Back to Journals » Journal of Pain Research » Volume 16
Interplay Between Innovation and Intersubjectivity: Therapists Perceptions of Phantom Motor Execution Therapy and Its Effect on Phantom Limb Pain
Authors Pilch M ![]() , van Rietschoten T, Ortiz-Catalan M
, van Rietschoten T, Ortiz-Catalan M ![]() , Lendaro E
, Lendaro E ![]() , van der Sluis CK
, van der Sluis CK ![]() , Hermansson L
, Hermansson L ![]()
Received 16 March 2023
Accepted for publication 12 July 2023
Published 8 August 2023 Volume 2023:16 Pages 2747—2761
DOI https://doi.org/10.2147/JPR.S412895
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jonathan Greenberg
Monika Pilch,1 Tijn van Rietschoten,2,3 Max Ortiz-Catalan,4– 6 Eva Lendaro,6,7 Corry K van der Sluis,2 Liselotte Hermansson8,9
1Centre for Health Policy & Management, School of Medicine, Trinity College Dublin, Dublin, Ireland; 2University of Groningen, University Medical Center Groningen, Department of Rehabilitation Medicine, Groningen, the Netherlands; 3University of Groningen, Faculty of Medical Sciences, Groningen, the Netherlands; 4Center for Bionics and Pain Research, Mölndal, Sweden; 5Bionics Institute, Melbourne, VC, Australia; 6Department of Electrical Engineering, Chalmers University of Technology, Gothenburg, Sweden; 7Department of Brain and Cognitive Sciences, McGovern Institute for Brain Research, Massachusetts Institute of Technology, Cambridge, MA, USA; 8Department of Prosthetics and Orthotics, Faculty of Medicine and Health, Örebro University, Örebro, Sweden; 9University Health Care Research Center, Faculty of Medicine and Health, Örebro University, Örebro, Sweden
Correspondence: Monika Pilch, Centre for Health Policy and Management, School of Medicine, Trinity College Dublin, 3-4 Foster Place, Dublin, Ireland, Tel + 353 851614350, Email [email protected] Corry K van der Sluis, University of Groningen, University Medical Center Groningen, Department of Rehabilitation Medicine, Groningen, the Netherlands, Tel + 31 503612295, Email [email protected]
Purpose: Interpersonal processes, including therapeutic alliance, may modulate the impact of interventions on pain experience. However, the role of interpersonal context on the effects of technology-enhanced interventions remains underexplored. This study elicited therapists’ perspectives on how a novel rehabilitative process, involving Phantom Motor Execution (PME), may impact phantom limb pain. The mediating role of therapeutic alliance, and the way PME influenced its formation, was investigated.
Methods: A qualitative descriptive design, using a framework method, was used to explore therapists’ (n=11) experiences of delivering PME treatment. Semi-structured online-based interviews were conducted.
Results: A 3-way interaction between therapist, patient, and the PME device was an overarching construct tying four themes together. It formed the context for change in phantom limb experience. The perceived therapeutic effects (theme 1) extended beyond those initially hypothesised and highlighted the mediating role of the key actors and context (theme 2). The therapeutic relationship was perceived as a transformative journey (theme 3), creating an opportunity for communication, collaboration, and bonding. It was seen as a cause and a consequence of therapeutic effects. Future directions, including the role of expertise-informed adaptations and enabling aspects of customised solutions, were indicated (theme 4).
Conclusion: This study pointed to intrapersonal, interpersonal, and contextual factors that should be considered in clinical implementation of novel rehabilitative tools. The results demonstrated that therapists have unique insights and a crucial role in facilitating PME treatment. The study highlighted the need to consider the biopsychosocial model of pain in designing, evaluating, and implementing technology-supported interventions.
Keywords: phantom limb experience, pain, rehabilitation, therapeutic alliance, innovation
Introduction
Phantom Limb Pain (PLP) is one of the most common problems following an amputation, with an estimated prevalence rate of 64%.1 It has been linked to reduced quality of life, diminished personal and economic independence, and negative mental health outcomes.2 The neurogenesis of PLP is not fully understood,3–5 which poses a challenge for identifying an effective treatment and makes the search for innovative PLP therapies an ongoing process.6 PLP treatments have been divided into pharmaceutical and non-pharmaceutical, and the latter are further sub-divided into surgical and non-surgical.7 Among the treatments that aim to promote neuroplasticity,8,9 which include virtual and augmented reality, Phantom Motor Execution (PME) is a promising, non-invasive therapy.10–12 However, pain is not experienced in isolation and may be influenced by processes occurring within an interpersonal context.13 The biopsychosocial model of pain highlights the need to consider a range of influences on pain experiences, including the mediating role of biological, psychological, social, and contextual factors.14 Ortiz-Catalan conceived several working hypotheses on the mechanisms of PME,15 and this study aimed to extend those conceptualisations by exploring potential non-biological influences of treatment effects.
PME utilises myoelectric pattern recognition, virtual reality, and augmented reality, and the intervention roughly consists of three elements.10–12 First, therapists place electrodes on the patient’s residual limb and use a webcam to reflect the patient’s body on a computer screen. A virtual limb is projected on the patient’s residual limb and the muscles’ electrical activity captured by the electrodes allows them to move the virtual limb. Second, patients perform several tasks in virtual environments, such as the Target Achievement Control (TAC) test,16 in which they match their phantom with a projected limb position on the monitor. The system awards patients with a score upon completion/non-completion of the task. Third, other tasks, such as playing serious games, are also controlled using phantom movements in the virtual environments. PME aims to engage the affected sensorimotor neural circuitry in an attempt to disassociate it from pain processing.15 The treatment employs principles used in mirror therapy,17 but addresses some of its limitations. Specifically, in mirror therapy, it is not always clear if patients are engaging the phantom limb in motor activity, as they are simply required to move the contralateral able limb and observe its reflection. In contrast, in PME, the engagement of the affected limb can be verified by using myoelectric pattern recognition to decode phantom limb movements, while virtual and augmented reality provide real-time visual feedback.15 In this process, the muscle activity of the residual limb is recorded by electrodes placed on the surface of the skin and is used to train a machine learning algorithm to decode the intended phantom movements.
PME ensures explicit execution of movements, facilitates the activation of the central and peripheral circuitry related to the phantom limb, and enforces motivation by providing feedback during interactive tasks.15 However, no intervention takes place in isolation and social processes operating within the healthcare context, including affective-motivational dynamics within the interpersonal context of pain and broader socioeconomic influences, may modulate both therapy and outcomes.13,18,19 Markedly, during the PME intervention, patients are supported by therapists, who are present for the entire duration of the treatment and provide expert guidance. A typical PME intervention involves 15 rehabilitative sessions, delivered one, two, or five times per week, each consisting of a two-hour long interaction between patient, therapist, and the PME system. However, the role of non-biological factors in PME implementation, and their link with pain experience, is underexplored.
The potential impact of interpersonal context on pain experience13 points to the need to consider the role of a therapeutic alliance, defined as a relationship between a patient and a therapist.20 While the quality of the therapeutic alliance is considered a reliable predictor of positive clinical outcomes, irrespective of the therapeutic approach taken,21 its role in the context of the PME treatment has not been examined. This is important, as a positive correlation between the therapist-patient relationship and patient outcomes, including pain, has been reported in physical rehabilitation.22 Interpersonal models emphasise the role of a therapeutic relationship and highlight beneficial effects of forming an affective bond between therapists and patients, including agreement on the intervention and its goals.20,21,23 However, the role of innovative tools in modulating patient-therapist relationships has been examined mainly in the context of mental health24–29 and the subjective experiences of a therapeutic alliance in a specific technology-enhanced rehabilitative process remain to be explored. This study aimed to bridge this gap.
PME execution is a relatively novel treatment and exploration of therapists’ subjective experiences of the intervention implementation in a clinical context may shed light on the key mechanisms of action30 or lead to the generation of hypotheses that could be tested in further research. Specifically, although the effects of the PME treatment on patients’ pain outcomes have been evaluated quantitatively within an international clinical trial,11,12 that investigation focused exclusively on changes in pre-specified health outcomes, including pain, and did not take interpersonal or contextual factors into account. Given the scarcity of research examining the possible interaction between novel technology and actors within a rehabilitative setting, and its potential significance for therapeutic outcomes, there is a need to use qualitative methods to explore therapists’ subjective experiences of delivering the PME treatment.
