Back to Journals » Journal of Pain Research » Volume 18
Factors in Surgical Placement and System Design to Reduce Pocket Awareness and Optimize the User Experience of Spinal Cord Stimulators – A Comprehensive Review
Authors Gish B ![]() , Al-Asadi Z, Tisler AT, Mata R
, Al-Asadi Z, Tisler AT, Mata R ![]() , Chopra H, Garcia RA, Schatman ME
, Chopra H, Garcia RA, Schatman ME ![]() , Tieppo Francio V
, Tieppo Francio V ![]() , AlFarra T
, AlFarra T ![]() , Bracero L, Karcz M
, Bracero L, Karcz M ![]() , Robinson CL
, Robinson CL ![]() , Shah A
, Shah A ![]() , Moreira A
, Moreira A ![]() , Sciascia AD, Deer T
, Sciascia AD, Deer T
Received 11 July 2025
Accepted for publication 15 November 2025
Published 14 December 2025 Volume 2025:18 Pages 6749—6768
DOI https://doi.org/10.2147/JPR.S551513
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Dawood Sayed
Brandon Gish,1 Zayd Al-Asadi,2 Abigail T Tisler,2 Robin Mata,3 Harman Chopra,4 Rosa Amelia Garcia,5 Michael E Schatman,6 Vinicius Tieppo Francio,7 Tariq AlFarra,8 Lucas Bracero,9 Marcin Karcz,9 Christopher L Robinson,10 Anuj Shah,9 Alexandra Moreira,11 Aaron D Sciascia,12 Timothy Deer9
1Interventional Pain Management Department, Lexington Clinic, Lexington, KY, USA; 2West Virginia School of Medicine, Morgantown, WV, USA; 3Department of Physical Medicine and Rehabilitation, University of Miami, Miami, FL, USA; 4Physical Medicine & Rehabilitation, Johns Hopkins University, Baltimore, MD, USA; 5Larkin Hospital Health Systems, Miami, FL, USA; 6Department of Anesthesiology, Perioperative Care and Pain Medicine Department of Population Health, Division of Medical Ethics, NYU Grossman School of Medicine, New York, NY, USA; 7Division of Pain Medicine, Department of Anesthesiology, Washington University School of Medicine, St. Louis, MO, USA; 8Mount Sinai Icahn School of Medicine, New York, NY, USA; 9The Spine and Nerve Center of the Virginias, Charleston, WV, USA; 10Department of Anesthesiology, Perioperative, and Pain Medicine, Brigham and Women’s Hospital, Boston, MA, USA; 11Pain Medicine Department, Rush University, Chicago, IL, USA; 12Institute for Clinical Outcomes and Research, Lexington Clinic, Lexington, KY, USA
Correspondence: Brandon Gish, Interventional Pain Management Department, Lexington Clinic, 1207 South Broadway, Lexington, KY, 40504, USA, Tel +1 859-258-6101, Email [email protected]
Abstract: Advancements in spinal cord stimulation (SCS) have enhanced patient outcomes, improved durability, and broadened the range of treatable pain conditions. Technological improvements in battery design have led to smaller implant size, while evolving societal guidelines have played a critical role in optimizing implant safety and quality. This review summarizes recent technological developments in SCS, the impact of such developments on patient satisfaction, and provides an overview of the major systems currently available. We also introduce and explore the emerging concept, “pocket awareness” – referring to a patient’s conscious perception of their implant. Several modifiable factors involving physicians, patients, and manufacturers can influence this awareness, and by extension, patient satisfaction. While pain relief is certainly the primary objective, fostering a comfortable and positive relationship between the patient and their device is essential and merits further clinical attention.
Plain Language Summary: Spinal Cord Stimulation (SCS) is a well-established therapy for chronic pain and has evolved significantly since its inception in the 1960s. Advancements in waveform delivery and battery technology have been significant, yet challenges still exist. One remaining gap in care is device and pocket awareness. The design goal of many devices we use regularly is to be seamless and natural without awareness of their existence. Such device integration becomes part of us. While much attention has been given to waveform optimization and energy delivery, sometimes the patient experience is neglected – ease of recharge, intuitive applications, and battery comfort. The success of SCS not only hinges on its ability to alleviate pain but also on optimizing the patient’s interaction with the device. Factors influencing pocket awareness include device features, surgical techniques, anatomical variations, and patient demographics. This review examines such variables, highlighting how pulse generator size, shape, and placement, along with the patient specific factors can influence outcomes. Recent innovations in battery technology and remote monitoring have advanced the cause, offering more convenience and improved programming; however, further addressing pocket awareness remains a critical area for improvement that involves device manufacturers, physicians, representatives, and patient support teams.
Keywords: spinal cord stimulation, implantable device, pain, spine, patient satisfaction
Introduction
Spinal cord stimulation (SCS) is a treatment that involves modulation of neural pathways responsible for chronic pain perception, altering pain signals traversing the central nervous system.1 This technology, first utilized in the 1960s has become the standard of care for many suffering pain from persistent spinal pain syndrome type 2 (PSPS-T2), complex regional pain syndrome, non-surgical back pain, diabetic peripheral neuropathy, and other neuropathic pain conditions.
Throughout the years, SCS technology has undergone significant innovation to improve its therapeutic efficacy and to address a broader range of chronic pain conditions. Early systems described in the 1970s and 1980s required the placement of electrodes through a laminectomy within the subdural space and were connected to external generators. Modern SCS systems now utilize fully implantable generators powered by batteries, offering increased convenience and safety.2 Additionally, the development of percutaneous techniques for placing electrodes reduces the risk of complications and allows for trial periods before permanent implantation.2 SCS systems have experienced advances in waveform technology which have further expanded the potential of this therapy. Emerging research suggests that SCS mechanisms are more complex than the original gate control theory proposed by Melzack and Wall in the 1960s and are believed to selectively activate certain areas of the dorsal horn within the spinal cord.2,3 Earlier stimulation therapies were based on tonic waveforms, providing continuous electrical pulses. Newer paresthesia-free devices include burst and high-frequency stimulation have led to more durable outcomes and patient satisfaction. Passive recharge burst waveforms as described by DeRidder may even have a primary action in the medial thalamus based on electroencephalogram (EEG) and functional Magnetic Resonance Imaging (fMRI) studies.4 The ability to tailor waveforms and stimulation parameters to individual patients represents a significant shift in the management of chronic pain, highlighting the adaptability and expanding utility of SCS in various clinical scenarios.5 In addition, newer systems that measure evoked compound action potentials and respond up to 4 million times per day via closed loop mechanism may have an impact on future product development.6
As technology advances, it is important to ensure that the patient experience maintains priority. Certainly, advances in waveforms and battery technology are more widespread, but one important aspect that cannot be overlooked is the patient experience and interaction with technology. This is critical, considering the overall experience may influence the desire to be maintained in therapy with a device. Not only is the interaction with the technology important but so is surgical technique. In this review, we review the available literature and current market products to provide guidance on how to optimize the user experience of spinal cord stimulators for manufacturers and health care providers.
Indications for SCS
Although internal pulse generators can be found in various medical devices, the focus of this review is its use in spinal cord stimulation for chronically painful conditions which are outlined here for context. Common SCS indications include pain of the trunk and limbs due to PSPS-T2, complex regional pain syndrome types I and II, ischemic pain syndromes, diabetic neuropathy, lumbar radiculopathy, persistent spinal pain syndrome type 1 (PSPS-T1), and historically intractable angina pectoris, although rarely treated in contemporary practice. In the United States, PSPS-T2 is the most common indication for SCS. Current evidence supports the use of SCS in treating these conditions in carefully selected patients.7–10 Dorsal root ganglion stimulation is similar in process but modulates the dorsal root ganglion and has been shown to be more efficacious in focal neuropathic pain such as complex regional pain syndrome.11 Despite its limited coverage and use in the United States, SCS has shown promise in treatment of peripheral vascular disease and limb salvage, but with the advent of stents, SCS use for intractable angina pectoris is rarely used in present day.7,12 A more recent indication for SCS is painful diabetic peripheral neuropathy which has gained more widespread use and is strongly supported by outcome studies.8,9 SCS use in treating chronic pelvic and visceral pain is evolving, and studies continue to address the efficacy of these indications. Based on current evidence dorsal root ganglion stimulation may have better utilization.10,13–15
Patient Demographics and SCS Explantation
Despite an estimated 71% trial success rate, some patients who undergo permanent implant require explantation of their device.16 One study estimated up to 30% of patients received an explant over 15.5 years, with the majority occurring within the first five years for reasons including infection, pocket pain, loss of efficacy, and device failure.17 Studies show that demographic, health, and pain-related factors may play a role. The relevance of demographic factors, like age and gender, is still evolving, but the most consistent finding is higher explant rates among females.18–20 Tobacco, cannabis, and opioid use have been linked to an increased risk of explant, but this has not been reproduced in prospective fashion, so the significance is uncertain.21 Patients with psychiatric comorbidities - anxiety, depression, and post-traumatic stress disorder – also tend to have higher rates of explantation.21,22 Conversely, those with back pain accompanied by radiculopathy and no prior surgery are less likely to undergo require explant.18,23 The interplay between demographic, health, and pain-related factors is complex, and individual patient assessment remains crucial. Future research with larger sample sizes and longer follow up periods may help clarify conflicting findings and provide a better understanding of the patient decision to pursue explantation.
Components of a SCS System
SCS systems consist of several components: the implantable pulse generator, leads, and external controller. The generator is the power center of the device. It not only generates waveforms but also interacts with external devices to change programming, alter modes, or upgrade software. The leads transmit the signal created by the implantable pulse generator (IPG) and lie adjacent to the target tissue. The external controller provides a patient interface to the SCS, and several platforms now offer remote programming where the patient can have a virtual visit in a different physical location than the representative programmer.
