Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Erroneous Thought in Inpatients with Major Depressive Disorder: The Role of Psychological Trauma During Childhood and Adulthood
Authors Chiu CD, Chou LS, Hsieh YC, Lin CH ![]() , Li DJ
, Li DJ ![]()
Received 6 November 2022
Accepted for publication 27 January 2023
Published 5 February 2023 Volume 2023:19 Pages 337—348
DOI https://doi.org/10.2147/NDT.S396451
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yu-Ping Ning
Chui-De Chiu,1 Li-Shiu Chou,2 Yung-Chi Hsieh,2 Ching-Hua Lin,2 Dian-Jeng Li3,4
1Department of Psychology, Clinical and Health Psychology Centre, and Centre for Cognition and Brain Studies, the Chinese University of Hong Kong, Sha Tin City, Hong Kong; 2Department of Adult Psychiatry, Kaohsiung Municipal Kai-Syuan Psychiatric Hospital, Kaohsiung City, Taiwan; 3Department of Addiction Science, Kaohsiung Municipal Kai-Syuan Psychiatric Hospital, Kaohsiung City, Taiwan; 4Department of Nursing, Meiho University, Pingtung, Taiwan
Correspondence: Dian-Jeng Li, Department of Addiction Science, Kaohsiung Municipal Kai-Syuan Psychiatric Hospital, 130, Kai-Syuan 2nd Road, Ling-Ya District, Kaohsiung, 802, Taiwan, Tel +886-7-751-3171 ext. 2343, Fax +886-7-16-1843, Email [email protected]
Background: The pathogenic role of trauma in psychotic-like experiences has yet to be clarified. The aim of this study was to investigate the role of childhood and adulthood trauma on erroneous thoughts among patients with major depressive disorder.
Materials and Methods: Inpatients with major depressive disorder (MDD) and healthy controls (HCs) were enrolled, and paper-and-pencil questionnaires were applied. Clinical rating and self-reported scales were used to measure levels of depression, dissociation, psychological trauma, parental maltreatment, and erroneous thoughts. Pearson’s correlation analysis was conducted to explore potentially significant associations between erroneous thoughts and other independent variables, and standardized regression coefficients of hierarchical regression analysis were used to predict the significant relationships between erroneous thoughts and adulthood or childhood trauma.
Results: A total of 99 participants were included into the analysis, of whom 59 were patients with MDD and 40 were HCs. After treatment, the patients with MDD showed significantly higher levels of depression, childhood maltreatment, interpersonal trauma and erroneous thoughts than the HCs. After estimating and verifying correlations with hierarchical regression among the patients with MDD, a link between adulthood betrayal trauma and higher level of conviction along with the number of erroneous thoughts was found. However, no significant association was identified between childhood trauma and erroneous thought. The concurrent level of depression significantly predicted a higher level of being preoccupied, along with the number of erroneous thoughts.
Conclusion: The current study fills a gap in the literature by showing a link between adulthood trauma and erroneous thoughts in non-psychotic patients. Further studies with well-controlled comparisons and prospective cohort with longer follow-up are warranted to extend the applicability and generalizability of the current study.
Keywords: depression, erroneous thought, adulthood trauma, childhood trauma, psychiatric inpatient
Introduction
Whether unresolved psychological trauma can distort the testing of reality has been revisited in the past two decades. Potentially traumatizing events are commonly reported in clinical patients with severe disturbance in reality testing, such as a psychotic disorder. Psychological trauma can be classified as either non-interpersonal or interpersonal trauma,1 and interpersonal trauma may indicate poorer outcome of mental health. In comparison with non-interpersonal trauma, interpersonal trauma demonstrates higher severity of post-traumatic stress disorder, depression, guilt, and risk of oppositional defiant disorder.2–4 Therefore, we focused on the association between interpersonal trauma and psychosis. A previous meta-analysis demonstrated a significant association between psychosis and childhood interpersonal trauma in both case–control studies of patients with psychotic disorders and population-based cross-sectional studies.5 This association was also reported in another meta-analysis focusing on childhood interpersonal trauma in help-seeking individuals with a recent decline in socio-occupational functioning and the presence of subthreshold positive symptoms in healthy controls (ie, ultra-high risk).6 Importantly, this link cannot be readily ascribed to the acute mental dysfunction of a psychotic state, as early traumatic experiences in a premorbid state have been reported to predict the emergence of psychotic symptoms in prospective studies.7,8 Trauma therefore appears to play a role in the pathogenesis of psychotic symptoms.
Existing knowledge including autobiographical memories and personal beliefs derived from prior experiences is the foundation for the understanding of the current environment,9,10 and thus its impact on the formation of psychotic symptoms is not surprising. However, on which dimensions of psychotic experiences trauma may exert an effect remains largely unknown. We hypothesized that examining the relationship between traumatic experiences and disparate aspects of erroneous thoughts may shed light into this question. Erroneous thoughts are a distorted interpretation, attribution, or appraisal toward the environment, the self or other people.11 For instance, a paranoid thought stands for being threatened in some way, such as being spied on, followed, secretly tested or plotted against, or suspecting that one’s spouse is being unfaithful.12 Erroneous thought can be seen to emerge understandably from the patient’s internal and external environment, especially from his mood state, and true delusions are psychologically irreducible.11 Similar to hallucinatory experiences, erroneous thoughts can occur in clinical patients with a full-blown psychotic disorder as well as neurotic patients and the general populations.13,14 Of note, patients with a psychotic disorder and psychoticism-prone individuals can differ in some aspects of erroneous thoughts. For example, although thematic similarity has been reported between these two groups with similar endorsement rates of common erroneous thoughts, patients with a psychotic disorder have been reported to be more preoccupied by these thoughts, to feel more distressed by them, and to have a stronger belief in their veracity.15,16 Different aspects of erroneous thoughts may relate differently to traumatic experiences.
