Back to Journals » Nutrition and Dietary Supplements » Volume 18
A Multidisciplinary Expert Consensus on Vitamin D Deficiency Diagnosis and Management in Saudi Arabia: Insights from a Modified Delphi Process
Authors Arab HA ![]() , Amir AA, Alotaibi M, Aljassir FF, Gazar YAE, Alshehri AA, Al Dalbhi S, Alsifri S, Alotaibi GS, Altwaim A
, Amir AA, Alotaibi M, Aljassir FF, Gazar YAE, Alshehri AA, Al Dalbhi S, Alsifri S, Alotaibi GS, Altwaim A ![]() , Mitwally N, Alomair M
, Mitwally N, Alomair M
Received 11 February 2026
Accepted for publication 19 June 2026
Published 26 June 2026 Volume 2026:18 602745
DOI https://doi.org/10.2147/NDS.S602745
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Ara Kirakosyan
Hisham A Arab,1 Ashraf A Amir,2 Metib Alotaibi,3 Fawzi Fahad Aljassir,4 Yasser A Elmotaleb Gazar,5,6 Ali A Alshehri,7 Sultan Al Dalbhi,8 Saud Alsifri,9 Ghazi S Alotaibi,10 Abdulaziz Altwaim,11– 14 Noha Mitwally,15 Mohammed Alomair16
1Maternal & Fetal Health Program, Dr. Arab Medical Center, Jeddah, Saudi Arabia; 2Family Medicine, Group CMO, International Medical Center, Jeddah, Saudi Arabia; 3University Diabetes Center, King Saud University Medical City, King Saud University, Riyadh, Saudi Arabia; 4Department of Orthopedic Surgery, College of Medicine, King Saud University, Riyadh, Saudi Arabia; 5Rheumatology and Rehabilitation, Al-Azhar University, Cairo, Egypt; 6Rheumatology, Madinah National Hospital, Madinah, Saudi Arabia; 7Obesity Endocrine & Metabolism Center, King Fahad Medical City, Riyadh, Saudi Arabia; 8Nephrology and Kidney Transplantation, Organs Repair and Transplantation Center of Excellence (Ortcoe), Riyadh, Saudi Arabia; 9Endocrinology Department, Alhada Armed Forces Hospital, Taif, Saudi Arabia; 10Oncology Center, Department of Medicine, College of Medicine, King Saud University, Riyadh, Saudi Arabia; 11King Saud bin Abdulaziz University for Health Sciences (KSAU-HS), Riyadh, Saudi Arabia; 12Pediatric Endocrinology, Diabetes Care Center, Jeddah, Saudi Arabia; 13Pediatric Endocrinology, Saudi German Hospital, Jeddah, Saudi Arabia; 14Saudi Pediatric Association, Department of Pediatrics, the College of Medicine, King Saud University, Riyadh, Saudi Arabia; 15Biochemistry Department, Faculty of Pharmacy, Cairo University, Cairo, Egypt; 16Academic Affairs and Research Center and Medicine Departments, Aseer Central Hospital (ACH), Abha, Saudi Arabia
Correspondence: Hisham A Arab, Email [email protected]
Background: Vitamin D is essential for skeletal health and has been increasingly recognized for potential extra-skeletal benefits. Despite this, vitamin D deficiency remains prevalent, with corrective efforts focused on skeletal outcomes, whereas extra-skeletal benefits remain controversial due to conflicting evidence between small-scale studies and randomized control trials (RCTs). Furthermore, region-specific challenges are a barrier to first-line corrective strategies.
Aim: This is the first Saudi-specific Delphi consensus, aiming to address skeletal and extra-skeletal outcomes, drive actionable corrective strategies, and encourage large-scale research in the Kingdom of Saudi Arabia (KSA).
Methods: Eleven multidisciplinary key opinion leaders from KSA participated in a modified Delphi process involving a premeeting survey, two in-person meetings, and three iterative survey rounds. Consensus, predefined as ≥ 75% agreement consistent with established Delphi thresholds, was achieved across all 38 statements, covering the landscape of vitamin D deficiency, strategies for correction, maintenance, monitoring, and safety considerations.
Results: Key consensus-based recommendations included: (i) vitamin D deficiency contributes to disease development, while correction could help improve outcomes; (ii) oral supplementation is the primary corrective strategy in the Saudi context; (iii) screening should be limited to patients in whom deficiency impacts disease or treatment, with empiric supplementation preferred otherwise; (iv) dosing regimens of 50,000 IU weekly for deficient or empirically treated patients and 1,000– 2,000 IU daily or 50,000 IU monthly for sufficient patients and the general population; (v) conditions associated with reduced response to standard dosing are eligible for higher dose; (vi) indefinite maintenance with monitoring every 3– 6 months for screened patients; (vii) expert-informed target serum 25-hydroxyvitamin D (25(OH)D) concentrations of ≥ 30 ng/mL for the general population, ≥ 50–< 60 ng/mL for the elderly, and ≥ 70 ng/mL for patients with comorbidities. The recommendations for broad empiric supplementation, indefinite maintenance, and the ≥ 70 ng/mL target diverge from current international guidance and rest on expert consensus and limited evidence; they require prospective regional validation and should be applied with appropriate caution and safety monitoring.
Conclusion: This framework provides the first Saudi-specific, Delphi-based recommendations for managing vitamin D deficiency, addressing both skeletal and extra-skeletal outcomes, and providing context for future research efforts.
Keywords: vitamin D, deficiency, Saudi Arabia, delphi consensus, supplementation, guidelines, endocrinology
Background
Globally, vitamin D deficiency is recognized as a significant public health problem. A meta-analysis reported that 76.6% of the world’s population has 25(OH)D concentrations below the sufficiency threshold of 30 ng/mL.1 The significance of this prevalence is better understood by examining vitamin D as an essential micronutrient. Vitamin D is metabolized in the liver into 25-hydroxyvitamin D (25(OH)D), transforming into 1,25-dihydroxyvitamin D (1,25(OH)2D) in the kidneys and other extra-renal tissues, exerting endocrine, autocrine, and paracrine effects.2 The causal role of vitamin D and its metabolites in musculoskeletal health is well established, as adequate concentrations prevent and treat metabolic bone disorders, whereas deficiency contributes to their development.3 Beyond their skeletal role, the expression of vitamin D receptors and metabolites in virtually all human cells suggests potential extra-skeletal functions. This activity includes regulation of cell proliferation, immune responses, skin differentiation, reproduction, as well as vascular and metabolic processes.3,4 This biological activity renewed interest in vitamin D. However, despite supportive observational data, large-scale randomized clinical trials (RCTs) have not confirmed causal relationships for extra-skeletal outcomes, leaving this role controversial.3,5
In the Kingdom of Saudi Arabia (KSA), vitamin D deficiency remains paradoxically prevalent despite year-round abundant sunlight, with recent cross-sectional studies reporting deficiency in 67.3% and 78.7% of the population.6,7 The lack of meaningful seasonal variation in deficiency rates further emphasizes this paradox.6 Several region-specific factors contribute to the high deficiency rates. Modest cultural clothing practices and deliberate avoidance of direct sunlight due to extreme heat substantially limit effective sun exposure. The predominantly darker skin pigmentation of the Saudi population also reduces cutaneous vitamin D synthesis from sun exposure. Dietary patterns also contribute to vitamin D deficiency, since vitamin D-rich food sources are limited in the typical Saudi diet, and systematic food fortification strategies remain insufficient. Collectively, these factors indicate that reliance on sunlight exposure alone is inadequate for ensuring sufficient 25(OH)D concentrations in this population, underscoring the need for structured supplementation strategies tailored to the regional context.6,8–10
Despite the widespread deficiency, most strategies addressing vitamin D insufficiency have primarily focused on musculoskeletal outcomes, often overshadowing potential extra-skeletal benefits as well as regional contexts.5,6,10 Within the KSA context, Al-Daghri et al10 established foundational thresholds for the diagnosis and correction of vitamin D deficiency in the KSA population under the auspices of the European Society for Clinical and Economic Aspects of Osteoporosis, Osteoarthritis and Musculoskeletal Diseases (ESCEO) in 2017. However, despite previous conclusions also by Al-Daghri et al11,12 that vitamin D status correction conferred metabolic benefit in diabetic Saudi patients, they opted to focus their recommendations on skeletal outcomes in the general and high-risk populations, featuring no special consideration for patients with metabolic diseases until further evidence emerged. Furthermore, the supplementation and dosing recommendations did not systematically incorporate the regional contextual barriers described above. Therefore, and in light of the growing body of observational and small-scale evidence in the vitamin D space focusing on the potential extra-skeletal benefits and the adoption of high-dose supplementation strategies, an expert panel advanced the foundational work of Al-Daghri et al10 by considering both skeletal and extra-skeletal outcomes and including multidisciplinary expertise rather than focusing on endocrinology only. This framework primarily aims to provide a structured, expert-informed approach tailored to the regional cultural and clinical context, including the insurance-based healthcare system that governs screening access. It confirms established recommendations where evidence is strong and extends consensus-based guidance to extra-skeletal management where the evidence base continues to evolve. In doing so, it aims to catalyze the regional large-scale prospective studies needed to confirm its clinical utility and strengthen the evidence base for vitamin D management in KSA.