Implantable Pulse Generator (IPG)
An IPG is an electrical power source that delivers current to neural tissue through lead electrodes. IPGs may be either rechargeable or non-rechargeable (primary cell). Initially, IPGs were powered by non-rechargeable lithium cells that required frequent replacement. Current primary cell batteries have longer lifespans, but this can vary based on each system’s energy consumption. To avoid frequent surgical replacement, IPGs with rechargeable batteries were developed. Unfortunately, over time the IPG’s ability to recharge can become less efficient and may even require daily recharging in some cases. Early evidence suggested that patients with rechargeable, high-frequency IPGs were more likely to undergo explantation in a retrospective analysis.24–26 Recharge burden was identified as an important variable due to greater energy usage for high frequency stimulation. Battery technology has continued to improve since these studies were published, and the recharge burden has lessened for some devices. There is now a trend towards smaller rechargeable IPGs over larger non-rechargeable primary cell IPGs, but ultimately this depends on patient preference. As such, it is important to outline the pros and cons with patients when discussing different devices. Table 1 highlights the various SCS IPGs on the market and their unique features. Figure 1 depicts images of each IPG when permission to do so was granted.
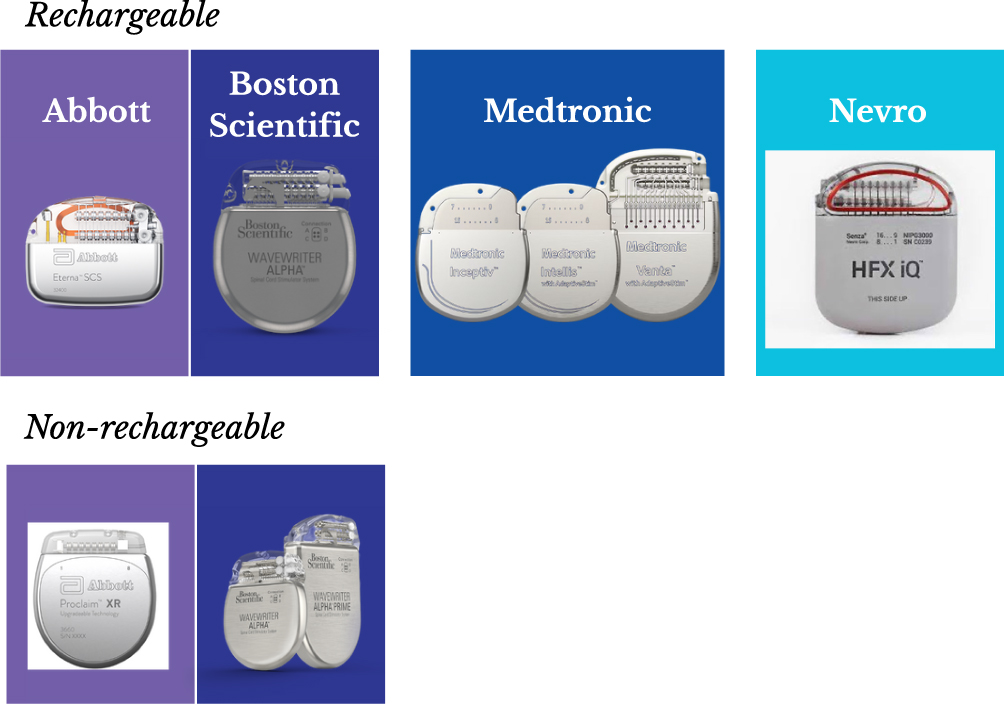 |
Figure 1 Various Internal Pulse Generators (IPG) on the market. Image provided courtesy of Boston Scientific. ©2025 Boston Scientific Corporation or its affiliates. All rights reserved. Images reproduced with permission from Medtronic. Images reproduced with permission from Abbott. Image reproduced with permission from Nevro. An image for Saluda was omitted as no permission was granted. |
 |
Table 1 Various SCS IPGs on the Market, Including Rechargeable and Non-Rechargeable with Features Highlighted |
IPG Magnetic Resonance Imaging (MRI) Compatibility
Early SCS IPG models were not MRI conditionally approved and created dilemmas when patients required imaging for spine or other medical conditions, even requiring explant in some cases. Recent technological innovation has allowed for MRI conditionally approved systems for most brands, although they have different specifications. Some systems are MRI compatible under certain conditions and others are MRI conditionally approved regardless of system integrity. A common cause of incompatibility is high impedance commonly caused by lead fracture, lead scarring, or contact issues in the generator. If Impedances are out of an approved range, MRIs for some systems are not possible. Studies have reported a range of 10–12% of SCS explants due to inability to undergo MRI.27,28 Barriers to standard care due to an implantable device can lead dissatisfaction and negative awareness of the device that leads to explantation. There is ongoing work with the FDA by several manufacturers to demonstrate safety despite the presence of lead fractures, and approval may be available after submission of this manuscript. Table 1 references different MRI compatibility across the market at time of writing.
SCS Leads
SCS leads may be cylindrical or paddle shaped. Cylindrical leads are placed percutaneously via needle epidural access, and SCS trials are performed with this technique. Permanent implantation may either be performed with percutaneous approach using cylindrical leads, or via laminectomy for paddle lead placement. Figure 2 shows SCS lead options. Paddle implantation is associated with slightly higher initial postoperative complications, but significantly lower long-term reoperation rates, likely due to reduced risk of migration compared to percutaneous leads. Percutaneous leads offer reduced initial complication risk and less invasiveness, while long-term healthcare costs are similar between paddle and percutaneous leads.29 There does appear to be an initial increase in postoperative pain with paddle placement, as it is a more invasive surgical procedure, but there is no evidence to suggest that this pain persists in the long term.29,30 A minimally invasive approach to paddle placement involving interlaminar flavectomy using tubular retractors appears to reduce immediate postoperative pain, which could be advantageous in improving patient experience in the long term.31
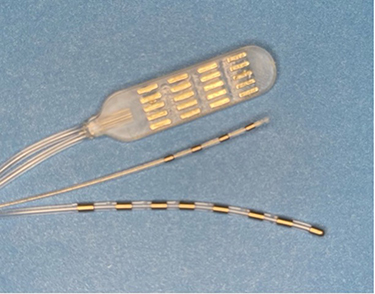 |
Figure 2 Various SCS lead types including paddle (top), dorsal root ganglion (middle) and dorsal column (bottom). (Personal photo). |
Patient Controller
Patients may access their SCS through handheld controllers or phone applications connected via Bluetooth. The controller allows users to toggle the device on/off, switch between preset programs, adjust individual parameters such as amplitude, and place the system in temporary modes to minimize interactions with external environments - airport security, electrocautery, radiofrequency, and MRI. Some systems allow for an application to be placed on their personal phone, reducing the need for an additional device. Interfacing with such applications can be a barrier for technologically illiterate or elderly patients and should be considered prior to moving forward. Simplifying the technical interface on these devices may make navigating easier for those patients that are less technologically savvy.
Remote Monitoring
A newer feature of SCS device management is remote monitoring, similar to technology that exists in cardiac monitoring. Patients with adequate internet connection can have their device accessed, interrogated, and reprogrammed remotely by a representative without having to be physically present in the office. These virtual visits allow providers to efficiently respond to patient needs and monitor for continued efficacy. This addresses a common pitfall – lack of close follow up. In this situation a patient may have felt the device was no longer efficacious but only needed reprogramming to return to their therapeutic window. This technology is expected to become more commonplace among patients and clinics, but changes to postoperative protocols and scheduling flow must be adopted. Reducing barriers to optimal stimulator programming and taking a proactive stance would logically improve the user experience and patient satisfaction.
Anatomic and Surgical Factors Affecting IPG Site Discomfort
SCS is safe and well established in treating chronic pain, but there are possible complications. Some are rare complications such as infection, spinal hematoma or spinal abscess. Others are less urgent but can compromise patient outcomes, such as lead fracture, lead migration, or IPG site pain – often termed pocket pain. The incidence of SCS related pocket pain is well described in literature, but reported rates are widely variable ranging from less than 1% to 60%. The presentation of pocket pain can also be variable. A recent literature review compiled over 50 studies with varying levels of evidence from Level I to IV. This was comprised of several retrospective reviews, but only a few included large sample sizes.32–34 Bao et al evaluated 785 patients with 43 (5.5%) reporting pocket pain. The average time described from initial surgery was 7.5 months with significantly more female than male.35 All patients ultimately required revision or explant. Another review by Cameron et al included 2,753 patients, 24 (0.9%) of which reported device-related discomfort.36
Three notable randomized controlled trials reported an incidence of pocket pain between 4% and 11.9%. In the studies reviewed, several interventions were offered, including repositioning the IPG to a different anatomical location, utilizing a smaller or differently shaped generator, and providing pharmacological management to alleviate pain. In many of these cases surgical revision of the IPG pocket was necessary to address the discomfort. Additionally, patients were counseled on the potential for long-term management strategies to cope with persistent pocket pain.37
Body Mass Index (BMI)
Clinical studies have shown that obese patients experience a 2% reduction in efficacy for every unit increase of BMI and a 20% improved response rate to pain relief in normal or underweight patients compared to morbidly obese individuals.38 Lead migration appears to be more likely in the subacute postoperative period in obese patients, placing emphasis on anchoring techniques in this patient population.39 Studies have also found a higher incidence of superficial wound dehiscence and infection in obese patients.40,41 Despite these risks, SCS can be safely performed in this patient population. Obesity can also make surgical technique more challenging due to large skin folds with excess tissue affecting the position of an IPG in different planes. An IPG that is skin parallel when implanted prone may be angled or protrude against the skin in the seated position. Surgeons must also be aware of tissue depth requirements for each device manufacturer as excess adipose tissue can make proper generator placement challenging with regards to depth. No direct correlation has been identified between and increased incidence of pocket pain and BMI, but evidence specific to this question is limited.32 The opposite situation can also present a problem, wherein a patient implanted loses a significant amount of weight. This can affect the original generator placement and may require revision. Direct evidence of the risk of migration, lead stability, or need for revision in patients that have lost weight is absent at the time of writing.
