Back to Journals » ClinicoEconomics and Outcomes Research » Volume 15
Examining the Burden of Potentially Avoidable Heart Failure Hospitalizations
Authors Zilberberg MD ![]() , Nathanson BH, Sulham K, Mohr JF, Goodwin M, Shorr AF
, Nathanson BH, Sulham K, Mohr JF, Goodwin M, Shorr AF
Received 1 June 2023
Accepted for publication 1 September 2023
Published 29 September 2023 Volume 2023:15 Pages 721—731
DOI https://doi.org/10.2147/CEOR.S423868
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Dean Smith
Marya D Zilberberg,1 Brian H Nathanson,2 Kate Sulham,3 John F Mohr,3 Matthew Goodwin,3 Andrew F Shorr4
1EviMed Research Group, LLC, Goshen, MA, USA; 2OptiStatim, LLC, Longmeadow, MA, USA; 3scPharmaceuticals, Burlington, MA, USA; 4Washington Hospital Center, Washington, DC, USA
Correspondence: Marya D Zilberberg, Department of Health Services Research, EviMed Research Group, LLC, PO Box 303, Goshen, MA, 01032, USA, Email [email protected]
Background: Two-thirds of the 1 million annual US CHF hospitalizations are for diuresis only; some may be avoidable. We describe a population of low-severity short-stay (Methods: We conducted a retrospective cohort study within the Premier Healthcare Database, 2016– 2021. CHF was defined via an administrative code algorithm. High severity (CHF-H) was marked by cardiogenic shock, the need for respiratory or circulatory support, and/or a Charlson comorbidity index > 2. We compared baseline characteristics, processes of care, and outcomes in low-severity (CHF-L) to CHF-H.
Results: Among 301,672 short-stay CHF patients, 135,304 (44.8%) were CHF-L. Compared to CHF-H, CHF-L was younger (70.5 ± 14.1 vs 72.1 ± 13.6 years, p < 0.001), more commonly female (48.6% vs 45.8%, p < 0.001), and more likely to receive IV ACE-I/ARB agents (0.5% vs 0.4%, p = 0.003). Most other IV medications were more common in CHF-H, and anticoagulation was the most prevalent non-diuretic IV therapy in both groups (23.8% vs 33.3%, p < 0.001). Hospital mortality (0.2% vs 1.5%, p < 0.001) and CHF-related 30-day readmissions (8.1% vs 10.5%, p < 0.001) were lower in CHF-L than CHF-H.
Conclusion: Among short-stay CHF patients, nearly ½ meet criteria for CHF-L, and are mainly admitted for fluid management. Avoiding these admissions could result in substantial savings.
Keywords: congestive heart failure, epidemiology, outcomes, hospital, costs
Introduction
Congestive heart failure (CHF) remains a frequent cause of hospitalization. According to the Agency for Healthcare Research and Quality’s (AHRQ) Healthcare Cost and Utilization Project (HCUP) Nationwide Inpatient Sample (NIS) database, in the year 2018 alone, there were nearly 5 ½ million discharges with CHF in the US. One-fifth of these were specifically for the management of heart failure as the principal reason for hospitalization. The cost for these admissions totaled US $15 billion in aggregate.1 Loop diuretics are the mainstay for managing fluid status in patients with heart failure. Unfortunately, in the presence of worsening congestion the absorption of oral loop diuretics is reduced, and their effectiveness is blunted.2,3 For this reason, it is not surprising that 4 out of 5 CHF admissions occur specifically for the treatment of volume overload with intravenous (IV) therapy.4 Moreover, nearly all of such hospitalizations are deemed uncomplicated since the sole intervention required is the IV agent to facilitate diuresis, and the dosage of the diuretic remains stable throughout the hospitalizations (without any need for escalation).5 On average, such patients spend about 3 days in the hospital.
While optimizing oral diuretics remains the mainstay for treating worsening congestion, schemes also exist to allow for outpatient management of CHF exacerbations with IV diuretics; however, they are rarely utilized.6 Among patients on Medicare, fewer than 1% of all CHF visits in the US are for outpatient IV diuresis, and among all visits specifically for the purpose of diuresis, outpatient IV diuresis accounts for no more than 15% of the total.6,7
One of the challenges in reducing the burden and consequences of hospitalizations for a CHF exacerbation lies in being able to identify at presentation patients who medically are both not so acutely ill that outpatient management is obviously contraindicated, but who are at the same time at low risk for progression while hospitalized (ie, those for whom outpatient management would be adequate). Hence, we set out to define a group of short-stay CHF inpatients in the US hospitals whose sole reason for the admission is IV diuresis (CHF-L). We compared these patients to other more complicated and severely ill short-stay CHF patients (CHF-H) along their demographic and baseline clinical characteristics, hospital processes, and outcomes.