Methods
Study Design
We conducted a modified Delphi consensus to develop expert recommendations on the management pathways for vitamin D deficiency, treatment goals, and dosing schedules tailored to the Saudi population. The process followed established guidance for Delphi studies in healthcare (CREDES).13
The Delphi approach is a systematic method for consensus development among a group of experts on a specific issue through anonymity, iterative rounds, and controlled feedback.13–15 Consensus was defined a priori as ≥75% agreement, consistent with established Delphi methodology thresholds to reflect the participants’ collective expertise.
The process spanned three and a half months (April 25th–August 9th, 2025), combining a pre-meeting survey, two in-person meetings, and three survey rounds. Anonymity of voting was ensured during group discussions by sharing controlled and depersonalized feedback of the answers and comments to the survey questions. Online surveys were administered using Google Forms® (Google LLC, Mountain View, CA, USA). Responses were collected anonymously. Data were exported into Microsoft Excel (Microsoft Corp., Redmond, WA, USA) for controlled feedback and summary statistics.
The work on this consensus document was funded by Jamjoom Pharma (Saudi Arabia). To protect the scientific independence of the panel, the sponsor provided financial and logistical support only; having no role or access to selecting the panelists, formulating or wording the statements, conducting or tabulating the votes, interpreting the results, or drafting the manuscript. No employee or representative of the sponsor is an author of this manuscript or reviewed the manuscript prior to submission. Administration of the Delphi process, including coordination of the in-person meetings, distribution of the surveys, and confidential collection and aggregation of votes, was facilitated by Noha Mitwally (N. M)., who was not a member of the voting clinical panel and who did not propose, draft, or vote on any clinical statement. The clinical statements were developed, deliberated, and voted upon solely by the eleven multidisciplinary panelists. Medical writing and editorial assistance were provided by an independent medical writer, funded by the sponsor; the writer did not influence statement development, voting, or data interpretation. All authors reviewed and approved the final manuscript, and take full responsibility for its content and for the decision to submit it for publication. All panelists received honoraria for their participation. N. M. also received an honorarium for methodological support.
Participants
Eleven multidisciplinary Saudi key opinion leaders with expertise in vitamin D and related topics were invited to participate in the modified Delphi Process. The panel comprised four endocrinologists, two rheumatologists, one orthopedic surgeon, one oncologist, one gynecologist, one nephrologist, and one family medicine specialist. Expert selection criteria included geographical distribution, healthcare sector, and specialty. The selected panel included experts representative of different geographical distributions, healthcare sectors, and specialties, with demonstrable clinical expertise in vitamin D deficiency management and commitment to standardizing its management in KSA, evidenced by their publication record, clinical practice, and/or active contribution to vitamin D-related initiatives in KSA. All participants completed the three survey rounds.
Modified Delphi Process
The process began on April 25th with a pre-meeting survey that gathered expert perspectives on the current vitamin D deficiency landscape and management strategies in KSA. In parallel, a literature search was conducted on topics of “vitamin D deficiency prevalence”, “skeletal benefits of vitamin D”, “extra-skeletal benefits of vitamin D”, “vitamin D deficiency management strategies in KSA”, and “vitamin D dosing strategies”. In the first in-person meeting, held on May 2nd, survey responses and the resulting data from the literature search were discussed through open-ended questions. Discussions focused on three main themes: assessing the prevalence of vitamin D deficiency in KSA; evaluating its impact beyond skeletal conditions; and advising strategies for its management. The resulting discussion and answers to the open-ended questions were used to formulate the first survey questions.
The first survey, after an initial pilot testing, was launched on July 9th and included 38 questions (13 multiple-choice, 23 yes/no, and two open-ended), each with space for optional comments. In this round, consensus was achieved for 25 statements. Findings were summarized and reported back to the panel prior to the second survey.
The second survey, launched on July 20th, included 23 yes/no questions derived from 13 non-consensus statements reformulated for clarity: the two top-ranking answers to multiple-choice questions were reformulated in two yes/no questions, the top-ranking answer to yes/no questions were reformulated in one yes/no question, and the most repeated answer to open-ended questions was reformulated in one yes/no question. In this round, consensus was reached for four statements.
The second in-person meeting, held on August 8th, was dedicated to validating and refining consensus statements as well as discussing and making amendments to the remaining nine non-consensus items. The discussed non-consensus items pertained to dosing, maintenance, and target concentrations. The structured discussion aimed to resolve residual disagreement by balancing the recommendations in accordance with the prevalent vitamin D deficiency, limited access to screening, and the differing needs of 25(OH)D concentrations among vulnerable and general populations. Following this discussion, a subset of these statements was amended before re-voting, while others were maintained. On August 9th, the third and final survey was conducted owing to scheduling constraints at the panel’s request. To preserve the independence and confidentiality of the final vote despite its proximity to the group discussion, votes were collected through separate, individual one-to-one sessions between N. M., the non-voting author and methodologist, and each panelist. Panelists remained blinded to one another’s individual responses throughout, and the methodologist recorded each vote confidentially and reported only deidentified, aggregate results. The convergence to consensus in this round reflects the resolution of residual disagreement through structured, face-to-face deliberation. We nonetheless acknowledge that the influence of the preceding group discussion on individual deliberation cannot be entirely excluded, and we address this explicitly in the Limitations. Consensus was reached for the remaining statements.
The survey questions and anonymous responses are detailed in the Supplementary Materials.
Results
Current Landscape of Vitamin D Deficiency in KSA
Vitamin D deficiency is prevalent across all age groups and therapy areas (11/11; 100%), representing 50–100% of seven panel members’ caseload in routine clinical practice, according to the pre-meeting survey. Additionally, a notably high prevalence is observed among females of childbearing age (10/11; 91%). Furthermore, vitamin D deficiency is a contributing factor in the development of numerous skeletal and extra-skeletal conditions, and based on the panel’s clinical experience and observational evidence, the correction of which is associated with observed improvements in patients’ comorbid conditions (11/11; 100%). Examples mentioned by the panel of such improvements included metabolic bone diseases (eg, osteopenia), autoimmune diseases (especially, systemic lupus erythematosus, ankylosing spondylitis, fibromyalgia), depression, hypothyroidism, polycystic ovary syndrome, diabetes mellitus, pre-eclampsia, and statin-induced myopathy However, the panel acknowledged that the extent of vitamin D’s extra-skeletal impact is not yet fully understood.
Table 1 summarizes the consensus statements on the current landscape of vitamin D deficiency in KSA.