Demographics
Previous studies have demonstrated gender disparities in the rates of pocket-mediated pain in patients undergoing spinal cord stimulation implantation.42,43 Females reported a higher incidence of IPG site pain attributable to psychosocial and biological factors.44 Biological factors include hormone variation in pain levels during the menstrual cycle in females and the testosterone mediated activation of the descending inhibitory pathway in males.45 Psychosocial factors include higher rates of depression among females, which may account for decreased efficacy. Authors have suggested that a lack of female experts in the field may result in less female-specific needs research.45 In addition, social pressures and prejudiced may cause males to report understated pain levels.46–48 Although previous research has demonstrated females have a higher risk of pain and explant, no significant correlation has been found between race or ethnicity in these patients other than small case studies.35,49,50
IPG Location
Clinical studies have shown that implant location may affect the propensity to develop pocket pain.51 A survey study included patients undergoing device implantation for movement disorders, chronic pain disorders, and psychiatric conditions. The anterior chest site was commonly chosen for movement disorder neuromodulation and abdominal, flank, and gluteal locations dominated for chronic pain indications.51 Results demonstrated significantly more pocket pain at the gluteal implant site in patients with psychiatric disorders, but when the general population was evaluated, no significant differences were found. This indicates that there may be a significant psychiatric component to implant site pain.
Sex dimorphisms should also be considered for IPG location, as men tend to have larger flank circumferences than females. Women also tend to have greater tissue distribution in the hips and thighs and lower flank circumference. Suboptimal device placement in the flank would thus be more noticeable in females.52 Clinical studies have shown significantly more females compared to males experiencing pocket pain with a tendency towards IPG placement in the buttocks.53 Ideally future studies would identify particular locations that may cause an increased incidence of pocket related pain. But current evidence suggests the question is much more complicated, that the propensity for IPG site-mediated pain can be affected by sex dimorphisms, implant indication, and psychiatric conditions, not one single factor. These influences should be accounted for when offering and planning SCS, with particular attention paid to IPG placement and incorporation of patient input. Some surgeons advocate for a temporary device worn externally prior to implantation so the patient can play a more active role in choosing an IPG site location. Additionally, one must account for the need for longer leads at some locations, particularly for cervical lead placement.
Patient Satisfaction
SCS is backed by years of clinical evidence supporting use in improving pain outcomes for certain conditions.7–10 Overall patient satisfaction is arguably a different measure than pain improvement on Visual Analog Scale (VAS) scale or functional improvement on Oswestry Disability Index (ODI). Patient satisfaction can vary and may be linked to factors other than pain relief. Salekiet al evaluated such factors and found an expected correlation between magnitude of pain relief and satisfaction. In patients receiving >50% pain relief, 81% reported satisfaction, and less so (38–41%) for patients receiving <50% relief.54 Findings also demonstrated significant changes in sleep, fatigue, and quality of life, which may contribute to improved psychological response to pain. Although other studies have previously identified the negative impact of psychological factors, BMI, and gender on SCS success, they have yet to look at pocket pain specifically.38,44,55–57 Measures of overall patient satisfaction, while closely correlated to pain relief, may encompass a variety of factors including ease of device interaction, remote interface, and charging convenience where applicable.
Role of Psychiatric Conditions on Pocket Pain
A thorough review of the literature suggests that there is a paucity of information on the psychological implications of pain caused by IPGs. However, this absence of literature does not suggest that pocket-pain related emotional sequelae are not real and distressing. Regarding etiology, a small 2021 study appears to have been the first to look at psychological factors as predictive of pocket pain - with findings suggesting that anxiety and depression were non-predictive.35
Although studies and systematic reviews have noted pocket pain as a frequent complication, none have examined the relationship between pocket pain and psychological phenomena. A 2017 article was dedicated solely to the phenomenon of pocket pain in neuromodulation.51 The authors covered important issues, including prevalence, etiology, demographics, coverage in the literature, and medical management of patients experiencing pocket pain, yet they chose not to address potential psychological sequelae.
Given this lack of empirical support, we warn against “common sense extrapolation”, and the resulting assumption that pocket pain is related to depression and/or anxiety. Of greatest concern, however, is the possibility that severe pocket pain has an adverse impact on quality of life. The study of such a potential association would not be particularly onerous, although would likely require a prospective approach to better understanding the broad impact of pocket pain. However, irrespective of the high incidence of post-IPG implantation pain well described in the empirical literature, researchers have curiously neglected what would potentially be a useful topic of investigation.
IPG Features and Potential Role in Pocket Pain
IPGs come in both rechargeable and non-rechargeable versions, each with distinct characteristics that may affect pocket awareness and patient experience. However, this awareness may vary based on patient preferences and priorities. Reviewing the features of each is important before proceeding with implantation.
Rechargeable
Rechargeable SCS devices must be recharged at varying intervals, depending on the device model and patient specific energy usage. Traditionally most devices required recharging every few days to weeks, although new technology has lengthened this interval to months in some cases. Experience with newer rechargeable batteries is limited and data on long-term use is still sparse.51 Rechargeable devices are generally designed to last 9 years or more, depending on the manufacturer, but their longevity depends more on usage patterns. Manufacturers estimate lifespans and provide warranties for IPGs if energy usage remains within a prescribed window.35 Early versions of rechargeable IPGs devices struggled to recover after an extended period of full depletion, but newer models have improved this issue.58,59 Table 1 lists the estimates for charge frequency and duration of charge from complete depletion, as provided by the manufacturer. These estimates are difficult as there is individual variance in energy usage based on unique programming options. Despite this, gathering estimates with nominal use from each manufacturer for the purpose of this manuscript was very difficult and, in some cases, impossible. We as authors and physicians call for greater transparency going forward to better inform patients of the expectations with rechargeable systems even if this is based on average energy requirements with the understanding that individual experiences may vary.
Recharging an IPG requires placement of an external charging unit over the IPG and repletes the battery via inductive coupling. Recharging capabilities, initially seen as a significant clinical advantage, have not always met patients’ expectations. For some, the necessity of regular recharging has become a burden rather than a convenience.60 While convenient, recharging can be uncomfortable, especially if the charging device causes pressure over the pocket or generates heat.59 In rare cases, the recharging process must be broken into multiple sequences to avoid excessive heating and discomfort.52 The need for precise alignment during charging increases patient interaction with the device, giving rise to greater pocket awareness. Because of the need for precise alignment, proper surgical placement is important and is addressed in a later section.
Conversely, an advantage of rechargeable IPGs is smaller size due to reduced capacity needs. Smaller IPGs tend to be less noticeable, easier to conceal under the skin, and allow for smaller incisions. Recent innovation in the battery sector has translated to charging improvements. The estimated frequency of recharge for current IPGs is noted in Table 1. Some manufacturers have not reported and did not respond to query as noted. As with other non SCS batteries, recharging capabilities can change over time, particularly with lithium-ion cell batteries. With age and many recharge sessions, lithium-ion cell batteries may experience decreased capacity and increased internal resistance by means of energy and power loss. This can translate to longer charging times and shorter duration on a full charge. Some manufacturers utilize a lithium-titanate cell in attempts to reduce this effect.61
One area that is not well understood is the pattern of recharging. Lithium-ion batteries are known to have greater lifespan if maintained within the range of 20–80% charge and demand higher energy with greater battery stress to charge from 90 to 100% than at lower capacities.62 Some patients may charge only when the battery is fully depleted, and others may charge a short amount every day. This interval may change over the life of the battery based on charging patterns and other factors. It is yet to be determined what the optimal schedule is, but future research should help elucidate this to optimize patient experience and battery function. Ideally a specific charging pattern should be prescribed. It should also be noted that complex recharging protocols may be too difficult for elderly patients or the technologically challenged.
Non-Rechargeable (Primary Cell)
Non-rechargeable IPG device lifespan can range on average from three to seven years, depending on patient energy usage.38 IPG capacity depletion ends pain therapy and requires surgical replacement. Replacing the IPG involves surgically accessing the pocket and risks worsening pain and discomfort. Despite eliminating the need for recharging, the larger size of non-rechargeable IPGs can increase risk of pocket discomfort, particularly in patients with a lower BMI.56 Studies have shown that larger pulse generators may shift within the pocket, contributing to greater pain and a higher likelihood of revision surgeries.63 Despite expected differences in battery lifespan, a real-world retrospective study of 106,462 Medicare beneficiaries found similar clinical longevity for primary cell and rechargeable batteries.64 Moreover, the pocket location itself plays a significant role in patient experience with non-rechargeable devices.52 Proper surgical planning and consideration of pocket location are crucial to minimizing discomfort with both rechargeable and non-rechargeable devices.55
While rechargeable devices offer a smaller form factor, frequent recharging can increase the patient’s device interaction, contributing to pocket awareness. On the other hand, non-rechargeable devices eliminate the need for recharging but may cause greater pocket pain due to their larger size and the need for surgical replacement. Careful consideration of these factors, along with patient specific attributes such as BMI and tissue density are essential in selecting the appropriate device and minimizing the risk of pocket pain and awareness. The authors of the Medicare study concluded that patient factors other than device lifespan should be considered when choosing an implantable device given their similar clinical longevity.64
Size
Currently available SCS IPGs vary significantly in volume, size, and shape. These factors may be relevant in influencing the propensity for developing pocket pain. The design and functionality of these devices have evolved, with focus on optimizing therapeutic outcomes and patient satisfaction, while minimizing invasiveness and complications. Smaller IPGs are associated with reduced rates of pocket pain and higher patient comfort and satisfaction than larger IPGs.51 Even smaller micro-IPGs have been found to reduce complications and improve usability.65 The implications of device size extend beyond patient comfort and surgical ease, as IPG size influences system capacity, lifespan, and recharge burden, particularly for high energy waveforms. Table 1 shows the various sizes of available IPGs on the market.
