Back to Journals » Clinical Ophthalmology » Volume 20
Refractive Risk Factors for Amblyopia in Turkish Preschoolers: A School-Based Vision Screening Study of 1126 Children
Authors Küçük N ![]() , Canturk Uğurbaş S, Alpay A, Uğurbaş SH
, Canturk Uğurbaş S, Alpay A, Uğurbaş SH
Received 19 January 2026
Accepted for publication 12 May 2026
Published 22 May 2026 Volume 2026:20 597262
DOI https://doi.org/10.2147/OPTH.S597262
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sotiria Palioura
Numan Küçük, Sılay Canturk Uğurbaş, Atilla Alpay, Suat Hayri Uğurbaş
Department of Ophthalmology, Zonguldak Bülent Ecevit University, Zonguldak, Turkiye
Correspondence: Numan Küçük, Zonguldak Bulent Ecevit University Faculty of Medicine, Department of Ophthalmology, Zonguldak, Turkiye, Tel +90 (536) 323 80 08, Email [email protected]
Purpose: To evaluate refractive risk factors for unilateral and bilateral amblyopia.
Methods: In October 2019, 1126 preschool and primary school 1st grade students in Kozlu district of Zonguldak province underwent eye screening with a pediatric autorefractometer in a school environment. 125 children who were above the threshold values determined for refractive errors or for whom measurements could not be taken due to patient compliance were referred to us for eye examination. The referred children underwent a comprehensive eye examination. Amblyopia risk factors were analyzed with a logistic regression model.
Results: Of the 125 referred children 106 were examined comprehensively. Of those 99 were analyzed. A total of 30 amblyopic children were identified (Unilateral amblyopia n=20, bilateral amblyopia n=10). The prevalence of amblyopia was found to be 2.6%. In regression analysis, presence of < 2 D and 2– 4 D hyperopia were found to be isolated risk factors for amblyopia (p< 0.05). Astigmatism was a risk factor unilateral and bilateral amblyopia in univariate analysis (p=0.001, p=0.001 respectively). Incrementing values of anisometropia did not influence the development of amblyopia. However, the incidence rate of amblyopia increased in the incrementing diopters of anisometropia (11.4% at 0.5 D and below, 25.9% at 0.5– 1 D range, 54.5% at 1– 2 D range, 100% for 2 D and above). Myopia association with amblyopia was not statistically significant.
Conclusion: We found lower than the generally accepted threshold values of hypermetropia, astigmatism and anisometropia to be risk factors for amblyopia. Our data can help shape threshold values and screening policies for refractive errors. More population-based studies are needed in different regions of our country in order to make guidelines consisting of optimal threshold values that can be used in amblyopia screening programs.
Keywords: amblyopia, strabismus, plusoptix, photoscreening
Introduction
Amblyopia is the most important cause of monocular visual impairment in children and is characterized by asymmetrical development of visual function in the absence of organic abnormalities. Strabismus and refractive errors are two well-known risk factors for amblyopia in children.1,2 The incidence of amblyopia varies between societies, but it varies between 1% and 5% in the world.3–6 Population-based reports from various regions of Turkiye have shown that the prevalence of amblyopia is between 1.1% and 5.5%.7–11 Visual impairment due to amblyopia continues throughout life and results in a more profound visual impairment if not treated promptly.12
Identification of refractive risk factors is essential to identify children who are expected to benefit from treatment and to assist in screening programs. PlusoptiX (PlusoptiX, Nuremberg, Germany) is an infrared-powered photoscanner primarily used for screening refractive errors in the pediatric population and was first introduced to the market in 1995. It performs this screening without requiring cycloplegia.13 It can measure binocular spherocylindrical refractive values between −7 and +5 diopters. At higher values, it alerts as HYP for hyperopia and MYO for high myopia. PlusotiX has set threshold referral values for the screening program, ranging from sensitive to specific, depending on the user.14
The absence of standardized threshold values continues to challenge amblyopia screening strategies. For example, recently published guidelines by French Strabismus Society provide evidence-based recommendations on refractive error cut-off values that may serve as a useful reference framework for screening programs.15
Methods
The study included preschool and first-grade primary school children aged 36 to 84 months in Kozlu district of Zonguldak province. All children underwent eye screening with a pediatric autorefractometer in a school environment. The students referred as a result of the screening were examined in the Eye Diseases Clinic of the Health Application and Research Center of the Faculty of Medicine of Bülent Ecevit University. The study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the Bülent Ecevit University Clinical Studies Ethics Committee in 2019. Informed consent and assent were obtained from the parents and guardians of the children. The screening program was conducted in 25 different schools in October 2019 and a total of 1126 children were screened with the PlusoptiX S12R (PlusoptiX S12R Nuremberg, Germany). The refractive thresholds used in this study were intentionally set to favor high sensitivity for amblyopia risk detection in preschool children. The criteria of hyperopia ≥ +2.50 D, astigmatism ≥ +1.50 D, and anisometropia ≥ 1.00 D correspond to lower refractive cut-offs within the Plusoptix screening range and are closer to the more sensitive ROC settings (ROC 1–2). The referral criteria for Plusoptix are presented in Table 1. This approach was chosen to minimize the risk of false-negative results, ensuring that children with clinically significant refractive errors are not missed during screening.
 |
Table 1 Referral Criteria Threshold Values for Plusoptix by Age |
Children for whom the device could not obtain measurements, who were above the threshold value, or for whom measurements could not be performed due to patient compliance underwent a comprehensive eye examination in our clinic (Figure 1). Of the 125 children referred as a result of the screening conducted between November 2019 and February 2020, 106 children were evaluated for amblyopia.
