")
Back to Journals » Patient Preference and Adherence » Volume 16
Urban-Rural Difference in Treatment Adherence of Chinese Hypertensive Patients
Authors Pan J , Yu H, Hu B, Li Q
Received 8 June 2022
Accepted for publication 2 August 2022
Published 15 August 2022 Volume 2022:16 Pages 2125—2133
DOI https://doi.org/10.2147/PPA.S377203
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Naifeng Liu
Jingjing Pan,1 Haizhen Yu,2 Bin Hu,1 Qiongge Li1
1Department of Pharmacy, Xi’an People’s Hospital (Xi’an Fourth Hospital), Xi’an, People’s Republic of China; 2Department of Clinical Laboratory, Xi’an People’s Hospital (Xi’an Fourth Hospital), Xi’an, People’s Republic of China
Correspondence: Jingjing Pan, Department of Pharmacy, Xi’an People’s Hospital (Xi’an Fourth Hospital), 21 JieFang Road, Xi’an, People’s Republic of China, Tel +86 029 61199691 ext 029, Email [email protected] Haizhen Yu, Department of Clinical Laboratory, Xi’an People’s Hospital (Xi’an Fourth Hospital), 21 JieFang Road, Xi’an, People’s Republic of China, Tel +86 029 61188149 ext 029, Email [email protected]
Objective: The aims of this study were to evaluate the treatment adherence and the main factors associated with adherence for Chinese hypertensive patients between urban and rural areas.
Participants and Methods: A total of 529 hypertensive patients with 328 from urban areas and 201 from rural areas hospitalized in a tertiary hospital in Xi’an, China during the period from May 1 to December 31, 2021 were invited to participate in the cross-sectional study. The adherence to treatment was assessed by “modified Chinese Hill-Bone compliance to high blood pressure therapy scale”. Binary logistic regression analysis was used to analyze independent risk factor for treatment adherence of hypertensive patients. General linear model was used to analyze the association of the independent risk factors to treatment adherence in each subgroup of the scale.
Results: The treatment adherence of Chinese hypertensive patients in rural areas was 23.88% and it was significantly lower than that in urban areas (36.59%). Age and gender were the factors that independently associated with treatment adherence of hypertensive patients regardless of urban or rural status. The duration of antihypertensive drugs used was identified to be the factor that independently associated with treatment adherence only in urban patients. The subgroups including reduced sodium intake and medication taking had significant effects on treatment adherence in certain factors.
Conclusion: The treatment adherence of Chinese hypertensive patients was low, especially in rural areas. More emphasis should be placed on patients in rural areas. Furthermore, more attention and effective strategies should be designed to address factors affecting treatment adherence in both urban and rural areas. Health programs should focus on education including the importance of taking continuous antihypertensive drugs and low sodium diet.
Keywords: hypertension, treatment adherence, urban-rural difference, China
Introduction
Hypertension (HTN) remains one of the greatest global health care challenges and is estimated to affect one-third of the world’s population by 2025.1 Uncontrolled blood pressure (BP) is a main risk factor for other diseases, such as cardiovascular disease,2 stroke3 and chronic kidney failure.4 The prevalence of HTN continues to grow rapidly especially in developing countries,5 yet it remains inadequately controlled. It was reported that an only 44% of adult US hypertensives are achieving minimal levels of BP(<140/90 mmHg),6 and the control rate among Chinese patients with HTN was only 15.3%.7
Lack of adherence to treatment regimens is considered a major reason for uncontrolled BP.8 Adherence has been defined as the extent to which a person’s behavior-taking medication, following a diet, and/or executing lifestyle changes corresponds with agreed recommendations from a health care provider.9
Factors that affect adherence behavior are diverse.10–12 Demographics and socioeconomic factors are one of the main influencing factors.13 Rural and urban communities have different characteristics of demographics, economic factors and social environments, and may vary in different treatment adherence of hypertensive patients. Rural residents tend to have less education, lower household income, lower insurance coverage, and more barriers to accessing healthcare than urban residents. A study by Tam et al reported that hypertension management was significantly lower in patients from rural areas than in those from urban areas.14 It was revealed in some studies that patients lived in rural areas were less adherent than those living in an urban setting.15,16 However, some other reports found that the adherence rates of hypertensive patients did not differ significantly between rural and urban dwellers.17,18
There were some studies about adherence in Chinese hypertensive populations, in which studies mainly focused on hypertensive patients in urban areas and rural hypertensive patients were often ignored. There were more than 240 million hypertensive patients in China, and the estimated prevalence of hypertension in urban areas and rural areas were 23.4% and 23.1%, respectively.7 There was a large number of hypertensive patients in rural areas, just like that in urban areas. The study data about treatment adherence found in urban areas cannot be extended to rural areas because of the difference of demographic and socioeconomic characteristics between urban and rural populations. Furthermore, there has been limited research to assess differences in hypertensive treatment adherence between rural and urban communities in China.
As a result, we conducted the study in order to compare the adherence and the associated factors for hypertensive patients between urban and rural areas in China in order to better understand adherence disparities.
