Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Factors Influencing Mechanical Ventilation and Inpatient Palliative Care Utilization in Patients With Chronic Obstructive Pulmonary Disease
Authors Kao LT, Yang CC, Wu YC ![]() , Ko SC, Liang YS, Liao KM
, Ko SC, Liang YS, Liao KM ![]() , Ho CH
, Ho CH ![]()
Received 27 November 2024
Accepted for publication 10 March 2025
Published 20 March 2025 Volume 2025:18 Pages 1695—1709
DOI https://doi.org/10.2147/JMDH.S509022
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Li-Ting Kao,1,* Chun-Chieh Yang,2,* Yu-Cih Wu,3 Shian-Chin Ko,4 Yi-Shan Liang,1 Kuang-Ming Liao,5,6 Chung-Han Ho3,7,8
1Department of Respiratory Therapy, Chi-Mei Medical Center, Tainan, Taiwan; 2Department of Intensive Care Medicine, Chi-Mei Medical Center, Tainan, Taiwan; 3Department of Medical Research, Chi-Mei Medical Center, Tainan, Taiwan; 4Department of Internal Medicine, Chi-Mei Medical Center, Tainan, Taiwan; 5Department of Internal Medicine, Chi Mei Medical Center Chiali, Tainan, Taiwan; 6Department of Nursing, Min-Hwei Junior College of Health Care Management, Tainan, Taiwan; 7Department of Information Management, Southern Taiwan University of Science and Technology, Tainan, Taiwan; 8Cancer Center, Taipei Municipal Wanfang Hospital, Taipei Medical University, Taipei, Taiwan
*These authors contributed equally to this work
Correspondence: Kuang-Ming Liao, Department of Internal Medicine, Chi Mei Medical Center Chiali, No. 606, Jialixing Jiali Dist, Tainan, 72263, Taiwan, Email [email protected] Chung-Han Ho, Department of Medical Research, Chi-Mei Medical Center, 901 Zhonghua Road Yongkang Dist, Tainan, 71004, Taiwan, Email [email protected]
Purpose: Palliative care is underutilized for severely ill patients with advanced chronic obstructive pulmonary disease (COPD) experiencing significant symptoms during hospitalization. The impact of mechanical ventilation on inpatient palliative care utilization remains largely unexplored. In this study, we aimed to investigate inpatient palliative care utilization among hospitalized patients with COPD requiring mechanical ventilation and examine the associated risk factors and clinical outcomes.
Patients and Methods: A retrospective nested case-control study was conducted using population-based claims datasets from 2017 to 2021. It included 36,848 hospitalized patients with COPD aged 40 and above, of which 16,118 (43.74%) required mechanical ventilation. Logistic regression was used to assess the association between mechanical ventilation and inpatient palliative care utilization, adjusting for relevant covariates.
Results: Of the total cohort, 5,596 patients (15.19%) utilized inpatient palliative care, including 1,275 (7.91%) requiring mechanical ventilation. Age, duration of mechanical ventilation, comorbidity severity, and hospital type influenced inpatient palliative care use. Patients with a Charlson Comorbidity Index score of 1– 2 and ≥ 3 were 24.06 and 51.59 times more likely, respectively, to receive palliative care compared to those with a Charlson Comorbidity Index score of 0. Ventilated patients in medical centers or regional hospitals were more likely to receive palliative care than those in district hospitals. Patients on mechanical ventilation who received care for 8– 30 days were over twice as likely to receive palliative care compared to those who received care for shorter durations.
Conclusion: Inpatient palliative care for patients with COPD was limited and varied based on the duration of mechanical ventilation and hospital type. To enhance patient-centered care, interdisciplinary teams should integrate palliative care throughout the illness journey.
Keywords: COPD, hospice palliative care, mechanical ventilation, end of life care, risk factor, mortality
Introduction
Chronic obstructive pulmonary disease (COPD) has been the third leading cause of death since 2020.1 Acute exacerbations of COPD (AECOPD) can lead to severe respiratory failure, often requiring mechanical ventilation for life support.2,3 The Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines recommend considering mechanical ventilation in patients with acute respiratory acidosis (pH < 7.35, PaCO2 > 45 mmHg), severe dyspnea with signs of increased work of breathing, or refractory hypoxemia despite oxygen therapy.4 Additionally, COPD progression may be exacerbated by coexisting chronic conditions such as heart failure or lung cancer, which not only share similar symptoms like dyspnea and increased ventilatory demand but also have been associated with significantly higher mortality rates in COPD patients.5,6 Conditions, including pneumonia, sepsis, and heart failure, often worsen respiratory failure in patients with COPD, often requiring intubation and mechanical ventilation.7–10 COPD exacerbation-related hospitalizations have an in-hospital mortality rate of approximately 6.2%.11 Poor prognosis is common in patients with COPD requiring mechanical ventilation in intensive care units (ICUs),12 with in-hospital mortality about 20–40%.14 The complex symptoms associated with COPD exacerbations, including insomnia, anxiety/depression, and respiratory distress, highlight the challenges in managing critically ill patients, emphasizing the need for targeted palliative care.15,16
Inpatient palliative care is recommended by professional societies for severely ill patients with COPD, alongside standard care, starting from the onset of symptoms or ICU admission and early in the treatment process.15,17 Palliative care, provided by an interdisciplinary team, focuses on managing symptoms, including breathlessness, anxiety, and depression, while respecting patient preferences and supporting families.18 Studies show that older age, cancer, and the severity of co-existing conditions significantly impact inpatient palliative care use and decisions regarding aggressive interventions.19,20 Moreover, palliative care is used less frequently for COPD symptom management compared to that for lung cancer.21 As in other countries, the use of opioids in palliative care could depend on whether patients with or without cancer condition, reflecting differences in clinical guidelines, ethical perspectives, and prescribing practices.22,23 Therefore, effective communication and the integration of palliative care are essential for comprehensive COPD management at all stages.15,24
Managing patients with severe respiratory illnesses during acute exacerbations can increase the need for prolonged mechanical ventilation and extend ICU stays.25 In acute settings, bundle care strategies are recommended to enhance care for mechanically ventilated patients. Daily sedation interruption can help reduce the incidence and duration of delirium, while early mobility interventions can decrease both hospital stay and ventilation duration.26 In Taiwan, the Integrated Prospective Payment program manages resources across ICUs, respiratory care centers, wards, and home-based ventilation programs. While the Integrated Prospective Payment program has prolonged hospital stays, increased mechanical ventilation duration, and raised costs, it has also improved survival rates for patients receiving prolonged mechanical ventilation.27,28 To reduce unnecessary interventions in severe chronic illness, Taiwan’s national health insurance program began reimbursing inpatient palliative care for non-cancer conditions, including COPD, in 2009 and launched a Pay-for-Performance program for COPD management in 2017. These initiatives focus on disease-specific treatment and patient-centered holistic care within a comprehensive healthcare system.29,30 In Taiwan, the 2013 Natural Death Act Amendment legally allows a multidisciplinary palliative care team to withdraw life-sustaining therapy, including mechanical ventilation, for terminally ill patients. The duration of mechanical ventilation and the timing of its withdrawal depended on disease progression, family discussions, and institutional protocols.31 However, limited studies exist on palliative care use among severely ill patients with COPD requiring mechanical ventilation. This study aimed to investigate factors influencing inpatient palliative care utilization among COPD patients requiring mechanical ventilation. We hypothesized that severely ill patients with COPD needing mechanical ventilation were more likely to utilize inpatient palliative care. Factors, such as older age, higher severity of comorbidities, presence of cancer, and hospital type were anticipated to affect the likelihood of palliative care utilization during hospitalization for patients with COPD.
Materials and Methods
Data Sources
We conducted a retrospective cross-sectional study of hospitalized patients with COPD exacerbation who received palliative care using linked health administrative data from the National Health Insurance Research Database (NHIRD) in Taiwan. The NHIRD is based on Taiwan’s National Health Insurance program, which covers almost 99% of the population. The database comprises detailed information regarding diagnostic codes, date of diagnosis, consultation payments, and prescription details. The diagnosis codes in NHIRD are based on the International Classification of Diseases, 10th Revision, and Clinical Modification (ICD-10-CM) for diagnoses and procedures.