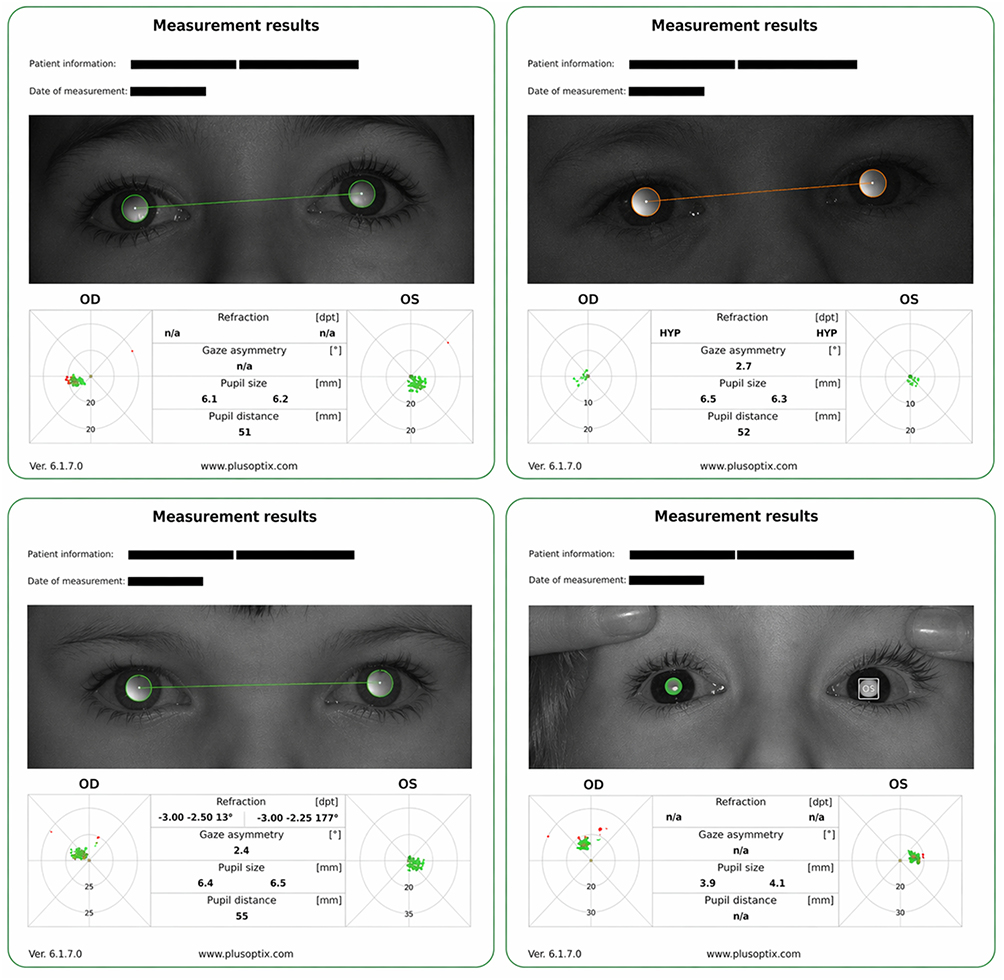 |
Figure 1 Patient who could not take measurements with Plusoptix (top left), Patient who was detected to have high hyperopia (top right), Patient who was above the threshold value (bottom left), Patient who could not take measurements due to poor compliance (bottom right). |
Best corrected visual acuity (BCVA), anterior segment and posterior segment examinations were recorded for all referred children. Snellen chart was used for literate children and Lea symbols were used for those who could not read and write. Cover test and alternating cover test were applied to each child for near fixation and far fixation. Eye movements in all directions were evaluated. Cycloplegic retinoscopy was performed 35 minutes after 1% cyclopentolate instillation. Children with low visual acuity for age were prescribed the necessary eyeglass lenses and called for a repeat visual examination 4–6 weeks later.
Children with no eye pathology other than amblyopia, strabismus and refractive error and participants with complete file examination findings were included in the study. Patients who were not within the appropriate age range (<36 months, >84 months), whose vision could not be assessed and who had undergone any eye surgery were excluded from the study.
Amblyopia was defined according to best-corrected visual acuity (BCVA) and interocular differences, using age-adjusted criteria. Unilateral amblyopia was defined as an interocular difference of at least two lines in BCVA between the two eyes, in the absence of any structural ocular pathology sufficient to account for the reduced vision. Bilateral amblyopia was defined based on age-specific BCVA thresholds reflecting expected visual development. For children aged 36–47 months, bilateral amblyopia was diagnosed when BCVA was worse than 20/50 (0.4 logMAR) in both eyes. For children aged 48–72 months, the threshold was BCVA worse than 20/30 (0.18 logMAR) in both eyes, consistent with improved visual acuity expected in older preschool children. The definitions are consistent with pediatric vision screening recommendations and amblyopia preferred practice pattern guidelines issued by AAPOS (American Association for Pediatric Ophthalmology and Strabismus).16
Classification of Risk Factors
Refractive errors were classified as <0.5 D, ≥0.5 D-<2 D, ≥2 D for myopia, <2 D, ≥2 D-<4 D, ≥4 D for hyperopia, <1 D, ≥1 D-<2 D, ≥2 D for astigmatism, and <0.5 D, ≥0.5 D-<1 D, ≥1 D-<2 D, ≥ 2 D for anisometropia. For the evaluation of unilateral amblyopia, the values of the poor eye with higher refractive errors were used for analysis, while for bilateral amblyopia, the spherical and cylindrical values of the good eye with lower refractive errors were used. The objective of the analysis was to determine the lowest refractive error thresholds associated with amblyopia by evaluating the relationship between increasing levels of hyperopia, astigmatism, and anisometropia and the presence of amblyopia. Strabismus examination was classified as strabismus present or no strabismus.
