Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Evaluation of Atherosclerosis Risk in Patients with Psoriasis
Authors Celik L ![]() , Akray A
, Akray A ![]() , Denli Y, Aksungur VL
, Denli Y, Aksungur VL
Received 14 October 2025
Accepted for publication 22 January 2026
Published 29 January 2026 Volume 2026:19 574241
DOI https://doi.org/10.2147/CCID.S574241
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Dr Jeffrey Weinberg
Lutfullah Celik,1 Anil Akray,2 Yasargul Denli,1 Varol Lutfu Aksungur1
1Cukurova University, Medical School, Department of Dermatology, Adana, Turkey; 2Cukurova University, Medical School, Department of Cardiology, Adana, Turkey
Correspondence: Lutfullah Celik, Cukurova University, Medical School, Department of Dermatology, Adana, 01330, Turkey, Tel +90 554 9482780, Fax +90 322 3387144, Email [email protected]
Background: Psoriasis is a systemic inflammatory disease with a chronic course that is not limited to the skin. Atherosclerosis can cause serious cardiovascular events such as cerebrovascular stroke and myocardial infarction, which can result in death. This study aimed to examine the atherosclerosis risk in psoriasis patients by measuring the carotid intima media thickness (CIMT), an important marker of atherosclerosis.
Methods: The study included 70 plaque psoriasis patients (41 male and 29 female) and 50 healthy volunteers (30 male and 20 female) between the ages of 18 and 65, from the Cukurova University Faculty of Medicine Department of Dermatology who did not use any systemic treatment in the previous 6 months. Clinical parameters were recorded. The presence of subclinical atherosclerosis was investigated by measuring carotid intima-media thickness (CIMT). CIMT was measured manually by the same cardiologist using B-mode ultrasonography.
Results: The median value of the CIMT measured individuals in the patient group was 0.8 mm (min: 0.5-max:1.4), and individuals in the control group was 0.6 mm (min: 0.4-max: 0.95). CIMT value in the patient group was statistically significantly higher than in the control group (p< 0.001). A statistically significant relationship was found between age, body mass index, cigarette use, waist and hip circumference, HBA1C, total cholesterol, triglycerides, duration. In multivariate linear regression analysis, cigarette use (p = 0.001) and disease duration (p = 0.024) remained significant, while the Psoriasis Area and Severity Index (PASI) showed a trend toward significance (p = 0.071).
Conclusion: Our study revealed that CIMT value increases in psoriasis patients. It can be said that this increase in CIMT is more serious in the presence of PASI, disease duration and smoking. In conclusion, psoriasis patients—especially those who smoke and those with a longer disease duration—should be regularly investigated and followed up for atherosclerosis.
Keywords: psoriasis, atherosclerosis, carotid intima media thickness
Introduction
Psoriasis is an immune-mediated, chronic and recurrent inflammatory skin disease with a genetic predisposition triggered by various environmental factors such as trauma, infection and drugs. It affects approximately 2% of the general population.1 The mechanism of psoriasis is chronic and systemic inflammation, which occurs due to pro-inflammatory cytokines such as TNF-α, IL-12, IL-17, IL-22 and IL-23, as well as signaling pathways such as IL-23/Th17, cAMP and JAK-STAT. Many comorbidities can occur as a result of this chronic, systemic inflammation.2 Psoriasis is a treatable but incurable disease that is widespread, significantly impacts quality of life, and can lead to serious comorbidities that may be life-threatening.3 Atherosclerosis is a progressive, inflammatory disease characterized by the deposition of lipids and fibrous elements in the walls of large and medium-sized arteries. The rupture of atherosclerotic plaques accumulated in the vascular walls causes thrombus in the vessels and causes the development of important cardiovascular and cerebrovascular events such as myocardial infarction and stroke, which can even result in death.4 It is thought that psoriasis may contribute to atherosclerosis due to traditional risk factors such as obesity, hypertension, diabetes, hyperlipidemia, metabolic syndrome and smoking, as well as systemic chronic inflammation caused by the disease itself.5 Although atherosclerosis is an important cause of morbidity and mortality, psoriasis may lead to an increased risk of death due to cardiovascular disease.6 Considering that atherosclerosis may cause mortality due to cardiovascular and cerebrovascular events, it is important to determine the presence of atherosclerosis in patients with psoriasis. Atherosclerosis causes various changes in the vessels before presenting clinical findings.7 Early atherosclerotic changes that cannot be detected by classical angiography can be demonstrated by measuring carotid intima media thickness (CIMT) with B-mode USG, which is a non-invasive and easily applicable method. CIMT measurement is used in the evaluation of subclinical atherosclerosis, which does not yet show clinical findings.8
Objectives
In present study, it was aimed to examine the presence of atherosclerosis in patients with psoriasis comparatively with the healthy population through CIMT measurement and to investigate the effect of atherosclerosis risk factors such as obesity, hypertension, diabetes, hyperlipidemia, metabolic syndrome and smoking on CIMT in patients with psoriasis. In addition, it was aimed to investigate the effects of disease severity and duration, psoriatic arthritis and nail involvement on CIMT.
