Back to Journals » Clinical Ophthalmology » Volume 19
Estimating the Prevalence and Severity of Isolated Small-Angle Strabismic Amblyopia
Authors Arnold RW ![]()
Received 12 June 2025
Accepted for publication 27 August 2025
Published 16 September 2025 Volume 2025:19 Pages 3409—3418
DOI https://doi.org/10.2147/OPTH.S546692
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Video abstract presented by Arnold.
Views: 55
Robert W Arnold
Alaska Blind Child Discovery, Alaska Children’s EYE & Strabismus, Anchorage, Alaska, 99508, USA
Correspondence: Robert W Arnold, Alaska Blind Child Discovery, Alaska Children’s EYE & Strabismus, 3500 Latouche #280, Anchorage, Alaska, 99508, USA, Tel +1 907 561-1917, Fax +1 907 563-5373, Email [email protected]
Background: Isolated small-angle (< 20PD) strabismic amblyopia (is-asa) is not obvious to parents and pediatricians and can be missed by current photoscreeners. To improve early screening methods, the previously unknown prevalence and severity of is-asa is estimated from a twenty-year prospective observation.
Methods: Published population data from the Multi-Ethnic and Baltimore Pediatric Eye Disease Studies (MEPEDS and BPEDS) were combined to estimate the cumulative prevalence. Then prospective, consecutive digital images of Brückner Test from 2003 to 2025 by one pediatric ophthalmologist were obtained with confirmatory exams. These were then compared to Alaska population and vision screening data.
Results: From MEPEDS and BPEDS community screening data, patients with all strabismus, constant strabismus and strabismic amblyopia were stratified by strabismus angle suggesting that isolated small-angle strabismus (is-as) may occur in 1/200 children while is-asa may be 1/400 children. Over 22 years, 34 Alaska Brückner patients had isolated, constant strabismus less than 20 prism diopters of which 9 presented with amblyopia of which 4 had post-treatment residual amblyopia worse than 20/40. Considering population, doctors and referral rates, the Alaska prevalence of is-as is about 1 in 700 (0.03– 0.24%) children while is-asa is about 1 in 7000 (0.006– 0.024%) children.
Conclusion: From two imperfect sources; review of large community screening studies and from prospective Brückner Test analysis, the prevalence of isolated small-angle strabismic amblyopia is so rare that future screening methods would require very high specificity. The Rebion blinq and 2WIN CR-function can identify is-asa in older children. Current photorefraction methods with early specific instrument referral criteria followed by sensitive acuity screening are still effective since is-asa is so rare.
Keywords: amblyopia, Brückner, strabismus, prevalence, vision screening
Introduction
The development of valid screening techniques requires an understanding of disease prevalence and severity.1 Deliberate community screening efforts are indicated for serious diseases that are occult meaning they do not manifest with obvious signs and symptoms. Severe, eccentric fixation strabismic amblyopia is precisely such a feared, blinding disease of children.
Amblyopia is the most common treatable reason for pediatric vision loss when the brain fails to acquire the ability to resolve fine visual acuity.2 Amblyopia is caused by one or more risk factors; refractive error, strabismus or deprivation. The prevalence of some of the amblyopia risk factors has already been estimated.3 While deprivational amblyopia can be severe due to early, dense cataract or media opacity, it is fortunately less common type of amblyopia than the two other forms. The newborn, red reflex test is an effective AAP-guideline method for timely detection of deprivational amblyopia. According to well-designed, large scale community studies called the Multi-Ethnic Pediatric Eye Disease Study (MEPEDS)4 and the Baltimore Pediatric Eye Disease Study (BPEDS),5 and through two decades of recruitment data from the multicentered Pediatric Eye Disease Investigator Group (PEDIG) studies,6 about 1/3 of pediatric amblyopia 20/40 and worse is due to refractive error, 1/3 due to pure strabismus and 1/3 due to a combination of strabismus and refractive error. Less than 5% of amblyopia cases are due to deprivation.7 Strabismic amblyopia with eccentric fixation is a particularly severe type of amblyopia.8 Strabismic amblyopia is usually due to constant misalignment and can have magnitudes of deviation that are large (angle between eyes of more than 20 prism diopters (PD) or it can be small angle (less than 15–20 PD). Strabismic amblyopia can occur by itself (isolated) or it can co-exist with high refractive error (mixed amblyopia). The interaction between amblyopia risk factors including isolated small-angle strabismus (is-as) and isolated small-angle strabismic amblyopia (is-asa) can be illustrated by a Venn Diagram (Figure 1).
