Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Depressive Symptoms and Its Associated Factors Among Primary Caregivers of Stroke Survivors at Amhara Regional State Tertiary Hospitals: Multicenter Study
Authors Eriku GA ![]() , Bekele G, Yitayal MM, Belete Y, Girma Y
, Bekele G, Yitayal MM, Belete Y, Girma Y ![]()
Received 20 April 2023
Accepted for publication 19 July 2023
Published 28 July 2023 Volume 2023:19 Pages 1675—1684
DOI https://doi.org/10.2147/NDT.S418074
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Getachew Azeze Eriku,1 Gebremariam Bekele,2 Melisew Mekie Yitayal,1 Yihalem Belete,1 Yisak Girma1
1Department of Physiotherapy, School of Medicine, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 2Department of Physiotherapy, College of Medicine and Health Sciences, Bahir Dar University, Bahir Dar, Ethiopia
Correspondence: Getachew Azeze Eriku, Department of Physiotherapy, College of Medicine and Health Sciences, University of Gondar, P. O. Box: 196, Gondar, Ethiopia, Tel +251918518075, Email [email protected]
Background: Stroke is one of the leading causes of severe disability and functional limitation, which are reasons for being dependent on their family for daily activities and participation in social affairs. After discharge from the hospital, most stroke survivors require physical, psychosocial, and financial support from caregivers at home, which is one of the most stressful events for families. The stroke survivors and their caregivers may influence each other during the caregiving process and social life. The stroke survivor’s disability and depressive symptoms affect the quality of life of the survivor and their caregivers. Therefore, the purpose of this study was to assess the prevalence and associated factors of depression among caregivers of stroke survivors.
Methods: An institution-based, cross-sectional study was conducted in Amhara regional state tertiary hospitals. A systematic random sampling technique was employed to select 424 participants. The data were collected using an interviewer-administered and chart-reviewed structured questionnaire. The Patient Health Questionnaire-9 (PHQ-9) was used to assess depression. Univariable and multivariable logistic regression analyses were performed to identify factors associated with depression. Adjusting the odds ratio with the corresponding 95% confidence interval and variables with a P-value < 0.05 was considered significantly associated with depression.
Results: The overall prevalence of depressive symptoms was 65.6% (95% CI: 60.8– 69.8). Being female, older than 40, having no formal education, having a low family monthly income, being the son or daughter, and spending more than six hours per day were associated with depression.
Conclusion: We found that depression was prevalent among primary caregivers of stroke survivors. To reduce the risk of developing depression, policymakers should fully recognize the role of caregivers in caring for stroke patients. More attention should be given to caregivers who are female, elderly, have a low income, are sons or daughters, and spend a long time caring per day.
Keywords: depression, caregivers, stroke, Ethiopia
Background
Stroke is the second-leading cause of death and the third-leading cause of disability globally.1 Due to the chronic nature and disabling conditions that highly affect the functional performance as well as the daily activities of stroke patients, there is a high burden on the caregivers of the survivors, which leads to depression in the long term.2 Not only the stroke survivors, but depression is also a commonly reported problem in the caregivers or families of the stroke survivors.3 It is greater than the depression of stroke patients sometimes,4 and it is associated with negative health outcomes such as anxiety, psychological impairments, morbidity, and mortality.5
Stroke is a major source of mental health problems for both stroke survivors and caregivers, particularly those who provide care for prolonged periods of time due to their exposure to physiological, psychological, and financial pressure.6,7 These days, caregivers play a significant role in the healthcare system. For example, the report of the National Center shows that family caregivers hold first place in stroke survivors care more than other formal agencies, which make up the largest healthcare providers in the US and share the largest market value by exceeding the spending on nursing home care and other formal care expenditures.8 They have a crucial role in maintaining the body’s function, facilitating recovery, and preventing post-stroke complications.9 In addition, since caregivers have a significant role in providing physical and emotional support, the long-term functional outcome and quality of life of stroke survivors are dependent on the caregivers’ commitment, readiness, and physical and psychological well-being.10,11
The stroke survivors and their caregivers may influence each other during the caregiving process and social life. The stroke survivor’s disability and depressive symptoms affect the quality of life of the survivor and their caregivers.12 It was reported that the burden of depression among caregivers of stroke survivors ranges from 23% to 57%,13–16 and its global pooled prevalence is 40.2.17 The problems are expected to increase in low- and middle-income countries like Ethiopia as the burden of stroke increases progressively among stroke survivors.18 As different studies show in Ethiopia, about 27.5% to 49.6% of stroke survivors suffer from post-stroke depression.19–21 Despite this, only a handful of studies have been done on the burden of caregiver depression in Africa, and none in Ethiopia. Based on the findings in developed countries, much of our knowledge regarding the problem is based on studies done in developed countries, which have significant differences in the major contributing factors to caregiver depression. Caregiver depression has a direct relationship with stroke survivors’ health outcomes. The negative mental status of caregivers adversely affects the quality of life, social status, psychology, and prognosis of stroke survivors.22 Several factors have been identified as predictors of caregiver depression, including sociodemographic factors such as gender, age, education, income, caregiving duration, and relationship with the patient,23–25 as well as clinical and care situation factors.26,27
Considering that to know the burden and address the problem of depression and the consequences among stroke survivor caregivers, a baseline assessment of the magnitude in the local context is mandatory. As a result, the purpose of this study was to determine the prevalence of depression and its associated factors among caregivers of stroke survivors in Ethiopia. The present study will paint a clearer picture of the mental health problem of stroke caregivers, identify the factors affecting it, and determine the extent of the problem in Ethiopia. This study will contribute to addressing the psychosocial problems of the caregivers and play its role in enhancing stroke rehabilitation, especially for community-dwelling stroke survivors, as well as the health system through identifying relevant predictors of depression.