Participants and Methods
This study was a cross-sectional survey carried out in Xi’an People’s Hospital (Xi’an Fourth Hospital) in Xi’an, China. Patients hospitalized during the period from May 1 to December 31, 2021 were invited to take part in the study if they met the following inclusion criteria. The inclusion criteria were as follows: (1) ≥18 years-old, (2) diagnosis of primary hypertension, (3) undergoing antihypertensive drug therapy, and (4) agreeing to participate in the study. The exclusion criteria included: (1) severe complications of hypertension (eg, severe heart failure and stroke), (2) could not communicate due to physical or mental problems, and (3) pregnant women. Finally, 529 hypertensive patients were randomly selected and were recruited in this study with 328 urban dwellers and 201 rural dwellers.
The study was approved by the ethics committee of Xi’an People’s Hospital (Xi’an Fourth Hospital). Written informed consent from all participants was obtained and all procedures were performed in accordance with the Declaration of Helsinki and policies in China. For illiterate patients, researchers read the informed consent form to them, and all illiterate patients agreed with the contents of the informed consent form by pressing their fingerprints.
Patients’ data referring to sociodemographic factors including age, gender, education level, occupational status, health insurance and part of clinical data such as BP categories were collected by reviewing the electronic medical records. Living conditions and some clinical data including duration of HTN and duration of antihypertensive drugs used which could not be obtained from the electronic medical records were collected through interview by trained clinical pharmacists.
HTN treatment adherence was measured using the Chinese version of the Hill-Bone compliance to high blood pressure therapy scale (HBTS). The scale was developed by Kim et al19 and was translated to Chinese version. The Chinese version of the Hill-Bone scale had been proved to be a valid and reliable instrument for measuring treatment adherence in Chinese hypertensive patients.20 The 14 item scale contains three subgroups: subgroup 1: reduced sodium intake (3 items), subgroup 2: appointment keeping (2 items) and subgroup 3: medication taking (9 items). Each item is a four-point Likert type scale and the score ranged from 1 (all the time) to 4 (none of