Given the similar link between trauma and psychosis across clinical and general populations, the effect of trauma may be evident on the theme, the shared features of both nonclinical and clinical erroneous thoughts, rather than other aspects more central to the clinical status of psychosis. Indeed, an intriguing link between the content of traumatic experiences and the theme of psychotic experiences has been demonstrated in patients with nonaffective psychosis and those with a first episode.17,18 It remains largely unknown whether traumatic experiences are related to the three pathological aspects of erroneous thoughts, however this is critical to clarify the pathogenic role of traumatic memories in erroneous thoughts. If trauma relates solely to the thematic content but not the three comparative pathological features of erroneous thoughts measured by the Peters et al. Delusional Inventory (PDI)15 (distress, preoccupation, and conviction), then childhood interpersonal trauma alone is not sufficient for the genesis of psychosis. That is to say, trauma may result in a distorted perception toward an ambivalent or benign situation. However, the response to the distorted thoughts that interfere with socio-occupational functioning may not be fully attributable to prior stressful experiences.
The aim of this study was to investigate this unresolved issue regarding the pathogenic role of trauma in psychotic-like experiences. More specifically, we aimed to test the hypothesis of whether traumatic experiences would relate to the thematic content of erroneous thoughts but not the pathological features of erroneous thoughts. Such associations between trauma and erroneous thoughts were verified in patients with a mood disorder, in whom erroneous thoughts were common,19 however no full-blown psychotic disorders developed. In this study, we selected patients with a current depressive episode, given that depression is a crucial covariate of psychotic experiences20 and can be an integral part of psychotic experiences, especially in psychosis of mild-to-moderate severity.21 There are two reasons to examine the association in a nonpsychotic clinical population. First, the retrospective report of early experiences of traumatic events may be influenced by a current psychotic state. Hence, the link between traumatic experiences and erroneous thoughts may be confounded by the deficient reality testing of a psychotic disorder. Second, the thematic dimension and three morbid features of erroneous thoughts may be intertwined in patients with a full-blown psychotic disorder, due to high-end scores. In addition, we also examined the characteristics of erroneous thoughts and related information in healthy subjects in order to compare differences in multiple dimensions for erroneous thoughts.
With respect to traumatic experiences, we assessed both childhood and adulthood trauma in the current study. Differentiating the two types of traumatic experiences is of conceptual importance. Childhood trauma has long been hypothesized to have a devastating impact on mental development and psychological well-being.22,23 Evidence of the influence of early traumatic stress on neurobiological development is also accumulating.24,25 However, childhood trauma survivors frequently experience potentially traumatizing events in adulthood (ie, revictimization26), as also seen in patients with psychosis.27 This correlation between childhood and adulthood trauma raises the question of whether the presenting features of erroneous thoughts should be ascribed to the remote unresolved issues that originated in early developmental stages or to recent traumatic stress. Finally, we also controlled for maladaptive parenting styles including indifference and overcontrol,28 a common covariate of childhood trauma,29 in the analysis.
We hypothesized that there should be a relationship between potentially traumatizing events and erroneous thoughts. In addition, we hypothesized that this link may be more readily detected with the number of erroneous thoughts (ie, thematic content) and that this link would remain significant after controlling for maladaptive parenting.17 The morbid aspects of erroneousness including conviction, preoccupation, and distress may be more tightly linked to current psychiatric status, and hence there may be an exclusive relationship with current depression. Regarding the distinction between childhood and adulthood trauma, an a priori hypothesis cannot be derived from the existing literature.
Methods
Ethics
This study derived data from two projects which aimed to investigate the stability of self‐reported childhood interpersonal adversity and relationships among interpersonal adversity, psychiatric status, and socio-cognitive functions.30 These investigations were approved by the Institutional Review Board of Kai-Syuan Psychiatric Hospital on 30th Dec 2014 and 1st May 2017 (KSPH-2014-34 and KSPH-2017-04) and conducted in accordance with the current revision of the Declaration of Helsinki and national legal requirements (Human Subjects Research Act, Taiwan). All participants signed written informed consent after the study had been explained in detail.
Participants and Procedures
This study included data from a project which mainly recruited newly admitted patients with the acute onset of major depressive disorder (MDD) at Kaohsiung Municipal Kai-Syuan Psychiatric Hospital, Taiwan, from December 30th, 2014 to December 21st, 2016. The inclusion criteria were 1) admission due to MDD according to the DSM-IV-TR diagnostic criteria;31 2) age between 20 and 50 years; and 3) a native speaker of Mandarin Chinese. Patients were not eligible for the study if they had 1) intellectual disability (full-scale IQ less than 80); 2) organic syndromes; or 3) difficulty in either receptive or expressive language. In addition, information of healthy subjects was derived from another project, which recruited participants from May 17th, 2014 to December 21st, 2020. The inclusion criteria for these healthy subjects were 1) being free from any neuro-psychiatric disorder; 2) age between 20 and 50 years; and 3) a native speaker of Mandarin Chinese. Subjects in the control group were excluded if they had difficulty in either receptive or expressive language.