The present study aimed to explore the perspectives of therapists delivering PME treatment12 and collected qualitative data on their views, perceptions, and experiences. We set out to identify how therapists made sense of the therapeutic processes and outcomes, and how they construed therapeutic effects. Factors associated with the treatment effects, as perceived by therapists, were of particular interest in this study and we aimed to shed light on the role of therapeutic alliance in this specific therapeutic approach. Therefore, the secondary objectives were: (a) to identify factors that, in the views of therapists, modulated health outcomes, and (b) to explore how therapists described the role of therapeutic alliance and its establishment in such a context.
Materials and Methods
Study Design and Research Paradigm
We used a descriptive, qualitative design and conducted semi-structured interviews to explore therapists’ experiences of the PME treatment. We embedded the study within the constructivist-interpretive paradigm and the critical interactionism perspectives.31 The ontological and epistemological assumptions were that reality is constructed and mediated by participants’ senses. While they experienced and perceived the world from their unique and relative perspectives, they were conscious meaning-makers and were also able to share their knowledge and insights with researchers.32 The Standards for Reporting Qualitative Research informed the reporting of this study.33
Sampling Strategy and Participants
We used the purposive sampling strategy, approached 19 therapists involved in delivering the PME treatment in the context of an international randomised controlled trial (RCT),12 and asked them to take part in this study. As these therapists also had the experience of delivering the intervention within a control group, namely Phantom Motor Imagery (PMI), we specifically asked them to focus on PME when sharing their experiences (see Supplemental Material). The participants were located in different countries in Europe and North America. To be eligible, they had to (1) deliver PME treatments and (2) speak English fluently. Eleven therapists agreed to take part in the study (response rate 58%). They were all females, had a mean age of 48.5 years, and had on average 19.7 years of experience as an occupational therapist or physical therapist (Table 1). All interviews were conducted in English and through video calls. We used the concept of saturation to assess how adequate our purposive sample was for the phenomenon studied.34–36 We used empirical data and the principle of thematic saturation to identify the point in data analysis when new information in relation to our research questions were no longer identified, repetition was observed, and further data collection was unlikely to provide new information.36,37 Saturation was determined as a post-hoc appraisal that did not influence the number of interviews sought or conducted. In our study, thematic saturation was achieved after analysing transcripts of the first eight interviews.
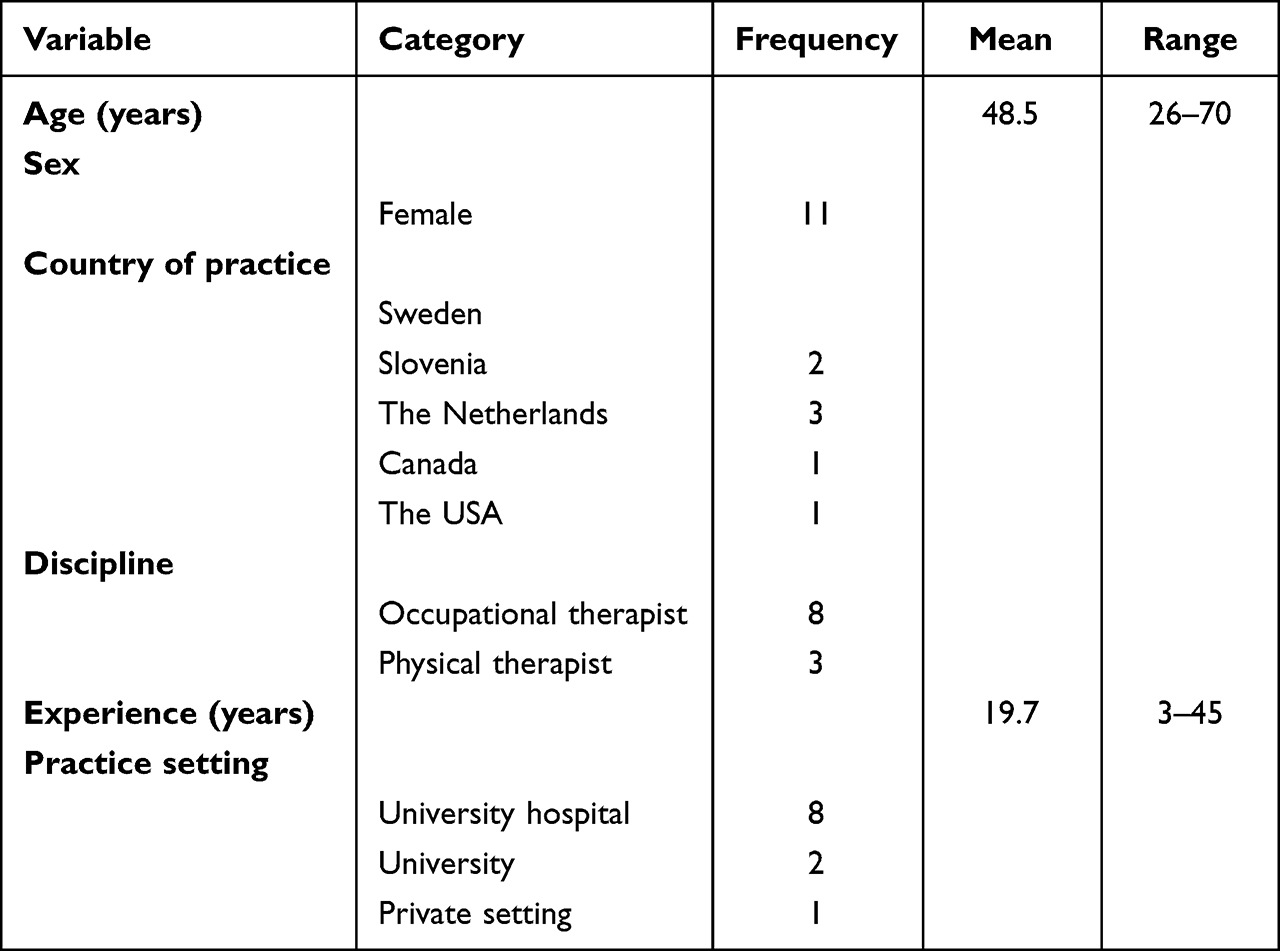 |
Table 1 Characteristics of the Participants (n=11) |
Ethical Issues
The Medical Ethics Review Board (METc 2020/289) of the University Medical Center Groningen, the Netherlands, labelled this study as non-clinical research with human subjects and provided a waiver for ethical approval. Potential participants received a Participation Information Sheet with information on data collection, processing, and storage. Participants signed a consent form and gave approval for using their accounts in this research. Participation was voluntary. Participants had the right to withdraw at any point, and with no consequences, and they did not receive compensation.
Data Collection Methods and Instrument
The participants were invited through email to take part in a semi-structured interview. After receiving a signed consent form, the second author (TvR) arranged an interview date with each participant. All interviews were conducted with the use of the online platform Zoom Video Communications, Inc. An interview guide (see Supplemental Material) facilitated data collection and its development was informed by a framework of contextual factors modulating therapeutic outcomes.19 The guide reflected research questions formulated in this study and consisted of four parts; labelled as: (a) the effect of the PME treatment, (b) phantom limb complaints, (c) evaluation of PME system, and (d) therapeutic alliance. All team members developed, reviewed, and contributed to the final version of an interview guide. The interviews were audio recorded and, after their completion, the recordings were stored in a safe location. They were transcribed verbatim, with pauses captured. The transcripts were sent to the participants for review, who were allowed to revise, add, or change content. The revised versions of the transcripts were pseudonymised and used for the analyses. Participants’ quotes are used to illustrate findings and the interviewees are represented by a numeric code to ensure their privacy.