the time). The overall adherence scores range from 14 to 56, with higher scores indicating better adherence. The score ≥48 is considered as adherence and the score <48 is considered as non-adherence.21 Before trained pharmacists distributed questionnaires to participants, they explained the goal of this study and gave the standardized instructions. The participants were asked to complete the questionnaires independently. For illiterate patients, the questions were read by trained pharmacists to facilitate survey completion.
Data Analysis
Sociodemographic data and clinical characteristics among the hypertensive patients were analyzed using descriptive statistics. The univariate analysis of factors for treatment adherence was conducted by using Chi-square test. Binary logistic regression analysis was used to analyze independent risk factor for treatment adherence of hypertensive patients. General linear model was used to analyze the association of demographic and clinical factors to treatment adherence in each subgroup of the scale. P<0.05 was considered to be statistically significant. All statistical analyses were performed using SPSS version 19 (IBM Corp., Armonk, NY, USA).
Results
The distribution frequencies of sociodemographic and clinical characteristics in urban and rural populations are shown in Table 1. Of the 529 participants, 328 (62.00%) patients were from urban areas and 201 (38.00%) patients were from rural areas (Table 1).
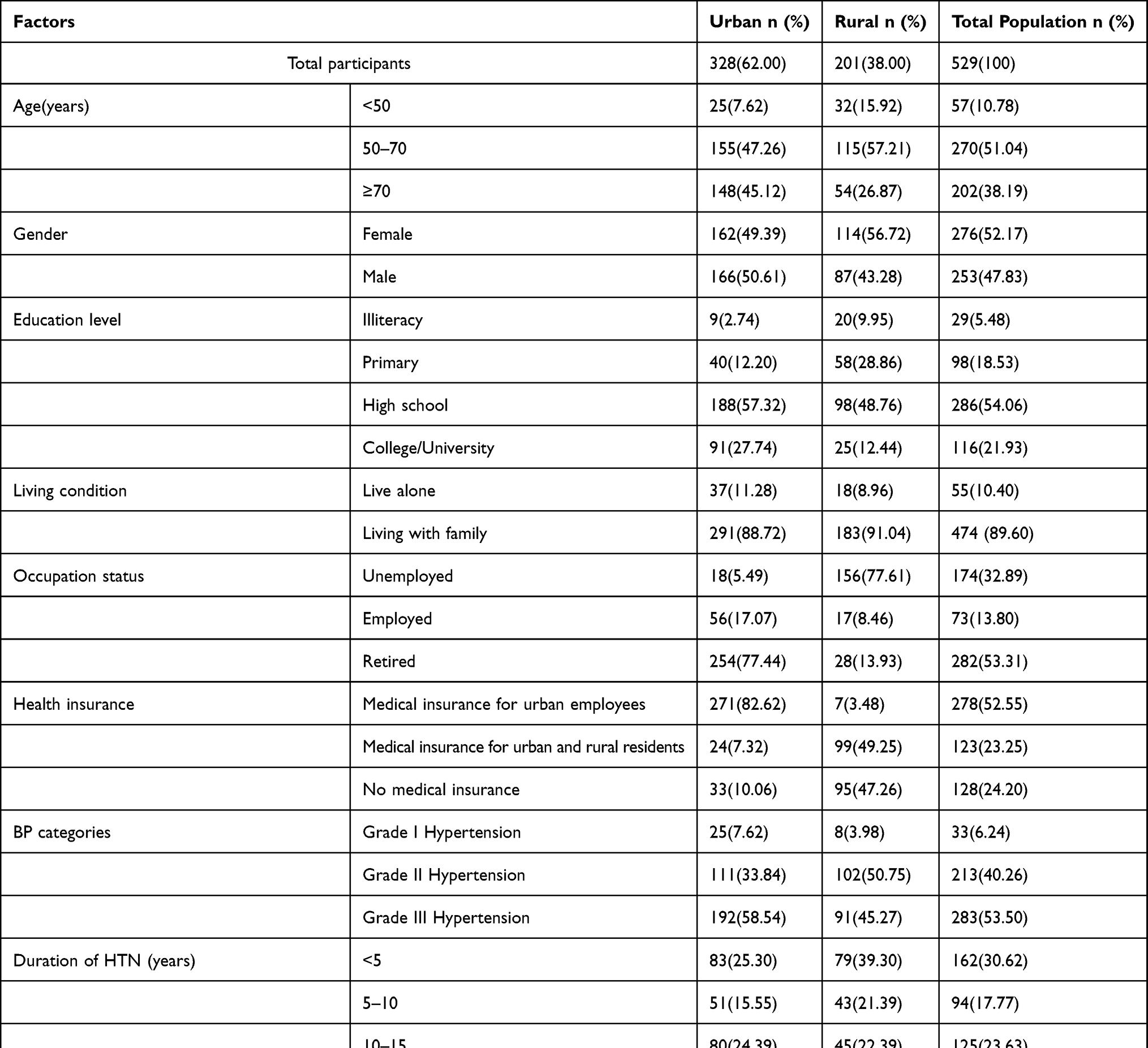 |
Table 1 Demographic and Clinical Characteristics of Hypertension Patients Based on Rural and Urban Populations (n=529) |
There were significant differences in the treatment adherence between urban and rural populations, with the adherence of 36.59% in urban population and 23.88% in rural population (Table 2). The univariate analysis of factors for treatment adherence based on rural and urban populations is provided in Table 2. Five factors including age, gender, occupation status, duration of HTN and duration of antihypertensive drugs used were significantly associated with adherence in urban population. Five factors including age, gender, living condition, duration of HTN and duration of antihypertensive drugs used were significantly associated with adherence in rural population.
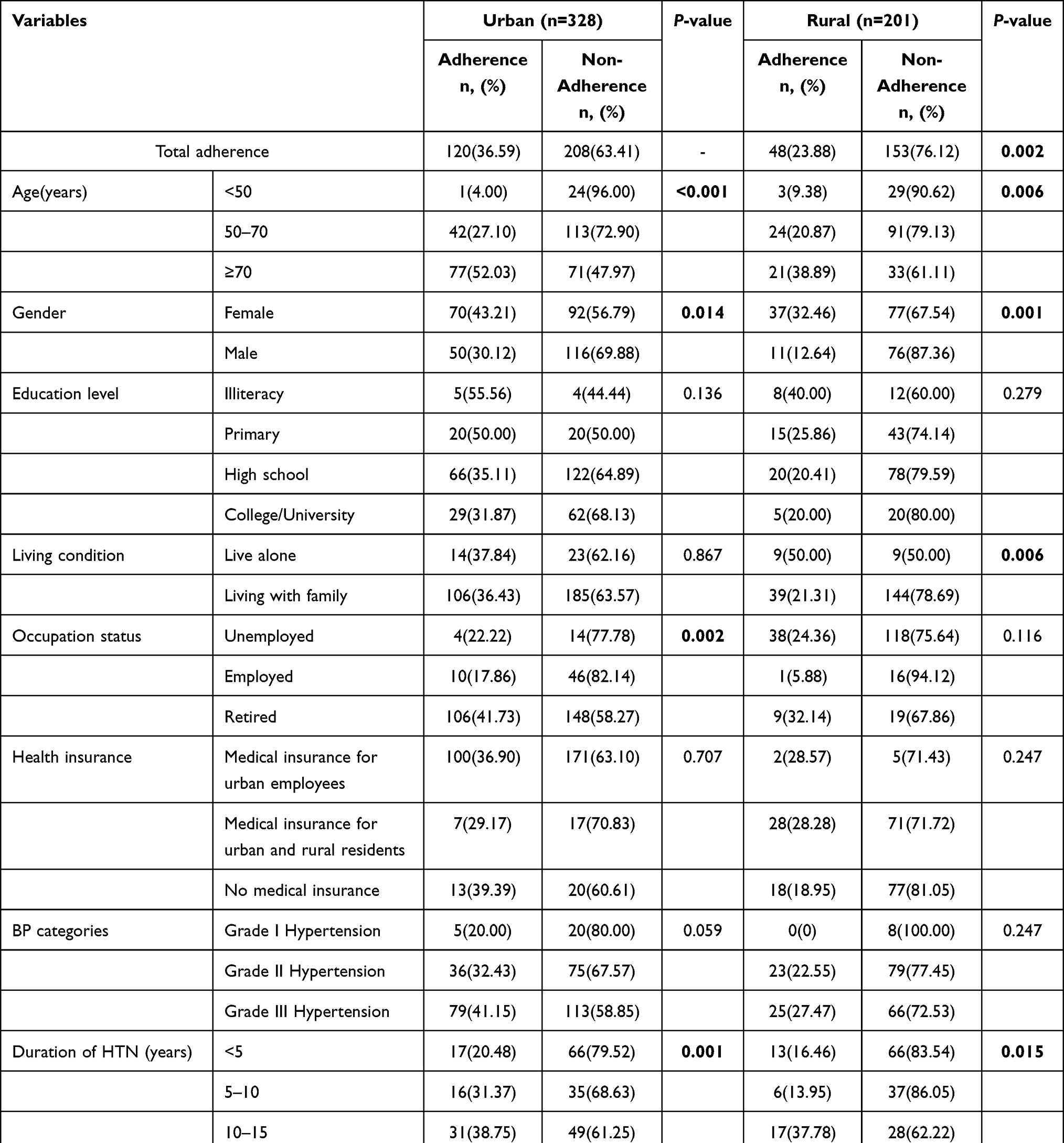 |
Table 2 Univariate Analysis of the Association Between Adherence and Socio-Demographic and Clinical Characteristics Based on Rural and Urban Populations (n=529) |