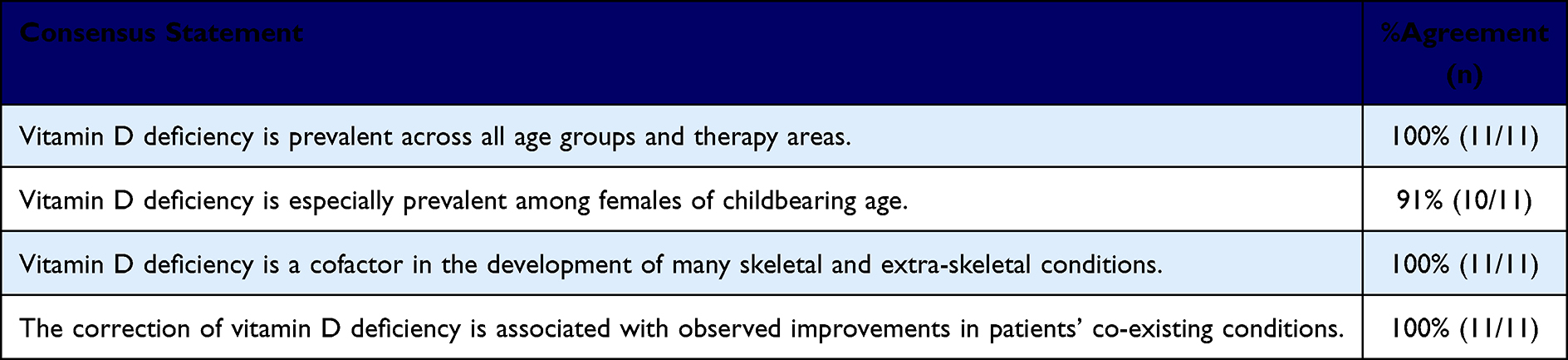 |
Table 1 Consensus Statements on the Current Landscape of Vitamin D Deficiency in KSA |
KSA-Specific Strategies for Vitamin D Correction
Current food fortification efforts in KSA are insufficient to address the widespread prevalence of vitamin D deficiency (11/11; 100%). In addition, intense daytime heat limits sun exposure as the main source of vitamin D (10/11; 91%). This limitation is further compounded by traditionally modest clothing among the Saudi population, which reduces the proportion of body surface area exposed to sunlight, and their darker skin tone, which reduces the amount of vitamin D synthesized by ultraviolet B (UVB) exposure. Sun exposure is also a risk factor for skin cancer and may exacerbate certain autoimmune disorders. Collectively, these factors were identified as key factors necessitating supplementation to achieve adequate vitamin D status among the Saudi population. According to the pre-meeting survey, 81% of panel members routinely prescribe cholecalciferol (vitamin D3) over ergocalciferol (vitamin D2), which they attributed to cholecalciferol’s affordability, wider availability, and higher potency.
Although serum 25(OH)D concentration is the only objective indicator that should inform vitamin D supplementation,16 the panel agreed that nationwide screening strategies were deemed inapplicable due to the lack of supporting cost-effectiveness data (10/11; 91%), and insurance companies often reject screening coverage, including alternative methods such as the rapid quantitative immunoassay, since they are considered unreliable. Therefore, the panel agreed that screening should be reserved for certain patient profiles before the prescription of supplementation (10/11; 91%; Figure 1). The importance of unifying the assay method for 25(OH)D was especially emphasized in order to accurately identify deficient patients without false over- or underestimation (10/11; 91%).
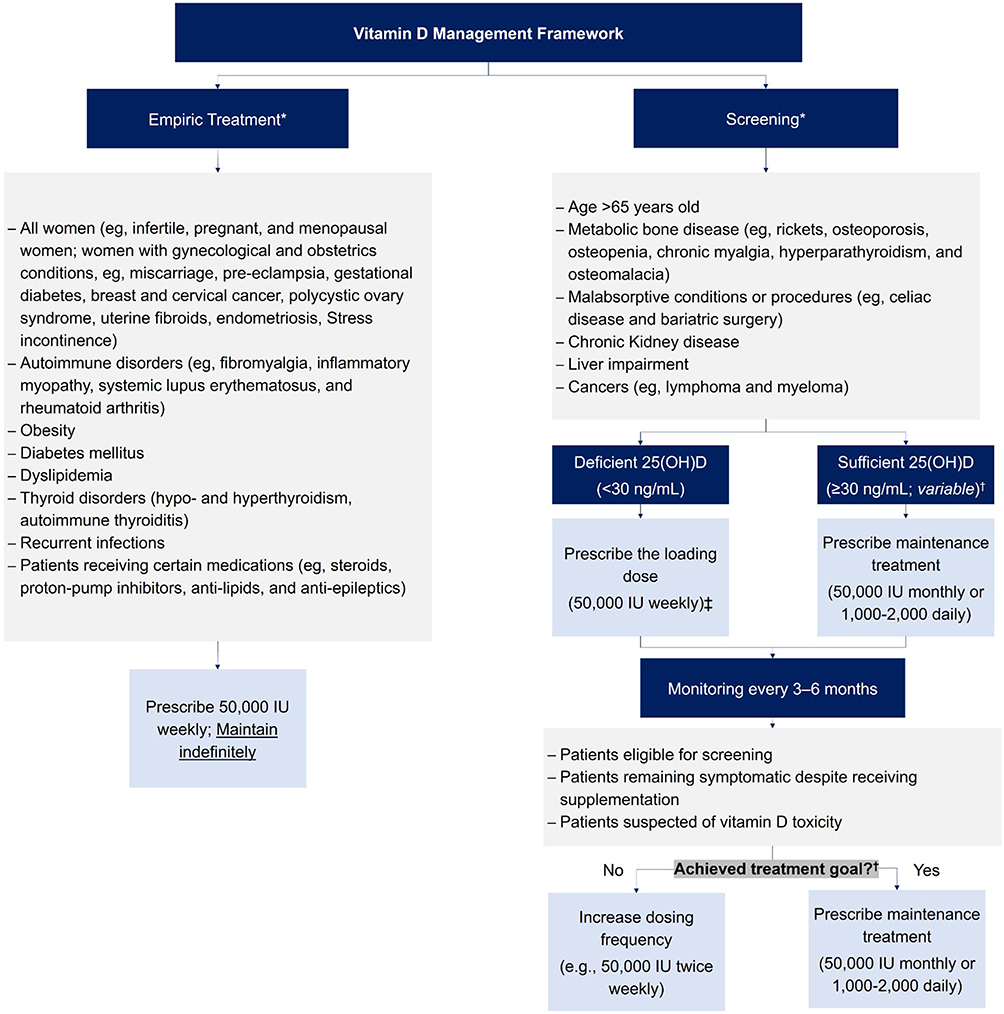 |
Figure 1 Vitamin D Management Framework*†‡. These lists are not exhaustive, but represent the most commonly encountered conditions in KSA. Non-mentioned conditions are screened or empirically treated upon the recommendations of the treating physician. †Treatment goal of serum 25(OH)D concentrations differs according to patients’ age, gender, and comorbid conditions. See Table 3. ‡Higher dosage could be recommended according to the discretion of the treating physician. See Tables 2 and 3 for recommendations regarding high-dose vitamin D supplementations. |
In this regard, screened patients with deficient serum 25(OH)D concentrations (<30 ng/mL) are advised to receive a loading vitamin D dose of 50,000 IU weekly (10/11; 91%). On the other hand, healthy adults and patients with comorbid conditions who have sufficient serum 25(OH)D concentrations (≥30 ng/mL) are advised to receive a maintenance dose of 1,000–2,000 IU daily (10/11; 91%) or 50,000 IU monthly (11/11; 100%). The choice between dosing schedules should factor in patient preference to enhance treatment adherence (10/11; 91%), noting that intermittent dosing is often preferred over daily dosing (11/11; 100%). Of note, insufficient serum 25(OH)D concentrations (≥20–<30 ng/mL) were not considered by the panel when deliberating the dosing regimens, in line with their objectives of achieving serum 25(OH)D concentrations ≥30 ng/mL in KSA.
Alternative to screening, empiric supplementation (9/11; 82%) was identified as the preferred approach. As such, specific patient populations are advised for empiric supplementation (Figure 1). These patients are advised to receive 50,000 IU weekly (9/11; 82%).
Specific patient populations are advised to receive a higher loading dose of supplementation than 50,000 IU weekly, such as patients with malabsorptive conditions (11/11;100%).
Table 2 summarizes the consensus statements on KSA-specific Strategies for Vitamin D Correction.