This study was approved by the Institutional Review Board of Chi Mei Medical Centre (IRB: 11012-E01) and conducted in compliance with the ethical standards and guidelines of the 2013 revision of the Declaration of Helsinki. Informed consent was waived by the Institutional Review Board due to the use of secondary databases and the absence of personal information in the study.
Study Population
This nested case-control study included a cohort of hospitalized patients aged 40 years or older who were newly diagnosed with COPD between 2017 and 2021, identified using ICD-10-CM codes J41-J44. Among these patients, we selected those who had a recorded death date and excluded individuals whose first COPD diagnosis occurred more than 15 months before death to reduce duration bias. This cutoff was chosen based on the median time from COPD diagnosis to inpatient palliative care utilization in our dataset, ensuring a comparable timeframe to assess inpatient palliative care utilization patterns. Additionally, we excluded patients with incomplete hospitalization records and those who had received inpatient palliative care before January 1, 2017. Within this cohort, we defined cases as patients who received inpatient palliative care before death, and controls were patients who did not receive inpatient palliative care before death. We then retrospectively examined mechanical ventilation use and other factors associated with inpatient palliative care utilization. The selection of study subjects was illustrated in Figure 1.
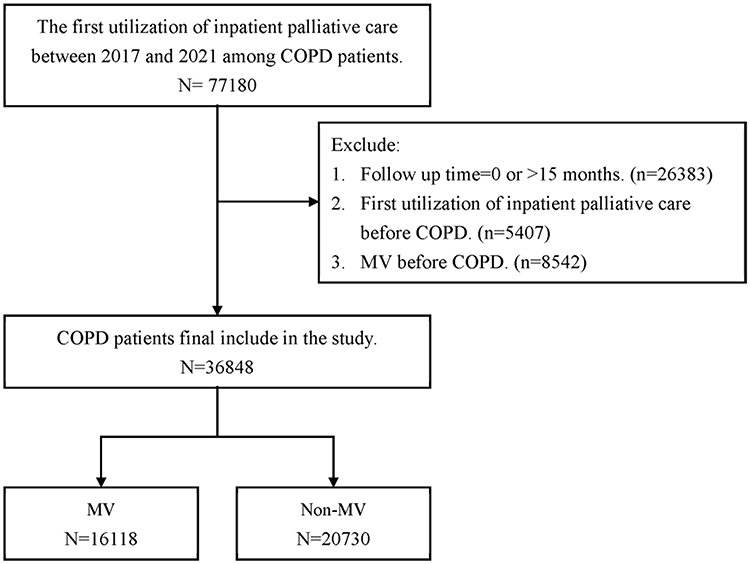 |
Figure 1 The flowchart of study subjects’ selection. |
Outcome and Measurements
According to the study aim, the exposure variable of this study was COPD patients with or without using mechanical ventilation during hospitalization. Mechanical ventilation use was identified using claim codes 57001 and 57023. The primary outcome was inpatient palliative care utilization, defined as study subjects receiving inpatient palliative care during hospitalization. The definition of inpatient palliative care was based on medical expenditure applications. Additionally, we investigated whether the duration of mechanical ventilation use influenced inpatient palliative care utilization. Mechanical ventilation duration was classified into <7 days, 8–30 days, and >30 days to estimate the association with inpatient palliative care utilization.
Critically ill patients with COPD were characterized by demographic factors, comorbidities, and healthcare services utilization. Demographic factors included sex and age. Age was classified into < 65, 65–74, 75–84, and >85 years. These age groups are commonly used in inpatient palliative care and COPD research to reflect differences in health status and care needs, as supported by prior studies.32–34 The Charlson Comorbidity Index (CCI) is a validated tool for assessing comorbidity burden and its impact on clinical outcomes. 35 In this study, we used CCI to quantify the severity of coexisting chronic conditions and adjust for their potential influence on inpatient palliative care utilization in COPD patients requiring mechanical ventilation. CCI has been used in prior research to assess hospital mortality and palliative care needs in critically ill COPD patients.32,36 The CCI scores were used to evaluate the severity of comorbidities, classified as 0, 1–2, and ≥3. Additionally, heart failure (ICD-10-CM: I50), ischemic heart disease (ICD-10-CM: I20-I25), atrial fibrillation (ICD-10-CM: I48), dementia (ICD-10-CM: F00-F03, F05.1, G30, G31.1), pneumonia (ICD-10-CM: J18.9), sepsis (ICD-10-CM: A40, A41, R57.2, R65.21), and cancer (ICD-10-CM: C00-C97) were considered. These concomitant diseases were recorded as dichotomous variables based on their presence or absence.
The utilization of healthcare services included hospital types, emergency room (ER) visits, length of stay in ICUs and hospitals, and mechanical ventilation implementation. Hospital types included medical centers, regional hospitals, and district hospitals. The frequency of ER visits was defined as 0, 1–3, and > 3 times per year, while the length of hospital stay was classified as 0, <30 days, 31–120 days, and >120 days per year, estimated retrospectively from patient death to the first instance of COPD diagnosis. ICU admission was recorded as a binary variable, which ‘yes’ for patients hospitalized in the ICU at least once within one year of COPD diagnosis and “no” for otherwise.
Statistical Analysis
Baseline information between COPD patients with and without mechanical ventilation was assessed using Student’s t-test for continuous variables and Pearson’s Chi-square test for categorical variables. Logistic regression was used to assess the association between mechanical ventilation and inpatient palliative care utilization, adjusting for relevant covariates. Crude and adjusted odds ratios with 95% confidence intervals are presented. Stratified analyses of each selected subgroups between mechanical ventilation and palliative care use were also conducted. Additionally, the association between mechanical ventilation duration and inpatient palliative care utilization among patients who received mechanical ventilation was estimated using multivariable logistic regression. Mechanical ventilation duration (<7 days, 8–30 days, >30 days) was treated as an exposure variable to estimate the association with inpatient palliative care utilization in both overall and subgroup analyses. The forest plot was used to visualize the associations between mechanical ventilation duration and inpatient palliative care utilization. All analyses were conducted using SAS statistical software version 9.4 (SAS Institute, Inc., Cary, NC, USA), with statistical significance set at a p-value < 0.05.
Results
Baseline Characteristics of COPD Patients
Table 1 presents the demographic characteristics of hospitalized patients with COPD. Out of 36,848 patients with COPD, 16,118 (43.74%) required mechanical ventilation during hospitalization. Those requiring mechanical ventilation had significantly more ER visits (4.74±11.00 vs 4.07±9.93, p < 0.0001) and longer hospital stays (68.43±80.40 vs 42.20±59.67, p < 0.0001) than those without mechanical ventilation. Over 50% of ventilated patients had one to three or more ER visits, with length of hospital stay ranging from 31 days to over 120 days. Among patients with COPD using mechanical ventilation, 40.85% visited the ER more than three times per year, 54.24% stayed in the hospital for over 30 days, and 45.55% received ICU care, all higher than those without mechanical ventilation. On average, mechanical ventilation was used 2.96±4.88 times and for 63.46±180.03 days per year among hospitalized patients with COPD. The duration from COPD diagnosis to death was 5.05±4.34 years for patients using mechanical ventilation and 4.72±4.27 years for those not using mechanical ventilation (p < 0.0001). Palliative care was provided to 15.19% of these patients, with a utilization rate of 7.91% for those requiring mechanical ventilation and 20.84% for those that did not require mechanical ventilation (p < 0.0001). The time from COPD diagnosis to palliative care utilization was 5.22 ± 4.07 years, with patients on mechanical ventilation averaging 5.87 ± 4.15 years and those without mechanical ventilation averaging 5.03 ± 4.03 years (p < 0.0001). Among hospitalized patients with COPD, 20.49% of those with mechanical ventilation and 14.56% of those without mechanical ventilation died from COPD (p < 0.0001).