The recruited patients from these original projects were assessed with two phases of examinations. Phase 1 assessments were conducted at the first week of admission. Both self-reported measures of psychopathology and childhood interpersonal adversity and clinical interview schedules of depression and psychosis were recorded. Phase 2 assessments were the same as in phase 1; however, they were conducted during the last week of admission or 6 weeks after the admission. In this study, we only analyzed data from phase 2 in order to prevent possible confounding effects due to exacerbations of their psychiatric disorders, for example, difficulty in recalling their past experience. The clinical interviews were conducted by three well-trained psychiatrists with intra-class correlation coefficients of at least 0.9.
Outcome Measures
To assess the different dimensions of psychopathology, the following self-reported scales were used. Erroneous thoughts were assessed using the PDI.15 The PDI measured 21 categories of erroneous thoughts (yes or no) such as grandiosity or paranoia, along with three dimensions of scoring (distress, preoccupation, and conviction). Each dimension was scored on a 5-point Likert scale from 1 (not at all) to 5 (extremely). Four subscales were used in the final analysis, including the number of responsive items, and mean scores of distresses, preoccupation, and conviction. With regard to evaluating childhood adversity, we specifically explored categories of parental dysfunction using the Measure of Parental Style (MOPS).28 The MOPS included 30 questions (15 for fathers and 15 for mothers) to measure perceived parental maltreatment. Subscales of indifference (eg uncaring of me) and over-control (eg sought to make me feel guilty) were selected into the analysis. Potentially traumatizing events were measured using the Brief Betrayal Trauma Questionnaire (BBTS).32 The 12-item BBTS covered a series of traumatic experiences, including natural disasters, traffic accidents, physical and sexual assault, emotional maltreatment, and being a witness to a catastrophic event. The frequency of each experience in childhood (before 18 years of age) and during adulthood was rated separately using a 3-point Likert scale (never, 1–2 times, >2 times). This instrument differentiated two levels of betrayal in psychological trauma. High betrayal trauma (Item 3, 5, 6, 8, and 10) indicated betrayal events by someone to whom you were very close, and low betrayal trauma (Item 4, 7 and 9) describes betrayal events by someone with whom you were not familiar. The clinical interview scales of depression were evaluated using the Hamilton Depression Rating Scale (HDS).33 The HDS contained 17 items with total scores ranging from 0 to 52. A higher HDS score indicated a more severe state of depression.
Statistical Analysis
We first summarized demographic data and outcome measures. Differences in characteristics between the patients with MDD and healthy subjects were estimated using Pearson’s χ2 test and the independent t test. Pearson’s correlations were calculated to explore potentially significant associations between erroneous thoughts (PDI) and other independent variables, including level of depression (HDS), parental dysfunction (MOPS), and potentially traumatizing events in childhood and in adulthood (BBTS). The analysis of PDI included four categories: number of items, distress, preoccupation, and conviction. Furthermore, standardized regression coefficients of hierarchical regression analysis34 were used to predict significant relationships between erroneous thoughts (PDI) and childhood or adulthood trauma with a controlled model. We measured invariance, which involves testing and comparing models that impose successive restrictions on model parameters with a systemic order of basic demographics (sex and age), level of depression, parental dysfunction, and interpersonal trauma (childhood and adulthood). Each model tested the invariance with target parameters, which included restrictions from the previous model. Hierarchical regression analysis could help to verify whether correlations with executive control remain significant when the effects of covariates were considered. Furthermore, we tested the mediating effect of parental dysfunction if the significance of the association between specific trauma and erroneous thoughts was identified. To verify the mediating effect, the model was tested using the PROCESS macro developed by Hayes 3.4.35,36 In the PROCESS macro, Hayes’s Model 4 was applied to fit the mediation model. The ordinary least squares regression was used to estimate the coefficients of the moderated mediation model with the PROCESS macro. All of the variables were centralized,37 and the 95th percentile bootstrap confidence interval (CI) with 5000 bootstrapping samples was estimated. The coefficients of mediation effect and its 95% CI was used to determine the statistical significance of the mediation effect.35 If the 95% CI did not include zero, the mediating effect was statistically significant, indicating that the model had been successfully established. All data were processed using SPSS version 23.0 for Windows (IBM Inc., USA). All tests were two-tailed without adjustments for multiple comparisons, and significance was defined as α ≤ 0.05.
Results
The descriptive statistics of the major studied variables, including means, standard deviations, and comparisons between the patients with MDD and healthy subjects are listed in Table 1. Potentially traumatizing events were more common in the patients with MDD, with 71.2% and 88.1% of the patients reporting more than one type of interpersonal traumatic experience in childhood and adulthood, respectively, compared to 30% and 20% of the healthy subjects. The rate of traumatic experiences among the patients with MDD was higher than that previously reported in college students (28.8%),38 highlighting the high rate of traumatization in this sample. As we predicted, multiple dimensions of erroneous thoughts were much more severe among the patients with MDD than in the healthy subjects. There was a similar trend in levels of childhood maltreatment and interpersonal trauma. In addition, correlation analysis with Pearson’s product-moment coefficients showed that the patients with childhood interpersonal trauma had a higher risk of childhood non-interpersonal trauma (r = 0.633, p < 0.001), as well as adulthood interpersonal (r = 0.638, p < 0.001) and non-interpersonal (r = 0.465, p < 0.001) trauma. As predicted, childhood interpersonal trauma was also correlated with parental dysfunction including indifference (r = 0.546, p < 0.001) and over-control (r = 0.685, p < 0.001).