Statistical Analysis
Statistical analysis was performed using SPSS 22.0 program. Significance level was considered as p<0.05. Mann Whitney U-test was used for pairwise comparisons of nonparametric independent groups and Chi-square test was used for comparisons of categorical variables. Fisher’s exact test was used for analysis of probability tables for small sample sizes. Risk factors for amblyopia were analyzed with a logistic regression model.
Results
Of 1126 students screened, 125 (11.1%) were referred based on PlusoptiX thresholds. Of these, 106 (84.8%) attended our clinic. Seven children were excluded: one with down syndrome, one with cerebral palsy, one with autism, one with twin-to-twin transfusion syndrome whose vision could not be assessed, one with marfan syndrome and pseudophakic eyes, and two outside the eligible age range. One child with optic nerve myelination was retained, as reduced acuity was attributed to high refractive error rather than the structural anomaly. Among 99 children meeting inclusion criteria, 20 had unilateral amblyopia and 10 had bilateral amblyopia. Assuming all non-referred children were non-amblyopic, estimated prevalence was 2.6% (30/1126). Risk factor analyses were conducted among the 99 examined children.
Of the children included in the study, 54% (n=53) were boys and 46% (n=46) were girls. The mean age was 5 years 6 months (65.5 ± 10.3 months; range: 3 years 1 month to 6 years 11 months). Age distribution was: 36–48 months (n=6), 48–60 months (n=20), 60–72 months (n=43), and 72–84 months (n=30). All refractive measurements were obtained under cycloplegia using 1% cyclopentolate.
The incidence of anisometropia (≥1 D) was 2.5% (28/1126) in our cohort. Descriptive statistics for age and cycloplegic refractive parameters in the children studied are shown in Table 2. Twenty-five children with amblyopia had hyperopia, and the mean spherical equivalent of these patients was 3.44 ± 2.1 D. The mean spherical equivalent of 51 patients with hyperopia and no amblyopia was 1.86 ± 1.09 D. The relationship between hyperopia and unilateral amblyopia was found to be significant (p = 0.026). Receiver operating characteristic (ROC) curve analysis using univariate predictors yielded an area under the curve of 80% and 57%, respectively (AUC 0.725 p=0.02). The optimal threshold sensitivity for unilateral amblyopia modeled by our data was 1.81 D hyperopia (Figure 2).
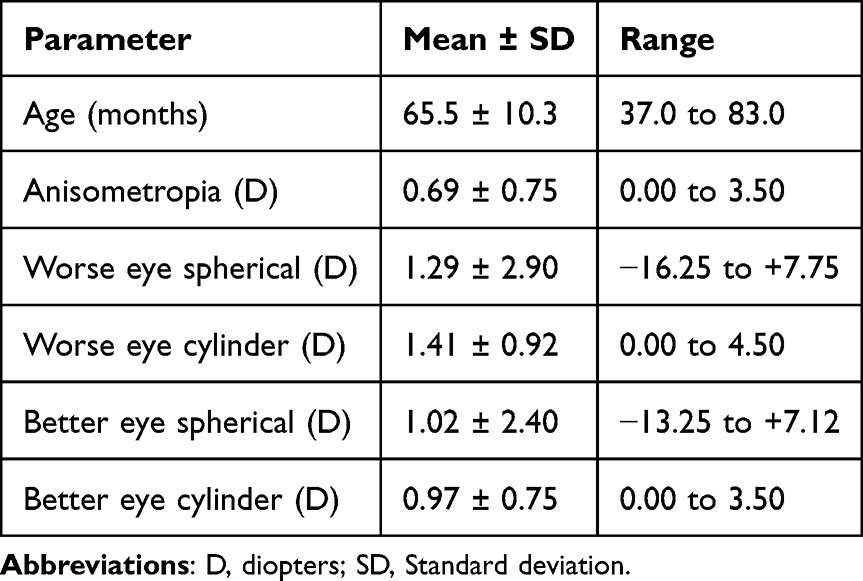 |
Table 2 Descriptive Statistics for Age and Cycloplegic Refractive Parameters Among Examined Children |
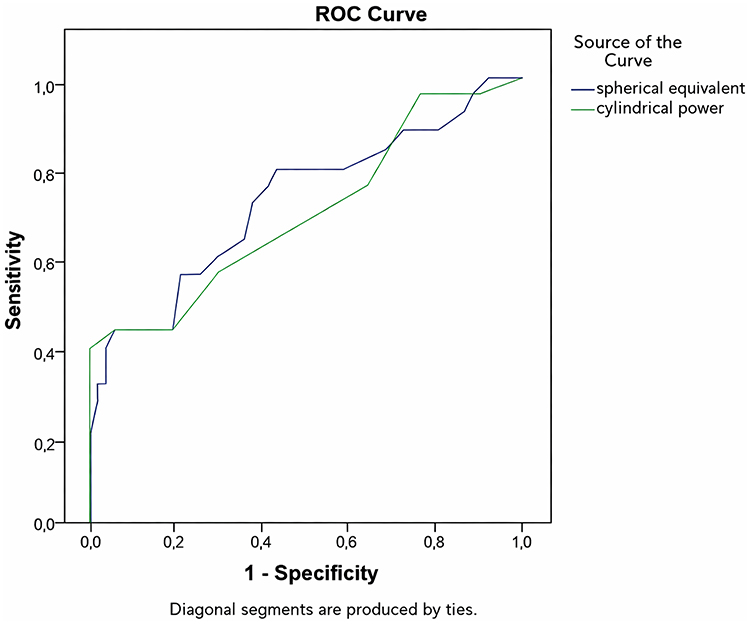 |
Figure 2 ROC curve for the sensitivity and specificity values of spherical and cylindrical (cut-off) measurements in distinguishing individuals with and without unilateral amblyopia. |
Five of the patients with amblyopia had myopia. The mean spherical equivalent of these patients was −5.10 diopters. The mean spherical equivalent of the 18 patients with myopia and no amblyopia was −1.54 diopters. The relationship between myopia and unilateral amblyopia was not found to be statistically significant (p>0.05).