Table 3 summarized the result of binary logistic regression analysis. Three factors were identified to be independently associated with antihypertensive treatment adherence in urban population; age (P=0.001), gender (P=0.042) and duration of antihypertensive drugs used (P=0.035). Two factors were identified to be independently associated with antihypertensive treatment adherence in rural population; age (P=0.016) and gender (P=0.003). Females were more adherent to their treatment than males in both urban population (P=0.042, odds ratio [OR] =0.602, 95% confidence interval [CI]: 0.369–0.982) and rural population (P=0.003, odds ratio [OR]=0.321, 95% confidence interval [CI]:0.150–0.687). Comparing to patients younger than 50, patients aged 70 and older were more adherent in both urban (P=0.014, OR=0.074, 95% CI 0.009–0.584) and rural (P=0.009, OR=0.172, 95% CI 0.046–0.648) populations. Refer to duration of the time antihypertensive drugs used, the adherence of patients who had used antihypertensive drugs over 20 years was higher than that of patients who used antihypertensive drugs with other years (P=0.004, OR=0.317, 95% CI: 0.146–0.689) in urban patients.
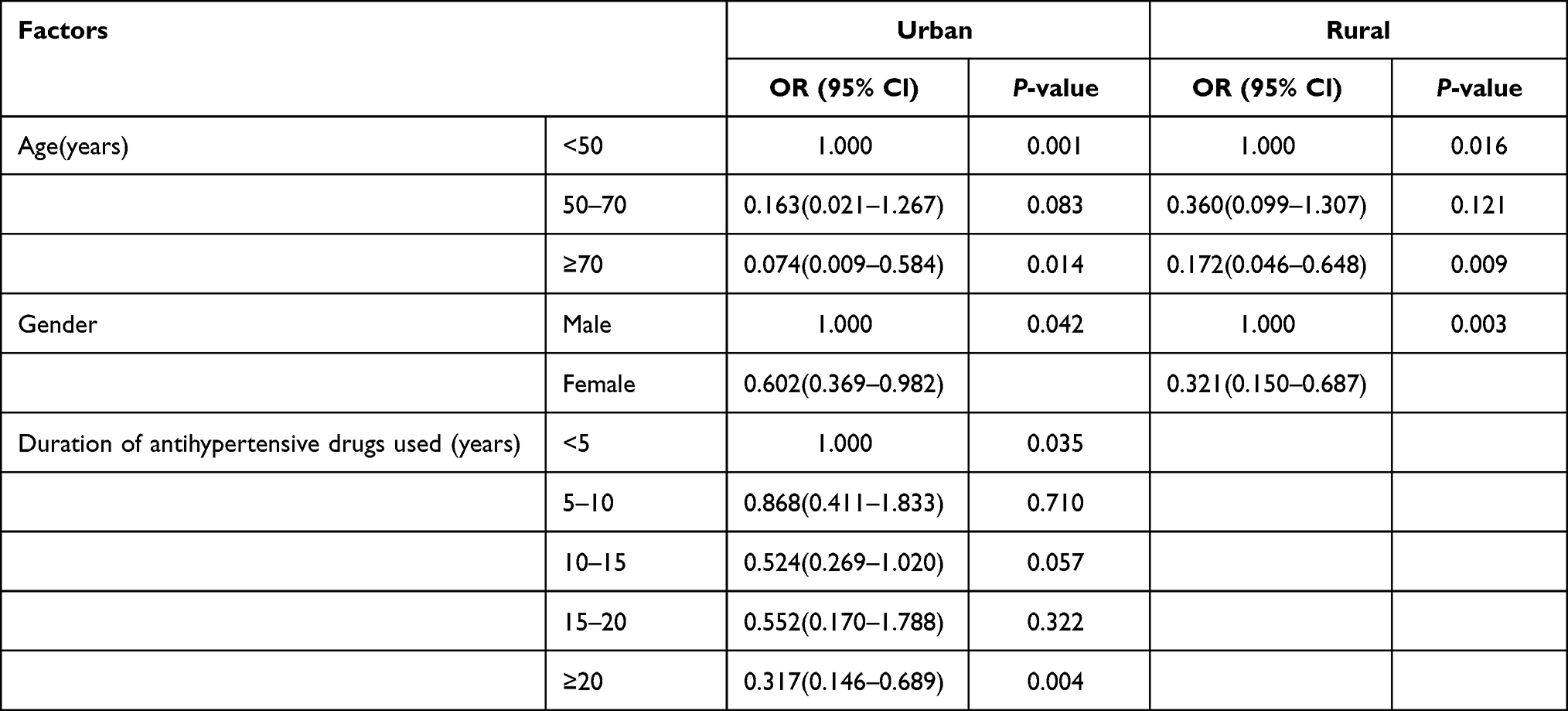 |
Table 3 Binary Logistic Regression Analysis of Factors Associated with Treatment Adherence in Urban and Rural Populations |
The results of the general linear model analysis in both urban and rural populations were shown in Table 4. Among the factors independently associated with adherence, different factors had different effects on certain subgroups of adherence. For example, we found that the higher adherence of patients older than 70 was mainly in subgroup 1 (reduced sodium intake) and subgroup 3 (medication taking) in both urban (subgroup 1: P=0.009, subgroup 3: P=0.002) and rural (subgroup 1: P=0.037, subgroup 3: P<0.001) populations. It means the patients aged older than 70 in both urban and rural areas were more adherent in the aspect of medication taking and control sodium intake. Our study also found that the higher adherence of females was mainly in subgroup 1 (reduced sodium intake) in both urban (P=0.003) and rural (P=0.008) areas. Duration of antihypertensive drugs used was independently associated with antihypertensive treatment adherence in urban population and the treatment adherence was better for those who have taken the antihypertensive drugs for more than 20 years. The influence of drug used time on adherence was mainly reflected in subgroup 3 (medication taking) (P=0.011).
