tests were used to explore the changes in SF-FAD and SDS scores at the two time points. The relationship between participants’ sociodemographic and disease-related characteristics and PSD was measured by the independent sample t-test and one-way analysis of variance. The Pearson correlation coefficient was used to examine the relationship between SF-FAD and SDS scores at the two time points. Multiple linear regression analysis (stepwise method) was used to verify the association between family functioning and PSD at baseline and 6 months post-discharge. All variables with P < 0.3 in the univariate analysis, as well as some common influencing factors (age, gender),29,30 were included as independent variables in the multivariate analyses at the two time points. All statistical analyses were performed by SPSS 25.0 (IBM Corp, Armonk, NY, USA), and P values less than 0.05 were considered statistically significant.
Results
Sociodemographic and Disease-Related Characteristics
The sociodemographic and disease-related characteristics are shown in Table 1. Eighty-five participants completed the 6 months follow-up. Among them, 62.4% participants were male, 51.8% were over 60 years old, 50.6% had a high school/technical secondary school education or higher, 91.8% had a spouse and 31.8% were in service. Of the participants, 35.3% had a family history of stroke, 31.8% were smokers, 30.6% also had diabetes, 44.7% also had hyperlipidemia, and 18.8% had post-stroke disability.
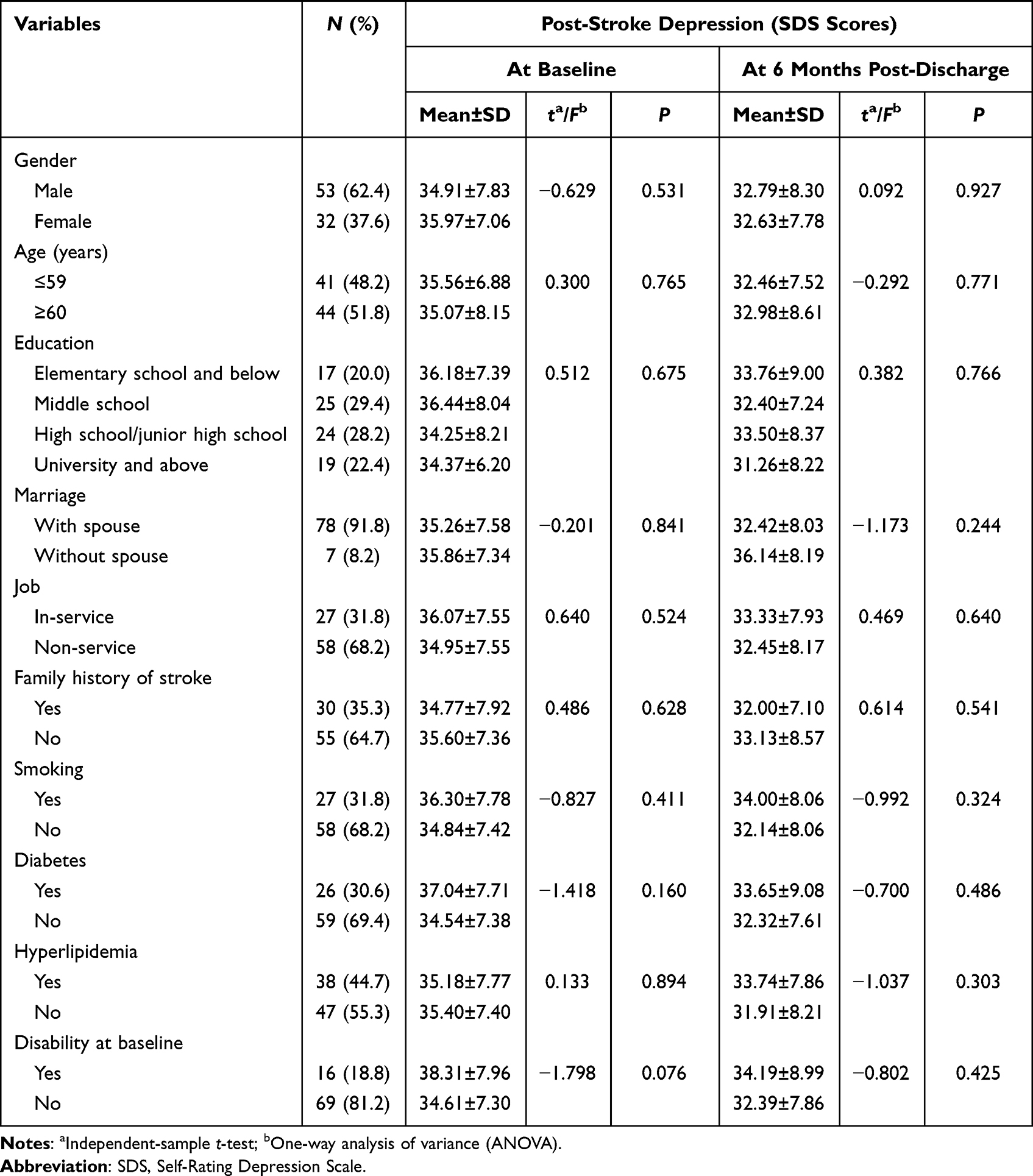 |
Table 1 Associations Between Sociodemographic and Disease-Related Characteristics of Participants and PSD at the Two Time Points (Univariate Analysis) |
The Levels and Changes in Family Functioning and PSD at T1 (at Baseline) and T2 (6 Months Post-Discharge)
The SDS scores were 35.31±7.52 at T1 and 32.73±8.06 at T2, reducing significantly (P=0.013). Table 2 indicates that 28 (32.9%) participants developed PSD during acute hospitalization, and 17 (20.0%) participants developed PSD at 6 months post-discharge, respectively.
