Back to Journals » Psoriasis: Targets and Therapy » Volume 16
Bidirectional Inflammatory Mechanisms and Hematological/Coagulation Dysregulation in Psoriasis Complicated with Atherosclerosis: A Retrospective Hospital-Based Case-Control Study Leveraging the SH-YIMED Clinical Database
Authors Zhang M, Hong M, Cao R, Chen J, Liu L, Sun X, Hong S, Li X ![]()
Received 6 March 2026
Accepted for publication 10 June 2026
Published 23 June 2026 Volume 2026:16 543978
DOI https://doi.org/10.2147/PTT.S543978
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Enzo Errichetti
Miao Zhang,1,2,* Munsoon Hong,3,4,* Ruiqing Cao,1,2,* Jiale Chen,1,2 Liu Liu,1,2 Xiaoying Sun,1,2 Seokgyeong Hong,1,2 Xin Li1,2
1Department of Dermatology, Yueyang Hospital of Integrated Traditional Chinese and Western Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China; 2Institute of Dermatology, Shanghai Academy of Traditional Chinese Medicine, Shanghai, People’s Republic of China; 3Department of National Postdoctoral Research Workstation, Lu’an Hospital of Traditional Chinese Medicine, Anhui, People’s Republic of China; 4School of Traditional Chinese Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xin Li, Department of Dermatology, Yueyang Hospital of Integrated Traditional Chinese and Western Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China, Tel +86216516178-3424, Fax +862165162629, Email [email protected] Seokgyeong Hong, Department of Dermatology, Yueyang Hospital of Integrated Traditional Chinese and Western Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China, Tel +86216516178-3424, Fax +862165162629, Email [email protected]
Background: Psoriasis is a chronic inflammatory skin disease associated with systemic inflammation, abnormal hemorheology, and coagulation dysfunction, all of which contribute to the development of atherosclerosis (AS). Inflammation and coagulation are closely intertwined processes; however, studies on the specific profiles of hemorheological and coagulation indices and their synergistic mechanisms remain limited.
Objective: To compare differences in hemorheological and coagulation parameters and preliminarily elucidate the regulatory mechanism of the inflammation-hemorheology-coagulation axis.
Methods: A total of 439 patients with psoriasis and 198 controls were enrolled; after PSM, 206 cases and 126 controls were included. All participants underwent vascular ultrasonography between May 2014 and February 2025. Patients were divided into the case group (psoriasis with AS) and control group (psoriasis without AS) based on vascular ultrasound and clinical assessment by specialized clinicians. PSM was used to balance baseline confounders, and sample sizes varied due to missing data. Statistical analyses included Spearman correlation and multivariate logistic regression.
Results: The case group had higher fibrinogen (FIB) levels (3.54 vs. 3.11, P = 0.005, Cohen’s d = 0.163) and shorter activated partial thromboplastin time (APTT) (26.40 vs. 27.60 s, P = 0.002, Cohen’s d = 0.181). FIB showed the strongest association, with a correlation coefficient of 0.56 (P < 0.001) for systemic immune inflammation index (SII) and 0.39 (P < 0.001) for neutrophil-to-lymphocyte ratio (NLR) in the case group, and there was a strong positive correlation between SII and FIB (r = 0.56, P < 0.001). Psoriasis inflammation directly promoted vascular inflammation with a large effect size (β = 0.45, P < 0.001). Multivariate logistic regression analysis showed WBV (whole blood viscosity) (1 mPa·s) was the strongest predictor, with an OR of 1.752 (95% confidence interval [CI]: 1.314– 2.651, P < 0.001).
Limitations: Selection and recall biases of retrospective single-center studies.
Conclusion: Patients with psoriasis, particularly those with severe disease, long disease duration, or complications from other thrombotic factors, should be closely monitored for hemorheological and coagulation parameters to prevent cardiovascular disease occurrence.