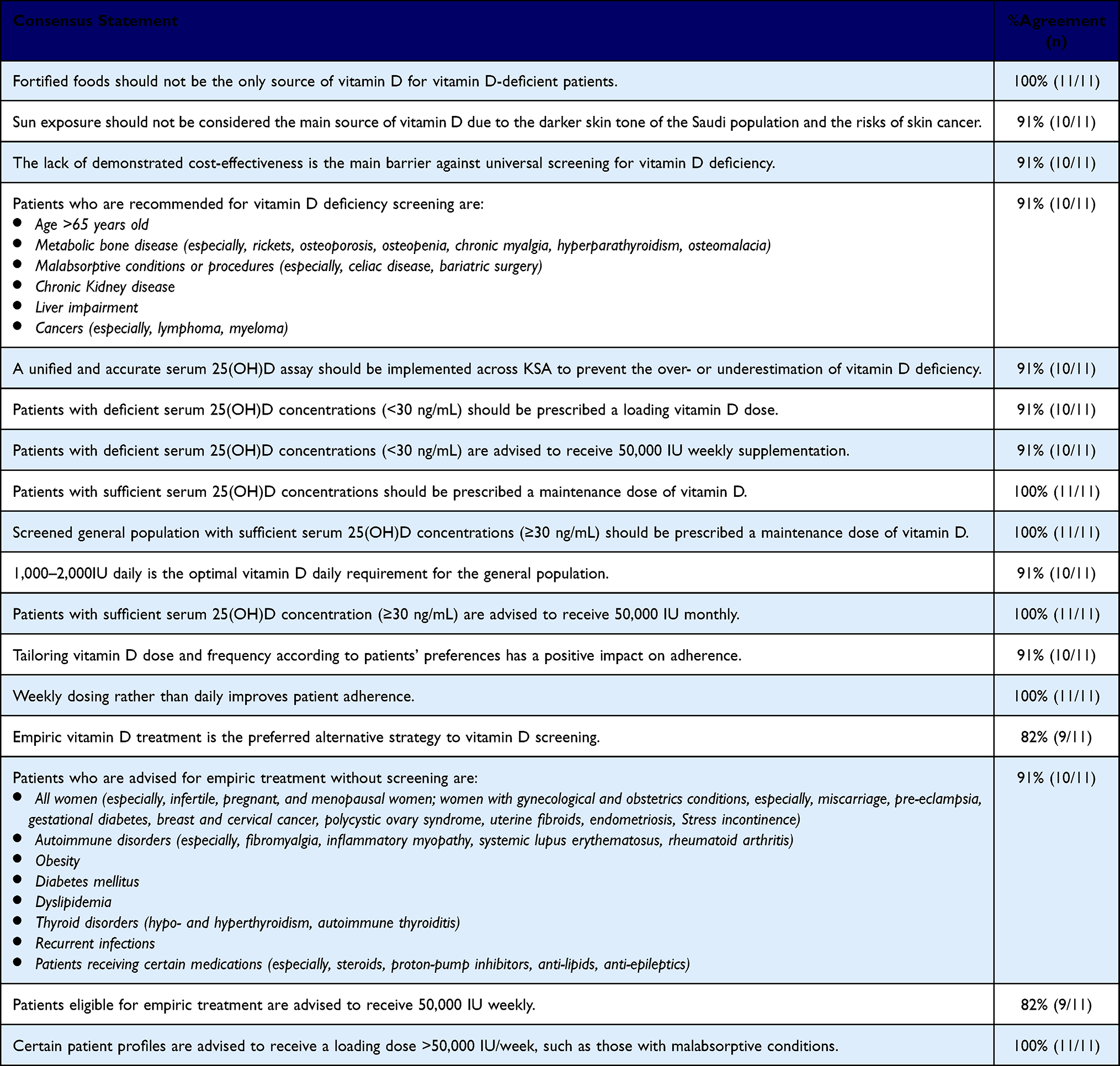 |
Table 2 Consensus Statements on KSA-Specific Strategies for Vitamin D Correction |
Maintaining Sufficient Vitamin D Concentrations
Regardless of the supplementation strategy, vitamin D treatment should be maintained rather than discontinued (10/11; 91%). This was attributed to the inevitable decline of 25(OH)D within months of discontinuation, which led to the emphasis that vitamin D deficiency should be recognized as a chronic condition so that healthcare providers are encouraged to effectively manage it as one.
To objectively assess patients’ maintenance regimen, patients eligible for screening, in addition to those who received supplementation yet remain symptomatic (10/11; 91%), are recommended for treatment monitoring every 3–6 months, wherein patients who achieved their recommended treatment goal are prescribed maintenance treatment (11/11; 100%). On the other hand, patients who failed to achieve their treatment goal are prescribed their previous dose on a more frequent dosing schedule (9/11; 82%). Empirically treated patients are recommended to maintain indefinite vitamin D supplementation at 50,000 IU weekly. The panel recognized that its endorsement of indefinite maintenance is consensus-based, reflecting regional barriers to laboratory testing and the chronic, recurring nature of deficiency in this setting, rather than high-level randomized trial evidence. Accordingly, the empiric and indefinite-supplementation pathways described here are intended for the high-risk and symptomatic populations, and should be applied with clinical judgement and safety monitoring detailed in Vitamin D Safety when applicable. Furthermore, patients who were prescribed high-dose vitamin D (>50,000 IU weekly) are also recommended to test for bone profile and renal function alongside serum 25(OH)D (10/11; 91%). This patient group is advised to receive a maintenance dose of 50,000 IU weekly or higher (twice weekly or even daily) according to the discretion and close monitoring of their treating physician, which should account for each patient’s serum 25(OH)D concentration, comorbid conditions, and overall health status (11/11; 100%) to avoid any detrimental effects of high-dose supplementation.
The goal of supplementation should be tailored according to patients’ age, gender, and comorbid conditions (11/11; 100%). From this perspective, a serum 25(OH)D concentration ≥30 ng/mL is sufficient for the general population (11/11; 100%), whereas patients older than 65 years should be maintained at ≥50 ng/mL (11/11; 100%). However, exceeding the 60 ng/mL threshold was advised against, since it is associated with an increased risk of falls among this patient population. Furthermore, patients with comorbid conditions should be maintained at ≥70 ng/mL unless otherwise contraindicated (11/11; 100%). Nevertheless, the panel acknowledged that this target serum concentration is a consensus-based position, not an evidence-based threshold. The panel therefore advances this target as a hypothesis requiring prospective validation in the Saudi comorbid population, to be applied only with careful patient selection, attention to total cumulative dose, and the biochemical safety monitoring described in Vitamin D Safety, rather than as an established standard of care.
Table 3 summarizes the consensus statements on the maintenance of sufficient vitamin D concentrations.
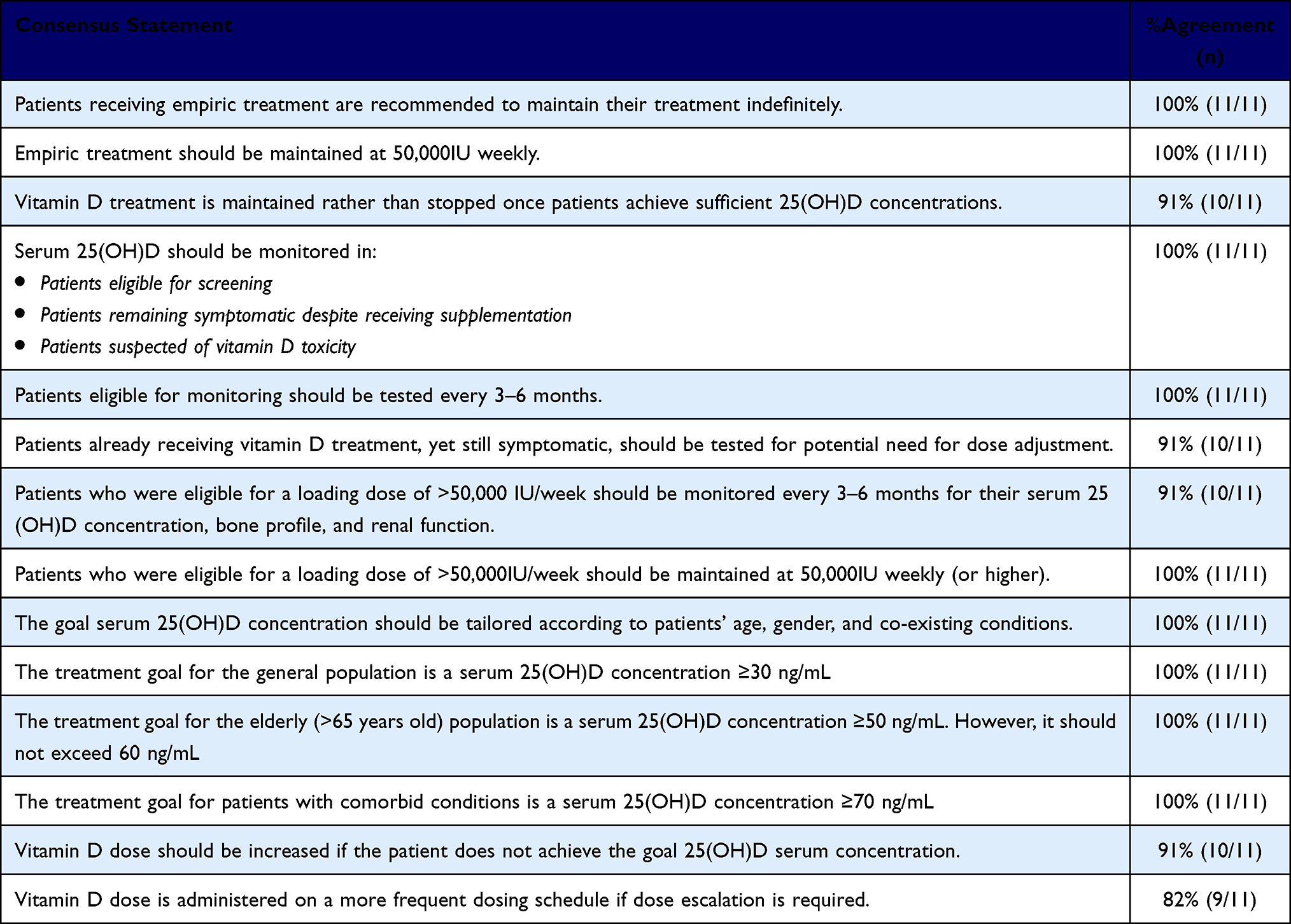 |
Table 3 Consensus Statements on the Maintenance of Sufficient Vitamin D Concentrations |
Vitamin D Safety
The panel agreed that vitamin D is safe at high doses, with only a rare occurrence of toxicity (11/11; 100%). However, 5,000 IU is the currently recommended maximum daily dose for the general population until further research supports the widespread use of higher doses, such as 10,000 IU (11/11; 100%).
