Back to Journals » International Journal of General Medicine » Volume 19
Establishment of Serum 25-Hydroxyvitamin D Reference Range for Healthy Adult Men Not Using Vitamin D Supplements in Alqurayyat, Saudi Arabia
Authors Aldaham AMS ![]() , Beheiry A, Hamza AA
, Beheiry A, Hamza AA ![]() , Albalawi MH
, Albalawi MH ![]() , Alanazi AM, Alanazi AS, Albilasi MM
, Alanazi AM, Alanazi AS, Albilasi MM ![]() , AlRuwaili AM, ALabdali AM
, AlRuwaili AM, ALabdali AM ![]() , Alanazi AS, Alanazi MR
, Alanazi AS, Alanazi MR ![]()
Received 21 April 2025
Accepted for publication 18 February 2026
Published 24 March 2026 Volume 2026:19 535665
DOI https://doi.org/10.2147/IJGM.S535665
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Woon-Man Kung
Azizah Mazi Saud Aldaham,1 Ashraf Beheiry,2 Alneil Abdalla Hamza,3 Marzoq Hassan Albalawi,2 Abdullah Maashi Alanazi,2 Abdullah Saud Alanazi,2 Mohammed Menwer Albilasi,2 Abdulaziz Mohammed AlRuwaili,2 Abdulwahab Mohammed ALabdali,2 Abdulhamid Salem Alanazi,2 Mashael Rahil Alanazi2
1Department of Laboratories and Blood Bank, Alqurayyat General Hospital, Alqurayyat, Saudi Arabia; 2Department of Regional Laboratory and Central Blood Bank, Alqurayyat Regional Laboratory and Central Blood Bank, Alqurayyat, Saudi Arabia; 3Department of Clinical Laboratory, College of Applied Medical Sciences, Al-Jouf University, Alqurayyat, Saudi Arabia
Correspondence: Azizah Mazi Saud Aldaham, Department of Laboratories and Blood Bank, Alqurayyat General Hospital, Alqurayyat, Saudi Arabia, Tel +966 559309362, Email [email protected]
Background: Vitamin D is a secosteroid, a lipid-soluble vitamin that is involved in various physiological responses, including skeletal metabolism and immune response. Vitamin D [25(OH)D] in the blood is also influenced by environmental factors, lifestyle, and is genetically determined. While there is abundant sunlight in every part of Saudi Arabia throughout the year, hypovitaminosis D is prevalent. The locally obtained reference interval has not yet been defined among the people of Alqurayyat. The study was conducted to identify population-specific serum 25(OH)D reference ranges among healthy adult Saudi men in Alqurayyat who do not receive vitamin D supplements.
Materials and Methods: The study was a cross-sectional design conducted between December 2022 and August 2023. 204 apparently healthy Saudi men aged 18– 45 years were selected after eliminating statistical exceptions. Participants were taken from voluntary blood donors at Alqurayyat General Hospital. Serum 25(OH)D was measured by chemiluminescence immunoprecipitation assay done on the UniCel DxI 800 analyzer. The extreme values were also removed by the Tukey method. The reference range was derived using the 95% central distribution, which is the 2.5th and 97.5th percentiles.
Results: The 25(OH)D mean was 12.47 ± 4.84 ng/mL (95% CI: 11.77– 13.17 ng/mL). The calculated reference interval was 4.22– 26.14 ng/mL, which is significantly lower than the international norms. Vitamin D was low in 93%, under 20 ng/mL, with 7% between 20– 29 ng/mL. None of the subjects had adequate levels (> 30 ng/mL).
Conclusion: The high prevalence of vitamin D deficiency (93%) in this population of non-supplementing healthy adult men is one of the key health issues of the population. The calculated reference range is quite low compared to international standards, which probably shows local lifestyle and cultural conditions restricting productive sun exposure. More research and specific treatment are justified.