Shape
How we interact with objects often depends more on shape than we may appreciate. The more an objects form resembles the natural world, the more likely we are to seek interaction. A common design theme used by technological companies incorporates rounded, smoother edges in objects with which we interact closely (ie – smartphones, watches) and reserves straighter lines and edges objects that we view at a distance (ie - desktop computer, television). Even these more squared objects have rounded edges, and have been referred to as “squircles”, shown in Figure 3.
 |
Figure 3 A “squircle”, is demonstrated as the outer edge of the object, compared to the circular shape in the center. (Personally created). |
The smooth, rounded edges draw us in to fidget with the device, a closer resemblance to the natural world. No current data has examined patient satisfaction specific to IPG shape, but more rounded edges approaching circular are expected to be favorable. Obviously, a patient cannot interact with an IPG as if it were a smartphone, but rounded edges can reduce erosion risk, stress on surrounding tissues, and are less likely to pinch the tissues when contacted. Various shapes of current IPGs on the market are shown in Table 1. Future IPGs might increasingly adopt a more circular design as they aim to build upon this design strategy.
Surgical Factors for Pocket Creation
Pocket pain can arise due to various factors, including patient body habitus, IPG characteristics, and surgical technique.35 The creation of the IPG pocket during SCS device implantation is a critical step to minimize postoperative pain and long-term discomfort at the IPG site, enhance SCS functionality and patient outcomes, and improve overall satisfaction. Studies suggest that the revision rates for SCS due to intractable IPG site pain range from 1% to 19%.51 On average, pocket pain develops 7.5 months post-surgery, with revision surgery occurring approximately 4.5 months after pain onset.35 As mentioned previously, sex-based and anthropometric differences are key factor in the preoperative planning and potential development of pocket pain.35,53
The location of IPG implantation correlates with the incidence of site-specific pain. The lowest rates of IPG related pain have been observed in the posterior chest wall (13%) and the highest in the abdomen (28%). Flank implants, both small rechargeable and non-rechargeable IPGs exhibited similarly low rates of pocket pain.52
Current literature underscores the importance of carefully selecting the IPG pocket location to minimize the risk of revision and pocket pain while optimizing patient comfort. Biomechanical and computer modeling studies have previously suggested the abdomen as the most appropriate site for thoracic SCS, and midaxillary placement for cervical SCS to reduce the mechanical forces on the system that contribute to lead fracture,66 but this is in conflict with the pocket pain reported to be associated with these implant sites. Implanters must therefore take each patient into account when deciding on an implant location to optimize patient comfort and system preservation.
The optimal IPG site thus remains controversial and should be individualized based on patient-specific factors, surgical technique, and device type. Chest wall placement risks damaging the supraclavicular nerves (anterior pectoral placement) or the anterior cutaneous branches of the upper thoracic nerves (posterior chest wall). Conversely, the subcutaneous fat density in the abdominal and posterior flank regions may offer an advantage for IPG placement, although the complex vascular and nerve structures in the anterior abdominal wall, including branches of the subcostal, thoracoabdominal, and iliohypogastric nerves can increase the likelihood of pocket pain.52 Flank placement may be preferred due to reduced lead extension length, decreased risk of IPG migration with proper anchoring, and improved patient comfort. An example of flank placement and proximity to the lead incision is shown in Figure 4. Although buttock placement is commonly performed, it has been associated with a higher incidence of pocket pain and revision surgery, due to the proximity to the posterior superior iliac spine and cluneal nerves as demonstrated in Figure 5.52 Moreover, IPG placement in the buttock has been linked to higher revision rates compared to flank placement.58 Several common IPG implant sites for thoracic SCS are shown in Figure 6.
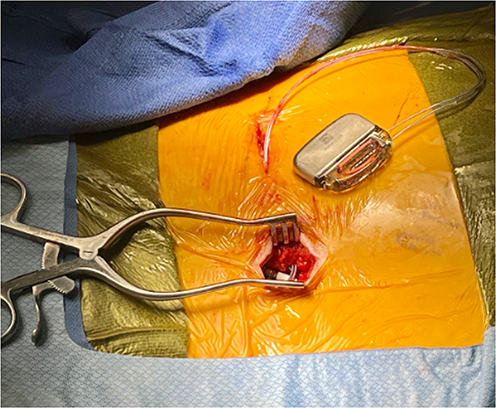 |
Figure 4 SCS leads placed near midline, anchored to thoracolumbar fascia and tunneled to the left flank for generator implantation. (personal photo). |
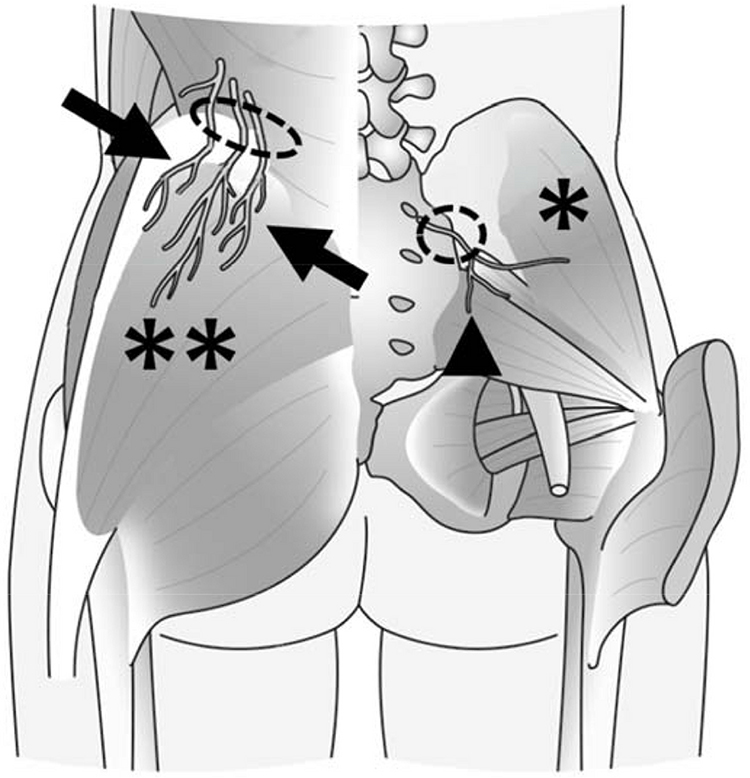 |
Figure 5 Anatomic depiction of superior (arrows) and middle (arrowhead) cluneal nerves. Note the superior cluneal nerve location relative to the iliac crest (dotted circles), which may be affected with gluteal generator placement. Gluteus medius muscle (*) and gluteus maximus muscles are represented (**)67 (Creative Commons Permissions). |
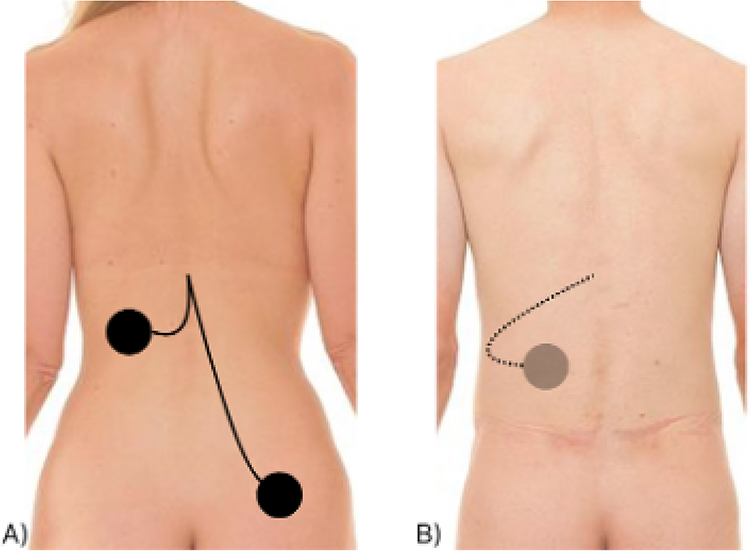 |
Figure 6 Possible locations for generator placement after thoracic SCS placement (A) paraspinal and gluteal, (B) abdominal (Adapted from Stockholm photos −109) Taken at City Studios in Stockholm (www.stockholmsfotografen.se), September 29, 2011, with assistance from KYO (The organisation of life models) in Stockholm. Wikimedia Commons. https://commons.wikimedia.org/wiki/File:Posterior_view_of_human_female_and_male_backs_(cropped).jpg. |
.jpg){kind=link}
Shared decision making is important when deciding on an IPG implant site, informed by a detailed discussion of the risks and benefits of each option. The patient’s preference should be documented during the preoperative visit, and the selected location should be marked on the skin with a surgical pen preoperatively in various positions. For gluteal placement, the patient should wear pants during the preoperative marking, and a model of the IPG should be positioned over the skin while the patient is both seated and standing to ensure that the device will not interfere with normal activities such as sitting or lying down. Similarly, for midaxillary placement, women should wear a bra during the preoperative marking process. A suggested strategy is to apply an IPG model to the patient’s body a few days before surgery to confirm the chosen site and reduce the likelihood of revision due to suboptimal placement.