Methods
Data Availability
The data that support the findings of this study are derived from a proprietary database, Premier Healthcare database, which is available to researchers through a direct agreement with Premier.
Ethics Statement
Because this study used fully de-identified administrative data, it was exempt from ethics review under US 45 CFR 46.101(b)4.8
Study Design and Patient Population
We conducted a multi-center retrospective cohort study of adult patients (age >/= 18 years) hospitalized for management of CHF. Our case identification approach relied on a previously published administrative algorithm, as recommended by the ACC/AHA guidelines and included the following ICD-10-CM codes: I11.0, I13.0, I13.2, I50.1, I50.20, I50.21, I50.22, I50.23, I50.30, I50.31, I50.32, I50.33, I50.40, I50.41, I50.42, I50.43, I50.9.9–12 To optimize the sensitivity of this algorithm we also included patients with DRG codes 291, 292, 293. Because we wanted to define a subpopulation of patients admitted specifically for the treatment of their CHF who could potentially avoid hospitalization, we included only those with the principal diagnosis of CHF and with the hospital length of stay (LOS) of four days or fewer. Patients were excluded if they had any of the following characteristics at admission (algorithms for all conditions available upon request):
- Age <18 years
- Hospital LOS > 4 days
- Transferred from another acute care facility
- Sepsis or severe sepsis or septic shock present on admission (POA)
- Pneumonia POA
- Acute respiratory failure/mechanical ventilation (MV) POA
- Acute myocardial infarction (MI) POA
- A major surgical procedure during hospitalization
- Vasopressor administration on day 1
- Hypertensive crisis POA
- Patient status is NOT nil-per-os (nothing by mouth, NPO) during the first 2 days of hospitalization, as evidenced by receipt of at least one oral medication within the time frame
Data Source
The data source was the Premier Healthcare Database (PHD), an electronic laboratory, pharmacy and billing data repository, for years 2018 through 2021. PHD is a large geographically representative source of data for approximately 25% of all US admissions to acute care institutions. In addition to the standard information contained in typical hospital claims (those derived from the Uniform Billing-04 form, UB-04), such as patient age, sex, race/ethnicity, principal and secondary diagnoses and procedures, the database contains a date-stamped log of all items and services charged to the patient or their insurer, including all medications, laboratory tests, and diagnostic and therapeutic services. Premier assigns each patient a unique identifier, so that previous and subsequent admissions to the same Premier hospital, along with principal and secondary diagnoses and procedure codes, can be readily ascertained. The database has been described in detail previously.13–15
Baseline Measures and Definitions
Potentially avoidable admissions (or CHF with low severity, CHF-L) were defined as those admissions without any markers of severe acute or chronic illness. Baseline characteristics included demographic data and type of insurance, as well as history of a hospitalization within the prior 30 days, comorbidity burden, and hospital characteristics. Charlson comorbidity score >2 was considered a signal of high chronic illness severity.16 Additionally, the following events during the index hospitalization served as markers for high acute illness severity (CHF-H) (algorithms available upon request):
- Cardiogenic shock
- Acute respiratory failure
- Acute MI
- Acute renal failure
- Dialysis
- ICU admission
- Cardiac catheterization17
- Pulmonary artery catheterization
- Arterial line placement
- IACD or pacemaker procedure
- The following physiologic alterations
- Hypotension or vasopressor use
- Hypoxemia
- Oliguria
- Altered mental status
- Tachycardia
- Bradycardia
Thus, hospitalizations of patients with Charlson score </= 2 and no factors defined determinative of severe acute illness were defined as potentially avoidable or CHF-L. All others were CHF-H and served as the comparator group. Other baseline characteristics included standard hospital and patients clinical and demographic characteristics. In addition to standard covariates, we explored the prevalence of prior hospitalization within 30 days of the index admission, as well as prior hospitalization within 30 days of the index admission for a surgical procedure.
