Back to Journals » Clinical Ophthalmology » Volume 17
Standard Amblyopia Therapy in Adults with Longstanding Amblyopia Improves Visual Acuity and Contrast Sensitivity
Authors Ridder WH III ![]() , Patel R, Li YX, Staubli U
, Patel R, Li YX, Staubli U
Received 16 March 2023
Accepted for publication 15 June 2023
Published 29 June 2023 Volume 2023:17 Pages 1847—1858
DOI https://doi.org/10.2147/OPTH.S410800
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
William H Ridder III,1 Reena Patel,1 Yong-Xin Li,2 Ursula Staubli2
1Southern California College of Optometry, Marshall B. Ketchum University, Fullerton, CA, USA; 2AbbVie, Inc, Irvine, CA, USA
Correspondence: William H Ridder III, Southern California College of Optometry, Marshall B. Ketchum University, 2575 Yorba Linda Blvd, Fullerton, CA, 92831, USA, Email [email protected]
Purpose: Perceptual learning or dichoptic training may result in improved acuity in adult amblyopes. However, for amblyopic children (< 18 years), most clinicians recommend standard part-time patching. The purpose of this study was to determine if standard amblyopia therapy results in an enhancement in vision in the amblyopic eye of adults.
Patients and Methods: Fifteen amblyopes (20/30 or worse) were recruited and nine (age (SD) 32.9 (16.31)) with anisometropia or anisometropia and strabismus (ie, combined mechanism amblyopia) completed the study. Previous therapy did not exclude subjects. The subjects received a comprehensive eye exam and wore their best correction for at least four weeks prior to baseline testing. The non-amblyopic eye was patched for 2 hours per day (Amblyopia iNET training for 30 minutes and near/distance activities for 1.5 hours). The subjects had a baseline amblyopia evaluation followed by one visit per week for 12 weeks. At 12 weeks, the treatment was tapered off over one month and the subjects had a final amblyopia evaluation at 24 weeks. Contrast sensitivity was measured at baseline and 12 weeks with the Quick CSF system.
Results: The subjects had a significant improvement in visual acuity across the weeks (p < 0.001). At baseline, weeks 12 and 24, the average logMAR acuities (SE) were 0.55 (0.09), 0.41 (0.08), and 0.38 (0.09), respectively. Weeks 4 to 24 were significantly different (p < 0.001) from baseline. The average acuity improvement over the 24 weeks was 1.7 logMAR lines. There was a significant increase in the area under the log contrast sensitivity function (p = 0.002) and its estimated acuity (p = 0.036) from baseline to 12 weeks.
Conclusion: Standard amblyopia treatment can result in an improvement in visual acuity and contrast sensitivity in adults with longstanding anisometropic or combined mechanism amblyopia even if they had prior therapy.
Keywords: amblyopia, anisometropia, strabismus, contrast sensitivity, visual acuity
Introduction
Functional amblyopia is an optically uncorrectable decrease in visual acuity with no apparent pathological or morphological cause.1,2 Anisometropia and strabismus are the two most prevalent etiological factors for amblyopia.1 Anisometropic amblyopia is a decrease in visual acuity that is the result of a difference in refractive error between the two eyes that results in chronic blur on one retina.3 Strabismic amblyopia is a decrease in visual acuity that is due to an eye misalignment early in life.1
A meta-analysis of 60 studies indicates that the world-wide prevalence rate for amblyopia is 1.44% (95% CI 1.17% to 1.78%).4 The rates are higher in Europe (2.90%) and North America (2.41%) compared with Asia (1.09%) and Africa (0.72%).4 There were approximately 99.2 million amblyopes world-wide in 2019, and it is estimated that there will be approximately 221.9 million by 2040.4 Thus, amblyopia is a significant world-wide health problem.
The most common treatment for amblyopia is part-time patching of the non-amblyopic eye.5–9 A Pediatric Eye Disease Investigator Group (PEDIG) study demonstrated that 180 children ages 3–7 obtained an average improvement in acuity of 1.1 lines after 5 weeks of patching with near visual activities.10 Other studies have suggested that older children (age 7–13) have less of an increase in acuity with patching than younger children (age 3–7).11,12
Historically, there have not been many publications on adult (≥18 years old) amblyopia therapy employing patching. This is because clinicians initially believed that amblyopia could not be treated after the end of the critical period, which was previously thought to be around 7–8 years of age. The prevailing theory was that the synaptic contacts between cells could only be modified during the critical period.13 However, recent studies have suggested that amblyopia can be treated in adults, even though the critical period has ended.14–19 Video games that employed dichoptic and threshold-training tasks were employed in these studies. However, other large multi-center studies have suggested that binocular perceptual learning techniques are not any more effective than traditional patching or non-binocular therapies in both children and adults with amblyopia.20–22
A recent article suggests that standard patching for 2 hours per day combined with near visual activities results in an improvement in acuity (average acuity improved from 0.37 ± 0.04 to 0.14 ± 0.03 logMAR) for previously untreated adults (age 17–35) with anisometropic amblyopia.23 However, another study suggests that previously untreated adults with amblyopia may only obtain a small improvement in acuity with patching (0.05 logMAR).24 The purpose of this study was to determine if standard amblyopia therapy (ie, part-time patching with near/distance visual activities) results in an enhancement in visual performance in adult subjects with anisometropic or combined mechanism amblyopia.