Keywords: Vitamin D, 25-hydroxyvitamin D, 25(OH)D, healthy adults, vitamin D deficiency, reference range, Saudi Arabia
Introduction
Vitamin D is a key secosteroid hormone that plays a vital role in bone and muscle metabolism, immune regulation, and calcium homeostasis regulation.1 Ergocalciferol (vitamin D2) and cholecalciferol (vitamin D3) are the main precursor forms of vitamin D. It is then passed on to the liver where vitamin D is converted into 25-hydroxyvitamin D [25(OH)D], which is hydroxylated further in the kidney to 1, 25-dihydroxyvitamin D, the biologically active form Serum 25(OH)D is the marker of choice of vitamin D status, as it is the product of cutaneous synthesis and dietary intake.2,3
Vitamin D levels in the blood change seasonally and are affected by diet, genetics, and the environment.4 Vitamin D3, essential for bone health, is produced in the skin through sun exposure. Vitamin D deficiency is a significant global public health issue affecting an estimated one billion people worldwide. It is associated with rickets, osteomalacia, and an increased risk of fractures, often because of limited sunlight exposure and low dietary intake of vitamin D–rich foods.5,6 Although Middle Eastern countries such as Saudi Arabia receive abundant sunlight, vitamin D deficiency remains highly prevalent.7,8 This paradox has been linked to predominantly indoor lifestyles, skin‑covering clothing, low levels of outdoor physical activity, widespread use of air conditioning, and low dietary intake of vitamin D in Saudi Arabia.9 Previous studies from Saudi Arabia have reported vitamin D deficiency rates ranging from 50% to 100% in ostensibly healthy populations, including 67.8% in Qassim and high prevalence among blood donors in northern regions.10,11
In Saudi adult men in particular, 76.1% deficiency was found.12 Vitamin D deficiency is still widespread in sunny areas, which highlights the necessity of regular checkups. No global agreement on diagnostic levels, however, specialists define adequacy at ≥30 ng/mL, insufficiency at 20–29 ng/mL, and deficiency as ≤20 ng/mL. The local aspects can make the level of 25(OH)D different from international standards and other parts of Saudi Arabia.13,14 It is, therefore, imperative to determine a population-specific reference range to diagnose and treat vitamin D deficiency more accurately. We hypothesized that the serum 25(OH)D level of healthy adult men in Alqurayyat who did not use vitamin D supplements would be lower than international standards.15,16 The purpose of the study was to set the serum 25(OH)D level in this population and identify the prevalence of vitamin D deficiency.
Materials and Methods
Study Design
The study is a cross-sectional research study that was conducted at the Regional Laboratory of Alqurayyat General Hospital, Northern Province, Saudi Arabia, during the period of December 2022 to August 2023. The study was carried out under the Declaration of Helsinki, and the participants gave their consent under the Health Affairs Research and Ethics Committee of Alqurayyat.
We selected 204 Saudi young men, who are healthy and aged 18 to 45 years, to donate their blood independently. The sample size was selected to be larger than 120, as the Clinical and Laboratory Standards Institute (CLSI) EP28-A3c guidelines suggest setting the reference intervals. This was suggested to increase the precision and validity of the produced reference interval.
Inclusion and Exclusion Criteria
The participants were reported to be healthy adults of the local community, which was defined by CLSI EP28-A3c criteria. A clinical examination and history were employed to rule out disorders known to influence vitamin D metabolism, such as malabsorption syndromes, chronic liver disease, renal impairment, nephrotic syndrome, obesity related disorders, use of vitamin D supplements, or medications affecting the vitamin D levels.
Sample Collection and Laboratory Analysis
The samples of blood were obtained by donating blood and then separated to be examined through serum analysis. Concentrations of serum 25-hydroxyvitamin D were determined by conducting a chemiluminescent immunoassay in the UniCel DxI 800 (Beckman Coulter, Brea, CA, USA) with a detection range ranging between 3.0–100.0 ng/mL and a quantifying limit of 4.0 ng/mL. The inter-assay coefficient of variation, intra-assay coefficient of variation, and accuracy were 5, 3, and 98%, respectively, relative to the LC-MS/MS/reference method. Even though the sampling was done between 2022 (December) and 2023 (August), the sampling design limits the evaluation of seasonal changes in 25(OH)D levels. The stratified future longitudinal research ought to be seasonal to consider sunlight exposure. The following were the vitamin D categories: deficiency at 20 ng/mL or below, insufficiency at 20–30 ng/mL, adequacy at 30 ng/mL or above.