Processes of Care During Index Hospitalization
To understand what further constraints, in addition to illness severity, could contribute to the need for hospitalization, we examined the prevalence and timing of the following procedures during the index hospitalization (Supplemental Table 1):
- Intravenous diuretic use
- O2 administration
- IV beta-blockers
- IV ACE-I/ARB
- IV calcium channel blockers
- IV potassium
- IV anticoagulation
- IV afterload reduction use
Outcome Variables
The primary outcome of interest was hospital mortality. Secondary outcomes included hospital LOS, hospital costs, 30-day readmission rates among survivors, and discharge destination.
Statistical Analyses
Standard descriptive statistics were used to compare CHF-L to CHF-H group across demographics, comorbidities, hospital characteristics and processes, as well as hospital outcomes. Continuous variables are reported as means with standard deviations and as medians with 25th and 75th percentiles. Differences between mean values were tested via the Student’s t-test, while those between medians were examined using the Mann–Whitney U-test. Categorical data are summarized as counts and percentages, and the Chi-square test or Fisher’s exact test for cell counts <4 was used to examine between-group differences. While statistical significance was set at p < 0.05, because of the large size of the database, statistical significance does not necessarily translate to a clinically important difference. Because the purpose of the current study was to quantify the differences between those hospitalizations that may be avoidable and those that are not, we did not undertake statistical modeling to adjust for confounding when comparing the groups.