Keywords: psoriasis, atherosclerosis, hematological, coagulation, inflammation-hemorheology-coagulation axis
Introduction
Psoriasis is a common immune-mediated skin disorder that affects approximately 2–4% of the global population.1 Cumulative evidence has confirmed that psoriasis is associated with a higher prevalence of cardiovascular risk factors such as atherosclerosis (AS), hypertension, dyslipidemia, obesity, and metabolic syndrome.2–5
Numerous large-sample epidemiological studies have confirmed that blood fluidity, plasma viscosity (PV), and hematocrit are independent risk factors for cardiovascular events.6–9 Hypercoagulability is a potential mechanistic link underlying the association between cardiovascular disease (CVD) and psoriasis. Notably, there is growing recognition that inflammation and coagulation are interconnected biological processes.10,11
Persistent inflammation in psoriasis may induce hemorheological abnormalities and inflammatory pathway activation, while concurrently activating the coagulation system and suppressing fibrinolytic function, which ultimately synergistically accelerates the occurrence and progression of AS.12,13 Systemic immune inflammation index (SII) and neutrophil-to-lymphocyte ratio (NLR) are well-established markers of systemic inflammation. However, research on the specific characteristics of hemorheological and coagulation indices and their synergistic mechanisms of action remains limited.
This study focused on patients with psoriasis complicated by AS, compared the differences in hemorheological and coagulation parameters, and preliminarily elucidated the regulatory mechanism of the inflammation-hemorheology-coagulation axis.
Methods
In accordance with the STROBE Statement for Observational Study Reporting, this study followed all the recommended guidelines, and the associated case–control study checklist is provided in Table S1.
Study Design
This study was approved by the Institutional Review Board of Yueyang Hospital of Integrated Traditional Chinese and Western Medicine, Shanghai University of Traditional Chinese Medicine (Approval No. 2024–034). All procedures were performed in accordance with the principles of the Declaration of Helsinki. The requirement for informed consent was waived due to the retrospective nature of the study. All collected datasets encompassing the vascular ultrasound findings were anonymized according to institutional medical record regulations.
This was a single-center, retrospective, case-control study that incorporated propensity score matching (PSM). A retrospective extraction and review of medical records was performed for inpatients with plaque psoriasis at our tertiary referral hospital from May 2014 to February 2025 using a standardized Clinical Data Retrieval System. The enrolled patients were divided into a case group (psoriasis combined with AS, defined as the comorbid group) and a control group (psoriasis without AS, defined as the simple psoriasis group) according to the vascular ultrasound results and evaluation by specialized clinicians.
Study Inclusion and Exclusion Criteria
For the case group, the enrollment criteria were defined as concurrent adherence to the diagnostic standards outlined in the 2023 Full Version of Chinese Guidelines for Psoriasis Diagnosis and Treatment14 and the Chinese Guidelines for Cardiovascular Disease Prevention,15 corroborated by comprehensive clinical, pathological, and imaging evidence. For the control group, eligible patients were those who met only the diagnostic criteria for psoriasis, were free of AS and other CVDs, and had unremarkable findings on corresponding diagnostic tests. Additionally, patients in both groups were required to satisfy the following inclusion criteria: (1) availability of complete, retrievable routine blood test results obtained within 3 months before enrollment; (2) age ranging from 18 to 75 years; and (3) completion of a vascular ultrasound examination at our hospital.
The exclusion criteria were as follows: (1) comorbidity with malignant tumors, decompensated liver cirrhosis, uremia, other autoimmune diseases, or a history of acute infection/trauma within one month before enrollment; (2) administration of glucocorticoids for >2 weeks or non-psoriasis immunosuppressants within 3 months before enrollment, including severe malnutrition, metabolic disorders, and heavy drinking history; and (3) missing key case data, refusal to provide informed consent, or poor treatment compliance.
Collection of Relevant Data
Demographic, clinical, and laboratory data of the enrolled patients were retrieved from the hospital’s electronic database. The evaluated laboratory parameters included whole blood viscosity (WBV) (200), WBV (50), WBV (1), PV, hematocrit, red blood cell (RBC) aggregation index, prothrombin time (PT), activated partial thromboplastin time (APTT), fibrinogen (FIB), D-dimer, neutrophils, lymphocytes, and platelets (PLT). For patients who visited multiple hospitals during the study period, the data from their first visit were extracted and included in the dataset.
Statistical Analysis
PSM was conducted in R v.3.3.3 (R Foundation for Statistical Computing) using the MatchIt package v.3.0.2. Baseline characteristics are summarized in Table 1, using the variables included in the propensity score model to assess covariate balance before and after matching. Subsequent analyses were performed in the matched cohort using all available data for each outcome of interest. Therefore, the sample size varied slightly across the analyses depending on data completeness. To secure an adequate sample size and optimal group balance, iterative testing of multiple calipers was conducted with the final number of calipers fixed at 0.15. The baseline characteristics of the two matched groups were compared, and standardized mean differences (SMDs) were calculated to verify the balance of the pre-specified confounders.