Statistical Analysis
The analysis of data was performed with SPSS version 20.0 (IBM Corp., Armonk, NY, USA). The visual and statistical control of normal distribution was performed, and the outliers were eliminated with the help of the Tukey method (interquartile range x 1.5). The reference ranges were the 2.5th and 97.5th percentiles of the rest of the data. Descriptive statistics are provided in terms of mean ±SD and 95% confidence interval (CI), where necessary. The Pearson correlation coefficients of 25 (OH) D, PTH, and calcium were determined. Measurement uncertainty was used in rounding off numerical values: Two significant figures were employed when the uncertainty was greater than 7. P-values that were below 0.05 were considered statistically significant.
Results
Levels of 25-hydroxyvitamin D [25(OH)D] in the blood of 204 healthy adult male blood donors from Saudi Arabia, aged 18 to 45 years, not taking any vitamin D supplement at all, were measured. Initially, the distribution of 25(OH)D was right-skewed, with most of the values in the lower part. This is illustrated in Figure 1.
 |
Figure 1 Distribution of serum 25-hydroxyvitamin D [25(OH)D] levels in healthy adult men not using vitamin D supplements in Alqurayyat, Saudi Arabia (n=204). X-axis: 25(OH)D concentration (ng/mL); Y-axis: Frequency. The distribution shows a right skew, with the majority of values concentrated at lower levels. |
Using the Tukey method, the twelve outliers, ranging from 40 to 50 ng/mL, were identified as outliers and hence excluded, since such values would not be biologically plausible in the population not taking supplements. Figure 2 illustrates the outliers and the subsequent reduction to the final population size of 192. The detailed calculation for the quartiles, the interquartile range, and the final reference range from the 2.5th to 97.5th percentiles after the exclusion of the outliers is illustrated in Table 1. Age groups, BMI, or the effect of seasonality on 25(OH)D levels could not be explored, since the data did not consider the effect of seasonality.
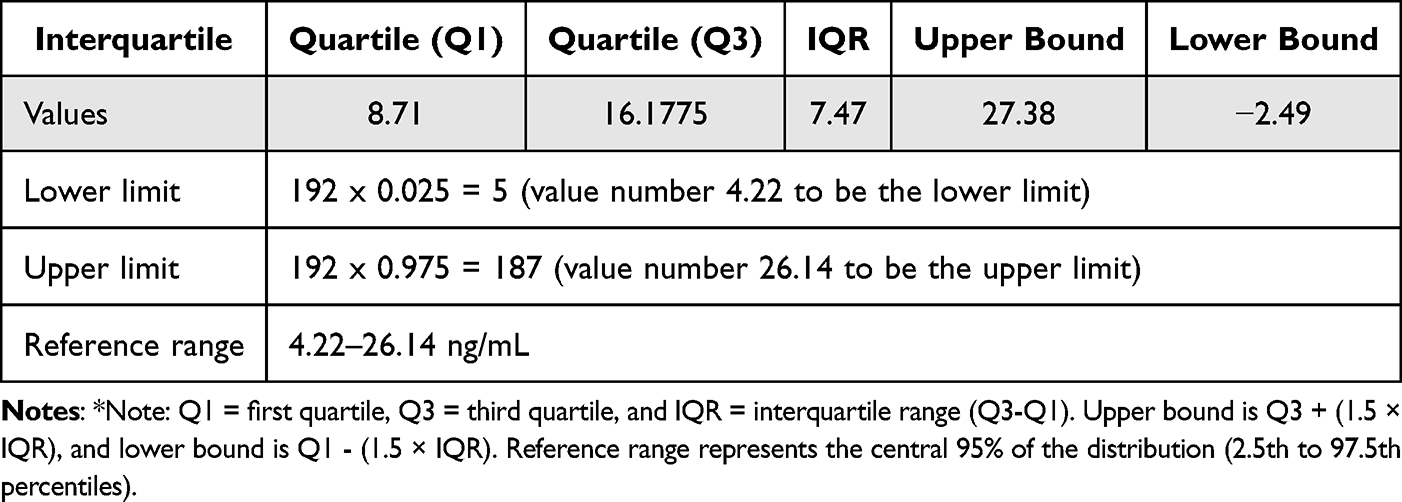 |
Table 1 Interquartile Calculation and Reference Range for Serum 25-Hydroxyvitamin D [25(OH)D] in Healthy Adult Men Not Using Vitamin D Supplements (n=192) |
 |
Figure 2 Identification and removal of outliers using the Tukey method. Twelve participants with 25(OH)D levels >30 ng/mL were excluded, leaving a final study population of 192 participants. These outliers likely represent unreported vitamin D supplement use. |
The mean 25(OH)D serum level in the last group was 12.47 ± 4.84 ng/mL, with a 95% CI of 11.77–13.17 ng/mL. The reference range for the population, which represents the central 95%, was from 4.22 to 26.14 ng/mL. The vitamin D levels were measured using the Endocrine Society criteria. As shown in Table 2, vitamin D deficiency was found in 93% of the subjects, insufficiency in 7%, and none of the subjects reached sufficiency.