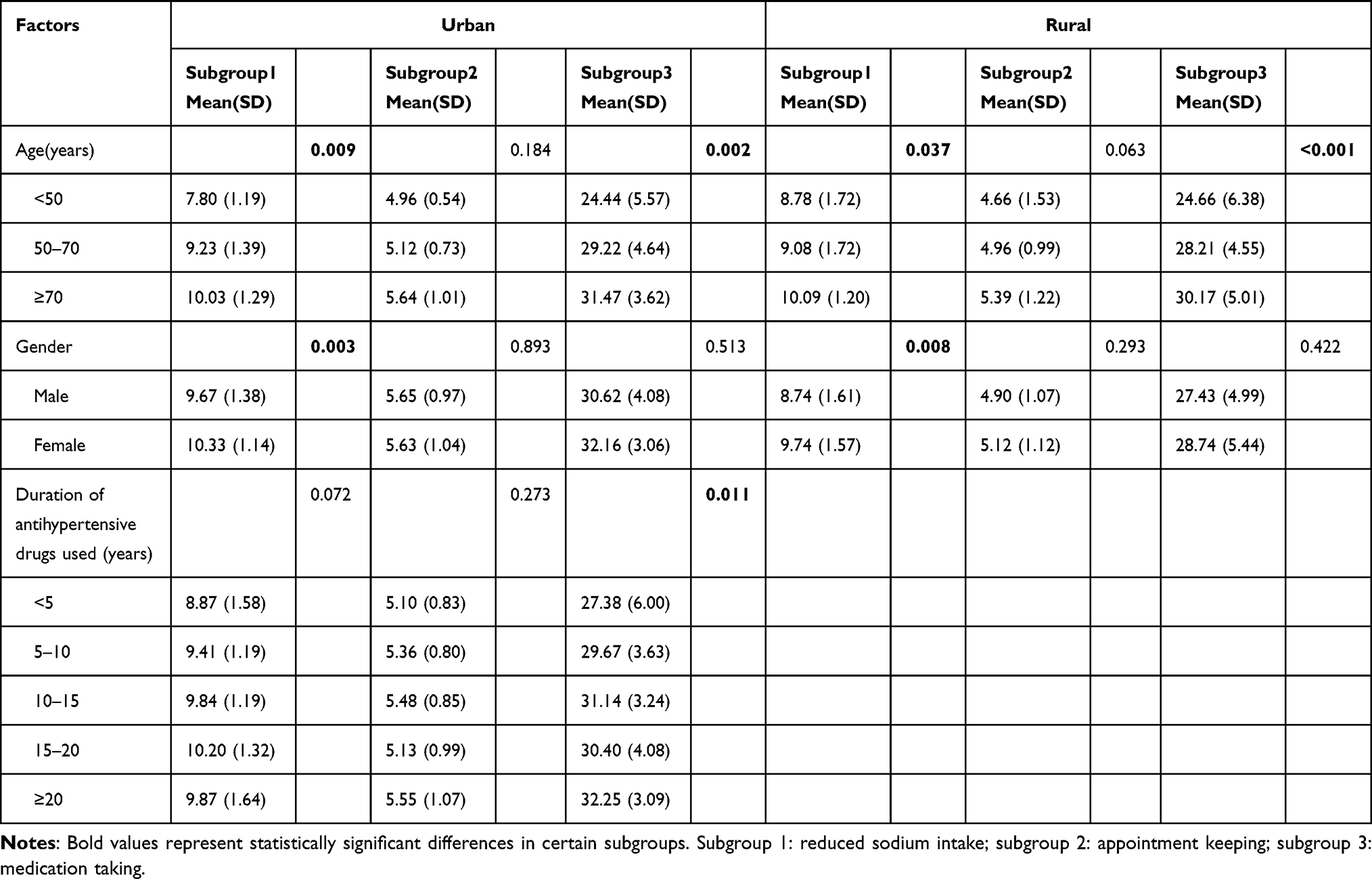 |
Table 4 General Linear Model Analysis in Certain Subgroup of Risk Factors in Urban and Rural Populations |
Discussion
The regional, economic and cultural differences between rural and urban areas may lead to differences in the treatment adherence of patients with hypertension between rural and urban populations. Understanding rural-urban differences in treatment adherence and its influence factors is an important step in determining strategies targeted to improve adherence for hypertensive people in different place of residents. The finding of this study showed that the rural hypertensive patients reported poorer treatment adherence than the urban ones. The result was in agreement with some earlier studies.16,22,23 This was explained by the high gap in socio-economic, cultural and education aspects between urban and rural areas in China. Economic status was one of the factors affecting adherence of hypertensive patients and lack of financial resources was a major barrier to adherence24. It was reported that patients with a low socio-economic level were seven times more likely to be poor-adherence than those with a high socio-economic level.25
Difference in educational levels might also be the possible reasons for different adherence,16 which can be explained by the fact that urban dwellers are more likely to be more educated than the rural population and have more knowledge of hypertension. Increased adherence proportion was observed as knowledge about hypertension improves.26 Patients with good knowledge about the disease and its complications were seven times more likely to have good adherence to medication.27
It is reported that lacking advice regarding hypertension management was also an obstacle to treatment adherence for rural population.14 Medication used knowledge and lifestyle recommendations offered by healthcare providers was insufficient for rural residents due to the differences in availability of healthcare services across geographical areas. Thus, improving the distribution of healthcare providers in rural areas and effectively delivering the hypertension-related health information for rural dwellers is a useful way to improve treatment adherence. A face-to-face medication education and regular medication follow-up by healthcare providers for hypertensive patients are effective methods for information delivery.28 Furthermore, mobile health messaging invention are also seen as the useful ways to educate, support, and remind patients in order to improve their adherence.29