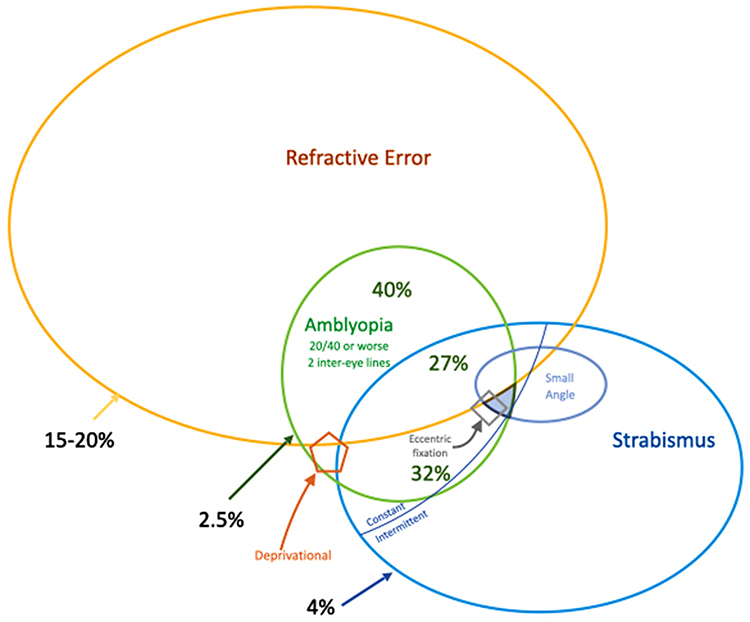 |
Figure 1 Venn diagram of inter-related amblyopia risk factors. The percent prevalence estimates for the main three non-deprivational types of amblyopia and risk factors are taken from MEPEDS and BPEDS published studies. The pentagon represents rare deprivational amblyopia prevalence. A sub-set of strabismus patients have isolated small-angle strabismus (is-as) without refractive error. In the constant strabismic patients, the filled blue “triangle” is for isolated small-angle strabismic amblyopia (is-asa) some of which may have feared-, and refractory- eccentric fixation. |
Strabismic amblyopia can be combined mechanism with refractive error, or isolated with just pure, constant strabismus. Strabismic amblyopia often manifests as an observable large deviation in the eyes with one eye fixing and the other deviating – usually esotropia or exotropia. Approximately 3–4% of children have strabismus.4,5 About half of pediatric strabismus is intermittent and therefore much less likely to cause amblyopia. As a result of being observable by parents and pediatricians, manifest, large-angle strabismus is less needy of deliberate well-child screening after the age of 1–2 years.9 There are also cases of strabismus with small angle which may not be obvious to the parent and previously very difficult to detect by the pediatrician. Small angle strabismus can be detected by the Brückner Test,10,11 by the Adaptica 2WIN with CR-infrared occluder function,12 and by the relatively new Rebion blinq.13 Strabismus less than 12 prism diopters is harder for observers to detect.14,15 Brückner Test is capable of detecting 2–3 degrees of strabismus or more.16 Careful inspection of some types of photoscreening images can miss small, constant ocular deviation and strabismus can exaggerate estimated refractive error.17 The prevalence of these cases of isolated small-angle strabismus (is-as) is not known. In addition, the severity of isolated, small-angle strabismic amblyopia (is-asa) is not yet known.
Once children are old enough to understand and communicate, monocular visual acuity screening can reliably identify strabismic amblyopia. Then a confirmatory examination can rule out other causes of vision loss including refractive amblyopia and deprivational amblyopia. Visual acuity testing takes 3–5 minutes per child whereas objective screening can be done in less than 30 seconds. School vision screening allocates time and monetary resources in various ways and at different grade levels. However, by age 8 years (3rd grade) most public-school students have had visual acuity screening. Unless the child peeks behind a hand or occluder, almost all cases of amblyopia can be detected by school-age, visual acuity screening. Unfortunately, severe, eccentric fixation amblyopia detected in school may be refractory to current, conventional amblyopia therapy. We do not yet know whether different methods should be employed for widespread early objective screening to capture eccentric fixation amblyopia earlier.