Data Analysis
The data analysis followed the seven phases of the Framework Approach27 and was led by the first author (MP). Although the framework method has a relatively short history,38 it has been updated.39 We drew on the successful application of this updated analytical approach in the context of health research.40,41 A combined approach to analysis was used, where both inductive (bottom-up) and deductive (top-down) qualitative research processes were utilized. The process involved recording and transcribing interviews, followed by revisions of transcripts applied by interviewees (transcription phase). After the first four interviews were conducted, four researchers (MP, TvR, CKS, LH) became familiar with their content (familiarization with the interviews phase); by listening to the recordings, reading through transcripts, and studying the notes. Initial ideas and recurrent patterns were identified at this stage. Pairs of researchers coded the transcripts (coding), and ideas were exchanged between the four researchers. The first author analysed the codes and examined similarities, differences, and/or discrepancies in coding. Based on the result of those analyses, the first and the second author developed an initial conceptual model, in which relationships between re-occurring patterns were identified (developing a working analytical framework). Recurrent issues, concepts, and initial themes were identified and labelled. After discussing the analytical framework among the four researchers, the framework was applied to the next two transcripts. It allowed the first author to add, change, remove, and specify codes and their descriptions in order to develop the final version of the framework. All other transcripts were coded with the use of this analytical framework (applying the analytical framework). Data was categorized in a framework matrix (charting data into the framework matrix). This process was facilitated by using the NVivo software (R1.6), where an overview of all codes, with corresponding citations, was created. The matrix was discussed and a conclusion for each theme was formulated (interpreting the data).
Positionality and Reflexivity
We incorporated personal, interpersonal, methodological, and contextual reflexivity in our research.42,43 The project was completed by an international and interdisciplinary team of researchers, including a psychologist/sociologist/pedagogist (MP), a master’s student in human movement science (TvR), an occupational therapist (LH), a consultant in rehabilitative medicine (CKS), and biomedical engineers (EL, MOC). The leading author (MP) had significant experience conducting quantitative, qualitative and mixed-methods research projects and was involved in the design of the international randomised control trial, aiming to evaluate the PME intervention.12 The second author (TvR) received training on qualitative research and had no connections with the participants nor prior knowledge about the treatment. Two researchers (LH and CKS) worked with some of the therapists, although neither was involved in the conduct of interviews. The biomedical engineers (EL, MOC) had the initial contact with the participants and provided them with training and support in using the PME system. All team members reflected on the findings from their own professional lenses, which facilitated a richness of perspectives. They also reflected on their positionality and professional perspectives, and considered their potential impact on the generated findings. MP and TvR kept a reflexive journal43 in which they noted their thoughts, feelings, and observations throughout the life of the study. Four team members (MP, TvR, CKS, LH) ensured methodological reflexivity by carefully discussing the meaning of each decision with the research team. We also reflected on the fact that most interviewees were employed in a university hospital of a high-income country and the potential impact of this situation on the findings.
Credibility and Trustworthiness
We considered credibility and trustworthiness criteria to ensure the high quality of the study.44 Reflexivity not only facilitated bracketing of our own subjectivity but also informed specific measures to account for the potential impact of our positionality and perspectives. For example, given the pre-study contact between biomedical engineers (EL, MOC) and the interviewees, the biomedical engineers were not involved in data collection or analysis. The interviewer’s (TvR) outsider perspective facilitated a reduction of potential bias and an impartial perspective.45 Two researchers (MP, TvR) maintained an audit trail, which involved collecting materials and notes (eg, transcripts, data analysis, report drafts) and documenting all decisions.46 Another two researchers (CKS, LH) reviewed the processes. Four team members (MP, TvR, CKS, LH) participated in regular interdisciplinary meetings to discuss all aspects of the research process. Two researchers (MP, TvR) completed the initial analyses and another two (CKS, LH) validated the findings. We used member checking to enhance trustworthiness. We ensured confirmability by providing rich quotes to illustrate the connection between the data, findings, and interpretation.44,47 We enhanced transferability by providing information about respondents and context in which the study was conducted.48 All team members commented on the consecutive draft of the report.
Results
Interviewees described the change that occurred within a complex 3-way interaction between the key actors; a patient, a therapist, and a PME device (see Figure 1). This 3-way interaction was influenced by intrapersonal, interpersonal, and contextual factors, leading to an interplay of effects at different levels of complexity. Four main themes were identified: (1) the Perceived Therapeutic Effects, (2) the Mediating Role of Key Actors and Context, (3) the Therapeutic Relationship as a Transformative Journey, and (4) the Potential of PME and Future Directions (see Table 2). The 3-way interaction was a context for change, representing the interlinkage between innovation and intersubjectivity, and became an overarching construct tying the four themes together. The intersubjectivity reflected the interchange of thought and feelings between patients and therapists, which was mediated by the presence of technology.
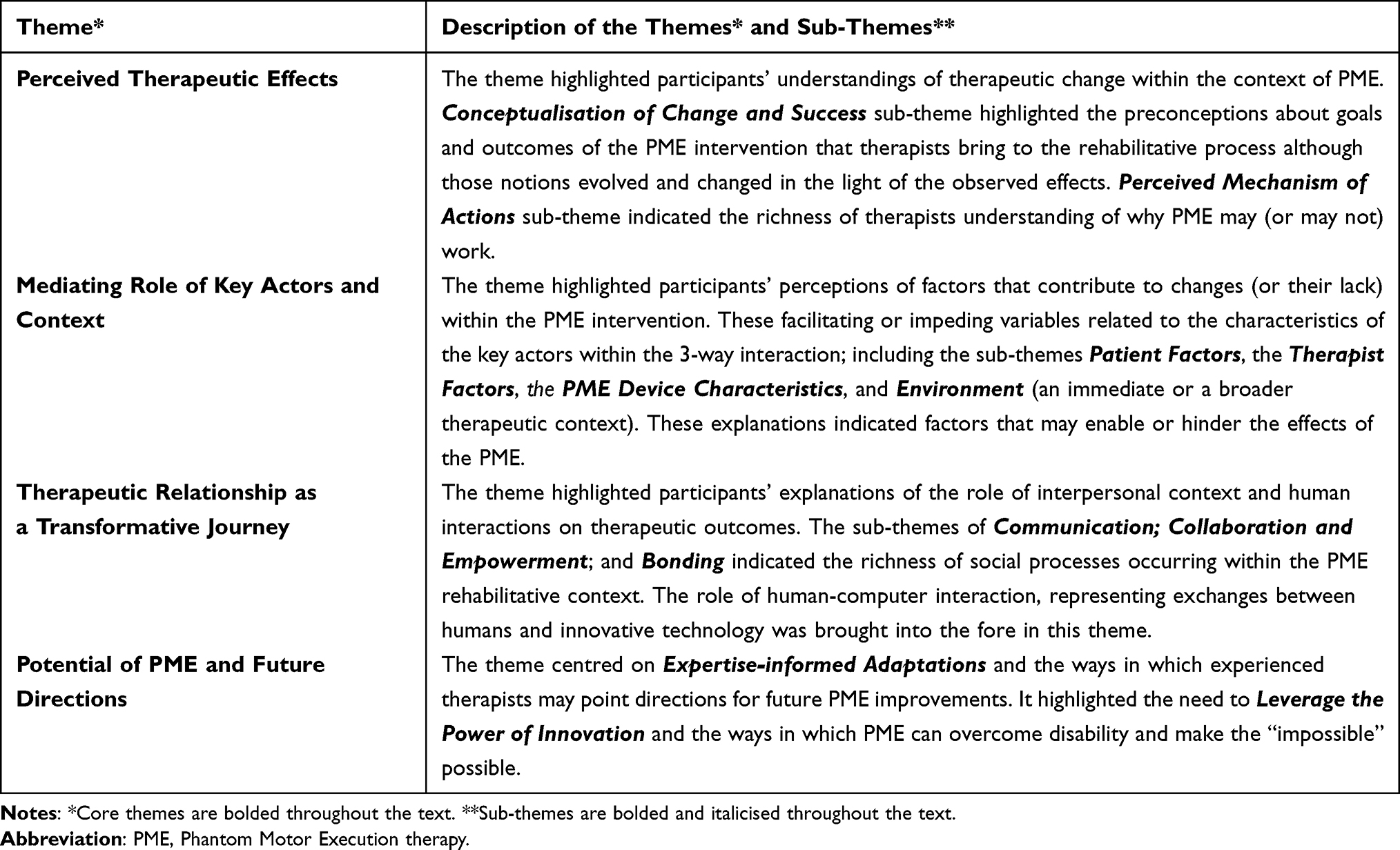 |
Table 2 Therapists Experiences of Providing Phantom Motor Execution Therapy as a Treatment for Phantom Limb Pain. An Overview of Themes and Related Sub-Themes with a Brief Description of Concepts |
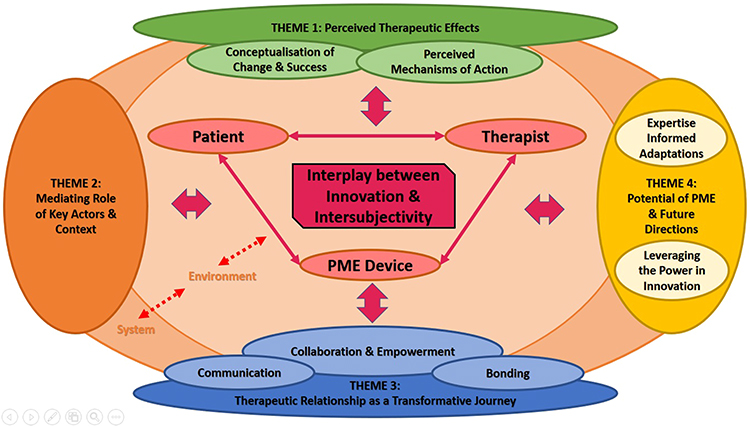 |
Figure 1 Graphical representation of the interplay between innovation and intersubjectivity incorporating four main themes. The overarching theme, Interplay between innovation and inter-subjectivity, is indicated in the red square. The overarching theme is covering the 3-way interaction between the three key actors: the patient, the therapist, and the PME device. Four main themes are indicated in darker ovals, with several sub-themes captured within corresponding light colour ovals. The large dark Orange oval (representing broader socioeconomic systems, including healthcare systems) and the large light Orange oval (indicating environment, including an immediate therapeutic setting and distant patients’ home and/or work contexts) belong to theme 2, but are also connected to all other main themes. |
Theme 1: Perceived Therapeutic Effects
