Back to Journals » International Journal of Women's Health » Volume 17
Exploring the Recurrence Risk Factors and Development of a Nomogram Prediction Model for Uterine Fibroid Patients Post-Myomectomy Based on Patient Medical Records
Received 3 January 2025
Accepted for publication 3 April 2025
Published 23 April 2025 Volume 2025:17 Pages 1157—1163
DOI https://doi.org/10.2147/IJWH.S515545
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Caixia Li,1,* Liumin Li,1,* Yingchun Hu2
1Department of Gynecology, Xiaolan People’s Hospital of ZhongShan (The Fifth People’s Hospital of ZhongShan), Zhongshan City, Guangdong Province, 528415, People’s Republic of China; 2Department of Nursing Care, Xiaolan People’s Hospital of ZhongShan (The Fifth People’s Hospital of ZhongShan), Zhongshan City, Guangdong Province, 528415, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yingchun Hu, Email [email protected]
Objective: This study aims to investigate the risk factors contributing to the recurrence of uterine fibroids in patients undergoing laparoscopic myomectomy, providing a basis for clinical treatment.
Methods: A retrospective analysis was conducted on 378 patients who underwent laparoscopic myomectomy between January 2022 and August 2023 and were subsequently followed up. Based on the recurrence status 6 months post-operation, patients were divided into a recurrence group (43 cases) and a non-recurrence group (335 cases). Clinical data of both groups were analyzed using univariate analysis, and factors statistically significant in univariate analysis were further evaluated through multivariate logistic regression to identify independent risk factors for recurrence post-laparoscopic myomectomy.
Results: Univariate analysis indicated that the proportion of patients with ≥ 2 fibroids, intramural fibroids, and preoperative serum C-reactive protein (CRP) levels ≥ 4.67 mg/L was significantly higher in the recurrence group (all P< 0.05). Multivariate logistic regression analysis revealed that having ≥ 2 fibroids, a uterine size ≥ 14 gestational weeks, intramural fibroids, and preoperative serum CRP levels ≥ 4.67 mg/L were independent risk factors for recurrence post-laparoscopic myomectomy (OR=1.855, 1.038, 1.917, 1.208, 1.154, respectively; all P< 0.05).
Conclusion: The presence of ≥ 2 fibroids, intramural fibroids, and preoperative serum CRP levels ≥ 4.67 mg/L are identified as independent risk factors for the recurrence of uterine fibroids post-laparoscopic myomectomy. Regular follow-ups should be conducted for patients with these risk factors to timely detect potential recurrence risks and implement preventive and therapeutic measures accordingly. The number of fibroids, their location, and preoperative serum CRP level have a strong predictive ability for recurrence after laparoscopic myomectomy, effectively identifying patients with recurrence while excluding those without recurrence.
Keywords: uterine fibroids, laparoscopic myomectomy, recurrence, risk factors
Uterine fibroids rank among the most common benign tumors in gynecology, impacting millions of women worldwide.1 While generally benign, their growth can lead to significant symptoms including pain, bleeding, infertility, and a marked decrease in quality of life.2 A variety of treatment options exist, with surgical removal being one of the most frequently employed methods. However, post-surgical recurrence remains a significant challenge in the management of uterine fibroids, with recurrence rates reaching up to 50%.3,4 Identifying the risk factors for post-operative recurrence is crucial for improving patient prognosis and guiding clinical practice. Previous research has focused on identifying clinical and pathological characteristics of patients, such as the size, number, and location of fibroids, as well as patient age and ethnicity.5 However, the predictive value of these factors remains limited and varies across different populations. Furthermore, the role of preoperative serum C-reactive protein (CRP) levels, a marker of inflammation, in predicting post-operative recurrence has not been fully explored.6 Therefore, developing a predictive model that takes into account multiple risk factors could provide clinicians with a more accurate assessment of recurrence risk, thereby offering personalized treatment plans to patients.
This study aims to analyze patient medical records to investigate the risk factors for post-operative recurrence in patients with uterine fibroids and to develop a risk prediction model based on these factors. Through this research, we aim to provide a more scientific and personalized basis for the post-operative management of patients with uterine fibroids, thereby reducing recurrence rates and improving patient quality of life. This study seeks to fill gaps in the existing literature and may guide future clinical practices, opening new avenues for the treatment and management of uterine fibroids.