The prevalence of various types of amblyopia and its risk factors can be influenced by racial and ethnic mix. The development, refinement and implementation of methods for early amblyopia detection are augmented by knowledge of risk factor prevalence.18
The Alaska Blind Child Discovery project (ABCD-Vision.org) over three decades has given local advice about methods and instrument referral criteria hoping for the most cost-effective amblyopia therapy in a region of America with very expensive travel.19,20 Hyper-sensitive strabismus screening by eccentric red-reflex photoscreeners was therefore discouraged.21 Parents and pediatricians can accurately screen for large-angle strabismic amblyopia.9,22 Experienced pediatricians can also have high yield with Enhanced Brückner screening.22
There are past, present and emerging tools for the early detection of amblyopia when therapy is most effective. The screening tools are imperfect, but much better than no screening. Optimization of imperfect screening tools requires knowledge of disease prevalence. Since, we do not yet know the prevalence and the severity of isolated small-angle strabismic amblyopia, therefore this estimate of the prevalence of isolated small-angle strabismic amblyopia comes from three sources; 1) careful analysis of published American pediatric population studies and from review of multicenter amblyopia studies and 2) from over two decades of a personal quest to deliberately record of all cases of isolated Brückner Test from one pediatric ophthalmologist (RWA). The third 3) is an illustrative case report:
Case Report
Actual scenario presented to highlight some screening and therapeutic challenges of a severe case: A child for their first five years had an undetected, isolated small-angle constant strabismus of 4–8 prism diopters esotropia with minimal hyperopia of +0.50 D OU. To the parents and pediatrician, the eyes looked normal. No photoscreening was done. In Kindergarten, the un-patched visual acuity was passed both eyes as 20/40. In first grade, the school nurse performed patched, distance 20/32 critical-line visual acuity screening and this child failed the left eye. The child replied, “You patched my good eye”. The confirmatory pediatric ophthalmology examination revealed externally normal appearing eyes, but a cover test of constant 4 PD esotropia and positive 4 base-out (BO) test. There was no family history of eye disease. The polarized Titmus stereo showed positive fly but 800 seconds of arc circles and the left eye suppressed distance and near. Retinomax showed −0.50 OU. Cycloplegic refraction showed +0.25+0.25x104 right eye and PLANO+0.25x96 left eye. The refractive estimate from the infrared multi-radial photoscreener (2WIN) was confounded since it reported 7–10 PD of left esotropia. Rebion blinq yielded a refer (Figure 2). Enhanced Brückner Test was positive left eye. Best corrected visual acuity was 20/25 right eye and 20/200 left eye and some eccentric fixation was observed in the left eye. Patching therapy 2 hours per day only resulted in acuity 20/20 right eye and 20/160 left eye after 4 months with moderate compliance. Dichoptic therapy with eye-tracking (Curesight, Airport City, Israel) 4 more months with +0.50 spectacles yielded 20/20 right eye, 20/100- left eye and 400 seconds of arc stereo. The parent, pediatrician, school nurse and pediatric ophthalmologist still hoped for a better result. The patient was also frustrated but preferred dichoptic videos over patching. Would earlier or other amblyopia screening or therapy have yielded better vision?
 |
Figure 2 Patient with Brückner Test and isolated small-angle strabismic amblyopia (is-asa) left eye holding binocular birefringent screener capable of detecting isolated, small-angle strabismus. |
Methods
Table 1 shows amblyopia and strabismus data from MEPEDs and BPEDs data totaling 11,342 children of whom 6771 had reliable visual acuities. These community screening findings are compared to 2306 patients from the Pediatric Eye Disease Investigator Group (PEDIG) which has conducted several multicenter trials of therapies for amblyopia called the Amblyopia Treatment Studies (ATS).23–31 Direct access to original data from MEPEDS, BPEDS or ATS was not available and thus this study relies on analysis of published summary results which may have differing cut-offs for strabismus angle levels. Typical patients with best corrected monocular visual acuity of 20/40 or worse or an inter-eye difference of 2 or more lines are then categorized as pure refractive, pure strabismic and mixed mechanism. Of 2306 from several ATS reports that excluded deprivational amblyopia, the patients with pure refractive were 40±6%, pure strabismic 32±7% and mixed mechanism amblyopia 27±6%. The difference in prevalence types between PEDIG and the community screening studies is related to initial pre-enrollment therapy. MEPEDS/BPEDS data represents initial screening prevalence while more recent PEDIG enrollment includes some patients with prior 16-week refractive therapy.
 |
Table 1 Summary Data from Amblyopia and Strabismus Numbers Separated by Race and Ethnicity for Multi-Ethnic Pediatric Eye Disease Study (MEPEDS) and the Baltimore Pediatric Eye Disease Study (BPEDS) Studies Compared to the Pediatric Eye Disease Investigator Group (PEDIG) Amblyopia Treatment Studies (ATS) |
Actual patients with Enhanced Brückner Test including some with isolated small-angle strabismus were prospectively recorded using available and emerging screening techniques over the last two decades from two consecutive private pediatric ophthalmology practices. Emerging devices were adjusted for luminance and distance to optimize refractive estimates and capture of red reflex asymmetry. The Brückner Test and photoscreening have been integral parts of every pediatric in-office eye exam32 for all these patients. The Alaska Blind Child Discovery has IRB approval from Providence Alaska Medical Center and is compliant with the Declaration of Helsinki and HIPAA. Parents provided written informed consent to share video/images for educational purposes.