Results
Among 301,672 patients with a short-stay CHF admission, 135,304 (44.8%) met criteria for CHF-L. Compared to CHF-H, CHF-L subjects were less common in the Midwest and more common in the Northeast (Table 1). There were no important differences in their distributions based on hospital size, academic affiliation, or urbanicity. All markers of severity of acute illness were prevalent in the CHF-H only, as per cohort definition. Their distributions in that group can be found in the Supplemental Table 2. CHF-L patients were younger (mean age 70.5±14.1 vs 72.1±13.6 years, p < 0.001), more commonly female (48.6% vs 45.8%, p < 0.001), and less likely to be covered by Medicare (70.7% vs 78.6%, p < 0.001) than those with CHF-H. IV diuretics were more commonly given in the CHF-L group (91.8%) than in CHF-H group (82.2%) over the entire hospitalization and across different time periods examined (p < 0.001) (Figure 1). While CHF-L patients were more likely to receive IV ACE-I/ARB agents (0.5% vs 0.4%, p = 0.003), most other IV medications were more commonly utilized in the CHD-H group (Table 2). Notably, with the exception of anticoagulation, all other IV treatments examined were used in fewer than 5% of the patients in the first two days of hospitalization irrespective of the group. Anticoagulation, the most prevalent IV therapy in both groups, was administered to 23.8% of the patients in CHF-L vs 33.3% in CHF-H, p < 0.001.