Materials and Methods
General Information
This study retrospectively analyzed the clinical data of 378 patients who underwent laparoscopic myomectomy at the People’s Hospital from January 2022 and August 2023 and were followed up postoperatively. Based on recurrence during the follow-up period, patients were divided into a recurrence group (43 cases) and a non-recurrence group (335 cases). Recurrence criteria were defined as the emergence of new uterine fibroids with a diameter >1 cm confirmed by pelvic ultrasound, gynecological examination, or surgery 6 months postoperatively. Inclusion criteria were as follows: patients in both groups met the related diagnostic criteria specified in the “Clinical Disease Diagnosis and Therapeutic Effect Judgment Standards” and were diagnosed with uterine fibroids via pathological examination; postoperative histopathological examination confirmed the diagnosis of uterine leiomyoma; patients had complete clinical and follow-up data; all underwent laparoscopic myomectomy; and postoperative imaging evaluations showed no residual fibroids. Exclusion criteria included patients with a history of uterine fibroid removal surgery; patients who had been treated with medications for uterine fibroids; and surgical procedures involving open surgery, combined laparoscopic and hysteroscopic myomectomy, or sole hysteroscopic myomectomy. The study was approved by the institutional medical ethics committee.
Surgical Procedure
Under general anesthesia and in the bladder lithotomy position, routine disinfection and draping were performed, followed by catheterization and the placement of a uterine manipulator. Three abdominal punctures were made for the insertion of the laparoscope and surgical instruments. Pitressin was injected at the fibroid junction to promote uterine contraction. The myometrial surface layer over the fibroid was incised with an electric hook, the fibroid capsule was isolated, and the fibroid was grasped with a clamping forceps for blunt dissection and complete removal.7 Continuous layered suturing was used to close the uterine incision, followed by inspection of the surgical field for hemostasis and pelvic cavity irrigation before suturing the abdominal incisions. All patients were regularly followed up for 6 months post-surgery to observe for recurrence.
Observation Indicators
(1) Univariate analysis was performed on the clinical data of both groups, including patient age, body mass index (BMI), age at menarche, number of fibroids, fibroid size, uterine size, fibroid location, use of ultrasound during surgery, preoperative serum hemoglobin (Hb) level, preoperative serum C-reactive protein (CRP) level, number of pregnancies before surgery, pathological type, postoperative treatment with gonadotropin-releasing hormone agonists (GnRH-a), and postoperative pregnancy and childbirth history.8 Serum Hb and CRP levels were measured as follows: approximately 4 mL of fasting venous blood was drawn preoperatively, centrifuged (3000 rpm, 10 minutes), and the serum was separated for serum Hb level determination with an automatic cell counter and serum CRP level measurement by immunoturbidimetry. (2) Multivariate logistic regression analysis was employed to compare variables with statistically significant differences in univariate analysis and identify independent risk factors for recurrence following laparoscopic myomectomy.
Statistical Methods
Data were analyzed using R version 3.5 software. Categorical data were presented as [number (%)] and analyzed using the χ2 test. Risk factor analysis was conducted using multivariate logistic regression. A P-value <0.05 was considered statistically significant.
Results
Univariate Analysis
The univariate analysis revealed that the proportions of patients with ≥2 fibroids, intramural fibroids, and preoperative serum CRP levels ≥4.67 mg/L were significantly higher in the recurrence group compared to the non-recurrence group, with statistically significant differences (all P<0.05). These findings are detailed in Table 1.