Suspicion of vitamin D toxicity should not be defined solely by high serum 25(OH)D concentrations. Instead, it should be labeled when hypercalciuria and hypercalcemia, very low or undetectable parathyroid hormone activity, and hyperphosphatemia are also detected (10/11; 91%).
Table 4 summarizes the consensus statements on the safety of vitamin D supplementation.
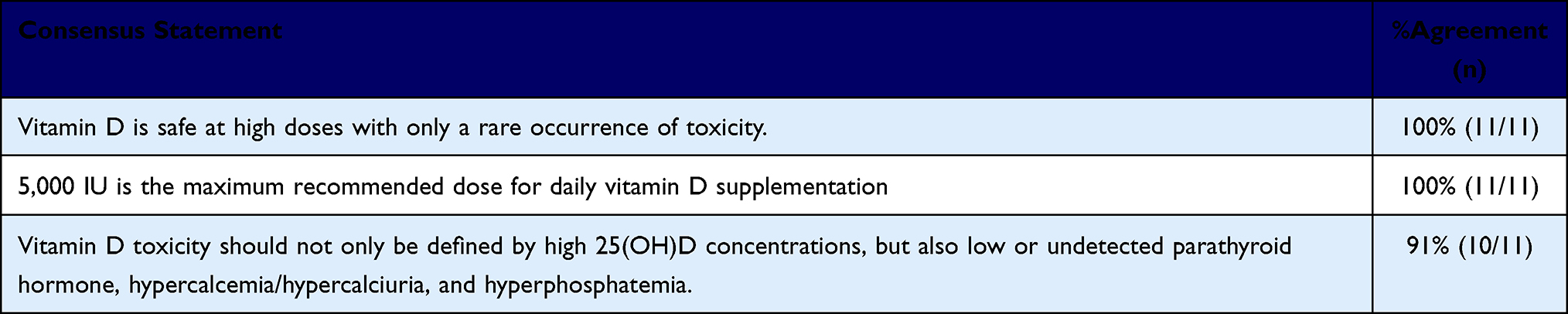 |
Table 4 Consensus Statements on the Safety Considerations for Vitamin D Supplementation |
Discussion
Our panel agreed on the high prevalence of vitamin D deficiency in KSA, reporting a disproportionate prevalence among females. This was consistently observed across all therapeutic areas involved, in which vitamin D deficiency and its correction were agreed to influence aspects of disease course or response to treatment.
This observed high prevalence aligns with recent epidemiological research in KSA, which reported a consistently higher prevalence among females compared to males, especially those aged 10–19 and 20–29 years.6 Furthermore, vitamin D deficiency was linked to the incidence and progression of multiple diseases outside the scope of skeletal health, which has already been repeatedly reported.4 For example, studies linked vitamin D deficiency to cancer incidence or its associated morbidity.17,18 However, the VITAL study found no significant benefit of supplementation in reducing the incidence of invasive cancer or major cardiovascular events. Nevertheless, in a secondary analysis, supplementation significantly reduced total cancer mortality, excluding early follow-up. Interestingly, supplementation conferred a benefit in cancer incidence among black participants in the VITAL trials,19 suggesting an interplay of ethnicity in vitamin D requirements and benefit.19 An earlier meta-analysis of RCTs also reported little effect on cancer incidence with supplementation, but a significant reduction in total cancer mortality.20 In the autoimmune disease space, Lombardo et al21 linked vitamin D deficiency to diffuse muscle pain associated with autoimmune diseases, such as fibromyalgia, linking its correction to the alleviation of this pain. Furthermore, an ancillary study of the VITAL study reported a reduced incidence of autoimmune disease by 22% with 5-year supplementation.22 A sub-cohort from this study also linked supplementation to modulating the chronic inflammatory processes involved in autoimmune diseases.23 Similarly, a systematic review by Galușca et al24 demonstrated that vitamin D deficiency was linked to numerous endocrine diseases, including hyper- and hypothyroidism and diabetes mellitus, and its correction was associated with improvement of key parameters in each of these diseases, such as hemoglobin A1C (HbA1C), homeostatic model assessment of insulin resistance (HOMA-IR), and thyroid-stimulating hormone (TSH).24 A regional prospective study also demonstrated a significant improvement in high-density lipoprotein/low-density lipoprotein (HDL/LDL) ratio, and HOMA-β function in patients with type 2 diabetes mellitus receiving oral Vitamin D3 supplementation, which was more pronounced among females. This benefit was observed after 6 months of supplementation, suggesting that sustained and prolonged supplementation might be necessary to achieve desirable metabolic effects.11 However, this remains an area of uncertainty and undefined causality, since large RCTs failed to establish such links in their cohorts.25
In light of conflicting evidence, we aimed to provide a framework for vitamin D supplementation to pursue potential extra-skeletal benefits to encourage regional evidence generation and implementation, especially considering the aforementioned regional benefit as well as the suggested implication of darker skin tone on vitamin D effects. The favorable safety profile of vitamin D provides additional assurance that these additional benefits can be pursued safely with the described monitoring.
From this perspective, our panel examined feasible strategies for correcting vitamin D deficiency in the Saudi population. Sun exposure is the source of 90% of vitamin D synthesis.8 Al-Daghri et al10 provided recommendations for sun exposure specific to KSA, incorporating sun exposure as a primary corrective strategy in the general population.10 However, vitamin D from sun exposure remains offset by the darker skin pigmentation of the Saudi population, limiting the amount of synthesized vitamin D, which necessitates a longer duration of sun exposure.9 This is further offset by the traditionally modest clothing that limits the recommended body surface area exposed.8,9 These factors would potentially compromise the fine balance of UVB radiation exposure essential in attaining vitamin D while avoiding the induction of skin carcinogenesis and inflammatory processes.26
Alternative to sun exposure, food fortification is considered safe and effective in addressing vitamin D deficiency. It is also a cost-effective alternative to oral supplementation.8 However, Alnafisah et al8 concluded the need for strategized efforts in order to optimally implement the proposed food fortification initiative in KSA, rendering it currently insufficient to address the wide prevalence of vitamin D deficiency.
These factors―supported by Joh et al’s27 demonstrated consistently superior efficacy of oral supplementation in achieving serum 25(OH)D sufficiency compared to sun exposure―further supported our recommendation of oral supplementation as the main source for vitamin D correction in KSA. A majority recommendation of vitamin D3 supplementation is grounded in two meta-analyses concluding that vitamin D3 leads to a greater increase of 25(OH)D compared with vitamin D2.28,29 Furthermore, a pharmacokinetic study demonstrated that, despite the two formulations having similar impact on 25(OH)D, vitamin D3 sustained adequate 25(OH)D concentration and delayed its decline.30 Of note, we did not discuss calcifediol during this Delphi process.
Typically, supplementation is guided by serum 25(OH)D concentration, as it is the most reliable indicator of vitamin D storage in the body.16 However, Aguiar et al31 concluded that nationwide screening is infeasible and is outweighed by empiric treatment from a cost-effectiveness standpoint.20 These findings, coupled with the insurance-led healthcare system in KSA, result in the frequent rejection of covering serum 25(OH)D testing. Therefore, our panel recommended screening high-risk populations whose serum 25(OH)D concentrations would influence their treatment or disease course, but empirically treating symptomatic and high-risk populations in whom screening would not provide a cost-effective benefit.