Participants shared their understandings of the potential effects of the rehabilitative system, including outcomes and mechanisms of action, and spoke about incorporating those appreciations and interpretations into the therapeutic context. They talked about Conceptualisations of Change and Success in the context of PME and described therapeutic effects in terms of perceived goals of treatment and their characteristics. Interviewees felt that patients should understand what goals could potentially be achieved with the support of the rehabilitative treatment, but also be aware of its limitations. This served the need to address a tension between the hope that the approach could work and the need to have “realistic expectations” (Interviewee [Int] 5), as “having a realistic goal meant that we were both determined to see it succeed” (Int 4). Although therapists highlighted the need for personalized goals, potentially facilitated by the PME system, standardization of the rehabilitative protocol sometimes posed a challenge to this ideal. It was expressed in their believe that “the programme is leading” the process (Int 2) and there was little room for goals exploration, negotiation, or agreement.
Interviewees considered diverse conceptualisations of a positive change and highlighted the role of alternative effects to pain reduction, especially if the latter was not achieved. For example, re-gaining control over the phantom limb, and the ability to relax it, were indicated as important aims of treatment, with some interviewees considering them as the primary goals of the therapy.
A successful treatment is, when a patient at the end has some kind of feeling of control over the experience and the feeling of their limb and is able to be more connected to the feeling. (Int 5)
Interviewees also saw the ability to change the position of the phantom limb as a positive therapeutic outcome as it facilitated phantom limb relaxation, eg, when it was stuck in a (cramped) position.
Research participants shared their explanations of therapeutic effects and perceived Mechanisms of Action. They referred to cortical reorganization and described it as an important mechanism of action that could influence PLP in the context of PME. They highlighted the role of patients’ insight into the brain-based mechanism and their understanding of “what was happening in their brain” (Int 1) for positive outcomes. They saw their own role in explaining these processes to patients:
[I] told them again and again what was happening and how it worked. In my opinion it was very important to keep telling them again, and again, and again (…), it was never too much. (Int 1)
The role of patients’ beliefs, perceptions, and expectations was described by many therapists. They frequently referred to the concept of “belief in the programme” (Int 1, 2, 3, 4, 8, 10), highlighting that patients’ outcomes could be negatively impacted if either the therapists or patients were sceptical or did not believe in the effectiveness of PME.
[If] the patient wouldn’t believe in the program, then you can have the most high-tech program, and the best therapist, and it wouldn’t work. (Int 8)
This belief was linked to the patients’ hope for pain relief and underlined the willingness to try the treatment as “they already have had several other treatments that didn’t work” (Int 7).
The role of social connectedness was also highlighted. Interviewees indicated that “just talking about their pain helped to improve their pain” (Int 4), as they felt understood and believed. Feeling connected within the therapeutic context facilitated both the patients’ performance and the chances of enhanced understanding.
Theme 2: Mediating Role of Key Actors and Context
Although therapeutic successes were mostly attributed to the effect of the rehabilitative system, the potential impact of patients’ and therapists’ characteristics, as well as the external context were indicated as facilitators or barriers to therapeutic efforts.
According to therapists, the ability to demonstrate and maintain motivation, combined with perseverance and determination, were seen as the strongest Patient Factors. Motivation was also perceived as critical for treatment adherence. The combination of motivational factors and patients’ personal qualities, including friendliness, positivity, open-mindedness, and being down-to-earth, as well as their impact on treatment outcomes are reflected in this statement:
…some people are fully motivated, and they really just go ahead, and they just go despite everything. And you have people that are closed, or they don’t want to open to new things. So, of course it depends on their personality. (Int 10)
Therapists paid attention to characteristics of patients’ cognition, indicating that the need to “place cognitive effort to manage the task” (Int 10), the ability to concentrate, focus attention, and imagine the movements contributed to positive outcomes. Inability to imagine movements was indicated as having a potential negative impact on the patients’ involvement in the therapy, leading to less positive outcomes. Participants also indicated the role of psychological and emotional variables and stated that “patients who presented with depression or other psychological issues” (Int 10) were less likely to benefit from the treatment.
Although PME therapy could technically be delivered by anyone with minimal training, the Therapist Factors, including therapists’ extensive experience of treating patients with amputations and PLP, as well as their ability to apply a variety of therapeutic methods and techniques was seen by interviewees as a prerequisite of good treatment delivery and outcomes. A good understanding of the PME system facilitated the therapists’ ability to explain its goals and provide clear instructions. In the interviewees’ views, their role was to manage complex therapeutic situations and add a human factor to the rehabilitative tasks, including “reassuring them that it’s okay if they don’t do well or you know, so they’re not feeling bad about it” (Int 6). It was expressed in their ability to facilitate, lead, guide, support, motivate, and coach a patient through the therapeutic process; and to keep the task challenging. Participants highlighted multiple aspects of their role during PME treatment, illustrated in this statement:
Well, you are a therapist, teacher, personal trainer, supporter, everything. All in one person. (Int 9)
Interviewees specifically highlighted the importance of instilling sense of trust and comfort in patients, to facilitate patients’ engagement. An important aspect of the therapists’ role was to manage motivational processes, negotiate realistic expectations, avoid making “false promises” (Int 4), and adjust the level of challenge.
The PME Device Characteristics played a significant role in the 3-way interaction. Although therapists had their preferences regarding the different aspects of the system, they tended to agree that “the combination of exercises makes the effect” (Int 7).
Therapists indicated that, given its unique features, the technology can empower both patients and therapists. They specifically pointed to the role of immediate feedback of the phantom limb movement received from the system for achieving therapeutic effects and focusing on the rehabilitative efforts. Interestingly, according to therapists, this real-time feedback also enhanced the therapists’ ability to support a patient, manage patients’ motivation, adjust levels of difficulty, and overcome the traditional challenges, eg in mirror therapy, of not being able to “see” or “know” what patients are “doing in their head” (Int 1).
So, this is a good way for us to be sure that they are doing what we think is going to help them. (Int 4)
According to therapists, Environment could both facilitate and impede therapeutic effects. Patients’ life circumstances, including family and work situation, could be a source of stress and negatively impact on therapeutic outcomes.
(…) sometimes, I just think (…), phantom limb complaints are affected sometimes from the treatment, but I also sometimes think that what’s going on at home (…) (Int 6)
While time commitment was a challenge for both patients and therapists, the time requirements also impacted on patients’ levels of fatigue and negatively influenced their participation. Time required to travel to treatment, or the need to take time off work, negatively influenced daily activities and caused stress, which in turn impacted on patients’ ability to focus within therapy.