Method
Study Design and Setting
An institution-based, cross-sectional study was conducted from April to June 2022 in Amhara regional state tertiary hospitals. The University of Gondar Specialized Hospital (UOGSH), Felege Hiwot Specialized Hospital (FHSH), Tibebe Ghion Specialized Hospital (TGSH), and Dessie Specialized Hospital (DSH) were randomly selected for this study from the six specialized hospitals in the region. Those hospitals are found in Gondar, Bahir Dar, and Dessie City. Gondar City is situated in northwest Ethiopia, 662 km from Addis Abeba and about 175 km from Bahir Dar City, the capital of the Amhara region. The UOGSH is the main tertiary care center for more than 7 million people from different Gondar zones, such as central Gondar, north Gondar, west Gondar, south Gondar, and northwest Gondar (setit humera wolkaite Tegede).
Both TGSH and FHCSH are found in Bahir Dar city, the capital of Amhara national regional state, 560 km from Addis Abeba. These hospitals provide tertiary-level healthcare services as a major referral center for more than 5 million people from six different zones (Bahir Dar city administration, West Gojjam, East Gojjam, Awi, South Gondar, and Central Gondar zones) and the neighboring Benishangul Gumuz region.
DSH is found in Dessie town, the capital of the south Wollo zone, 401 km from Addis Abeba, and is the only tertiary care center in the south Wollo zone that provides service for more than 5 million people from south Wollo, north Wollo, Oromia special zone, and the neighboring Afar region.
Source Population, Study Population Inclusion and Exclusion Criteria
All primary caregivers of the stroke survivors who attend medical wards and outpatient physiotherapy clinics in selected hospitals were included in this study.
Primary caregivers who are willing to participate, aged 18 years or above, being able to communicate, being a principal caregiver for at least two weeks, and not being paid for the care provided.
Primary caregivers who have been providing care for at least two weeks and are aged 18 or older were included in the study.
The caregivers who had known intellectual or psychiatric impairments, disabilities, or underlying medical conditions were excluded from the study.
Sample Size Determination and Sampling Procedures
The sample size the study was calculated a using a single population proportion formula by considering 50% prevalence of caregiver burden, 95% confidence interval and 5% margin of error. Finally, the sample of 424 was obtained by addition of 10% non-response rate.

Where n=samples, P-prevalence d-margin of error.
The study participants were allocated proportionally from each specialized hospital according to the report obtained from each hospital from medical record (registration book). According to the monthly report obtained from each hospital, the average number of stroke survivors admitted to each hospital ranges from 65 to 80. Taking this into account, the average number of primary caregivers admitted in University of Gondar Specialized Hospital (UOGSH), Tibebe Ghion Specialized Hospital (TGSH), Felege Hiwot Specialized Hospital (FHSH), and Dessie Specialized Hospital (DSH) per three months was 218; 207; 228; and 218 respectively. Therefore, during the three-month data collection period, 871 primary caregivers of stroke survivors visited the selected hospitals. Thereafter, the skipping interval kth was calculated by dividing the three-month report by the calculated sample size (871/424), which resulted in 2. The study participants were selected every 2nd interval. The first case was selected randomly using a lottery method. Finally, a systematic random sampling technique was used to select all eligible caregivers of stroke survivors using the K interval. The participants included from UOGSH, TGSH, FHSH, and DSH were 106, 101, 111, and 106, respectively.
Data Collection Tools and Procedures
The data was collected using a structured interviewer administered questionnaire that was developed from different literature sources.5,17,28–30 The data collection instruments have three sections. The first section covered the sociodemographic characteristics of the participants, including sex, age, marital status, residence, educational level, occupation, family income, and relationship with the stroke survivors. The second section included the clinical characteristics of the participants, such as the duration of the stroke, duration of caregiving from onset, and caregiving hours per day.
The dependent variable, depression, was measured using the patients’ health questionnaire (PHQ-9) depression scale. Depression in the primary caregivers of the stroke survivors was assessed using the PHQ-9 depression assessment tool. The questionnaire was prepared in English and then translated into the local language, Amharic. The scale has been validated in Ethiopia with a sensitivity of 88%.31,32 According to the tool, the caregivers who scored greater than or equal to 10 were considered to have positive depression symptoms, whereas those scoring less than 10 were considered to have no depression.33
The data were collected by four trained physiotherapists, one from each hospital, and training was given to them by supervisors about the purpose of the study, how to approach the study participants, and data collection procedures.
Definition of Variables
The primary caregiver was defined as the person (family or non-family member) who spent most of the time providing daily care for the stroke survivors or the person who took on the main caregiving tasks.34
Anxiety disorder- is a 7-item instrument developed to identify generalized anxiety disorder in informal care patients. A score of 10 or greater on the GAD-7 represents a cut point for identifying GAD.35
Data Quality Assurance and Management
The data were collected through a pretested face-to-face interview using an interview-administered questionnaire, and the patient’s medical record was reviewed to confirm the duration of stroke. The pretest A pretest was done on 5% of the sample size at Debre Tabor Referral Hospital to check the response and language clarity. The questionnaire was checked for accuracy, completeness, and consistency daily by the study supervisor and principal investigator.