Materials and Methods
Subjects
Fifteen adult amblyopic subjects were assessed and met the enrollment criteria for the study. Of the initial 15, 2 withdrew before the baseline visit, 3 withdrew before visit 1, and 1 withdrew before visit 2. The remaining nine (average age (SD) 32.9 (16.31), range 18–60 years) completed the therapy (Table 1). The six subjects (age (SD) 30.3 (7.34), range 21–38) that discontinued had similar demographics to the nine that completed the study. Of the six subjects, two had anisometropic amblyopia and four had combined mechanism amblyopia. Five subjects had previous therapy and three were male. The partial data sets (a maximum of 1 visit) of the discontinued subjects were not included in further analysis. A sample size estimate was made using data from Hou et al (2011).25 They measured contrast sensitivity in nine subjects with amblyopia before and after therapy. For their 12 cycles per degree (cpd) data (from Figure 3 in Hou et al (2011)25), they show average pre- and post-therapy contrast sensitivities (SD) of 2 (0.5) and 6 (1.0). Assuming an alpha of 0.05, power of 0.80, and a pooled standard deviation of 3, the estimated sample size is nine, which is the number of subjects enrolled in the present study.
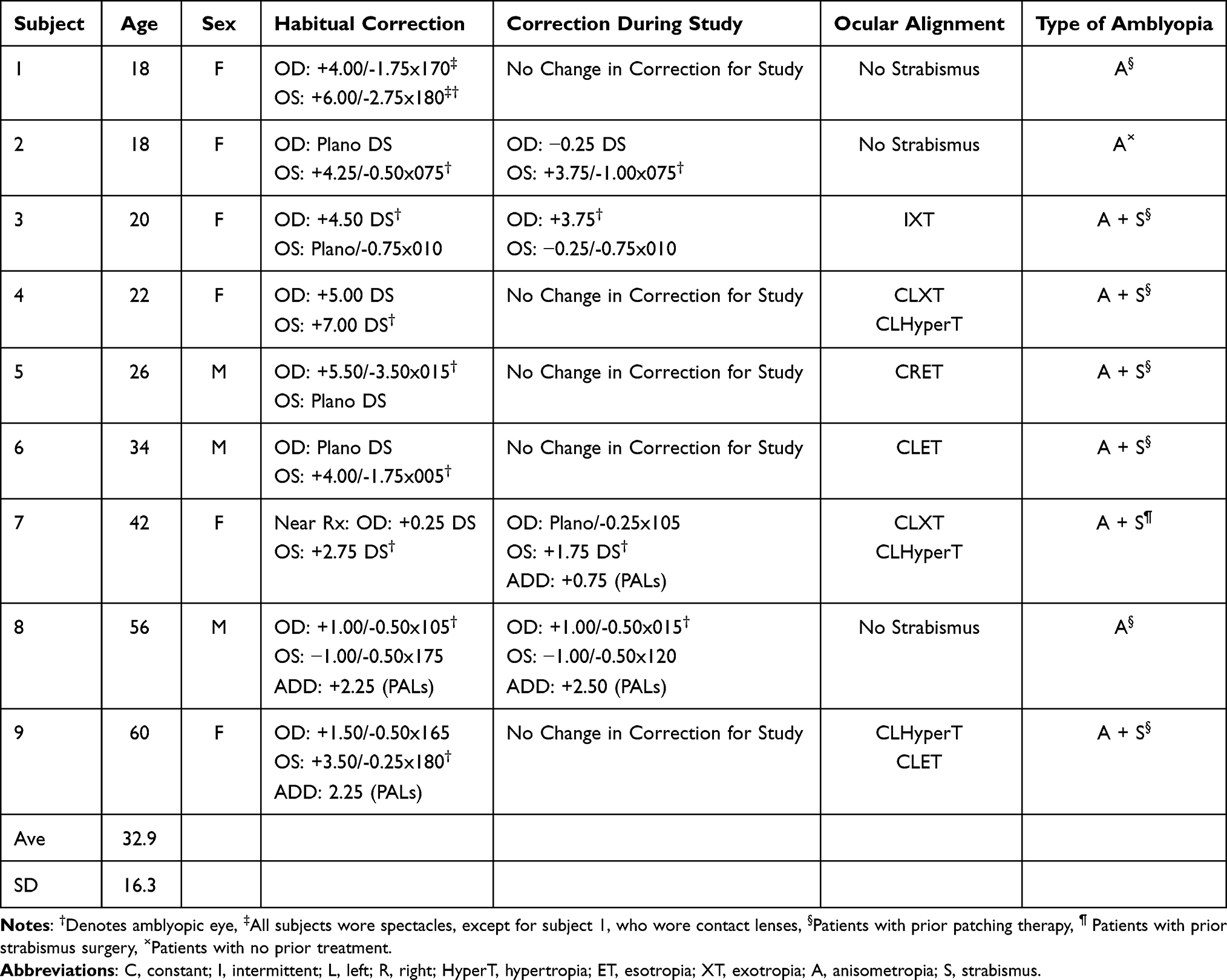 |
Table 1 Subject Demographics |
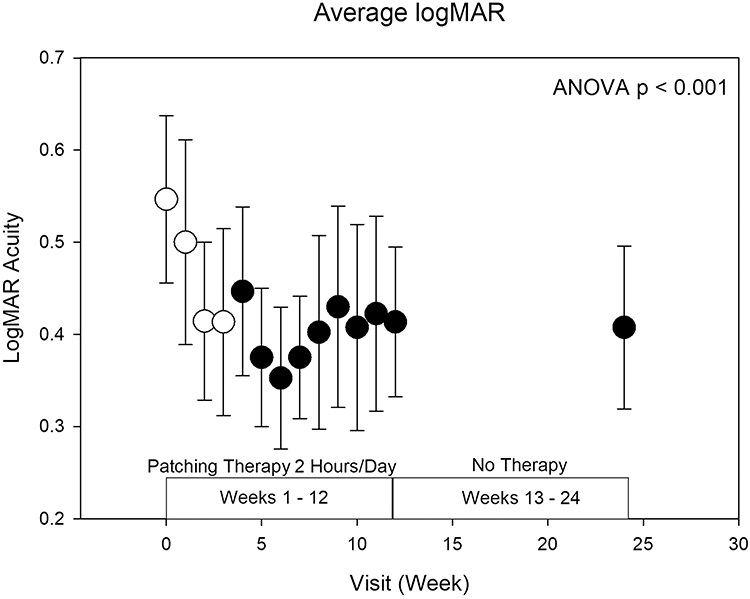 |
Figure 1 Average logMAR acuity (± SE) for all amblyopes for each office visit. An ANOVA (p < 0.001) indicated there was a change in acuity across visits. Post-hoc Dunnett multiple comparisons indicated that weeks 4 through 24 (indicated by the filled circles) are significantly different from baseline (week 0). Acuities at weeks 12 and 24 were not significantly different (paired t-test, t8 = 1.34, p = 0.22). |
Subjects were recruited from the University Eye Center at Ketchum Health as well as referred by local optometrists. Informed consent was obtained from all subjects after the study procedures were explained to them and all procedures adhered to the tenets of the Declaration of Helsinki. The procedures were approved by Sterling IRB (ID number: 4813). All subjects had amblyopia (BCVA 20/30 or worse in the amblyopic eye) due to anisometropia (N = 3) or anisometropia and strabismus (N = 6, Table 1). Seven of the subjects had prior patching, one had prior strabismus surgery (subject number 7), and one had no prior treatment (subject number 2). All subjects received a comprehensive eye examination with dilation and an amblyopia work-up to determine eligibility for this study. The subjects’ average baseline acuity (SE) was 0.55 (0.09) logMAR (Table 2). The amblyopia work-up performed at the baseline and week 24 visits consisted of the following tests and the procedures are summarized in Caloroso and Rouse:26
- Distance visual acuity with E-ETDRS protocol
- Near visual acuity with ATS 4 HOTV card
- Distance and near cover test
- Distance stereopsis with distance randot stereo test
- Near stereopsis with randot preschool stereo test
- Sensory fusion with worth 4 dot
- Accommodative amplitude with push-up method (for pre-presbyopic subjects)
- Dynamic retinoscopy with monocular estimate method
- Dry retinoscopy
- Manifest refraction
- Cycloplegic retinoscopy (for pre-presbyopic subjects)
 |
Table 2 Amblyopic Eye Subject Data for the AULCSF and CSF VA in Cycles per Degree (Cpd) for Baseline and the Week 12 Visit. The logMAR VA is Shown for the Baseline and Weeks 12 and 24 Visits. The Baseline and Week 12 or 24 Data are Statistically Significantly Different (paired t-tests, p < 0.05). |