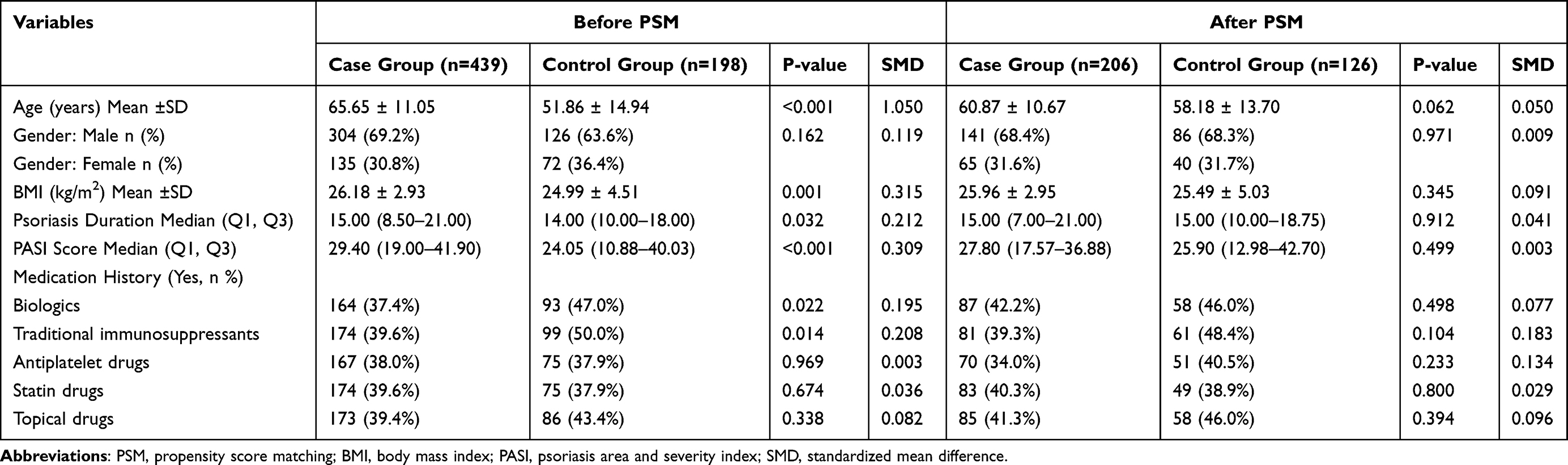 |
Table 1 Baseline Characteristics of Case and Control Groups Before and After PSM |
The Shapiro–Wilk test was used to assess the data distribution normality. Categorical variables were presented as frequencies (n) and percentages (%), whereas continuous variables were expressed as mean ± standard deviation (SD) if normally distributed or median (interquartile range, [IQR]) if non-normally distributed. Intergroup comparisons for continuous variables were performed using the Mann–Whitney U-test, those for categorical variables were performed using the chi-square test, and Spearman correlation coefficients were calculated to assess the correlations between variables. A multivariate logistic regression model was used to calculate the odds ratio (OR), 95% confidence interval (95% CI), and P value for each indicator.
Results
Characteristics of the Study Population
After PSM, the matched cohort comprised 206 patients and 126 controls, with all baseline covariates achieving statistical balance (Table 1). All P-values exceeded 0.05, and the SMDs for all variables were < 0.1, a threshold indicative of a negligible imbalance. As key examples, the SMD for age decreased from 1.050 to 0.050, and the SMD for the PASI score dropped from 0.309 to 0.003. The improvement in covariate balance is clearly visualized in Figures S1, and S2 further supports the effectiveness of the PSM.
Comparison of Hemorheological Indicators and Coagulation Levels Between Groups
Furthermore, the hemorheological and coagulation parameters were compared between the case and control groups, with the key findings summarized in Table 2, Figures S3 and S4. The case group exhibited substantially elevated WBV across all shear rates: at 200 s−1, the median WBV was 7.75 mPa·s (IQR: 5.26–9.43) in cases versus 5.31 mPa·s (IQR: 4.88–5.68) in controls. The PV, Hct, and RBC aggregation indices were also significantly higher in the case group, with the RBC aggregation index showing the largest effect size (Cohen’s d = 0.699). Statistically significant differences were also observed for both FIB and APTT: the case group had higher FIB levels (3.54 vs. 3.11, P = 0.005, Cohen’s d = 0.163) and a shorter APTT (26.40 vs. 27.60 s, P = 0.002, Cohen’s d = 0.181), with both effects being small in magnitude.