Data Processing and Analysis
The data were entered, cleaned, and analyzed using SPSS version 23. The frequencies, tables, proportions and cross tabs were used to present the deceptive findings. Univariable and multivariable logistic regression analysis was employed to identify the factors associated with depression. Variables with p-values less than 0.25 were chosen for multivariable analysis. The strength of association was presented by the odds ratio with a 95% confidence interval (CI). A p-value of less than 0.05 was considered statistically significant in the multivariable analysis of the study. There was no problem of multicollinearity, and the fitness of the model was checked by using the Hosmer-Lemeshow test.
Ethical Consideration and Consent to Participant
The ethical clearance obtained from the ethical review committee of the school of medicine under the delegation of the ethical review board of the university of Gondar with reference number (SOM/1546/2022). An official letter of support was received from the University of Gondar and sent to the clinical directors of the respective hospitals. Before the data collection, the purpose of the study, the potential indirect benefits, and the right to refuse were explained to each study participant. Finally, written informed consent was obtained from each study participant. The confidentiality of the information was assured throughout the data collection. The study was done in compliance with the Helsinki Declaration.
Result
Sociodemographic Characteristics of Primary Caregivers of Stroke Survivors
A total of 424 participants were included in this study. All the caregivers agreed to participate in the study, with a 100% response rate. The mean age of the participants was 40.2406 (SD± 10.95) years. More than half of the caregivers were female (54.2%) and aged 40 or younger (58.5%). Most of them were married (65.3%) and from urban residents (69.1%). More than one third of the participants had only primary education or had formal education, with 18.2% and 21.7%, respectively. See Table 1
 |
Table 1 Sociodemographic Characteristics of Characteristics of Primary Caregivers of Stroke Survivors in Amhara Regional State Tertiary Hospitals, (n=424) |
Clinical and Care Situation Characteristics of Primary Caregivers of Stroke Survivors
The majority of the stroke survivors (64.4%) had a duration of more than three months, and a majority of the caregivers (63.2%) were providing care for more than three months. More than one third of the caregivers (37.5%) spend more than six hours per day. See Table 2
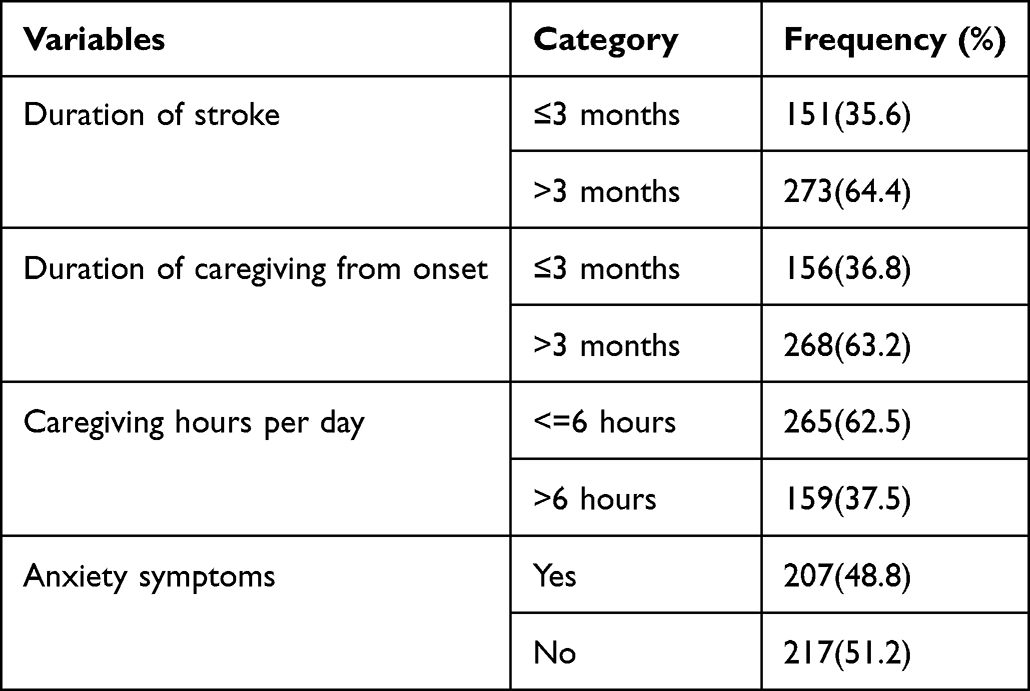 |
Table 2 Clinical and Care Situation Characteristics of Primary Caregivers of Stroke Survivors in Amhara Regional State Tertiary Hospitals, (n=424) |
Prevalence of Depression Among Caregivers of Stroke Survivors
The prevalence of depression among caregivers of stroke survivors was found to be 65.6% (95% CI: 60.8–69.8). Among respondents with depression, 80.9% were female, 71% were over the age of 40, and nearly 85% had a family monthly income of less than 3000 ETB.