All subjects wore a habitual prescription (Table 1). If greater than a 0.50 D change in refractive error was found at the eligibility visit, the subject’s spectacle or contact lens prescription was updated and they wore the new correction for at least four weeks prior to baseline testing to ensure adaptation.24,27–29 Five of the subjects had no prescription change (subjects 1, 4, 5, 6, and 9) and the remaining subjects had small changes (generally about a 0.5 diopter sphere change or cylinder and/or axis changes). Thus, it is unlikely that refractive adaptation influenced the results. At home, therapy consisted of part-time patching of the non-amblyopic eye for 2 hours/day. While patching, the subjects performed near training exercises on the Amblyopia iNET program (http://www.visiontherapysolutions.net/ambp.php#1, HTS, Inc., Gold Canyon, AZ) for 30 minutes/day and were instructed to do near work tasks (ie, reading, writing, or computer use) for the remaining 1.5 hours. They were also told that it would be acceptable to do distance activities (ie, watching television or cooking) while patching. The amblyopia iNet program is a computer program that is designed to start training at the patient’s visual acuity level, with the targets altering their size depending on the patient’s performance. For example, if the patient is doing very well with the program, the target size will become progressively smaller to continue to challenge the patient at a reasonable demand. The patient’s performance and compliance can be assessed online through the computer program. All subjects were educated to discontinue treatment and let us know immediately if they started to experience diplopia; however, this did not occur with any of the subjects in the study.
The subjects attended weekly visits for 12 weeks. At the weekly visit, visual acuity was measured for the amblyopic eye with the E-ETDRS protocol. This test begins with a screening phase to determine an appropriate visual acuity testing starting point. The threshold phase then determines an upper level at which 5 out of 5 letters are correctly identified and a lower level at which 0 out of 5 letters are correctly identified. The advantage of using the E-ETDRS protocol for clinical research is good test–retest reliability and reduction of potential bias from the examiner.29 At 12 weeks, the treatment was tapered off over one month to prevent regression. They were instructed to patch 1 hour per day for one month and then discontinue patching. The subjects came in at the 24 week visit for a final amblyopia evaluation. Quick CSF was measured at baseline and 12 weeks.
Inclusion Criteria
The subjects had acuities between 20/30 (0.176 logMAR) and 20/200 (1.00 logMAR) in the amblyopic eye. The etiology of the amblyopia was anisometropia and/or strabismus. All subjects were over the age of 18 years. Prior amblyopia therapy was not an exclusion criterion. Informed consent was obtained from all subjects after the study procedures were explained to them.
Exclusion Criteria
Subjects were excluded if they had a visually significant cataract, glaucoma, diabetes, uncontrolled high blood pressure or were pregnant/breastfeeding or expecting to become pregnant during the study period. Other ocular or systemic diseases that affect visual acuity, use of medications that may affect neural function, or the inability to give informed consent also resulted in study exclusion.