Social support was regarded as important, including help and understanding from family and employers, and was frequently lacking. Interviewees pointed to the cumulative impact of multiple barriers on therapeutic effects. As one of the participants stated:
When there are too many difficulties, they won’t succeed. Then, it will influence on their motivation. (Int 2)
Theme 3: Therapeutic Relationship as a Transformative Journey
Interpersonal context and intersubjectivity played an important role in the rehabilitative process. Interviewees highlighted the significance of interactions and the ability to develop a therapeutic alliance, as it facilitated the processes of guiding and coaching patients, supporting the achievement of the goals, translating the observed effects into common language, and helping patients realise that the effect had indeed occurred. They indicated that if “there is this bonding, then it is easier to achieve these movements” (Int 10).
While construed as a mechanism underlying perceived change, therapeutic alliance was sometimes described as a by-product of rehabilitative efforts and the energy created by the observed effects.
I thought it was really special, actually, to see and to experience with the patient if they actually got reduction of the complaints. And they thought, well, I can really move my limb again. And so yeah, that is really valuable, and I think yeah, very useful. (Int 5)
The unique features of the rehabilitative system opened up new opportunities, including its ability to enable, restore, or enhance human experience and function. As such, the technology glued human efforts together, resulting in a “teamwork relationship with the patients” (Int 10), and modulated the nature of therapeutic alliance.
Therapeutic relationship was a platform that facilitated therapeutic change; however, the presence of technology modulated its nature.
I think, with my other treatments as a hand therapist, I find more therapeutic relation than with this treatment. (…) I find my influence not all that big. (…) of course, I have some influence, but I don’t have to think about what is best for this patient. (Int 2)
Communication was important as PME intervention was imbedded in talks, conversations, and verbal and nonverbal instructions. Feedback, professional guidance, and “guiding the patients through verbal instructions” (Int 3) as well as less formal narratives and discourses, became a part of linguistic context that was perceived to drive a positive change.
I give a lot of verbal instructions, because I think it’s easier for them to be guided, especially in the beginning because they don’t know what to do (…) everything is new. I don’t know if verbal instruction is a tool, but I think it is a good strategy. (Int 10)
Collaboration and Empowerment were seen as important social processes underlying positive outcomes. The therapeutic work was described as a “real collaboration” between the three actors. The need to “work together”, and “hand in hand” for the best possible outcomes, was highlighted.
The client and I, as a therapist, are highly motivated to make the treatment work. This gave a good cooperation. (Int 1)
Although therapists described PME in terms of its power to enhance human experience and function, the role of power dynamics within interpersonal context was also acknowledged. Specifically, therapists highlighted that the patients needed to “rely on” the therapists’ skills before they could competently manage the requirements of the programme.
Bonding developed over time and was facilitated by the length of PME therapy, as “the treatment always lasts 2 hours, and we get to know each other a little better” (Int 1). The ability to develop a bond with a patient was attributed to the therapists’ characteristics and their professional training and experience. Bonding was enhanced by the learning and development opportunities within the therapeutic context. Trust building resulted from witnessing and experiencing diverse therapeutic effects.
Theme 4: Potential of PME and Future Directions
Interviewees pointed to the need for technical improvements, environmental adjustments, and equipment requirements.
Have the equipment in a suitable space is important. Now we always had to unpack and repack everything that took a lot of time. A large screen that displays the client well and not extra wide, which is currently the case. (Int 1)
Technical problems were indicated as the key barrier that impeded full participation and prevented patients from benefitting from the planned treatment. Access to technical support was indicated as a necessary ingredient, as the technology was perceived as effective as long as it worked and technical difficulties, including the inability to place electrodes, could be avoided.
Interviewees shared their unique insights and indicated Expertise-informed Adaptations of the rehabilitative system. They named specific rehabilitative solutions, including techniques and strategies that could improve patient outcomes. The most tangible example related to the use of functional tasks and creative ways of incorporating them into the therapeutic process. Interviewees also stressed the importance of verbal and nonverbal instructions, such as describing the movements in different ways, in the context of PME therapy.
I will support patients to think in a functional task when they do something, support them thinking on activity. (Int 4)
As a discrepancy was sometimes observed between the challenge posed by the rehabilitative treatment and patients’ ability to engage in the specific treatment components, therapists thought that the potential of PME treatment should be leveraged by customising it to patients’ needs, preferences, and characteristics. Variability in exercises and their different levels of difficulty were highlighted as important in personalisation. Participants also highlighted that “you have to meet the patients where they want to be met” (Int 10).
Finally, interviewees highlighted that PME treatment had the potential to build on its ability to overcome the limitations of other treatments, eg, mirror therapy, as it enabled bilateral amputees to take part:
We also had bilateral amputees that could do this program and that’s not possible with mirror therapy, you don’t have anything for the mirror. So, for them it was the only option. (Int 9)
However, interviewees highlighted that, in order to become truly inclusive, PME would need to account for individual differences, eg, by adjusting the skin colour of the limb. This inclusive approach, with the system’s ability to flexibly address and adapt to the needs of individual patients, was seen as the biggest strength of PME and interviewees felt that it should inform efforts towards Leveraging the Power of Innovation.
Discussion
The four themes identified in this qualitative study pointed to intrapersonal, interpersonal, and contextual factors that should be considered in future clinical implementations of PME treatment. The findings enriched the understanding of the social processes involved in the application of innovative solutions within rehabilitative contexts.13 Importantly, the explanations of therapeutic outcomes went beyond the biological pathways of change originally conceived for the PME treatment.15 Therapists offered insights into the intricacies of the therapeutic process, including interpersonal and contextual variables, and indicated conditions under which, in their view, the pain reduction might have been more likely to occur. The findings showed how the quality of human exchanges within PME treatment, and an interplay between contributing factors, could facilitate an extended and mutually agreed understanding of a positive therapeutic change (eg, pain reduction was not the only marker of success). Importantly, the study illustrated how the presence of innovation and the variables related to human-computer interactions impacted not only on patients but also on therapists, influencing the ways in which therapeutic goals were achieved within a rehabilitative context. The study also indicated the significance of cognitive variables operating within the interpersonal context of PME; including the role of preconceptions held by therapists, their subjective understandings of the PME, interpretations of goals and outcomes, and explanations for why PME may (or may not) work. The study also showed how experienced and knowledgeable therapists might contribute to leveraging current approaches and inform their future adaptations.
The therapists saw patients’ understanding of the brain structures and functions as the foundation of the intended therapeutic outcomes. They highlighted the need to activate patients’ awareness of bodily systems in order to achieve a positive change. This finding extends the well-established link between health literacy and patient outcomes49 and suggests that increased patients’ insight into the hypothesised mechanism of action may increase patients’ chances of recovery.50 These findings raise cautions against mechanistic involvement of patients in the PME intervention and highlight the role of therapists in providing a tailored education within clinical encounters. Second, the desired effects were also linked to both patients’ and therapists’ beliefs in the effectiveness of the PME system. While the indicated link might be partially explained by the health beliefs models,51 highlighting the impact of the perceived benefit of the intervention and the belief in own capacity to execute behaviours (self-efficacy), the reported focus on patients’ positive expectations also point to the possible placebo effect that might have played a role in the therapeutic context.19,52,53 Third, when justifying the reasons for which PME worked for some patients, but not others, participants suggested the need to consider patients’ cognitive profiles, including attentional processes and motor imagery ability. This finding should be seen in the light of the reports of individual differences in patients’ ability to use motor imagery54 and its impact on patients’ engagement in treatment.55 Specifically, it has been suggested that kinaesthetic and visual modalities, along with imagining movements from first person perspective, are required to provide appropriate stimulation of the somatosensory and motor cortices, which may underlie reversal of maladaptive plasticity following PLP. However, due to individual differences, not all patients are equally able to engage in these activities.56,57 Further research is required to explore the phenomena and shed light on these possible links in the context of PME.