Factors Associated with Depression Among Caregivers of Stroke Survivors
Variables with a p-value < 0.25 in univariable logistic regression analysis were exported to multivariable logistic regression analysis. Among these variables, being female, being older than 40 years, having no formal educations, low family income, being sons or daughters, and caregiving time were significantly associated with depression in multivariable logistic regression analysis.
The odds of being a female were four times more likely to have depression compared to males (AOR = 4.01, 95% CI (2.41, 6.66)). The odds of being older than 40 were two times more likely to develop depression compared to being 40 or younger (AOR = 1.98, 95% CI (1.096, 3.661). The odds of having no formal education are 0.43 times less likely to have depression than those who have a diploma and above (AOR = 0.43, 95% CI (0.204, 0.899)). The odds of having a monthly income of less than 3000 ETB 6 times more likely to develop depression as compared to caregivers who have a family monthly income of more than 6000 ETB (AOR = 5.9, 95% CI (2.856, 12.106)). Being a son or daughter is 2.5 times more likely to develop depression compared with being a spouse (AOR = 2.5, 95% CI (1.26, 4.867)). Caregivers who spent more than 6 hours per day were three times more likely to develop depression compared with caregivers who spent less than 6 hours per day (AOR = 2.8, 95% CI (1.56, 4.91). See Table 3
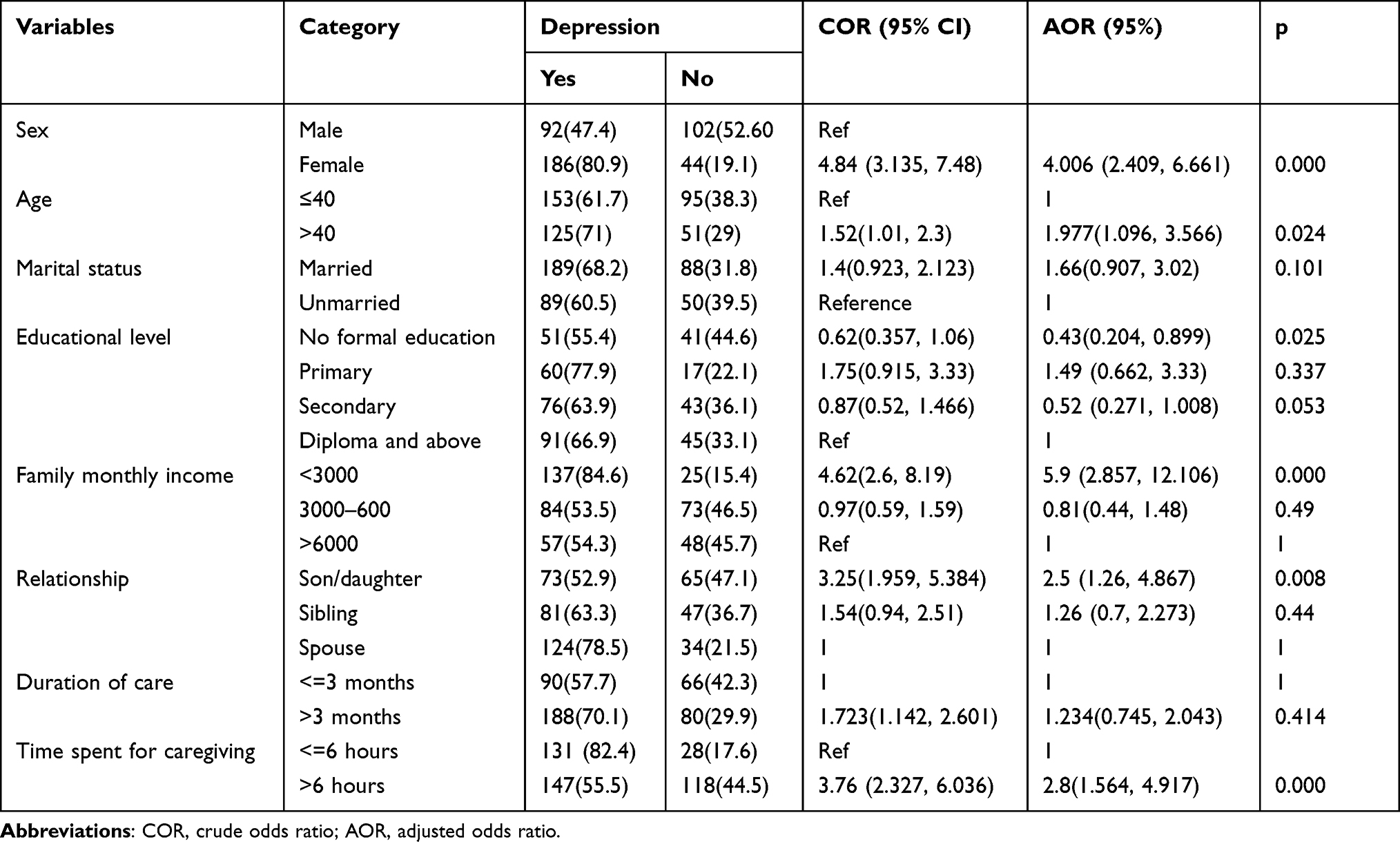 |
Table 3 Multivariate Logistic Regression of Factors Associated with Depression Among Primary Caregivers of Stroke Survivors in Amhara Regional State Tertiary Hospitals, (n=424) |
Discussion
The aim of this study was to assess the prevalence and associated factors of depression among primary caregivers of stroke survivors in Amhara regional state tertiary hospitals. The study showed that the overall prevalence of depression was reported to be 65.6% (95% CI: 60.8–69.8).