Contrast Sensitivity
Contrast sensitivity was measured with the quick CSF system (Adaptive Sensory Technology, San Diego, CA, USA).30 The quick CSF method employs a Bayesian adaptive procedure that predetermines the most efficient and effective stimulus to present on each trial.31 It does this by assuming a typical shape to the contrast sensitivity function. The stimuli were band-pass filtered Sloan letters, and threshold was determined using a 10 alternative forced choice technique. This program determines the area under the log contrast sensitivity function (AULCSF) and the visual acuity (Table 2). The contrast sensitivity at 5 spatial frequencies (1.5, 3, 6, 12, and 18.5 cycles per degree (cpd)) is also determined.
Data Analysis
The visual acuities were analyzed with a general linear model ANOVA to determine if there were any differences in the test results over time. The factors in the ANOVA were visit and subject. Of the total possible visits for all the subjects (14 visits × 9 subjects = 126 visits), 12 visits were missed (subjects 2, 4, and 7 each missed 4 visits). Missed data was handled by carrying forward the last value. A post-hoc Dunnett multiple comparison test was performed to determine which weeks were significantly different from baseline. The contrast sensitivity data was analyzed with a general linear model ANOVA. The factors in the ANOVA were spatial frequency, visit, and subject. Post-hoc paired t-tests were used to determine differences at each spatial frequency. Two sample t-tests were used for other comparisons. Statistical significance for the tests was set at a p ≤ 0.05.
Results
The average (± SE) logMAR visual acuities for the weekly visits are displayed in Figure 1. Two hours of daily patching therapy were carried out through week 12. Treatment was then tapered off over the next month, and a final amblyopia evaluation was done at week 24. An ANOVA indicated that there was a significant difference in acuity across the weeks (F13, 125 = 4.54, p < 0.001). Dunnett multiple comparisons indicated that weeks 4–24 (filled symbols) were significantly different from the baseline acuity (open symbol at week 0). The increase in visual acuity plateaued after about 4 weeks of treatment. There was no difference in acuities for weeks 12 and 24 (paired t-test, t8 = 1.34, p = 0.22). Figure 2 displays the average logMAR visual acuity (SE) for the baseline (0.55 (0.09) logMAR) and week 24 (0.38 (0.09) logMAR) visits for all the subjects. A paired t-test indicated there was a significant improvement in visual acuity (t8 = 3.485, p = 0.008) over this time-period. The data is also displayed for the subjects with anisometropic (SE) (0.41 (0.12) logMAR, 0.19 (0.02) logMAR, t2 = 2.043, p = 0.18) and combined mechanism amblyopia (SE) (0.61 (0.13) logMAR, 0.48 (0.10) logMAR, t5 = 2.874, p = 0.04).
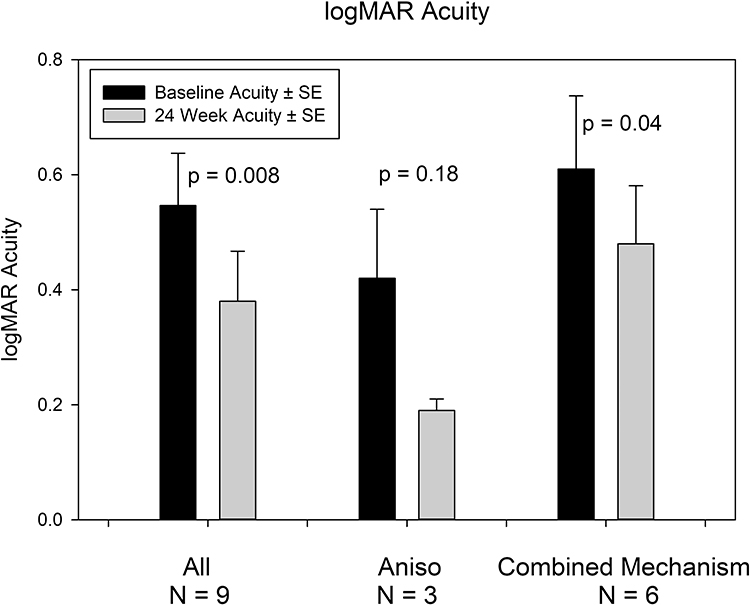 |
Figure 2 Average visual acuity (± SE) for all subjects (N = 9), anisometropic subjects (N = 3), and combined mechanism subjects (N = 6) for the baseline and week 24 visit. The baseline and week 24 acuities are different for all the subjects (p = 0.008) and the combined mechanism subjects (p = 0.04). |
 |
Figure 3 Patient acuity improvement in letters between baseline and week 12 versus age. The circles refer to patients that had prior patching therapy. The squares refer to patients that either had no prior patching therapy (18 year old patient) or had prior strabismus surgery (42 year old patient). The therapy compliance is given next to each data point. The data points with an “A” are the anisometropic subjects. The best fit line and equation are shown. The acuity improvement decreases 2.2 letters for each decade of life. |
Figure 3 displays the age of the subjects versus the acuity improvement from baseline to week 12 in letters. The symbols with an “A” are the subjects with only anisometropia. The circles refer to patients that had prior patching therapy and the squares refer to patients that either had no prior patching therapy (18-year-old patient) or only prior strabismus surgery (42-year-old patient). Treatment compliance is displayed next to each data symbol. Compliance was determined from the iNET program usage records. 100% compliance indicates that the subject performed the iNET program for 30 minutes per day, five days per week for 12 weeks. The best fit line to the data is shown (y = (−0.2176x) + 13.82, r = −0.68, p = 0.045). The slope of the line indicates that acuity improvement drops about 2.2 letters per decade of life. Thus, the maximum improvement in acuity decreases with age. The average increase in acuity from baseline to 12 weeks was 1.8 lines for the subjects 18 to 35 years of age and 0.4 lines for subjects 36 to 60 years of age.