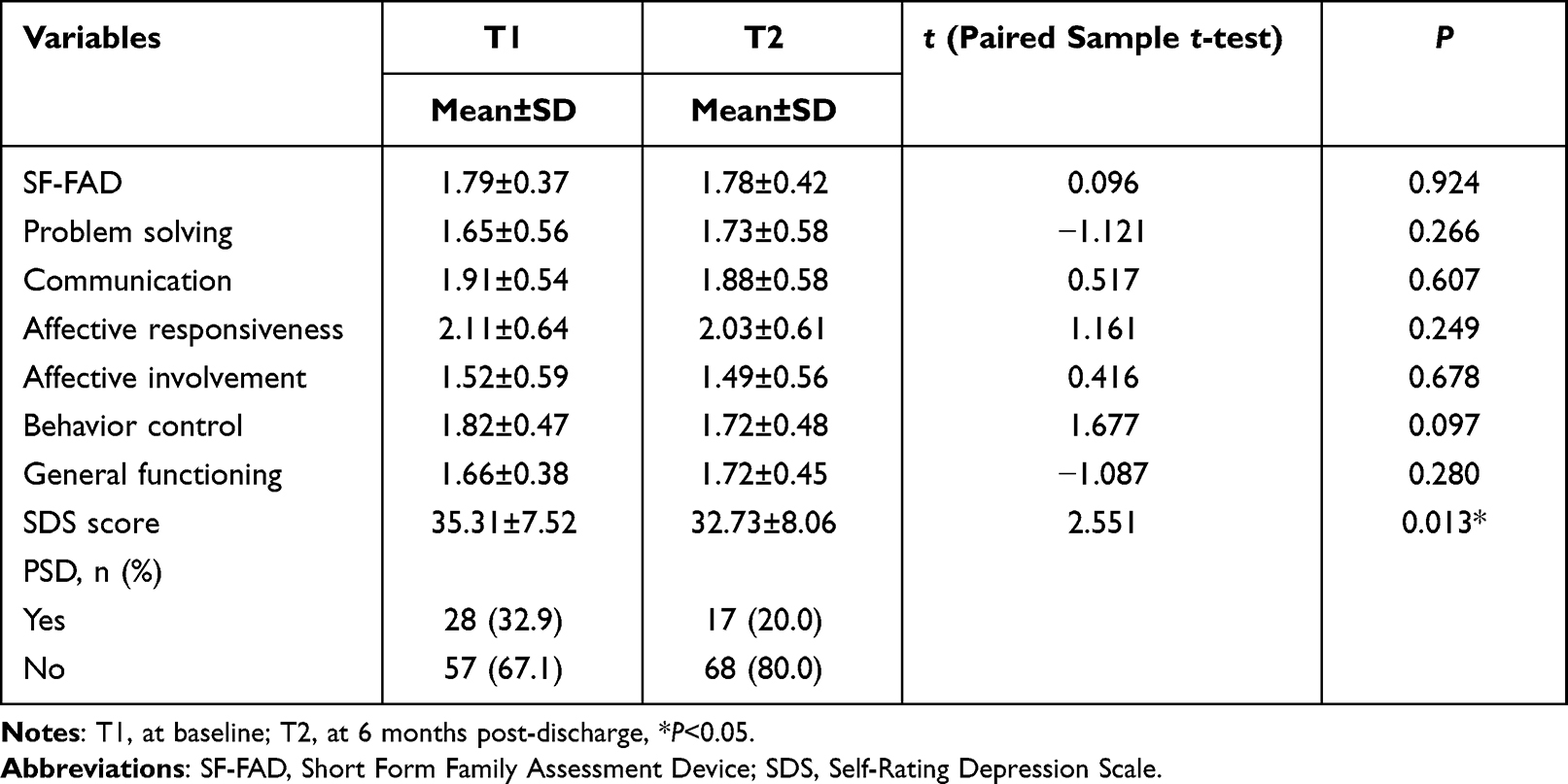 |
Table 2 Changes in Family Functioning and PSD at the Two Time Points |
The SF-FAD scores were 1.79±0.37 and 1.78±0.42 at the two time points, with no statistical difference in the SF-FAD scores during this period (P>0.05, Table 2). All sub-scale scores of the SF-FAD were not statistically changed between T1 and T2 (P>0.05).