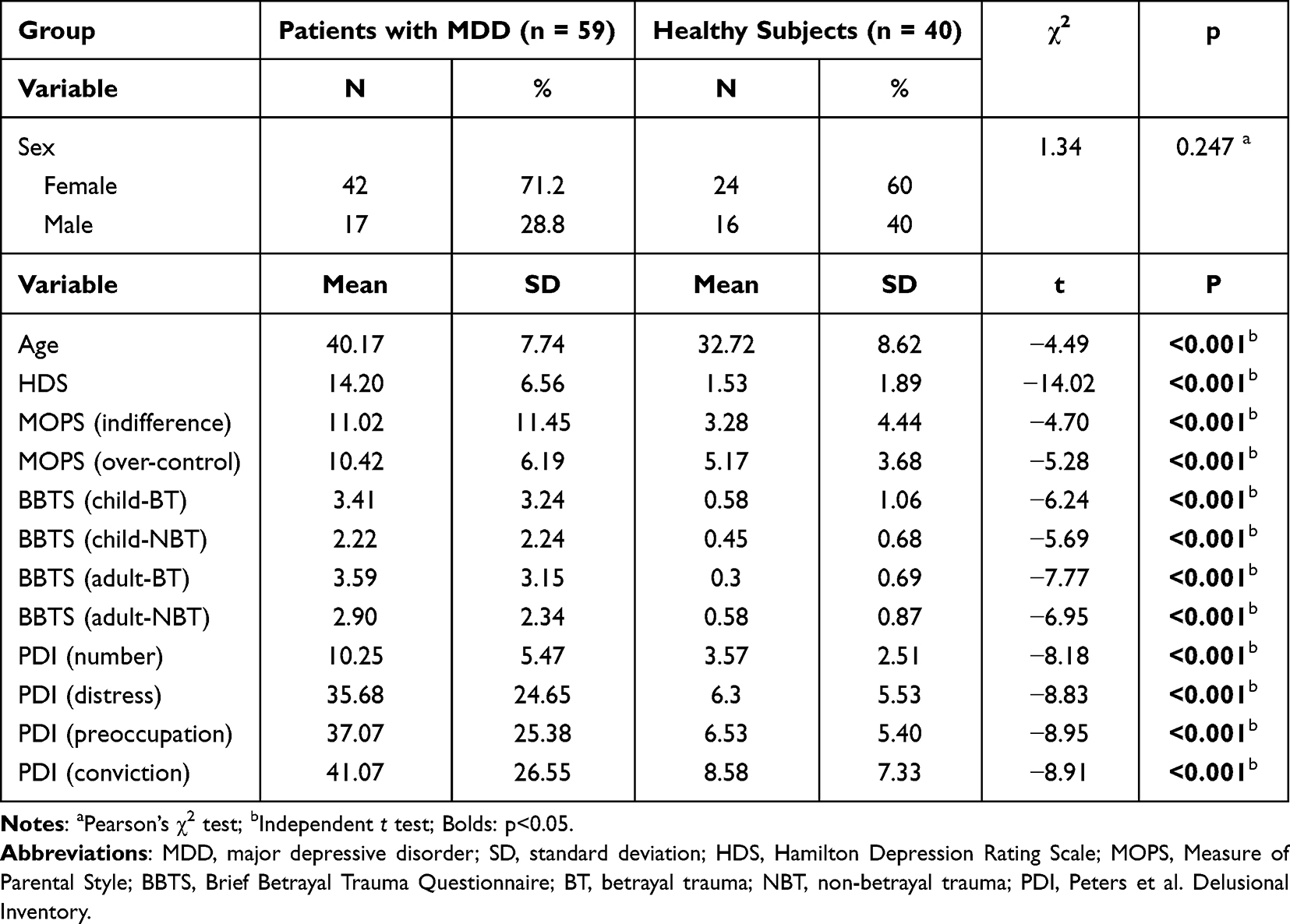 |
Table 1 Characteristics of Demographic and Quantitative Variables (n = 99) |
Next, we investigated associations between erroneous thoughts and potentially traumatizing events as well as the covariates. We performed Pearson’s correlation analysis, with the four measures of erroneous thoughts as dependent variables and potentially traumatizing events as well as the covariates as predictors. The results are summarized in Table 2. As predicted, potentially traumatizing events were positively correlated with erroneous thoughts, including the number of items and levels of distress, preoccupation, and conviction. Of note, these features of erroneous thoughts were also correlated with covariates including state of depression and parental dysfunction.