The mean cylindrical value of 30 cases with unilateral amblyopia was measured as 2.63 ± 1.13 D. The mean cylindrical power of 69 cases without amblyopia was measured as 1.28 ± 0.79 D. The relationship between astigmatism and unilateral amblyopia was found to be statistically significant (p=0.02). Receiver operating characteristic (ROC) curve analysis using univariate predictors yielded an area under the curve of 76% and 35%, respectively (AUC 0.696, p=0.006). The optimal threshold sensitivity modeled by our data was 0.88 D of astigmatism (Figure 2). In terms of astigmatism axes, among amblyopic children, 2 had an oblique axis, while 27 had an orthogonal axis. Among non-amblyopic children, 8 had an oblique axis, and 52 had an orthogonal axis. We found no evidence of association between astigmatism axis (oblique vs orthogonal) and amblyopia.
The mean anisometropia value of 30 cases with unilateral amblyopia was 1.30 ±1.01 D. The mean anisometropia value of 69 cases without amblyopia was calculated as 0.42 ± 0.38 D. The relationship between anisometropia and unilateral amblyopia was found to be statistically significant (p=0.00). The condition that has the greatest effect on amblyopia was found to be anisometropia. With anisometropia, the probability of unilateral amblyopia increases by 8.9 times. With hyperopia, the probability of unilateral amblyopia increases by 6.2 times compared to the probability of not having amblyopia. With astigmatism, the probability of unilateral amblyopia increases by 2.4 times compared to the probability of not having amblyopia (Table 3).
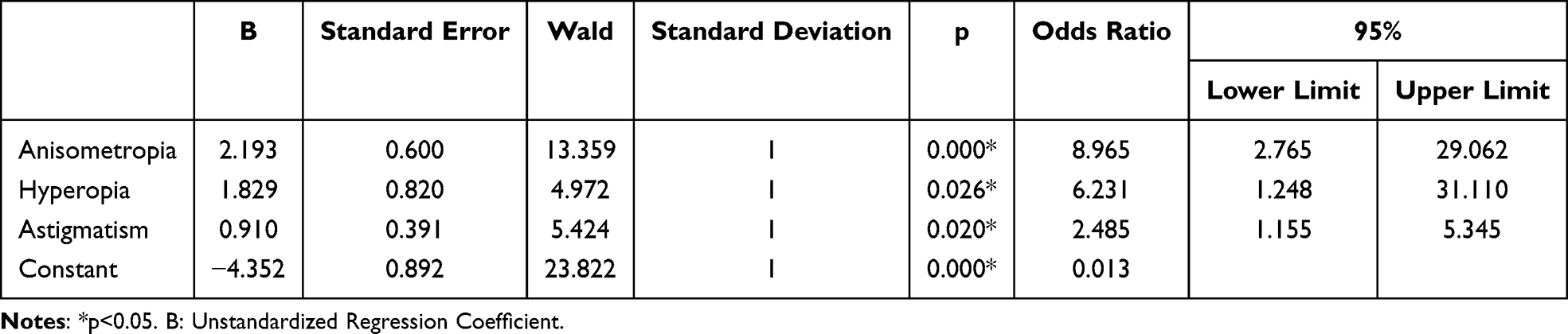 |
Table 3 Risk Relationship Between Unilateral Amblyopia and Anisometropia, Hyperopia and Astigmatism |
Hyperopia was present in 7 children with bilateral amblyopia. The mean spherical equivalent of these cases was 3.55 D. The relationship between hyperopia and bilateral amblyopia was not found to be statistically significant (p=0.084) (Table 4). The mean cylindrical value of 10 cases with bilateral amblyopia was 2.00 D. The mean cylindrical power of 89 cases without bilateral amblyopia was measured as 0.86 D. The relationship between astigmatism and bilateral amblyopia was found to be statistically significant (p=0.001).
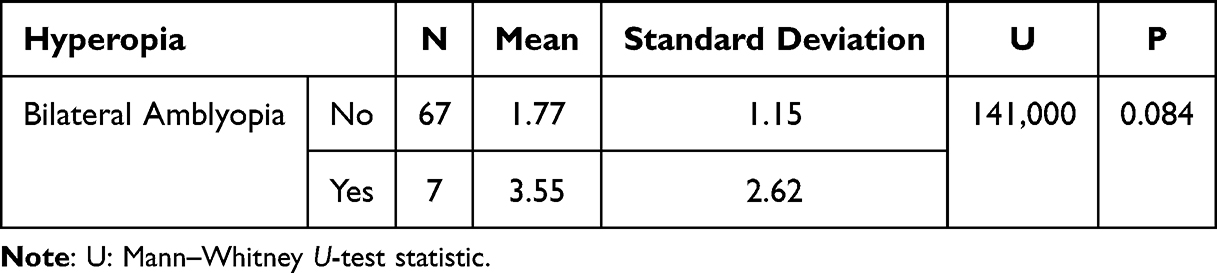 |
Table 4 The Relationship Between Bilateral Amblyopia and Hyperopia |
Strabismus was present in a total of 7 children. Strabismus was detected in only 2 of the cases with unilateral or bilateral amblyopia (2 esotropia). No amblyopia was observed in the other 5 strabismus cases (3 esotropia, 1 exotropia, 1 superior oblique palsy). There was no child with a history of strabismus surgery.