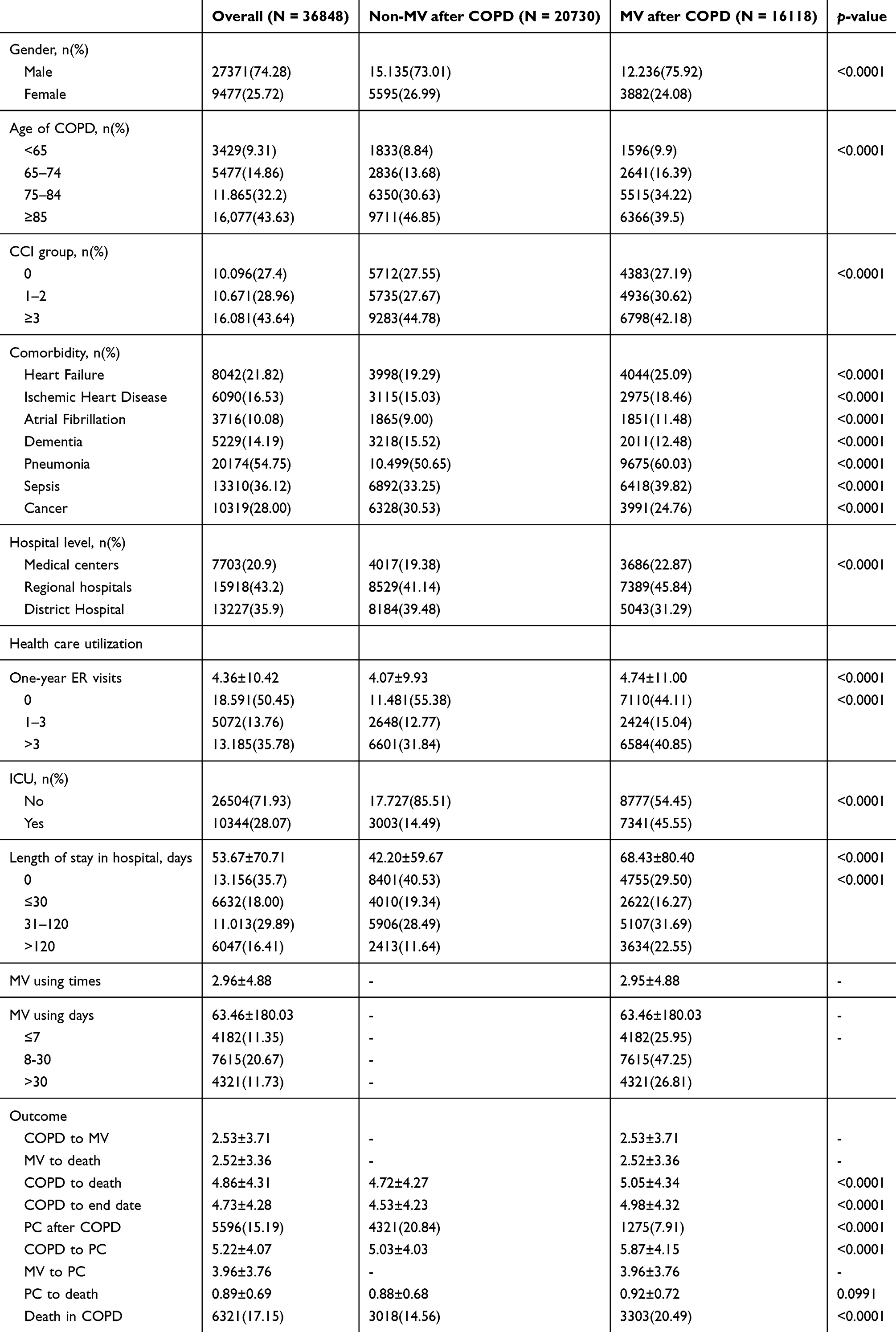 |
Table 1 The Demographic Characteristics of Hospitalized Patients With COPD |
Factors Associated With Inpatient Palliative Care Utilization
Table 2 shows the association between inpatient palliative care and various factors in hospitalized patients with COPD. Those requiring mechanical ventilation were significantly less likely to receive palliative care (adjusted odds ratio [AOR]: 0.40, 95% CI: 0.37–0.43, p < 0.0001). Age played a key role, patients aged 65–74 (AOR: 0.83, 95% CI: 0.73–0.94, p = 0.0025), 75–84 (AOR: 0.62, 95% CI: 0.56–0.70, p < 0.0001), and ≥85 (AOR: 0.58, 95% CI: 0.52–0.65, p < 0.0001) had progressively lower probabilities of receiving palliative care than patients <65 years. Comorbidity severity also influenced palliative care use, with higher CCI scores (≥3) significantly increasing the likelihood of palliative care utilization (AOR: 51.80, 95% CI: 43.49–61.69, p < 0.0001), especially for patients with cancer (AOR: 2.73, 95% CI: 2.53–2.95, p < 0.0001). Conversely, patients with dementia were less likely to receive palliative care (AOR: 0.74, 95% CI: 0.67–0.83, p < 0.0001). Hospital type significantly impacted care, with patients in medical centers (AOR: 4.89, 95% CI: 4.40–5.43, p < 0.0001) and regional hospitals (AOR: 3.07, 95% CI: 2.79–3.39, p < 0.0001) more likely to receive palliative care than those in district hospitals. Frequent ER visits (>3 times/year) slightly reduced the likelihood of palliative care use (AOR: 0.94, 95% CI: 0.86–1.02, p = 0.1093), although this was not statistically significant. Patients treated in the ICU had a decreased likelihood of receiving palliative care (AOR: 0.48, 95% CI: 0.43–0.53, p < 0.0001), and longer length of hospital stay were negatively associated with palliative care utilization. The subgroup analysis of association between mechanical ventilation use and inpatient palliative care in COPD patients illustrated as Supplementary Table 1.