Our findings suggest that, given the length of individual PME sessions (2 hours), and the overall therapy (15 sessions), there is a need to consider and account for the role of social interactions within the PME rehabilitative process.58 This supports existing literature and highlights a positive influence of social connectedness and bonding on therapeutic outcomes.59,60 However, this also extends existing knowledge by indicating that the establishment of a therapeutic alliance is influenced by the presence of the technology and the complex interchange between the three actors (patient, therapist, and the device). Participants perceived the presence of technology as modulating their approach and saw the “restrictive” protocol as limiting their freedom. The therapeutic process was often perceived as pre-determined and led by the PME device. This included agreement on the therapy goals, which is important as goal formation is seen as an important element of a therapeutic alliance formation.20,22 However, the human interactions also seemed to modulate the use of a technology, often re-defining its empowering features. Specifically, being a context for PME intervention, the quality of the human interactions contributed to the quality of the therapeutic outcomes; as this supportive and collaborative interpersonal context enriched the therapeutic process and allowed both therapists and patients to consider alternative and equally important therapeutic effects. The novel rehabilitative context, with all its affordances and opportunities, made the key actors think differently about possibilities and helped them redefine what a good therapeutic outcome could be. Although the additional effects of therapeutic alliance in a rehabilitative context have been reported in the literature,23,61–63 our findings extend these understandings and demonstrate how the presence of a technology can enrich, but also impede, the development of an alliance; including its mediating impact on intervention outcomes.
Although PME has been designed to mainly improve pain experience, participants indicated that it might have more diverse effects, including psychosocial outcomes. For example, regaining control over the phantom was an important alternative goal, and if achieved, it was linked to the sense of satisfaction, relaxation, acceptance, and relief. These findings highlight the need to explore the link between PME and sense of agency and extend the understanding of psychological factors in PLP.5 Importantly, therapists drew on their comprehensive professional training and experience and provided patients with informal support through diverse communication channels, including carefully tailored instructions and nonverbal language. They facilitated patients’ understanding of the changes and engaged them in a positive interpretation of observed outcomes. Importantly, our findings point to the need to consider the content and function of communication between the key actors within the PME intervention, including human-computer interaction, and explore the role of technology in enriching these information, ideas, and feelings exchanges.58 Future research should build on the efforts to link elements of a communication process to improve rehabilitation outcomes,64 as well as explore the role of the language use in the context of interactional trajectories.65
Finally, participants indicated that expertise-informed adaptations should guide revisions of the technological solutions and possible opportunities should be addressed in parallel with the reported technological restrictions and limitations. They saw potential in PME and gave examples of adaptations. The participants described PME in terms of its power to enhance human experience and function, as well as a means of overcoming disability. They highlighted the benefits of PME when working with patients with bilateral amputations, for whom the use of other treatments, eg, mirror therapy, was not possible. Although PME treatment likely increases the sense of agency among patients, similar processes within therapists have been highlighted in this study, highlighting that the use of PME treatment may empower both patients and therapists. Specifically, the therapy was facilitated by the feedback received from the PME system, which not only gave the providers insight into “invisible” processes and aspects of patients’ activity but also formed grounds for more interpersonal encounters within the clinical context. Importantly, our findings indicate that therapists played a pivotal role in the delivery of the PME intervention as they provided necessary guidance and helped patients navigate through the complex intervention. The therapists’ efforts were seen as particularly important when change in the primary outcome (pain perception) was not noticed but alternative benefits (eg, movement control) were strikingly present. Although PME treatment has been delivered at home, with patients demonstrating capability to be engaged in the self-treatment PME mode,66 the findings of this study support the conclusion that the positive effects of a home-based approach may need to build on the initial clinic-based encounters. Therefore, a proper balance of clinical and in-home treatment has yet to be established.66
Strengths and Limitations
The findings should be seen in the light of their strengths and limitations. This study shed light on the ways in which a novel therapeutic tool may have influenced both human interactions and outcomes within a rehabilitative context. Although any attempt to transfer the findings to other technology-supported rehabilitative treatments requires caution, the findings may inform the design and implementation of similar therapeutic approaches in real-life settings. However, therapists represent only one perspective and the exploration of patients’, informal caregivers’, healthcare service managers’, economists’, or policymakers’ perspectives might have shed light on factors not identified in this study. It is also important to acknowledge that interviews were conducted in English (not a native language for most participants) and through video conversations. Although these measures facilitated participation and exploration of therapists’ views from across international sites, they might have influenced the interview flow and limited the richness of conversations. Also, all participants were females and male participants’ perspectives might have enriched the understanding of the explored phenomena. Moreover, given that PME is at the evaluation stage of its development, all of the included participants delivered the intervention as part of the RCT.12 It means that they also have the experience of delivering PMI intervention within a control group. Although they were asked to focus on the PME treatment when reporting experiences, their perspectives were likely formed with reference to the PMI treatment. Finally, we conducted most interviewees in university hospitals of high-income countries; therefore, potential mechanisms of action identified in this study apply only to these types of settings.
Research and Clinical Implications
Future research, following approaches taken elsewhere,67,68 should employ collective intelligence methodologies and take an interdisciplinary approach to leverage the power of PME treatment. The findings of this study indicate the need to explore the indicated factors further in the context of PME and with the aim of optimising patient outcomes, including accounting for individual differences and unique patients’ needs. As this study demonstrated a potential impact of an interpersonal context on rehabilitative outcomes, future implementation efforts should build on these learnings. The co-production efforts, underpinned by true collaborative efforts between the key stakeholders (eg, patients, therapists, family members, service managers, policy makers, technology designers); and as per published recommendations,69,70 should inform future innovative steps. A series of experimental studies should be conducted to investigate the link between patients’ cognitive profiles, including attentional processes and motor imagery ability, and therapeutic outcomes. Observational approaches, including the analyses of recorded patient-therapists’ interactions, may provide insight into the potential impact of language and nonverbal communications (including the use of body language when providing instructions) on therapeutic outcomes and inform future approaches. The insights from those studies might guide the design of quantitative studies aiming to investigate the modulating role of contextual factors on pain experience. This could be particularly important in the light of patients’ wishes for home treatment, where the therapeutic interaction and bonding cannot be exploited to the full extent, compared to a clinical treatment. Given the richness of informal therapist-patient exchanges, and their potential impact on therapeutic outcomes, future PME evaluations should take a systematic approach to measuring intervention implementation fidelity.71,72
Conclusions
The biopsychosocial model of pain14 should be considered when designing, evaluating, and implementing technology-supported interventions. There is a need to account for the impact of therapeutic alliance and other interpersonal processes on patient outcomes within technology- supported interventions.13 The possible bidirectional links between therapeutic alliance and technology, and the impact of innovation on human exchanges, require further exploration. As therapists have unique insights and play a crucial role in facilitating PME treatment, future home-based treatments should build on initial patient-therapist interactions.
Acknowledgments
We thank all the therapists who took part in this study.
Disclosure
Professor Max Ortiz-Catalan reports grants from Promobilia Foundation, grants from IngaBritt och Arne Lundbergs Forskningsstiftelse, grants from Swedish Research Council, Consultancy fees from Integrum AB, during the conduct of the study; Consultancy fees from Integrum AB, outside the submitted work; In addition, Professor Max Ortiz-Catalan is an author of the patent but do not own it: EP3082591A4. MOC has consulted for the company that provided the devices used in the PME therapy. The authors declare no other conflicts of interest.
References
1. Limakatso K, Bedwell GJ, Madden VJ, Parker R. The prevalence and risk factors for phantom limb pain in people with amputations: a systematic review and meta-analysis. PLoS One. 2020;15(10 October):1–21. doi:10.1371/journal.pone.0240431
2. Kuffler DP. Coping with phantom limb pain. Mol Neurobiol. 2018;55(1):70–84. doi:10.1007/s12035-017-0718-9
3. Erlenwein J, Diers M, Ernst J, Schulz F, Petzke F. Clinical updates on phantom limb pain. PAIN Reports. 2021;6(1):e888. doi:10.1097/pr9.0000000000000888
4. Di Pino G, Piombino V, Carassiti M, Ortiz-Catalan M. Neurophysiological models of phantom limb pain: what can be learnt. Minerva Anestesiol. 2021;87(4):481–487. doi:10.23736/S0375-9393.20.15067-3
5. Fuchs X, Flor H, Bekrater-Bodmann R. Psychological factors associated with phantom limb pain: a review of recent findings. Pain Res Manag. 2018;2018. doi:10.1155/2018/5080123
6. Limakatso K, Parker R. Treatment Recommendations for Phantom Limb Pain in People with Amputations: an Expert Consensus Delphi Study. PM R. 2021;13(11):1216–1226. doi:10.1002/pmrj.12556
7. Batsford S, Ryan CG, Martin DJ. Non-pharmacological conservative therapy for phantom limb pain: a systematic review of randomized controlled trials. Physiother Theory Pract. 2017;33(3):173–183.