In the multiple regression analysis, <2 D hyperopia, 2–4 D hyperopia and <1 D astigmatism, 1–2 D and ≥2 D astigmatism were found to be risk factors for unilateral amblyopia (p<0.05). The number of patients with hyperopia over 4 diopters was not sufficient for statistical calculation. It was seen that myopia values were not associated with amblyopia. When the increasing value of anisometropia in any range was evaluated separately, the relationship between anisometropia and the formation of amblyopia was not found to be statistically significant. It was found that the rate of amblyopia increased in increasing anisometropia value ranges (11.4% in the range of 0.5 D and below, 25.9% in the range of 0.5–1 D, 54.5% in the range of 1–2 D, and 100% for 2 D and above) (Table 5).
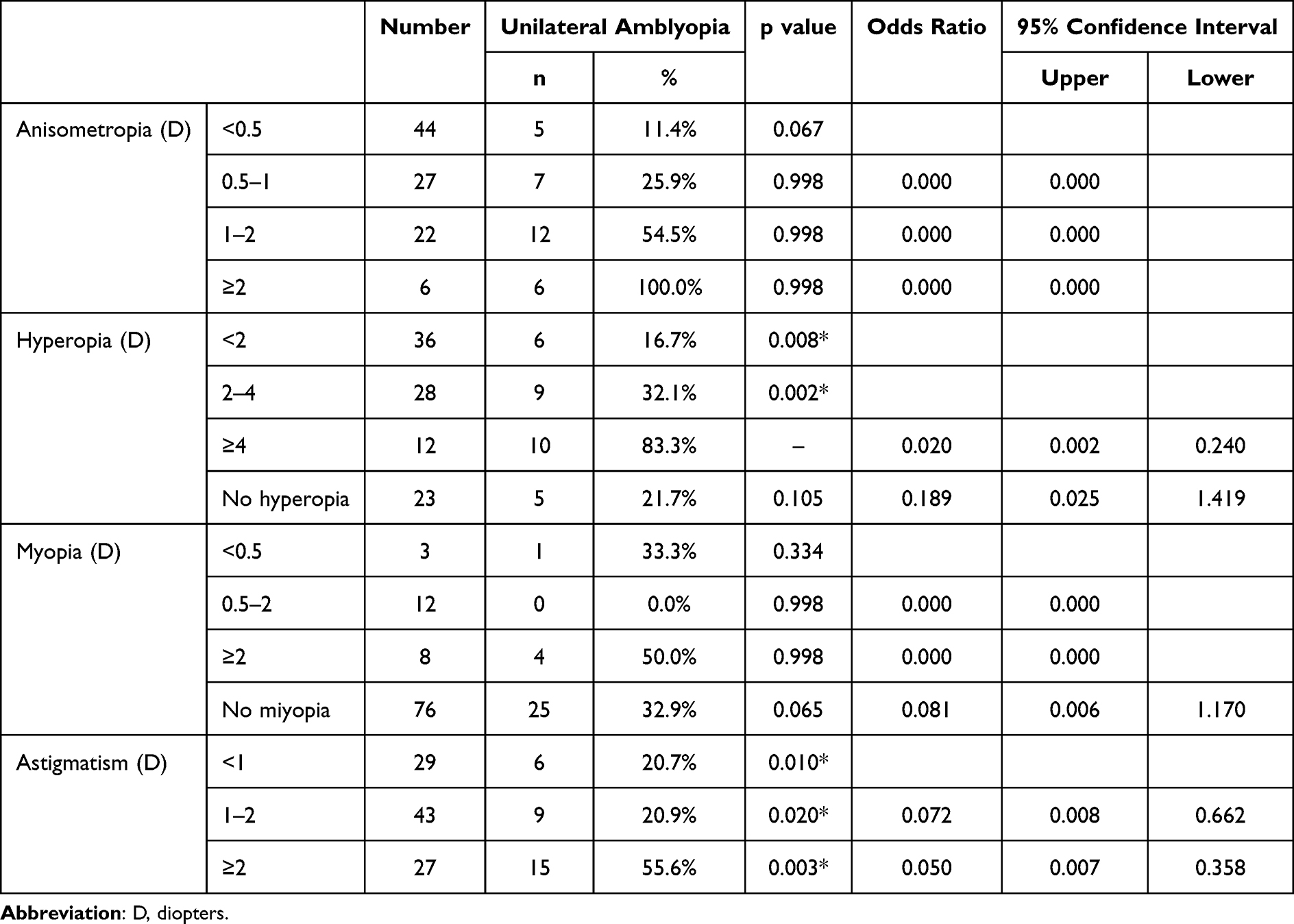 |
Table 5 Logistic Regression Analysis for Unilateral Amblyopia Risk Factors |
Discussion
Considering that visual impairment due to refractive errors can lead to decreased school success and social problems in children, it is important to perform screenings for the preschool age group with valid and reliable methods to diagnose and treat refractive errors early. Determining the risk factors for these screenings and determining the threshold values of these risk factors are important for community screening.