Our study showed more adherence among elderly both in rural and urban patients, where people of 70 years old or older were more adherent to treatment than patients of less than 50 years old. This finding was consistent with some previous studies30,31 but opposite to a study conducted on a Poland population, which showed that older age was determinant of the lower adherence.32 There was also a significant association between age and adherence to both a low-salt diet and medication adherence regardless of urban or rural populations (Table 4). This relationship indicated that people older than 70 had a more rigorous adherence to a low-salt diet and had better adherence to their medication regimens than the younger groups. The possible reason is that as age increases, the patients become more sensitive about their disease and start to take healthy diets and take medications regularly in order to control blood pressure.
In terms of gender, females with hypertension adhered more to treatment regardless of rural or urban status with a statistically significant difference, which was consistent with some previous studies.15,28,33 Refer to the subgroups, females in both urban (P=0.003) and rural (P=0.008) areas were more adherent than males mainly in the subgroup of reducing sodium intake. This finding was in line with the previous study that reported participants who were adhered to a low-salt diet were more likely to be older and women as compared to the non-adherent participants.34 Prolonged modest reduction in salt intake induces a relevant fall in blood pressure in hypertensive individuals irrespective of sex.35 The WHO advises every adult should consume less than 5 grams (2000 mg) of sodium each day.36 However, the salt intake is considerably above the recommended level in China and most dietary sodium intake is from salt added in home cooking.37 Our finding showed that females with hypertension consumed less salt than males. This may be related to the fact that females have more knowledge of controlling hypertension and pay more attention to healthy diet.