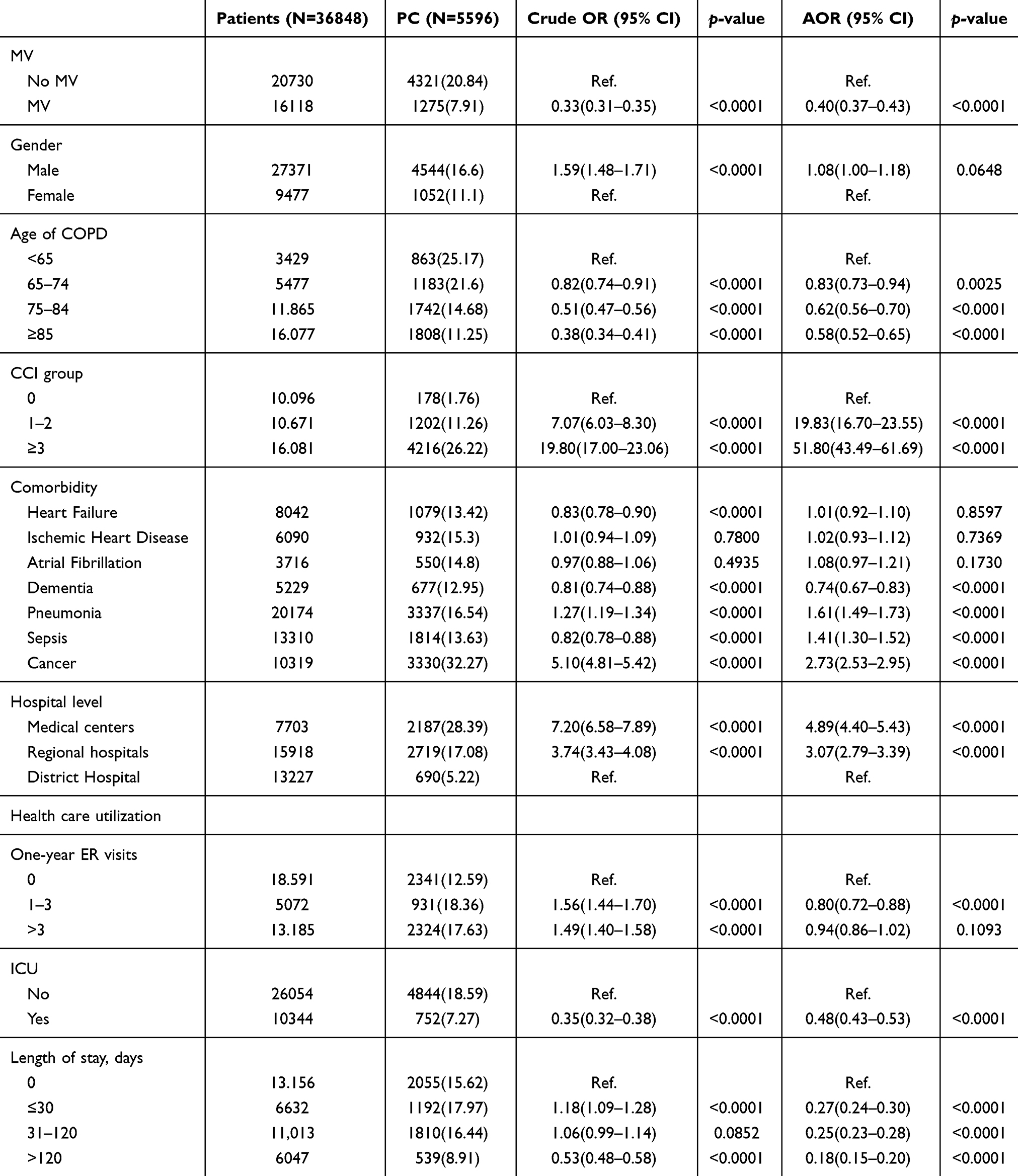 |
Table 2 The Association Between Inpatient Palliative Care and Various Factors in Hospitalized Patients With COPD |
Palliative Care Utilization in Ventilated COPD Patients by Mechanical Ventilation Duration
Table 3 presents the association between palliative care and related factors among patients with COPD receiving mechanical ventilation. Patients who had 8–30 days of mechanical ventilation (AOR: 2.20, 95% CI: 1.86–2.61, p < 0.0001) and those with more than 30 days (AOR: 2.13, 95% CI: 1.74–2.61, p < 0.0001) had a higher likelihood of receiving palliative care compared to those with mechanical ventilation days ≤7. Males were more likely to require inpatient palliative care than females. Patients aged 75–84 years and those 85 years and older were less likely to utilize palliative care compared to those <65 years. Patients with CCI scores of 1–2 (AOR: 24.06, 95% CI: 17.40–33.28, p < 0.0001) and scores ≥3 (AOR: 51.59, 95% CI: 36.97–72.00, p < 0.0001) were significantly more likely to utilize inpatient palliative care. Among comorbidities, pneumonia, sepsis, and cancer were significantly associated with higher inpatient palliative care utilization. Hospital level also influenced inpatient palliative care likelihood, with patients in medical centers (AOR: 4.92, 95% CI: 4.01–6.03, p < 0.0001) and regional hospitals (AOR: 2.52, 95% CI: 2.06–3.07, p < 0.0001) showing an increased likelihood of receiving inpatient palliative care. ICU admission negatively impacted inpatient palliative care utilization (AOR: 0.56, 95% CI: 0.48–0.65, p < 0.0001). Longer length of hospital stay was inversely related to inpatient palliative care utilization, with patients staying ≤30 days (AOR: 0.21, 95% CI: 0.17–0.26, p < 0.0001), 31–120 days (AOR: 0.19, 95% CI: 0.15–0.23, p < 0.0001), and more than 120 days (AOR: 0.15, 95% CI: 0.12–0.19, p < 0.0001) having significantly lower inpatient palliative care utilization than those without a hospital stay.
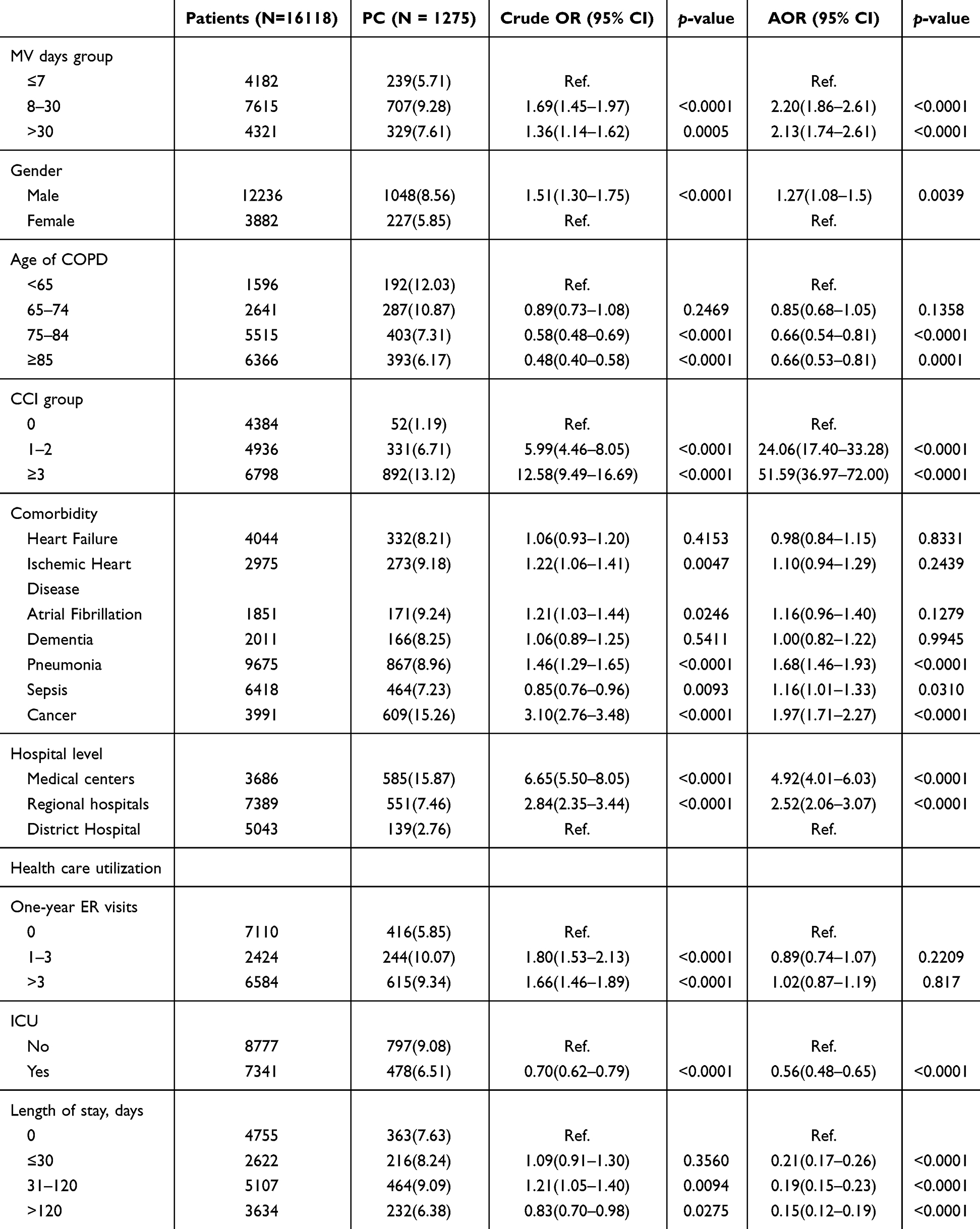 |
Table 3 The Association Between Palliative Care and Related Factors Among Patients With COPD Receiving Mechanical Ventilation |
Furthermore, the subgroups based on mechanical ventilation duration (<7 days, 8–30 days, >30 days) illustrated as Figure 2. Across all subgroups, the association between mechanical ventilation duration and increased palliative care utilization remained consistent. Especially, in regional hospitals, patients receiving 8–30 days (AOR: 3.25, 95% CI: 2.45–4.31, p < 0.0001) and >30 days (AOR: 3.26, 95% CI: 2.35–4.52, p < 0.0001) of mechanical ventilation had approximately a 3-folds increased likelihood of receiving inpatient palliative care compared to those ventilated for <7 days. Among patients with ICU records, those ventilated for 8–30 days (AOR: 3.02, 95% CI: 2.08–4.38, p < 0.0001) and >30 days (AOR: 2.87, 95% CI: 1.93–4.26, p < 0.0001) also demonstrated a significantly higher likelihood of receiving palliative care. For patients with a hospital stay of <30 days, those with 8–30 days of mechanical ventilation had a 3.48-fold increased likelihood of receiving inpatient palliative care, while those with >30 days had a 1.98-fold increased likelihood, compared to those ventilated for ≤7 days.