8. Collins KL, Russell HG, Schumacher PJ, et al. A review of current theories and treatments for phantom limb pain. J Clin Invest. 2018;128(6):2168–2176.
9. Matthie NS, Giordano NA, Jenerette CM, et al. Use and efficacy of virtual, augmented, or mixed reality technology for chronic pain: a systematic review. Pain Manag. 2022;12(7):859–878. doi:10.2217/pmt-2022-0030
10. Ortiz-Catalan M, Sander N, Kristoffersen M, Håkansson B, Brånemark R. Treatment of phantom limb pain (PLP) based on augmented reality and gaming controlled by myoelectric pattern recognition: a case study of a chronic PLP patient. Front Neurosci. 2014;8(8 FEB):1–7. doi:10.3389/fnins.2014.00024
11. Ortiz-Catalan M, Guðmundsdóttir R, Kristoffersen M, et al. Phantom motor execution facilitated by machine learning and augmented reality as treatment for phantom limb pain: a single group, clinical trial in patients with chronic intractable phantom limb pain. Lancet. 2016;6736(16):56.
12. Lendaro E, Hermansson L, Burger H, et al. Phantom motor execution as a treatment for phantom limb pain: protocol of an international, double-blind, randomised controlled clinical trial. BMJ Open. 2018;8(7):e021039.
13. Vervoort T, Trost Z. Examining Affective-Motivational Dynamics and Behavioral Implications Within The Interpersonal Context of Pain. J Pain. 2017;18(10):1174–1183. doi:10.1016/j.jpain.2017.03.010
14. Adams LM, Turk DC. Central sensitization and the biopsychosocial approach to understanding pain. J Appl Biobehav Res. 2018;23(2):1–19. doi:10.1111/jabr.12125
15. Ortiz-Catalan M. The Stochastic Entanglement and Phantom Motor Execution Hypotheses: a Theoretical Framework for the Origin and Treatment of Phantom Limb Pain. Front Neurol. 2018;9(1–16):65.
16. Simon AM, Hargrove LJ, Lock BA, Kuiken TA. The Target Achievement Control Test: evaluating real-time myoelectric pattern recognition control of a multifunctional upper-limb prosthesis. J Rehabil Res Dev. 2012;23(1):1–7.
17. Ramachandran VS, Rogers-Ramachandran D. Synaesthesia in Phantom Limbs Induced with Mirrors. Proc R Soc B Biol Sci. 1996;263(1369):377–386. doi:10.1098/rspb.1996.0058
18. Pilch M, O’Hora D, Jennings C, et al. Perspective-taking influences attentional deployment towards facial expressions of pain: an eye-tracking study. Pain. 2020;161(6):1286–1296.
19. Testa M, Rossettini G. Enhance placebo, avoid nocebo: how contextual factors affect physiotherapy outcomes. Man Ther. 2016;24:65–74.
20. Bordin ES. The generalizability of the psychoanalytic concept of the working alliance. Psychother Theory, Res Pract. 1979;16(3):252–260. doi:10.1016/B978-0-12-809324-5.05450-X
21. Ardito RB, Rabellino D. Therapeutic alliance and outcome of psychotherapy: historical excursus, measurements, and prospects for research. Front Psychol. 2011;2(3):270. doi:10.3389/fpsyg.2011.00270
22. Hall AM, Ferreira PH, Maher CG, Latimer J, Ferreira ML. The influence of the therapist-patient relationship on treatment outcome in physical rehabilitation: a systematic review. Phys Ther. 2010;90(8):1099–1110. doi:10.2522/ptj.20090245
23. Taylor RR, Lee SW, Kielhofner G. Practitioners’ use of interpersonal modes within the therapeutic relationship: results from a nationwide study. OTJR Occup Particip Heal. 2011;31(1):6–14. doi:10.3928/15394492-20100521-02
24. Balcombe L, De Leo D. Human-Computer Interaction in Digital Mental Health. Informatics. 2022;9(1). doi:10.3390/informatics9010014
25. D’Alfonso S, Lederman R, Bucci S, Berry K. The digital therapeutic alliance and human-computer interaction. JMIR Ment Heal. 2020;7(12):e21895. doi:10.2196/21895
26. Lederman R, D’Alfonso S. The digital therapeutic alliance: prospects and considerations. JMIR Ment Heal. 2021;8(7):e31385. doi:10.2196/31385
27. Lopez A, Schwenk S, Schneck CD, Griffin RJ, Mishkind MC. Technology-Based Mental Health Treatment and the Impact on the Therapeutic Alliance. Curr Psychiatry Rep. 2019;21(8):1–7. doi:10.1007/s11920-019-1055-7
28. Richards P, Simpson S, Bastiampillai T, Pietrabissa G, Castelnuovo G. The impact of technology on therapeutic alliance and engagement in psychotherapy: the therapist’s perspective. Clin Psychol. 2018;22(2):171–181. doi:10.1111/cp.12102
29. Wehmann E, Köhnen M, Härter M, Liebherz S. Therapeutic alliance in technology-based interventions for the treatment of depression: systematic review. J Med Internet Res. 2020;22(6):e17195. doi:10.2196/17195
30. Skivington K, Matthews L, Simpson SA, et al. A new framework for developing and evaluating complex interventions: update of Medical Research Council guidance. BMJ. 2021;374(2018):1–11. doi:10.1136/bmj.n2061
31. Burbank PM, Martins DC. Symbolic interactionism and critical perspective: divergent or synergistic?: original article. Nurs Philos. 2010;11(1):25–41. doi:10.1111/j.1466-769X.2009.00421.x
32. Scotland J. Exploring the philosophical underpinnings of research: relating ontology and epistemology to the methodology and methods of the scientific, interpretive, and critical research paradigms. English Lang Teach. 2012;5(9):9–16. doi:10.5539/elt.v5n9p9
33. O’Brien BC, Harris IB, Beckman TJ, Reed DA, Cook DA. Standards for reporting qualitative research: a synthesis of recommendations. Int J Med. 2014;89(9):1245–1251.
34. Morse JM. The significance of saturation. Qual Health Res. 1995;5(2):147–149.
35. Morse JM. Determining Sample Size. Qual Health Res. 2000;10(1):3–5. doi:10.1177/104973200129118183
36. Hennink M, Kaiser BN. Sample sizes for saturation in qualitative research: a systematic review of empirical tests. Soc Sci Med. 2022;292:114523. doi:10.1016/j.socscimed.2021.114523
37. Hennink MM, Kaiser BN, Marconi VC. Code Saturation Versus Meaning Saturation: how Many Interviews Are Enough? Qual Health Res. 2017;27(4):591–608. doi:10.1177/1049732316665344
38. Furber C. Framework analysis: a method for analysing qualitative data. Afr J Midwifery Womens Health. 2010;4(2):97–100. doi:10.12968/ajmw.2010.4.2.47612
39. Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. Med Res Methodol. 2013;13(117):1–8.