We also found that the longer the duration they were using antihypertensive drugs, the more adherent were the patients in urban populations, but no relationship was found in rural populations. Some studies came to the same conclusion.21,38 In the study, differences in treatment adherence with hypertension caused by the duration of antihypertensive drugs used were mainly reflected in medication taking (subgroup 3). It was indicated that as the time of taking hypertensive medication increased, the medication adherence of patients increased. A possible reason for this is that with the extension of treatment time, the hypertensive patients become knowledgeable about hypertension and its risks. It leads patients gradually accept the fact that they are supposed to take their medication every day, so they have better medication-taking behaviors.
The limitations of the study were that samples from the urban or rural areas were conveniently selected from a hospital in one region rather than randomly sampled from multiregional urban or rural areas. Moreover, the measurement of treatment adherence was based on self-reported questionnaires, which may introduce recall bias. In addition, the sample size was small. Therefore, larger scale investigations of random sampling and in wider areas should be carried out in the future. Finally, factors that affect adherence behavior are diverse and this study only included part of the possible influencing factors. Some other factors such as the comorbidities, number of medications used and frequency of medication were not included in this study.
Conclusions
In our study, the prevalence of non-adherence to treatment adherence of hypertensive patients in rural areas was significantly higher than that in urban areas. Age and gender were found to be the main factors affecting treatment adherence in both urban and rural hypertensive patients. The duration of hypertensive drug used was found to affect the treatment adherence only in urban patients. The subgroups including reduced sodium intake and medication taking had significant effects on treatment adherence in certain factors. These findings implied that in order to improve adherence of hypertensive patients more emphasis should be placed on patients in rural areas. Refer to the factors influencing the adherence, more emphasis should be placed on men and young people regardless of rural or urban areas, and people with short duration of antihypertensive drugs used in urban areas. Health programs should focus on education including the importance of taking continuous antihypertensive drugs and low sodium diet.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Oliveros E, Patel H, Kyung S, et al. Hypertension in older adults: assessment, management, and challenges. Clin Cardiol. 2020;43(2):99–107.
2. Perumareddi P. Prevention of Hypertension Related to Cardiovascular Disease. Prim Care. 2019;46(1):27–39.
3. Furie K. Epidemiology and Primary Prevention of Stroke. Continuum. 2020;26(2):260–267.
4. Stompór T, Perkowska-Ptasińska A. Hypertensive kidney disease: a true epidemic or rare disease? Pol Arch Intern Med. 2020;130(2):130–139.
5. Schutte AE, Srinivasapura Venkateshmurthy N, Mohan S, Prabhakaran D. Hypertension in Low- and Middle-Income Countries. Circ Res. 2021;128(7):808–826.
6. Milani RV, Lavie CJ, Ventura HO. New aspects in the management of hypertension in the digital era. Curr Opin Cardiol. 2021;36(4):398–404.
7. Wang Z, Chen Z, Zhang L, et al. Status of Hypertension in China: results From the China Hypertension Survey, 2012-2015. Circulation. 2018;137(22):2344–2356.
8. Piercefield EW, Howard ME, Robinson MH, Kirk CE, Ragan AP, Reese SD. Antihypertensive medication adherence and blood pressure control among central Alabama veterans. J Clin Hypertens. 2017;19(5):543–549.
9. De Geest S, Sabaté E. Adherence to long-term therapies: evidence for action. Eur J Cardiovasc Nurs. 2003;2(4):323.
10. Macquartde Terline D, Kane A, Kramoh KE, et al. Factors associated with poor adherence to medication among hypertensive patients in twelve low and middle income Sub-Saharan countries. PLoS One. 2019;14(7):e0219266.
11. Aberhe W, Mariye T, Bahrey D, et al. Prevalence and factors associated with uncontrolled hypertension among adult hypertensive patients on follow-up at Northern Ethiopia, 2019: cross-sectional study. Pan Afr Med J. 2020;36:187.
12. Lelong H, Blacher J, Baudry J, et al. Combination of Healthy Lifestyle Factors on the Risk of Hypertension in a Large Cohort of French Adults. Nutrients. 2019;11:7.
13. Lee GK, Wang HH, Liu KQ, Cheung Y, Morisky DE, Wong MC. Determinants of medication adherence to antihypertensive medications among a Chinese population using Morisky Medication Adherence Scale. PLoS One. 2013;8(4):e62775.
14. Tam HL, Chung SF, Wang Q. Urban-rural disparities in hypertension management among middle-aged and older patients: results of a 2018 Chinese national study. Chronic Illn. 2022;2:17423953221102627.
15. Pan J, Wu L, Wang H, et al. Determinants of hypertension treatment adherence among a Chinese population using the therapeutic adherence scale for hypertensive patients. Medicine. 2019;98(27):e16116.