 |
Table 2 Comparison of Hemorheological and Coagulation Indicators Between Case Group and Control Group |
Associations of SII and NLR with Key Hemorheological and Coagulation Parameters
First, as shown in Figure S5, the case group exhibited significantly higher levels of the inflammatory markers SII and NLR than the control group. The case group exhibited markedly higher SII values (median: 1,245 vs. 123, P < 0.001) and significantly elevated NLR (median: 4.2 vs. 1.8, P < 0.001) than the controls.
Following these observations, the relationships between SII, NLR, and key hemorheological and coagulation parameters were further examined (Figure 1). Specifically, FIB showed the strongest association, with a correlation coefficient of 0.56 (P < 0.001) for the SII and 0.39 (P < 0.001) for NLR in the case group, respectively (Figure 2). In contrast, hemorheological parameters, including WBV, PV, and hematocrit, showed only weak or insignificant correlations with SII and NLR, with correlation coefficients generally < 0.15.
 |
Figure 1 Spearman correlation heatmap of hemorheological/coagulation indicators with SII and NLR in case vs. control groups. Spearman correlation heatmap showing the correlation between hemorheological/coagulation parameters, SII and NLR. The heatmap is divided into two panels: left for the case group and right for the control group. Columns represent SII and NLR, and rows represent hemorheological and coagulation indicators as labeled on the left axis. The color gradient indicates the magnitude of Spearman correlation coefficient r, with red representing positive correlation and blue representing negative correlation. Significance levels: *P < 0.05, ***P < 0.001. Analyses were conducted in a propensity score-matched cohort. Abbreviations: SII, systemic immune inflammation index; NLR, neutrophil-to-lymphocyte ratio; WBV, whole blood viscosity; RBC, red blood cell; FIB, fibrinogen; PT, prothrombin time; APTT, activated partial thromboplastin time; FDP, fibrin/fibrinogen degradation product. |
 |
Figure 2 Correlation between SII and FIB in case vs. control groups. Scatter plot showing the correlation between SII (x-axis) and FIB (y-axis) levels. Red triangles and red linear regression line represent the case group (n = 180), blue circles and blue linear regression line represent the control group (n = 117). Spearman correlation analysis showed a strong positive correlation between SII and FIB in the case group (r = 0.56, da 0.001) but no significant correlation in the control group (r = 0.09, P = 0.356). Analyses were conducted in a propensity score-matched cohort using the available data for each variable. Abbreviations: SII, systemic immune-inflammation index; FIB, fibrinogen. |
There was a strong positive correlation between the SII and FIB (r = 0.56, P < 0.001), with the red scatter points and fitted line clearly demonstrating that the FIB levels increased significantly as the SII increased. No statistically significant correlations were observed between the SII and hemorheological parameters in either group (Figure S6).
Mediation Pathway of Psoriasis Inflammation Promoting AS via Vascular Inflammation and Coagulation Dysfunction
Figure S7 illustrates the mediation pathway through which psoriatic inflammation contributes to AS, involving vascular inflammation and rheology/coagulation dysfunction. Psoriasis inflammation directly promoted vascular inflammation with a large effect size (β = 0.45, P < 0.001). Vascular inflammation also exerted a direct positive effect on AS (β = 0.28, P = 0.010). AS was also found to exacerbate vascular inflammation via a feedback mechanism (β = 0.33, P = 0.002), pointing to a self-reinforcing vicious cycle that may accelerate disease progression.
As demonstrated in the clustering heatmap (Figure 3), the case group displayed a distinct systemic disorder profile, progressing sequentially from skin inflammation to systemic inflammation, coagulation dysfunction, and vascular injury.
