Back to Journals » Patient Preference and Adherence » Volume 20
Factors Associated with Treatment Adherence in People with Both Hypertension and Pre-Diabetes: A Cross-Sectional Study in a Semi-Rural Community in Thailand
Authors Chomchoo N, Maneesriwongul W ![]() , Chaladthanyagid K
, Chaladthanyagid K ![]() , Keawpugdee J
, Keawpugdee J ![]()
Received 11 December 2025
Accepted for publication 29 April 2026
Published 29 May 2026 Volume 2026:20 583856
DOI https://doi.org/10.2147/PPA.S583856
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Dr Ramón Morillo-Verdugo
Nutchayaporn Chomchoo, Wantana Maneesriwongul, Karn Chaladthanyagid, Jantra Keawpugdee
Ramathibodi School of Nursing, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Wantana Maneesriwongul, Ramathibodi School of Nursing, Faculty of Medicine Ramathibodi Hospital, Mahidol University, 270 Rama VI Road, Thung Phaya Thai, Ratchathewi, Bangkok, 10400, Thailand, Email [email protected]
Purpose: Hypertension (HTN) combined with prediabetes (pre-DM) has become an important public health concern worldwide. Patients need to adhere to both pharmacological and non-pharmacological treatments in order to regulate both blood pressure and blood glucose levels and reduce the risk of serious complications. This study examined factors associated with treatment adherence in people with both HTN and pre-DM.
Methods: A cross-sectional study was conducted between January and March 2025. A sample of 275 people with both HTN and pre-DM was recruited from 11 subdistrict health-promoting hospitals (HPHs) in Sai Noi, a semi-rural district in Nonthaburi Province, Thailand. Data were collected using structured questionnaires. Multiple regression analysis was used to examine factors associated with treatment adherence.
Results: It was revealed that female sex, knowledge about HTN and pre-DM/T2DM, social support, patient–provider relationship, convenience of traveling to health services, and convenience in using these services were significantly positively correlated with adherence to treatment. Meanwhile, experience of medication side effects, smoking, and alcohol consumption were negatively correlated with it. The multiple regression model was statistically significant in predicting treatment adherence (F = 11.36 (5, 269), p < 0.001) and included overall support from family (B = 2.23, p < 0.001), smoking (B = − 132.61, p < 0.001), experience of medication side effects (B = − 89.51, p = 0.004), knowledge of pre-DM/T2DM (B = 14.67, p = 0.013), and patient–provider relationship (B = 2.23, p = 0.033) as significant factors.
Conclusion: Disease–related knowledge, support from family, and patient–provider relationship positively influence treatment adherence of people with both HTN and pre-DM, while side effects of medication and smoking negatively influence it. These findings provide valuable insights for health officials that could inform future intervention and management strategies for this dual-risk population.
Keywords: treatment adherence, knowledge, social support, patient–provider relationship, side effects, smoking, pre-DM
Introduction
Prediabetes (pre-DM), also known as impaired glucose tolerance, has become an important public health concern. According to the International Diabetes Federation (IDF), the worldwide prevalence of pre-DM rose from 318 million (6.7%) in 20151 to 541 million (10.6%) in 2021,2 while the prevalence in low-and middle-income countries (LMICs) was higher at 13.1%.3 A clinical review reported that pre-DM significantly increases the likelihood of developing type 2 diabetes mellitus (T2DM) with progression rates of 10% annually,4 and a meta-analysis of 103 prospective cohort studies reported up to 50% progression within 5 years.5 In addition, a large prospective cohort study of adults ≥18 years in the US showed that the prevalence of pre-DM combined with hypertension (HTN) was 14.7% (5,011/34,047).6 Evidence from several prospective cohort studies has also indicated that combined pre-DM/T2DM and HTN, known as “dual risk,” is linked to an increased risk of cardiovascular disease (CVD).7–9 A prospective cohort study in China (N=4,193) also reported that CVD risk was significantly elevated in patients with pre-DM plus HTN and T2DM plus HTN compared with that in a reference group.7 Moreover, compared with HTN alone, combined pre-DM and HTN was significantly associated with all-cause and cardiovascular mortality, with higher hazard ratios.6,9 Against this background, HTN and T2DM are known as leading modifiable risk factors for CVD and death.10–13
In the context of dual-risk patients with HTN and pre-DM, adherence to treatment is a crucial determinant of the extent to which both blood pressure and blood glucose levels are regulated. Adherence to treatment can reduce the risk of serious health complications14–16 and lower healthcare expenditures.17 According to the World Health Organization (WHO), adherence is defined as “The extent to which a person’s behavior – taking medication, following a diet, executing lifestyle changes – follows medical advice.” Adherence has also been defined as “The extent to which patient behavior corresponds with recommendations from a healthcare provider” (p.136).14 However, poor adherence to long-term treatment of chronic diseases is a striking problem worldwide, making adherence improvement a priority of the public health agenda. The most common barrier to treatment adherence is the lack of perceived immediate benefit, particularly in people with asymptomatic or chronic conditions.14 A systematic review of 10 studies from 6 countries (N = 3,218) on adherence to antihypertensive medication reported that the rate of adherence ranged widely from 8.9% to 96.8%.18 Another systematic review of 27 studies from 12 countries (N = 463,711) on adherence to T2DM medication reported adherence rates of 38.5% to 93.1%.19 In addition to pharmacological treatment, non-pharmacological treatment involving lifestyle modifications/long-term behavioral changes is essential for people with HTN20 and pre-DM,17 particularly those with both.
The clinical guidelines for the management of individuals with pre-DM by the American Diabetes Association Professional Practice Committee21 recommend combining metformin therapy with lifestyle modifications to manage pre-DM and delay or prevent its progression to T2DM, particularly for high-risk individuals. However, pharmacological uptake was limited, particularly in LMICs with resource-constrained health systems.21 Similarly, pharmacological interventions for this group remain limited in Thailand. The Thai clinical practice guidelines for diabetes primarily emphasize lifestyle modification for individuals with pre-DM.22 The use of T2DM medications for individuals with pre-DM is considered on a case-by-case basis at the physician’s discretion.22 For individuals with both HTN and pre-DM attending a non-communicable disease (NCD) clinic at the subdistrict health-promoting hospitals (HPHs), the prescribed pharmacological treatment generally focuses on controlling blood pressure, but not blood sugar, while the management of pre-DM focuses on non-pharmacological behavioral modification.22 Therefore, patients are required to adhere to treatment emphasizing lifestyle modifications/long-term behavioral changes, including a healthy diet, regular physical activity, appropriate weight management, stress management, and avoidance of risk behaviors (such as smoking and alcohol consumption). Good treatment adherence to these recommendations can help regulate blood pressure23 and blood glucose levels,24 thereby reducing the risk of developing associated complications.
In Thailand, the sixth National Health Examination Survey of individuals aged 15 years or older reported that the prevalence of HTN, T2DM, and pre-DM was 25.4%, 9.5%, and 10.7%, respectively.25 According to the Thai Health Data Center of Nonthaburi, a province neighboring Bangkok, the incidence of HTN per 100,000 population there increased from 806.45 in 2022 to 937.74 in 2023 and to 1,033.93 in 2024, while the corresponding figures for T2DM were 423.64, 461.00, and 517.89. A report based on health screenings also revealed an increase in pre-DM rates in Nonthaburi Province, from 3.95% (5,123/129,417) in 2023 to 6.87% (6,202/90,204) in 2024. Notably, Sai Noi District, the northwesternmost semi-rural district of Nonthaburi, reported the highest rate of pre-DM cases in the province, with an increase in pre-DM from 8.74% (1,285/14,699) in 2023 to 10.14% (1,254/12,396) in 2024.26
Although Sai Noi is located near Bangkok, many of its residents have a lifestyle that more closely resembles that of rural populations rather than urban ones, and much of the community is directly involved in agriculture (eg, farming and fruit gardening) Despite urbanization having developed more slowly in Sai Noi than in other districts in Nonthaburi, the area of its farmland, predominantly in the form of smallholdings, has decreased by one-third over the last two decades. Recently, Sai Noi has also experienced a demographic transition, with the proportion of older people increasing from 18% to 23% between 2022 and 2025.26 These changes, along with the associated aging of the agricultural workforce, could have led people to change their occupations and lifestyles in ways that may increase the prevalence of age-associated chronic conditions such as HTN, T2DM as well as pre-DM. Similar changes have been reported in other rural areas in LMICs.27
To the best of our knowledge, no study has focused on treatment adherence (medication and lifestyle) among people with both HTN and pre-DM in Thailand, particularly at subdistrict HPHs. This study was thus conducted to examine factors associated with treatment adherence in people with both HTN and pre-DM at the subdistrict HPHs in Sai Noi District, Nonthaburi. The findings should be beneficial for health officials in providing a better understanding of treatment adherence and its related factors in people with both HTN and pre-DM.