The quick CSF data for baseline and week 12 are displayed in Figure 4. The horizontal axis is spatial frequency in cycles per degree (cpd), and the vertical axis is contrast sensitivity. The filled symbols are the baseline data, and the open symbols are the 12-week data. None of the subjects could see the highest spatial frequency at either visit (18 cpd). An ANOVA found a significant difference between the baseline and week 12 data (F1, 58 = 11.02, p = 0.002). A post-hoc paired t-test analysis indicated that the data at 1.5 (t8 = 3.36, p = 0.01), 3 (t8 = 3.40, p = 0.01), and 6 cpd (t6 = 2.62, p = 0.04) are significantly different between baseline and 12 weeks. The data at 12 cpd were not significantly different (t5 = 1.61, p = 0.17) between baseline and week 12. This may have resulted because only 6 of the 9 subjects could see the 12 cpd stimulus resulting in low statistical power for the comparison (power = 0.26). The quick CSF calculated AULCSF (SE) for the baseline (0.94 (0.14)) and week 12 (1.09 (0.14)) visits are significantly different (t8 = 4.41, p = 0.002, Table 2). The visual acuity (cpd) (SE) calculated from the quick CSF for baseline (8.9 (1.33) cpd) and week 12 (10.38 (1.57) cpd) are also significantly different (t8 = 2.52, p = 0.036, Table 2).
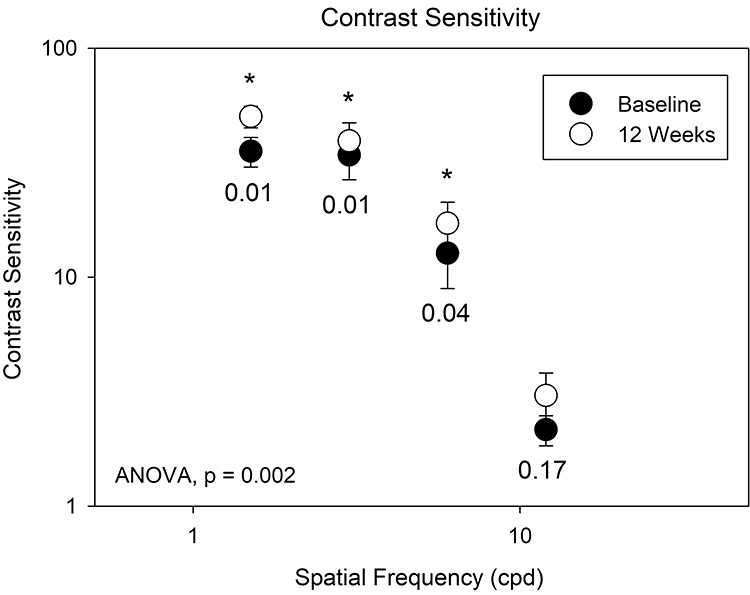 |
Figure 4 The average contrast sensitivity for all the subjects at baseline and week 12. An ANOVA indicated that the baseline and week 12 data are significantly different (p = 0.002). A post-hoc paired t-test analysis indicated that the data at 1.5, 3, and 6 cpd (p values below the symbols) are significantly different (indicated with an asterisk) at baseline and 12 weeks. |
There were no significant changes in ocular alignment, sensory fusion, or accommodation. However, many of the subjects had an improvement in stereopsis, specifically lateral disparity. Better depth perception can lead to an improvement in activities of daily living, such as walking down the stairs or driving. The stereopsis findings (both random dot and lateral disparity) are included in Table 3.
 |
Table 3 The Baseline, 12-, and 24-Week Visit Stereopsis Results for the Subjects |
Discussion
The nine adult subjects (ages 18–60) with anisometropic or combined mechanism amblyopia that participated in this study demonstrated a significant increase in visual acuity (average 0.17 logMAR increase, p = 0.008) with 12 weeks of standard patching therapy for 2 hours per day combined with near or distance activities (Table 2). The visual acuity did not change from week 12 to 24 (p = 0.22) indicating there was no regression in visual acuity after patching treatment was stopped. Their AULCSF (p = 0.002) and visual acuity (p = 0.036) also improved significantly (Table 2). Contrast sensitivity increased at 1.5 (p = 0.01), 3.0 (p = 0.01), and 6.0 (p = 0.04) cpd.
The maximum number of patching hours for the 12 weeks of this study was 120 (2 hours per day × 5 days per week × 12 weeks = 120 hours). A previous study with children with amblyopia demonstrated a 1–2 line improvement in logMAR acuity with about 200 hours of patching therapy.32 The 1.7 line improvement in acuity found in the adult subjects with amblyopia in the current study agrees with previous publications on children with amblyopia. However, unlike studies with children, the acuity in adults with amblyopia did not continue to improve past about 4 weeks of therapy.33,34 Thus, there may be an upper limit on acuity improvement for adults. The increase in acuity with patching therapy may depend on several factors: previous treatment,11 age at initiation of treatment,8,11,12 patching compliance with treatment,35 initial visual acuity,8 and etiology of amblyopia.