Materials and Methods
Study Design and Patients
The study included 70 plaque psoriasis patients (41 male and 29 female) who did not use any systemic treatment in the last 6 months, and age and gender-matched 50 healthy volunteers (30 male and 20 female) between the ages of 18 and 65, who presented to the Cukurova University Balcalı Hospital Dermatology Outpatient Clinic, Adana, Turkey. All patients had plaque psoriasis. Participants were enrolled between July 2022 and June 2023. For each participant, clinical assessments and CIMT measurements were performed on the same day to ensure temporal consistency in data collection. A positive history of malignancy, age <18 years and >65 years, pregnancy, lactation, diabetes mellitus, hypertension, cardiovascular and cerebrovascular disease, renal failure, active infection, systemic inflammatory disease other than psoriasis that may cause atherosclerosis (rheumatoid arthritis, systemic lupus erythematosus, inflammatory bowel disease, etc).; Patients using anti-atherosclerosis drugs such as antihypertensive, antiplatelet, statin group were exclusion criteria. The study protocol was approved by the Cukurova University School of Medicine Ethics Committee for Non-Interventional Studies (date: 04.11.2022, number: 27). All study strategies were performed according to the ethical principles of the 1964 Declaration of Helsinki, and all subjects provided written informed consent before being included. Age, gender, disease duration, presence of a family history, pregnancy/lactation, smoking, alcohol use, Psoriasis Area and Severity Index (PASI), the presence of nail and joint involvement, previous treatments for psoriasis were noted. PASI scores were independently evaluated by a second dermatologist, and any discrepancies were resolved by consensus to reduce subjective bias. Height, weight, waist and hip circumference were measured. Smoking status was assessed in terms of pack-years, with one pack defined as 20 cigarettes. Participants were classified as current smokers if they had smoked within the past 6 months, and as past smokers otherwise. Body mass index (BMI) was calculated. A sphygmomanometer was used to measure blood pressure.
Laboratory Measurements
Fasting blood glucose, HBA1C, C- reactive protein (CRP), lipid profiles were measured in 5 mL of venous blood taken from individuals selected for the research group after at least 8 hours of fasting, using the Beckman Coulter DXH device in the Biochemistry laboratory of our hospital. Laboratory tests were performed using standard measurement techniques. Diabetes mellitus (DM) was diagnosed in cases with fasting blood glucose ≥126 mg/dl or HBA1C >6.4%. All participants were evaluated for metabolic syndrome using the National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III) criteria.
Imaging Methods
Right and left common carotid arteries were used for measurements. The evaluation was performed with the patient in a supine position, the neck slightly extended, and the head turned in the opposite direction to the examined side. USG images of CIMT were measured from the posterior walls of longitudinal images taken proximally at the lower 1/3 of the cervical region and distally at the level of 1 cm caudal to the carotid bulb. CIMT was measured at three points along the far wall of each common carotid artery, spaced 1 cm apart. Images with poor quality or unclear arterial walls were excluded from analysis. Measurements were made by the same cardiologist using an advanced technological echocardiography device (GE VIVID 09). CIMT measurements were performed by a single experienced cardiologist who was blinded to participants’ clinical and laboratory data to minimize measurement bias. In the evaluation of the data, the average of right and left common carotid arteries was used as CIMT. The clinical and CIMT images of two patients with psoriasis are shown in Figure 1.