Images were collected from retrievable digital images of positive Brückner Tests from 2003 through 2025. Patients from the multi-location practice of one pediatric ophthalmologist were included in this prevalence estimate study if able to complete acuity and get a digital image/assessment of Brückner Test. They were excluded if they had PEDIG-ATS qualifying high refractive error and were greater than 20 PD constant strabismus or with prior eye surgery. Table S1 gives de-identified data regarding consecutive, prospectively collected cases of Brückner Test due to isolated small angle strabismus (is-as).
Characteristics of the Brückner Test were captured by various, evolving vision screening devices including digital flash cameras, infrared photoscreeners, and the birefringent binocular Rebion blinq. Refractions were estimated by photorefractive devices and confirmed by retinoscopy with accommodation appropriately relaxed (cycloplegia). Visual acuity was performed with best correction and monocularity insured with a “No-Peeking” patch. Stereopsis was measured with Titmus fly and/or PDI Check.
The numbers of children by age seen by single pediatric ophthalmologist, in the only subspecialty pediatric ophthalmology practice and for the entire state of Alaska are collected from practice data and state public health data. Alaska is unique in that it is vastly separated from the continental United States and very little eye care crosses state lines. The Alaska Blind Child Discovery, a charitable research project (www.ABCD-Vision.org) has been developing, validating and utilizing state-of-the-art sensory and objective vision screening technology from 1995 through 2025 following deliberate early experience with teaching and utilizing Brückner Test.10 Estimates on vision screening efficiency are taken from school nursing, charitable Lion’s club screening and Alaska Blind Child Discovery data.
Results
The cumulative prevalence from MEPEDS and BPEDS data (Table 1) of all strabismus, constant strabismus and strabismic amblyopia as a function of strabismus angle is shown in Figure 3. The confidence for these estimates is greatest for all cases of strabismus separated by divisions of angle less than 10 prism diopters, 10–25 prism diopters and for all angles since only this data was published. Confidence is also high for the prevalence of all angles of constant strabismus and for all angles of strabismic amblyopia. Less confidence (unpublished data) is indicated in Figure 3 with dashed instead of solid lines as the proportion of all strabismus due to constant angle and due to strabismic amblyopia for smaller angles; this interpolation assumes similar percent contributions for constant and amblyopic strabismus by angle. If that assumption is close, then constant small angle strabismus less than 15 prism diopters is about 0.6% and isolated small-angle strabismic amblyopia (is-asa) less than 15 prism diopters is less than 0.2%.
 |
Figure 3 Estimated cumulative prevalence of all strabismus, constant strabismus and strabismic amblyopia based on strabismic angle from MEPEDS and BPEDS population screening studies. Superimposed are box plots from Alaska Brückner Test patients providing an estimate of the rarity of isolated small-angle strabismus (is-as; orange) and isolated small-angle strabismic amblyopia (is-asa; green). |
Table S2 gives data for calculation of prevalence of isolated small-angle strabismus (is-as) and amblyopia (is-asa) in Alaska. The medians and ranges of this data are estimated from extensive coordination of the Alaska Blind Child Discovery (www.ABCD-Vision.org). From 2003 to 2025, pediatric ophthalmology was covered by two, and later three specialists. The birthrate in Alaska has stayed steady at about 10,000 babies per year. Intense vision screening education for pediatricians including emerging technology was provided through this period, at times emphasizing Brückner and at other times, reducing instrument referral rates for small-angle strabismus. Patients with refractory amblyopia have a high likelihood of secondary referral to pediatric ophthalmologists while an older, isolated strabismus with good visual acuity from remote optometrists in Alaska are less likely to expend resources to travel for tertiary care. In a given year, the majority of Brückner referrals from Alaska pediatricians could have been directed to the author, while other years they would have been equally divided between three pediatric ophthalmologists. Therefore, the low prevalence estimates assume almost all cases are included in the database from 10,000 children per year. The higher prevalence assumes three times this number of cases and only half the state of Alaska available for referral. Estimates of actual isolated, small-angle strabismic amblyopia (is-asa) are likely more thorough than small angle strabismus with good presenting acuity since remote optometrists are more likely to seek expensive referral travel for cases of sight-threatening refractory strabismic amblyopia.