A recent study with previously untreated adults (17–35 years old) with anisometropic amblyopia performing patching (2 hours/day for 5 weeks) with near visual activities found an increase in visual acuity (0.23 logMAR).23 The three subjects with anisometropia in the current study also displayed an increase in acuity of 0.23 logMAR (t2 = 2.043, p = 0.18), whereas the six subjects with combined mechanism amblyopia only had an acuity increase of 0.13 logMAR (t5 = 2.874, p = 0.04). Most subjects in the present study had a history of previous patching (7/9) or strabismus surgery (1/9) thus previous treatment is not a limiting factor for acuity improvement. The change in acuity for the subjects with anisometropia did not reach significance because of the small number of subjects and a lack of significant test power (alpha = 0.05, power = 0.394). There was no difference in the average age of these two groups (30.6 years old for both groups). Unlike children, adults with strabismic amblyopia may not gain as much improvement in acuity from the standard treatment as adults with anisometropic amblyopia.34
Figure 3 suggests that there is a decrease in best obtainable acuity with age. Similar findings have been seen in children.11 For all of the amblyopes in the present study, the improvement in acuity decreased by about 2.2 letters with each decade of life between the ages of 18 and 60. The average improvement in acuity was 1.8 lines for those under 35 years of age and 0.4 lines for those over 35 years of age. These results suggest that acuity in adults with amblyopia can be improved, but the potential for this improvement decreases gradually throughout adulthood.
The present results indicate that there are other, unidentified reasons affecting the post-therapy acuity. For example, subjects 5 and 6 have similar ages and etiologies for their amblyopia. Compared to subject 5, subject 6 had poorer therapy compliance but a much better improvement in acuity. The only identified difference that may explain this acuity outcome may be the poorer baseline acuity for subject 6 (Table 2). It is also possible that unknown biological factors (eg, neuromodulators) alter the duration of the critical period differently across individuals.36
Previous studies have indicated that contrast sensitivity increases in the amblyopic eye of children treated for amblyopia.37,38 Depending on the magnitude of the baseline amblyopia, the contrast sensitivity may be abnormal only at high spatial frequencies37 or abnormal at all spatial frequencies tested.38 The adult subjects in the current study demonstrated an increase in contrast sensitivity at 1.5 (p = 0.01), 3 (p = 0.01), and 6 cpd (p = 0.04) after treatment. The data at 12 cpd were not significantly different (p = 0.17) between baseline and week 12 because of low statistical test power (power = 0.26). The increase in the calculated quick CSF acuity was not significantly different from the ETDRS logMAR acuity at week 12 (t8 = 1.46, p = 0.18). The log of the area under the curve for the baseline and week 12 visits were also significantly different (t8 = 4.41, p = 0.002). Thus, the adult subjects with amblyopia demonstrated an increase in contrast sensitivity due to treatment.
A previous report in amblyopic children (<17 years old) found an increase in log contrast sensitivity (SD) at 3 (0.17 (0.23)), 6 (0.30 (0.24)), 12 (0.44 (0.32)), and 18 (0.51 (0.38)) cpd with the CSV-1000 test after 1 month of training with the amblyopia iNET program (30 minutes per day for 5 days per week) combined with patching.38 The adult subjects in the current study demonstrated an increase in log contrast sensitivity (SD) of 0.19 (0.17), 0.16 (0.15), 0.16 (0.16), and 0.19 (0.29) at 1.5, 3, 6, and 12 cpd, respectively. The increase in contrast sensitivity was similar between the two groups for low spatial frequencies, but the children demonstrated a greater average increase at higher spatial frequencies compared to the adults. This could be explained if the children also exhibited a greater increase in visual acuity; however, the average increase in acuity was 0.2 logMAR for the children which is similar to the 0.17 logMAR increase seen in the adults in this study.
Patching compliance has a significant effect on the outcome of amblyopia therapy.24,35,39,40 The adult subjects in this study had 70.3 ± 28.9% compliance with the iNET training program and demonstrated a significant increase in acuity and contrast sensitivity. A prior study with children indicated that subjects with good compliance (80% ± 32%) with treatment had better acuity outcomes than those with poor compliance (34% ± 31%).35 Previous studies in adults with amblyopia may have had poor outcomes because of poor compliance with treatment. Simonsz-Toth et al (2019) carried out optical correction and patching therapy in 11 adults with amblyopia and 6 children (<18 years of age) with amblyopia.24 The average increase in acuity was only 0.05 logMAR, which may have been the result of poor compliance with treatment (overall compliance of 17%). They suggested that compliance in adults is more difficult than in children. Thus, if compliance with therapy is poor, visual acuity will not improve to the maximum potential in either children or adults.
This study does have a few limitations that may have affected the conclusions. Only nine subjects completed this study. A larger number of anisometropes would likely have resulted in a significant difference in their acuity from baseline to 24 weeks post-therapy. A sample size assessment suggested that nine subjects were adequate to reach statistical significance, so subdividing the amblyopes into groups resulted in less power for the statistical analysis. Another limitation is that eccentric fixation was not consistently assessed in this study. The presence of eccentric fixation in individuals with strabismic amblyopia can impact the potential improvement in visual acuity. This should be properly assessed and monitored in future amblyopia studies. Furthermore, to best monitor overall compliance with patching, subjects should have been asked to document the amount of patching that was done with a daily log. Additionally, the study was not masked and there were no untreated subjects. Masking would likely have little effect on the results since visual acuity and contrast sensitivity were measured with computerized systems. However, following untreated subjects would allow for the determination of a learning effect.
Previous studies employing the ETDRS chart suggested that the acuity must change by at least 0.14 logMAR to be statistically significant.41 The average acuity increase in the present study was similar to this at 0.17 logMAR. However, Figure 1 demonstrates that the average acuity consistently improved over the first 4 weeks suggesting that the increase in acuity is not random and is significant.
Conclusion
In conclusion, adults with amblyopia due to anisometropia or combined mechanism demonstrate an improvement in acuity and contrast sensitivity with 12 weeks of patching therapy combined with near and/or distance visual activities. The improvement in acuity and contrast sensitivity is age dependent and did not depend on a history of previous therapy. Baseline visual acuity and compliance with therapy may be other major factors in acuity improvement in adults. However, other unidentified factors may also play a role in acuity improvement.