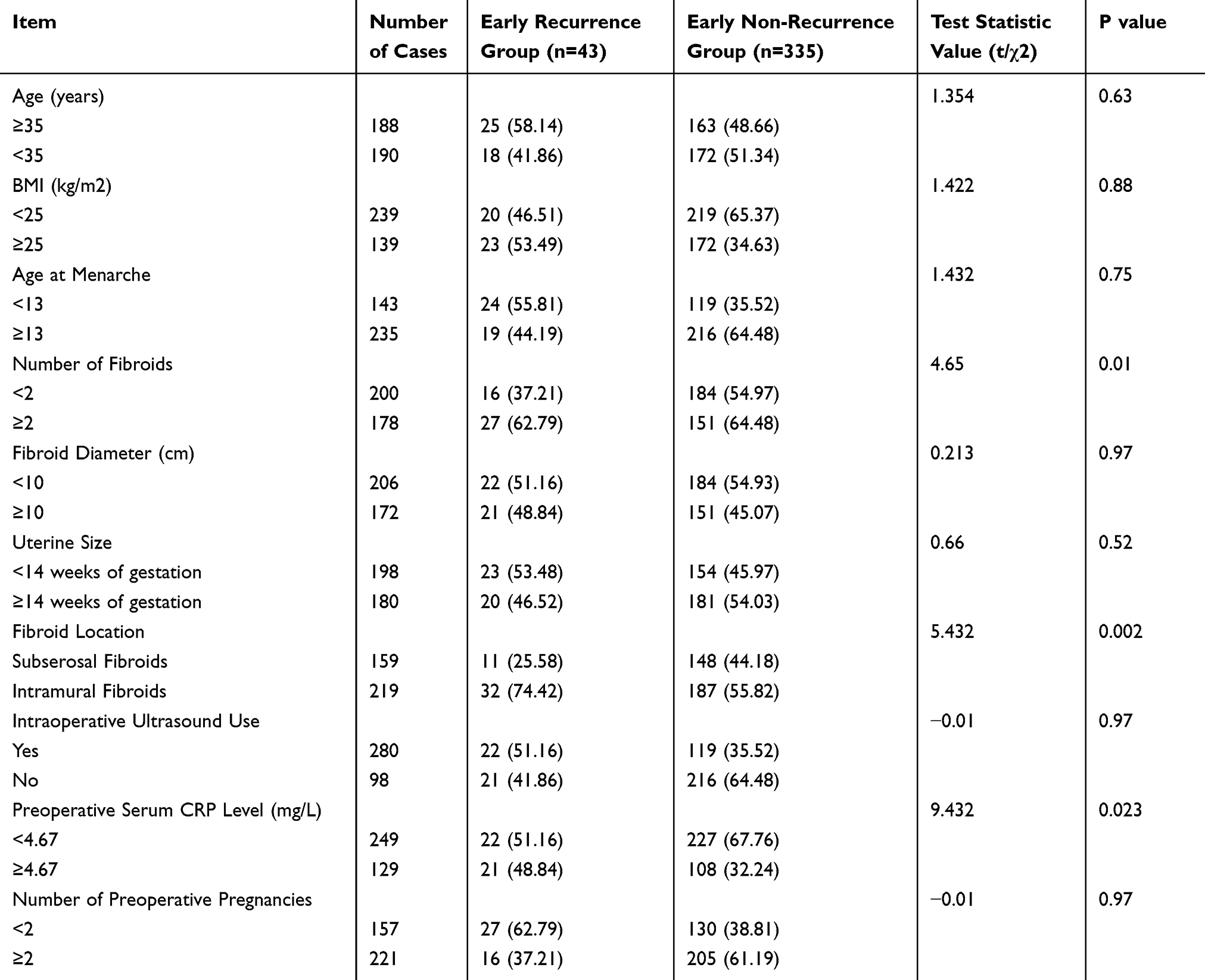 |
Table 1 Comparison of Clinical Data and Electrocardiogram Information Between Early Recurrence Group and Early Non-Recurrence Group |
Multivariate Logistic Regression Analysis
Using the recurrence after laparoscopic myomectomy as the dependent variable, and the indicators with statistically significant differences in the univariate analysis as independent variables, a multivariate logistic regression model was applied. The results indicated that having ≥2 fibroids, intramural fibroids, and preoperative serum CRP levels ≥4.67 mg/L were identified as risk factors for recurrence after laparoscopic myomectomy (OR=1.038, 1.321, 1.543, respectively), with each showing statistically significant differences (all P<0.05). These findings are presented in Table 2.