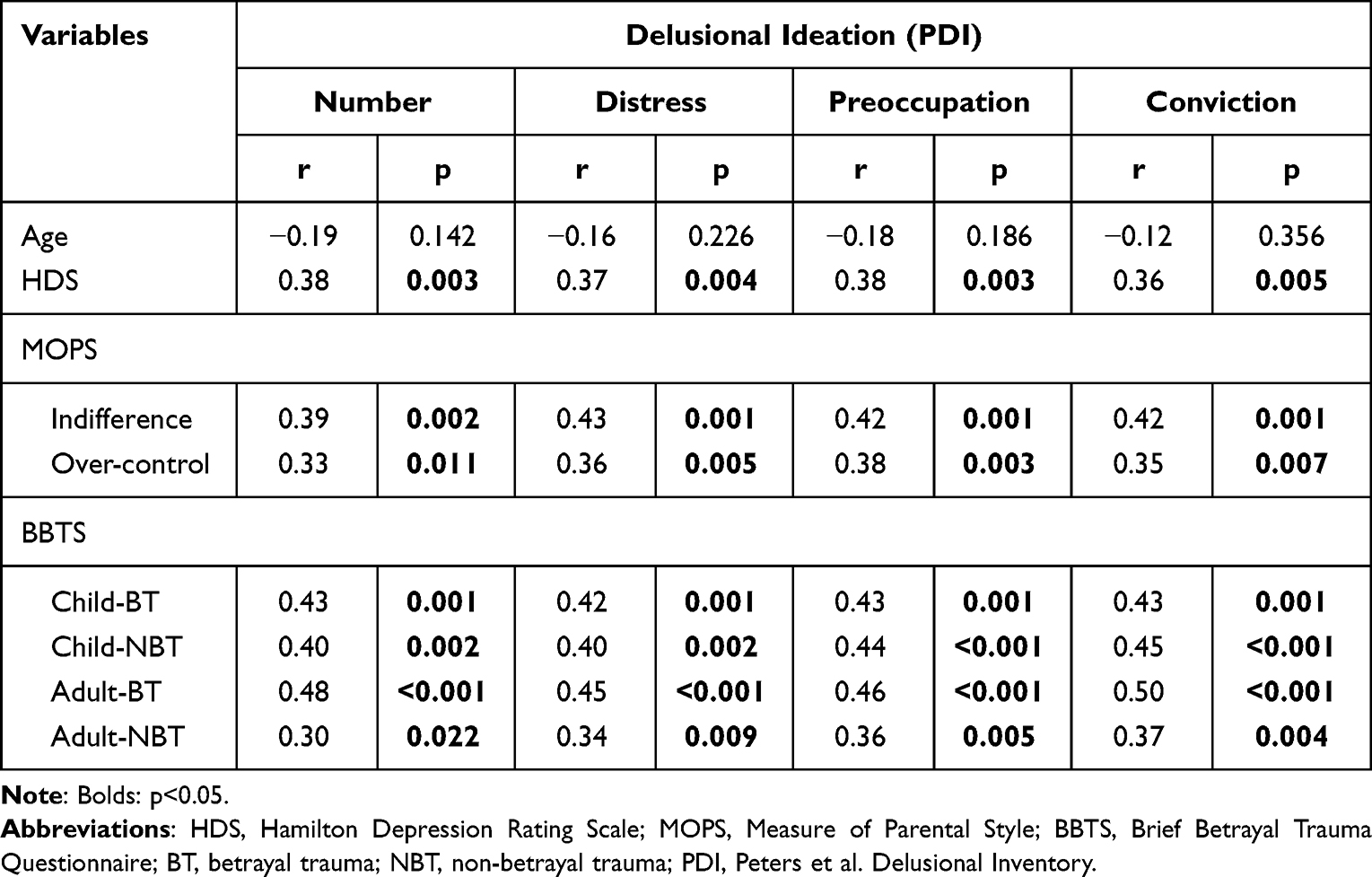 |
Table 2 Pearson’s Correlation Coefficients Among PDI Scores and Continuous Variables Within Patients with Major Depressive Disorder |
The intertwined relationship between psychopathology (including erroneous thoughts and depression) and stressful interpersonal experiences (including the four types of potentially traumatizing events as well as parental over-control) raised doubts about the specificity between erroneous thoughts and potentially traumatizing events. The manifestation of erroneous thoughts has been correlated with other clinical variables including age.39–41 To address this issue, we performed multiple regression analysis. By including the covariates with potentially traumatizing events in the same model, we could control the covariance and test whether there was a unique association between erroneous thoughts and potentially traumatizing events. The results of the preliminary model are summarized in Table 3.
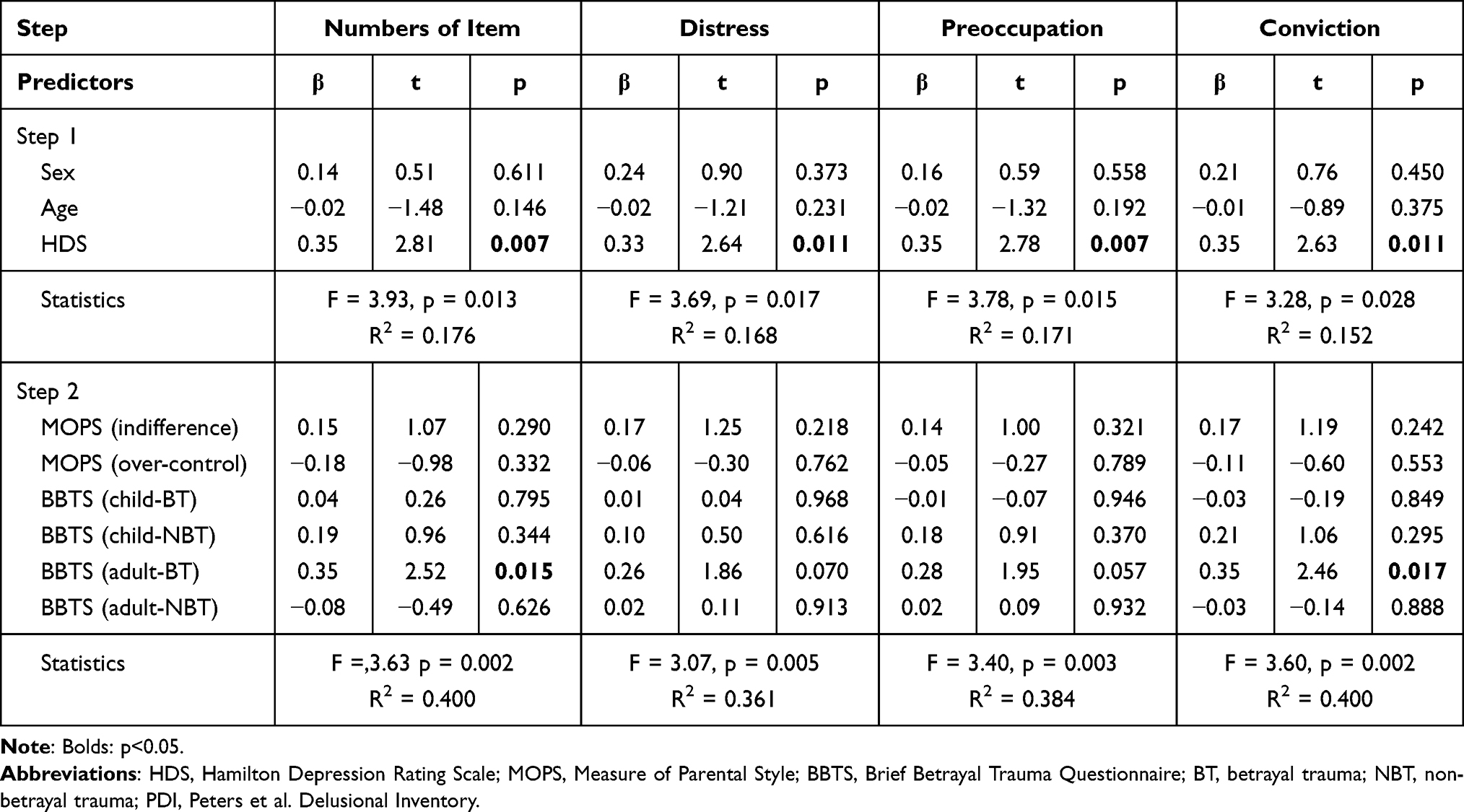 |
Table 3 Preliminary Model with Hierarchical Regression Analysis for Predictors of PDI Scores Among Patients with Major Depressive Disorder |
Several correlations between erroneous thoughts and potentially traumatizing events became insignificant after controlling for the covariates and incorporating the other types of potentially traumatizing events, including those involving childhood interpersonal trauma and adulthood non-interpersonal trauma (Table 4). Intriguingly, there was a significant link between adulthood interpersonal trauma and the number of unusual ideations, and this significance remained in the analysis. Among the three dimensions of erroneous thoughts, only the level of conviction