The finding of the present study was higher than that of Indonesia 56.7%,36 United States, 47.9%,37 Pakistan, 47.1%,5 Helsinki, 31 to 33%,24 Nigeria, 46.1%,38 Netherlands 23%,39 and Malaysia, 20.3%,40 and systematic review and meta-analysis of 12 studies 40.2%.17 The discrepancy of results might be due to the assessment tool, study design, sample size, the health care delivery system, economic status, life style and other sociodemographic factors. For instance, studies done in Nigeria, Helsinki, and Malaysia used the Beck depression inventory tool, whereas a study in Pakistan used the HAM-D-U scale to assess depression The other reason for the difference may be that in the Nigerian study, most of the caregivers were male and relatively younger than those in our study, which found participants in the age range of 19 to 39 years. In the Netherland, a small sample size was used, and only stroke patients with subarachnoid subtypes were included. In Helsinki, a different study design, the prospective follow-up study, was used, and depression was assessed at different points in time in the acute phase, at 6 months and 18 months, and additionally, most of the study participants were males, who are less likely to develop depression than females. The cultural and lifestyle differences, the quality of health care delivery, and the educational and economic factors could be contributing factors to the variation in findings. In comparison to other nations, Ethiopia’s health policy prioritizes disease prevention and control, with less emphasis on rehabilitation. These could be the factors that contribute to the burden and mental health problems of stroke survivors’ families.
The second objective of this study was to identify factors associated with depression among primary caregivers of stroke survivors. Being female, being older, having no formal education, having low family income, being a daughter, and spending long caregiving hours were significantly associated with depression.
Female caregivers were 4.01 times more likely to have depression than male caregivers (AOR = 4.01, 95% CI (2.41, 6.66)). This is supported by the studies conducted in Ethiopia with caregivers of cancer,41 epilepsy,42 and mental illness43,44 survivors. A systematic review and meta-analysis also revealed that female caregivers were significantly associated with a higher prevalence of depression among caregivers of stroke survivors.17 Although there is no clear evidence that shows the clear relationship why females were more likely to develop depression than males, females have more internalized symptoms, whereas males have more externalized symptoms;45 And also, the hormonal changes after premenstrual and menopausal transition, which are associated with a decrease in estrogen, may be another potential factor that would increase the risk of developing depression.46 Another possible explanation is that many people, particularly in Ethiopia, perceive female caregivers as more caring and trustworthy than male caregivers. Women’s numerous duties and obligations, such as child care, meal preparation, and homework, will raise their vulnerability to depression, especially in Ethiopian women.
The odds of developing depression among caregivers over the age of 40 were 1.98 times more likely compared with caregivers younger than 40 (AOR = 1.98, 95% CI (1.09, 3.66)). This was consistent with other studies conducted in Malaysia,40 and Pakistan.5 The possible explanation could be that everyone needs social connections to survive and thrive, but the elderly spends most of their time alone and socially isolated. Loneliness and social isolation are closely associated with a high burden of depression.47
Caregivers who have no formal education were 0.43 times less likely to develop depression as compared with those who have a diploma or higher (AOR = 0.43, 95% CI (0.204, 0.899)). In contrast with the previous studies, which revealed the education level of the caregiver was a protective factor for depression.5,19,48 Possible reasons are that although stroke is a leading cause of severe disability and poor quality of life, participants who have no formal education may have limited knowledge about the poor prognosis, the possible complications, and the psychosocial and economic impact it has on the survivors and their families, which could increase the risk of developing depression.
Caregivers with an average family income less than 3000 ETB were 5.9 times more likely to develop depression than those with an average family income greater than 6000 ETB (AOR = 5.9, 95% CI (2.857, 12.106)). This finding is consistent with the studies done in Ethiopia on caregivers of cancer survivors.41 Possible reasons include unexpected medication, food, and other related costs during care, but Ethiopia’s health insurance is not sufficient to cover the high costs of treatment. As a result, family and caregiver involvement is required, and more money is needed to cover the necessary expenses.
Being son or daughter of the stroke survivors are 2.5 times more likely to develop depression compared with caregivers who are spouses (AOR= 2.5, 95% CI (1.26, 4.867). The spouses may have several additional commitments at home, which increase the possibility of developing depression, as reported in several previous studies. In contrast to this, our study reported that caregivers who are the sons or daughters of stroke survivors are more likely to develop depressive symptoms than caregivers who are spouses. The possible reasons could be that sons and daughters are young in their age, which may make them less experienced in coping with such a stressful situation, and since they are economically dependent on the family, the economic crisis is also one of the other factors contributing to depressive symptoms.
Caregivers who spent more than 6 hours per day were 2.8 times more likely to develop depression compared with caregivers who spent less than 6 hours per day (AOR = 2.8, 95% CI (1.56, 4.91). This is in line with studies conducted in Malaysia,40 Indonesia,36 Ethiopia.44 The possible reasons could be that the longer duration spent on care provision increases the physical and mental load from caregiving activities, which causes fatigue, reduces quality of life, and is more likely to increase the risk of having depressive symptoms. This may also be due to the long care time per day occupying too much private time for the caregivers and thus reducing their work, social, and entertainment time.