In accordance with the WHO’s adherence model,14 treatment adherence is defined as the extent to which a patient’s behavior, including taking medication and implementing recommended lifestyle modifications such as a healthy diet and physical activity, corresponds with mutually agreed recommendations from a healthcare provider. This definition complies with a patient-centered perspective that emphasizes collaborative decision-making and mutual agreement rather than passive compliance. Within this framework, patients are viewed as active participants in caring for their health, particularly in the long-term management of chronic conditions.14
Guided by the WHO’s adherence model,14 this study categorized variables into five domains: patient-related, disease-related, treatment-related, healthcare provider-related, and healthcare system-related factors. Although social and economic factors are identified as a separate dimension in the WHO’s adherence model, this study operationalized individual-level social and economic characteristics (eg., education, income, and social support) under patient–related factors.28 Conceptualizing treatment adherence as a dependent behavioral variable enables the examination of multiple factors that potentially influence it. In this study, treatment adherence covers both pharmacological treatment and non-pharmacological interventions, including behavioral and lifestyle modifications.
Materials and Methods
Study Design and Settings
A cross-sectional study was conducted between January 2025 and March 2025 at 11 subdistrict HPHs in Sai Noi District, Nonthaburi Province, Thailand. Sai Noi is one of the six districts of Nonthaburi Province bordering Bangkok. In Thailand, the district health system is an integrated network providing decentralized primary care at subdistrict HPHs close to people’s homes and coordinated secondary and tertiary care with the district hospitals and the provincial hospital.29 In Sai Noi, there are 11 subdistrict HPHs serving 76,440 people. In addition to primary care, an extended NCD clinic is scheduled at each HPH at least once a month. Patients with NCDs (eg, diabetes, hypertension, hyperlipidemia) have scheduled follow-up visits with a doctor every 1 to 3 months, depending on their medical condition People with both HTN and pre-DM undergo annual blood chemistry monitoring, which includes a test of fasting blood sugar (HbA1c testing is provided only for people with T2DM undergo annual blood chemistry monitoring).
Study Sample
A convenience sample of 275 people with both HTN and pre-DM attending the NCD clinic at 11 subdistrict HPHs in Sai Noi District was recruited to participate in this study. The inclusion criteria were as follows: (1) aged 35 years or older, (2) a diagnosis of HTN and being prescribed antihypertensive medication for more than 3 months, (3) blood sugar level (FBS/DTX) of 100–125 mg/dL, (4) able to communicate in Thai, and (5) willingness to participate in this study. Patients were excluded if their Mini-Cog score was ≤ 3.30
For sample size estimation, a power analysis for linear multiple regression was conducted using G*power (version 3.1.9.7). A fixed model with R2 deviation from zero was specified, with an alpha level of 0.05, statistical power of 0.90, a medium effect size (ƒ2=0.15) as defined by Cohen,31 and 30 predictors. The minimum required sample size was 226. This was increased to 272 to account for an anticipated 20% of incomplete or missing data. Thus, 25 participants were recruited from each HPH (25 × 11 HPHs = 275).
Instruments
The structured questionnaires used in this study included measures of Background characteristics, Treatment adherence, Knowledge about hypertension and pre-diabetes/diabetes (HTN and pre-DM/T2DM), Social support, Disease–related information, Treatment–related information, Healthcare provider–related information, Patient–provider relationship, and Healthcare system–related information. Content validity of the questionnaires was determined by three experts (two faculty members specializing in adult nursing and nutrition, and an advanced practice nurse specializing in diabetic care). The scale content validity index (S-CVI) of these instruments ranged from 0.91 to 1, indicating good content validity, with high item relevance and good coverage of the construct domain. Prior to data collection, a pilot study was conducted among 30 participants to test the internal consistency reliability of the questionnaires.
Dependent Variable
Treatment Adherence
Treatment adherence refers to behaviors related to medication taking, diet, exercise, and daily activity, risk factor avoidance, stress management, and medication and follow-up visits. It was measured by the Adherence to Hypertensive Treatment Scale. Higher total scores indicate greater adherence to treatment. This scale was developed by Meekusol et al32 and adapted by Taengsakha et al33 to measure treatment adherence among Thai patients at a semi-rural district hospital in Thailand.33 In this study, the modified scale comprised 24 items relevant to people with both HTN and pre-DM. This scale encompassed both pharmacological and non-pharmacological aspects, including diet (6 items), exercise and daily activity (5 items), risk factor avoidance (4 items), stress management (3 items), and medication and follow-up visits (6 items). Examples of the items include, “I choose to cook or eat food cooked by boiling, blanching, or steaming, instead of frying with oil,” “Each workout I do takes at least 30 minutes,” and “I keep doctor’s appointments.” Participants were asked to respond to each item on a visual analog scale (VAS) from 0 (“never”) to 100 (“always”). The overall Cronbach’s for this scale was 0.75, representing acceptable internal consistency.
Independent Variables
Participants’ Background Characteristics
Participants’ background characteristics included sex, age, healthcare coverage scheme, healthcare costs, education level, income, smoking, and alcohol consumption.
Knowledge About HTN and Pre-DM/T2DM
The HTN and pre-DM/T2DM knowledge scale was developed by the researchers based on a literature review.33–35 It comprises 23 items, measuring knowledge across two subscales: HTN (15 items) and pre-DM/T2DM (8 items). The participants responded to each item in the form of “yes,” “no,” or “don’t know.” Each correct answer earns 1 point. We calculated the scores by summing the item response scores of each subscale; a higher total score reflected more knowledge about HTN and pre-DM/T2DM. The Kuder–Richardson 20 (KR-20) that of the subscale measuring knowledge about HTN was 0.83, and that of knowledge about pre-DM/T2DM was 0.77, representing acceptable reliability.
Social Support
The Social Support Scale was developed by Wongyai et al35 and later modified by Taengsakha et al33 This scale has been used among people with diabetes35 and hypertension32 in Thailand. The scale separately measures social support from two distinct sources: family members and healthcare providers. In each of these cases, four subscales are used: emotional (6 items), appraisal (5 items), informational (7 items), and instrumental support (6 items). Participants respond to each item on the scale using a five-point Likert scale (1 = strongly disagree, 2 = disagree, 3 = neutral, 4 = agree, 5 = strongly agree). An example of the social support items is, “When you feel tired of taking medicine every day, do you have someone to encourage you?” We calculated the overall scores for each source by summing the individual item response scores. A higher total score corresponds to a higher level of social support. Cronbach’s for the overall Social Support Scale was 0.96, indicating adequate internal reliability.
Disease–Related Information
Disease–related information collected from medical records included blood pressure, blood sugar, comorbidities, duration of HTN, and duration of pre-DM.
Treatment–Related Information
Treatment–related information, including the number of medication types and the total number of pills per day, was collected from medical records. The experience of medication side effects associated with antihypertensive medications was reported by the participants.
Healthcare Provider–Related Factors
Characteristics of providers included the type of physician (Family medicine versus general practitioner) as well as the patient–provider relationship.
The patient–provider relationship was measured using a VAS developed by Wongyai et al35 This evaluated the patient’s perceptions of the quality of their relationship with their healthcare provider.
Participants were asked to rate their perceived relationship on a 100 mm horizontal line. The scale ranged from 0 (“very poor”) to 100 (“very good”).
Healthcare System–Related Factors
This study employed a questionnaire on health service accessibility developed by Wongyai et al,35 which was used in previous studies33,35 It includes fill-in-the-blank questions on distance, travel time, and the cost of travel to the health service setting, waiting time for services, and the frequency of follow-up appointments.
The Convenience Access Scale consists of two items that assess participants’ convenience in accessing health services using a VAS: “How convenient is it for you to travel for health services?” and “How convenient is it for you to use the health services?” Participants were asked to rate their perceived convenience on a 100 mm horizontal VAS, marking the point that best represented their assessment of convenience. The scale ranged from 0 (“not at all convenient”) to 100 (“very convenient”).
Data Collection
Following ethical approval, permission to conduct the study was obtained from the Public Health Office of Nonthaburi Province. The researcher coordinated with the directors and in-charge nurses at NCD clinics at the 11 subdistrict HPHs in Sai Noi District to schedule recruitment. Patients with HTN who were registered at these subdistrict HPHs were screened for eligibility by the in-charge nurse. Eligible patients attending the clinics during the data collection period were approached through convenience sampling by the researcher or trained research assistant (RA) and informed about the study. Those who provided written informed consent completed a structured questionnaire independently. For participants with limited literacy, the researcher or RA read the questions aloud to them. Data collection was conducted in a quiet area to ensure confidentiality and minimize interruptions. It took place at each site within 3–4 days. A total of 298 eligible individuals were initially approached. Of these, ten were inconvenient to participate in, and eight were excluded due to Mini Cog screening score ≤ 3. An additional five patients were unable to complete the questionnaire. As a result, 275 participants successfully completed the study, yielding an overall response rate of 92.3%.
To ensure consistency in data collection, the RA was trained, and a practice session was conducted prior to the study. Guidance on standardized procedures was also provided for administering the questionnaire and for assisting participants with limited literacy to minimize bias. Data collection began after the RA demonstrated consistent and accurate administration, and the principal researcher continuously monitored the process to ensure adherence to the study protocol.
Ethical Considerations
Prior to data collection, this study was approved by the Ethics Committee of the Faculty of Medicine Ramathibodi Hospital, Mahidol University, Thailand (COA No. MURA2024/806). Participation in the study was voluntary and confidential. The participants were also informed that they could withdraw from the study at any time without any adverse effect on the care they receive. All participants provided written informed consent prior to participating in this study.