The use of multivariate analysis in our study allowed us to independently assess the contribution of these risk factors to amblyopia, despite the frequent coexistence of different refractive errors. All children with unilateral amblyopia (100%) had significant refractive errors (2.0 D ≥ hyperopia, 1.0 D ≥ astigmatism, 0.5 D ≥ anisometropia). The refractive errors reported in 87% of amblyopic children in the Vision In Preschoolers (VIP) study and in 85% of amblyopic children in the Multi-Ethnic Pediatric Eye Disease Study (MEPEDS) study were within these ranges.17,18 Dirani et al reported that 85% of amblyopic Chinese children in Singapore had refractive errors within these ranges.19
The relationship between hyperopia and unilateral amblyopia was found to be statistically significant, while no significant relationship was found with bilateral amblyopia. We found that the risk of developing unilateral amblyopia was 6.2 times higher in children with hyperopia. In the regression analysis, we found statistically significant results for <2 D and 2–4 D hyperopia values. In the VIP study, it was reported that the risk of unilateral amblyopia in hyperopia increased by 1.8 times for the 2–3 D range and 4.3 times for 4 D and above. In the same study, it was reported that the risk of bilateral amblyopia increased by 2.8 times for the 3–4 D range and 5 times for 5 D and above. Since the number of children with hyperopia over 4 D was small in our study, statistical calculations could not be made for bilateral amblyopia. In the Sidney Pediatric Eye Disease Study (SPEDS), hyperopia of over 3 D was detected in 55% of amblyopic children and hyperopia of over 6 D was detected in 18%.20
In our study, a statistically significant relationship was observed between astigmatism and both unilateral and bilateral amblyopia, and the risk of developing unilateral amblyopia was found to be 2.4 times higher in children with astigmatism. The SPEDS study reported that astigmatism of 1 D and above increased the risk of amblyopia by 5.7 times. The VIP study reported that astigmatism increased the risk of developing unilateral amblyopia by 2.2 times for the 1–2 D range, 2.8 times for the 2–3 D range, and 1.9 times for 3 D and above. The MEPEDS and Baltimore Pediatric Eye Disease Study (BPEDS) evaluated 6504 children aged 30–72 months, and reported that astigmatism increased amblyopia by 2.3 times for the 1–2 D range, and 17.6 times for 2 D and above.21
The relationship between anisometropia and unilateral amblyopia was found to be statistically significant, and anisometropia was shown to increase unilateral amblyopia by 8.9 times. When anisometropia ranges were evaluated separately, no statistically significant results were obtained in the logistic regression analysis. However, it was found that the rate of amblyopia increased in increasing value ranges (11.4% for 0.5 D and below, 25.9% for 0.5–1 D, 54.5% for 1–2 D, 100% for 2 D and above). In the VIP study, anisometropia was reported to be a major risk factor, and it was reported that the risk of unilateral amblyopia increased by 1.7 times for 0.5–1 D range, 4.3 times for 1–2 D range, and 9.2 times for 2 D and above. Weakley reported in 361 patients that amblyopia was 13 times more common in children with anisometropia ranging from 1.00 D to 2.00 D than in children with anisometropia ranging from 0.00 D to 1.00 D.22 However, he showed that cylindrical hyperopia or cylindrical myopic anisometropia greater than 1.5 D, myopic anisometropia greater than 2 D, and hyperopic anisometropia greater than 1 D were significantly associated with amblyopia. Many studies have reported that amblyopia associated with anisometropia due to hyperopia is more common and severe than that seen in anisometropia due to myopia.23–27 In contrast to the older child population targeted by our study, Steltman et al found anisometropia greater than 15 D in only 5 of 601 children with a mean age of 14.5 months in the Early Glasses Study.28
Strabismus is not as common as ametropia, but it is one of the important risk factors for amblyopia. In our study, no relationship was found between amblyopia and strabismus, but the number of patients with strabismus (n=7) was not sufficient for statistics. PlusoptiX has reduced sensitivity for small-angle and intermittent deviations. However, these carry lower amblyopia risk than constant large-angle strabismus, minimizing the impact on prevalence estimates while limiting conclusions about strabismus-amblyopia associations.
In the VIP study, esotropia (n=91) and exotropia (n=49) were evaluated separately and it was reported that the risk of unilateral amblyopia increased 7.8 times for esotropia and 3.1 times for exotropia. In the SPEDS study, the risk of amblyopia increased 9.3 times for esotropia and 7.6 times for exotropia, and strabismus was reported in 37% (n=10) of amblyopic children. In the MEPEDS and BPEDS studies, it was reported that esotropia was associated with amblyopia, but exotropia was not statistically significant. This study showed that esotropia caused a 9-fold and exotropia a 1.2-fold increase in risk.
No increased risk was found for unilateral or bilateral amblyopia in myopic children. The SPEDS study evaluated 1422 children aged 30–72 months, and although not statistically significant, it was reported that the risk of amblyopia in children with 0.5 D or more myopia increased by 2.2 times. The VIP study included 3869 children aged 3–5 years, and compared to children without myopia (<0.5 D), it was found that myopia between 0.5 and 2 D increased the risk of unilateral amblyopia by 1.7 times, and myopia of 2 D or more increased the risk of unilateral amblyopia by 4.1 times.