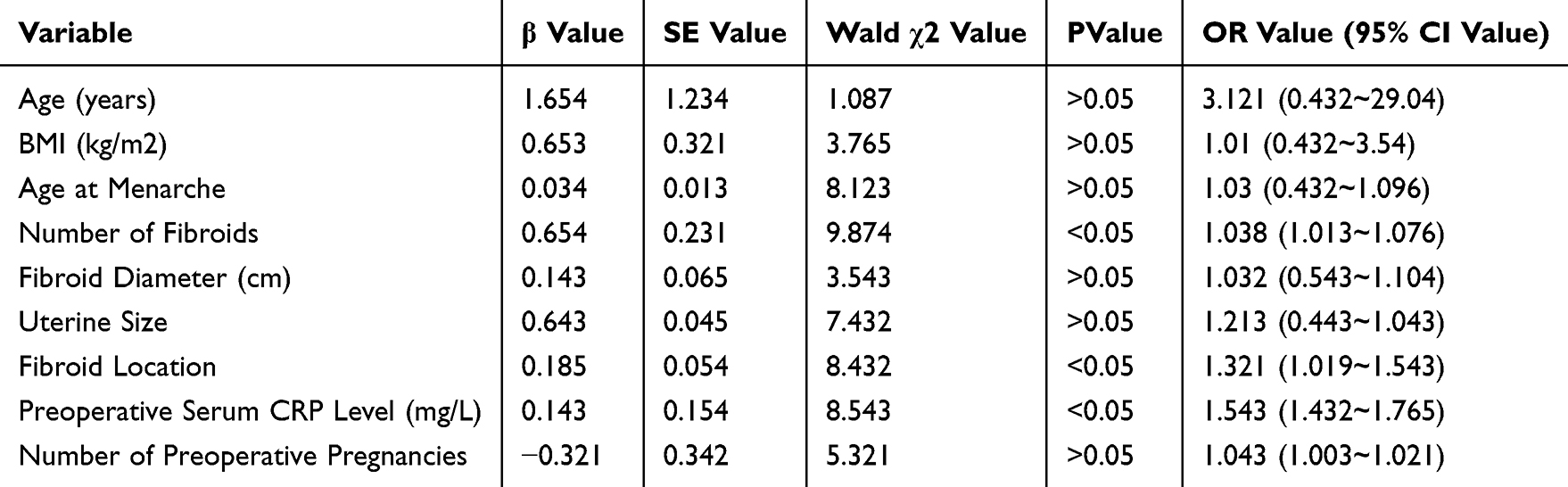 |
Table 2 Multivariate Unconditional Logistic Regression Analysis of Factors Affecting Recurrence After Laparoscopic Myomectomy in Patients with Uterine Fibroids |
Despite no statistically significant differences in basic demographic information and related medical histories between the two groups, the most significant indicators identified in both univariate and multivariate analyses were the number of fibroids, location of fibroids, and preoperative serum CRP level (mg/L). These variables were further analyzed using logistic regression based on statistical outcomes, and ROC curves were drawn. The results suggested that the area under the ROC curve (AUC) for predicting recurrence after laparoscopic myomectomy based on the number of fibroids was 0.863 (95% CI: 0.826 to 0.901, P<0.001), for fibroid location was 0.749 (95% CI: 0.580 to 0.697, P<0.001), and for preoperative serum CRP level was 0.839 (95% CI: 0.797 to 0.881, P<0.001). The combined predictive value of the number of fibroids, fibroid location, and preoperative serum CRP level for recurrence after laparoscopic myomectomy had an AUC of 0.903, with a sensitivity of 73.7% and a specificity of 84.2% (Table 3, Figure 1).