Data Analysis
Descriptive statistics were used to analyze participant–, disease–, treatment–, healthcare provider–, and healthcare system–related factors. Data were tested to determine whether they met the assumption of normality. Pearson’s product-moment correlation, Spearman’s product-moment correlation, or point-biserial correlation was used to test the relationship between the dependent variable and each independent variable as appropriate. To control for confounding factors, stepwise multiple linear regression was used to identify factors associated with treatment adherence, based on predefined criteria for entering (p < 0.05) and removing (p > 0.10) variables. Multicollinearity among predictors was assessed using variance inflation factors (VIFs) and tolerance statistics to ensure that each predictor contributed independently to the regression model. In this study, VIF values near 1 and tolerance values near 1 indicate minimal multicollinearity, suggesting that the predictor has little linear association with other independent variables and that coefficient estimates are not substantially inflated. All statistical analyses were performed using IBM SPSS version 31.36
Reporting Guidelines
This study was reported in accordance with the STROBE guidelines. The checklist items were integrated throughout the manuscript, and the completed checklist is provided as supplementary material.
Results
Background Characteristics, Knowledge, and Social Support
Most of the participants were 60 years or older (n = 191, 69.5%) and were female (n = 180, 65.5%), had a primary school education or lower (n = 230, 83.6%), and had a monthly income of 5,000 baht (~US$150) or less (n = 192, 69.8%) (Table 1).
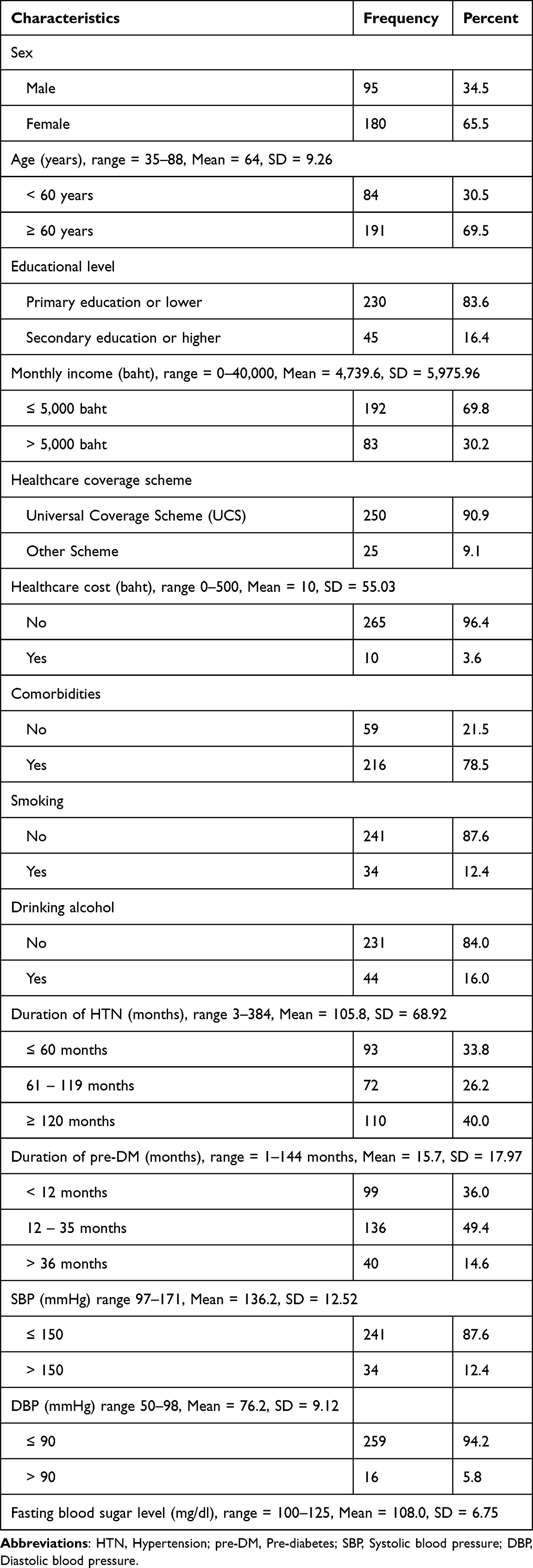 |
Table 1 Background Characteristics of Participants (n = 275) |
Table 2 shows that most participants had moderate overall knowledge scores of HTN and pre-DM/T2DM. When analyzing medical conditions in more detail, it was observed that participants possessed moderate knowledge of HTN, including its causes, symptoms, complications, and management. For pre-DM/T2DM, participants also demonstrated a moderate understanding of symptoms and complications; however, their specific knowledge of causes of the disease was only fair.
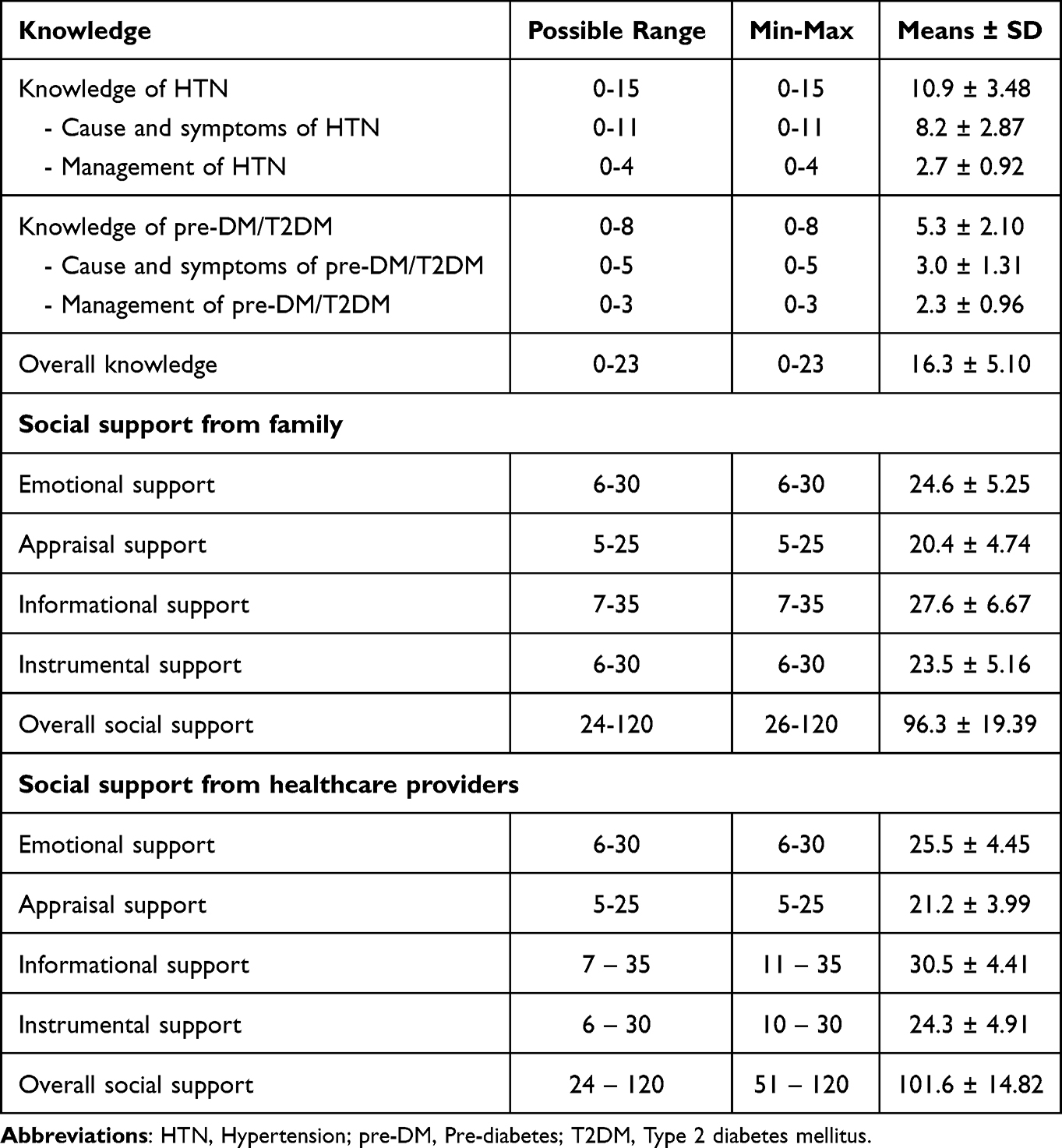 |
Table 2 Knowledge of HTN and Pre-DM/T2DM and Social Support by Source (n = 275) |
The participants had good overall social support scores across informational, emotional, and appraisal support. However, instrumental support was found to be moderate. Considering the sources of support, it was found that participants received more support from healthcare providers (mean = 101.6, SD = 14.82) than from family members (mean = 96.3, SD = 19.39), particularly in terms of informational and instrumental support (Table 2).
Treatment, Provider, and Service Settings
Regarding prescribed treatments, most participants had three types of medications or fewer (n = 214, 77.8%). The majority had also experienced some side effects from their medications (n = 219, 79.6%), such as polyuria, dizziness, fatigue, cough, and peripheral edema.