was correlated with adulthood interpersonal trauma, and the other dimensions were insignificant. Among the other covariates, state of depression appeared to be a critical factor in predicting more erroneous thoughts and higher level of preoccupation, as well as insignificant trends of distress and conviction.
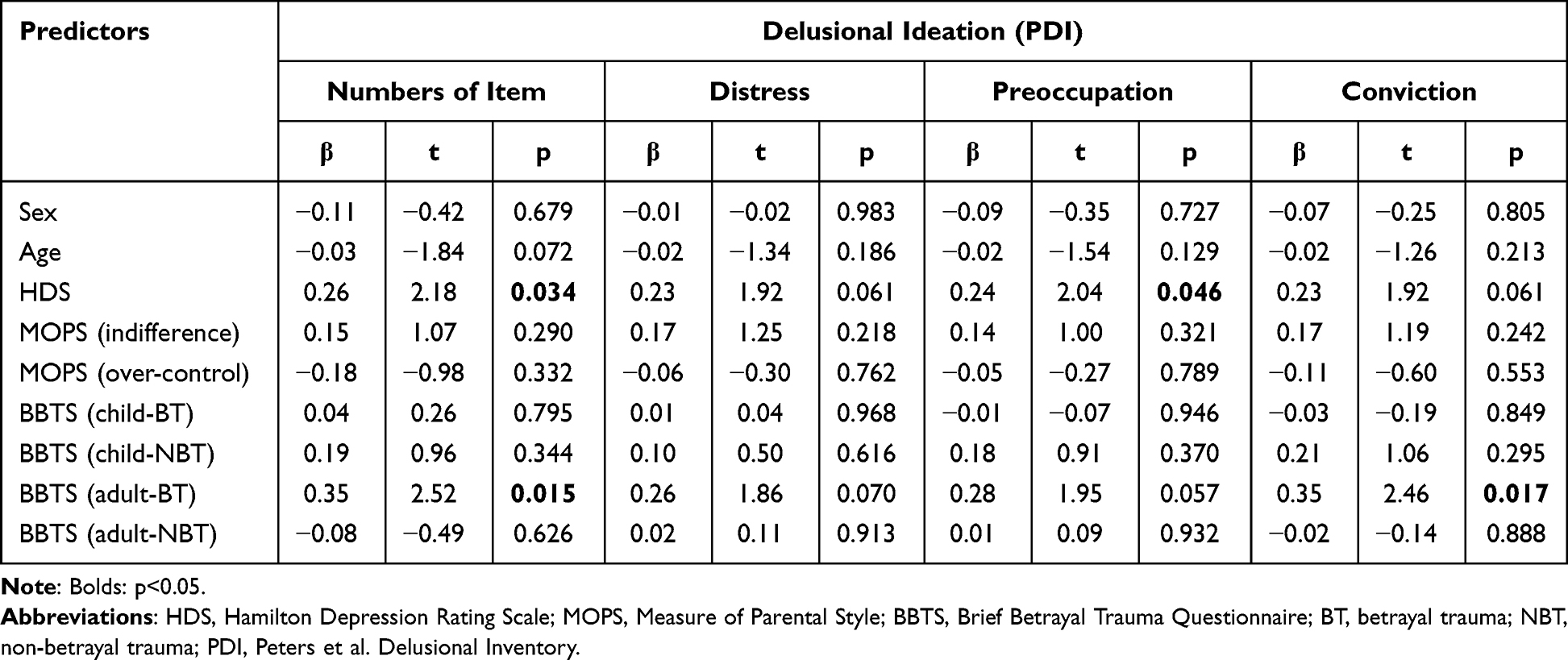 |
Table 4 Final Model for Predictors of PDI Scores Estimated with Hierarchical Regression Analysis Among Patients with Major Depressive Disorder |
Since the significant association between adulthood betrayal trauma and erroneous thought (numbers of items and conviction) was identified, we further tested the mediating effect of parental dysfunction (indifference and over-control) on this association. The results of ordinary least squares regression analysis in the mediation model are summarized in the supplementary tables (Supplementary Tables 1-4). Among the tested models, only one model with significantly mediating effect was identified. Adulthood betrayal trauma was positively associated with the severity of indifference (β = 1.406, p = 0.003). The severity of indifference was also positively correlated with conviction of erroneous thought (β = 0.625, p = 0.029). The coefficient of indirect effect in the mediation model was 0.878 with a 95% CI of 0.053 to 1.975, indicating the significantly positive effect of moderation. Taken together, these findings demonstrated the positive indirect effect of adulthood betrayal trauma on conviction of erroneous thought through the positive mediating effect of indifference of parental dysfunction (Supplementary Table 3). Other models did not reveal a significantly mediating effect (Supplementary Tables 1, 2 and 4).