Among our selected populations, the elderly population was recommended for treatment due to their compromised skeletal health,32 their increased risk of falls with high serum 25(OH)D concentrations exceeding 60 ng/mL,33 and the cost-effectiveness of their screening.8 Patients with metabolic bone disease require sufficient serum 25(OH)D concentrations before initiating their bone-specific treatment.34 Therefore, we agreed that an alternative decision of empiric treatment would unnecessarily delay their bone treatment. Furthermore, we also recommended screening for patients with malabsorptive conditions and procedures, chronic kidney diseases, and chronic liver disease, since they often require high-dose supplementation and frequent monitoring to prevent the incidence of avoidable metabolic bone diseases.35–37 Cancer patients are also recommended for screening in light of the aforementioned reduced mortality and associations with reduced incidence.17–20 Of note, the list of patient groups selected for either screening or empiric (Table 2 and Figure 1) treatment is not exhaustive, but rather based on the most frequently encountered groups by the panel members.
In our framework, patients with deficient serum 25(OH)D concentrations are advised a loading dose of 50,000 IU weekly, while those with sufficient serum concentrations are advised a maintenance dose of 1,000–2,000 IU daily, which largely aligns with the recommendations by Al-Daghri et al10 The maintenance dose could alternatively be administered as 50,000 IU monthly. Despite concerns that intermittent dosing may compromise the efficacy of supplementation, a network meta-analysis by Zhuang et al38 demonstrated the similar efficacy of both daily and intermittent (weekly or monthly) dosing schedules.38 Additionally, intermittent dosing schedules are considered more convenient,38 whereas daily dosing is associated with adherence challenges, as demonstrated in a cross-sectional electronic survey among 50 nursing homes in Denmark.39 Empirically treated patients, on the other hand, are advised to receive 50,000 IU weekly indefinitely. Our decision to recommend indefinite supplementation in this population stems from the decline in serum 25(OH)D concentrations after treatment discontinuation,30 which is further compounded by the regional reality of prevalent vitamin D deficiency without effective non-medicinal corrective strategies, placing supplementation as the primary vitamin D deficiency corrective strategy, as well as the frequent insurance rejection of serum 25(OH)D concentration testing. Importantly, our recommendation is based on the absence of toxicity in trials conducted in healthy adults at doses up to 10,000 IU daily, and is also supported by the safety demonstrated by Jetty et al, across 12 months of 50,000–100,000 IU weekly administration.40,41 However, we acknowledge that, though our clinical experience also demonstrates the safety of this regimen, this recommendation diverges from the general recommendations in the published literature for a time-limited 50,000 IU weekly dosing.42 Therefore, we advise caution when following this recommendation and encourage regional data generation in controlled clinical settings.
Certain conditions are associated with reduced efficacy and response to standard supplementation regimens due to increased vitamin D catabolism, including obesity, malabsorptive conditions and procedures, as well as renal and liver disease. Therefore, these patients often require high-dose regimens.19,35–37,43 These findings, supported by Ataide et al,44 who reported the efficacy and safety of mega-dose vitamin D, directed our recommendation that certain patient populations are eligible for a more intense vitamin D dosing Importantly, however, we recommended comprehensive screening and monitoring to avoid hypervitaminosis D.
Serum 25(OH)D concentration of ≥30 ng/mL is recognized in a review of guidelines across the world. However, to address most disorders, it is recommended to maintain serum 25(OH)D concentrations >50 ng/mL within the range of 40–80 ng/mL.43 Therefore, and consistently with Al-Daghri et al,10 we recommend a serum 25(OH)D concentration of ≥30 ng/mL as the treatment goal for the general population However, we diverge from Al-Daghri et al10 in our recommendations for the elderly as well as the comorbid populations, but remain within the recommended optimal range. In the elderly, we recommend a target serum 25(OH)D concentration at ≥50–<60 ng/mL, in accordance with the abovementioned risk of falls in this patient population.33 In the comorbid population, we considered target serum concentrations at ≥50 and ≥60 ng/mL during the initial two waves of the Delphi survey, but ultimately decided to pursue ≥70 ng/mL. Although this recommendation remains within the abovementioned optimized range, we acknowledge that this is based on limited clinical data and requires further research to confirm its clinical efficacy and safety in this patient population. Furthermore, we note that the Endocrine Society moved away from specifying numerical 25(OH)D thresholds in their most recent update, citing insufficient evidence to define precise cutoffs for sufficiency across populations.45 Therefore, we reiterate the need for large-scale trials confirming these thresholds in our population.
Vitamin D is repeatedly reported to be safe across varying dosing regimens.4,5,44,46 In fact, research has reported that high serum 25(OH)D concentrations are safe without impacting calcium or parathyroid hormone concentrations.46 Therefore, we recommend against labeling vitamin D toxicity solely based on high serum 25(OH)D concentrations. Instead, we recommend labeling toxicity based on the metabolic effects of excessive vitamin D, manifesting as hypercalciuria and hypercalcemia, very low or undetectable parathyroid hormone activity, and hyperphosphatemia, as demonstrated across the literature.47–49
Overall, our framework spans skeletal and extra-skeletal aspects of vitamin D supplementation. However, we expect challenges with its implementation with respect to the extra-skeletal and high-dose recommendations, considering the limited supporting evidence. Therefore, we recommend initial implementation under structured clinical studies to confirm the efficacy and safety in the Saudi population and make refinements to the framework where needed before proceeding with nationwide implementation.
Our framework should be read as an extension of, rather than a replacement for, the 2017 ESCEO-endorsed Saudi consensus by Al-Daghri et al10 We concur with and reaffirm their foundational positions on the high regional prevalence of deficiency, the value of correcting deficiency for skeletal health, and a general-population sufficiency target of ≥30 ng/mL. The present consensus is distinct in four respects. First, it is grounded in a multidisciplinary panel, spanning rheumatology, orthopedics, oncology, nephrology, gynecology, and family medicine in addition to endocrinology, rather than a predominantly endocrinology-focused one, broadening the clinical perspectives applied to each statement. Second, it offers consensus-based guidance on the management of patients with comorbidities and on extra-skeletal considerations, an area the 2017 consensus deliberately deferred pending further evidence. Third, it examined the regional realities, and consequently positioned supplementation as the primary corrective strategy for vitamin D deficiency. In addition, it proposes a pragmatic screening-versus-empiric-treatment pathway tailored to the insurance-based reimbursement environment that constrains access to 25(OH)D testing in KSA, a contextual barrier not addressed in the earlier document. Fourth, it specifies population-specific target serum concentrations for the elderly (≥50–<60 ng/mL) and for patients with comorbidities (≥70 ng/mL). We explicitly diverge from Al-Daghri et al10 in these latter targets and in recommending indefinite empiric supplementation; consistent with the framing above, these specific additions rest on expert consensus and limited evidence and are offered as hypotheses for regional validation rather than as established, evidence-based standards. The intended contribution of this work is thus to update and broaden the regional guidance first established in 2017, within a structured Delphi consensus framework.
This Delphi study resulted in the development of a practical framework that translates expert consensus into clear, region-specific recommendations for the management of vitamin D deficiency. Nevertheless, certain limitations should be acknowledged when interpreting these recommendations.