 |
Table 2 Vitamin D Status of Participants (According to Endocrine Society Guidelines).17 |
Additional biochemical parameters, including parathyroid hormone (PTH) and serum calcium, are summarized in Table 3.
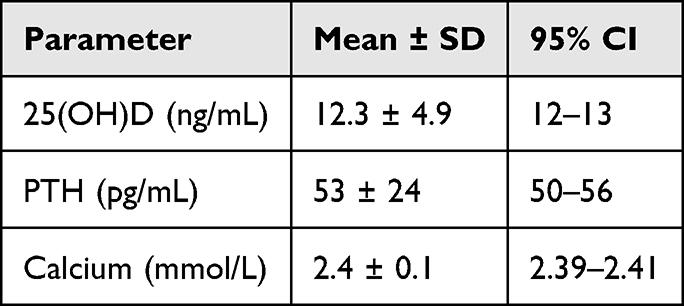 |
Table 3 Biochemical Parameters (Mean ± SD; 95% CI) |
Pearson correlation coefficients between 25(OH)D, PTH, and calcium are presented in Table 4. This means that people with 25(OH)D levels below 25 ng/mL had higher PTH levels, as shown in Figure 3. Also, a weak positive correlation was noted between 25(OH)D and serum calcium (r = 0.12, p = 0.095), as depicted in Figure 4.
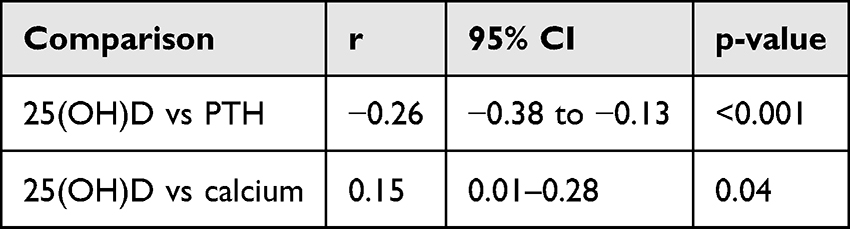 |
Table 4 Correlations Between 25(OH)D, PTH, and Calcium |
 |
Figure 3 Correlation between serum 25(OH)D and parathyroid hormone (PTH) levels. Pearson correlation coefficient r = −0.26 (p < 0.001), indicating a weak negative relationship. X-axis: 25(OH)D (ng/mL); Y-axis: PTH (pg/mL). |
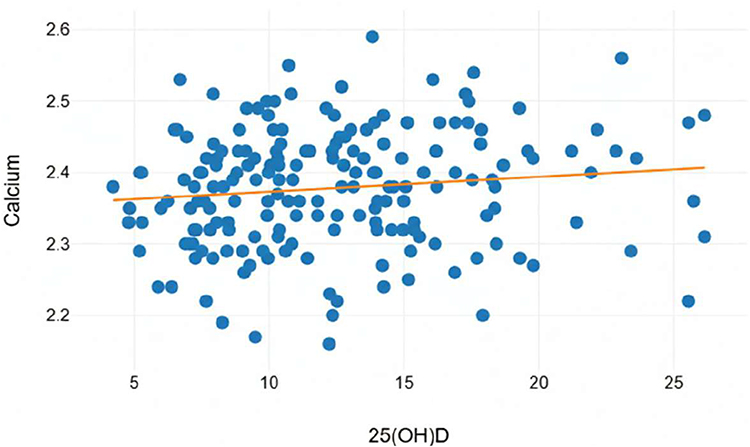 |
Figure 4 Correlation between serum 25(OH)D and calcium levels. Pearson correlation coefficient r = 0.15 (p = 0.04), indicating a weak positive relationship. X-axis: 25(OH)D (ng/mL); Y-axis: Calcium (mmol/L). |
These findings show that the population is significantly deficient in vitamin D, and the obtained reference range falls well below international standards. The results designate the necessity of interventions, since the sample was selected among blood donors, which might have included both women and older adults, active and healthy men in Alqurayyat, but it is still unclear whether the results should be generalized to the general population.