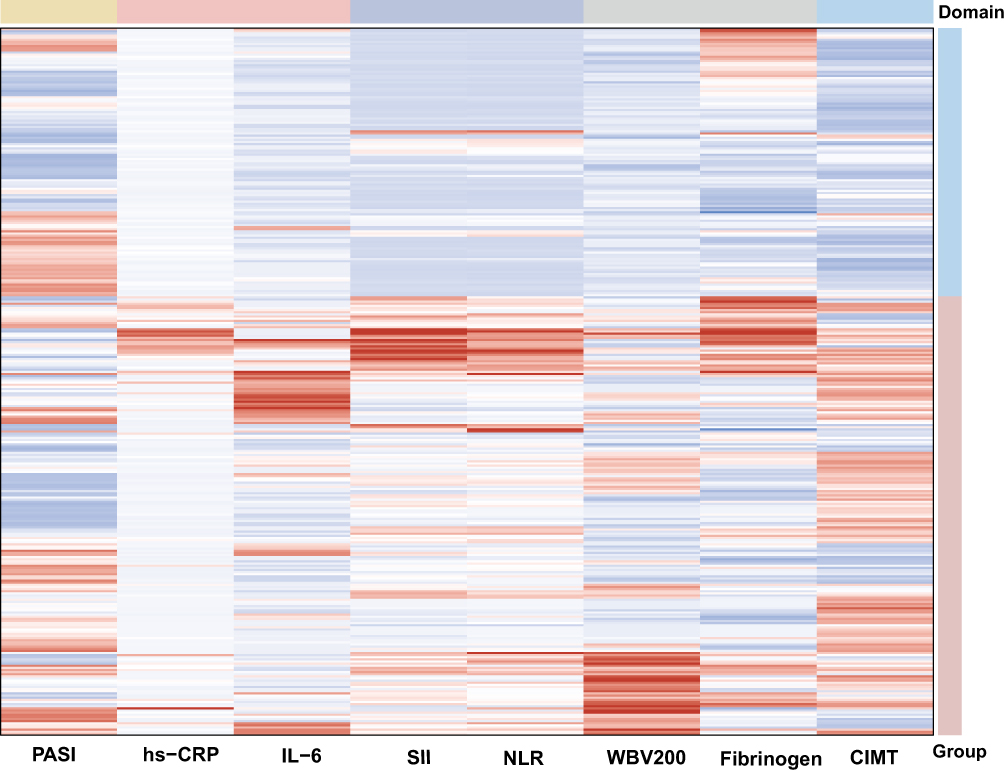 |
Figure 3 Integrated heatmap of inflammation–coagulation–vascular injury profiles in case vs. control groups. Heatmap of normalized and integrated Z-score showing the expression profiles of inflammation, hemorheological–coagulation, and vascular injury indicators. Columns represent detected indicators including PASI, hs-CRP, IL-6, SII, NLR, WBV200, fibrinogen, and CIMT as labeled on the bottom axis. Rows represent individual subjects. The color gradient represents Z-score values, ranging from negative (blue) to positive (red). Vertical color bars on the right indicate sample groups: pink for case group (n = 206), light blue for control group (n = 126). Top horizontal color bars indicate indicator domains: yellow for skin inflammation, blue for systemic inflammation, pink for vascular inflammation, grey for rheology/coagulation, light blue for vascular injury. Abbreviations: SII, systemic immune inflammation index; NLR, neutrophil-to-lymphocyte ratio; WBV, whole blood viscosity; hs-CRP, high-sensitivity C-reactive protein; IL-6, interleukin-6; CIMT, carotid intima-media thickness. |
Disease Duration-Dependent Differences in FIB Levels Between Groups
The subgroup analysis showed that FIB elevation was significantly correlated with the duration of psoriasis (Figure S8). The case group exhibited significantly higher FIB levels (3.82 ± 1.40) compared with the control group (3.19 ± 0.90) (P < 0.001).
Multivariate Logistic Regression Analysis of Independent Risk Factors for AS in Patients with Psoriasis
Multivariate logistic regression analysis showed WBV (1 mPa·s) was the strongest predictor, with an OR of 1.752 (95% CI: 1.314–2.651, P < 0.001). Per 1-SD increase, the OR rose to 424.060 (95% CI: 18.942–36,850.113, P < 0.001). The RBC aggregation index was also a significant independent risk factor, with an OR of 3.546 (95% CI: 2.105–7.275, P < 0.001). Per 1-SD increase, the OR was 65.052 (95% CI: 11.648–696.234, P < 0.001) (Table S2).
Discussion
Our case-control analysis revealed that patients with psoriasis complicated by AS had significantly higher WBV, PV, and RBC aggregation indices than those with psoriasis alone (P < 0.05). This comorbid group also presented with markedly elevated FIB and platelet counts, coupled with a significant reduction in APTT (P < 0.05). In contrast, the psoriasis-only group exhibited only mild FIB elevation and abnormal whole-blood viscosity. These findings suggest that hemorheological disorders and a hypercoagulable state play crucial roles in the development and progression of psoriasis complicated by AS.