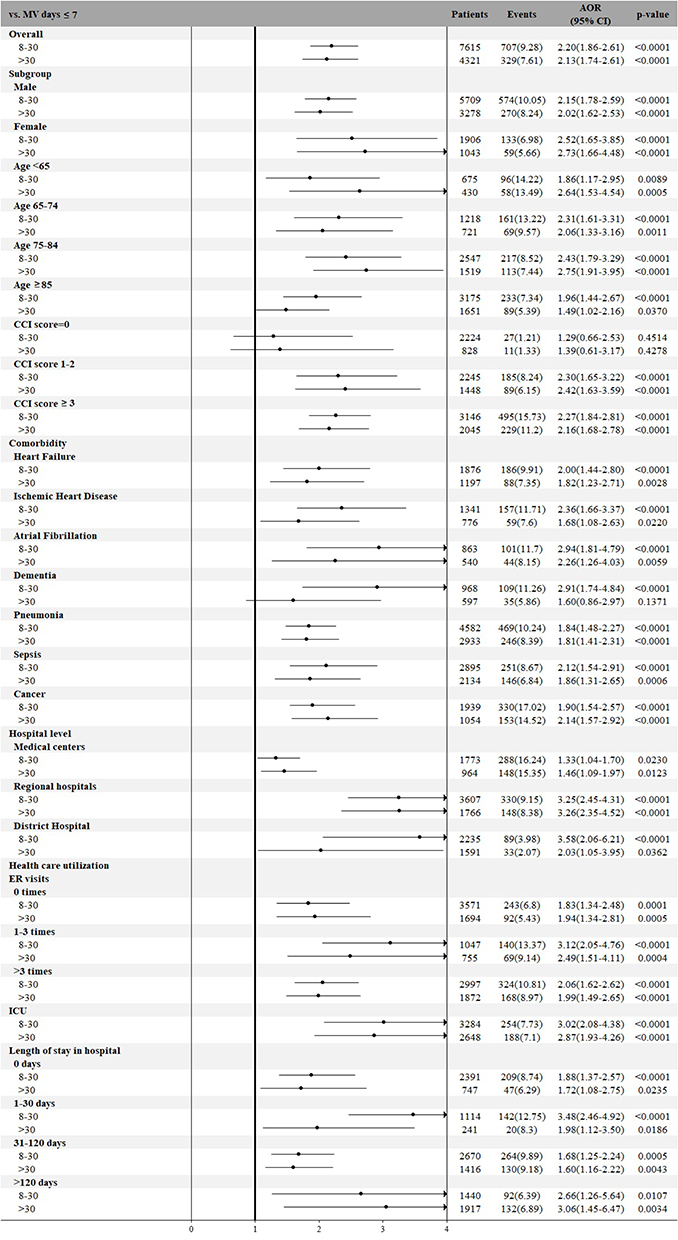 |
Figure 2 Association of mechanical ventilation duration with inpatient palliative care utilization in COPD patients receiving mechanical ventilation: overall and subgroup analysis. |
Discussion
Main Findings/results of the Study
Our study found that hospitalized patients with COPD were predominantly older male with severe comorbidities, admitted to medical centers or regional hospitals. Approximately 15.19% utilized inpatient palliative care, including 7.91% on mechanical ventilation. COPD-related mortality reached 20.49%. Patients on mechanical ventilation survived slightly longer after their COPD diagnosis. Factors, such as mechanical ventilation duration, comorbidity severity, and hospital level significantly influenced inpatient palliative care utilization. Our study found that patients with COPD requiring mechanical ventilation had more severe comorbidities, higher healthcare utilization, and more frequent admissions to high-level care.
What This Study Adds
Clinicians consider demographic factors as crucial when assessing palliative care needs.37 Previous study had indicated the significant factors of palliative care utilization included advanced age, prolonged non-invasive mechanical ventilation beyond 8 days, and therapy failure.38 Disease severity, malignancy, comorbidities, and mechanical ventilation use exceeding 72 hours were indicators of poor outcomes.39 Consistent with these findings, our results showed that patients with severe comorbidities (CCI >3) or cancer had a significantly higher likelihood of receiving palliative care. Compared to Japanese patients, Taiwanese patients repeatedly hospitalized for pneumonia had their timing of advance care planning discussions influenced by factors, including advanced age, stronger social support, and a tendency to decline life-sustaining treatment.40 These factors, along with hospital stay duration, prompted physicians to discuss end-of-life preferences with patients and caregivers.13 However, patients in our study typically received palliative care late, near death, indicating it was often viewed as end-of-life care, similar to hospice care for patients with cancer.
In acute care settings, intubation and mechanical ventilation are urgent interventions for critically ill patients. Non-invasive mechanical ventilation is often used as a preliminary trial before intubation or to facilitate weaning from invasive mechanical ventilation.41–43 It has been shown to enhance survival rates and reduce intubation requirements for patients with COPD during acute exacerbations while addressing palliative needs.41–44 Delays in initiating palliative care for these patients are often due to the unpredictable progression of chronic diseases.45 Therefore, integrating COPD diagnosis, mechanical ventilation use, and inpatient palliative care into routine practices may help avoid aggressive or unwanted medical interventions that prolong suffering for severely ill patients.
The utilization of mechanical ventilation and healthcare resources significantly influenced palliative care use in ventilated patients with COPD. Our results indicated those requiring mechanical ventilation for over 8 days, with higher comorbidity severity, infections, or cancer, and treated in medical centers or regional hospitals were more likely to receive inpatient palliative care. Increased ICU stays and longer hospitalizations were linked to higher palliative care utilization. The extensive healthcare resources used for severely ill patients with COPD needing prolonged mechanical ventilation may prompt the initiation of palliative care during hospitalization, possibly driven by the Integrated Prospective Payment program. Previous studies indicate that factors, such as age, hospital type, frequency of hospitalizations, and length of stay, may independently reflect mortality risk in patients with COPD.13,46 Older age and multiple comorbidities can increase disease severity and the chances of prolonged mechanical ventilation, while decreasing the likelihood of successful weaning.47,48 Therefore, palliative care utilization for patients needing mechanical ventilation for over 30 days should prioritize those with stable conditions, low chances of successful weaning, and risks of ventilator-associated complications, including pneumonia and pneumothorax.49,50 Our study indicated that patients with prolonged mechanical ventilation (8–30 days: AOR: 2.20, 95% CI: 1.86–2.61; >30 days: AOR: 2.13, 95% CI: 1.74–2.61) and multiple chronic conditions (CCI≥3: AOR: 51.59, 95% CI: 36.97–72.00) were more likely to receive inpatient palliative care. As patients experienced prolonged mechanical ventilation and had multiple chronic conditions, physicians were more likely to incorporate inpatient palliative care into their time-limited treatment plans during hospitalization.