Relationship Between Family Functioning and PSD at T1 (Baseline)
At T1, there was a positive correlation between SF-FAD and SDS score (r1=0.341, P=0.001, Table 3). Since higher SF-FAD and SDS score represent poorer family functioning and higher levels of depression severity, respectively, poor family functioning is positively associated with PSD at baseline. Scores on the sub-scales of “problem solving”, “communication”, “affective responsiveness”, “affective involvement”, and “general functioning” were positively correlated with SDS score (r1=0.297, 0.219, 0.288,0.296, 0.257, all P < 0.05).
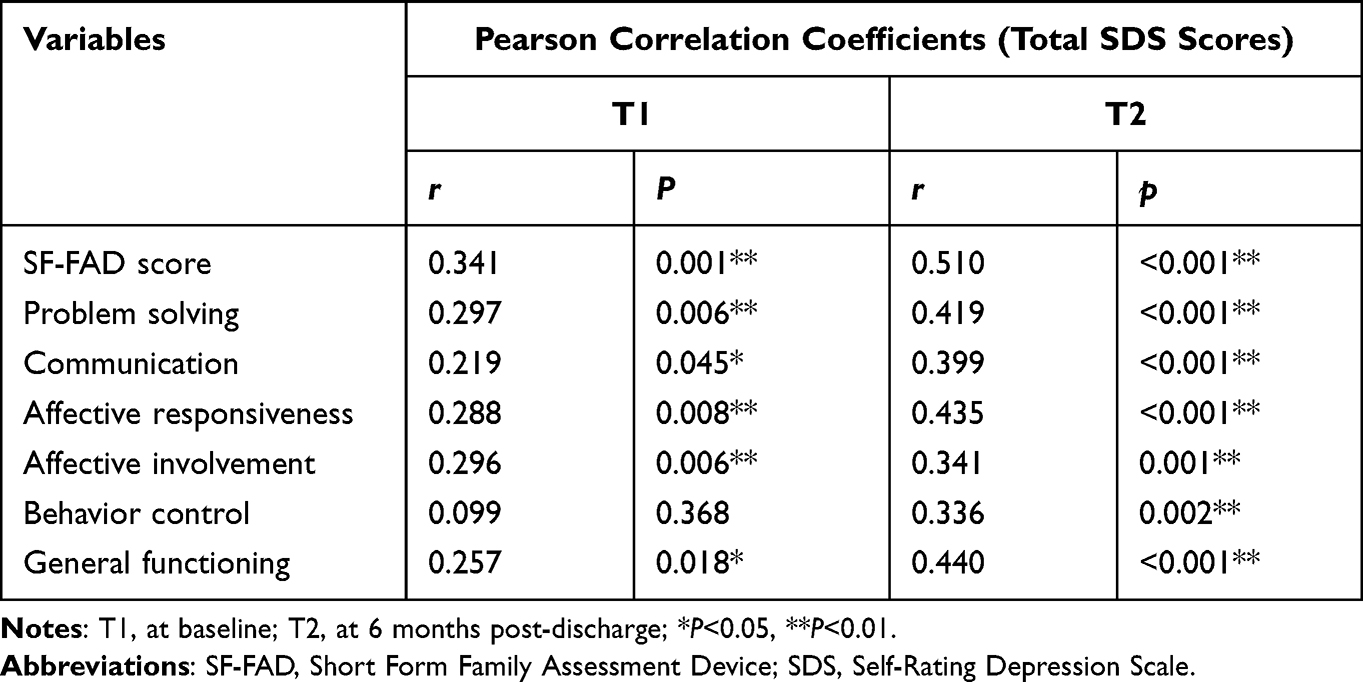 |
Table 3 The Association Between Family Functioning and PSD by Pearson Correlation Coefficients at the Two Time Points |
At baseline, the results of univariate analysis showed that sociodemographic and disease-related characteristics of participants were not associated with PSD (Table 1). The results of multiple linear regression analysis with the stepwise method at T1 showed that family functioning was the only factor for PSD (Table 4), and patients with higher SF-FAD score (poorer family functioning) had more severe depressive symptoms (unstandardized coefficient: 7.010, P=0.001, for model 1). This model explained approximately 10.5% of the variance in PSD at baseline (Rad2=0.105).