From 22 years, deliberate surveillance of Brückner test in by one of Alaska’s 3 pediatric ophthalmologists, 34 cases of digitally imaged, isolated, small-angle constant strabismus less than 20 prism diopters were retrieved (Table S1). Of these, 31 had esotropia and 3 had constant exotropia. The maximum angle of 15–20 prism diopters was chosen as a not visibly obvious magnitude and would only be included in a small subset of PEDIG patients if they are eventually published. All refractive errors were less than 3 diopters of hyperopia, less than 1.5 diopters spherical equivalent anisometropia, less than 1.75 diopters of cylinder and myopia magnitude less than 1.5 diopters. Early visible-light screeners including the iPhone 4 which led to David Huang’s commercial development of GoCheck Kids photoscreener, and the Canon TX-1 were particularly helpful.33–36 Since 2019, the Rebion blinq correctly referred seven of seven cases of isolated small-angle constant strabismus with or without amblyopia (https://vimeo.com/502462313?share=copy). Of the 9 of the 34 cases who presented with amblyopia worse than 20/40, treatment improved vision in 7 with residual amblyopia worse than 20/40 in 4. No residual amblyopia worse than 20/40 persisted in the 11 cases between 14 and 20 prism diopters but three of them eventually had strabismus surgery for increased magnitude manifest strabismus of 20–25 prism diopters esotropia.
Table S2 gives estimates of prevalence of isolated small-angle strabismus (is-as) and associated amblyopia (is-asa) from a single investigator and for the entire state of Alaska. The range of estimation is influenced by several factors including population, number of pediatric ophthalmologists, years collecting digital Brückner, efficiency of referral and access to pediatric ophthalmology including during COVID-19. From retrieved sequential digital images of Brückner test over 22 years, 34 cases were between 5 and 20 prism diopters and 23 cases had constant strabismus less than 15 prism diopters. Of those presenting with amblyopia worse than 20/40, 9 (26%) were between 5 and 20 prism diopters and 8 (35%) were less than 15 prism diopters. Over the 22 years, two or three pediatric ophthalmologists examined patients throughout Alaska, however this data is only from one. The intensity of deliberate urban and remote37 Alaskan vision screening by Brückner Testing,22 photoscreening21 and patched acuity testing38,39 varied over two decades for which estimates of prevalence are adjusted. The median and range estimate of all cases of Brückner test due to isolated constant strabismus less than 20 diopters is about 1 in 700 (280–2300) children. Similarly, the prevalence of isolated strabismic amblyopia less than 20 prism diopters is estimated to be 1 in 7000 (3700–14,000) Alaskan children while those amblyopia cases due to strabismus less than 15 prism diopters are estimated to be 1 in 8000 (4200–15,000).
Discussion
This paper highlights more than 3 decades of my quest to comprehend the impact of a feared, occult reason for pediatric vision loss. Two of my brilliant colleagues, David Guyton and David Hunter, developed portable binocular birefringent vision screening.40 Rebion blinq can detect isolated, small-angle strabismus however there remain challenges with this complex technology. The patient must fixate on a tiny, flashing red smiley face which is difficult for many infants and toddlers. As a result, blinq is quite reliable in older, amblyopic children, but has a high inconclusive rate for early amblyopia screening. It is not known whether very early detection of small-angle strabismus might afford better treatment options for eccentric fixation, but we suspect it might.41
Isolated small-angle constant strabismus is very rare with about 1 case in 700 children less than 20 prism diopters and about 1 in 1000 smaller magnitude than 15 prism diopters. The majority had presenting vision of 20/40 or better. The prevalence of isolated small-angle strabismic amblyopia is very rare; it is estimated to be just 1 in 8000 children, however about half of those had persistent amblyopia worse than 20/40 despite therapy. In comparison, this may be less than the prevalence of deprivational amblyopia at about 0.03–0.1%.7
Limitations of this prevalence estimation study include assuming similar angle-based proportions of amblyopia and constant smaller-angle given known total strabismus prevalence. Direct granular data from MEPEDS, BPEDS and PEDIG ATS would be helpful. The Alaska data has consistent, deliberate attempts to capture images of Brückner Test during confirmatory examinations when refractive error, visual acuity and strabismus angle could be quantified. Early in this period, non-digital photographic methods were being replaced by digital and thus some cases were possibly missed in a digital review. The ability to capture Brückner may have differed somewhat between contemporary devices. Alaska has had a concerted vision screening effort in urban and remote areas, but referral efficiency for cases of small angle constant strabismus and for strabismic amblyopia may have varied over the study period. The Rebion blinq has been used in confirmatory exams, but not widely in community screening due to the concern that the expensive, round device could roll off a table as the result of frequent Alaskan natural, or child-induced “earthquakes”. The dichoptic therapy used in this study was Curesight with eye-tracking and it is not known if virtual headset Luminopia or Vivid Vision would have achieved similar results.