16. Teshome DF, Bekele KB, Habitu YA, Gelagay AA. Medication adherence and its associated factors among hypertensive patients attending the Debre Tabor General Hospital, northwest Ethiopia. Integr Blood Press Control. 2017;10:1–7.
17. Arbuckle C, Tomaszewski D, Aronson BD, et al. Evaluating Factors Impacting Medication Adherence Among Rural, Urban, and Suburban Populations. J Rural Health. 2018;34(4):339–346.
18. Murphy GK, McAlister FA, Weir DL, Tjosvold L, Eurich DT. Cardiovascular medication utilization and adherence among adults living in rural and urban areas: a systematic review and meta-analysis. BMC Public Health. 2014;14:544.
19. Kim MT, Hill MN, Bone LR, Levine DM. Development and testing of the Hill-Bone Compliance to High Blood Pressure Therapy Scale. Prog Cardiovasc Nurs. 2000;15(3):90–96.
20. Pan J, Hu B, Wu L, Wang H, Lei T, Liu Z. The Translation, Reliability and Validity of the Chinese Version of the Hill-Bone Compliance to High Blood Pressure Therapy Scale in Adults with Hypertension. Patient Prefer Adherence. 2020;14:1853–1860.
21. Pan J, Hu B, Wu L, Li Y. The Effect of Social Support on Treatment Adherence in Hypertension in China. Patient Prefer Adherence. 2021;15:1953–1961.
22. Hussein A, Awad MS, Mahmoud HEM. Patient adherence to antihypertensive medications in upper Egypt: a cross-sectional study. Egypt Heart J. 2020;72(1):29.
23. Liu J, Yang Y, Zhou J, et al. Prevalence and Associated Factors of Compliance Behaviors among Middle-Aged and Older Hypertensive Patients in China: results from the China Health and Retirement Longitudinal Study. Int J Environ Res Public Health. 2020;17:19.
24. Mamaghani EA, Hasanpoor E, Maghsoodi E, Soleimani F. Barriers to Medication Adherence among Hypertensive Patients in Deprived Rural Areas. Ethiop J Health Sci. 2020;30(1):85–94.
25. Gniwa Omezzine R, Akkara A, Abdelkafi Koubaa A, Belguith Sriha A, Rdissi A, Amamou K. Predictors of Poor Adherence to Hypertension Treatment. Tunis Med. 2019;97(4):564–571.
26. Ayodapo AO, Elegbede OT, Omosanya OE, Monsudi KF. Patient Education and Medication Adherence among Hypertensives in a Tertiary Hospital, South Western Nigeria. Ethiop J Health Sci. 2020;30(2):243–250.
27. Algabbani FM, Algabbani AM. Treatment adherence among patients with hypertension: findings from a cross-sectional study. Clin Hypertens. 2020;26:18.
28. Pan J, Lei T, Hu B, Li Q. Post-discharge evaluation of medication adherence and knowledge of hypertension among hypertensive stroke patients in northwestern China. Patient Prefer Adherence. 2017;11:1915–1922.
29. Steinman L, Heang H, van Pelt M, et al. Facilitators and Barriers to Chronic Disease Self-Management and Mobile Health Interventions for People Living With Diabetes and Hypertension in Cambodia: qualitative Study. JMIR Mhealth Uhealth. 2020;8(4):e13536.
30. Choi HY, Oh IJ, Lee JA, et al. Factors Affecting Adherence to Antihypertensive Medication. Korean J Fam Med. 2018;39(6):325–332.
31. Rolnick SJ, Pawloski PA, Hedblom BD, Asche SE, Bruzek RJ. Patient characteristics associated with medication adherence. Clin Med Res. 2013;11(2):54–65.
32. Uchmanowicz B, Chudiak A, Uchmanowicz I, Rosińczuk J, Froelicher ES. Factors influencing adherence to treatment in older adults with hypertension. Clin Interv Aging. 2018;13:2425–2441.
33. Khanam MA, Lindeboom W, Koehlmoos TL, Alam DS, Niessen L, Milton AH. Hypertension: adherence to treatment in rural Bangladesh–findings from a population-based study. Glob Health Action. 2014;7:25028.
34. Hu H, Li G, Arao T. Prevalence rates of self-care behaviors and related factors in a rural hypertension population: a questionnaire survey. Int J Hypertens. 2013;2013:526949.
35. Grillo A, Salvi L, Coruzzi P, Salvi P, Parati G. Sodium Intake and Hypertension. Nutrients. 2019;11(9):854.
36. WHO Guidelines Approved by the Guidelines Review Committee. Guideline: Potassium Intake for Adults and Children. Geneva: World Health Organization Copyright © 2012. World Health Organization; 2012.
37. Xian J, Zeng M, Zhu R, et al. Design and implementation of an intelligent monitoring system for household added salt consumption in China based on a real-world study: a randomized controlled trial. Trials. 2020;21(1):349.
38. Yue Z, Bin W, Weilin Q, Aifang Y. Effect of medication adherence on blood pressure control and risk factors for antihypertensive medication adherence. J Eval Clin Pract. 2015;21(1):166–172.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.