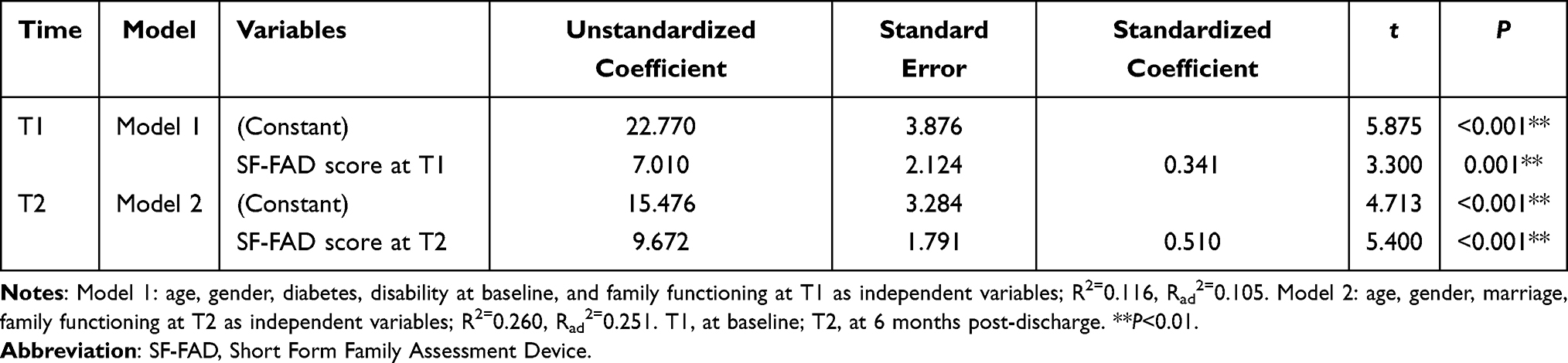 |
Table 4 The Association Between Family Functioning and PSD at the Two Time Points by Multiple Linear Regression (Stepwise Method) |
Relationship Between Family Functioning and PSD at T2 (at 6 Months Post-Discharge)
At T2, scores on SF-FAD and its six sub-scales (including problem solving, communication, affective responsiveness, affective involvement, behavior control and general functioning) were positively correlated with SDS score (r2=0.510, 0.419, 0.399, 0.435, 0.341, 0.336, 0.440, respectively, all P<0.05, Table 3).
Univariate analysis showed that there were no significant relationships between sociodemographic and disease-related characteristics and PSD at T2 (Table 1). The multiple linear regression results showed that family functioning remained associated with PSD at T2 (unstandardized coefficient: 9.672, P<0.001, Table 4). Family functioning explained approximately 25.1% of the variance in PSD at 6 months post-discharge in stroke patients (Rad2=0.251).
Discussion
This study shows that first-ever stroke survivors had a high risk of PSD. The prevalence of PSD at acute hospitalization and 6 months post-discharge was 32.9% and 20.0%, respectively. Poor family functioning is positively associated with PSD at the two time points, and good family functioning is an important factor in preventing PSD.
A previous study has found that depressive symptoms show a non-statistically significant downward trend from 1 month to 3 months post-stroke.31 This study further found that depressive symptoms significantly decreased from baseline to 6 months post-discharge. This study also found a high prevalence of PSD in the acute phase, which is similar to that in other studies.32,33 Of first-ever stroke survivors, 32.9% developed depression at acute hospitalization that needed attention. This study indicated that the risk of PSD is gradually reduced from acute hospitalization to 6 months post-discharge. It is noteworthy that one-fifth of participants suffered from PSD at 6 months post-discharge. PSD could contribute to a decline in the stroke patient’s physical function.34 Therefore, early identification and treatment of PSD are necessary. However, the screening and diagnosis of depression in stroke patients is seriously insufficient.35 One study found that only approximately 5% of stroke patients were diagnosed with depression in clinical practice.36 Considering stroke patients have a high risk of PSD, attention should be paid to depression screening of hospitalized stroke patients and continuous follow-up post-discharge.