Since very rare, methods of screening require very high specificity which is beyond the capacity of current technology. Over two decades of ABCD screening, early visible-light screeners including the iPhone and the Canon TX-1 were particularly helpful at documenting Brückner Test.33–36 One current technologically complex method, the Rebion blinq, has good sensitivity for detection of isolated small-angle constant strabismus in cooperative children.13 Further advances in fixation methods may improve blinq testability in very young children but the ideal device must have low un-readable rates and high specificity. Emerging dichoptic therapeutic options offer new hope for certain cases of amblyopia.42 If isolated small-angle strabismic amblyopia can be detected earlier and intensely treated, there might be hope to reduce my 44% failure rate in eliminating the permanent vision loss from this hidden, feared pediatric blinding disease.
Conclusion
Isolated, small-angle strabismus seems quite rare, but occasionally is associated with severe amblyopia. Effective future screening techniques should be designed to work for very young children and have very high specificity. Until then, current photorefractive screening methods with specific instrument referral criteria that might not directly target isolated small-angle strabismus are still satisfactory and cost effective since this feared condition appears to be exceedingly rare.
Abbreviations
2WIN, infrared photoscreener from Adaptica, Padova, Italy; 4 BO, 4 PD base-out strabismus test; ABCD, Alaska Blind Child Discovery (www.ABCD-Vision.org); ambly, amblyopia; Aniso, anisometropia; ATS, Amblyopia Treatment Study; Bilat, bilateral; Blinq: Rebion birefringent scanner; BPEDS, Baltimore Pediatric Eye Disease Study; CR, corneal reflex infrared occluder function of the Adaptica 2WIN; D, diopter; ET, esotropia; HIPAA, Health Insurance portability and accountability act; IRB, institutional review board; Is-as, isolated small-angle strabismus; Is-asa, isolated small-angle strabismic amblyopia; MEPEDS, Multi-Ethnic Pediatric Eye Disease Study; MTI, Polaroid photoscreener; P, Plusoptix infrared photoscreener from Nuremberg, Germany; PD, prism diopters; PDI Check, autostereoscopic vision game (Anchorage, Alaska); PEDIG, Pediatric Eye Disease Investigator Group; Strab, strabismic; TX-1, Canon high-magnification digital camera model; XT, exotropia.
Acknowledgment
Thanks to my partners Robin Grendahl, MD and Kevin Winkle, MD, and to Sean P Donahue, MD, PhD, Sue Cotter, OD and Michael X. Repka, MD, MPH for data and encouragement.
Disclosure
Dr. Arnold coordinates the Alaska Blind Child Discovery project which has received discounted vision screening technology from several vendors. He is a board member and patent holder for PDI Check which provides autostereoscopic vision screening games. Dr. Arnold is also a protocol developer and investigator for the Pediatric Eye Disease Investigator Group.
References
1. Wilson J, Junger G. Principles and practice of screening for disease. Public Health paper No 34. World Health Organization; 1968.
2. Wu C, Hunter DG. Amblyopia: diagnostic and therapeutic options. Am J Ophthalmol. 2006;141(1):175–184. doi:10.1016/j.ajo.2005.07.060
3. Arnold RW. Amblyopia risk factor prevalence. J Pediatr Ophthalmol Strabismus. 2013;50(4):213–217. doi:10.3928/01913913-20130326-01
4. MEPEDS, Multi-ethnic Pediatric Eye Disease Study G. Prevalence of amblyopia and strabismus in African American and Hispanic children ages 6 to 72 months the multi-ethnic pediatric eye disease study. Ophthalmology. 2008;115(7):1229–1236e1. doi:10.1016/j.ophtha.2007.08.001.
5. Friedman DS, Repka MX, Katz J, et al. BPEDS. Prevalence of amblyopia and strabismus in white and African American children aged 6 through 71 months the baltimore pediatric eye disease study. Research Support, N.I.H. Extramural. Ophthalmology. 2009;116(11):2128–34e1–2. doi:10.1016/j.ophtha.2009.04.034.
6. Holmes JM, Lazar EL, Melia BM, et al. Effect of age on response to amblyopia treatment in children. meta-analysis research support, N.I.H. extramural research support, Non-U.S. Gov’t. Arch Ophthalmol. 2011;129(11):1451–1457. doi:10.1001/archophthalmol.2011.179.