Pocket Depth, Size, and Orientation
In addition to location, other surgical factors such as pocket size, depth, and tunneling techniques also contribute to IPG site pain. The pocket should be created with precision to closely match the dimensions of the IPG, minimizing dead space and reducing the risk of migration or rotation. Pockets that are too tight may cause compression of the device against surrounding tissues and potentially cause ischemia, while overly large pockets can lead to excessive mobility. Large pockets with excess dead space may allow the IPG to flip or turn inside the pocket. The torsional strain placed on the leads can cause coiling followed by migration or fracture, requiring revision surgery. Furthermore, constant friction can increase the incidence of pocket pain. Patients with less subcutaneous tissue may be at higher risk for battery flipping or device movement, as there is less tissue to stabilize the device. Furthermore, the composition of the soft tissue (eg, muscle versus fat) can also affect device stability. This can be exacerbated by excessive body movement causing the device to flip or angle within the pocket. Using an IPG template during surgery helps ensure proper pocket sizing.68
The depth of the pocket and whether the IPG is placed subcutaneous or subfascial are important considerations. All devices communicate wirelessly and require specific depths to reduce interference. Subfascial placement, while sometimes recommended, may interfere with recharging or communication capabilities.68 The recommended implant depth for individual rechargeable and non-rechargeable IPGs are listed in Table 1. If the pocket is too shallow, the recharging process becomes paradoxically inefficient, leading to longer recharging sessions. Conversely, a pocket that is too deep can reduce the recharging coil’s energy transfer.14,51,60 Implanters should reference the recommended implant depth per manufacturer specification to allow for proper device communication.
The orientation of the incision relative to the IPG may affect IPG aesthetics and position. If the incision is the superior or inferior most portion of the IPG it is more likely that the IPG could angle within the pocket and potentially create pressure points. To avoid this an incision that crosses the center of the IPG is ideal as in Figure 7. When creating the pocket blunt dissection is performed just above and below the incision at the appropriate size to accommodate the chosen IPG.
 |
Figure 7 (A) Lateral and (B) Coronal view of IPG (brown) orientation relative to incision (dotted line) and potential for IPG angulation or flipping relative to the incision. (Personally created). |
Surgical Dissection
Surgical dissection techniques include blunt, sharp, and electrosurgical dissection. Blunt dissection is the separation of tissues along natural tissue planes utilizing non-cutting edges. Blunt dissection is less likely to damage to surrounding structures but may lead to tissue edema and seroma formation if excess force is used.69 Sharp dissection uses a cutting edge, is necessary for skin incision, and may be utilized in deep tissues at the surgeon’s discretion. However, excessive use can cause damage to surrounding structures, particularly peripheral nerves. Electrosurgical dissection with monopolar electrocautery is often utilized for cutting and hemostasis, resulting in decreased blood loss and operative times when compared to traditional cold sharp dissection.70 While electrocautery has also been shown to decrease postoperative pain and tissue damage, excessive electrocautery use may lead to seroma formation and poor wound closure. Postoperative wound complications can lead to heightened awareness of pocket pain. Additionally, it is important to ensure that the dissection is performed within the same tissue plane, so that the IPG remains parallel to the skin surface, as angulation of the IPG may place unnecessary pressure on the skin and underlying tissues increasing the risk of pocket discomfort.
Wound Closure
There are various described methods for wound closure. Wound closure can be completed in one or multiple layers, utilizing any combination of sutures, staples, and/or topical skin adhesive. The Neurostimulation Appropriateness Consensus Committee (NACC) recommends utilization of a multi-layer closure to reduce tissue tension and thus the risk of circulatory compromise and wound dehiscence.71 This technique also minimizes dead space which decreases the risk of hematoma, seroma, and IPG movement. A multilayer closure involves closure of tissue planes in a sequential order. Typically, absorbable braided sutures, such as Vicryl (Polyglactin 910, Ethicon Inc., New Jersey, USA), in running interrupted fashion are used to approximate the deep tissue layers due to their high tensile strength. Sutures should be placed in an inverted fashion as to bury the knot to reduce the risk of stitch abscess and inflammatory reaction.72 For skin closure, non-absorbable sutures (silk, nylon) can be placed in a transdermal fashion (simple interrupted, running, vertical mattress, etc) or an absorbable running subcuticular suture such as Monocryl (copolymer glycolide and caprolactone, Ethicon Inc., New Jersey, USA) can be utilized. A running subcuticular suture is preferred to transdermal sutures for cosmesis.73,74 The risk of wound dehiscence with running subcuticular closure can be mitigated by applying a topical skin adhesive. If staples are used for closing the superficial layer, it is imperative to use proper technique of eversion for approximating the skin edges, allowing for proper wound healing and cosmesis. Staples offer the advantage of speed when compared to sutures and topical skin adhesive75,76 however, there is evidence to suggest that there is less acute postoperative pain and increased cosmetic satisfaction when using sutures compared to staples.77 Topical skin adhesive such as Dermabond (Ethicon Inc., New Jersey, USA), can be used as an alternative to or in conjunction with suture or staples for the skin. Studies suggest that topical skin adhesive decreases postoperative pain, decreases risk of surgical site infection, and provides better cosmesis when compared to sutures and staples.76,78,79 Despite this evidence, a retrospective review compared postoperative pain levels after SCS implant closed with running suture and staples and found no difference in pain scores between the two cohorts at postoperative days 1 and 10.80
Wound dressings provide protection of the wound from injury and contamination and should adequately cover the entire wound closure. A multi-center retrospective review of 2,737 SCS implants and revisions found a statistically significant reduction in surgical site infection (SSI) rates with the application of a sterile occlusive dressing in the operating room. Although the data in SCS patients supports the use of a sterile occlusive dressing, it should be noted that a Cochrane systematic review was unable to determine with any certainty whether covering a surgical wound with a wound dressing decreases the rate of SSI or if a particular wound dressing (transparent film, silver-containing, hydrocolloid) was more effective at reducing SSI or reducing pain.81 Despite the findings of the systematic review, the Neurostimulation Appropriateness Consensus Committee (NACC) continue to recommend the use of a sterile occlusive dressing for 24 to 48 hours for surgical wounds healing under primary intention to reduce the risk of SSI.71
When implanting SCS systems, patient safety and positive outcomes are priority, however we argue that reduced pocket pain and awareness is as important as relief of preoperative pain. Meticulous planning and operative skill during surgical placement can reduce risk of infection, tissue trauma, and postoperative pain, as has been described. Minimizing postoperative pocket pain reduces patient focus on the newly implanted IPG and is expected to reduce pocket awareness in the long term, although this has not yet been formally evaluated.
Anchoring the Generator
Anchoring the generator by placing a nonabsorbable stitch reduces the risk of the IPG moving or flipping within the pocket. The ability of the IPG to move significantly increases risk of pocket awareness and discomfort. The IPG is typically anchored at the level of the Scarpa’s fascia in the abdomen or the thoracolumbar paraspinal fascia posteriorly but may vary based on the patient’s body mass index.82 A combination of sharp and blunt dissection is often used to delineate an anchor plane and subsequently anchored the IPG.82,83 Depth may vary based on individual body habitus and battery requirements, but the optimal plane for the pulse generator to reduce the risk of erosion and allow for successful telemetry is approximately 0.5 to 2 cm when anatomically possible and always considering the manufacturer recommendations (Table 1).84 If the IPG is not anchored to fascia appropriately or if sutures absorb over time, movement risk increases.85 Therefore, it is recommended to use 2–0 non-absorbable sutures when anchoring is performed.85,86
Strain Relief Loops
Strain relief loops in the pocket not only absorb the pushing and pulling forces exerted on the lead wires during use but also increase their bend radius. An increase in the bend radius increases the force required to cause lead displacement. It is well appreciated that implanting SCS leads in the IPG pocket without strain relief loops may reduce the functional survival time of the leads.85 The use of multiple strain relief loops might provide an additional buffer against potential effects of longitudinal forces, minimizing the potential for lead migration.86 A bend radius that is too small, however, may increase the risk of lead compromise due to lack of strain relief. Tissue encapsulation around the loops is expected to prevent such an occurrence. It is also important to consider that knot tightness and possible tissue ingrowth may restrict the free movement of the loop during a patient’s range of motion.66
External Pocket Factors
IPG rotation within the pocket can be caused by a condition called Twiddler’s syndrome.66 There are two recognized forms of this phenomenon: spontaneous and external. In the spontaneous form, the IPG moves without external manipulation by the patient.66 Factors that predispose a patient to spontaneous syndrome include subcutaneous pouches that are too large, become filled with fluid such as seromas, or IPGs that are not anchored.66,87 In these circumstances, even normal patient activity can cause twiddling. External Twiddler’s syndrome is caused by digital manipulation of the IPG by the patient, usually soon after implantation before the device has had adequate time to scar.87 Either form can lead to complications, including IPG flipping, lead fracture, lead migration due to winding, and pocket pain. IPGs must be implanted with the label facing the skin for external programmers to be able to communicate and IPGs to charge. If the IPG flips, communication with external devices may be rendered nonfunctional, the known exceptions being Abbott (Texas, USA) Eterna and Medtronic (Minnesota, USA) Intellis/Vanta/Inceptiv which allows communication in both IPG directions. The lead wires can also twist around each other, placing a tremendous amount of strain on the leads potentially leading to lead migration. Fractures of the leads as they enter the IPG ports can result in localized paresthesia’s, loss of efficacy, and current drain from an open circuit with rapid depletion of the IPG.73
It is important to take care when creating subcutaneous pockets, anchoring the IPG to the wall of the pouch with a nonabsorbable suture, and counseling patients to avoid manipulation. Subfascial pouches have much less potential space than subcutaneous pouches, and the incidence of IPG movement and seroma formation seems to have been reduced significantly.73 Creating an IPG pocket in a single plane, in a low strain area, and utilizing the above surgical techniques to reduce pocket pain should reduce pocket awareness and result in enhanced patient outcomes.