The results showed that participants in this study had good family functioning at baseline and 6 months post-discharge, which is better than that one Chinese study of outpatient stroke patients.37 There were no significant differences in family functioning between the two time points. This suggests that the family system of the participants was robust enough to withstand the challenges of stroke post-discharge. This may have something to do with the family’s active coping with stroke. After a stroke, Chinese families make full use of family resources to meet the patient’s care and emotional needs,38 which contributes to the stability of the family system. Gawulayo’s study suggests that when families provide a support system for stroke patients, stroke may improve family relationships and strengthen emotional ties.39
This is the first longitudinal study to explore the association between family functioning and depression in stroke survivors. The results demonstrated the positive correlation between poor family functioning and PSD at baseline and 6 months post-discharge, and good family functioning is an important factor in preventing PSD. In addition, the sub-scale of general functioning represents overall functioning of family, and the “general functioning” sub-scale score is also positively related to PSD at the two time points. This further confirms the important role of family functioning in overcoming post-stroke depression. The observed preventive effect of good family functioning on PSD can be attributed to the stroke patients’ seeking support from their families. Family support and health status were found to be the most important protective factors against depression in Chinese older adults in one study.40 Elderly people with good family functioning had a comfortable home environment and better care, thereby reducing depressive symptoms.41 Stroke patients are dependent on family support, especially those with disabilities. One study showed that harmonious relationships between stroke patients and family members (including spouses and children) could enhance their life satisfaction.42 Therefore, when a stroke patient has a good and stable family support system, family members provide adequate life and emotional support to the patient, which helps to reduce the psychological stress in stroke patients.
An interesting finding was that “problem solving” sub-scale score was positively associated with PSD over time. Problem solving refers to the family’s ability to cope with challenges and resolve instrumental or emotional problems and conflicts to maintain the effective functioning of the family system.43 When a problem persists and cannot be solved, it will threaten the family system. For stroke patients and families, the onset of a stroke is a huge challenge, and it leads to a range of problems over time, including physical disability, psychological problems, and caregiving issues.
Caring for stroke patients is regarded as long-term, painful, and hard work for family caregivers that might impair their own physical and mental health.44,45 Family caregivers required a broad range of caregiving skills (such as medication administration, physical care, and nutrient), and they rely on clinical workers to obtain these relevant education.44 However, the truth is that it is difficult for caregivers to get the information they need from clinical workers.44 An intervention study found that problem-solving therapy was effective in reducing anxiety and depression levels and improving quality of life in stroke patients.46 Therefore, clinical workers should educate stroke patients’ families on skills for daily living and caregiving to improve their problem-solving abilities and thus improve the mental health of stroke patients.
This study found that a positive association between “communication” sub-scale score and PSD over time. A previous study in patients with major depression has found poor communication ability of families was associated with longer depression duration.21 This suggests that there should be a focus on the importance of family communication in alleviating the patient’s depressive symptoms.
There has been interest in studying the role of emotional support of family in preventing depression. The “affective involvement” sub-scale refers to family members taking an interest in each other’s affairs, and the “affective responsiveness” sub-scale indicates that family remember could provide appropriate affective reactions.17 The findings in this study showed the scores of “affective involvement” and “affective responsiveness” were positively correlated to PSD at the two time points, which means poor affective involvement and affective responsiveness ability was associated with more severe depressive symptoms. Fang’s study found that the positive attitude of family member would improve patients’ cognitive recovery.47
While the scores on “affective responsiveness” and “communication” sub-scales at the two time points indicate that stroke patients were performed poorly in these areas, which is consistent with the results of Jiang’s study.37 This may be related to the introverted character of the Chinese people, especially the elderly, who are not good at expressing their thoughts and emotions directly. Therefore, family members should be encouraged to pay attention to the patient’s psychological condition and actively communicate and respond to the patient’s emotional needs to help alleviate depressive symptoms.
It is noteworthy that first-ever stroke patients had a high incidence of PSD. This study demonstrated that good family functioning is an important factor in preventing PSD. This study makes important contributions for management of PSD in stroke patients: (1) Clinical staff should recognize the importance of involving family systems in caring for patients’ mental health; (2) Current interventions for PSD in stroke patients typically target the individual and ignore the impact of the family system on the individual’s mental health. Studies in patients with major depression have found positive outcomes of family interventions in alleviating depressive symptoms.48 This suggests that clinical workers should conduct family-based psychosocial interventions to prevent and treat PSD. (3) Family members should improve family functioning, including improving problem-solving skills, providing good care, offering adequate emotional support and communicating effectively to decrease stroke patients’ depressive symptoms.
Study Limitations
There are some limitations in this study. For instance, the participants enrolled in this study are from a single region in China, which may limit the generalization of the results. Patients’ family functioning and PSD were self-reported and therefore prone to bias. The sample size of this study was limited and future studies could expand the sample size to further investigate the relationship between family functioning and sociodemographic and disease-related factors and PSD.