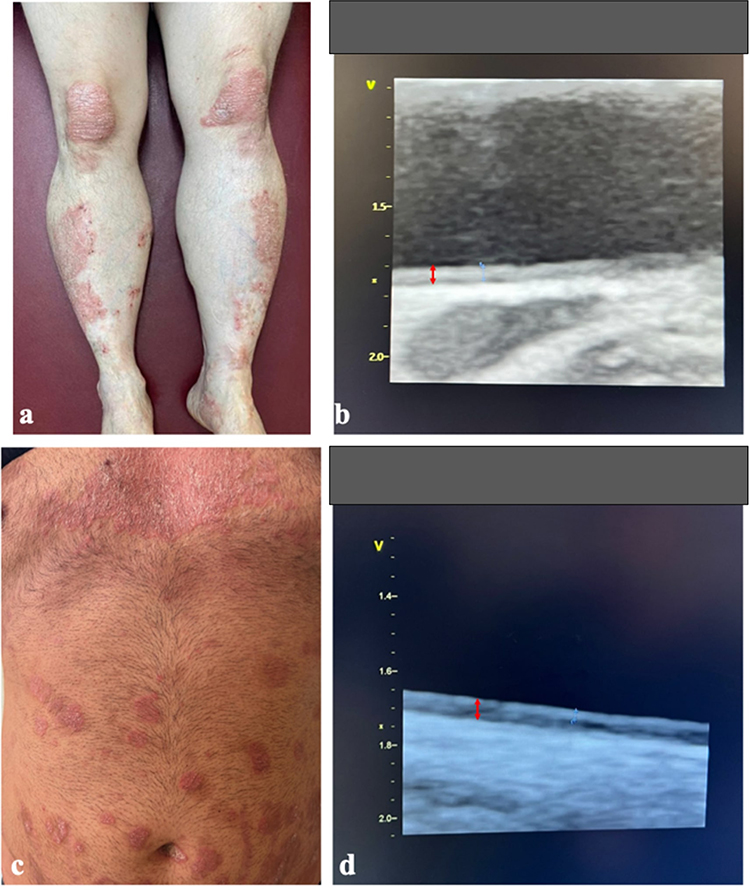 |
Figure 1 (a) Erythematous, scaly plaques in a patient (PASI score: 13.6). (b) Ultrasonographic image of CIMT measured as 0.9 mm, indicated by the double-headed red arrow. (c) Erythematous, scaly plaques in a patient (PASI score: 12). (d) Ultrasonographic image of CIMT measured as 0.8 mm, indicated by the double-headed red arrow. The double-headed red arrows indicate CIMT measurements, while the blue arrows have no specific significance. |
Statistical Analysis
R Statistical Computing Program (Vienna, Austria; 2018. Available at: https://www.R-project.org/) was used in the statistical analysis of the data. Descriptive statistics were used to describe demographic characteristics of participants. Categorical variables were given in percentage and frequency. Chi Square test was used to compare categorical variables. Distributions were checked to compare continuous measurements between groups; Student’s T test was used for variables showing parametric distribution, and Mann Whitney U-test was used to analyze variables that did not. Situations where the p value was <0.05 were considered statistically significant. Pearson correlation analysis was used in correlation analysis. In the second stage, multivariate linear regression analysis was applied for independent variables showing significant relationships. Extreme CIMT values were evaluated using boxplot inspection. No data points were removed from the analysis, as all measurements were considered valid.
Results
Clinical, demographic and laboratory examinations of the study group are presented in Table 1. The study included 70 plaque-type psoriasis patients (41 male (58.6%) and 29 female (41.4%)) and 50 controls (30.0 male (60%) and 20 female (40.0%)). The mean age of patients and controls were 41.5 years (SD ±14.2, range 19–64, median 40.0) and 40.6 years (SD ±10.6, range 20–61, median 42.0)), respectively. There was no statistical difference between the groups in terms of gender, age, BMI, blood pressure, hip circumference, fasting blood glucose, lipid profile and CRP. The mean cigarette use of