Most participants had family medicine physicians as their primary providers (n = 165, 60%). Additionally, most participants reported that they had a good patient–provider relationship (n = 243, 88.4%). Most participants attended health service settings within 5 km (n = 250, 90.9%), with the trip typically taking less than 10 min (n = 175, 63.6%). Their waiting time for health services was mostly 60 min or less (n = 176, 64.0%). Most felt that their attendance of (n = 255, 92.7%) and use of health services were convenient (n = 247, 89.8%) (Table 3).
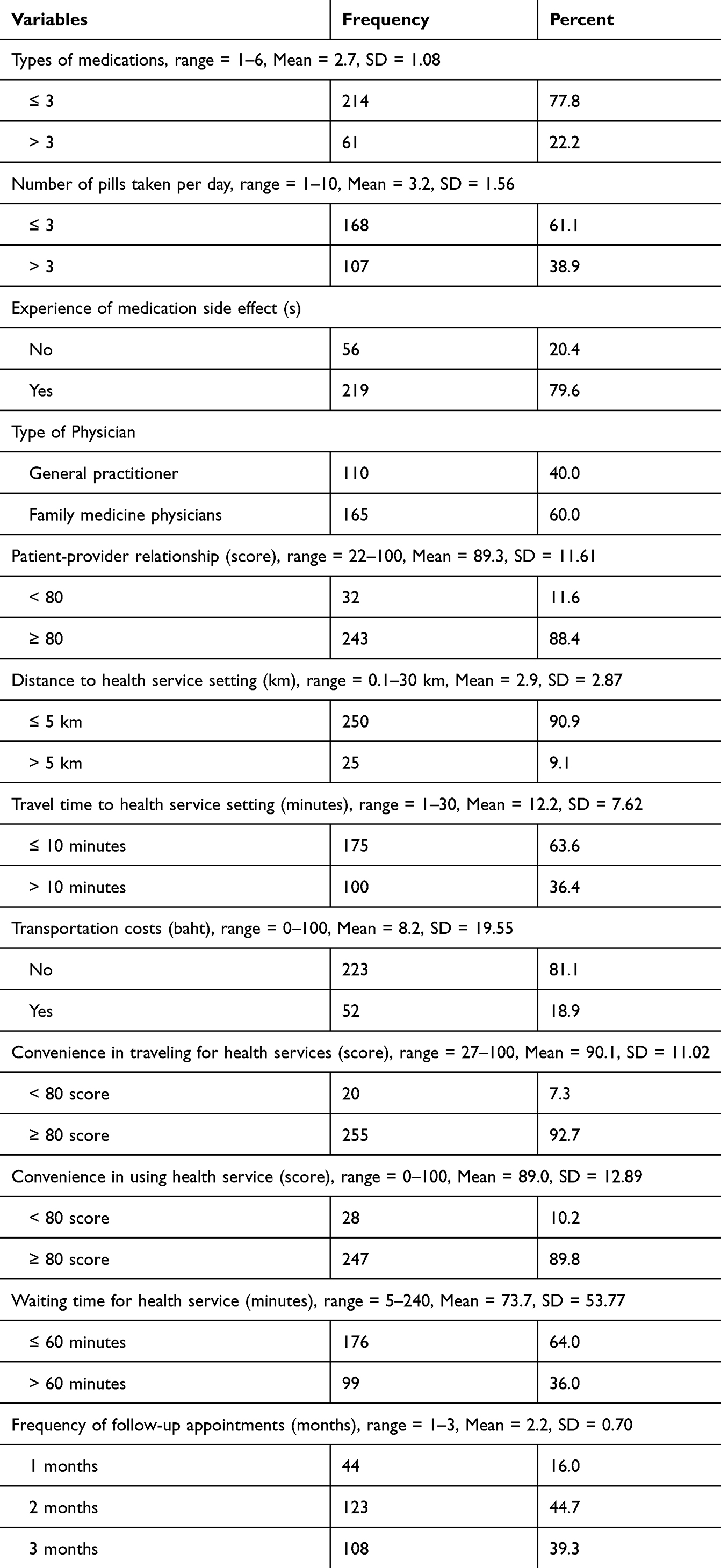 |
Table 3 Treatment-Related Variables, Healthcare Provider-Related Variables and Accessibility to Healthcare Service (n = 275) |
Most participants had a moderate self-reported level of overall treatment adherence (mean = 1604.1, SD = 216.99). When considering each aspect of treatment adherence, it was found that adherence to medication and follow-up appointments (mean = 482.1, SD = 76.28), risk factor avoidance (mean = 279.5, SD = 75.66), and stress management (mean = 204.5, SD = 78.09) were at moderate levels. Meanwhile, adherence to recommendations about diet (mean = 362.2, SD = 74.76) and adherence to exercise and daily activity (mean = 275.7, SD = 103.72) were at fair levels (Table 4).
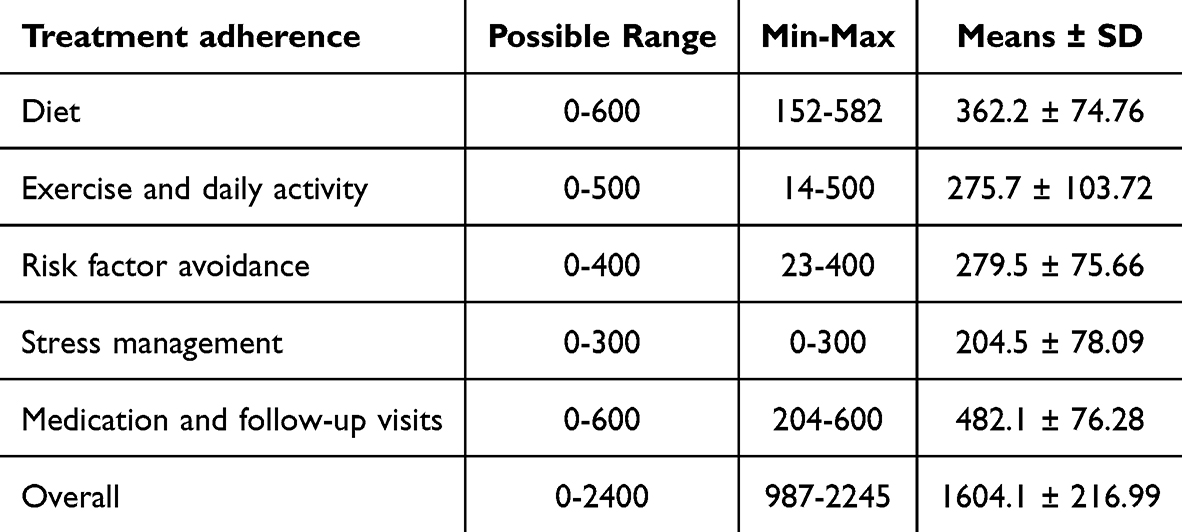 |
Table 4 Participants’ Treatment Adherence (n = 275) |
Factors Related to Treatment Adherence
For background characteristics, it was revealed that sex had a significant relationship with treatment adherence (rpb = 0.183, p = 0.002). Specifically, females exhibited higher adherence than males. Smoking and alcohol consumption had significant negative relationships with treatment adherence (rpb = −0.213, p < 0.001; rpb = −0.166, p = 0.006, respectively). Educational level, healthcare coverage scheme, and healthcare cost were not significantly related to treatment adherence (p > 0.05).
Knowledge about HTN, pre-DM/T2DM had significant positive relationships with treatment adherence (rs = 0.142, p = 0.018; rs = 0.179, p = 0.003, respectively). Overall, social support from family and healthcare personnel was significantly related to treatment adherence (rs = 0.240, p < 0.001; rs = 0.159, p = 0.008, respectively). None of the disease-related characteristics was significantly associated with treatment adherence (p > 0.05) (Table 5).