Strength and Limitation
To the best of our knowledge, this is the first study in Ethiopia that examines the prevalence of depression and related variables among carers of stroke survivors.
The causal relationship could not be established since the study was cross-sectional. In Ethiopia, more prospective research with a large sample size, including the control group, is needed to establish the causal relationship. Furthermore, the research used different assessment tools to evaluate depression, so making valid comparisons across the various studies is difficult.
Conclusion
We found that depression was prevalent among primary caregivers of stroke survivors. Being female, older than 40, having no formal education, having a low average family income, and spending prolonged hours on caregiving were factors significantly associated with depression. The results of this study have several clinical implications for health services and policymakers. Because of the high prevalence of depressive symptoms among the caregivers of stroke survivors, mental health screening is needed not only for survivors but also for their caregivers. Prompt referral to mental health professionals and early intervention reduce the severity of depression in caregivers. Physicians and physical therapists caring for stroke survivors should pay particular attention to the mental health of caregivers who are women, over 40, low-income, and long-term caregivers.
Abbreviations
ETB, Ethiopian birr; SD, Standard deviation; ORs, Odds Ratios; CIs, Confidence Intervals; PHQ-9, Patient Health questionnaire-9; UOGSH, University of Gondar Specialized Hospital; TGSH, Tibebe Ghion Specialized Hospital; FHSH, Felege Hiwot Specialized Hospital; DSH, Dessie Specialized Hospital.
Data Sharing Statement
Please contact the corresponding author for data requests.
Ethical Approval and Consent to Participate
The ethical clearance was obtained from the ethical review committee of the school of medicine under the delegation of the University of Gondar institutional review board. Before enrollment, all participants provided written informed consent.
Acknowledgment
The authors would like to thank the University of Gondar and all the participants of the study for their cooperation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed to the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Feigin VL, Brainin M, Norrving B, et al. World Stroke Organization (WSO): global stroke fact sheet 2022. Int J Stroke. 2022;17(1):18–29. doi:10.1177/17474930211065917
2. Choi HL, Yang K, Han K, et al. Increased risk of developing depression in disability after stroke: a Korean nationwide study. Int J Environ Res Public Health. 2023;20(1):842. doi:10.3390/ijerph20010842
3. Hultman MT, Everson-Rose SA, Tracy MF, Lindquist R, Hadidi NN. Associations between characteristics of stroke survivors and caregiver depressive symptoms: a critical review. Top Stroke Rehabil. 2019;26(7):528–537. doi:10.1080/10749357.2019.1641010
4. Nuwamanya S, Nkola R, Najjuka SM, et al. Depression in Ugandan caregivers of cancer patients: the role of coping strategies and social support. Psycho-Oncology. 2023;32(1):113–124. doi:10.1002/pon.6057
5. Mansoor M, Pirani S, Aftab R, Nadeem T. Prevalence of depression in caregivers of stroke patients in Karachi, Pakistan. Pakist J Neurol Sci. 2022;17(02). doi:10.56310/pjns.v17i02.192
6. Imarhiagbe FA, Asemota AU, Oripelaye BA, et al. Burden of informal caregivers of stroke survivors: validation of the Zarit burden interview in an African population. Ann Afr Med. 2017;16(2):46–51. doi:10.4103/aam.aam_213_16
7. Jaracz K, Grabowska-Fudala B, Górna K, Kozubski W. Caregiving burden and its determinants in Polish caregivers of stroke survivors. Arch Med Sci. 2014;10(5):941–950. doi:10.5114/aoms.2014.46214
8. Parish SL, Pomeranz-Essley A, Braddock D. Family support in the United States: financing trends and emerging initiatives. Ment Retard. 2003;41(3):174–187. doi:10.1352/0047-6765(2003)41<174:FSITUS>2.0.CO;2
9. Glass TA, Matchar DB, Belyea M, Feussner JR. Impact of social support on outcome in first stroke. Stroke. 1993;24(1):64–70. doi:10.1161/01.STR.24.1.64
10. Young ME, Lutz BJ, Creasy KR, Cox KJ, Martz C. A comprehensive assessment of family caregivers of stroke survivors during inpatient rehabilitation. Disabil Rehabil. 2014;36(22):1892–1902. doi:10.3109/09638288.2014.881565
11. Pucciarelli G, Buck HG, Barbaranelli C, et al. Psychometric characteristics of the mutuality scale in stroke patients and caregivers. Gerontologist. 2016;56(5):e89–98. doi:10.1093/geront/gnw083
12. Yuliana S, Yu E, Rias YA, Atikah N, Chang HJ, Tsai HT. Associations among disability, depression, anxiety, stress, and quality of life between stroke survivors and their family caregivers: an actor-partner interdependence model. J Adv Nurs. 2023;79(1):135–148. doi:10.1111/jan.15465
13. Boerboom W, Ribbers G, Ribbers G, Heijenbrok-Kal MH, Center RR, Heijenbrok-Kal M. The relationship of coping style with depression, burden, and life dissatisfaction in caregivers of patients with subarachnoid haemorrhage. J Rehabil Med. 2014;46:321–326. doi:10.2340/16501977-1273
14. Epstein-Lubow GP, Beevers CG, Bishop DS, Miller IW. Family functioning is associated with depressive symptoms in caregivers of acute stroke survivors. Arch Phys Med Rehabil. 2009;90(6):947–955. doi:10.1016/j.apmr.2008.12.014