Discussion
Even though there is a lot of sunlight, the vitamin D deficiency rate is 93% because of a number of factors. Some of these are clothes, living indoors, genetic differences in vitamin D binding protein and CYP2R1, not eating enough foods that are high in vitamin D, and using sunscreen.18 Wearing regular clothes that cover most of the skin cuts down on vitamin D production by a lot. Also, some cultures like to stay inside when it’s sunny, which makes it even harder to get vitamin D.18 The 25(OH)D levels in this group are much lower than the global average of 30 ng/mL.19
Although Saudi Arabia enjoys all-year-round access to sunlight, which is considered sufficient to allow people to produce sufficient cutaneous vitamin D, the very high prevalence of such deficiency in this country is consistent with numerous previous studies in the nation.20 This paradox can be mostly attributed to the values and lifestyle aspects that severely restrict the ability to spend time in the sun. Such factors are the traditional clothes that cover most of the body, the preference to spend most of the time indoors and use air conditioning, insufficient physical exercise, and low dietary intake of foods rich in vitamin D.21 The contributing factors that were not evaluated in the present study could include genetic variation of vitamin D binding proteins or metabolism.
The derived reference range shows that there are regional effects. Studies from other Saudi regions, like Qassim (67.8% deficiency) and the northern areas, show that the deficiency rate is high among healthy adults and blood donors.22 A study that came before found that 76.1% of Saudi men were lacking. The fact that Alqurayyat is in the north and has stricter rules for excluding supplement users may explain why our study found a higher prevalence (93%). This shows how important it is to have data from the area when making medical decisions. Gulf countries that are close by have also had similarly high rates of incidence.23,24 Elimination of 12 outliers because of a level greater than 30 ng/mL points to the lack of unreported vitamin D supplementation, since these levels are rare in non-supplementing groups. This observation supports the idea that supplementation is able to achieve adequate levels in high-risk groups.25 Therefore indicates that secondary hyperparathyroidism is compensating for a vitamin D deficiency of some sort in the long term to maintain calcium in the blood at normal levels. Although these changes may be of no significant consequence, they can eventually result in chronic issues such as a decrease in bone density and increased fracture risk.26
In Alqurayyat and the more northern part, the 93% deficiency rate among adult males is a significant public health risk.27,28 This requires certain measures, including routine screening of risk groups, educational initiatives of healthy adults regarding safe sun exposure and food sources, food fortifications, and localized guidelines on supplementation.29 Since the research only focused on men aged 18 to 45 years, it cannot be extended to women or older adults, as well as to less healthy people. The cross-sectional nature of the study also renders it difficult to determine whether the occurrence of changes or causes is seasonal. These demographics should be considered in future research, and such variables as BMI, sun exposure, and dietary habits should be investigated to determine the complete national ranges of reference.30
Conclusions
The study is a reference range of serum 25(OH)D in healthy men aged above 18 years without vitamin D supplements in Alqurayyat, Saudi Arabia. The range is 4.22–26.14 ng/mL. The high prevalence of deficiency of 93% highlights an important problem in sun-rich region in terms of public health. The future multicenter investigations should be gender inclusive, factor seasonal changes, and combine lifestyle factors towards development of comprehensive national reference ranges towards clinical guidance.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Abdulrahman MA, Alkass SY, Mohammed NI. Total and free vitamin D status among apparently healthy adults living in Duhok Governorate. Sci Rep. 2022;12(1):3422. doi:10.1038/s41598-022-05775-x
2. Yu J, He X, Huang S. The establishment of serum 25-hydroxyvitamin D reference intervals in children aged 0–14 years in Zigong area, China. J Physiol Anthropol. 2021;40(1):1–8. doi:10.1186/s40101-021-00265-x
3. Kennel KA, Drake MT, Hurley DL. Vitamin D deficiency in adults: when to test and how to treat. Mayo Clin Proc. 2010;85(8):752–758. doi:10.4065/mcp.2010.0138
4. Kudlacek S, Schneider B, Peterlik M, et al. Assessment of vitamin D and calcium status in healthy adult Austrians. Eur J Clin Invest. 2003;33(4):323–331. doi:10.1046/j.1365-2362.2003.01127.x
5. Siddiqee MH, Bhattacharjee B, Siddiqi UR, MeshbahurRahman M. High prevalence of vitamin D deficiency among the South Asian adults: a systematic review and meta-analysis. BMC Public Health. 2021;21(1):1823. doi:10.1186/s12889-021-11888-1
6. Marwaha RK, Tandon N, Garg MK, et al. Vitamin D status in healthy Indians aged 50 years and above. J Assoc Physicians India. 2011;59:706–709.