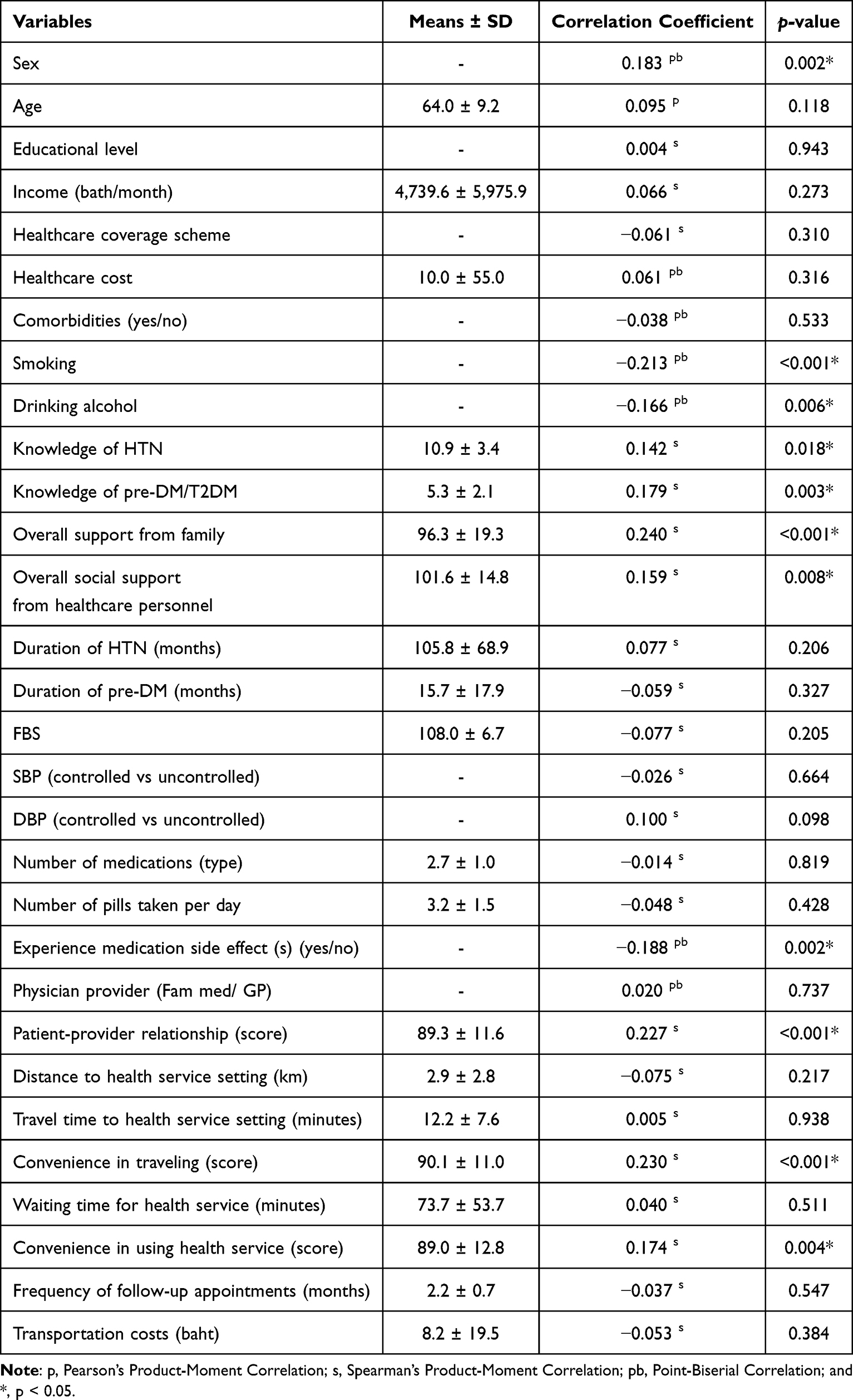 |
Table 5 Correlations of Patients’ Factors, Disease Characteristics Factors, Medication Factors, Provider Factors, and Clinical Setting Factors with Treatment Adherence (n = 275) |
For medication–related factors, only one factor, “experience of medication side effects,” was found to have a significantly negative relationship with treatment adherence (rpb = −0.188, p = 0.002). For provider–related factors, it was found that only the patient–provider relationship had a significant positive relationship with treatment adherence (rs = 0.227, p < 0.001). For factors related to clinical settings, it was found that convenience of traveling to health services and convenience in using the services were significantly positively related to treatment adherence (rs = 0.230, p < 0.001; rs = 0.174, p = 0.004, respectively) (Table 5).
Multiple Regression Model Predicting Treatment Adherence
A multiple linear regression model comprising five variables was found to be statistically significant in predicting treatment adherence among people with both HTN and pre-DM (F(5,269) = 11.36, p < 0.001; R2 = 0.174). The model indicated that social support from family (B = 2.23, p < 0.001), smoking (B = −132.61, p < 0.001), experience of medication side effects (B = −89.51, p = 0.004), knowledge of pre-DM/T2DM (B = 14.67, p = 0.013), and patient–provider relationship (B = 2.23, p = 0.033) were factors significantly influencing treatment adherence (Table 6).
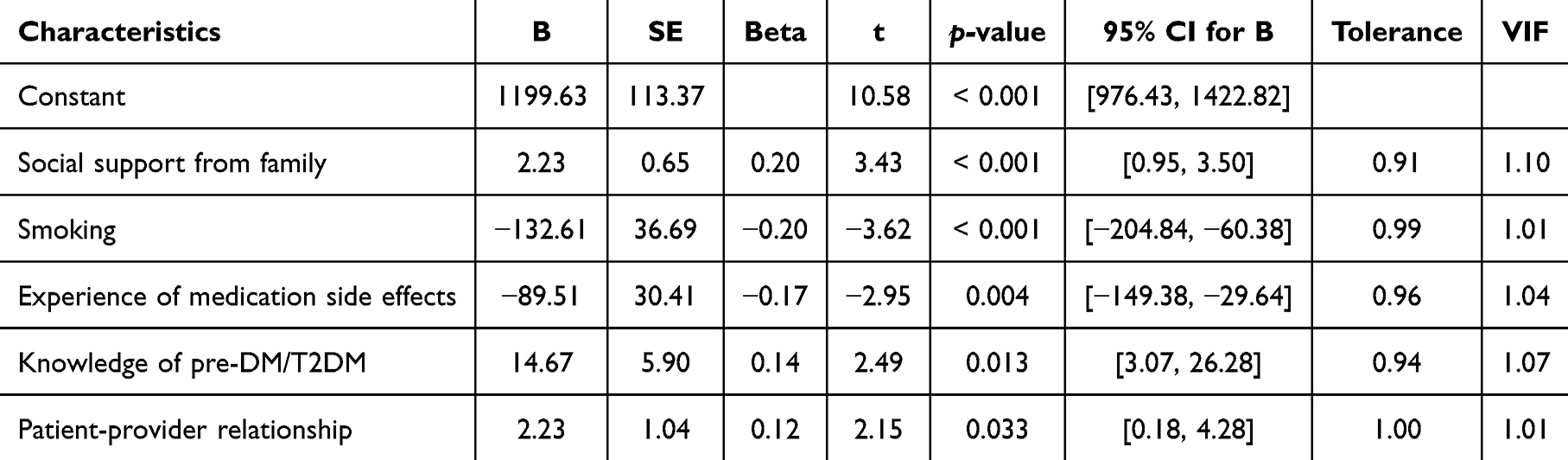 |
Table 6 Multiple Regression Analysis Predicting Treatment Adherence (n = 275) |
Discussion
In this study, the participants were 275 patients with both HTN and pre-DM recruited from 11 HPHs in Sai Noi, a semi-rural district of Nonthaburi Province, Thailand.
From bivariate analysis, this study revealed that female sex, knowledge about HTN and pre-DM/T2DM, social support, patient–provider relationship, convenience of traveling to health services, and convenience in using attending such services were significantly positively correlated with adherence to treatment. Conversely, experience of medication side effects, smoking, and drinking alcohol were negatively correlated with treatment adherence. The factors influencing treatment adherence can be categorized into five domains based on the WHO’s adherence framework.14
The study findings can be explained based on the Health Belief Model in that individuals who perceive greater benefits and fewer barriers to health-related behaviors are more likely to engage in them (Rosenstock, 1974).37 In this study, knowledge of HTN and pre-DM/T2DM likely enhanced perceived susceptibility and potential future severity of their health conditions, thereby enhancing treatment adherence. In addition to knowledge, social support and a positive patient-provider relationship may act as cues to action, promoting adherence to treatment. In contrast, the experience of medication side effects is perceived as significantly discouraging treatment adherence.
In terms of patient-related factors, our finding of better adherence among females is consistent with previous studies in France, Malaysia, and China.38–42 Females tend to seek healthcare and receive healthcare services, including health behavior modifications, more regularly than males.43–47 Meanwhile, smoking and drinking alcohol can be viewed as competing risk behaviors and are significantly and negatively related to treatment adherence, indicating that smokers and drinkers were more likely to fail to adhere to treatment than non-smokers or those who do not consume alcohol.48,49 individuals engaging in these behaviors may have lower perceived risk and greater perceived barriers to treatment adherence.48,49
Better knowledge about HTN and pre-DM/T2DM increases perceived susceptibility and severity, thereby enhancing treatment adherence. Individuals who understand their diseases are more likely to exhibit better treatment adherence.50,51 Despite two-thirds of the participants having HTN for more than five years and nearly half having pre-DM for one to three years, they have only a moderate level of knowledge about their conditions. This may be because hypertension is often a silent condition, despite being emphasized during routine care and prioritized in treatment with antihypertensive medications. In contrast, when health education is insufficiently addressed to both HTN and pre-DM, patients may have limited awareness of their dual risk and the importance of managing both conditions. A lack of knowledge and understanding of their own health conditions may result in poor adherence to treatment, particularly lifestyle modifications (eg, diet and exercise), and an increased likelihood of developing various complications in the future.12,52
We also found that social support from both sources (family members and healthcare providers) had a significantly positive correlation with treatment adherence. This is in line with previous studies in LMICs.32,53,54 Thai family culture remains highly influential, emphasizing extended families living together, where members support each other in various aspects of life, including finances, childcare, and eldercare.55 Healthcare providers also play an important role in promoting adherence to treatment, as they can be a valuable source of social support by providing health information and guidance regarding treatment.56,57 Similar to other Asian patients,58 Thai patients often perceived the physician as the authoritative source of knowledge and management of their illnesses.59 However, overall support by family is relatively essential in managing diet, medications, and daily activities.59 Our study found that family support had a stronger positive relationship than support from healthcare providers, reflecting the family’s role in caring for patients mentally and emotionally, monitoring treatment adherence behaviors, and helping with daily activities.58,60–62
The existence of a good relationship between patient and provider was also found to have a statistically significant positive relationship with treatment adherence in this study. Overall, the patients in this study had good relationships with healthcare providers. The people in the semi-rural area mostly had UCS and used primary care services at their local subdistrict HPHs, and the healthcare team also regularly provides home visits to the elderly and people with disabilities and runs health-promoting activities in the community. These programs may foster familiarity and facilitate trust between patients and providers.52,63 Such trust can make patients more open to discussions with healthcare providers, which in turn improves treatment adherence.64 Indeed, several previous studies also reported that strong patient–provider relationships are positively related to treatment adherence.32,58,65,66
Regarding treatment–related factors, the experience of medication side effects after taking antihypertensive medications was significantly negatively related to treatment adherence. This is consistent with previous studies,67,68 which reported that a history of allergic reactions to drugs or the occurrence of side effects reduces adherence to medication regimens. The most commonly reported side effects of antihypertensive medications are frequent urination and dry cough, which affect daily life and cause physical discomfort.