Given the paucity of hemorheological and coagulation studies focusing on patients with psoriasis complicated by AS, it is difficult to compare our findings with those of other relevant studies. Alpsoy et al demonstrated that FIB levels were elevated in patients with psoriasis, which were negatively correlated with aortic strain and aortic compliance but positively correlated with the β-stiffness index.16 This finding is consistent with the conclusions of our study. Increased FIB synthesis induced by inflammatory stimulation is causally associated with thrombosis.17,18
Patients with psoriasis exhibit a persistent inflammatory state.19 Inflammatory cytokines such as tumor necrosis factor – α and interleukin - 6 can damage the structure of RBC membranes, leading to decreased RBC deformability and increased aggregation.20–22 AS directly induces vascular wall thickening and luminal stenosis, while elevated blood viscosity further exacerbates blood stasis and tissue perfusion defects, continuously aggravating vascular endothelial injury.23,24
Admittedly, inflammation and coagulation are interconnected processes.10,25 The vascular endothelium also plays a critical role in clot formation, as it acts as the interface linking inflammation and coagulation.26,27 Chronic inflammation in psoriasis activates the extrinsic coagulation pathway, prompting vascular endothelial cells to release tissue factors and leading to hypercoagulability.28,29 Meanwhile, inflammation suppresses the expression of anticoagulant factors, including proteins C and S, thereby exacerbating the hypercoagulable state.30
The study’s results identified striking associations between inflammatory indices and key hemorheological and coagulation parameters, with FIB increasing in parallel with increasing SII values. Heatmaps revealed a unique systemic disorder profile in the case group, featuring a sequential pathological cascade from cutaneous to systemic inflammation, coagulation dysfunction, and vascular injury. These observations underscore a pivotal inflammation-vascular-coagulation axis. Psoriasis is associated with increased circulating inflammatory cytokines that promote endothelial inflammation and dysfunction, which further induce platelet activation and coagulation abnormalities, thereby increasing the risk of cardiovascular events in affected patients.
This study has several notable limitations. First, reliance on a single-center patient cohort with a relatively small sample size may have compromised the statistical power, hindering the ability to validate potential causal associations. Second, this study was restricted to a retrospective review of routine clinical records from our institution, which may have omitted critical confounding variables and detailed anamnesis information, leading to potential retrospective biases. Moreover, recall bias may have introduced inaccuracies into the data reported by clinicians or patients. Large-scale, multicenter, prospective cohort studies are needed to determine the predictive role of hemorheological and coagulation parameters for AS risk in patients with psoriasis.
Conclusion
Patients with psoriasis, especially those with severe disease, long disease duration, or other thrombotic predisposing factors, should be closely monitored for hemorheological and coagulation parameters to prevent CVD occurrence. Further studies are warranted to comprehensively elucidate the roles of hemorheological and coagulation parameters, including their potential diagnostic and prognostic utility.
Role of Funder/Sponsor Statement
The National Natural Science Foundation of China had no role in the design or conduct of the study; the collection, management, analysis, and interpretation of the data; the preparation, review, or approval of the manuscript; or the decision to submit the manuscript for publication.
Access To Data And Data Analysis
The corresponding author of this article (Xin Li) had full access to all study data and took responsibility for the integrity of the data and the accuracy of the data analysis.
Abbreviation
APTT, Activated partial thromboplastin time; AS, Atherosclerosis; CI, Confidence interval; CVD, Cardiovascular disease; FIB, Fibrinogen; IQR, Interquartile range; OR, Odds ratio; PLT, Platelet; PT, Prothrombin time; PV, Plasma viscosity; PSM, Propensity score-matched; RBC, Red blood cell; SD, Standard deviations; SMDs, Standardized mean differences; WBV, Whole blood viscosity.
Data Sharing Statement
Data supporting the findings of this study are available from the corresponding author (Xin Li) upon request.
Ethical Approval
This study was approved by the Institutional Ethics Committee of Yueyang Hospital of Integrated Traditional Chinese and Western Medicine, Shanghai University of Traditional Chinese Medicine (#2024-034). All procedures were performed in accordance with the Declaration of Helsinki. Informed consent was waived due to the retrospective and anonymous nature of the study. The authors are accountable for all aspects of this study and ensure that questions related to the accuracy or integrity of any part of the study are investigated and resolved appropriately.