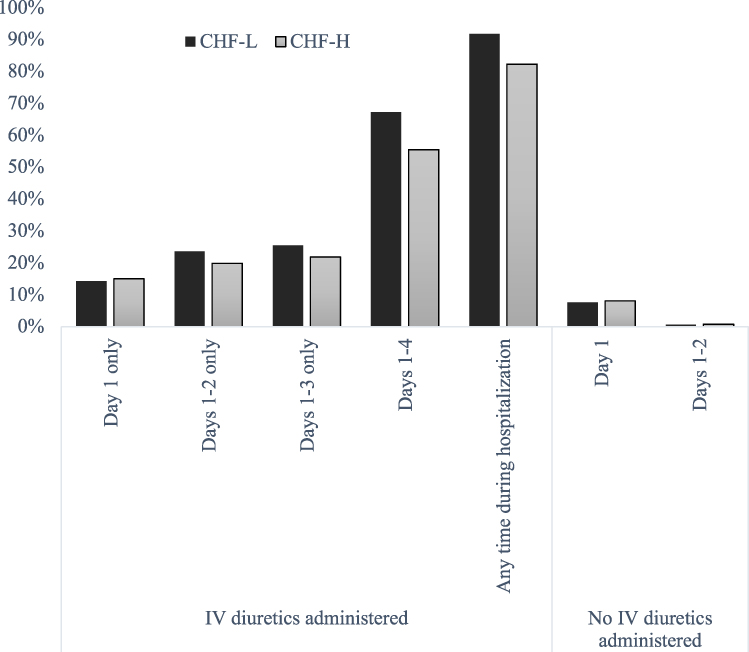 |
Figure 1 Intravenous diuretic administration*. Abbreviations: CHF-L, congestive heart failure low severity; CHF-H, congestive heart failure high severity; IV, intravenous. Note: *All comparisons reached statistical significance at p < 0.001. |
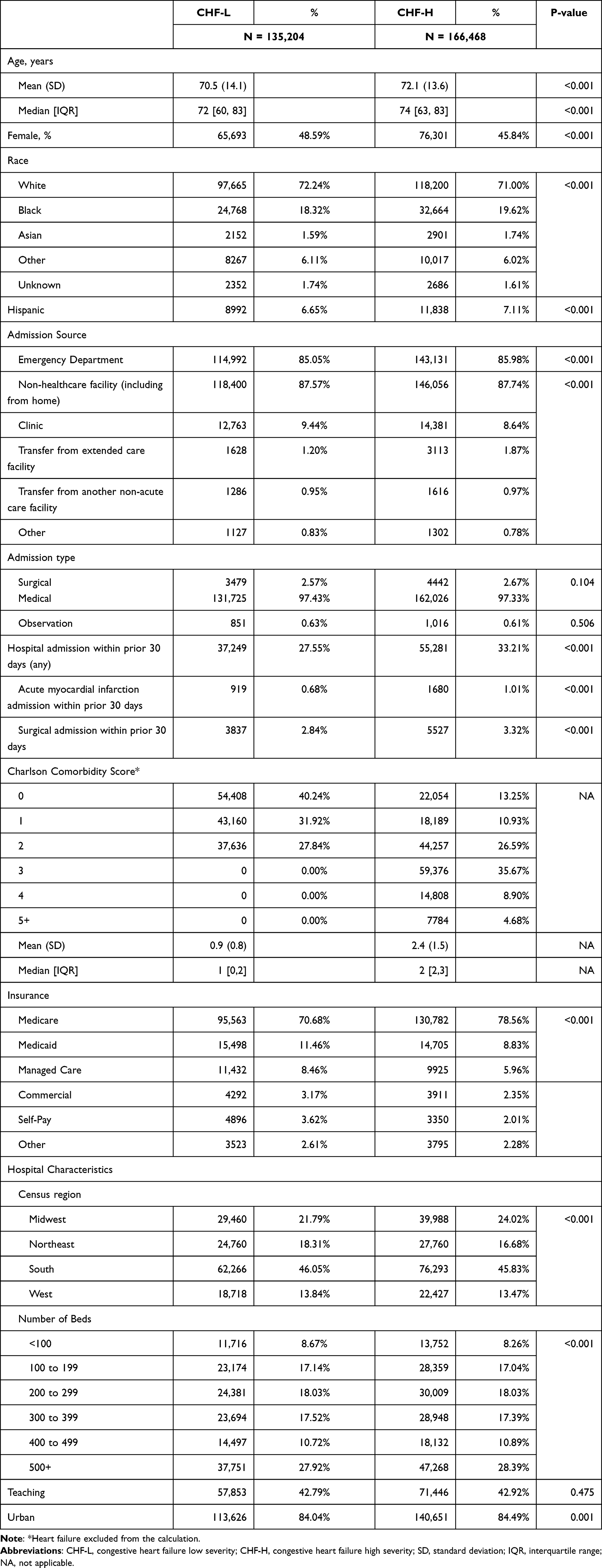 |
Table 1 Baseline Characteristics |
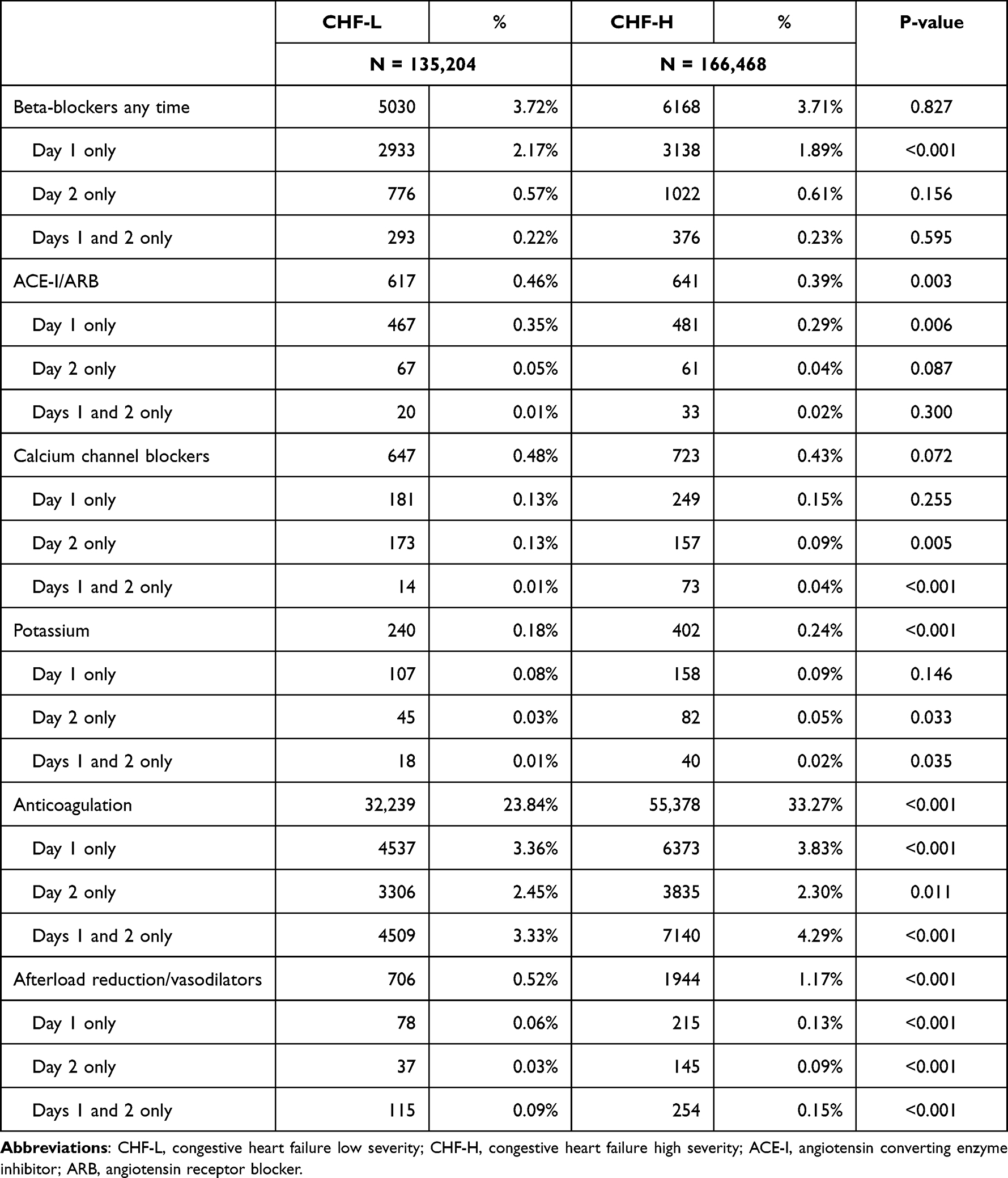 |
Table 2 Intravenous Medications Other Than Diuretics Administered During Hospitalization |
Hospital mortality was lower in CHF-L (0.2%) than in CHF-H (1.5%) group. An additional 1.3% of CHF-L and 3.0% of CHF-H group were discharged to hospice (p < 0.001) (Figure 2). While a total of 85.7% in the CHF-L and 79.8% in the CHF-H groups were able to be sent directly home, more patients in the CHF-L group did not require home health care than in the CHF-H group (65.7% vs 56.5%, p < 0.001) (Figure 2). Despite similar durations of hospitalization (albeit statistically different), mean hospital costs in the CHF-L were substantially lower than those in CHF-H ($6,138 ± $5,558 vs $6,884 ± $6,124, p < 0.002). These trends in mortality, LOS, and costs persisted across all strata examined (Supplemental Table 3). Both all-cause (21.0% vs 26.2%, p < 0.001) and CHF-related (8.1% vs 10.5%, p < 0.001) 30-day readmissions were lower among persons classified as CHF-L than CHF-H.