patients and controls were 7.6 package/year (SD ±7.6, range 0–40, median 2.0) and 4.5 package/year (SD ±6.7, range 0–20, median 0)), respectively. Cigarette use showed a trend toward difference between the patient and control groups (p = 0.054). The mean waist circumference of patients and controls were 94.8 cm (SD ±10.2, range 72–123, median 94.5) and 90.5 cm (SD ±8.6, range 71–116, median 90.5)), respectively. The mean HBA1C levels of patients and controls were 5.6% (SD ±0.5, range 4.5–8.3, median 5.5) and 5.4% (SD ±0.2, range 5–6, median 5.4)), respectively. There was a statistically significant difference in waist circumference and HBA1C levels between the patient and control groups (Table 1). Psoriatic arthritis was present in 14 of the 70 patients in the study group.
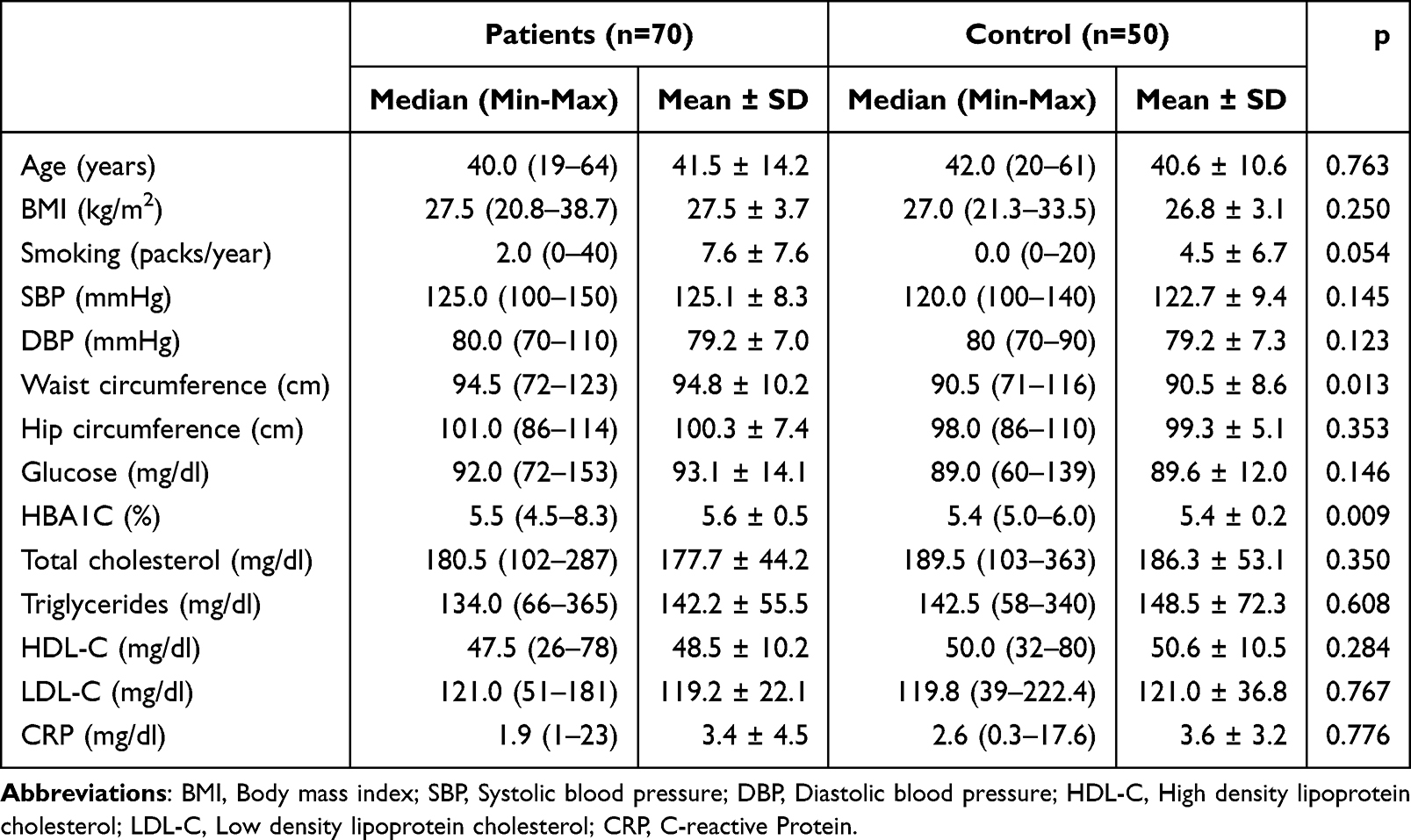 |
Table 1 Clinical, Demographic and Laboratory Examinations of the Study Group |
The mean CIMT value was higher in patients with psoriasis than in the control group. The mean CIMT value of patients and controls were 0.8 mm (SD ±0.1, range 0.5–1.4, median 0.8) and 0.6 mm (SD ±0.1, range 0.5–0.95, median 0.6)), respectively. There was a statistically significant difference in CIMT value between the patient and control groups (p<0,001) (Table 2). The distribution of carotid intima media thickness between the patient and control groups is shown in Figure 2.
 |
Table 2 CIMT Value Comparison Between Patients with Psoriasis and Controls |
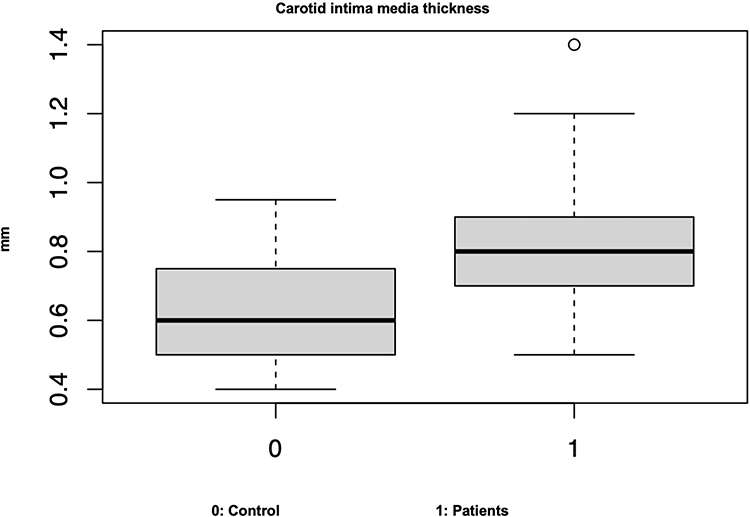 |
Figure 2 Distribution of carotid intima media thickness between patient and control groups. |
There was no significant relationship between the CIMT value of the individuals in the patient group and gender, alcohol use, high density lipoprotein cholesterol (HDL-C), low density lipoprotein cholesterol (LDL-C), CRP and fasting blood glucose, presence of family history, nail involvement and blood pressure. There was a statistically significant difference between age, BMI, disease duration, smoking, psoriatic arthritis, waist and hip circumference, PASI, HBA1C, total cholesterol, and triglyceride (Table 3).