With regard to healthcare system–related factors, our study showed that the healthcare scheme and healthcare costs were not significantly related to treatment adherence. This may be because the vast majority of the participants (96%) receive free healthcare services at the subdistrict HPHs through the different health insurance schemes.69 Convenience of traveling to health services and convenience in using the services were significantly positively related to treatment adherence, which is consistent with previous studies.33,35,70,71 It is assumed that the participants in this study felt that it was convenient to attend the service setting and use the services due to their subdistrict HPH’s proximity to their residence or in a community with easy access.64,71
As treatment adherence is influenced by a complex interplay of personal, clinical, and contextual factors; thus, any single factor is unlikely to demonstrate strong relationships when examined independently. When controlling for confounding factors, knowledge about pre-DM/T2DM, social support from the family, patient–provider relationship, smoking, and the experience of medication side effects were significantly predictive of treatment adherence among people with both HTN and pre-DM. These findings provide valuable insights for health officials by highlighting the factors influencing adherence to treatment among individuals with both HTN and pre-DM. They could also inform future intervention and management strategies for this dual-risk population. When a patient has fasting glucose between 100 and 125 mg/dL, a pre-DM alert should be generated, necessitating management based on the National practice guidelines. This could help to ensure that more emphasis is placed on pre-DM as a disease state, rather than a silent precursor.17,72
The provision of information about HTN together with pre-DM/T2DM increases patients’ knowledge and understanding of their conditions, their perceived susceptibility, and the severity of the dual risk to which they are exposed. This can, in turn, enhance adherence to medications and recommendations to follow a healthy lifestyle, such as via improved diet, more physical activities, and support for smoking cessation.73–76 This supports the assertion that Thailand’s Universal Healthcare Coverage should cover the integration of self-management education for people with chronic diseases.
As family support is essential for promoting treatment adherence, this study suggests that family-based interventions, particularly those targeting dietary management, physical activity, and medication adherence, with a specific emphasis on older adults who may rely more heavily on family support. Community-based peer or family support groups integrated within primary care networks, as well as telehealth strategies for patient education77 could be considered as additional interventions to enhance self-management and medication adherence. These interventions may be particularly beneficial in rural and semi-rural communities in Thailand and other LMICs54 with comparable healthcare and resource contexts. Furthermore, enhancing the quality of patient–provider relationships is essential, ultimately promoting more effective and sustained treatment adherence. This can be achieved through building trust, ensuring continuity of care by the same care team, and involving patients in treatment decisions tailored to their individual contexts,52 which may vary across social and health system settings.
Strengths and Limitations
To the best of our knowledge, this study is the first to examine treatment adherence among individuals living with both HTN and pre-DM, particularly at subdistrict health facilities in a semi-rural district of Thailand. Nevertheless, several limitations of this work should be acknowledged. First, the use of convenience sampling may have introduced selection bias. This study may be subject to healthy volunteer bias, as individuals attending the NCD clinic who agreed to participate may have been more health-conscious or motivated to follow treatment recommendations and engage in health–related behaviors than those who declined participation. Specifically, those with higher treatment adherence are more likely to have agreed to participate in this study. In addition, the participants who attended the HPHs’ NCD clinic would be more likely to have higher adherence than those who did not. Second, some participants may have over-reported their adherence to the treatment due to social desirability bias. Third, the sample was relatively homogeneous—predominantly female, older, and with lower income and education levels—which may limit the generalizability of the findings to other populations. Last, its cross-sectional design hinders the establishment of causal relationships between variables.
Conclusions
This study revealed that female sex, knowledge about HTN and pre-DM/T2DM, social support, good patient–provider relationship, convenience of traveling to healthcare services, and convenience in using these services were significantly positively correlated with adherence to treatment in semi-rural Thai patients with pre-DM and HTN. Meanwhile, the experience of medication side effects, smoking, and consumption of alcohol were negatively correlated with treatment adherence. Controlling for confounders, knowledge of pre-DM/T2DM, social support from family, good patient–provider relationship, smoking, and the experience of medication side effects were statistically significant in predicting treatment adherence among people with both HTN and pre-DM. These findings provide valuable insights for health officials by enhancing understanding of treatment adherence among individuals with both HTN and pre-DM and should inform future intervention and management strategies for this dual-risk population in the primary care settings. Future research should include longitudinal studies, intervention studies, and studies in diverse populations.
Data Sharing Statement
Data supporting this study are available from the corresponding author.
Ethics Approval and Informed Consent
This study was approved by the Committee on Human Rights Related to Research Involving Human Subjects, the Faculty of Medicine Ramathibodi Hospital, Mahidol University.
All participants were informed about the purposes, procedures, and preservation of confidentiality and anonymity in this study, as well as the potential risks and benefits. This study was conducted in accordance with the tenets of the Declaration of Helsinki.
Acknowledgement
We would like to convey our sincere appreciation to all respondents who participated in the study. We are also deeply grateful to the Ramathibodi Foundation for the partial support.
Funding
This study received no external funding. The Faculty of Medicine Ramathibodi Hospital and Mahidol University supported the publication fees.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. International Diabetes Federation. IDF Diabetes Atlas. Brussels: International Diabetes Federation; 2015. Available from: https://globaldiabeteseducation.wordpress.com/wp-content/uploads/2017/03/idf_atlas-2015_uk.pdf.
2. International Diabetes Federation. IDF Diabetes Atlas. Brussels: International Diabetes Federation; 2021. Available from: https://fmdiabetes.org/wp-content/uploads/2022/01/IDF_Atlas_10th_Edition_2021-comprimido.pdf.
3. Joseph A, Sewor C, Kodapally B, Manda CE, Joseph J, Mathews E. The burden of prediabetes in low- and middle-income countries: a systematic review and meta-analysis. Eur J Clin Nutr. 2025;79(9):827–17. doi:10.1038/s41430-025-01578-1
4. Echouffo-Tcheugui JB, Perreault L, Ji L, Dagogo-Jack S. Diagnosis and management of prediabetes: a review. JAMA. 2023;329(14):1206–1216. doi:10.1001/jama.2023.4063
5. Richter B, Hemmingsen B, Metzendorf MI, Takwoingi Y. Development of type 2 diabetes mellitus in people with intermediate hyperglycaemia. Cochrane Database Syst Rev. 2018;10(10):CD012661. doi:10.1002/14651858.CD012661.pub2
6. Huang YQ, Liu L, Huang JY, et al. Prediabetes and risk for all-cause and cardiovascular mortality based on hypertension status. Ann Transl Med. 2020;8(23):1580. doi:10.21037/atm-20-1155
7. Liu -H-H, Cao Y-X, Li S, et al. Impacts of prediabetes mellitus alone or plus hypertension on the coronary severity and cardiovascular outcomes. Hypertension. 2018;71(6):1039–1046. doi:10.1161/HYPERTENSIONAHA.118.11063
8. Liu X, Song Q, Wu S, Zhou W, Wang X. Prediabetes and risk for myocardial infarction by hypertension status in a Chinese population: a prospective cohort study. J Hypertens. 2021;39(1):77–83. doi:10.1097/HJH.0000000000002607
9. Hubbard D, Colantonio LD, Tanner RM, et al. Prediabetes and risk for cardiovascular disease by hypertension status in black adults: the jackson heart study. Diabetes Care. 2019;42(12):2322–2329. doi:10.2337/dc19-1074
10. Haile TG, Mariye T, Tadesse DB, Gebremeskel GG, Asefa GG, Getachew T. Prevalence of hypertension among type 2 diabetes mellitus patients in Ethiopia: a systematic review and meta-analysis. Int Health. 2023;15(3):235–241. doi:10.1093/inthealth/ihac060
11. Roth GA, Mensah GA, Johnson CO, et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: update from the GBD 2019 study. J Am Coll Cardiol. 2020;76(25):2982–3021. doi:10.1016/j.jacc.2020.11.010
12. Hamrahian SM, Maarouf OH, Fülöp T. A critical review of medication adherence in hypertension: barriers and facilitators clinicians should consider. Patient Prefer Adherence. 2022;16:2749–2757. doi:10.2147/PPA.S368784
13. Petrie JR, Guzik TJ, Touyz RM. Diabetes, hypertension, and cardiovascular disease: clinical insights and vascular mechanisms. Can J Cardiol. 2018;34(5):575–584. doi:10.1016/j.cjca.2017.12.005
14. World Health Organization. Adherence to long-term therapies: evidence for action. Geneva: World Health Organization; 2003. Available from: https://iris.who.int/server/api/core/bitstreams/121c6b73-8651-442f-9560-e3b1d9c8a75c/content.