7. Elflein HM, Fresenius S, Lamparter J, et al. The prevalence of amblyopia in Germany: data from the prospective, population-based Gutenberg Health Study. Dtsch Arztebl Int. 2015;112(19):338–344. doi:10.3238/arztebl.2015.0338
8. Mehmed B, Fronius M, Pohl T, et al. Electronically monitored occlusion therapy in amblyopia with eccentric fixation. Graefes Arch Clin Exp Ophthalmol. 2022;260(5):1741–1753. doi:10.1007/s00417-021-05416-5
9. Rosner J, Rosner J. Parents as screeners for strabismus in their children. J Visual Impair Blindness. 1988;82:193–194. doi:10.1177/0145482X8808200508
10. Arnold RW. Vision screening in Alaska: experience with enhanced Brückner test. Alaska Med. 1993;35(2):204–208.
11. Tongue A, Cibis G. Bruckner test. Ophthalmol. 1981;88:1041–1044. doi:10.1016/S0161-6420(81)80034-6
12. Arnold SL, Arnold AW, Sprano JH, Arnold RW. Performance of the 2WIN photoscreener with “CR” strabismus estimation in high risk patients. Am J Ophthalmol. 2019;207:195–203. doi:10.1016/j.ajo.2019.04.016
13. Arnold RW. Comparative AAPOS validation of the blinq birefringent amblyopia screener with isolated small-angle strabismus. Clin Ophthalmol. 2020;14:325–329. doi:10.2147/OPTH.S242335
14. Moses MA, Spurrier RL, Ange BL, Brooks SE. Small-angle strabismus detection by telemedicine in an experimental model. J AAPOS. 2023;27(5):279e1–279e4. doi:10.1016/j.jaapos.2023.08.003
15. Larson SA, Keech RV, Verdick RE. The threshold for the detection of strabismus. J AAPOS. 2003;7(6):418–422. doi:10.1016/j.jaapos.2003.09.011
16. Miller JM, Hall HL, Greivenkamp JE, Guyton DL. Quantification of the Bruckner test for strabismus. Invest Ophthalmol Vis Sci. 1995;36(5):897–905.
17. Miller JM, Schwiegerling J, Leising-Hall H, Surachatkumtonekul T. Detection of improper fixation in MTI photoscreening images. J AAPOS. 2001;5(1):35–43. doi:10.1067/mpa.2001.111012
18. Arnold RW, Donahue SP, Silbert DI, et al. Uniform guidelines for pediatric vision screen validation 2021. J AAPOS. 2022;26(1):p1.e1–1.e6. doi:10.1016/j.jaapos.2021.09.009
19. Arnold RW, Gionet EG, Jastrzebski AI, et al. The Alaska Blind Child Discovery project: rationale, methods and results of 4000 screenings. Alaska Med. 2000;42(3):58–72.
20. Arnold RW, Donahue SP. The yield and challenges of charitable state-wide photoscreening. Binocul Vis Strabismus Q. 2006;21(2):93–100.
21. Arnold RW, Tulip D, McArthur E, et al. Predictive value from pediatrician Plusoptix screening: impact of refraction and binocular alignment. Binoc Vis and Strabismus Quart. 2012;27(4):227–232.
22. Arnold RW, Stange CA, Ryan C. The compared predictive value of Bruckner, acuity and strabismus from pediatric referrals. Am Orthopt J. 2006;56(1):15–21. doi:10.3368/aoj.56.1.15
23. PEDIG. A randomized trial of atropine vs. patching for treatment of moderate amblyopia in children. Arch Ophthalmol. 2002;120(3):268–278. doi:10.1001/archopht.120.3.268
24. Repka MX. A randomized trial of patching regimens for treatment of moderate amblyopia in children. Arch Ophthalmol. 2003;121(5):603–611.
25. PEDIG, Repka MX, Cotter SA. A randomized trial of atropine regimens for treatment of moderate amblyopia in children. Ophthalmology. 2004;111(11):2076–2085.
26. Scheiman MM, Hertle RW, Beck RW, et al. Randomized trial of treatment of amblyopia in children aged 7 to 17 years. Arch Ophthalmol. 2005;123(4):437–447.
27. Pediatric Eye Disease Investigator G. A randomized trial of near versus distance activities while patching for amblyopia in children aged 3 to less than 7 years. multicenter study randomized controlled trial research support, N.I.H. extramural research support, Non-U.S. Gov’t. Ophthalmology. 2008;115(11):2071–2078. doi:10.1016/j.ophtha.2008.06.031.
28. PEDIG. Pharmacological plus optical penalization treatment for amblyopia: results of a randomized trial. Comparative study multicenter study randomized controlled trial research support, N.I.H. Extramural. Arch Ophthalmol. 2009;127(1):22–30. doi:10.1001/archophthalmol.2008.520.