Discussion
Summarized Findings
The current study aimed to clarify the link between traumatic experiences and psychosis in a clinical sample of depression in patients with varying degrees of erroneous thoughts. Consistent with previous studies, we found a simple correlation between traumatic experiences and erroneous thoughts, despite similar correlations between erroneous thoughts with maladaptive parenting and current level of depression. Nevertheless, when entering all of the predictors into a regression model, a more exclusive link between the number of erroneous thoughts and adulthood, rather than childhood trauma, was found. In addition, the number of erroneous thoughts was also significantly correlated with the level of conviction but not distress and preoccupation. Intriguingly, the level of current depression appeared to be a major contributory factor for preoccupation and the number of erroneous thoughts, along with insignificant trends of distress and conviction. In addition, indifference of parental dysfunction significantly mediated the association between adulthood betrayal trauma and conviction of erroneous thought.
Psychoticism in Depressive Disorder
Since the concept of the psychosis continuum was introduced in 199442 and expanded in recent years,43,44 investigations into psychosis have been conducted in both clinical subjects with psychotic disorders and also subclinical subjects such as community residents and college students with proneness to psychotic-like experiences. However, few studies have investigated individuals along this continuum with disturbed psychiatric function who have not yet reached a profound decline in reality testing. Despite the link between mood symptoms and psychotic symptoms, previous studies on psychotic symptoms in mood disorders have focused mainly on the conceptual debate between neurosis and psychosis (eg, neurotic versus psychotic depression).45–47 In the current study, we demonstrated the importance of understanding psychoticism in patients with depressive disorders. Not surprisingly, erroneous thoughts were found to be more prevalent in this clinical population than in the nonclinical population (healthy subjects). More importantly, the severity of symptoms in terms of conviction, preoccupation, and distress varied across individuals.
The first important finding of the current study is the link between the current level of depression and the three morbid aspects of erroneous thoughts. Our results showed a reliable association between them, including preoccupation and trends of the other two aspects. These morbid aspects of erroneous thoughts appeared to be sensitive to the clinical status of a disorder. In other words, patients with a more severe status of depression may predominantly have been occupied by their erroneous thoughts. This result is congruent with the literature in that it emphasizes the relevancy of these three aspects (distress, preoccupation, and conviction) with socio-occupational disability, and helps to differentiate clinical (deluded) from subclinical (not deluded) erroneous thoughts.15 Recent studies assessing delusion multi-dimensionally have also found that dimensions of delusional experience, especially distress and preoccupation, are helpful to distinguish psychotic patients from community samples.48,49 As a result, dimensions of erroneous thoughts may be more important than the counts or contents of belief alone among depressive patients.
Psychological Trauma and Erroneous Thoughts
The results of the current study suggest that depression may have a minor effect in relation to erroneous thoughts, but that traumatic experiences still exert an effect on erroneous thoughts through depression.50 There is growing interest in the link between childhood trauma and psychoticism,51 and our findings indicate that several confounding variables including adulthood traumatic stress and childhood parental dysfunction, which have been overlooked in previous empirical studies, should be considered when examining this link. The role of childhood trauma in psychoticism cannot be clarified if clinical and environmental covariates are not considered.
Importantly, traumatic experiences may play an exclusive role in the formation of psychotic symptoms through the formation of thematic content. Qualitative analyses of themes in previous studies in patients with a psychotic disorder have shown a link between the content of psychotic symptoms including hallucination17 and delusion18 and preceding life events. Consistent with these findings, our results demonstrated that traumatic experiences were positively correlated with the number of erroneous thoughts, but that they were not a predominant pathological feature of erroneous thoughts. Only conviction reached significance among the three dimensions. Our results therefore extend the literature by showing that this link was also evident in individuals with a currently major depressive episode rather than a full-blown psychotic disorder, after controlling for their current state of depression. Psychological trauma has long been understood to be a devastating life event that cannot be readily assimilated into the existing autobiographical schema of a survivor.52 This disintegration may keep traumatic experiences fragmented from other autobiographical experiences and intrusions, and it is supposed to affect the perception and interpretation of daily events, which is associated with the conviction of erroneous thought.