Abbreviations
A, anisometropia; ANOVA, analysis of variance; AULCSF, area under the log of the contrast sensitivity function; C, constant; cpd, cycles per degree; CSF, contrast sensitivity function; E-ETDRS, electronic-early treatment diabetic retinopathy study visual acuity tester; ET, esotropia; XT, exotropia; HyperT, hypertropia; I, intermittent; logMAR, Logarithm of the Minimum Angle of Resolution; S, strabismus; SD, standard deviation; SE, standard error.
Data Sharing Statement
The data for visual acuity and contrast sensitivity are in Table 2. The stereopsis data are in Table 3.
Statement of Ethics
Research was conducted ethically in accordance with the Declaration of Helsinki. For better efficiency, the study protocol was reviewed and approved by a commercial IRB company externally from the University (Sperling Institutional Review Board, Atlanta, Georgia). Written informed consent was obtained from all participants in the study.
Acknowledgments
The authors thank Apoorva Karsolia for collecting some of the data and Loc Nguyen, PhD (California State University) for the statistical analysis. This paper was presented at the Association for Research in Vision and Ophthalmology as an abstract presentation with preliminary findings. The poster’s abstract was published in “Poster Abstracts” in Investigative Ophthalmology & Visual Science July 2018, Vol.59, 4112.
Author Contributions
All authors met the IMCJE authorship guidelines for inclusion. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This project was partially funded by Allergan (prior to acquisition by AbbVie). They had no role in study design or manuscript development.
Disclosure
Ursula Staubli is a prior employee and Yong-Xin Li is a current employee of AbbVie. Inc. (formerly Allergan, Inc.). Ursula Staubli is currently affiliated with Center for Neurobiology of Learning and Memory, University of California Irvine, Irvine, CA, USA. The authors have no other conflict of interest in this work.
References
1. von Noorden GK. Amblyopia: a multidisciplinary approach. Proctor lecture. Invest Ophthalmol Vis Sci. 1985;26(12):1704–1716.
2. Michaels DD. Visual Optics and Refraction: A Clinical Approach. St Louis, MO: C.V. Mosby Co.; 1980.
3. London R, Wick B. Patients with amblyopia and strabismus. In: Benjamin WJ, editor. Borish’s Clinical Refraction.
4. Fu Z, Hong H, Su Z, Lou B, Pan CW, Liu H. Global prevalence of amblyopia and disease burden projections through 2040: a systematic review and meta-analysis. Br J Ophthalmol. 2020;104(8):1164–1170.
5. Pediatric Eye Disease Investigator Group Writing C. A randomized trial of atropine vs. patching for treatment of moderate amblyopia in children. Arch Ophthalmol. 2002;120(3):268–278.
6. Hertle RW, Scheiman MM, Beck RW, et al. Stability of visual acuity improvement following discontinuation of amblyopia treatment in children aged 7 to 12 years. Arch Ophthalmol. 2007;125(5):655–659.
7. Holmes JM, Edwards AR, Beck RW, et al. A randomized pilot study of near activities versus non-near activities during patching therapy for amblyopia. J Aapos. 2005;9(2):129–136.
8. Holmes JM, Kraker RT, Beck RW, et al. A randomized trial of prescribed patching regimens for treatment of severe amblyopia in children. Ophthalmology. 2003;110(11):2075–2087.
9. Loudon SE, Simonsz HJ. The history of the treatment of amblyopia. Strabismus. 2005;13(2):93–106.
10. Wallace DK, Edwards AR. A randomized trial to evaluate 2 hours of daily patching for strabismic and anisometropic amblyopia in children. Ophthalmology. 2006;113(6):904–912.
11. Holmes JM, Lazar EL, Melia BM, et al. Effect of age on response to amblyopia treatment in children. Arch Ophthalmol. 2011;129(11):1451–1457.
12. Holmes JM, Repka MX, Kraker RT, Clarke MP. The treatment of amblyopia. Strabismus. 2006;14(1):37–42.
13. Morishita H, Hensch TK. Critical period revisited: impact on vision. Curr Opin Neurobiol. 2008;18(1):101–107.
14. Levi DM. Linking assumptions in amblyopia. Vis Neurosci. 2013;30(5–6):277–287.
15. Levi DM, Li RW. Perceptual learning as a potential treatment for amblyopia: a mini-review. Vision Res. 2009;49(21):2535–2549.
16. Levi DM, Li RW. Improving the performance of the amblyopic visual system. Philos Trans R Soc Lond B Biol Sci. 2009;364(1515):399–407.
17. Hess RF, Mansouri B, Thompson B. A new binocular approach to the treatment of amblyopia in adults well beyond the critical period of visual development. Restor Neurol Neurosci. 2010;28(6):793–802.
18. Li J, Thompson B, Deng D, Chan LY, Yu M, Hess RF. Dichoptic training enables the adult amblyopic brain to learn. Curr Biol. 2013;23(8):R308–309.
19. Tsirlin I, Colpa L, Goltz HC, Wong AM. Behavioral training as new treatment for adult amblyopia: a meta-analysis and systematic review. Invest Ophthalmol Vis Sci. 2015;56(6):4061–4075.
20. Gao TY, Guo CX, Babu RJ, et al. Effectiveness of a binocular video game vs placebo video game for improving visual functions in older children, teenagers, and adults with amblyopia: a randomized clinical trial. JAMA Ophthalmol. 2018;136(2):172–181.
21. Holmes JM, Manh VM, Lazar EL, et al. Effect of a binocular iPad game vs part-time patching in children aged 5 to 12 years with amblyopia: a randomized clinical trial. JAMA Ophthalmol. 2016;134(12):1391–1400.