7. Binkley N, Novotny R, Krueger D, et al. Low vitamin D status despite abundant sun exposure. J Clin Endocrinol Metab. 2007;92(6):2130–2135. doi:10.1210/jc.2006-2250
8. Khosravi-Boroujeni H, Sarrafzadegan N, Sadeghi M, et al. Prevalence and trends of vitamin D deficiency among Iranian adults: a longitudinal study from 2001 to 2013. J Epidemiol. 2017;27(6):284–290.
9. Al-Daghri NM, Yakout S, Aljohani N, et al. Vitamin D status and its correlation with parathyroid hormone level among the population in Riyadh, Saudi Arabia. J King Saud Univ Sci. 2020;32(3):2016–2019. doi:10.1016/j.jksus.2020.02.002
10. Naeem Z, Almohaimeed A, Sharaf FK, Ismail H, Shaukat F, Inam SB. Vitamin D status among the population of Qassim Region, Saudi Arabia. Int J Health Sci. 2011;5(2):116–124.
11. Elsammak MY, Al-Wossaibi AA, Al-Howeish A, Alsaeed J. High prevalence of vitamin D deficiency in the sunny Eastern region of Saudi Arabia: a hospital-based study. East Mediterr Health J. 2011;17(4):317–322. doi:10.26719/2011.17.4.317
12. Farhat KH, Arafa MA, Rabah DM, Amin HS, Ibrahim NK. Vitamin D status and its correlates in the Saudi male population. BMC Public Health. 2019;19(1):211. doi:10.1186/s12889-019-6527-5
13. Alsuwaida AO, Farag YM, Al Sayyari AA, et al. Prevalence of vitamin D deficiency in Saudi adults. Saudi Med J. 2013;34(8):814–818.
14. Martins JS, Palhares MDO, Teixeira OCM, Gontijo Ramos M. Vitamin D status and its association with parathyroid hormone concentration in Brazilians. J Nutr Metab. 2017;2017:9056470. doi:10.1155/2017/9056470
15. Sadat-Ali M, AlElq A, Al-Turki H, Al-Mulhim A, Al-Ali A. Vitamin D levels in healthy men in eastern Saudi Arabia. Ann Saudi Med. 2009;29(5):378–382. doi:10.4103/0256-4947.55168
16. Malacova E, Cheang P, Dunlop E, et al. Prevalence and predictors of vitamin D deficiency in a nationally representative sample of adults participating in the 2011–2013 Australian Health Survey. Br J Nutr. 2019;121(8):894–904. doi:10.1017/S0007114519000151
17. Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96(7):1911–1930. doi:10.1210/jc.2011-0385
18. Al-Daghri NM. Vitamin D in Saudi Arabia: prevalence, distribution, and disease associations. J Steroid Biochem Mol Biol. 2018;175:102–107. doi:10.1016/j.jsbmb.2016.12.017
19. Brandenburg V, Ketteler M. Vitamin D and secondary hyperparathyroidism in chronic kidney disease: a critical appraisal of the past, present, and the future. Nutrients. 2022;14(15):3009. doi:10.3390/nu14153009
20. Al-Alani H, Al-Turki HA, Al-Essa ON, Alani FM, Sadat-Ali M. Vitamin D deficiency in Saudi Arabians: a reality or simply hype: a meta-analysis (2008-2015). J Family Community Med. 2018;25(1):1–4. doi:10.4103/jfcm.JFCM_73_17
21. Sindi AA, Albanghali MA, Izhari MA, et al. Prevalence of vitamin D deficiency and its association with age, sex and ethnicity in Albaha, Saudi Arabia. J Res Med Dent Sci. 2021;9(12):150–160.