Our results showed significant differences in inpatient palliative care utilization and the time from COPD diagnosis to death between patients with and without mechanical ventilation. The absence of a continuous care plan likely affected inpatient palliative care utilization for ventilated COPD patients, varying across healthcare facilities, as seen in previous studies.37,51 Successful management of advanced COPD relies on primary care physicians’ ability to recognize breathlessness and assess patients’ reported respiratory difficulties, ensuring timely administration of palliative care.52,53 Awareness of advanced COPD conditions and physicians’ comfort with the uncertain prognosis related to mechanical ventilation use significantly influenced discussions about intubation, mechanical ventilation, and end-of-life decisions.54,55 In acute settings, physicians often regard inpatient palliative care as essential for critically ill patients, addressing symptom distress and facilitating timely discussions with patients, families, or surrogates about prognosis, care quality, and patient preferences. This collaborative approach is particularly important for patients on prolonged mechanical ventilation, highlighting the need for interdisciplinary teamwork.17,56
Inpatient palliative care utilization for patients with COPD on mechanical ventilation may be uncommon in ICU settings. Factors, including metastatic cancer, unrealistic care goals, end-of-life decisions, and persistent organ failure, were considered more appropriate reasons for requesting palliative care consultations than age, ICU stay length, or life support duration.57 Our study found that alongside comorbidity severity, mechanical ventilation duration, and hospital type significantly influenced inpatient palliative care utilization in patients with COPD. Especially, patients in medical centers (AOR: 4.92, 95% CI: 4.01–6.03) and regional hospitals (AOR: 2.52, 95% CI: 2.06–3.07) were more likely to receive palliative care than those in district hospitals. Understanding COPD prognosis, including age, comorbidities, clinical presentation, and length of stay, can help healthcare professionals predict outcomes, develop timely care plans, and ensure consistent care.17,58–60 A study found that patients with COPD who were educated on physician-led palliative and hospice care were more likely to use these services, although utilization declined among those with pneumonia.61 Patients with pulmonary and critical illnesses, along with their families, faced various needs, including managing severe symptoms, improving quality of life, facilitating clear communication about care goals, making treatment decisions, and accessing emotional, social, and spiritual support. Addressing these needs underscores the importance of integrating palliative care into their holistic treatment approach.62
Strength and Weakness/Limitations of the Study
Our study’s strength lies in the large, diverse sample from hospitals across Taiwan, enhancing generalizability. Our comprehensive data allows for the analysis of demographic differences and inpatient palliative care utilization, outcomes, and related factors. However, some limitations should be mentioned. NHIRD lacks data on occupation, marital status, vital signs, laboratory results, pulmonary function tests, and APACHE II scores, which are vital for assessing COPD severity and factors affecting palliative care utilization. Additionally, although previous studies have demonstrated a strong association between smoking history and COPD severity, as well as mechanical ventilation use,63 smoking status and intensity were not available in our dataset. Moreover, key weaning parameters, such as the rapid shallow breathing index, were not included, limiting insights into weaning difficulties for these patients on mechanical ventilation. Similarly, our dataset lacked clinical details on mechanical ventilation withdrawal, making it unclear whether mechanical ventilation was actively withdrawn as part of end-of-life care or discontinued due to clinical deterioration. This limitation may impact the association between mechanical ventilation duration and palliative care utilization. Furthermore, the absence of data on palliative medication use, such as opioids, limits our ability to assess how symptom management strategies influenced the timing of inpatient palliative care initiation. Additionally, we could not determine post-MV withdrawal care decisions, such as whether patients transitioned directly to palliative care or received other supportive interventions. Future research should include detail clinical records to explore the impact of mechanical ventilation withdrawal on palliative care utilization.
Another important limitation was the lack of data on family meetings and shared decision-making, so we could not fully recognize patient care goals and preferences, potentially impacting the analysis of physician-patient communication. These challenges may be further compounded by barriers to optimal COPD care, such as caregivers’ emotional burden, limited access to palliative care resources, and difficulties navigating complex healthcare systems.64 Therefore, improving care quality should combine interdisciplinary care models, increase communication strategies, and establish caregiver support programs. Additionally, our study population could not be generalizable to the broader COPD population, as we focused on hospitalized patients with newly diagnosed COPD. Specifically, our study excluded patients with longstanding COPD (diagnosed more than 15 months before death). While this approach may reduce the duration bias and ensure a more comparable study population, it may limit the applicability of our findings to patients with long-term COPD, who may have different disease process and palliative care utilization patterns. Moreover, differences in healthcare systems and palliative care resource availability may also limit the generalizability of our findings to other countries because variations in healthcare policies, reimbursement models, and the availability of specialized palliative care services could affect inpatient palliative care utilization patterns. Finally, our study period (2017–2021) overlapped with the COVID-19 pandemic. However, Taiwan’s major COVID-19 outbreaks did not occur until April 2022, when daily cases exceeded 500.65 Since our study ended in 2021, the impact of the pandemic on mechanical ventilation use and palliative care utilization was likely minimal.
Conclusion
Critically ill patients with COPD requiring mechanical ventilation were less likely to receive inpatient palliative care compared to non-ventilated patients. Factors, including prolonged ventilation, comorbidity severity, and hospital type, influenced palliative care utilization. This study highlights under-recognized barriers to palliative care in this population, emphasizing the need for interdisciplinary, patient-centered approaches. However, the lack of detailed clinical parameters, including the frequency and duration of palliative care services, limits the interpretation of these findings. Future research should focus on interventions to improve palliative care integration and examine the extent of palliative care utilization among ventilated COPD patients.
Data Management and Sharing
The data sources are the Taiwan Nation Health Insurance Database and Taiwan Cancer Registry. The data are available with permission from the Taiwan Health and Welfare Data Science Center (https://dep.mohw.gov.tw/DOS/cp-5119-59201-113.html, accessed on September 30, 2024). Re-strictions apply to the availability of these data, which were used under license for this study.
Acknowledgments
We are grateful to the Health Data Science Center, National Cheng Kung University Hospital for providing administrative and technical support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was supported from the Chi-Mei Medical Center (CMFHR112035). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors declare no conflict of interest.
References
1. Chen S, Kuhn M, Prettner K, et al. The global economic burden of chronic obstructive pulmonary disease for 204 countries and territories in 2020–50: a health-augmented macroeconomic modelling study. Lancet Glob Health. 2023;11(8):e1183–e1193. doi:10.1016/S2214-109X(23)00217-6
2. MacIntyre N, Huang YC. Acute exacerbations and respiratory failure in chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2008;5(4):530–535. doi:10.1513/pats.200707-088ET
3. Baqdunes MW, Leap J, Young M, Kaura A, Cheema T. Acute exacerbation of chronic obstructive pulmonary disease. Crit Care Nurs Q. 2021;44(1):74–90. doi:10.1097/CNQ.0000000000000341
4. Agusti A, Böhm M, Celli B, et al. GOLD COPD DOCUMENT 2023: a brief update for practicing cardiologists. Clin Res Cardiol. 2024;113(2):195–204. doi:10.1007/s00392-023-02217-0
5. Schwab P, Dhamane AD, Hopson SD, et al. Impact of comorbid conditions in COPD patients on health care resource utilization and costs in a predominantly medicare population. Int J Chronic Obstr. 2017:735–744.
6. Agustí A, Anzueto A, Celli BR, Mortimer K, Salvi S, Vogelmeier CF. GOLD 2023 executive summary: responses from the GOLD scientific committee. Europ resp J. 2023;61(6):2300616. doi:10.1183/13993003.00616-2023
7. Nguyen PL, Uddin MM, Mir T, et al. Trends in incidence, and mortality of acute exacerbation of chronic obstructive pulmonary disease in the United States emergency department (2010–2018). COPD. 2021;18(5):567–575. doi:10.1080/15412555.2021.1979500
8. Whittaker H, Rubino A, Müllerová H, et al. Frequency and severity of exacerbations of COPD associated with future risk of exacerbations and mortality: a UK routine health care data study. Int J Chronic Obstr. 2022:427–437.