Conclusion
First-ever stroke survivors are at high risk of depression at acute hospitalization and 6 months post-discharge. Medical workers need to monitor depressive symptoms in hospitalized stroke patients and continue to track their mental health post-discharge. This study demonstrates that family functioning is associated with PSD at acute hospitalization and 6 months post-discharge, and good family functioning is an important factor in preventing depression. Future interventions based on family systems should be considered to alleviate depression in post-stroke patients.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study was approved by the ethics committee of The Third Affiliated Hospital of Sun Yat-sen University (Approval no. [2018]02-421-01) in Guangzhou, China. This study was carried out in accordance with the Declaration of Helsinki. All participants signed the informed consent prior to their participation.
Acknowledgment
We thank all the participants in this study.
Funding
This study was funded by the General Project of the National Natural Science Foundation of China in 2018 (Grant number 71874211).
Disclosure
All authors report no conflicts of interest in this work.
References
1. Wang L, Peng B, Zhang H, et al. Brief report on stroke prevention and treatment in China, 2020. Chin J Cerebrovasc Dis. 2022;19(2):136–144.
2. Feigin VL, Nguyen G, Cercy K, et al. Global, regional, and country-specific lifetime risks of stroke, 1990 and 2016. N Engl J Med. 2018;379(25):2429–2437. doi:10.1056/NEJMoa1804492
3. Tu W, Hua Y, Yan F, et al. Prevalence of stroke in China, 2013–2019: a population-based study. Lancet Reg Health West Pac. 2022:100550. doi:10.1016/j.lanwpc.2022.100550
4. Ma Q, Li R, Wang L, et al. Temporal trend and attributable risk factors of stroke burden in China, 1990–2019: an analysis for the Global Burden of Disease Study 2019. Lancet Public Health. 2021;6(12):e897–e906. doi:10.1016/S2468-2667(21)00228-0
5. O’Donnell MJ, Chin SL, Rangarajan S, et al. Global and regional effects of potentially modifiable risk factors associated with acute stroke in 32 countries (INTERSTROKE): a case-control study. Lancet. 2016;388(10046):761–775. doi:10.1016/S0140-6736(16)30506-2
6. Mitchell AJ, Sheth B, Gill J, et al. Prevalence and predictors of post-stroke mood disorders: a meta-analysis and meta-regression of depression, anxiety and adjustment disorder. Gen Hosp Psychiatry. 2017;47:48–60. doi:10.1016/j.genhosppsych.2017.04.001
7. Babkair LA. Risk factors for poststroke depression: an integrative review. J Neurosci Nurs. 2017;49(2):73–84. doi:10.1097/JNN.0000000000000271
8. Terroni L, Sobreiro MFM, Conforto AB, et al. Association among depression, cognitive impairment and executive dysfunction after stroke. Dement Neuropsychol. 2012;6(3):152–157. doi:10.1590/S1980-57642012DN06030007
9. Edelkraut L, López-Barroso D, Torres-Prioris MJ, et al. Spectrum of neuropsychiatric symptoms in chronic post-stroke aphasia. World J Psychiatry. 2022;12(3):450–469. doi:10.5498/wjp.v12.i3.450
10. Williams OA, Demeyere N. Association of depression and anxiety with cognitive impairment 6 months after stroke. Neurology. 2021;96(15):e1966–e1974. doi:10.1212/WNL.0000000000011748
11. Kobylańska M, Kowalska J, Neustein J, et al. The role of biopsychosocial factors in the rehabilitation process of individuals with a stroke. Work. 2018;61(4):523–535. doi:10.3233/WOR-162823
12. Cai W, Mueller C, Li Y, Shen W, Stewart R. Post stroke depression and risk of stroke recurrence and mortality: a systematic review and meta-analysis. Ageing Res Rev. 2019;50:102–109. doi:10.1016/j.arr.2019.01.013
13. Bartoli F, Pompili M, Lillia N, et al. Rates and correlates of suicidal ideation among stroke survivors: a meta-analysis. J Neurol Neurosurg Psychiatry. 2017;88(6):498–504. doi:10.1136/jnnp-2017-315660
14. Wu QE, Zhou AM, Han YP, et al. Poststroke depression and risk of recurrent stroke: a meta-analysis of prospective studies. Medicine. 2019;98(42):e17235. doi:10.1097/MD.0000000000017235