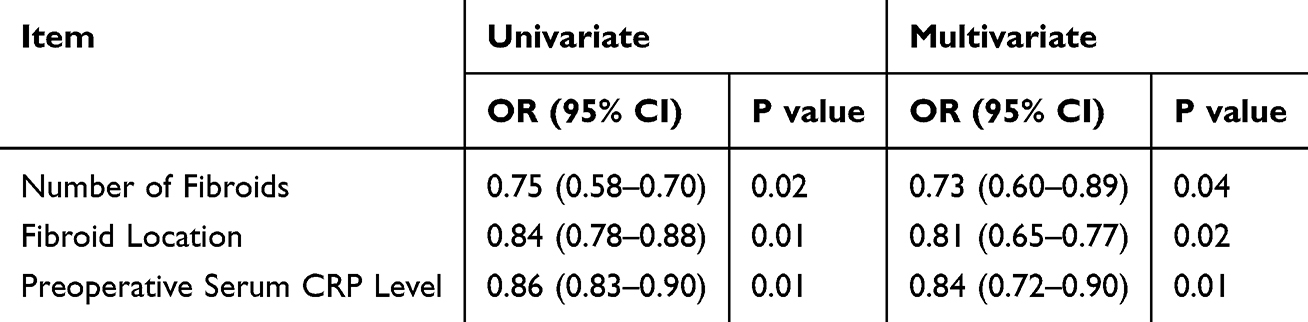 |
Table 3 Logistic Regression Analysis of Predictive Factors for Recurrence After Laparoscopic Myomectomy |
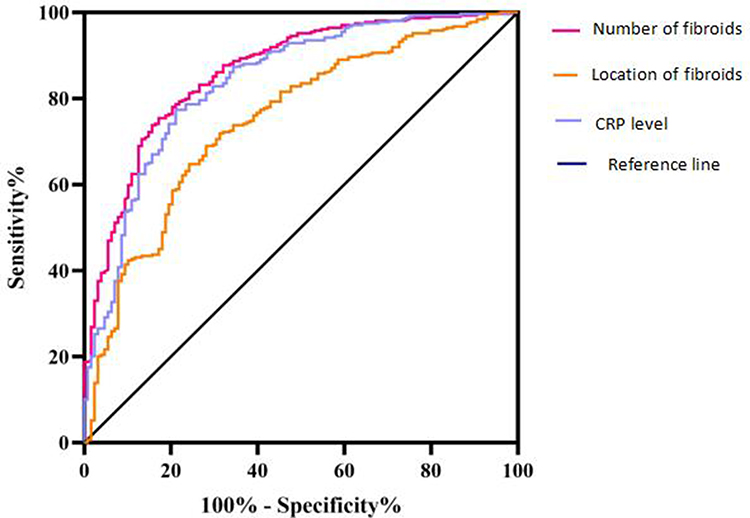 |
Figure 1 Illustrates the Receiver Operating Characteristic (ROC) curves for predicting recurrence after laparoscopic myomectomy based on three indicators: number of fibroids, location of fibroids, and preoperative serum CRP levels. |
Discussion
Uterine fibroids are most prevalent among women of reproductive age and are hormone-dependent benign tumors. Initially, the condition is often asymptomatic, lacking distinct symptoms or signs.9,10 As it progresses, some patients may experience abdominal pain and irregular vaginal bleeding. Fibroid size can rapidly increase during pregnancy or with the use of oral contraceptives but may decrease postpartum or upon discontinuation of contraceptives.11 After menopause, fibroid growth ceases, indicating a close relationship between the development of uterine fibroids and the internal levels of estrogen and progesterone. If left untreated, uterine fibroids can progress to malignancy, reducing the patient’s quality of life. Many factors influence the recurrence of uterine fibroids after surgery, including incomplete removal during surgery, leading to regrowth under hormonal influences, or the persistence of pathological factors post-surgery.12 Despite numerous studies on post-myomectomy recurrence, a consensus has not been reached. This study focuses on identifying risk factors for recurrence after laparoscopic myomectomy in patients with uterine fibroids to provide a basis for targeted preventative measures and reference for future research on preventing recurrence.13
Multivariate logistic regression analysis in this study identified the number of fibroids ≥2, uterine size ≥14 weeks of gestation, intramural fibroids, and preoperative serum CRP level ≥4.67 mg/L as risk factors for recurrence post-laparoscopic myomectomy. This may be due to the earlier onset of menstruation leading to earlier peaks of estrogen, more menstrual cycles, and higher hormone levels, making early menarche an independent risk factor for recurrence.14 Patients with early menarche should be encouraged to have regular postoperative follow-ups to detect potential recurrence early and possibly undergo medical intervention with mifepristone or short-acting oral contraceptives to improve prognosis and avoid rehospitalization and surgery.15 The fundamental cause of high recurrence risk is incomplete fibroid removal and postoperative residuals. The more fibroids identified during surgery, the harder complete removal becomes, with small fibroids often being missed.4,16 Additionally, a higher number of fibroids indicates more pathological factors in the patient, and surgery alone cannot remove these factors, thus increasing the risk of postoperative recurrence. To avoid recurrence, clinicians should conduct thorough gynecological examinations using color Doppler ultrasound and select highly skilled surgeons for laparoscopic operations to minimize the risk of residual fibroids and improve surgical outcomes.17,18 A uterine size ≥14 weeks suggests a larger uterine morphology, narrowing the surgical field under laparoscopy and limiting operational space, thus increasing the risk of injuring surrounding tissues and perioperative complications. Therefore, careful preoperative pelvic examination, understanding the size and location of fibroids, and formulating the best surgical plan are crucial. Preoperative medication to reduce gonadotropin release and shrink tumor size can also create more operational space, minimizing damage to surrounding tissues and improving patient outcomes.19,20 Intramural fibroids, being enclosed by myometrium on all sides, are easily overlooked and more likely to be left behind, increasing the risk of postoperative recurrence. CRP, which rises sharply in the plasma during infection or tissue damage, can activate complement and enhance phagocytosis. Abnormal CRP levels indicate an inflammatory response, and long-term inflammation in patients with uterine fibroids can exacerbate the proliferation of spindle smooth muscle cells and fibrous connective tissue, increase hormone receptor expression, and disrupt the normal uterine structure, raising the risk of recurrence. Clinically, the expression of inflammatory factors can be suppressed with antibiotics, antivirals, and biologics to eliminate inflammation and control further disease progression postoperatively.