Pocket Awareness
Providers who implant and manage SCS devices often focus on the obvious goals of improving chronic pain. As growing evidence has supported the use of SCS for a variety of indications, we should now begin to focus more closely on the user experience. First and foremost, improvement of preoperative pain is the objective, but patients interreact with their device physically, emotionally, and electronically. As we have demonstrated in this manuscript, a variety of factors affect this experience.
Here we introduce a new term - pocket awareness. Success should be defined as the patient having a seamless interaction with the device and passively unaware of its existence. Pocket pain obviously increases pocket awareness, and we have reviewed the engineering and surgical factors that increase the risk of pain, but the technical interface for changing programs, mechanism of recharging, MRI compatibility, and other factors greatly influence a patient’s satisfaction with their device.
Consumers have grown accustomed to interacting with technology as an extension of themselves. The more seamless and natural this interaction, the greater device attraction, be it conscious or not. Achieving this goal begins with the engineers who design and manufacturers who produce. We have made the case for choosing appropriate candidates and devoting proper attention to surgical implantation. Thorough preoperative education helps patients maximize device function, and long-term care should include regular follow up after implantation to ensure the device is meeting therapeutic goals.
Management of an Existing Painful Generator Pocket
Though there are currently no guidelines for addressing pocket pain, management can range from conservative to explanting the entire SCS system.32 Obviously, explanting a functioning system is the least desirable route. After infection and other acute issues have been ruled out, initial management may include topical analgesics, neuropathic medications, and physical therapy accounting for patient comorbidities.35,37,51 Topical analgesics such as lidocaine, capsaicin patches, or EMLA (a eutectic mixture of lidocaine 2.5% and prilocaine 2.5%) cream can be utilized.88–91 Oral medications may include duloxetine, gabapentin, and pregabalin for pocket neuralgia symptoms, but may be fraught with side effects.42,51,88,92,93
If conservative management has been trialed and pain persists, surgical revision should be considered.32 The pocket may be revised to create a single level plane for IPG positioning if there is undue skin pressure from a mispositioned battery. If appropriate, the IPG should be repositioned to avoid skin folds or pressure points. The IPG may also be relocated deep to the current location so long as depth is still compatible with manufacturer recommendations. Finally, the IPG can be moved to an alternate site, possibly the contralateral side. If replacement is necessary, a smaller IPG may cause less discomfort.32 Alternatively, a non-rechargeable IPG would allow the pocket to be created deeper, however manufacturers may still require a minimum depth to communicate with an external device for programming changes. If pain continues despite revision or replacement, explant may then be required after a thorough discussion with the patient.
Above all, managing patient expectations may reduce the risk of pocket pain and decrease awareness of the implanted device.37 Furthermore, cognitive behavioral therapy is an option to reduce the awareness or angst associated with the implanted device, as has been demonstrated in other conditions.94 Though these treatments are suggested options for pocket pain, future research is necessary to evaluate the efficacy and safety.
Conclusion
Arguably the best strategy for managing pocket discomfort is prevention. Several patient and device specific strategies have been discussed here, and inferences can be made regarding application to individual practice. A comprehensive conversation with the patient should include rechargeable versus non-rechargeable batteries, implant location, lead type, and potential demographic and psychosocial factors that increase the risk of pocket pain. A detailed operative plan with implementation of proper surgical skills is necessary for positive outcomes. Future studies, and perhaps guidelines, should provide clarity and specific recommendations for providers and manufacturers to reduce the risk of pocket pain and even awareness to optimize device interaction for success and longevity of neurostimulation. Additionally, components of the system such as remote monitoring and technical interface are important considerations manufacturers should pursue to improve the patient experience with their device. A common barrier to spinal cord stimulation is patient resistance to an implantable device. Manufacturers should and are pursuing device development to minimize this patient burden, which would be expected to increase patient interest in the therapy in the future. As an established therapy for various chronic painful conditions future advancements may be therapy related, however we hope this manuscript highlights the important factors that contribute to a positive or negative patient experience based on device features, patient factors, and surgical implementation.
Disclosure
Grant funding was provided by Abbott Technologies to cover the cost of manuscript submission and was not involved in the editorial process.
No conflicts of interest to disclose for Harman Chopra, Lucas Bracero, Rosa A. Garcia, Robin Mata, Abigail T. Tisler, Marcin Karcz, Christopher L. Robinson, Zayd Al-Asadi, Aaron D. Sciascia.
Tariq AlFarra is a consultant for Saluda Medical.
Vinicius Tieppo Francio is a consultant for Mainstay Medical and receives research funding from an Investigator Initiated Study (IIS) grant from Nevro corp.
Timothy Deer is a consultant for: Abbott, Saluda, Boston Scientific (relivant), Nervonik, Painteq, Spinal Simplicity, Cornorloc, Aurora
Michael E. Schatman is the Senior Medical Advisor to APURANO Pharma
Brandon Gish is consultant for Abbott and has received research funding from Abbott.
References
1. Hagedorn JM, Deer TR, Falowski SM, et al. An observational study of intraoperative neuromonitoring as a safety mechanism in placement of percutaneous dorsal root ganglion stimulation and spinal cord stimulation systems. J Pain Res. 2020;13:3349–3353. doi:10.2147/JPR.S289416
2. Lam CM, Latif U, Sack A, et al. Advances in spinal cord stimulation. Bioengineering. 2023;10(2). doi:10.3390/bioengineering10020185.
3. Jensen MP, Brownstone RM. Mechanisms of spinal cord stimulation for the treatment of pain: still in the dark after 50 years. Eur J Pain. 2019;23(4):652–659. doi:10.1002/ejp.1336
4. Deer T, Slavin KV, Amirdelfan K, et al. Success using neuromodulation with BURST (SUNBURST) study: results from a prospective, randomized controlled trial using a novel burst waveform. Neuromodulation. 2018;21(1):56–66. doi:10.1111/ner.12698
5. Joosten EA, Franken G. Spinal cord stimulation in chronic neuropathic pain: mechanisms of action, new locations, new paradigms. Pain. 2020;161(1):S104–s113. doi:10.1097/j.pain.0000000000001854
6. Mekhail NA, Levy RM, Deer TR, et al. ECAP-controlled closed-loop versus open-loop SCS for the treatment of chronic pain: 36-month results of the EVOKE blinded randomized clinical trial. Reg Anesth Pain Med. 2024;49(5):346–354. doi:10.1136/rapm-2023-104751
7. Mannheimer C, Eliasson T, Augustinsson LE, et al. Electrical stimulation versus coronary artery bypass surgery in severe angina pectoris: the ESBY study. Circulation. 1998;97(12):1157–1163. doi:10.1161/01.CIR.97.12.1157
8. de Vos CC, Meier K, Zaalberg PB, et al. Spinal cord stimulation in patients with painful diabetic neuropathy: a multicentre randomized clinical trial. Pain. 2014;155(11):2426–2431. doi:10.1016/j.pain.2014.08.031
9. Petersen EA, Stauss TG, Scowcroft JA, et al. Effect of high-frequency (10-kHz) spinal cord stimulation in patients with painful diabetic neuropathy: a randomized clinical trial. JAMA Neurol. 78(6):687–698. doi:10.1001/jamaneurol.2021.0538
10. Hunter C, Davé N, Diwan S, Deer T. Neuromodulation of pelvic visceral pain: review of the literature and case series of potential novel targets for treatment. Pain Pract. 2013;13(1):3–17. doi:10.1111/j.1533-2500.2012.00558.x
11. Deer TR, Levy RM, Kramer J, et al. Dorsal root ganglion stimulation yielded higher treatment success rate for complex regional pain syndrome and causalgia at 3 and 12 months: a randomized comparative trial. Pain. 2017;158(4):669–681. doi:10.1097/j.pain.0000000000000814
12. Ubbink DT, Vermeulen H. Spinal cord stimulation for non-reconstructable chronic critical leg ischaemia. Cochrane Database Syst Rev. 2013;2013(2):Cd004001. doi:10.1002/14651858.CD004001.pub3
13. Gish B, Langford B, Sobey C, et al. Neuromodulation for the management of chronic pelvic pain syndromes: a systematic review. Pain Pract. 2024;24(2):321–340. doi:10.1111/papr.13295
14. Baranidharan G, Simpson KH, Dhandapani K. Spinal cord stimulation for visceral pain--a novel approach. Neuromodulation. 2014;17(8):753–758. doi:10.1111/ner.12166
15. Kapural L, Nagem H, Tlucek H, Sessler DI. Spinal cord stimulation for chronic visceral abdominal pain. Pain Med. 2010;11(3):347–355. doi:10.1111/j.1526-4637.2009.00785.x
16. Mekhail NA, Mathews M, Nageeb F, Guirguis M, Mekhail MN, Cheng J. Retrospective review of 707 cases of spinal cord stimulation: indications and complications. Pain Pract. 2011;11(2):148–153. doi:10.1111/j.1533-2500.2010.00407.x
17. Simopoulos T, Aner M, Sharma S, Ghosh P, Gill JS. Explantation of percutaneous spinal cord stimulator devices: a retrospective descriptive analysis of a single-center 15-year experience. Pain Med. 2019;20(7):1355–1361. doi:10.1093/pm/pny245
18. Al-Kaisy A, Royds J, Al-Kaisy O, et al. Explant rates of electrical neuromodulation devices in 1177 patients in a single center over an 11-year period. Reg Anesth Pain Med. 2020;45(11):883–890. doi:10.1136/rapm-2020-101681
19. Dougherty MC, Woodroffe RW, Wilson S, Gillies GT, Howard MA 3rd, Carnahan RM. Risk factors and survival analysis of spinal cord stimulator explantation. Neuromodulation. 2021;24(1):61–67. doi:10.1111/ner.13173
20. Buchanan P, Vodapally S, Lee DW, et al. Successful diagnosis of sacroiliac joint dysfunction. J Pain Res. 2021;14:3135–3143. doi:10.2147/JPR.S327351
21. Hussain N, Boulos R, Malik TM, et al. Identifying predictors for early percutaneous spinal cord stimulator explant at one and two years: a retrospective database analysis. Neuromodulation. 2023;26(1):124–130. doi:10.1016/j.neurom.2022.01.021
22. Patel SK, Gozal YM, Saleh MS, Gibson JL, Karsy M, Mandybur GT. Spinal cord stimulation failure: evaluation of factors underlying hardware explantation. J Neurosurg Spine. 2020;32(1):133–138. doi:10.3171/2019.6.SPINE181099
23. Hagedorn JM, Lam CM, D’Souza RS, et al. Explantation of 10 kHz spinal cord stimulation devices: a retrospective review of 744 patients followed for at least 12 months. Neuromodulation. 2021;24(3):499–506. doi:10.1111/ner.13359
24. Garcia K, Wray JK, Kumar S.Spinal cord stimulation.StatPearls.Treasure Island (FL).StatPearls Publishing.2025.
25. North RB, Linderoth B. Spinal cord stimulation for chronic pain. In: Quinones-Hinojosa A, editor. Schmidek and Sweet: Operative Neurosurgical Techniques.