15. Henderson JG, Pollard CA. Prevalence of various depressive symptoms in a sample of the general population. Psychol Rep. 1992;71(1):208–210. doi:10.2466/pr0.1992.71.1.208
16. Sallim AB, Sayampanathan AA, Cuttilan A, Ho RC-M. Prevalence of mental health disorders among caregivers of patients with Alzheimer disease. J Am Med Dir Assoc. 2015;16(12):1034–1041. doi:10.1016/j.jamda.2015.09.007
17. Loh AZ, Tan JS, Zhang MW, Ho RC. The global prevalence of anxiety and depressive symptoms among caregivers of stroke survivors. J Am Med Dir Assoc. 2017;18(2):111–116. doi:10.1016/j.jamda.2016.08.014
18. Mukherjee D, Patil CG. Epidemiology and the global burden of stroke. World Neurosurg. 2011;76(6 Suppl):S85–90. doi:10.1016/j.wneu.2011.07.023
19. Zemed A, Sany K, Gahaw M. Burden of depression and predictors among Ethiopian stroke survivors: cross-sectional study. Ann Med Surg. 2021;71:102926. doi:10.1016/j.amsu.2021.102926
20. Wubshet TY, Geberemichael SG, Adilo TM, et al. Prevalence and associated factors of poststroke depression among outpatient stroke patients who have a follow-up at the outpatient neurology clinic of Zewditu Memorial Hospital in Addis Ababa, Ethiopia. Depress Res Treat. 2022;2022:9750035. doi:10.1155/2022/9750035
21. Tsehayneh F, Tafesse A. High prevalence of poststroke depression in ischemic stroke patients in Ethiopia. Neurol Res Int. 2020;2020:8834299. doi:10.1155/2020/8834299
22. Atteih S, Mellon L, Hall P, et al. Implications of stroke for caregiver outcomes: findings from the ASPIRE-S study. Int J Stroke. 2015;10(6):918–923. doi:10.1111/ijs.12535
23. Roth DL, Haley WE, Sheehan OC, et al. Depressive symptoms after ischemic stroke: population-based comparisons of patients and caregivers with matched controls. Stroke. 2020;51(1):54–60. doi:10.1161/STROKEAHA.119.027039
24. Berg A, Palomäki H, Lönnqvist J, Lehtihalmes M, Kaste M. Depression among caregivers of stroke survivors. Stroke. 2005;36(3):639–643. doi:10.1161/01.STR.0000155690.04697.c0
25. Saban KL, Mathews HL, Bryant FB, O’Brien TE, Janusek LW. Depressive symptoms and diurnal salivary cortisol patterns among female caregivers of stroke survivors. Biol Res Nurs. 2012;14(4):396–404. doi:10.1177/1099800412439458
26. Grant JS, Elliott TR, Weaver M, Glandon GL, Raper JL, Giger JN. Social support, social problem-solving abilities, and adjustment of family caregivers of stroke survivors. Arch Phys Med Rehabil. 2006;87(3):343–350. doi:10.1016/j.apmr.2005.09.019
27. Grant JS, Bartolucci AA, Elliot TR, Giger JN. Sociodemographic, physical, and psychosocial characteristics of depressed and non-depressed family caregivers of stroke survivors. Brain Injury. 2000;14(12):1089–1100. doi:10.1080/02699050050203586
28. Cameron JI, Cheung AM, Streiner DL, Coyte PC, Stewart DE. Stroke survivor depressive symptoms are associated with family caregiver depression during the first 2 years poststroke. Stroke. 2011;42(2):302–306. doi:10.1161/STROKEAHA.110.597963
29. King RB, Raad JH, Flaherty J, Hartke RJ. Stroke caregiver depression: qualitative comparison of treatment responders and nonresponders at 1 year. J Cardiovasc Nurs. 2022;37(6):581–588. doi:10.1097/JCN.0000000000000852
30. Suh M, Kim K, Kim I, Cho N, Choi H, Noh S. Caregiver’s burden, depression and support as predictors of post-stroke depression: a cross-sectional survey. Int J Nurs Stud. 2005;42(6):611–618. doi:10.1016/j.ijnurstu.2004.10.002
31. Degefa M, Dubale B, Bayouh F, Ayele B, Zewde Y. Validation of the PHQ-9 depression scale in Ethiopian cancer patients attending the oncology clinic at Tikur Anbessa Specialized Hospital. BMC Psychiatry. 2020;20(1):446. doi:10.1186/s12888-020-02850-3
32. Woledesenbet MA, Shumet Mekonen S, Sori LM, Abegaz TM. Epidemiology of depression and associated factors among asthma patients in Addis Ababa, Ethiopia. Psychiatry J. 2018;2018:5934872. doi:10.1155/2018/5934872
33. Achilike S, Beauchamp JE, Cron SG, et al. Caregiver burden and associated factors among informal caregivers of stroke survivors. J Neurosci Nurs. 2020;52(6):277–283. doi:10.1097/JNN.0000000000000552
34. Akosile CO, Banjo TO, Okoye EC, Ibikunle PO, Odole AC. Informal caregiving burden and perceived social support in an acute stroke care facility. Health Qual Life Outcomes. 2018;16(1):1–7. doi:10.1186/s12955-018-0885-z
35. Spitzer R, Kroenke K, Williams J, Löwe B. Generalized anxiety disorder 7-item (GAD-7) scale. Arch Intern Med. 2006;166:1092–1097. doi:10.1001/archinte.166.10.1092
36. Fauziah W, Kato M, Shogenji M, Tsujiguchi H, Taniguchi Y. Factors associated with depression among family caregivers of patients with stroke in Indonesia: a cross-sectional study. J Nurs Res. 2022;30(5):e231. doi:10.1097/jnr.0000000000000515
37. McLennon SM, Bakas T, Jessup NM, Habermann B, Weaver MT. Task difficulty and life changes among stroke family caregivers: relationship to depressive symptoms. Arch Phys Med Rehabil. 2014;95(12):2484–2490. doi:10.1016/j.apmr.2014.04.028
38. Chuka Ifeanyi U, Shehu Sa’ad F, Chukwukdi Martin O, Stanley monday M, Juliet Onyinyechukwu N. Prevalence of depression among primary caregivers of stroke survivors in Nigeria. Middle East J Rehabil Health Stud. 2018;5(2):e65080. doi:10.5812/mejrh.65080
39. Boerboom W, Jacobs EA, Khajeh L, van Kooten F, Ribbers GM, Heijenbrok-Kal MH The relationship of coping style with depression, burden, and life dissatisfaction in caregivers of patients with subarachnoid hemorrhage. J Rehabil Med. 2014;46(4):321–326.