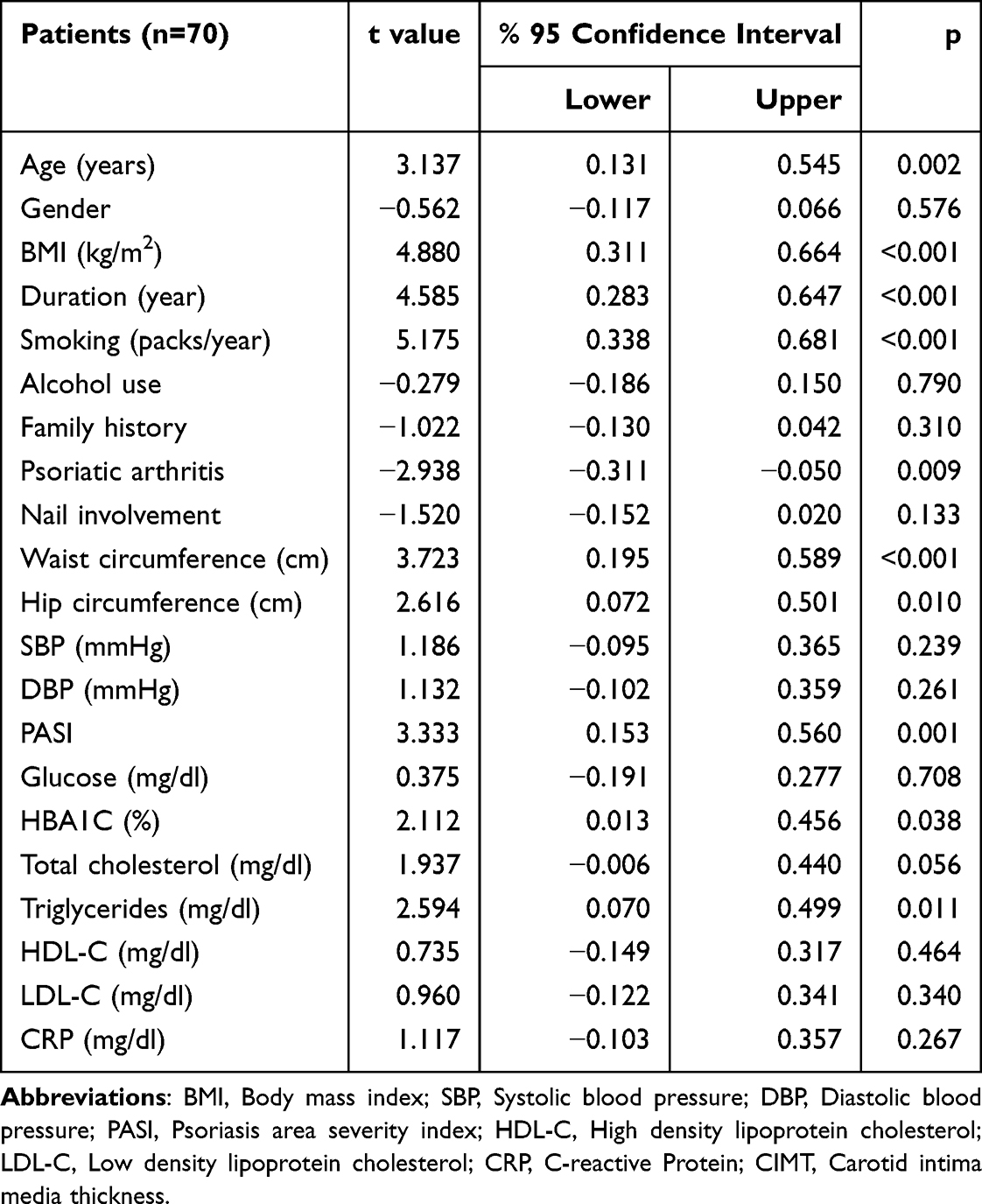 |
Table 3 Correlation Between CIMT Value and Demographic, Clinical and Laboratory Parameters in Patients with Psoriasis |
Age, BMI, smoking, waist and hip circumference, HBA1C, total cholesterol, triglyceride, disease duration, psoriatic arthritis and PASI, which were significant findings in bivariate analysis, were treated as independent variables. Multivariate linear regression test was performed using CIMT as the dependent variable. As a result of this analysis, smoking (p = 0.001), disease duration (p = 0.024) and PASI (p = 0.074) remained significant (Table 4).