First, the panel comprised eleven experts, and while this size is consistent with established Delphi methodology, it means that a single dissenting response shifts agreement from 100% to 91%, making results sensitive to individual outlier responses. The panel, though multidisciplinary and geographically distributed across KSA, may not fully represent the breadth of clinical practice and regional diversity within the Kingdom. Second, expert selection, while informed by clinical expertise, publication record, and commitment to vitamin D management in KSA, involved an element of subjectivity that may have introduced selection bias. Third, the final voting round was conducted the day after the second in-person group discussion, at the panel’s request due to scheduling constraints. This is an inherent feature of the modified, consensus-meeting design we adopted: several statements reached agreement only after structured face-to-face deliberation, and—as shown in the supplementary round-by-round data—a number were re-voted with unchanged wording. Although the final vote was collected confidentially and independently, with panelists blinded to one another’s individual responses, the influence of the preceding group discussion on individual judgement cannot be excluded and should be weighed when interpreting the final-round agreement levels. Fourth, all statements presented in this document represent consensus-based expert opinion rather than evidence-graded clinical recommendations. The reported percentage agreement reflects only the level of consensus among the panel and should not be interpreted as a measure of evidentiary strength. The recommendations are informed by a targeted literature review rather than a systematic review or GRADE-based evidence classification, which limits the ability to formally distinguish the strength of evidence underlying different recommendations. In particular, recommendations pertaining to extra-skeletal benefits and the ≥70 ng/mL serum 25(OH)D target for patients with comorbidities are not yet supported by large-scale RCTs and require prospective validation before being adopted as formal clinical guidelines. Similarly, the recommendation for indefinite empiric supplementation at 50,000 IU weekly diverges from general published guidance and should be applied with caution and close monitoring until regional data confirm its long-term safety and efficacy. This document is therefore intended as a regional consensus framework to guide practice where evidence is limited or conflicting and to prioritize questions for future research, and not as a substitute for formal, evidence-based clinical practice guidelines. Fifth, although response bias cannot be entirely eliminated in any expert consensus process, participants may have drawn on individual clinical experience and routine practice patterns rather than standardized evidence, particularly for statements where RCT-level data are limited or conflicting. Finally, this consensus was financially supported by Jamjoom Pharma. While the sponsor had no role in the scientific discussions, statement development, or voting process, all of which were administered by N. M. rather than by the sponsor, the potential for perceived bias inherent to commercially sponsored consensus panels should be considered by readers when interpreting these recommendations.
These findings should therefore be viewed as a foundation for future work aimed at generating regional prospective data, developing formal national guidelines, and evaluating the long-term impact of these recommendations on both skeletal and extra-skeletal health outcomes in the Saudi population.
Conclusion
This modified Delphi consensus provides a region-specific, expert-informed framework for the diagnosis and management of vitamin D deficiency in Saudi Arabia. Based on both clinical realities and feasibility, oral supplementation was identified as the primary correction strategy, with recommendations for empiric supplementation in symptomatic and high-risk populations and selective screening where clinically justified. The consensus further emphasized continuous supplementation, tailored dosing goals, and monitoring strategies that account for age, comorbidities, and safety considerations. Collectively, these recommendations address gaps in existing guidelines by integrating cultural and regional factors, providing a practical and clinically actionable framework for improving vitamin D outcomes in Saudi Arabia. Future research should evaluate the implementation and long-term impact of these recommendations on both skeletal and extra-skeletal health outcomes.
Data Sharing Statement
The datasets generated and analyzed during the current study (including Delphi survey rounds and aggregate, anonymized responses) are available as Supplementary Materials.
Informed Consent Statement
Informed consent was obtained from all participants involved in the study. Completion of the Delphi survey was considered to indicate informed consent, as outlined in the invitation letter and survey introduction. Participation was entirely voluntary, and participants could withdraw at any time without consequence.
Acknowledgment
We thank Mai Shaat for her medical writing and editorial support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was funded by Jamjoom Pharma (Saudi Arabia), which supported a pre-meeting survey, two in-person meetings, and three rounds of Delphi surveys. Jamjoom Pharma had no role in the study design, in the collection, analysis, or interpretation of data, or in the preparation of the manuscript. Commercial influence on the Delphi Process was safeguarded by the administration of the Delphi process independent of the sponsor, whereby the coordination of the in-person meetings, distribution of the surveys, and confidential collection and aggregation of votes, was facilitated by N. M., who was not a member of the voting clinical panel and who did not propose, draft, or vote on any clinical statement. Thus, the clinical statements were developed, deliberated, and voted upon solely by the eleven multidisciplinary panelists.
Disclosure
All authors received honoraria from Jamjoom Pharma for their participation in the consensus meetings and Delphi survey process. N. M. also received an honorarium for methodological support. The authors declare no other conflicts of interest in this work.
References
1. Cui A, Zhang T, Xiao P, Fan Z, Wang H, Zhuang Y. Global and regional prevalence of vitamin D deficiency in population-based studies from 2000 to 2022: a pooled analysis of 7.9 million participants. Front Nutr. 2023;10. doi:10.3389/fnut.2023.1070808
2. Pludowski P, Takacs I, Boyanov M, et al. Clinical practice in the prevention, diagnosis and treatment of vitamin D deficiency: a central and eastern european expert consensus statement. Nutrients. 2022;14(7):1483. doi:10.3390/nu14071483
3. Bouillon R, Marcocci C, Carmeliet G, et al. Skeletal and extraskeletal actions of vitamin D: current evidence and outstanding questions. Endocr Rev. 2019;40(4):1109–14.
4. Pludowski P. Supplementing vitamin D in different patient groups to reduce deficiency. Nutrients. 2023;15(17):3725. doi:10.3390/nu15173725
5. Grant WB, Wimalawansa SJ, Pludowski P, Cheng RZ. Vitamin D: evidence-based health benefits and recommendations for population guidelines. Nutrients. 2025;17(2):2. doi:10.3390/nu17020277
6. Madkhali Y, Janakiraman B, Alsubaie F, et al. Prevalence and trends of vitamin D deficiency in a Saudi Arabian population: a five-years retrospective study from 2017 to 2021. Front Public Health. 2025;13.
7. Alratrout R, Alsenbesi T. Prevalence and trends of vitamin D deficiency among patients undergoing testing at the Maternity and Children Hospital, Dammam, Eastern Province of Saudi Arabia (2023–2025). Front Public Health. 2026;14. doi:10.3389/fpubh.2026.1800317
8. Alnafisah RY, Alragea AS, Alzamil MK, Alqahtani AS. The impact and efficacy of vitamin D fortification. Nutrients. 2024;16(24):4322. doi:10.3390/nu16244322
9. Mendes MM, Botelho PB, Ribeiro H. Vitamin D and musculoskeletal health: outstanding aspects to be considered in the light of current evidence. Endocr Connect. 2022;11(10):e210596. doi:10.1530/EC-21-0596
10. Al-Daghri NM, Al-Saleh Y, Aljohani N, et al. Vitamin D status correction in Saudi Arabia: an experts’ consensus under the auspices of the european society for clinical and economic aspects of osteoporosis, osteoarthritis, and musculoskeletal diseases (ESCEO). Arch Osteoporos. 2017;12(1):1. doi:10.1007/s11657-016-0295-y
11. Al-Daghri NM, Alkharfy KM, Al-Othman A, et al. Vitamin D supplementation as an adjuvant therapy for patients with T2DM: an 18-month prospective interventional study. Cardiovasc Diabetol. 2012;11:85. doi:10.1186/1475-2840-11-85