15. Das J, R GK. Post stroke depression: the sequelae of cerebral stroke. Neurosci Biobehav Rev. 2018;90:104–114. doi:10.1016/j.neubiorev.2018.04.005
16. Chi I, Chou K. Social support and depression among elderly Chinese people in Hong Kong. Int J Aging Hum Dev. 2001;52(3):231–252. doi:10.2190/V5K8-CNMG-G2UP-37QV
17. Epstein NB, Bishop DS, Levin S. The McMaster model of family functioning. J Marital Fam Ther. 1978;4:19–31. doi:10.1111/j.1752-0606.1978.tb00537.x
18. García-Huidobro D, Puschel K, Soto G. Family functioning style and health: opportunities for health prevention in primary care. Br J Gen Pract. 2012;62(596):e198–e203. doi:10.3399/bjgp12X630098
19. Cheng Y, Zhang L, Wang F, Zhang P, Ye B, Liang Y. The effects of family structure and function on mental health during China’s transition: a cross-sectional analysis. BMC Fam Pract. 2017;18(1):59. doi:10.1186/s12875-017-0630-4
20. Baumann M, Le Bihan E, Chau K, Chau N. Associations between quality of life and socioeconomic factors, functional impairments and dissatisfaction with received information and home-care services among survivors living at home two years after stroke onset. BMC Neurol. 2014;14:92. doi:10.1186/1471-2377-14-92
21. Song J, Chen H, Liang T. Family functioning and 1-year prognosis of first-episode major depressive disorder. Psychiatry Res. 2019;273:192–196. doi:10.1016/j.psychres.2019.01.021
22. Nan H, Lee PH, McDowell I, Ni MY, Stewart SM, Lam TH. Depressive symptoms in people with chronic physical conditions: prevalence and risk factors in a Hong Kong community sample. BMC Psychiatry. 2012;12:198. doi:10.1186/1471-244X-12-198
23. Yang L, Zhao Q, Liu H, Zhu X, Wang K, Man J. Family functioning mediates the relationship between activities of daily living and poststroke depression. Nurs Res. 2021;70(1):51–57. doi:10.1097/NNR.0000000000000472
24. Towfighi A, Ovbiagele B, El Husseini N, et al. Poststroke depression: a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2017;48(2):e30–e43. doi:10.1161/STR.0000000000000113
25. Banks JL, Marotta CA. Outcomes validity and reliability of the modified Rankin Scale: implications for stroke clinical trials. Stroke. 2007;38(3):1091–1096. doi:10.1161/01.STR.0000258355.23810.c6
26. Wang M. The Construction of the Ecological Model of Healthy Behavior of Hypertension Patients with Stroke at the End of Recovery Period. Sun Yat-sen University; 2020.
27. Miller IW, Epstein NB, Bishop DS, Keitner GI. The McMaster family assessment device: reliability and validity. J Marital Fam Ther. 1985;11:345–356. doi:10.1111/j.1752-0606.1985.tb00028.x
28. Zung W, Gianturco J. Personality dimension and the self-rating depression scale. J Clin Psychol. 1971;27(2):247–248. doi:10.1002/1097-4679(197104)27:2<247::aid-jclp2270270230>3.0.co;2-6
29. Almhdawi KA, Alazrai A, Kanaan S, et al. Post-stroke depression, anxiety, and stress symptoms and their associated factors: a cross-sectional study. Neuropsychol Rehabil. 2021;31(7):1091–1104. doi:10.1080/09602011.2020.1760893
30. Lyu Y, Li W, Tang T. Prevalence trends and influencing factors of post-stroke depression: a study based on the National Health and Nutrition Examination Survey. Med Sci Monit. 2022;28:e933367. doi:10.12659/MSM.933367
31. Hu R, Wang X, Liu Z, et al. Stigma, depression, and post-traumatic growth among Chinese stroke survivors: a longitudinal study examining patterns and correlations. Top Stroke Rehabil. 2022;29(1):16–29. doi:10.1080/10749357.2020.1864965
32. Zhou X, Liu Z, Zhang W, Zhou L. Resilience is associated with post-stoke depression in Chinese stroke survivors: a longitudinal study. J Affect Disord. 2020;273:402–409. doi:10.1016/j.jad.2020.04.042
33. Isuru A, Hapangama A, Ediriweera D, Samarasinghe L, Fonseka M, Ranawaka U. Prevalence and predictors of new onset depression in the acute phase of stroke. Asian J Psychiatr. 2021;59:102636. doi:10.1016/j.ajp.2021.102636
34. El Husseini N, Goldstein LB, Peterson ED, et al. Depression status is associated with functional decline over 1-year following acute stroke. J Stroke Cerebrovasc Dis. 2017;26(7):1393–1399. doi:10.1016/j.jstrokecerebrovasdis.2017.03.026