Acknowledgment
The authors thank all participants involved in the study.
Author Contributions
Miao Zhang, Munsoon Hong, and Ruiqing Cao share first authorship. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Key Research and Development Program (No. 2024YFC3505301, 2024YFC3505304), the 2National Natural Science Foundation of China (No: 82374445, W2433194), Shanghai Hospital Development Center Foundation(No. SHDC12025132),CACMS Innovation Fund(No. CI2023C018LH), Shanghai Oriental Talent Program for Top-notch Project (No. BJWS2024046), CACM Eaglet Program for Cultivating Young Clinical Talents in Chinese Medicine(CYJH2024022),2025 Shanghai Municipal Health Commission Seed Program for Medical New Technology Researchand Translation(No.2025ZZ1010), and the Clinical Cohort Shanghai (No. SHDC2025CCsS013).
Disclosure
The authors declare no conflict of interest.
References
1. Armstrong AW, Read C. Pathophysiology, clinical presentation, and treatment of psoriasis: a review. JAMA. 2020;323(19):1945–11. doi:10.1001/jama.2020.4006
2. Takeshita J, Grewal S, Langan SM, et al. Psoriasis and comorbid diseases: epidemiology. J Am Acad Dermatol. 2017;76(3):377–390. doi:10.1016/j.jaad.2016.07.064
3. Wang J, Yu Y, Liu L, et al. Global prevalence of obesity in patients with psoriasis: an analysis in the past two decades. Autoimmun Rev. 2024;23(6):103577. doi:10.1016/j.autrev.2024.103577
4. Zhang M, Fan S, Hong S, et al. Epidemiology of lipid disturbances in psoriasis: an analysis of trends from 2006 to 2023. Diabetes Metab Syndr. 2024;18(8):103098. doi:10.1016/j.dsx.2024.103098
5. Zhang M, Chen J-L, Fan S-W, et al. Epidemiology of hypertension in psoriasis: an analysis of trends from 2006 to 2023. Psoriasis. 2025;15:443–453. doi:10.2147/PTT.S532112
6. Yarnell JW, Patterson CC, Sweetnam PM, et al. Haemostatic/inflammatory markers predict 10-year risk of IHD at least as well as lipids: the Caerphilly collaborative studies. Eur Heart J. 2004;25(12):3468–3477. doi:10.1016/j.ehj.2004.04.011
7. Lowe G, Rumley A, Norrie J, et al. Blood rheology, cardiovascular risk factors, and cardiovascular disease: the West of Scotland coronary prevention study. Thromb Haemost. 2000;84(10):553–558. doi:10.1055/s-0037-1614066
8. Koenig W, Sund M, Ernst E, et al. Association between plasma viscosity and blood pressure: results from the MONICA-project augsburg. Am J Hypertens. 1991;4(6):529–536. doi:10.1093/ajh/4.6.529
9. Ernst E, Koenig W. Hemorheology, thrombogenesis, and atherosclerosis. Semin Thromb Hemost. 1993;19(2):99–103.
10. Foley JH, Conway EM. Cross talk pathways between coagulation and inflammation. Circ Res. 2016;118(9):1392–1408. doi:10.1161/CIRCRESAHA.116.306853
11. Esmon CT. The interactions between inflammation and coagulation. Br J Haematol. 2005;131(4):417–430. doi:10.1111/j.1365-2141.2005.05753.x
12. Piaserico S, Orlando G, Messina F. Psoriasis and cardiometabolic diseases: shared genetic and molecular pathways. Int J Mol Sci. 2022;23(16).
13. Siegel D, Devaraj S, Mitra A, et al. Inflammation, atherosclerosis, and psoriasis. Clin Rev Allergy Immunol. 2013;44(2):194–204. doi:10.1007/s12016-012-8308-0
14. Committee on Psoriasis Chinese Society of Dermatology. Guideline for the diagnosis and treatment of psoriasis in China (2023 edition). Chin J Dermatol. 2023;56(7):573–625.
15. Thrombosis CMACBCAoRMCPaRCCSoGaGCCCMDACPB. Chinese guidelines for primary prevention of cardiovascular diseases. Chinese J Cardiovascular Dis. 2020;48(12):1000–1038.
16. Alpsoy S, Akyuz A, Erfan G, et al. Atherosclerosis, some serum inflammatory markers in psoriasis.. Giornale italiano di dermatologia e venereologia: organo ufficiale. Societa italiana di dermatologia e sifilografia. 2014;149(2):167–175.