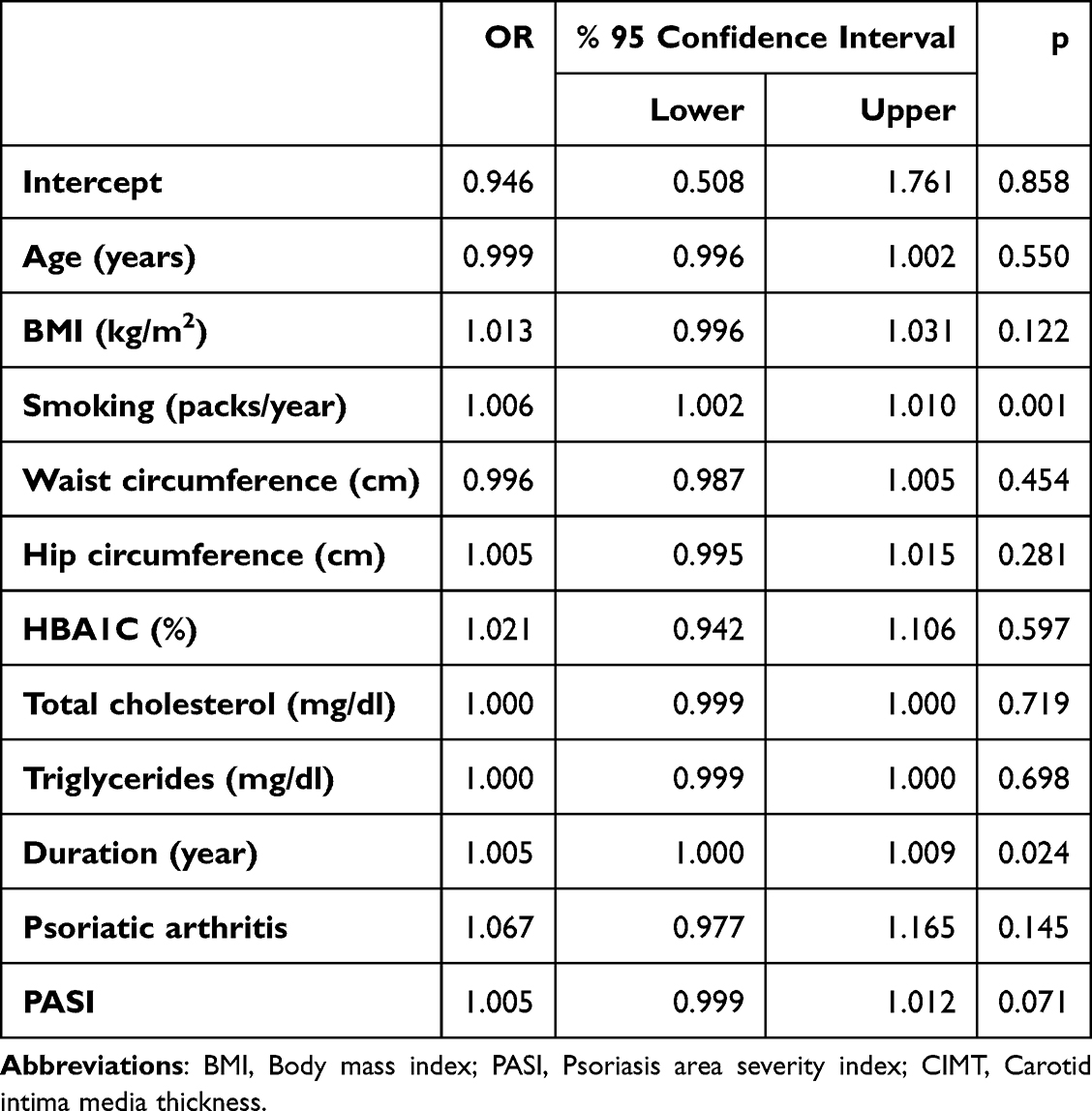 |
Table 4 The Association Between CIMT and Atherosclerosis Risk Factors in Patients with Psoriasis |
Discussions
Although psoriasis is basically a skin disease, it is not limited to the skin but affects many systems, causing various comorbidities such as psoriatic arthritis, metabolic syndrome, autoimmune diseases and cardiovascular diseases. Psoriasis has become an important disease that needs to be addressed in a multidisciplinary manner, as it progresses together with many of these diseases in which widespread systemic inflammations are observed, and complications that sometimes cause mortality occur as a result of these diseases.9
Atherosclerosis is a progressive, inflammatory disease characterized by the accumulation of lipid and fibrous elements in artery walls. In the future, it can lead to serious complications such as myocardial infarction and stroke. Although the reason for the relationship between psoriasis and atherosclerosis is not fully understood, risk factors such as obesity, hypertension, diabetes, hyperlipidemia, metabolic syndrome and smoking, as well as pro-inflammatory cytokines such as TNF-α, IL-1β and IL-6, which are involved in the pathogenesis of psoriasis, cause atherosclerotic plaque formation.4
CIMT is an important parameter that can be easily measured non-invasively with B-mode USG and indicates subclinical atherosclerosis. In this study, the presence of atherosclerosis in patients with psoriasis was examined in comparison with the healthy population through CIMT measurement, which is an important marker of subclinical atherosclerosis. A statistically significant difference was detected between the patient and control groups in terms of mean CIMT (p<0.001). As in studies investigating the direct effect of psoriasis on atherosclerosis after excluding other comorbidities, in this study, the presence of psoriasis alone is a direct risk factor for atherosclerosis.10–14
Smoking and alcohol use are important risk factors for the development of both psoriasis and atherosclerosis.15 This effect of smoking has been attributed to the oxidative stress it causes. As the amount of cigarettes consumed increases, the risk of developing psoriasis increases, as does the severity of psoriasis. In addition, there is a decrease in treatment response due to the effect of various comorbidities caused by smoking.16 In present study, while there was a significant relationship between cigarette use and CIMT in bivariate analysis, this relationship remained significant in multivariate linear regression analysis.