 |
Figure 2 Discharge destinations*. Abbreviations: CHF-L, congestive heart failure low severity; CHF-H, congestive heart failure high severity; SNF, skilled nursing facility. Note: *All comparisons reached statistical significance at p < 0.001. |
Discussion
We demonstrate that nearly one-half of all short-stay hospitalizations for management of a CHF exacerbation are of low severity and, therefore, may be avoidable. By defining a group of patients whose only potential issue is diuresis, we have identified possible markers present at the time of acute presentation that may help clinicians in their decision-making process regarding which persons can be safely managed out of the hospital. Additionally, we have quantified the potential economic consequences associated with avoiding hospitalization in this cohort. Assuming approximately 1 million annual admissions in the US for CHF exacerbations and a 4-day median LOS, of whom 45% are CHF-L, given the mean costs of around $6,000 per case (this number reflects the arithmetic mean of the costs for these patients’ hospitalizations), avoiding these hospitalizations could result in annual savings of over $1.3 billion.1
Our study confirms several important points reported by others. First, only a small proportion of patients admitted for the management of worsening CHF require intravenous vasoactive agents. While the ADHERE registry noted that under ¼ of all of them receive these agents, our numbers are much lower.18 This is likely in part due to the vastly differing time frames between the two studies (ADHERE reflects data from approximately 15 years ago, while ours is contemporary). Another probable reason for this disparity is the population differences, ours being only patients with a short-stay CHF admission. Hence, there was a reduced exposure time for these treatments in our study.
Prior work has borne out the idea that hospitalization costs constitute the vast majority of overall expenditures in the treatment of heart failure. That is, 80 cents out of every dollar spent on CHF are dedicated to inpatient treatment, of which 15% is specifically spent on the treatment of worsening heart failure.19 It has been postulated that approximately 2/3 of all CHF admissions who require simply aggressive IV diuresis may be effectively treated as outpatients, resulting in billions of dollars in savings.5 Despite this potential to avoid hospitalizations, emergency departments continue to admit the bulk of all patients presenting with a CHF exacerbation. The reasons for this are multifold.20 First, as of 2015, the prevalence of outpatient IV diuresis infrastructure was less than 20%.6 Second, and potentially more concerning, is that among those hospitals where IV diuresis infrastructure was available, these locations accounted for a disappointing 1.4% of all heart failure visits.6 It is likely that the latter reflects a paucity of robust risk stratification strategies.
A review and recommendation statement by Collins et al addressed this lack of viable risk stratification strategies.20 They proposed a two-tier ED-based evaluation to improve triaging of these patients such that more are able to avoid hospitalization. Their schema is aimed at the middle portion of CHF exacerbations in the ED who neither respond fully to nor worsen following emergent treatment of their symptoms. While those who respond readily can be discharged without much risk, the group in the middle, those with a partial response, require further risk stratification. The authors suggest that certain high-risk features, such as ongoing symptoms, worsening renal function, elevated troponin levels, or the need for blood pressure support, would distinguish patients who do from those who do not require further inpatient management. The recommendation for those patients is for a period of observation instead of a full hospital admission.20
Despite availability of this stratification schema, more aggressive efforts at avoiding hospitalizations have not been successful. While it is estimated that nearly ½ of all patients presenting to the ED with worsening HF could be safely discharged home right away or after a short period of observation, in reality only under 5% end up in observation, and in 2015, nearly 30% of all CHF exacerbations presenting for treatment were treated as inpatients.6 Our study narrows the population that may be a viable target for hospital avoidance strategies, as it focuses specifically on patients with not only brief stays (well under 1% of our cohort had the status of “observation”) but also those not complicated by a heavy comorbidity burden or severe decompensation requiring aggressive hospital-based interventions. We build on prior efforts to paint a picture of what these patients may look like at the point of decision-making with respect to admission. That is, patients with low Charlson comorbidity scores and those who are not NPO, in shock, or requiring surgery or other procedures, constitute a significant fraction of all CHF admissions. If these patients were treated in the outpatient setting, they would not only avoid the inconvenience and risks associated with hospitalization but may save the already financially strained healthcare system over $1 billion annually.
Furthermore, finding viable alternatives for outpatient diuresis will also carry important implications for emergency departments. Following the global pandemic with SARS-CoV-2, hospitals continue to experience exceedingly high volumes, with emergency departments in particular being unusually busy with long wait times and staff shortages.21 Robust alternatives to hospital-based evaluation and diuresis could mitigate at least some of this overload.
Our study has a number of strengths and limitations. Its major strength is the large number and a wide range of hospitals analyzed, lending our results generalizability. Our rigorous cohort definition reduces the risk and magnitude for a selection bias. Nevertheless, the retrospective nature of this study exposes our results to this potential. There is also a risk of misclassification, particularly as it relates to exposure. Because we used billing data to establish the prevalence of various interventions and severity markers, it is possible that a small number may have been undercoded. This may be true in particular for coding for physiologic markers, such as hypotension, hypoxemia, and related conditions. Underreporting of these conditions would result in classifying patients who may actually be CHF-H into the CHF-L category, thus overestimating the numbers of patients in this group. In the same vein, we did not have access to such clinical data as NYHA classification, natriuretic peptide measurements, or assessment of the left ventricular function, which makes our definitions prone to misclassification. To mitigate this, we utilized algorithms similar studies have used to answer similar questions. Confounding, while an issue in all observational studies, is not a limitation, as we make no claims of causality or attribution, focusing instead simply on descriptive data.