9. Alzaabi O, Guerot E, Planquette B, Diehl J-L, Soumagne T. Predicting outcomes in patients with exacerbation of COPD requiring mechanical ventilation. Ann Intens Care. 2024;14(1):159. doi:10.1186/s13613-024-01394-z
10. Pirera E, Di Raimondo D, D’Anna L, Tuttolomondo A. Risk trajectory of cardiovascular events after an exacerbation of chronic obstructive pulmonary disease: a systematic review and meta-analysis. Eur J Internal Med. 2025. doi:10.1016/j.ejim.2025.01.016
11. Waeijen-Smit K, Crutsen M, Keene S, et al. Global mortality and readmission rates following COPD exacerbation-related hospitalisation: a meta-analysis of 65 945 individual patients. ERJ Open Res. 2024;10(1):00838–2023. doi:10.1183/23120541.00838-2023
12. Ai-Ping C, Lee K-H, Lim T-K. In-hospital and 5-year mortality of patients treated in the ICU for acute exacerbation of COPD: a retrospective study. Chest. 2005;128(2):518–524. doi:10.1378/chest.128.2.518
13. Batzlaff CM, Karpman C, Afessa B, Benzo RP. Predicting 1-year mortality rate for patients admitted with an acute exacerbation of chronic obstructive pulmonary disease to an intensive care unit: an opportunity for palliative care. Mayo Clin Proc. 2014;89:638–643. doi:10.1016/j.mayocp.2013.12.004
14. Prediletto I, Giancotti G, Nava S. COPD exacerbation: why it is important to avoid ICU admission. J Clin Med. 2023;12(10):3369. doi:10.3390/jcm12103369
15. Lanken PN, Terry PB, DeLisser HM, et al. An official American thoracic society clinical policy statement: palliative care for patients with respiratory diseases and critical illnesses. Am J Respir Crit Care Med. 2008;177(8):912–927. doi:10.1164/rccm.200605-587ST
16. Maddocks M, Lovell N, Booth S, Man WD, Higginson IJ. Palliative care and management of troublesome symptoms for people with chronic obstructive pulmonary disease. Lancet. 2017;390(10098):988–1002. doi:10.1016/S0140-6736(17)32127-X
17. Sullivan DR, Iyer AS, Enguidanos S, et al. Palliative care early in the care continuum among patients with serious respiratory illness: an official ATS/AAHPM/HPNA/SWHPN policy statement. Am J Respir Crit Care Med. 2022;206(6):e44–e69. doi:10.1164/rccm.202207-1262ST
18. Campion EW, Kelley AS, Morrison RS, Campion EW. Palliative care for the seriously ill. N Engl J Med. 2015;373(8):747–755. doi:10.1056/NEJMra1404684
19. Kuo L-C, Chen J-H, Lee C-H, Tsai C-W, Lin -C-C. End-of-life health care utilization between chronic obstructive pulmonary disease and lung cancer patients. J Pain Sympt Manage. 2019;57(5):933–943. doi:10.1016/j.jpainsymman.2019.01.011
20. Faes K, Cohen J, Annemans L. Resource use during the last six months of life among COPD patients: a population-level study. J Pain Sympt Manage. 2018;56(3):318–326.e317. doi:10.1016/j.jpainsymman.2018.06.002
21. Wysham NG, Cox CE, Wolf SP, Kamal AH. Symptom burden of chronic lung disease compared with lung cancer at time of referral for palliative care consultation. Ann Am Thoracic Soc. 2015;12(9):1294–1301. doi:10.1513/AnnalsATS.201503-180OC
22. Kang K-H, Kuo L-F, Cheng I-C, Chang C-S, Tsay W-I. Trends in major opioid analgesic consumption in Taiwan, 2002–2014. JFormos Med Assoc. 2017;116(7):529–535. doi:10.1016/j.jfma.2016.09.004
23. Peralta T, Castel-Branco MM, Reis-Pina P, Figueiredo D IV, Dourado M. Prescription trends at the end of life in a palliative care unit: observational study. BMC Palliat Care. 2022;21(1):65. doi:10.1186/s12904-022-00954-z
24. Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. Am J Respir Crit Care Med. 2017;195(5):557–582. doi:10.1164/rccm.201701-0218PP
25. MacIntyre NR, Epstein SK, Carson S, Scheinhorn D, Christopher K, Muldoon S. Management of patients requiring prolonged mechanical ventilation: report of a NAMDRC consensus conference. Chest. 2005;128(6):3937–3954. doi:10.1378/chest.128.6.3937
26. Chen CM, Cheng AC, Chou W, Selvam P, Cheng CM. Outcome of improved care bundle in acute respiratory failure patients. In: In. Vol 26. Wiley Online Library; 2021:380–385.
27. Liu C-J, Kung P-T, Chu -C-C, Chou W-Y, Wang Y-H, Tsai W-C. Propensity score-matching analyses on the effectiveness of integrated prospective payment program for patients with prolonged mechanical ventilation. Health Policy. 2018;122(9):970–976. doi:10.1016/j.healthpol.2018.07.009
28. Liu C-J, Chu -C-C, Chen W, et al. Impact of Taiwan’s integrated prospective payment program on prolonged mechanical ventilation: a 6-year nationwide study. Respiratory Care. 2013;58(4):676–682. doi:10.4187/respcare.01242
29. Hung Y-S, Chen C-H, Yeh K-Y, et al. Potential benefits of palliative care for polysymptomatic patients with late-stage nonmalignant disease in Taiwan. JFormos Med Assoc. 2013;112(7):406–415. doi:10.1016/j.jfma.2011.08.021
30. Cheng S-L, Li Y-R, Huang N, et al. Effectiveness of Nationwide COPD pay-for-performance program on COPD exacerbations in Taiwan. Int J Chronic Obstr;2021. 2869–2881. doi:10.2147/COPD.S329454
31. Hung Y-S, Lee S-H, Hung C-Y, et al. Clinical characteristics and survival outcomes of terminally ill patients undergoing withdrawal of mechanical ventilation. JFormos Med Assoc. 2018;117(9):798–805. doi:10.1016/j.jfma.2017.09.014
32. Kao L-T, Ko S-C, Chen P-J, et al. Trend analysis of palliative care utilization in patients with chronic obstructive pulmonary disease during hospitalization from 2007 to 2018 in Taiwan. Int J Chronic Obstr. 2023;Volume 18:3015–3026. doi:10.2147/COPD.S435954
33. Amegadzie JE, Lee TY, Sadatsafavi M, Lynd LD, Sin DD, Johnson KM. Trends in hospital admissions for chronic obstructive pulmonary disease over 16 years in Canada. CMAJ. 2023;195(35):E1172–E1179. doi:10.1503/cmaj.221051
34. Hsu C-H, Hung YM, Chu K-A, Chen C-F, Yin C-H, Lee -C-C. Prognostic nomogram for elderly patients with acute respiratory failure receiving invasive mechanical ventilation: a nationwide population-based cohort study in Taiwan. Sci Rep. 2020;10(1):13161. doi:10.1038/s41598-020-70130-x
35. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
36. Quach S, Hennessy DA, Faris P, Fong A, Quan H, Doig C. A comparison between the APACHE II and Charlson Index Score for predicting hospital mortality in critically ill patients. BMC Health Serv Res. 2009;9:1–8. doi:10.1186/1472-6963-9-129
37. Chatterjee K, Goyal A, Kakkera K, Harrington S, Corwin HL. National trends (2009–2013) for palliative care utilization for patients receiving prolonged mechanical ventilation. Crit Care Med. 2018;46(8):1230–1237. doi:10.1097/CCM.0000000000003182
38. Sprooten RT, Rohde GG, Janssen MT, Cobben NA, Wouters EF, Franssen FM. Predictors for long‐term mortality in COPD patients requiring non‐invasive positive pressure ventilation for the treatment of acute respiratory failure. Clin Respir J. 2020;14(12):1144–1152. doi:10.1111/crj.13251
39. Nevins ML, Epstein SK. Predictors of outcome for patients with COPD requiring invasive mechanical ventilation. Chest. 2001;119(6):1840–1849. doi:10.1378/chest.119.6.1840
40. Miyashita J, Kohno A, Cheng S-Y, et al. Patients’ preferences and factors influencing initial advance care planning discussions’ timing: a cross-cultural mixed-methods study. Palliative Medicine. 2020;34(7):906–916. doi:10.1177/0269216320914791
41. Burns KE, Meade MO, Premji A, Adhikari NK. Noninvasive positive‐pressure ventilation as a weaning strategy for intubated adults with respiratory failure. Cochrane Database Syst Rev. 2013;2013(12). doi:10.1002/14651858.CD004127.pub3
42. Osadnik CR, Tee VS, Carson‐Chahhoud KV, Picot J, Wedzicha JA, Smith BJ. Non‐invasive ventilation for the management of acute hypercapnic respiratory failure due to exacerbation of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2017(7).