15. Hossain A, Ahsan GU, Hossain MZ, et al. Medication adherence and blood pressure control in treated hypertensive patients: first follow-up findings from the PREDIcT-HTN study in Northern Bangladesh. BMC Public Health. 2025;25:250. doi:10.1186/s12889-025-21409-z
16. Religioni U, Barrios-Rodríguez R, Requena P, Borowska M, Ostrowski J. Enhancing therapy adherence: impact on clinical outcomes, healthcare costs, and patient quality of life. Medicina. 2025;61(1):153. doi:10.3390/medicina61010153
17. Glechner A, Keuchel L, Affengruber L, et al. Effects of lifestyle changes on adults with prediabetes: a systematic review and meta-analysis. Prim Care Diabetes. 2018;12(5):393–408. doi:10.1016/j.pcd.2018.07.003
18. Shin J, Konlan KD. Prevalence and determinants of medication adherence among patients taking antihypertensive medications in Africa: a systematic review and meta-analysis 2010-2021. Nurs Open. 2023;10(6):3506–3518. doi:10.1002/nop2.1613
19. Krass I, Schieback P, Dhippayom T. Adherence to diabetes medication: a systematic review. Diabetic Med. 2015;32(6):725–737. doi:10.1111/dme.12651
20. Maniero C, Lopuszko A, Papalois K-B, Gupta A, Kapil V, Khanji MY. Non-pharmacological factors for hypertension management: a systematic review of international guidelines. Eur. J. Prev. Cardiol. 2022;30(1):17–33. doi:10.1093/eurjpc/zwac163
21. American Diabetes Association Professional Practice Committee. 3. Prevention or delay of diabetes and associated comorbidities: standards of care in diabetes—2025. Diabetes Care. 2025;48(Suppl 1):S50–S58. doi:10.2337/dc25-S003.
22. The Diabetes Association of Thailand. Clinical practice guideline for diabetes 2023. Bangkok: The Diabetes Association of Thailand; 2023. Available from: https://drive.google.com/file/d/1OAIDiCyGsJYA1-wTAxoOu6yL_YL9c7IG/view.
23. Tsai HY, Chuang HJ, Liao WH, et al. Lifestyle modifications and non-pharmacological management in elderly hypertension. J Formos Med Assoc. 2025;124(Suppl 1):S32–S41. doi:10.1016/j.jfma.2024.10.022
24. García-Pérez LE, Alvarez M, Dilla T, Gil-Guillén V, Orozco-Beltrán D. Adherence to therapies in patients with type 2 diabetes. Diabetes Ther. 2013;4(2):175–194. doi:10.1007/s13300-013-0034-y
25. Aekplakorn W, Puckcharern H, Satheannoppakao W. editors.. The 6th Thai National Health Examination Survey 2019–2020. Nakhon Pathom. Institute for Population and Social Research, Mahidol University; 2021. Available from https://www.hiso.or.th/hiso/picture/reportHealth/report/sreport6/sreport6_full.pdf.
26. Ministry of Public Health. Health data center [Internet]. Nonthaburi: Ministry of Public Health. Available from: https://hdc.moph.go.th/nbi/public/standard-report-detail/eeeab22e386d32e7f5f5ecefebce0001.
27. Flood D, Geldsetzer P, Agoudavi K, et al. Rural-urban differences in diabetes care and control in 42 low- and middle-income countries: a cross-sectional study of nationally representative individual-level data. Diabetes Care. 2022;45(9):1961–1970. doi:10.2337/dc21-2342
28. Ickovics JR, Meade CS. Adherence to antiretroviral therapy among patients with HIV: a critical link between behavioral and biomedical sciences. J Acquir Immune Defic Syndr. 2002;31(Suppl 3):S98–S102. doi:10.1097/00126334-200212153-00002
29. Primary Health System Support Division. Office of the permanent secretary, ministry of public health. primary care unit standards manual 2025–2027. Nonthaburi: Ministry of Public Health; 2025. Available from: https://pcustandard.moph.go.th/login.php.
30. Department of Medical Services, Ministry of Public Health. Elderly screening manual 2021. Bangkok: Najanta Creation Co.; 2021. Available from: https://drive.google.com/file/d/1AzA7XPBrra2btoqeTs9O5Mhk0oD7naNZ/view.
31. Cohen J. Statistical Power Analysis for the Behavioral Sciences.
32. Meekusol S, Maneesriwongul W, Orathai P, Pongtharomkamzol K, Sharps PW. Factors predicting women’s adherence to hypertensive treatment. Pac Rim Int J Nurs Res. 2021;25(1):131–142 Available from: https://he02.tci-thaijo.org/index.php/PRIJNR/article/view/241920.
33. Taengsakha K, Maneesriwongul W, Putawatana P. Factors related to adherence to treatment in essential hypertensive patients with early renal insufficiency. Nurs Res Innov J. 2019;25(1):87–101 Available from: https://he02.tci-thaijo.org/index.php/RNJ/article/view/125605.
34. Tanchaitechawut T. A Comparison of Knowledge about prediabetes amongst prediabetes and Non-prediabetes adults that receiving Health Checkups in Sungaikolok Hospital. Thai J Public Health Health Sci. 2023;6(1):87–98 Available from: https://he02.tci-thaijo.org/index.php/tjph/article/view/258857.
35. Wongyai S, Maneesriwongul W, Putawatana P. Factors related to medication adherence among patients with diabetes type 2 at diabetic clinics. J Health Nurs Res. 2014;30(2):
36. IBM Corp. IBM SPSS Statistics for Windows, Version 31.0. Armonk, NY: Licensed to Mahidol University; 2025.
37. Rosenstock IM, Strecher VJ, Becker MH. Social learning theory and the health belief model. Health Educ Q. 1988;15(2):175–183. doi:10.1177/109019818801500203
38. Lefort M, Neufcourt L, Pannier B, et al. Sex differences in adherence to antihypertensive treatment in patients aged above 55: the French League Against Hypertension Survey (FLAHS). J Clin Hypertens. 2018;20(10):1496–1503. doi:10.1111/jch.13387
39. Ramli A, Ahmad NS, Paraidathathu T. Medication adherence among hypertensive patients of primary health clinics in Malaysia. Patient Prefer Adherence. 2012;6:613–622. doi:10.2147/PPA.S34704
40. Chia YC, Devaraj NK, Ching SM, et al. Relationship of an adherence score with blood pressure control status among patients with hypertension and their determinants: findings from a nationwide blood pressure screening program. J Clin Hypertens. 2021;23(3):638–645. doi:10.1111/jch.14212
41. Pan J, Wu L, Wang H, et al. Determinants of hypertension treatment adherence among a Chinese population using the therapeutic adherence scale for hypertensive patients. Medicine. 2019;98(27):e16116. doi:10.1097/MD.0000000000016116
42. Win T, Thanaslip S, Polsook R. Factors predicting treatment adherence among patients with hypertension: a systematic review and meta-analysis. Natl J Community Med. 16(07):720–732. doi:10.55489/njcm.160720255266
43. Khanam MA, Lindeboom W, Koehlmoos TL, Alam DS, Niessen L, Milton AH. Hypertension: adherence to treatment in rural Bangladesh--findings from a population-based study. Glob Health Action. 2014;7:25028. doi:10.3402/gha.v7.25028
44. Thompson AE, Anisimowicz Y, Miedema B, Hogg W, Wodchis WP, Aubrey-Bassler K. The influence of gender and other patient characteristics on health care-seeking behaviour: a QUALICOPC study. BMC Fam Pract. 2016;17:38. doi:10.1186/s12875-016-0440-0
45. Everett B, Zajacova A. Gender differences in hypertension and hypertension awareness among young adults. Biodemography Soc Biol. 2015;61(1):1–17. doi:10.1080/19485565.2014.929488
46. Muiesan ML, Salvetti M, Rosei CA, Paini A. Gender differences in antihypertensive treatment: myths or legends? High Blood Press Cardiovasc Prev. 2016;23(2):105–113. doi:10.1007/s40292-016-0148-1
47. Chow CK, Teo KK, Rangarajan S, et al. Prevalence, awareness, treatment, and control of hypertension in rural and urban communities in high-, middle-, and low-income countries. JAMA. 2013;310(9):959–968. doi:10.1001/jama.2013.184182
48. Abbas H, Kurdi M, de Vries F, et al. Factors associated with antihypertensive medication non-adherence: a cross-sectional study among Lebanese hypertensive adults. Patient Prefer Adherence. 2020;14:663–673. doi:10.2147/PPA.S238751
49. Chou C-P, Chen C-Y, Huang K-S, Lin S-C, Huang C-F, Koo M. Factors associated with nonadherence to antihypertensive medication among middle-aged adults with hypertension: findings from the Taiwan National Health Interview Survey. J Int Med Res. 2020;48(8). doi:10.1177/0300060520936176