26. Van Buyten JP, Wille F, Smet I, et al. Therapy-related explants after spinal cord stimulation: results of an international retrospective chart review study. Neuromodulation. 2017;20(7):642–649. doi:10.1111/ner.12642
27. Dupre DA, Tomycz N, Whiting D, Oh M. Spinal cord stimulator explantation: motives for removal of surgically placed paddle systems. Pain Pract. 2018;18:500–504. doi:10.1111/papr.12639
28. Moeschler SM, Sanders RA, Hooten WM, Hoelzer BC. Spinal cord stimulator explantation for magnetic resonance imaging: a case series. Neuromodulation. 2015;18:285–288. doi:10.1111/ner.12254
29. Babu R, Hazzard MA, Huang KT, et al. Outcomes of percutaneous and paddle lead implantation for spinal cord stimulation: a comparative analysis of complications, reoperation rates, and health-care costs. Neuromodulation. 2013;16(5):418–426. doi:10.1111/ner.12065
30. Beletsky A, Liu C, Vickery K, et al. Spinal Cord Stimulator (SCS) placement: examining outcomes between the open and percutaneous approach. Neuromodulation. 2023;26:1067–1073. doi:10.1016/j.neurom.2022.11.010
31. Shamji MF, Paul D, Mednikov A. Minimally invasive placement of spinal cord stimulator paddle electrodes is associated with improved perioperative and long-term experience among neuropathic pain patients. Spine. 2018;43:324–330. doi:10.1097/BRS.0000000000002050
32. Mekhail N, Levy RM, Deer TR, et al. Long-term safety and efficacy of closed-loop spinal cord stimulation to treat chronic back and leg pain (Evoke): a double-blind, randomised, controlled trial. Lancet Neurol. 2020;19(2):123–134. doi:10.1016/S1474-4422(19)30414-4
33. Kapural L, Yu C, Doust MW, et al. Comparison of 10-kHz high-frequency and traditional low-frequency spinal cord stimulation for the treatment of chronic back and leg pain: 24-month results from a multicenter, randomized, controlled pivotal trial. Neurosurgery. 2016;79(5):667–677. doi:10.1227/NEU.0000000000001418
34. Kapural L, Jameson J, Johnson C, et al. Treatment of nonsurgical refractory back pain with high-frequency spinal cord stimulation at 10 kHz: 12-month results of a pragmatic, multicenter, randomized controlled trial. J Neurosurg Spine. 2022;37(2):188–199. doi:10.3171/2021.12.SPINE211301
35. Bao J, Khazen O, Olmsted ZT, et al. Treatment strategies for generator pocket pain. Pain Med. 2021;22(6):1305–1311. doi:10.1093/pm/pnab007
36. Cameron T. Safety and efficacy of spinal cord stimulation for the treatment of chronic pain: a 20-year literature review. J Neurosurg. 2004;100(3 Suppl Spine):254–267. doi:10.3171/spi.2004.100.3.0254
37. Burke L, Desai MJ. Pocket pain following spinal cord stimulator generator implantation: a narrative review of this under-reported risk. Pain Pract. 2024;24(4):659–669. doi:10.1111/papr.13336
38. Mekhail N, Mehanny D, Armanyous S, Saweris Y, Costandi S. The impact of obesity on the effectiveness of spinal cord stimulation in chronic spine-related pain patients. Spine J. 2019;19(3):476–486. doi:10.1016/j.spinee.2018.08.006
39. Dombovy-Johnson ML, D’Souza RS, Ha CT, Hagedorn JM. Incidence and risk factors for spinal cord stimulator lead migration with or without loss of efficacy: a retrospective review of 91 consecutive thoracic lead implants. Neuromodulation. 2022;25:731–737. doi:10.1111/ner.13487
40. Sommer TW, Ivankovic S, McCall TD. Effect of body mass index on paddle lead spinal cord stimulator safety implantation for chronic pain management. World Neurosurg. 2023;170:e712–e715. doi:10.1016/j.wneu.2022.11.101
41. Bharthi R, Rogowski BC, Moran M, Norris JN, Esplin N, Tomycz ND. Paddle lead spinal cord stimulation in the morbidly obese patient population: outcomes and complications in a single-surgeon cohort. World Neurosurg. 2023;177:e532–e539. doi:10.1016/j.wneu.2023.06.092
42. Prabhala T, Sabourin S, DiMarzio M, Gillogly M, Prusik J, Pilitsis JG. Duloxetine improves spinal cord stimulation outcomes for chronic pain. Neuromodulation. 2019;22(2):215–218. doi:10.1111/ner.12872
43. Bartley EJ, Fillingim RB. Sex differences in pain: a brief review of clinical and experimental findings. Br. J. Anaesth. 2013;111(1):52–58. doi:10.1093/bja/aet127
44. Slyer J, Scott S, Sheldon B, Hancu M, Bridger C, Pilitsis JG. Less pain relief, more depression, and female sex correlate with spinal cord stimulation explants. Neuromodulation. 2020;23(5):673–679. doi:10.1111/ner.13036
45. Melchior M, Poisbeau P, Gaumond I, Marchand S. Insights into the mechanisms and the emergence of sex-differences in pain. Neuroscience. 2016;338:63–80. doi:10.1016/j.neuroscience.2016.05.007
46. Shamji MF, Rodriguez J, Shcharinsky A, Paul D. High rates of undiagnosed psychological distress exist in a referral population for spinal cord stimulation in the management of chronic pain. Neuromodulation. 2016;19(4):414–421. doi:10.1111/ner.12373
47. Sparkes E, Raphael JH, Duarte RV, LeMarchand K, Jackson C, Ashford RL. A systematic literature review of psychological characteristics as determinants of outcome for spinal cord stimulation therapy. Pain. 2010;150(2):284–289. doi:10.1016/j.pain.2010.05.001
48. Levy RM. Women in neuromodulation. Neuromodulation. 2014;17(2):111–116. doi:10.1111/ner.12160
49. Mekhail N, Costandi S, Saweris Y, Armanyous S, Chauhan G. Impact of biological sex on the outcomes of spinal cord stimulation in patients with chronic pain. Pain Pract. 2022;22(4):432–439. doi:10.1111/papr.13097
50. Plesh O, Adams SH, Gansky SA. Racial/Ethnic and gender prevalences in reported common pains in a national sample. J Orofac Pain. 2011;25(1):25–31.
51. Dietvorst S, Decramer T, Lemmens R, Morlion B, Nuttin B, Theys T. Pocket pain and neuromodulation: negligible or neglected? Neuromodulation. 2017;20(6):600–605. doi:10.1111/ner.12637
52. Baranidharan G, Bretherton B, Richert G, et al. Pocket pain, does location matter: a single-centre retrospective study of patients implanted with a spinal cord stimulator. Reg Anesth Pain Med. 2020;45(11):891–897. doi:10.1136/rapm-2020-101752
53. Wells JCK. Sexual dimorphism of body composition. Best Pract Res Clin Endocrinol Metab. 2007;21:415–430. doi:10.1016/j.beem.2007.04.007
54. Saleki M, Khabbass M, Bretherton B, Baranidharan G. Exploring patient satisfaction and other outcome measures with pain relief in spinal cord stimulation: a single-site, cohort audit. Cureus. 2023;15(12):e51339. doi:10.7759/cureus.51339
55. De La Cruz P, Fama C, Roth S, et al. Predictors of spinal cord stimulation success. Neuromodulation. 2015;18(7):599–602. doi:10.1111/ner.12325
56. Marola O, Cherala R, Prusik J, et al. BMI as a predictor of spinal cord stimulation success in chronic pain patients. Neuromodulation. 2017;20(3):269–273. doi:10.1111/ner.12482
57. Sparkes E, Duarte RV, Mann S, Lawrence TR, Raphael JH. Analysis of psychological characteristics impacting spinal cord stimulation treatment outcomes: a prospective assessment. Pain Physician. 2015;18(3):E369–377.