29. Scheiman MM, Hertle RW, Kraker RT, et al. Patching vs atropine to treat amblyopia in children aged 7 to 12 years: a randomized trial. Comparative Study Multicenter Study Randomized Controlled Trial Research Support, N.I.H. Extramural Research Support, Non-U.S. Gov’t. Arch Ophthalmol. 2008;126(12):1634–1642. doi:10.1001/archophthalmol.2008.107
30. Rutstein RP, Quinn GE, Lazar EL, et al. A randomized trial comparing Bangerter filters and patching for the treatment of moderate amblyopia in children. Comparative study multicenter study randomized controlled trial research support, N.I.H. extramural. Ophthalmology. 2010;117(5):998–1004e6. doi:10.1016/j.ophtha.2009.10.014
31. Wallace DK, Lazar EL, Holmes JM, et al. Pediatric Eye Disease Investigator Group. A randomized trial of increasing patching for amblyopia. Ophthalmology. 2013;120(11):2270–2277. doi:10.1016/j.ophtha.2013.04.008.
32. Schaafsma JD, Arnold RW. Pre-cycloplegic exam benefit of photoscreening and accommodation-relaxing skiascopy. Clin Ophthalmol. 2024;18:833–846. doi:10.2147/OPTH.S454430
33. Arnold RW, Davis B, Arnold LE, Rowe KS, Davis JM. Calibration and validation of nine objective vision screeners with contact lens-induced anisometropia. J Pediatr Ophthalmol Strabismus. 2013;50(3):184–190. doi:10.3928/01913913-20130402-02
34. Arnold RW, Armitage MD. Performance of four new photoscreeners on pediatric patients with high risk amblyopia. J Pediatr Ophthalmol Strabismus. 2014;51(1):46–52. doi:10.3928/01913913-20131223-02
35. Arnold RW, Arnold AW, Stark L, Arnold KK, Leman RE, Armitage MD. Amblyopia detection by camera (ADBC): gateway to portable, inexpensive, vision screening. Alaska Med. 2004;46(3):63–72.
36. Raza SA, Amitava AK, Gupta Y, et al. Canon CP-TX1 camera - As a screening tool for amblyogenic risk factors. Ind j ophthalmol. 2022;70(4):1313–1316. doi:10.4103/ijo.IJO_2161_21
37. Lang D, Leman R, Arnold AW, Arnold RW. Validated portable pediatric vision screening in the Alaska Bush. A VIPS-like study in the Koyukon. Alaska Med. 2007;49(1):2–15.
38. Clausen MM, Armitage MD, Arnold RW. Overcoming barriers to pediatric visual acuity screening through education plus provision of materials. J AAPOS. 2009;13(2):151–154. doi:10.1016/j.jaapos.2008.10.018
39. Arnold RW, Stark L, Leman R, Arnold KK, Armitage MD. Tent photoscreening and patched HOTV visual acuity by school nurses: validation of the ASD-ABCD protocol. (Anchorage School District- Alaska Blind Child Discovery program). Binocul Vis Strabismus Q. 2008;23(2):83–94.
40. Gramatikov BI, Zalloum OH, Wu YK, Hunter DG, Guyton DL. Directional eye fixation sensor using birefringence-based foveal detection. Appl Opt. 2007;46(10):1809–1818. doi:10.1364/ao.46.001809
41. Kirk VG, Clausen MM, Armitage MD, Arnold RW. Preverbal photoscreening for amblyogenic factors and outcomes in amblyopia treatment: early objective screening and visual acuities. Arch Ophthalmol. 2008;126(4):489–492. doi:10.1001/archopht.126.4.489
42. Wygnanski-Jaffe T, Kushner BJ, Moshkovitz A, Belkin M, Yehezkel O, CureSight Pivotal Trial G. An eye-tracking-based dichoptic home treatment for amblyopia: a multicenter randomized clinical trial. Ophthalmology. 2023;130(3):274–285. doi:10.1016/j.ophtha.2022.10.020
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The UCI EyeMobile Preschool Vision Screening Program: Refractive Error and Amblyopia Results from the 2019–2020 School Year
Hunter SC, He J, Han M, Suh DW
Clinical Ophthalmology 2022, 16:4249-4255
Published Date: 20 December 2022
Standard Amblyopia Therapy in Adults with Longstanding Amblyopia Improves Visual Acuity and Contrast Sensitivity
Ridder WH III, Patel R, Li YX, Staubli U
Clinical Ophthalmology 2023, 17:1847-1858
Published Date: 29 June 2023
Refractive Risk Factors for Amblyopia in Turkish Preschoolers: A School-Based Vision Screening Study of 1126 Children
Küçük N, Canturk Uğurbaş S, Alpay A, Uğurbaş SH
Clinical Ophthalmology 2026, 20:597262
Published Date: 22 May 2026