40. Omar O, Abdul Aziz AF, Ali MF, Ja SEH A, Eusof Izzudin MP. Caregiver depression among home-bound stroke patients in an Urban community. Cureus. 2021;13(9):e17948. doi:10.7759/cureus.17948
41. Wassie LA, Azagew AW, Bifftu BB. Depression and its associated factors among primary caregivers of adult cancer patients at Northwest Amhara Regional States Referrals Hospitals oncology treatment units, Northwest Ethiopia, 2021. BMC Psychiatry. 2022;22(1):533. doi:10.1186/s12888-022-04182-w
42. Tsehay M, Necho M, Belete A, Srahbzu M. Depression and anxiety and their associated factors among caregivers of children and adolescents with epilepsy in three selected hospitals in Amhara region, Ethiopia: a cross-sectional study. PLoS One. 2022;17(7):e0271885. doi:10.1371/journal.pone.0271885
43. Minichil W, Getinet W, Derajew H, Seid S. Depression and associated factors among primary caregivers of children and adolescents with mental illness in Addis Ababa, Ethiopia. BMC Psychiatry. 2019;19(1):249. doi:10.1186/s12888-019-2228-y
44. Derajew H, Tolessa D, Feyissa GT, Addisu F, Soboka M. Prevalence of depression and its associated factors among primary caregivers of patients with severe mental illness in southwest, Ethiopia. BMC Psychiatry. 2017;17(1):88. doi:10.1186/s12888-017-1249-7
45. Albert PR. Why is depression more prevalent in women? J Psychiatry Neurosci. 2015;40(4):219–221. doi:10.1503/jpn.150205
46. Bartels M, Cacioppo JT, van Beijsterveldt TC, Boomsma DI. Exploring the association between well-being and psychopathology in adolescents. Behav Genet. 2013;43(3):177–190. doi:10.1007/s10519-013-9589-7
47. Zhang Y, Kuang J, Xin Z, et al. Loneliness, social isolation, depression and anxiety among the elderly in Shanghai: findings from a longitudinal study. Arch Gerontol Geriatr. 2023;110:104980. doi:10.1016/j.archger.2023.104980
48. Li N, Shou J. The prevalence and correlates of depression in elderly outpatients in community health centers. J Affect Disord Rep. 2021;3:100044. doi:10.1016/j.jadr.2020.100044
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Family Functioning is Associated with Post-Stroke Depression in First-Ever Stroke Survivors: A Longitudinal Study
Wang X, Hu CX, Lin MQ, Liu SY, Zhu FY, Wan LH
Neuropsychiatric Disease and Treatment 2022, 18:3045-3054
Published Date: 29 December 2022
The Morbidity and Associated Factors of Depression in Caregivers of Patients with Depressive Disorder
Lee Y, Lin PY, Huang YC, Chiu NM, Hung CF, Wang LJ
Neuropsychiatric Disease and Treatment 2023, 19:1853-1864
Published Date: 24 August 2023
Risk Factors for Post-Stroke Depression Following the Lifting of COVID-19 Restrictions
Luo S, Hu X, Hong Y, Gao Y, Liu X, Peng Y, Tong X, Zhang X, Wen J
International Journal of General Medicine 2024, 17:3479-3491
Published Date: 13 August 2024
Clinical Efficacy of Acupuncture Combined with Escitalopram Oxalate in the Treatment of Mild-to-Moderate Post-Stroke Depression
Liu Y, Zhang G, Li J, Lv Y, Qi R
Neuropsychiatric Disease and Treatment 2025, 21:917-925
Published Date: 17 April 2025
Rate of Post-Stroke Depression and Associated Factors in Saudi Single Tertiary Medical Center
Aljuhani T, Alsubaie S, Al-Mutairi AM, Altheyab AS, Alsahali AM, Alhamdan AS, Alqahtani FM, Olayan LH, Senitan M
Journal of Multidisciplinary Healthcare 2025, 18:5421-5430
Published Date: 2 September 2025