17. Machlus KR, Cardenas JC, Church FC, et al. Causal relationship between hyperfibrinogenemia, thrombosis, and resistance to thrombolysis in mice. Blood. 2011;117(18):4953–4963. doi:10.1182/blood-2010-11-316885
18. Macrae FL, Swieringa F, Heemskerk JWM, et al. High fibrinogen γ′ levels in patient plasma increase clot formation at arterial and venous shear. Blood Adv. 2021;5(17):3468–3477. doi:10.1182/bloodadvances.2020003346
19. Arican O, Aral M, Sasmaz S, et al. Serum levels of TNF- α, IFN- γ, IL-6, IL-8,IL-12, IL-17, and IL-18 in patients with active psoriasis andcorrelation with disease severity. Mediators Inflamm. 2005;2005(5):273–279. doi:10.1155/MI.2005.273
20. Lazari D, Freitas Leal JK, Brock R, et al. The relationship between aggregation and deformability of red blood cells in health and disease. Front Physiol. 2020;11:288. doi:10.3389/fphys.2020.00288
21. Kim DS, Shin D, Jee H, et al. Red blood cell distribution width is increased in patients with psoriasis vulgaris: a retrospective study on 261 patients. J Dermatol. 2015;42(6):567–571. doi:10.1111/1346-8138.12865
22. Şener G, Inan Yuksel E, Gökdeniz O, et al. The relationship of hematological parameters and C-reactive Protein (CRP) with disease presence, severity, and response to systemic therapy in patients with psoriasis. Cureus. 2023;15(8):e43790. doi:10.7759/cureus.43790
23. Lynch M, Ahern T, Sweeney CM, et al. Adipokines, psoriasis, systemic inflammation, and endothelial dysfunction. Int J Dermatol. 2017;56(11):1103–1118. doi:10.1111/ijd.13699
24. Harrington CL, Dey AK, Yunus R, et al. Psoriasis as a human model of disease to study inflammatory atherogenesis. Am J Physiol Heart Circ Physiol. 2017;312(5):H867–h73. doi:10.1152/ajpheart.00774.2016
25. Ma Y, Zhou Y, Wu F, et al. The bidirectional interactions between inflammation and coagulation in fracture hematoma. Tissue Eng Part B Rev. 2019;25(1):46–54. doi:10.1089/ten.teb.2018.0157
26. Abeyama K, Stern DM, Ito Y, et al. The N-terminal domain of thrombomodulin sequesters high-mobility group-B1 protein, a novel antiinflammatory mechanism. J Clin Invest. 2005;115(5):1267–1274. doi:10.1172/JCI22782
27. Iwaki T, Cruz DT, Martin JA, et al. A cardioprotective role for the endothelial protein C receptor in lipopolysaccharide-induced endotoxemia in the mouse. Blood. 2005;105(6):2364–2371. doi:10.1182/blood-2004-06-2456
28. Levi M, van der Poll T. Two-way interactions between inflammation and coagulation. Trends Cardiovasc Med. 2005;15(7):254–259. doi:10.1016/j.tcm.2005.07.004
29. Szotowski B, Antoniak S, Poller W, et al. Procoagulant soluble tissue factor is released from endothelial cells in response to inflammatory cytokines. Circ Res. 2005;96(12):1233–1239. doi:10.1161/01.RES.0000171805.24799.fa
30. Samad F, Ruf W. Inflammation, obesity, and thrombosis. Blood. 2013;122(20):3415–3422. doi:10.1182/blood-2013-05-427708
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comorbid Psoriasis and Metabolic Syndrome: Clinical Implications and Optimal Management
De Brandt E, Hillary T
Psoriasis: Targets and Therapy 2022, 12:113-126
Published Date: 25 May 2022
The SELP, CD93, IL2RG, and VAV1 Genes Associated with Atherosclerosis May Be Potential Diagnostic Biomarkers for Psoriasis
Liu S, Liu F, Zhang Z, Zhuang Z, Yuan X, Chen Y
Journal of Inflammation Research 2023, 16:827-843
Published Date: 27 February 2023
Evaluation of Atherosclerosis Risk in Patients with Psoriasis
Celik L, Akray A, Denli Y, Aksungur VL
Clinical, Cosmetic and Investigational Dermatology 2026, 19:574241
Published Date: 29 January 2026