The prevalence of amblyopia was found to be 2.6% in our study. In population-based studies from various regions in our country, the prevalence of amblyopia was found to be 1.1% in a study conducted by Turaçlı et al with 23,810 school students.7 Çaça et al reported the prevalence of amblyopia as 2.6% in a study conducted on 20,062 children aged 6–14.8 In another study conducted by Ergin with 2386 participants, the prevalence was found to be 1.21%.11 Other large-scale studies reported SPEDS as 1.9%, BPEDS as 1.8% and MEPEDS as 2.1%. In a study conducted in Sweden, which is notable for its low rate, Kvarnstrom et al reported the prevalence of amblyopia in 10-year-old children as 0.3%.29
Demographic characteristics such as age and gender were not found to be associated with amblyopia. Amblyopia rates may differ in studies comparing urban and rural populations, but the children in our study were predominantly from urban schools and preschool education areas. The MEPEDS and BPEDS studies reported that lack of health insurance reduced children’s access to early interventions with glasses, resulting in bilaterally reduced visual acuity. They also reported a 2-fold increased risk of unilateral amblyopia in Hispanics. The VIP study found significant results in terms of demographic characteristics, but reported a 1.4-fold increased risk of unilateral amblyopia in Hispanics.
There are some limitations to our study. In our study, children who were deemed risky and could not be measured were referred to our clinic. There may be children who passed the screening but had refractive error amblyopia below the threshold values. Considering the high specificity values shown in screening studies of the Plusoptix device, we think that this will not change our statistical results. The children who participated in the screening were children who received preschool education or primary school 1st grade students. Considering that the entire population cannot access preschool education due to the socioeconomic differences in our region and that the amblyopia rate may be different in the urban and rural population, our cohort may not represent the entire population. Another shortcoming of our study is that our amblyopia prevalence may have been affected by the fact that children with glasses were not referred to our clinic during the school screening. In addition, children with small-angle tropia who were not detected by the photo scanner may not have been referred to us.
Supporting the results of other previously reported population-based studies, the results obtained in our study are lower than the generally accepted threshold values for amblyopia. In addition, our results emphasize the importance of correcting refractive errors in the treatment of children with amblyopia. Early treatment of refractive errors can prevent amblyopia. The effectiveness of screening methods performed with pediatric autorefractometers increases as the screening age decreases.
In our study, risk factors for unilateral and bilateral amblyopia were evaluated in preschool children and first grade primary school students. Our data may help shape threshold values and screening policies for refractive errors. More population-based studies are needed in different regions to create guidelines consisting of ideal threshold values that can be used in amblyopia screening programs.
Conclusion
In this school-based screening of 1126 Turkish preschoolers, amblyopia prevalence was 2.6%, with refractive errors present in all affected children. Anisometropia, hyperopia, and astigmatism were independently associated with amblyopia risk, with a ROC analysis suggesting potentially lower screening thresholds than conventional guidelines. However, as referral criteria were based solely on refractive parameters, these findings apply primarily to refractive amblyopia; strabismic amblyopia was likely underascertained. Prospective population-based studies examining the full refractive error spectrum are needed before these thresholds can inform screening policy. Early detection of significant refractive errors remains essential for amblyopia prevention in preschool populations.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
Approval for the study was obtained from Zonguldak Bulent Ecevit Ethics Committee (Ref No 2018-250-19/12). The study approved to the tenets of Declaration of Helsinki. Written informed consent was required from at least one parent of each child and verbal assent of all children were obtained before examination.
Acknowledgments
This study was presented in the 54th TOA National Congress, 9–13 December 2020, Antalya/TURKIYE.
Author Contributions
Material preparation and data collection were performed by NK, data analysis was performed by SCU. The first draft of the manuscript was written by NK. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Disclosure
The authors have no conflicts of interest to declare for this work.
References
1. Simons K. Preschool vision screening: rationale, methodology and outcome. Surv Ophthalmol. 1996;41:3–10.
2. Glaser SR, Matazinski AM, Sclar DM, et al. A randomized trial of atropine vs patching for treatment of moderate amblyopia in children. Arch Ophthalmol. 2002;120:268–278.
3. He M, Huang W, Zheng Y, Huang L, Ellwein LB. Refractive error and visual impairment in school children in rural southern China. Ophthalmology. 2007;114(2):374–382. doi:10.1016/j.ophtha.2006.08.020
4. Goh PP, Abquariyah Y, Pokharel GP, Ellwein LB. Refractive error and visual impairment in school-age children in Gombak District, Malaysia. Ophthalmology. 2005;112(4):678–685. doi:10.1016/j.ophtha.2004.10.048
5. Lai YH, Hsu HT, Wang HZ, Chang SJ, Wu WC. The visual status of children ages 3 to 6 years in the vision screening program in Taiwan. J AAPOS. 2009;13(1):58–62. doi:10.1016/j.jaapos.2008.07.006
6. Sapkota YD, Adhikari BN, Pokharel GP, Poudyal BK, Ellwein LB. The prevalence of visual impairment in school children of upper-middle socioeconomic status in Kathmandu. Ophthalmic Epidemiol. 2008;15(1):17–23. doi:10.1080/09286580701772011
7. Turacli ME, Aktan SG, Dürük K. Ophthalmic screening of school children in Ankara. Eur J Ophthalmol. 1995;5(3):181–186. doi:10.1177/112067219500500307
8. Caca I, Cingu AK, Sahin A, et al. Amblyopia and refractive errors among school-aged children with low socioeconomic status in southeastern Turkey. J Pediatr Ophthalmol Strabismus. 2013;50(1):37–43. doi:10.3928/01913913-20120804-02
9. Azizoğlu S, Crewther SG, Şerefhan F, Barutchu A, Göker S, Junghans BM. Evidence for the need for vision screening of school children in Turkey. BMC Ophthalmol. 2017;17(1):230. doi:10.1186/s12886-017-0618-9
10. Gursoy H, Basmak H, Yaz Y, Colak E. Vision screening in children entering school: Eskisehir, Turkey. Ophthal Epidemiol. 2013;20(4):232–238. doi:10.3109/09286586.2013.808672
11. Ergin A. Eye screening results at the primary schools In Kirikkale. Turkiye Klin J Med Sci. 2001;21(3):166–172.
12. Carlton J, Kaltenthaler E. Amblyopia and quality of life: a systematic review. Eye. 2011;25(4):403–413. doi:10.1038/eye.2011.4
13. PlusoptiX GmbH. User manuals. Available from: https://www.plusoptixinc.com/support/support-area/vision-screener/s12r/user-manuals.