22. Clinical and Laboratory Standards Institute (CLSI). Defining, Establishing, and Verifying Reference Intervals in the Clinical Laboratory.
23. Abukanna AM. Prevalence of vitamin d deficiency among university female students in northern border region of Kingdom of Saudi Arabia (KSA). Ann Med Health Sci Res. 2017;7:280–283.
24. Singh P, Kumar M, Al Khodor S. Vitamin D deficiency in the gulf cooperation council: exploring the triad of genetic predisposition, the gut microbiome and the immune system. Front Immunol. 2019;10:1042. doi:10.3389/fimmu.2019.01042
25. Al-Daghri NM, Abd-Alrahman SH, Panigrahy A, et al. Efficacy of Vitamin D interventional strategies in Saudi children and adults. J Steroid Biochem Mol Biol. 2018;180:84–90.
26. Mukhopadhyay P, Ghosh S, Bhattacharjee K, Chowdhury S. Inverse relationship between 25 hydroxy vitamin d and parathormone: are there two inflection points? Indian J Endocrinol Metab. 2019;23(4):422–427. doi:10.4103/ijem.IJEM_322_19
27. Hussein D, Ahmed G, Ahmed S, et al. Pattern of vitamin D deficiency in a Middle Eastern population: a cross-sectional study. Int J Funct Nutr. 2022;3:30. doi:10.3892/ijfn.2022.30
28. Sampat N, Al-Balushi B, Al-Subhi L, Al-Adawi S, Essa MM, Qoronfleh MW. Vitamin D: public health status, regional gulf region. Int J Nutr Pharmacol Neurol Dis. 2019;9(4):117–135.
29. Adebayo FA, Itkonen ST, Öhman T, Kiely M, Cashman KD, Lamberg-Allardt C. Safety of vitamin d food fortification and supplementation: evidence from randomized controlled trials and observational studies. Foods. 2021;10:3065. doi:10.3390/foods10123065
30. Von Heimburg P, Baber R, Willenberg A, et al. Effect of sex, pubertal stage, body mass index, oral contraceptive use, and C-reactive protein on vitamin D binding protein reference values. Front Endocrinol. 2025;16. doi:10.3389/fendo.2025.1470513
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical and Prognostic Significance of Baseline Serum Vitamin D Levels in Hospitalized Egyptian Covid-19 Patients
Mostafa S, Mohammed SA, Elshennawy SI, Zakaria DM, Mahmoud SAK, Alsadek AM, Ahmad IH, Mohammed DS, Mohammed MA, Eltrawy HH
International Journal of General Medicine 2022, 15:8063-8070
Published Date: 7 November 2022
Serum Vitamin D and Vaspin Levels Among Patients with Acute Myocardial Infarction and Their Association with Risk Factors
Baig M, Alghalayini KW, Gazzaz ZJ, Murad MA
International Journal of General Medicine 2024, 17:2907-2917
Published Date: 2 July 2024
Serum Vitamin D Profiles of Children with Asthma in Southwest Saudi: A Comparative Cross-Sectional Study
Asseri AA
International Journal of General Medicine 2024, 17:6323-6333
Published Date: 17 December 2024
A Multidisciplinary Expert Consensus on Vitamin D Deficiency Diagnosis and Management in Saudi Arabia: Insights from a Modified Delphi Process
Arab HA, Amir AA, Alotaibi M, Aljassir FF, Gazar YAE, Alshehri AA, Al Dalbhi S, Alsifri S, Alotaibi GS, Altwaim A, Mitwally N, Alomair M
Nutrition and Dietary Supplements 2026, 18:602745
Published Date: 26 June 2026