In present study, PASI, one of the most used scorings to express the clinical severity of psoriasis, was used. When PASI was examined in the patient group, a strong positive relationship was detected between mean CIMT and PASI (Table 3). In the multivariate linear regression analysis, PASI remained significant (Table 4). When similar studies in the literature were reviewed, it was reported that a significant relationship was observed between PASI and CIMT in most of the studies.17–19 Based on this, it can be said that as the clinical severity of psoriasis increases, the CIMT value, in other words, the risk of subclinical atherosclerosis, increases significantly.
The duration of psoriasis disease may increase the severity of systemic inflammation caused by the disease. For this reason, it is thought that the duration of the disease may play an important role in the emergence and severity of possible comorbidities. In our study, a strong positive relationship was detected between the average CIMT level and disease duration in the patient group (Table 3). This relationship remained significant as a result of multivariate linear regression analysis. Talaee et al, in their study including 31 psoriasis patients and 31 healthy controls, observed that the CIMT value was measured higher in the patient group and that there was a positive correlation between this value and the duration of the disease.20 Shadidi-Dadras et al included 60 patients with psoriasis and 60 healthy controls in their study and observed that the CIMT value was higher in patients with psoriasis than in the control group. In the patient group, they emphasized that the CIMT value showed a positive correlation with the duration and severity of the disease.12 In the present study, LDL, HDL, and CRP levels did not show a significant association with CIMT. This may be attributable to the modest sample size, exclusion of patients with cardiovascular comorbidities. Although no significant difference in CRP levels was observed between patients and controls, systemic inflammation in psoriasis is well-documented and may not be fully captured by CRP alone. Specific inflammatory mediators, such as IL-17 and IL-23, rather than systemic CRP, may contribute to vascular injury, highlighting the need for future studies to assess these cytokines. Due to the relatively small number of patients with psoriatic arthritis (n=14) and nail involvement, the potential impact of these clinical features on CIMT could only be assessed to a limited extent. New studies with larger and more heterogeneous populations are needed to further investigate these relationships.
Limitations
In our study, manual measurement methods were used in B-mode USG evaluation. The most important limitation of the manual measurement method is the variability in measurements between practitioners and between examinations performed by a single practitioner at different times. In this study, to avoid inter-practitioner variability, the same cardiologist, who was unaware of the clinical diagnosis, gave his opinion in obtaining B-mode USG images. The second limitation is the small number of participants since it was a study conducted in a single center. Multicenter studies with large participants are needed. Another limitation of our study is that a family history of atherosclerosis, which is an important risk factor for atherosclerotic disease, and dietary habits were not systematically assessed. The impact of psoriatic arthritis and nail involvement on CIMT was limited by the small sample size larger studies are needed to confirm these findings.
Conclusion
As in previous similar studies, we observed in our study that psoriasis is a direct risk factor for atherosclerosis after excluding other comorbidities. In addition, according to the results of the multivariate linear regression analysis we performed in patients with psoriasis in our study, the risk of atherosclerosis increases significantly as smoking, disease duration and disease severity increase. As a result, we would like to emphasize that patients with psoriasis should be examined for atherosclerotic disease, and especially those with high smoking status, disease duration and PASI value should be examined more frequently. Considering that psoriasis may increase the risk of atherosclerosis due to systemic inflammation caused by other comorbidities, we would like to emphasize that other comorbidities that may accompany psoriasis should also be investigated.
Ethical Approval
Ethical approval was provided by the Medical Ethics Committee of the Cukurova University Medical School (date: 04.11.2022, number: 27). Informed consent was obtained from each patient. This study was conducted in accordance with the principles of the Declaration of Helsinki.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Van de Kerkhof MCP, Nestle OF. Psoriasis. In: Bolognia JL, Schaffer VJ, Cerroni L, editors. Bolognia Dermatology 4th Ed. China: Elsevier; 2018.