40. Collaço N, Wagland R, Alexis O, Gavin A, Glaser A, Watson EK. Using the Framework Method for the Analysis of Qualitative Dyadic Data in Health Research. Qual Health Res. 2021;31(8):1555–1564. doi:10.1177/10497323211011599
41. Frazer I, Orr C, Thielking M. Applying the framework method to qualitative psychological research: methodological overview and worked example. Qual Psychol. 2022;10(1):44–59. doi:10.1037/qup0000238
42. Olmos-Vega FM, Stalmeijer RE, Varpio L, Kahlke R. A practical guide to reflexivity in qualitative research: AMEE Guide No. 149. Med Teach. 2023;45(3):241–251. doi:10.1080/0142159X.2022.2057287
43. Mantzoukas S. The inclusion of bias in reflective and reflexive research: a necessary prerequisite for securing validity. J Res Nurs. 2005;10(3):279–295. doi:10.1177/174498710501000305
44. Cope DG. Methods and meanings: credibility and trustworthiness of qualitative research. Oncol Nurs Forum. 2014;41(1). doi:10.7748/nr2009.07.16.4.40.c7160
45. Darwin Holmes AG. Researcher Positionality - A Consideration of Its Influence and Place in Qualitative Research - A New Researcher Guide. Shanlax Int J Educ. 2020;8(4):1–10. doi:10.34293/education.v8i4.3232
46. Ryan-Nicholls KD, Will CI. Rigour in qualitative research: mechanisms for control. Nurse Res. 2009;16(3):70–85. doi:10.7748/nr2009.04.16.3.70.c6947
47. Tobin GA, Begley CM. Methodological rigour within a qualitative framework. J Adv Nurs. 2004;48(4):388–396. doi:10.1111/j.1365-2648.2004.03207.x
48. Houghton C, Casey D, Shaw D, Murphy K. Rigour in qualitative case-study research. Nurse Res. 2013;20(4):12–17. doi:10.7748/nr2013.03.20.4.12.e326
49. Yin HS, Jay M, Maness L, Zabar S, Kalet A. Health Literacy: an Educationally Sensitive Patient Outcome. J Gen Intern Med. 2015;30(9):1363–1368. doi:10.1007/s11606-015-3329-z
50. Grol R, Wensing M, Eccles M, Davis D, ed. Improving Patient Care: The Implementation of Change in Health Care. John Wiley & Sons; 2013.
51. Orji R, Vassileva J, Mandryk R. Towards an effective health interventions design: an extension of the health belief model. Online J Public Health Inform. 2012;4(3).
52. Price DD, Finniss DG, Benedetti F. A comprehensive review of the placebo effect: recent advances and current thought. Annu Rev Psychol. 2008;59:565–590. doi:10.1146/annurev.psych.59.113006.095941
53. Rief W, Hofmann SG, Nestoriuc Y. The Power of Expectation - Understanding the Placebo and Nocebo Phenomenon. Soc Personal Psychol Compass. 2008;2(4):1624–1637. doi:10.1111/j.1751-9004.2008.00121.x
54. Richardson A. Individual Differences in Imaging: Their Measurement, Origins, and Consequences. Routledge; 2020.
55. Mercier CSA. Training with virtual visual feedback to alleviate phantom limb pain. Neurorehabil Neural Repair. 2009;23(6):587–594.
56. McAvinue LP, Robertson IH. Measuring motor imagery ability: a review. Eur J Cogn Psychol. 2008;20(2):232–251. doi:10.1080/09541440701394624
57. Mcavinue LP, Robertson IH. Individual differences in response to phantom limb movement therapy. Disabil Rehabil. 2011;33(22–23):2186–2195.
58. Oliveira VC, Ferreira ML, Pinto RZ, Filho RF, Refshauge K, Ferreira PH. Effectiveness of Training Clinicians’ Communication Skills on Patients’ Clinical Outcomes: a Systematic Review. J Manipulative Physiol Ther. 2015;38(8):601–616. doi:10.1016/j.jmpt.2015.08.002
59. Ferreira PH, Ferreira ML, Maher CG, Refshauge KM, Latimer J, Adams RD. The therapeutic alliance between clinicians and patients predicts outcome in chronic low back pain. Phys Ther. 2013;93(4):470–478. doi:10.2522/ptj.20120137
60. Fuentes J, Armijo-Olivo S, Funabashi M, et al. Enhanced therapeutic alliance modulates pain intensity and muscle pain sensitivity in patients with chronic low back pain: an experimental controlled study. Phys Ther. 2014;94(4):477–489. doi:10.2522/ptj.20130118
61. Taylor RR, Lee SW, Kielhofner G, Ketkar M. Therapeutic use of self: a nationwide survey of Practitioners’ attitudes and experiences. Am J Occup Ther. 2009;63(2):198–207. doi:10.5014/ajot.63.2.198
62. Babatunde F, MacDermid J, MacIntyre N. Characteristics of therapeutic alliance in musculoskeletal physiotherapy and occupational therapy practice: a scoping review of the literature. BMC Health Serv Res. 2017;17(1). doi:10.1186/s12913-017-2311-3
63. Nienhuis JB, Owen J, Valentine JC, et al. Therapeutic alliance, empathy, and genuineness in individual adult psychotherapy: a meta-analytic review. Psychother Res. 2018;28(4):593–605. doi:10.1080/10503307.2016.1204023
64. Jesus TS, Silva IL. Toward an evidence-based patient-provider communication in rehabilitation: linking communication elements to better rehabilitation outcomes. Clin Rehabil. 2016;30(4):315–328. doi:10.1177/0269215515585133
65. Wilson D, Williams M, Butler D. Language and the pain experience. Physiother Res Int. 2009;14(1):56–65. doi:10.1002/pri
66. Lendaro E, Middleton A, Brown S, Ortiz-Catalan M. Out of the clinic, into the home: the in-home use of phantom motor execution aided by machine learning and augmented reality for the treatment of phantom limb pain. J Pain Res. 2020;13:195–209. doi:10.2147/JPR.S220160
67. Hanlon M, Hogan M, Durand H, et al. Designing an e-learning tool to support health practitioners caring for patients taking multiple medications. HRB Open Res. 2021;3:59. doi:10.12688/hrbopenres.13110.2
68. Ma J, Hogan MJ, Eyre ELJ, Lander N, Barnett LM, Duncan MJ. Enhancing the implementation and sustainability of fundamental movement skill interventions in the UK and Ireland: lessons from collective intelligence engagement with stakeholders. Int J Behav Nutr Phys Act. 2021;18(1):1–18. doi:10.1186/s12966-021-01214-8
69. Palmer VJ, Weavell W, Callander R, et al. The Participatory Zeitgeist: an explanatory theoretical model of change in an era of coproduction and codesign in healthcare improvement. Med Humanit. 2019;45(3):247–257. doi:10.1136/medhum-2017-011398
70. Ward ME, De BA, Beirne D, et al. Using co-design to develop a collective leadership intervention for healthcare teams to improve safety culture. Int J Environ Res Public Health. 2018;15(6):1–17. doi:10.3390/ijerph15061182
71. Carroll C, Patterson M, Wood S, Booth A, Rick J, Balain S. A conceptual framework for implementation fidelity. Implement Sci. 2007;2(1):1–9. doi:10.1186/1748-5908-2-40
72. Toomey E, Hardeman W, Hankonen N, et al. Focusing on fidelity: narrative review and recommendations for improving intervention fidelity within trials of health behaviour change interventions. Heal Psychol Behav Med. 2020;8(1):132–151. doi:10.1080/21642850.2020.1738935
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Non-Surgical and Rehabilitative Interventions in Patients with Frozen Shoulder: Umbrella Review of Systematic Reviews
de Sire A, Agostini F, Bernetti A, Mangone M, Ruggiero M, Dinatale S, Chiappetta A, Paoloni M, Ammendolia A, Paolucci T
Journal of Pain Research 2022, 15:2449-2464
Published Date: 19 August 2022
Veteran Perspectives on Phantom Limb Pain and Non-Drug Interventions
Rich TL, Phelan HL, Gravely AA, Falbo KJ, Finn JA, Matsumoto ME, Muschler KJ, Olney CM, Kiecker JE, Hansen AH
Journal of Pain Research 2023, 16:1391-1400
Published Date: 25 April 2023
The Importance of the Diaphragm in Neuromotor Function in the Patient with Chronic Obstructive Pulmonary Disease
Bordoni B, Escher A, Compalati E, Mapelli L, Toccafondi A
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:837-848
Published Date: 11 May 2023
A Systematic Review and Meta-Analysis of the Effects of Rehabilitation Using Digital Healthcare on Musculoskeletal Pain and Quality of Life
Jang S, Lee B, Lee E, Kim J, Lee JI, Lim JY, Hwang JH, Jang S
Journal of Pain Research 2023, 16:1877-1894
Published Date: 31 May 2023
Factors in Surgical Placement and System Design to Reduce Pocket Awareness and Optimize the User Experience of Spinal Cord Stimulators – A Comprehensive Review
Gish B, Al-Asadi Z, Tisler AT, Mata R, Chopra H, Garcia RA, Schatman ME, Tieppo Francio V, AlFarra T, Bracero L, Karcz M, Robinson CL, Shah A, Moreira A, Sciascia AD, Deer T
Journal of Pain Research 2025, 18:6749-6768
Published Date: 14 December 2025