12. Al-Daghri NM, Alkharfy KM, Al-Saleh Y, et al. Modest reversal of metabolic syndrome manifestations with vitamin D status correction: a 12-month prospective study. Metabolism. 2012;61(5):661–666. doi:10.1016/j.metabol.2011.09.017
13. Nasa P, Jain R, Juneja D. Delphi methodology in healthcare research: how to decide its appropriateness. World J Methodol. 2021;11(4):116–129. doi:10.5662/wjm.v11.i4.116
14. Rosenfeld RM, Nnacheta LC, Corrigan MD. Clinical consensus statement development manual. Otolaryngol Neck Surg. 2015;153(S2):S1–S14. doi:10.1177/0194599815601394
15. Diamond IR, Grant RC, Feldman BM, et al. Defining consensus: a systematic review recommends methodologic criteria for reporting of Delphi studies. J Clin Epidemiol. 2014;67(4):401–409. doi:10.1016/j.jclinepi.2013.12.002
16. Gruber-Bzura BM. Vitamin D—is the sun enough for us? Nutr Metab. 2025;22(1):70. doi:10.1186/s12986-025-00962-9
17. Kolnsberg L, Riffelmann M, Friedrich M. Comparison of serum 25-Hydroxyvitamin D Levels in patients with malignant and benign gynaecological disease. Anticancer Res. 2020;40(1):545–550. doi:10.21873/anticanres.13983
18. Torfadottir JE, Aspelund T, Valdimarsdottir UA, et al. Pre-diagnostic 25-hydroxyvitamin D levels and survival in cancer patients. Cancer Causes Control CCC. 2019;30(4):333–342. doi:10.1007/s10552-019-01143-9
19. Manson JE, Cook NR, Lee IM, et al. Vitamin D supplements and prevention of cancer and cardiovascular disease. N Engl J Med. 2019;380(1):33–44. doi:10.1056/NEJMoa1809944
20. Keum N, Giovannucci E. Vitamin D supplements and cancer incidence and mortality: a meta-analysis. Br J Cancer. 2014;111(5):976–980. doi:10.1038/bjc.2014.294
21. Lombardo M, Feraco A, Ottaviani M, et al. The efficacy of vitamin d supplementation in the treatment of fibromyalgia syndrome and chronic musculoskeletal pain. Nutrients. 2022;14(15):3010. doi:10.3390/nu14153010
22. Hahn J, Cook NR, Alexander EK, et al. Vitamin D and marine omega 3 fatty acid supplementation and incident autoimmune disease: VITAL randomized controlled trial. THE BMJ. 2022;376:e066452. doi:10.1136/bmj-2021-066452
23. Dong Y, Zhu H, Chen L, et al. Effects of vitamin D3 and marine omega-3 fatty acids supplementation on biomarkers of Systemic inflammation: 4-year findings from the VITAL randomized trial. Nutrients. 2022;14(24):5307. doi:10.3390/nu14245307
24. Galușca D, Popoviciu MS, Babeș EE, et al. Vitamin D Implications and effect of supplementation in endocrine disorders: autoimmune thyroid disorders (Hashimoto’s Disease and Grave’s Disease), diabetes mellitus and obesity. Medicina (Mex). 2022;58(2):194. doi:10.3390/medicina58020194
25. Bouillon R, Manousaki D, Rosen C, Trajanoska K, Rivadeneira F, Richards JB. The health effects of vitamin D supplementation: evidence from human studies. Nat Rev Endocrinol. 2022;18(2):96–110. doi:10.1038/s41574-021-00593-z
26. Uçar N, Holick MF. Illuminating the connection: cutaneous vitamin D3 synthesis and its role in skin cancer prevention. Nutrients. 2025;17(3):386. doi:10.3390/nu17030386
27. Joh HK, Hwang SS, Cho B, Lim CS, Jung SE. Effect of sun exposure versus oral vitamin D supplementation on serum 25-hydroxyvitamin D concentrations in young adults: a randomized clinical trial. Clin Nutr. 2020;39(3):727–736. doi:10.1016/j.clnu.2019.03.021
28. Tripkovic L, Lambert H, Hart K, et al. Comparison of vitamin D2 and vitamin D3 supplementation in raising serum 25-hydroxyvitamin D status: a systematic review and meta-analysis. Am J Clin Nutr. 2012;95(6):1357–1364. doi:10.3945/ajcn.111.031070
29. Van den Heuvel EGHM, Lips P, Schoonmade LJ, et al. Comparison of the effect of daily vitamin D2 and vitamin D3 Supplementation on Serum 25-Hydroxyvitamin D concentration (Total 25(OH)D, 25(OH)D2, and 25(OH)D3) and importance of body mass index: a systematic review and meta-analysis. Adv Nutr. 2024;15(1):100133. doi:10.1016/j.advnut.2023.09.016
30. Oliveri B, Mastaglia SR, Brito GM, Seijo M, A E. Vitamin D3 seems more appropriate than D2 to sustain adequate levels of 25OHD: a pharmacokinetic approach. Eur J Clin Nutr. 2015;69(6):697–702. doi:10.1038/ejcn.2015.16
31. Aguiar M, Andronis L, Pallan M, Högler W, Frew E. Preventing vitamin D deficiency (VDD): a systematic review of economic evaluations. Eur J Public Health. 2017;27(2):292–301. doi:10.1093/eurpub/ckw270
32. Padilla Colón CJ, Molina-Vicenty IL, Frontera-Rodríguez M, et al. Muscle and bone mass loss in the elderly population: advances in diagnosis and treatment. J Biomed Syd NSW. 2018;3:40–49.
33. Dawson-Hughes B. Effect of vitamin D on risk of falls and fractures – the contribution of recent mega-trials. Metab Open. 2024;23:100300. doi:10.1016/j.metop.2024.100300
34. Bertoldo F, Cianferotti L, Di Monaco M, et al. Definition, assessment, and management of vitamin D inadequacy: suggestions, recommendations, and warnings from the Italian society for osteoporosis, mineral metabolism and bone diseases (SIOMMMS). Nutrients. 2022;14(19):4148. doi:10.3390/nu14194148
35. Lanzarini E, Nogués X, Goday A, et al. High-Dose vitamin D supplementation is necessary after bariatric surgery: a prospective 2-year follow-up study. Obes Surg. 2015;25(9):1633–1638. doi:10.1007/s11695-015-1572-3
36. Bendotti G, Biamonte E, Leporati P, et al. Practical advice in different clinical settings. Nutrients. 2025;17(5):783. doi:10.3390/nu17050783
37. Imani PD, Vega M, Pekkucuksen NT, Srivaths P, Arikan AA. Vitamin D and metabolic bone disease in prolonged continuous kidney replacement therapy: a prospective observational study. BMC Nephrol. 2024;25(1):265. doi:10.1186/s12882-024-03705-9
38. Zhuang Y, Zhu Z, Chi P, et al. Efficacy of intermittent versus daily vitamin D supplementation on improving circulating 25(OH)D concentration: a Bayesian network meta-analysis of randomized controlled trials. Front Nutr. 2023;10:1168115. doi:10.3389/fnut.2023.1168115
39. Mortensen C, Tetens I, Kristensen M, Snitkjaer P, Beck AM. Adherence and barriers to the vitamin D and calcium supplement recommendation at Danish nursing homes: a cross-sectional study. BMC Geriatr. 2022;22(1):27. doi:10.1186/s12877-021-02719-4
40. Hathcock JN, Shao A, Vieth R, Heaney R. Risk assessment for vitamin D. Am J Clin Nutr. 2007;85(1):6–18. doi:10.1093/ajcn/85.1.6
41. Jetty V, Glueck CJ, Wang P, et al. Safety of 50,000-100,000 units of Vitamin D3/week in Vitamin D-Deficient, hypercholesterolemic patients with reversible statin intolerance. North Am J Med Sci. 2016;8(3):156–162. doi:10.4103/1947-2714.179133
42. Pludowski P, Marcinowska-Suchowierska E, Togizbayev G, et al. Daily and weekly “High Doses” of cholecalciferol for the prevention and treatment of vitamin D deficiency for obese or multi-morbidity and multi-treatment patients requiring multi-drugs—a narrative review. Nutrients. 2024;16(15):2541. doi:10.3390/nu16152541
43. Wimalawansa SJ, Weiss ST, Hollis BW. Integrating endocrine, genomic, and extra-skeletal benefits of vitamin D into national and regional clinical guidelines. Nutrients. 2024;16(22):22. doi:10.3390/nu16223969
44. Ataide FL, Carvalho Bastos LM, Vicente Matias MF, Skare TL, Freire de Carvalho J. Safety and effectiveness of vitamin D mega-dose: a systematic review. Clin Nutr ESPEN. 2021;46:115–120. doi:10.1016/j.clnesp.2021.09.010
45. Demay MB, Pittas AG, Bikle DD, et al. Vitamin D for the prevention of disease: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2024;109(8):1907–1947. doi:10.1210/clinem/dgae290
46. McCullough PJ, Lehrer DS, Amend J. Daily oral dosing of vitamin D3 using 5000 TO 50,000 international units a day in long-term hospitalized patients: insights from a seven year experience. J Steroid Biochem Mol Biol. 2019;189:228–239. doi:10.1016/j.jsbmb.2018.12.010
47. Marcinowska-Suchowierska E, Kupisz-Urbańska M, Łukaszkiewicz J, Płudowski P, Jones G. Vitamin D toxicity–a clinical perspective. Front Endocrinol. 2018;9:550. doi:10.3389/fendo.2018.00550
48. Holick MF. Vitamin D is not as toxic as was once thought: a historical and an up-to-date perspective. Mayo Clin Proc. 2015;90(5):561–564. doi:10.1016/j.mayocp.2015.03.015
49. Batman A, Saygili ES, Yildiz D, et al. Risk of hypercalcemia in patients with very high serum 25‐OH vitamin D levels. Int J Clin Pract. 2021;75(7):e14181. doi:10.1111/ijcp.14181
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Establishment of Serum 25-Hydroxyvitamin D Reference Range for Healthy Adult Men Not Using Vitamin D Supplements in Alqurayyat, Saudi Arabia
Aldaham AMS, Beheiry A, Hamza AA, Albalawi MH, Alanazi AM, Alanazi AS, Albilasi MM, AlRuwaili AM, ALabdali AM, Alanazi AS, Alanazi MR
International Journal of General Medicine 2026, 19:535665
Published Date: 24 March 2026