2. Vičić M, Kaštelan M, Brajac I, Sotošek V, Massari LP. Current concepts of psoriasis ımmunopathogenesis. Int J Mol Sci. 2021;22(21):11574. doi:10.3390/ijms222111574
3. Chen HH, Abed SR. Update aetiopathogenesis and treatment of psoriasis: a literature review. J Dermatol Res. 2023;4(1):1–9. doi:10.46889/JDR.2023.4201
4. Szentpetery A, Haroon M, FitzGerald O. Cardiovascular comorbidities in psoriatic disease. Rheumatol Ther. 2020;7:5–17. doi:10.1007/s40744-019-00185-4
5. Reich K. The concept of psoriasis as a systemic inflammation: implications for disease management. J Eur Acad Dermatol Venereol. 2012;26(2):3–11. doi:10.1111/j.1468-3083.2011.04410.x
6. Samarasekera EJ, Neilson JM, Warren RB, Parnham J, Smith CH. Incidence of cardiovascular disease in individuals with psoriasis: a systematic review and meta-analysis. J Invest Dermatol. 2013;133(10):2340–2346. doi:10.1038/jid.2013.149
7. Hansa G, Bhargava K, Bansal M, et al. Carotid intima-media thickness and coronary artery disease: an indian perspective. Asian Cardiovasc Thorac Ann. 2003;11(3):217–221. doi:10.1177/021849230301100308
8. Sinha AK, Eigenbrodt M, Mehta JL. Does carotid intima media thickness indicate coronary atherosclerosis? Curr Opin Cardiol. 2002;17:526–530. doi:10.1097/00001573-200209000-00013
9. Atakan N, Dogan S. Psoriazis sistemik bir hastalık mıdır? Turk J Dermatol. 2012;6(3):123–126. doi:10.5152/tdd.2012.27
10. Yiu K-H, Yeung C-K, Zhao C-T, Chan JC, Siu C-W, Tam S. Prevalence and extent of subclinical atherosclerosis in patients with psoriasis. J Intern Med. 2013;273(3):273–282. doi:10.1111/joim.12002
11. Talari HR, Sehat M, Shayestehpour M, Minaee K, Zamani B. The association of psoriatic arthritis with carotid intima-media thickness. J Kerman Univ Med Sci. 2021;28(2):173–178.
12. Shahidi-Dadras M, Haghighatkhah HR, Abdollahimajd F, Younespour S, Partovi Kia M, Zargari O. Correlation between vascular endothelial growth factor and subclinical atherosclerosis in patients with psoriasis. Int J Dermatol. 2016;55(1):52–59. doi:10.1111/ijd.12842
13. Votrubova J, Juzlova K, Dzambova M, Hercogova J, Gopfertova D. Cardiovascular comorbidities in patients with psoriasis: risk profile including carotide ultrasonography assessed in hospital-based case control study. Acta Dermatovenerol Croat. 2016;24:187–192.
14. Girisha BS, Shibina S, Raghuraja U, Subramanyam K. Carotid intima-media thickness and epicardial fat thickness predict precoronary artery disease status in psoriasis. Indian J Dermatol Venereol Leprol. 2021;87:357–363. doi:10.25259/IJDVL_214_19
15. Naldi L. Psoriasis and smoking: links and risks. Psoriasis Auckl. 2016;6:65–71. doi:10.2147/PTT.S85189
16. Gerdes S, Zahl VA, Weichenthal M, Mrowietz U. Smoking and alcohol intake in severely affected patients with psoriasis in Germany. Dermatology. 2010;220(1):38–43. doi:10.1159/000265557
17. Banska-Kisiel K, Haberka M, Bergler-Czop B, Brzezinska-Wcislo L, Okopien B, Gsior Z. Carotid intima-media thickness in patients with mild or moderate psoriasis. Postep Dermatologi Alergol. 2016;33(4):286–289. doi:10.5114/ada.2016.61605
18. Karoli R, Fatima J, Shukla V, et al. A study of cardio-metabolic risk profile in patients with psoriasis. J Assoc Physicians India. 2013;61:798–803.
19. Ramírez-Terán AL, Vega-Memije ME, Torres-Tamayo M, Martínez-Alvarado MR. Carotid intima-media thickness in patients with psoriasis with and without metabolic syndrome. Arch Cardiol Mex. 2022;92(3):305–311. doi:10.24875/ACM.21000106
20. Talaee R, Talari HR, Moussavi N, Moghaddam AY. Studying the relevance of psoriasis with increased artery intima-media thickness, in patients of skin disease clinics of Kashan Medical Science University in 2016. Int Arch Health Sci. 2020;7:68–72. doi:10.4103/iahs.iahs_49_19
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comorbid Psoriasis and Metabolic Syndrome: Clinical Implications and Optimal Management
De Brandt E, Hillary T
Psoriasis: Targets and Therapy 2022, 12:113-126
Published Date: 25 May 2022
The SELP, CD93, IL2RG, and VAV1 Genes Associated with Atherosclerosis May Be Potential Diagnostic Biomarkers for Psoriasis
Liu S, Liu F, Zhang Z, Zhuang Z, Yuan X, Chen Y
Journal of Inflammation Research 2023, 16:827-843
Published Date: 27 February 2023
Bidirectional Inflammatory Mechanisms and Hematological/Coagulation Dysregulation in Psoriasis Complicated with Atherosclerosis: A Retrospective Hospital-Based Case-Control Study Leveraging the SH-YIMED Clinical Database
Zhang M, Hong M, Cao R, Chen J, Liu L, Sun X, Hong S, Li X
Psoriasis: Targets and Therapy 2026, 16:543978
Published Date: 23 June 2026