Conclusions
In summary, we have shown that nearly one-half of all short-stay hospitalizations for a CHF exacerbation occur among low-risk patients and require almost exclusively IV diuresis. Although low-risk, ½ of them spend longer than two days in the hospital with the aggregate annual costs totaling $1.3 billion. Better outpatient alternatives could not only hold a considerable economic advantage but also help streamline patient care for both CHF and non-CHF patients presenting to the emergency department for evaluation.
Abbreviations
CHF, congestive heart failure; AHRQ, Agency for Healthcare Research and Quality; HCUP, Healthcare Cost and Utilization Project; NIS, Nationwide Inpatient Sample; IV, intravenous; CHF-L, low-severity CHF hospitalization; CHF-H, high-severity CHF hospitalization; LOS, length of stay; POA, present on admission; MV, mechanical ventilation; MI, myocardial infarction; NPO, nil-per-os (nothing by mouth); PHD, Premier Healthcare Database; UB-04, Uniform Billing-04 form; ACC, American College of Cardiology; AHA, American Heart Association.
Data Sharing Statement
The data that support the findings of this study are derived from a proprietary database, Premier Healthcare database, which is available to researchers through a direct agreement with Premier.
Ethics Statement
Because this study used fully de-identified administrative data, it was exempt from ethics review under US 45 CFR 46.101(b)4 [8].
Acknowledgments
No person other than the listed authors participated in the study, its design, or its reporting.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by a grant from scPharmaceuticals, Burlington, MA, USA. Portions of these data have been presented as an abstract at the ACC annual meeting 2023.
Disclosure
MDZ’s employer, EviMed Research Group, LLC, has received research grant support from scPharmaceuticals, Burlington, MA, USA. BHN’s employer, OptiStatim, LLC, has received support from EviMed Research Group, LLC, Goshen, MA, USA. KS is an employee of scPharmaceuticals, Burlington, MA, USA. JFM is an employee scPharmaceuticals, Burlington, MA, USA. MG is an employee scPharmaceuticals, Burlington, MA, USA. AFS is a clinical consultant to and has received consulting fees from EviMed Research Group, LLC, Goshen, MA, USA. MDZ and AFS have received grant support and/or have served as consultants to Spero, Melinta, Pfizer, Astellas, Shionogi, and Lungpacer. The authors report no other conflicts of interest in this work.
References
1. Agency for Healthcare Research and Quality HCUPNet, Healthcare Cost and Utilization Project. Available from: hcupnet.ahrq.gov.
2. Vasko MR. Furosemide absorption altered in decompensated congestive heart failure. Ann Intern Med. 1985;102(3):314–318. doi:10.7326/0003-4819-102-3-314
3. Ellison DH, Felker GM. Diuretic treatment in heart failure. N Engl J Med. 2017;377:1964–1975. doi:10.1056/NEJMra1703100
4. Nieminen MS, Brutsaert D, Dickstein K, et al.; EuroHeart Survey Investigators. EuroHeaart Failure Survey II (EHFS II): a survey on hospitalized acute heart failure patients: description of population. Eur Heart J. 2006;27(22):2725–2736. doi:10.1093/eurheartj/ehl193
5. Greene SJ, Triana TS, Ionescu-Ittu R, et al. In-Hospital therapy for heart failure with reduced ejection fraction in the United States. JACC Heart Fail. 2020;8:943–953. doi:10.1016/j.jchf.2020.05.013
6. Greene SJ, Wilson LE, Abbasi SA, Yusuf AA, Hammill BG. Outpatient intravenous diuretic therapy for heart failure in the United States. J Am Coll Cardiol. 2019;73:1101–1103. doi:10.1016/j.jacc.2018.12.034
7. Greene SJ, Goto D, Wang D, Hilkert R, Lautsch D, Fonarow GC. Outpatient versus inpatient intravenous diuretic therapy for heart failure in the United States. Eur J Heart Fail. 2022;24(11):2199–2202. doi:10.1002/ejhf.2727
8. US Department of Health and Human Services Office for Human Research Protections. Human subject regulations decision charts. Available from: https://www.hhs.gov/ohrp/regulations-and-policy/decision-charts/index.html.