This study is limited by its retrospective design, which may introduce selection bias. The sample size, although large, is from a single institution, limiting the generalizability of the findings. Additionally, the follow-up duration of 6 months may not capture long-term recurrence patterns, and other potential confounding factors, such as genetic predispositions or lifestyle factors, were not fully explored. Further multi-center, prospective studies with longer follow-up are needed to validate these results.
Conclusion
This study found that intraoperative ultrasound, ≥2 previous births, and postoperative GnRH-a treatment are protective factors against recurrence after laparoscopic myomectomy in uterine fibroid patients. Additionally, the number and location of fibroids, along with preoperative serum CRP levels, are strong predictors of recurrence, enabling effective identification of at-risk patients while excluding those without recurrence.
Data Sharing Statement
The experimental data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Consent to Participate
All experimental protocols were approved by the Ethics Committee of Xiaolan People’s Hospital, Informed consent was obtained from all the participants. All methods were carried out in accordance with Declaration of Helsinki.
Funding
This study was supported by the 2013 Zhongshan Municipal Science and Technology Bureau project “Survey on compliance with prenatal checkups and management countermeasures for non-household pregnant women in Xiaolan area” (No. 20132A147) 2018 Zhongshan City Social Public Welfare Science and Technology Research Project “Qualitative Research on Nursing Human Resource Management in Basic Hospitals under the Two-Child Policy” (No. 2018B1078).
Disclosure
The authors declared that they have no conflicts of interest regarding this work.
References
1. Yan W, Yuan S, Zhou D, et al. Status and treatment of patients with uterine fibroids in hospitals in central China: a retrospective study from 2018 to 2021. BMJ Open. 2024;14(1):e081736. doi:10.1136/bmjopen-2023-081736
2. Shi X, Wu H, Liu J, et al. Laparoscopic continuous seromuscular circumsuture for myomectomy: a real-world, retrospective, East-Asian cohort study. BMJ Open. 2024;14(3):e081550. doi:10.1136/bmjopen-2023-081550
3. Tinelli A, Mynbaev OA, Vergara D, et al. Uterine-preserving operative therapy of uterus myomatosus. Hysterect Comprehen Surg App. 2018;429–466.
4. Donnez J, Dolmans M-M. Uterine fibroid management: from the present to the future. Hum Reprod Update. 2016;22(6):665–686. doi:10.1093/humupd/dmw023
5. Frederick J, Hardie M, Reid M, et al. Operative morbidity and reproductive outcome in secondary myomectomy: a prospective cohort study. Hum Reprod. 2002;17(11):2967–2971.
6. Yuk J-S, Yoon S-H. Relationship between myomectomy and risk of osteoporosis or fracture: a population-based cohort study. PLoS One. 2023;18(11):e0294405. doi:10.1371/journal.pone.0294405
7. Heitmann RJ, Duke CM, Catherino WH, et al. Surgical treatments and outcomes. Fibroids. 2013;109–119.
8. Sparić R, Andjić M, Nejković L. Uterine fibroids and infertility: a controverse but concrete link. Clin Exper Obs Gynecol. 2022;49(1). doi:10.31083/j.ceog4901018
9. Ukaonu Chigozieblessed, Ibinaiye PO, Owoeye SC, et al. Prevalence and sonographic patterns of uterine fibroid among women of reproductive age in jos, plateau state, Nigeria. Radiology. 2017.