50. Pristianty L, Hingis ES, Priyandani Y, Rahem A. Relationship between knowledge and adherence to hypertension treatment. J Public Health Afr. 2023;14(Suppl 1):2502. doi:10.4081/jphia.2023.2502
51. Algabbani FM, Algabbani AM. Treatment adherence among patients with hypertension: findings from a cross-sectional study. Clinical Hypertension. 2020;26(1):18. doi:10.1186/s40885-020-00151-1
52. Chauke GD, Nakwafila O, Chibi B, Sartorius B, Mashamba-Thompson T. Factors influencing poor medication adherence amongst patients with chronic disease in low-and-middle-income countries: a systematic scoping review. Heliyon. 2022;8(6):e09716. doi:10.1016/j.heliyon.2022.e09716
53. Dhar L, Dantas J, Ali M. A systematic review of factors influencing medication adherence to hypertension treatment in developing countries. Open J Epidemiol. 7(03):211–250. doi:10.4236/ojepi.2017.73018
54. Sohal T, Sohal P, King-Shier KM, Khan NA. Barriers and facilitators for type-2 diabetes management in South Asians: a systematic review. PLoS One. 10(9):e0136202. doi:10.1371/journal.pone.0136202
55. Manasatchakun P, Roxberg Å, Asp M. Conceptions of healthy aging held by relatives of older persons in isan-thai culture: a phenomenographic study. J Aging Res. 2018;2018:3734645. doi:10.1155/2018/3734645
56. Shahin W, Kennedy GA, Stupans I. The association between social support and medication adherence in patients with hypertension: a systematic review. Pharm Pract. 2021;19(2):2300. doi:10.18549/PharmPract.2021.2.2300
57. Tavares Rdos S, da Silva DM. A implicação do apoio social no viver de pessoas com hipertensão arterial [The implication of social support in the lives of people with hypertension]. Rev Gaucha Enferm. 2013;34(3):14–21. doi:10.1590/s1983-14472013000300002
58. Gutierrez MM, Sakulbumrungsil R. Factors associated with medication adherence of hypertensive patients in the Philippines: a systematic review. Clin Hypertens. 2021;27(1):19. doi:10.1186/s40885-021-00176-0
59. Jiraporncharoen W, Pinyopornpanish K, Junjom K, et al. Exploring perceptions, attitudes and beliefs of Thai patients with type 2 diabetes mellitus as they relate to medication adherence at an out-patient primary care clinic in Chiang Mai, Thailand. BMC Family Practice. 21(1):173. doi:10.1186/s12875-020-01233-7
60. Guo A, Jin H, Mao J, et al. Impact of health literacy and social support on medication adherence in patients with hypertension: a cross-sectional community-based study. BMC Cardiovasc Disord. 2023;23(1):93. doi:10.1186/s12872-023-03117-x
61. Świątoniowska-Lonc N, Tański W, Polański J, Jankowska-Polańska B, Mazur G. Psychosocial determinants of treatment adherence in patients with type 2 diabetes - a review. Diabetes Metab Syndr Obes. 2021;14:2701–2715. doi:10.2147/DMSO.S308322
62. Kvarnström K, Westerholm A, Airaksinen M, Liira H. Factors contributing to medication adherence in patients with a chronic condition: a scoping review of qualitative research. Pharmaceutics. 2021;13(7):1100. doi:10.3390/pharmaceutics13071100
63. Kitreerawutiwong N, Jordan S, Hughes D. Facility type and primary care performance in sub-district health promotion hospitals in Northern Thailand. PLoS One. 2017;12(3):e0174055. doi:10.1371/journal.pone.0174055
64. Ikai T, Yamtree S, Takemoto T, et al. Medical care ideals among urban and rural residents in Thailand: a qualitative study. Nt J Equity Health. 2016;15(1):2. doi:10.1186/s12939-015-0292-6
65. Schäfer C. Reimagining medication adherence: a novel holistic model for hypertension therapy. Patient Prefer Adherence. 2024;18:391–410. doi:10.2147/PPA.S442645
66. Ren Z, Xu X, Yue R. Preferences and adherence of people with prediabetes for disease management and treatment: a systematic review. Patient Preference Adherence. 2023;17(null):2981–2989. doi:10.2147/PPA.S437267
67. Margolis KL, Crain AL, Pawloski PA, et al. Blood pressure medication side effect symptoms and patient treatment satisfaction and adherence. J Am Board Family Med. 2025;38(2):312–329. doi:10.3122/jabfm.2024.240288R1
68. Burnier M, Egan BM. Adherence in Hypertension. Circulation Research. 2019;124(7):1124–1140. doi:10.1161/CIRCRESAHA.118.313220
69. World Bank. Thailand public revenue and spending assessment: promoting an inclusive and sustainable future. Washington (DC): World Bank; 2024. Available from: https://documents1.worldbank.org/curated/en/099052523201510112/pdf/P17715703a68af0590b7290234ea94ba989.pdf.
70. Kisigo GA, Mcharo OC, Robert JL, Peck RN, Sundararajan R, Okello ES. Understanding barriers and facilitators to clinic attendance and medication adherence among adults with hypertensive urgency in Tanzania. PLOS Glob Public Health. 2022;2(8):e0000919. doi:10.1371/journal.pgph.0000919
71. Kuria N, Reid A, Owiti P, et al. Compliance with follow-up and adherence to medication in hypertensive patients in an urban informal settlement in Kenya: comparison of three models of care. Trop Med Int Health. 2018;23(7):785–794. doi:10.1111/tmi.13078
72. Howells L, Musaddaq B, McKay AJ, et al. Clinical impact of lifestyle interventions for the prevention of diabetes: an overview of systematic reviews. BMJ Open. 2016;6:e013806 doi:10.1136/bmjopen-2016-013806
73. Verma N, Rastogi S, Chia YC, et al. Non-pharmacological management of hypertension. J Clin Hypertens. 2021;23(7):1275–1283. doi:10.1111/jch.14236
74. Montealegre L, Amador E, Pulido T, Cabrera C, Rivera A, Rebolledo R. Main factors that determine adherence to pharmacological treatment in hypertensive patients: systematic review. J Hypertens. 2022;40(Suppl 1):e308. doi:10.1097/01.hjh.0000838740.81890.19
75. Maniki PT, Chaar BB, Aslani P. Impact of interventions on medication adherence in patients with coexisting diabetes and hypertension. Health Expect. 2024;27(5):e70010. doi:10.1111/hex.70010
76. Xiao J, Ren WL, Liang YY, et al. Effectiveness of lifestyle and drug intervention on hypertensive patients: a randomized community intervention trial in rural China. J Gen Intern Med. 2020;35(12):3449–3457. doi:10.1007/s11606-019-05601-7
77. Sawaengsri N, Maneesriwongul W, Schorr EN, Wangpitipanit S. Effects of telephone-based brief motivational interviewing on self-management, medication adherence, and glycemic control in patients with uncontrolled type 2 diabetes mellitus in a rural community in Thailand. Patient Prefer Adherence. 2023;17:2085–2096. doi:10.2147/PPA.S418514
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Urban-Rural Difference in Treatment Adherence of Chinese Hypertensive Patients
Pan J, Yu H, Hu B, Li Q
Patient Preference and Adherence 2022, 16:2125-2133
Published Date: 15 August 2022
Independent Association of 25[OH]D Level on Reduced Glutathione and TNF-α in Patients with Diabetes and/or Hypertension
AlRadini FA, El-Sheikh AAK, Al Shahrani AS, Alzamil NM, Fayed AA, Alsayed E, Alharbi SS, Altulihee MA, Andijani SA, AlShaiddi WK, Alamri FA
International Journal of General Medicine 2022, 15:7065-7075
Published Date: 5 September 2022
Interventions Incorporating Therapeutic Alliance to Improve Medication Adherence in Black Patients with Diabetes, Hypertension and Kidney Disease: A Systematic Review
Desta R, Blumrosen C, Laferriere HE, Saluja A, Bruce MA, Elasy TA, Griffith DM, Norris KC, Cavanaugh KL, Umeukeje EM
Patient Preference and Adherence 2022, 16:3095-3110
Published Date: 14 November 2022
A Systematic Review of the Hill-Bone Compliance to Blood Pressure Therapy Scale
Commodore-Mensah Y, Delva S, Ogungbe O, Smulcer LA, Rives S, Dennison Himmelfarb CR, Kim MT, Bone L, Levine D, Hill MN
Patient Preference and Adherence 2023, 17:2401-2420
Published Date: 28 September 2023
Knowledge of Cardiovascular Disease Risk Factors and Its Primary Prevention Practices Among the Saudi Public – A Questionnaire-Based Cross-Sectional Study
Bashatah A, Syed W, Al-Rawi MBA
International Journal of General Medicine 2023, 16:4745-4756
Published Date: 20 October 2023