22. Holmes JM, Manny RE, Lazar EL, et al.; Pediatric Eye Disease Investigator G. A randomized trial of binocular dig rush game treatment for amblyopia in children aged 7 to 12 years. Ophthalmology. 2019;126(3):456–466.
23. Sharbatoghli L, Hashemi H, Mohamadi A, et al. Visual acuity improvement in adult anisometropic amblyopes after active vision therapy. Clinical Optometry. 2020;12:183–187.
24. Simonsz-Toth B, Joosse MV, Besch D. Refractive adaptation and efficacy of occlusion therapy in untreated amblyopic patients aged 12 to 40 years. Graefes Arch Clin Exp Ophthalmol. 2019;257(2):379–389.
25. Hou F, Huang CB, Tao L, Feng L, Zhou Y, Lu ZL. Training in contrast detection improves motion perception of sinewave gratings in amblyopia. Invest Ophthalmol Vis Sci. 2011;52(9):6501–6510.
26. Caloroso E, Rouse MW. Clinical Management of Strabismus. Boston: Butterworth-Heinemann; 2007.
27. Gao TY, Anstice N, Babu RJ, et al. Optical treatment of amblyopia in older children and adults is essential prior to enrolment in a clinical trial. Ophthalmic Physiol Opt. 2018;38(2):129–143.
28. Moseley MJ, Fielder AR, Stewart CE. The optical treatment of amblyopia. Optom Vis Sci. 2009;86(6):629–633.
29. Wang J, Feng L, Wang Y, Zhou J, Hess RF. Binocular benefits of optical treatment in anisometropic amblyopia. J Vis. 2018;18(4):6.
30. Hou F, Lesmes L, Bex P, Dorr M, Lu ZL. Using 10AFC to further improve the efficiency of the quick CSF method. J Vis. 2015;15(9):1–18.
31. Lesmes LA, Lu ZL, Baek J, Albright TD. Bayesian adaptive estimation of the contrast sensitivity function: the quick CSF method. J Vis. 2010;10(3):1–21.
32. Stewart CE, Moseley MJ, Stephens DA, Fielder AR. Treatment dose-response in amblyopia therapy: the Monitored Occlusion Treatment of Amblyopia Study (MOTAS). Invest Ophthalmol Vis Sci. 2004;45(9):3048–3054.
33. Wallace DK, Lazar EL, Crouch ER, et al. Time course and predictors of amblyopia improvement with 2 hours of daily patching. JAMA Ophthalmol. 2015;133(5):606–609.
34. Pediatric Eye Disease Investigator Group Writing C. The Course of Moderate Amblyopia Treated with Patching in Children: experience of the Amblyopia Treatment Study. Am J Ophthalmol. 2003;136(4):620–629.
35. Loudon SE, Polling JR, Simonsz HJ. A preliminary report about the relation between visual acuity increase and compliance in patching therapy for amblyopia. Strabismus. 2002;10(2):79–82.
36. Bavelier D, Levi DM, Li RW, Dan Y, Hensch TK. Removing brakes on adult brain plasticity: from molecular to behavioral interventions. J Neurosci. 2010;30(45):14964–14971.
37. Polat U, Ma-Naim T, Spierer A. Treatment of children with amblyopia by perceptual learning. Vision Res. 2009;49(21):2599–2603.
38. Hernandez-Rodriguez CJ, Fukumitsu H, Ruiz-Fortes P, Soto-Negro R, Merino-Suarez M, Pinero DP. Efficacy of perceptual learning-based vision training as an adjuvant to occlusion therapy in the management of amblyopia: a pilot study. Vision. 2021;5(1):54.
39. Awan M, Proudlock FA, Gottlob I. A randomized controlled trial of unilateral strabismic and mixed amblyopia using occlusion dose monitors to record compliance. Invest Ophthalmol Vis Sci. 2005;46(4):1435–1439.
40. Stewart CE, Fielder AR, Stephens DA, Moseley MJ. Treatment of unilateral amblyopia: factors influencing visual outcome. Invest Ophthalmol Vis Sci. 2005;46(9):3152–3160.
41. Arditi A, Cagenello R. On the statistical reliability of letter-chart visual acuity measurements. Invest Ophthalmol Vis Sci. 1993;34(1):120–129.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Profile of Amblyopia Among Children Aged from 5 to 15 Years at Hawassa University Comprehensive Specialized Hospital Pediatric Eye Clinic, South Ethiopia, 2020/21
Gebru EA, Alem KD, G/Silassie MG
Clinical Optometry 2022, 14:149-157
Published Date: 10 August 2022
Acuity Comparison Methods via Timed Test-Retest Precision of Matching-Card e-ETDRS Compared to PDI Check in Treated Amblyopes and Superb Normals

Hepler LE, Martin SJ, Fuglseth K, Cuddihee L, Giannulis P, Arnold RW
Clinical Optometry 2023, 15:81-95
Published Date: 2 May 2023
Effects of Dexamethasone Intravitreal Implant on Multifocal Electroretinography in Diabetic Macular Oedema
Tranos P, Koukoula S, de Politis PB, Tranou M, Giamouridou O, Stavrakas P, Panos GD
Drug Design, Development and Therapy 2024, 18:5367-5375
Published Date: 25 November 2024
Efficacy of Dichoptic Treatment vs Eye Patching in Pediatric Patients with Amblyopia: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Nughays RO, Almazroy EA, Elyas SK, Alamoudi A, Batais WT, Bogari AM, Alnabihi A, Alkharboush DH, Almarzouki H
Clinical Ophthalmology 2025, 19:1999-2009
Published Date: 26 June 2025
Estimating the Prevalence and Severity of Isolated Small-Angle Strabismic Amblyopia

Arnold RW
Clinical Ophthalmology 2025, 19:3409-3418
Published Date: 16 September 2025