10. Chizen DR, Rislund DC, Robertson LM, et al. A randomized double-blind controlled proof-of-concept study of alanyl-glutamine for reduction of post-myomectomy adhesions. Europ J Obs Gynecol Reprod Biol. 2023;284:180–188. doi:10.1016/j.ejogrb.2023.03.032
11. Hatasaka HH. Acquired uterine factors and infertility. Reprod Endocrinol Infert Integra Modern Clin Lab Prac. 2010;235–264.
12. Trew G, Pistofidis G, Pados G, et al. Gynaecological endoscopic evaluation of 4% icodextrin solution: a European, multicentre, double-blind, randomized study of the efficacy and safety in the reduction of de novo adhesions after laparoscopic gynaecological surgery. Hum Reprod. 2011;26(8):2015–2027. doi:10.1093/humrep/der135
13. Purandare N, Kramer KJ, Minchella P, et al. Intraperitoneal triamcinolone reduces postoperative adhesions, possibly through alteration of mitochondrial function. J Clin Med. 2022;11(2):301. doi:10.3390/jcm11020301
14. Shi X, Guo J, Saravelos S, et al. The use of intrauterine balloon therapy in reproductive medicine and surgery: a guidance for practice. Hum Fert. 2023;26(4):742–756.
15. McLACHLAN ROBERTI, Healy DL, Burger HG. Clinical aspects of LHRH analogues in gynaecology: a review. BJOG Inter J Obst Gynaecol. 1986;93(4):431–454. doi:10.1111/j.1471-0528.1986.tb08652.x
16. Gnanachandran C, Penketh R, Banzal R, et al. Myomectomy benefits, risks, long-term outcomes, and effects on fertility and pregnancy outcomes: a literature review. J Gynecol Surg. 2023;39(4):151–157. doi:10.1089/gyn.2022.0127
17. Orlando M, Kollikonda S, Hackett L, et al. Non-hysteroscopic myomectomy and fertility outcomes: a systematic review. J Mini Invasive Gynecol. 2021;28(3):598–618. doi:10.1016/j.jmig.2020.10.006
18. Napoli A, Scipione R, Hans-Peter E, et al. Uterus-sparing treatment options for the management of fibroids. Obstet Gynecol Cases Rev. 2018;5:131.
19. Radosa MP, Owsianowski Z, Mothes A, et al. Long-term risk of fibroid recurrence after laparoscopic myomectomy. Europ J Obst, Gynecol Reprod Biol. 2014;180:35–39. doi:10.1016/j.ejogrb.2014.05.029
20. Ma Y, Weng J, Zhu Y. Impact of serum lipid on recurrence of uterine fibroids: a single center retrospective study.BMC Women’s Health. 2024;24(677). doi:10.1186/s12905-024-03530-0
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Recurrent Cellulitis: Who is at Risk and How Effective is Antibiotic Prophylaxis?
Ong BS, Dotel R, Ngian VJJ
International Journal of General Medicine 2022, 15:6561-6572
Published Date: 10 August 2022
Risk Factors and the Role of the Albumin-to-Globulin Ratio in Predicting Recurrence Among Patients with Idiopathic Granulomatous Mastitis
Ciftci AB, Bük F, Yemez K, Polat S, Yazıcıoğlu M
Journal of Inflammation Research 2022, 15:5401-5412
Published Date: 18 September 2022
Prognostic Factors of Adrenocortical Carcinoma: Experience from a Regional Medical Center in Eastern China
Li P, Su X, Zhang X, Sun L, Zhang G
International Journal of General Medicine 2023, 16:453-465
Published Date: 3 February 2023
Construction and Validation of a Novel Nomogram for Predicting the Recurrence of Diffuse Large B Cell Lymphoma Treated with R-CHOP
Gong Y, Yan H, Yang Y, Zhai B, Huang Z, Zhang Z
Pharmacogenomics and Personalized Medicine 2023, 16:291-301
Published Date: 1 April 2023
Analysis of Pathogenic Bacteria Distribution and Related Factors in Recurrent Acute Cholangitis
Li K, Hu X, Lu Q, Zhang H, Zhou J, Tian S, Zhou F
Infection and Drug Resistance 2023, 16:4729-4740
Published Date: 20 July 2023