14. Singman E, Matta N, Tian J, et al. A comparison of referral criteria used by the plusoptiX photoscreener. Strabismus. 2013;21(3):190–194. doi:10.3109/09273972.2013.811606
15. Lequeux L, Thouvenin D, Couret C, et al. Vision screening for children: Recommended practices from AFSOP. J Fr Ophtalmol. 2021;44(2):244–251. doi:10.1016/j.jfo.2020.07.005
16. Wallace DK, Morse CL, Melia M, et al. Pediatric eye evaluations preferred practice pattern®: i. Vision screening in the primary care and community setting; II. Comprehensive ophthalmic examination. Ophthalmology. 2018;125(1):184–P227. doi:10.1016/j.ophtha.2017.09.032
17. Pascual M, Huang J, Maguire MG, Kulp MT, Quinn GE, Ciner E; Vision in Preschoolers (VIP) Study Group. Risk factors for amblyopia in the vision in preschoolers study. Ophthalmology. 2014;121(3):622–629. doi:10.1016/j.ophtha.2013.08.040
18. Multi-ethnic Pediatric Eye Disease Study Group. Prevalence of amblyopia and strabismus in African American and Hispanic children ages 6 to 72 months: the Multi-ethnic Pediatric Eye Disease Study. Ophthalmology. 2008;115(7):1229–1236. doi:10.1016/j.ophtha.2007.08.001
19. Dirani M, Zhou B, Hornbeak D, et al. Prevalence and causes of decreased visual acuity in Singaporean Chinese preschoolers. Br J Ophthalmol. 2010;94(12):1561–1565. doi:10.1136/bjo.2009.173104
20. Pai ASI, Rose KA, Leone JF, et al. Amblyopia prevalence and risk factors in Australian preschool children. Ophthalmology. 2012;119(1):138–144. doi:10.1016/j.ophtha.2011.06.024
21. Tarczy-Hornoch K, Varma R, Cotter SA, et al. Risk factors for decreased visual acuity in preschool children: the multi-ethnic pediatric eye disease and Baltimore pediatric eye disease studies. Ophthalmology. 2011;118(11):2262–2273. doi:10.1016/j.ophtha.2011.06.033
22. Weakley DR Jr. The association between nonstrabismic anisometropia, amblyopia, and subnormal binocularity. Ophthalmology. 2001;108(1):163–171. doi:10.1016/S0161-6420(00)00425-5
23. Phillips CI. Strabismus, anisometropia, and amblyopia. Br J Ophthalmol. 1959;43(8):449. doi:10.1136/bjo.43.8.449
24. Copps LA. Vision in anisometropia. Am J Ophthalmol. 1944;27(6):641–644. doi:10.1016/S0002-9394(44)91523-0
25. Jampolsky A, Flom BC, Weymouth FW, Moses LE. Unequal corrected visual acuity as related to anisometropia. Arch Ophthalmol. 1955;54(6):893–905. doi:10.1001/archopht.1955.00930020899013
26. Kutschke PJ, Scott WE, Keech RV. Anisometropic amblyopia. Ophthalmology. 1991;98(2):258–263. doi:10.1016/S0161-6420(91)32307-8
27. Sen DK. Anisometropic amblyopia. J Pediatr Ophthalmol Strabismus. 1980;17(3):180–184. doi:10.3928/0191-3913-19800501-13
28. Steltman JS, Nordmann M, Sanders S, et al. Baseline characteristics of children in the Early Glasses Study. Graefe’s Arch Clin Exp Ophthalmol. 2025;263(2):555–563.
29. Kvarnstrom G, Jakobsson P, Lennerstrand G. Visual screening of Swedish children: an ophthalmological evaluation. Acta Ophthalmol Scand. 2001;79(3):240–244. doi:10.1034/j.1600-0420.2001.790306.x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparative Validation of PlusoptiX and AI-Optic Photoscreeners in Children with High Amblyopia Risk Factor Prevalence

Arnold RW
Clinical Ophthalmology 2022, 16:2639-2650
Published Date: 16 August 2022
The UCI EyeMobile Preschool Vision Screening Program: Refractive Error and Amblyopia Results from the 2019–2020 School Year
Hunter SC, He J, Han M, Suh DW
Clinical Ophthalmology 2022, 16:4249-4255
Published Date: 20 December 2022
Standard Amblyopia Therapy in Adults with Longstanding Amblyopia Improves Visual Acuity and Contrast Sensitivity
Ridder WH III, Patel R, Li YX, Staubli U
Clinical Ophthalmology 2023, 17:1847-1858
Published Date: 29 June 2023
Estimating the Prevalence and Severity of Isolated Small-Angle Strabismic Amblyopia

Arnold RW
Clinical Ophthalmology 2025, 19:3409-3418
Published Date: 16 September 2025