43. Rochwerg B, Brochard L, Elliott MW, et al. Official ERS/ATS clinical practice guidelines: noninvasive ventilation for acute respiratory failure. Eur Respir J. 2017;50(2):1602426. doi:10.1183/13993003.02426-2016
44. Wedzicha JA, Miravitlles M, Hurst JR, et al. Management of COPD exacerbations: a European respiratory society/American thoracic society guideline. Eur Respir J. 2017;49(3):1600791. doi:10.1183/13993003.00791-2016
45. Gill TM, Gahbauer EA, Han L, Allore HG. Trajectories of disability in the last year of life. N Engl J Med. 2010;362(13):1173–1180. doi:10.1056/NEJMoa0909087
46. Müllerova H, Maselli DJ, Locantore N, et al. Hospitalized exacerbations of COPD: risk factors and outcomes in the ECLIPSE cohort. Chest. 2015;147(4):999–1007. doi:10.1378/chest.14-0655
47. Su J, Lin C-Y, Chen S-K, Peng M-J, Wu C-L. Characteristics and outcome for very elderly patients (≥ 80 years) admitted to a respiratory care center in Taiwan. Int J Gerontol. 2012;6(4):262–266. doi:10.1016/j.ijge.2012.01.030
48. Dermot Frengley J, Sansone GR, Shakya K, Kaner RJ. Prolonged mechanical ventilation in 540 seriously ill older adults: effects of increasing age on clinical outcomes and survival. J Am Geriatr Soc. 2014;62(1):1–9. doi:10.1111/jgs.12597
49. Ruan S-Y, Teng N-C, Huang C-T, et al. Dynamic changes in prognosis with elapsed time on ventilators among mechanically ventilated patients. Ann Am Thoracic Soc. 2020;17(6):729–735. doi:10.1513/AnnalsATS.201908-646OC
50. Slutsky AS, Ranieri VM. Ventilator-induced lung injury. N Engl J Med. 2013;369(22):2126–2136. doi:10.1056/NEJMra1208707
51. Rush B, hertz P, Bond A, McDermid RC, Celi LA. Use of palliative care in patients with end-stage COPD and receiving home oxygen: national trends and barriers to care in the United States. Chest. 2017;151(1):41–46. doi:10.1016/j.chest.2016.06.023
52. Parshall MB, Schwartzstein RM, Adams L, et al. An official American Thoracic Society statement: update on the mechanisms, assessment, and management of dyspnea. Am J Respir Crit Care Med. 2012;185(4):435–452. doi:10.1164/rccm.201111-2042ST
53. Bausewein C, Booth S, Gysels M, Kühnbach R, Haberland B, Higginson IJ. Understanding breathlessness: cross-sectional comparison of symptom burden and palliative care needs in chronic obstructive pulmonary disease and cancer. J Palliat Med. 2010;13(9):1109–1118. doi:10.1089/jpm.2010.0068
54. Sullivan KE, Hébert PC, Logan J, Am O, McNeely PD. What do physicians tell patients with end-stage COPD about intubation and mechanical ventilation? Chest. 1996;109(1):258–264. doi:10.1378/chest.109.1.258
55. Schmidt M, Demoule A, Deslandes-Boutmy E, et al. Intensive care unit admission in chronic obstructive pulmonary disease: patient information and the physician’s decision-making process. Critical Care. 2014;18:1–9. doi:10.1186/cc13906
56. Aslakson RA, Curtis JR, Nelson JE. The changing role of palliative care in the ICU. Crit Care Med. 2014;42(11):2418–2428. doi:10.1097/CCM.0000000000000573
57. Wysham NG, Hua M, Hough CL, et al. Improving ICU-based palliative care delivery: a multicenter, multidisciplinary survey of critical care clinician attitudes and beliefs. Crit Care Med. 2017;45(4):e372–e378. doi:10.1097/CCM.0000000000002099
58. Singanayagam A, Schembri S, Chalmers JD. Predictors of mortality in hospitalized adults with acute exacerbation of chronic obstructive pulmonary disease. A systematic review and meta-analysis. Ann Am Thoracic Soc. 2013;10(2):81–89. doi:10.1513/AnnalsATS.201208-043OC
59. Ho T-W, Tsai Y-J, Ruan S-Y, et al. In-hospital and one-year mortality and their predictors in patients hospitalized for first-ever chronic obstructive pulmonary disease exacerbations: a nationwide population-based study. PLoS One. 2014;9(12):e114866. doi:10.1371/journal.pone.0114866
60. Connors AF Jr, Dawson NV, Thomas C, et al. Outcomes following acute exacerbation of severe chronic obstructive lung disease. The SUPPORT investigators (study to understand prognoses and preferences for outcomes and risks of treatments). Am J Respir Crit Care Med. 1996;154(4):959–967. doi:10.1164/ajrccm.154.4.8887592
61. Chuang M-H, Lee F-N, Shiau Y-T, et al. Physician palliative education associated with high use of hospice care service. Am J Hospice Palliat Med®. 2022;39(2):237–242. doi:10.1177/10499091211014160
62. Aslakson RA, Reinke LF, Cox C, Kross EK, Benzo RP, Curtis JR. Developing a research agenda for integrating palliative care into critical care and pulmonary practice to improve patient and family outcomes. J Palliat Med. 2017;20(4):329–343. doi:10.1089/jpm.2016.0567
63. Li X, Wu Z, Xue M, Du W. Smoking status affects clinical characteristics and disease course of acute exacerbation of chronic obstructive pulmonary disease: a prospectively observational study. Chron Respir Dis. 2020;17:1479973120916184. doi:10.1177/1479973120916184
64. Siu DCH, Gafni-Lachter L. Addressing barriers to chronic obstructive pulmonary disease (COPD) care: three innovative evidence-based approaches: a review. Int J Chronic Obstr. 2024;Volume 19:331–341. doi:10.2147/COPD.S426050
65. Chen Y-H, Cheuh Y-N, Chen C-M, Kuo H-W. Epidemiological characteristics of the three waves of COVID-19 epidemic in Taiwan during April 2022 to March 2023. JFormos Med Assoc. 2023;122(11):1174–1182. doi:10.1016/j.jfma.2023.05.027
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Six-Minute Walking Test and 30 Seconds Chair-Stand-Test as Predictors of Mortality in COPD – A Cohort Study
Höglund J, Boström C, Sundh J
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2461-2469
Published Date: 4 October 2022
Hospital Burden of Chronic Obstructive Pulmonary Disease in Hong Kong – The Trend from 2006 to 2014
Chan HS, Ko FWS, Chan JWM, Choo KL, So LKY, Lam DCL, Sin KM, Wong WY, Cheng YL, Wong MML
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:507-519
Published Date: 6 April 2023
Prognostic Properties of the GOLD 2023 Classification System
Brat K, Svoboda M, Zatloukal J, Plutinsky M, Volakova E, Popelkova P, Novotna B, Dvorak T, Koblizek V
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:661-667
Published Date: 20 April 2023
RETRO-POPE: A Retrospective, Multicenter, Real-World Study of All-Cause Mortality in COPD
Koblizek V, Milenkovic B, Svoboda M, Kocianova J, Holub S, Zindr V, Ilic M, Jankovic J, Cupurdija V, Jarkovsky J, Popov B, Valipour A
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2661-2672
Published Date: 17 November 2023
Respiratory Infection Triggering Severe Acute Exacerbations of Chronic Obstructive Pulmonary Disease
Abi Abdallah G, Diop S, Jamme M, Legriel S, Ferré A
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:555-565
Published Date: 27 February 2024