9. Akintoye E, Briasoulis A, Egbe A, et al. National trends in admission and in-hospital mortality of patients with heart failure in the United States (2001–2014). J Am Heart Assoc. 2017;6:e006955. doi:10.1161/JAHA.117.006955
10. American Heart Association Get with the Guidelines – Heart Failure HF Factsheet, February 2016. Available from: https://www.heart.org/idc/groups/heart-public/@wcm/@hcm/@gwtg/documents/downloadable/ucm_467882.pdf.
11. Presley CS, Min JY, Chipman J, et al. Validation of an algorithm to identify heart failure hospitalisations in patients with diabetes within veterans health administration. BMJ Open. 2018;8(3):e020455. doi:10.1136/bmjopen-2017-020455
12. Zilberberg MD, Nathanson BH, Sulham K, Mohr JF, Goodwin MM, Shorr AF. Descriptive epidemiology and outcomes of patients with short stay hospitalizations for the treatment of congestive heart failure in the US. Clinicoecon Outcomes Res. 2023;8:139–149. doi:10.2147/CEOR.S400882
13. Zilberberg MD, Nathanson BH, Sulham K, Fan W, Shorr AF. A novel algorithm to analyze epidemiology and outcomes of carbapenem resistance among patients with hospital-acquired and ventilator-associated pneumonia: a retrospective cohort study. Chest. 2019;155:1119–1130. doi:10.1016/j.chest.2018.12.024
14. Zilberberg MD, Nathanson BH, Sulham K, Fan W, Shorr AF. Multidrug resistance, inappropriate empiric therapy, and hospital mortality in Acinetobacter baumannii pneumonia and sepsis. Crit Care. 2016;20(1):221. doi:10.1186/s13054-016-1392-4
15. Zilberberg MD, Nathanson BH, Sulham K, Fan W, Shorr AF. Carbapenem resistance, inappropriate empiric treatment and outcomes among patients hospitalized with Enterobacteriaceae urinary tract infection, pneumonia and sepsis. BMC Infect Dis. 2017;17(1):279. doi:10.1186/s12879-017-2383-z
16. Lodise TP, Chopra T, Nathanson BH, Sulham K. Hospital admission patterns of adult patients with complicated urinary tract infections who present to the hospital by disease acuity and comorbid conditions: how many admissions are potentially avoidable? Am J Infect Control. 2021;49:1528–1534. doi:10.1016/j.ajic.2021.05.013
17. Derington CG, Heath LJ, Kao DP, Delate T, den Uil C. Validation of algorithms to identify elective percutaneous coronary interventions in administrative databases. PLoS One. 2020;15(4):e0231100. doi:10.1371/journal.pone.0231100
18. Abraham WT, Adams KF, Fonarow GC, et al.; The ADHERE Scientific Advisory Committee and Investigators, and the ADHERE Study Group. In-hospital mortality in patients with acute decompensated heart failure requiring intravenous vasoactive medications: an analysis from the Acute Decompensated Heart Failure National Registry (ADHERE). J Am Coll Cardiology. 2005;46:57–64.
19. Heidenreich PA, Fonarow GC, Opsha Y, Sandhu AT, Sweitzer NK, Warraich HJ; HFSA Scientific Statement Committee Members Chair. Economic issues in heart failure in the United States. J Card Fail. 2022;28(3):453–466. doi:10.1016/j.cardfail.2021.12.017
20. Collins SP, Pang PS, Fonarow GC, Yancy CW, Bonow RO, Gheorghiade M. Is hospital admission for heart failure really necessary?: the role of emergency department and observation unit in preventing hospitalization and rehospitalization. J Am Coll Cardiology. 2013;61:121–126. doi:10.1016/j.jacc.2012.08.1022
21. Mole B. US hospitals are so overloaded that one ER called 911 on itself. ArsTechnica; November 7, 2022. Available from: https://arstechnica.com/science/2022/11/us-hospitals-are-so-overloaded-that-one-er-called-911-on-itself/.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Glucarpidase for Treating Adults with Delayed Methotrexate Elimination Due to Impaired Renal Function: An Economic Simulation Analysis
Kala J, Nelson R, Drudge C, Zhou A, Ward S, Bourque M
ClinicoEconomics and Outcomes Research 2023, 15:165-179
Published Date: 8 March 2023