35. Bhattacharjee S, Axon DR, Goldstone L, Lee JK. Patterns and predictors of depression treatment among stroke survivors with depression in ambulatory settings in the United States. J Stroke Cerebrovasc Dis. 2018;27(3):563–567. doi:10.1016/j.jstrokecerebrovasdis.2017.09.047
36. Swartz RH, Bayley M, Lanctôt KL, et al. Post-stroke depression, obstructive sleep apnea, and cognitive impairment: rationale for, and barriers to, routine screening. Int J Stroke. 2016;11(5):509–518. doi:10.1177/1747493016641968
37. Jiang S, Shen L, Ruan H, Li L, Gao L, Wan L. Family function and health behaviours of stroke survivors. Int J Nurs Sci. 2014;1:272–276. doi:10.1016/j.ijnss.2014.05.024
38. Qiu X, Sit J, Koo FK. The influence of Chinese culture on family caregivers of stroke survivors: a qualitative study. J Clin Nurs. 2018;27(1–2):e309–e319. doi:10.1111/jocn.13947
39. Gawulayo S, Erasmus CJ, Rhoda AJ. Family functioning and stroke: family members’ perspectives. Afr J Disabil. 2021;10:801. doi:10.4102/ajod.v10i0.801
40. Yu J, Li J, Cuijpers P, Wu S, Wu Z. Prevalence and correlates of depressive symptoms in Chinese older adults: a population‐based study. Int J Geriatr Psychiatry. 2012;27(3):305–312. doi:10.1002/gps.2721
41. Souza RA, Costa GDD, Yamashita CH, et al. Family functioning of elderly with depressive symptoms. Rev Esc Enferm USP. 2014;48(3):469–476. doi:10.1590/s0080-623420140000300012
42. Liu Y, Liu J, Zhou S, et al. Life satisfaction and its influencing factors of middle-aged and elderly stroke patients in China: a national cross-sectional survey. BMJ Open. 2022;12(8):e059663. doi:10.1136/bmjopen-2021-059663
43. Zhang Y. Family functioning in the context of an adult family member with illness: a concept analysis. J Clin Nurs. 2018;27(15–16):3205–3224. doi:10.1111/jocn.14500
44. Camak DJ. Addressing the burden of stroke caregivers: a literature review. J Clin Nurs. 2015;24(17–18):2376–2382. doi:10.1111/jocn.12884
45. Zhang J, Lee DTF. Meaning in stroke family caregiving: a literature review. Geriatr Nurs. 2017;38(1):48–56. doi:10.1016/j.gerinurse.2016.07.005
46. Chalmers C, Leathem J, Bennett S, Mcnaughton H, Mahawish K. The efficacy of problem solving therapy to reduce post stroke emotional distress in younger (18–65) stroke survivors. Disabil Rehabil. 2019;41(7):753–762. doi:10.1080/09638288.2017.1408707
47. Fang Y, Tao Q, Zhou X, et al. Patient and family member factors influencing outcomes of poststroke inpatient rehabilitation. Arch Phys Med Rehabil. 2017;98(2):249–55.e2. doi:10.1016/j.apmr.2016.07.005
48. Katsuki F, Watanabe N, Yamada A, Hasegawa T. Effectiveness of family psychoeducation for major depressive disorder: systematic review and meta-analysis. BJPsych Open. 2022;8(5):e148. doi:10.1192/bjo.2022.543
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Bidirectional Association Between Probable Depression and Multimorbidity Among Middle-Aged and Older Adults in Thailand
Pengpid S, Peltzer K, Anantanasuwong D
Journal of Multidisciplinary Healthcare 2023, 16:11-19
Published Date: 7 January 2023
Depressive Symptoms and Its Associated Factors Among Primary Caregivers of Stroke Survivors at Amhara Regional State Tertiary Hospitals: Multicenter Study
Eriku GA, Bekele G, Yitayal MM, Belete Y, Girma Y
Neuropsychiatric Disease and Treatment 2023, 19:1675-1684
Published Date: 28 July 2023
Risk Factors for Post-Stroke Depression Following the Lifting of COVID-19 Restrictions
Luo S, Hu X, Hong Y, Gao Y, Liu X, Peng Y, Tong X, Zhang X, Wen J
International Journal of General Medicine 2024, 17:3479-3491
Published Date: 13 August 2024
Family Functioning, Anxiety and Depression in Chinese Higher Vocational School Students: A Network Analysis
Ye L, Chen S, Chen QW, Luo X
Psychology Research and Behavior Management 2024, 17:4399-4412
Published Date: 25 December 2024
Clinical Efficacy of Acupuncture Combined with Escitalopram Oxalate in the Treatment of Mild-to-Moderate Post-Stroke Depression
Liu Y, Zhang G, Li J, Lv Y, Qi R
Neuropsychiatric Disease and Treatment 2025, 21:917-925
Published Date: 17 April 2025