58. Mehta SH, Hoelscher CM, Sharan AD, Thalheimer S, Wu C. Implantable pulse generator site may be associated with spinal cord stimulation revision surgeries. Neuromodulation. 2021;24(8):1336–1340. doi:10.1111/ner.12976
59. Eldabe S, Buchser E, Duarte RV. Complications of spinal cord stimulation and peripheral nerve stimulation techniques: a review of the literature. Pain Med. 2016;17(2):325–336. doi:10.1093/pm/pnv025
60. García Baos J, Marañés Á H, Á M, et al. A pain in the pocket: prevalence of pocket pain in patients with implantation of neuromodulation systems: a retrospective study. Rev Esp Anestesiol Reanim. 2024;71(9):645–651. doi:10.1016/j.redar.2024.02.001
61. Hu C, Ye H, Jain G, Schmidt C. Remaining useful life assessment of lithium-ion batteries in implantable medical devices. J Power Sources. 2018;375:118–130. doi:10.1016/j.jpowsour.2017.11.056
62. Eskandari M, Rajabi A, Savkin AV, Moradi MH, Dong ZY. Battery energy storage systems (BESSs) and the economy-dynamics of microgrids: review, analysis, and classification for standardization of BESSs applications. J Energ Storage. 2022;55:105627. doi:10.1016/j.est.2022.105627
63. Choi H, Gaiha R, Moeschler SM, et al. Factors associated with implantable pulse generator site pain: a multicenter cross-sectional study. Neuromodulation. 2021;24(8):1351–1356. doi:10.1111/ner.13317
64. Deer TR, Pope JE, Falowski SM, et al. Clinical Longevity of 106,462 rechargeable and primary cell spinal cord stimulators: real world study in the medicare population. Neuromodulation. 2023;26(1):131–138. doi:10.1016/j.neurom.2022.04.046
65. Malinowski MN, Heit G, Poree LR, Makous J, Amirdelfan K. Novel spinal cord stimulation system with a Battery-Free micro-implantable pulse generator. Pain Pract. 2022;22:592–599. doi:10.1111/papr.13124
66. Henderson JM, Schade CM, Sasaki J, Caraway DL, Oakley JC. Prevention of mechanical failures in implanted spinal cord stimulation systems. Neuromodulation. 2006;9(3):183–191. doi:10.1111/j.1525-1403.2006.00059.x
67. Isu T, Kim K, Morimoto D, Iwamoto N. Superior and middle cluneal nerve entrapment as a cause of low back pain. Neurospine. 2018;15:25–32. doi:10.14245/ns.1836024.012
68. Pritzlaff SG, Kreis PG, Fishman SM. Permanent spinal cord stimulator placement. In: K PG, editor. Spinal Cord Stimulation: Percutaneous Implantation Techniques.
69. Brenner BR, Ericson T, Singla P, Kohan L. Surgical Instruments. In: Spinal Fusion Techniques. New York: Elsevier; 2024:26–39.
70. Obermeier KT, Liokatis P, Smolka W. Monopolar electrocautery versus sharp dissection in the neck dissection: a retrospective study. Sci Rep. 2023;13(1):4365. doi:10.1038/s41598-023-31328-x
71. Deer TR, Russo MA, Grider JS, et al. The Neurostimulation Appropriateness Consensus Committee (NACC): recommendations for surgical technique for spinal cord stimulation. Neuromodulation. 2022;25(1):1–34. doi:10.1016/j.neurom.2021.10.015
72. Yilmaz E, Tawfik T, O’Lynnger TM, et al. Wound closure after posterior multi-level lumbar spine surgery: an anatomical cadaver study and technical note. Cureus. 2018;10(11):e3595. doi:10.7759/cureus.3595
73. Zhu J, Gutman G, Giere Collins J, Colonna J. A review of surgical techniques in spinal cord stimulator implantation to decrease the post-operative infection rate. J Spine. 2014;4:1000202.
74. Luo W, Tao Y, Wang Y, Ouyang Z, Huang J, Long X. Comparing running vs interrupted sutures for skin closure: a systematic review and meta-analysis. Int Wound J. 2023;20(1):210–220. doi:10.1111/iwj.13863
75. Kanegaye JT, Vance CW, Chan L, Schonfeld N. Comparison of skin stapling devices and standard sutures for pediatric scalp lacerations: a randomized study of cost and time benefits. J Pediatr. 1997;130(5):808–813. doi:10.1016/S0022-3476(97)80025-X
76. Mastud K, Lamture Y, Nagtode T, Rewale V. A comparative study between conventional sutures, staples, and adhesive glue for clean elective surgical skin closure. Cureus. 2022;14(11):e31196. doi:10.7759/cureus.31196
77. Cochetti G, Abraha I, Randolph J, et al. Surgical wound closure by staples or sutures?: systematic review. Medicine. 2020;99(25):e20573. doi:10.1097/MD.0000000000020573
78. Lee CS, Han SR, Kye BH, et al. Surgical skin adhesive bond is safe and feasible wound closure method to reduce surgical site infection following minimally invasive colorectal cancer surgery. Ann Surg Treat Res. 2020;99(3):146–152. doi:10.4174/astr.2020.99.3.146
79. Goto S, Sakamoto T, Ganeko R, Hida K, Furukawa TA, Sakai Y. Subcuticular sutures for skin closure in non-obstetric surgery. Cochrane Database Syst Rev. 2020;4(4):Cd012124. doi:10.1002/14651858.CD012124.pub2
80. Bendel MA, D’Souza RS, North TJ, Pittelkow TP, Hagedorn JM. Skin closure technique and postprocedural pain after spinal cord stimulator implantation: a retrospective review. Pain Res Manag. 2021;2021:9912861. doi:10.1155/2021/9912861
81. Dumville JC, Gray TA, Walter CJ, et al. Dressings for the prevention of surgical site infection. Cochrane Database Syst Rev. 2016;12(12):Cd003091. doi:10.1002/14651858.CD003091.pub4
82. Kumar K, Wilson JR, Taylor RS, Gupta S. Complications of spinal cord stimulation, suggestions to improve outcome, and financial impact. J Neurosurg Spine. 2006;5(3):191–203. doi:10.3171/spi.2006.5.3.191
83. Deer TR, Narouze S, Provenzano DA, et al. The Neurostimulation Appropriateness Consensus Committee (NACC): recommendations on bleeding and coagulation management in neurostimulation devices. Neuromodulation. 2017;20(1):51–62. doi:10.1111/ner.12542
84. Hayek SM, Veizi E, Hanes M. Treatment-limiting complications of percutaneous spinal cord stimulator implants: a review of eight years of experience from an academic center database. Neuromodulation. 2015;18(7):603–608. doi:10.1111/ner.12312
85. Deer TR, Mekhail N, Provenzano D, et al. The appropriate use of neurostimulation: avoidance and treatment of complications of neurostimulation therapies for the treatment of chronic pain. neuromodulation appropriateness consensus committee. Neuromodulation. 2014;17(6):571–597. doi:10.1111/ner.12206
86. Deer TR, Provenzano DA, Hanes M, et al. The Neurostimulation Appropriateness Consensus Committee (NACC) recommendations for infection prevention and management. Neuromodulation. 2017;20(1):31–50. doi:10.1111/ner.12565
87. Israel Z, Spivak A. A tremulous twiddler. Stereotact Funct Neurosurg. 2008;86(5):297–299. doi:10.1159/000155231
88. Carroll I, Hah J, Mackey S, et al. Perioperative interventions to reduce chronic postsurgical pain. J Reconstr Microsurg. 2013;29(4):213–222. doi:10.1055/s-0032-1329921
89. Finnerup NB, Attal N, Haroutounian S, et al. Pharmacotherapy for neuropathic pain in adults: a systematic review and meta-analysis. Lancet Neurol. 2015;14(2):162–173. doi:10.1016/S1474-4422(14)70251-0
90. Likar R, Demschar S, Kager I, Neuwersch S, Pipam W, Sittl R. Treatment of localized neuropathic pain of different etiologies with the 5% lidocaine medicated plaster - a case series. Int J Gen Med. 2015;8:9–14. doi:10.2147/IJGM.S74802
91. Mankowski C, Poole CD, Ernault E, et al. Effectiveness of the capsaicin 8% patch in the management of peripheral neuropathic pain in European clinical practice: the ASCEND study. BMC Neurol. 2017;17(1):80. doi:10.1186/s12883-017-0836-z
92. Vinik A. CLINICAL REVIEW: use of antiepileptic drugs in the treatment of chronic painful diabetic neuropathy. J Clin Endocrinol Metab. 2005;90(8):4936–4945. doi:10.1210/jc.2004-2376
93. Lynch ME, Watson CP. The pharmacotherapy of chronic pain: a review. Pain Res Manag. 2006;11(1):11–38. doi:10.1155/2006/642568
94. Maia AC, Braga AA, Soares-Filho G, Pereira V, Nardi AE, Silva AC. Efficacy of cognitive behavioral therapy in reducing psychiatric symptoms in patients with implantable cardioverter defibrillator: an integrative review. Braz J Med Biol Res. 2014;47(4):265–272. doi:10.1590/1414-431X20133418
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Interventional Pain Procedures: A Narrative Review Focusing On Safety and Complications. PART 2 Interventional Procedures For Back Pain
Lo Bianco G, Tinnirello A, Papa A, Marchesini M, Day M, Palumbo GJ, Terranova G, Di Dato MT, Thomson SJ, Schatman ME
Journal of Pain Research 2023, 16:761-772
Published Date: 9 March 2023
Interplay Between Innovation and Intersubjectivity: Therapists Perceptions of Phantom Motor Execution Therapy and Its Effect on Phantom Limb Pain
Pilch M, van Rietschoten T, Ortiz-Catalan M, Lendaro E, van der Sluis CK, Hermansson L
Journal of Pain Research 2023, 16:2747-2761
Published Date: 8 August 2023
Comparison of Closed Irrigation and Drainage vs Repeated Wound Dressing Changes for Iliac Crest Bone Donor Site Infection in Spine Surgery
Li X, Xiao Q, Zeng JH
Journal of Pain Research 2025, 18:1935-1943
Published Date: 9 April 2025
Machine Learning Approach to Predict Postoperative Pain and Opioid Usage in Elective Primary Spine Surgery: A Retrospective Study
Saksenberg DL, Lee RY, Vaidya S, Yuan A, Jeong SJ, Lockwood N, Li J, Russo GS
Journal of Pain Research 2026, 19:596384
Published Date: 27 March 2026