Impact of Adulthood Trauma and Childhood Adversity on Erroneous Thoughts
Interestingly, links between erroneous thoughts were found between both childhood trauma and adulthood trauma. More importantly, in the hierarchical regression model, the link with adulthood trauma remained significant, whereas it disappeared with childhood trauma. This finding suggests that recent life events may be more important than remote stressful experiences with regard to the formation of a symptom, at least for the thematic content of erroneous thoughts. Adulthood may be a proximal factor within the significant correlation between childhood trauma and erroneous thoughts. With regard to the etiology, re-victimization may be a crucial factor. In the literature of child abuse, re-victimization has been found to be a reliable phenomenon, and survivors of child maltreatment tend to expose themselves repeatedly to potentially traumatizing events in adulthood.26,53–56 In nonclinical studies, this overlaps between adulthood and childhood trauma with regard to their impact on psychiatric function such as suicidal behavior and psychotic-like experiences has been observed.57,58 This result suggests that childhood experience may not play a unique role in the formation of erroneous thoughts, and instead suggests the importance of recent significant life events, especially interpersonal trauma involving others to whom the subject is close. Furthermore, parenting style, which has been associated with childhood interpersonal trauma, may not be related to erroneous thoughts regarding either thematic contents or dimensions. Previous studies have reported associations between parenting style and psychosis59 or psychotic-like experiences (schizotypy).60 Our results of simple correlation analysis are comparable with previous studies; however, the association was insignificant after multiple adjustments. Therefore, recent adulthood trauma may have a greater impact on erroneous thoughts than early experiences, including childhood trauma or parenting style.
Mediating Effect of Parental Dysfunction
We also found that parental dysfunction of indifference positively mediated the association between adulthood betrayal trauma and erroneous thought. The association between psychological trauma and parenting style had been investigated. A previous literature demonstrated that individuals with psychological trauma were likely to have a poor parenting style.61 Moreover, psychological trauma was reported to be more prevalent in patients exposed to the parenting style of affectionless control.62 On the other hand, family-related factors were also reported to be associated with the formation of psychotic symptoms. Previous research also indicated that positive symptoms, such as delusions or hallucinations, have been associated with a higher level of parental maltreatment, including rejection and overprotection/control.61 Our findings further extended the applications of previous literatures to the association between psychological trauma, parental dysfunction, and psychotic symptoms with the specific type of trauma (adulthood betrayal trauma) and parental dysfunction (indifference). Further studies may be helpful to explore the etiologies within it.
Clinical Implication of Psychoticism Among Depressive Patients
Severe depressive patients may be more likely to have erroneous thoughts throughout the day and get into trouble due to disturbing behavior, and psychotic symptoms may be particularly hazardous for these patients. A 2-year prospective study on patients with psychotic depression showed that those with more severe depression or psychosis at baseline had a slower recovery from the syndrome.63 Previous studies have also demonstrated that depressive patients with psychotic features have a more chronic course, more recurrence, slower recovery, and more re-hospitalizations than those without psychotic features.64,65 Therefore, attention should be paid to psychotic symptoms, including erroneous thoughts, in clinical practice. The dimensions of conviction should also be evaluated because they may persist after treatment for depression. Previous studies have shown the efficacy of treatment on PDI-21 scores, particularly on the preoccupation and conviction dimensions.66,67 Our results indicate that treating depressive symptoms may be beneficial to reduce the maladaptive responses of erroneous thoughts, at least for a non-full-blown psychotic disorder. On the other hand, our results imply that the evaluative aspect of erroneous thoughts, a component related more intimately to mental illness characterized by functional impairment, involves a dysregulated negative affective state. In contrast, thematic content, which has a closer association with recent personal stressful experiences, may not be necessary pathologically. Therefore, whilst earlier studies tended to report PDI total scores,68 it has become more common for researchers to analyze the dimension scores.
Limitations
Several limitations should be addressed. First, all of the measurements in phase 2 were used. The self-reported PDI, BBTS, and MOPS questionnaires in phase 1 were not used due to the possible confounding effects of acute depression. Therefore, all of the associations in this study are correlational, and their interpretation should be made with caution and the causality of their inter-relationships should be clarified in future studies. Second, traumatic experiences were self-reported. Even though subjective traumatic stress is a crucial element of trauma, this retrospective measure may suffer from recall bias due to clinical status and/or reinterpretation with late-life experiences including psychotherapy.69 Third, healthy participants were recruited as a control group rather than participants with other mental illness and it may need further study to compare the difference between groups with differently mental illness. Fourth, inclusion of individuals with both childhood and adult trauma is potentially confounding to distinguish the impact of different trauma. However, the confounded effect may be minimized after multiple adjustment in the hierarchical regression analysis. Fifth, the level of cumulative trauma was not identified in the questionnaires of the current study, which might be helpful to disentangle recency and revictimization effects. Sixth, as the unpredictable nature of depression, it is possible that participants may have severer level of depression in the Phase 2, which may potentially confound the result of the current study. Finally, this is a naturalistic observation study which recruited participants under the treatment of various teams. Therefore, the treatment plan of the participants was individualized according to their clinical status and the judgment of their clinical team rather than being standardized, such as titration doses of antidepressants. However, our study clarified the association between erroneous thoughts and adulthood and childhood trauma, which has rarely been reported before. Moreover, the state of depression was assessed prospectively by board-certified psychiatrists, which is also a strength of the current study.
Conclusions
In conclusion, this study demonstrated an association between adulthood betrayal trauma and the number of thematic contents in erroneous thoughts after controlling for multiple confounders. In addition, adulthood betrayal trauma was also associated with level of conviction among erroneous thought. We also found a similar association between age and the number of thematic contents. Furthermore, the severity of depression was positively correlated with dimensions of erroneous thoughts including subjective preoccupation. On the other hand, indifference of parental dysfunction mediated the association between adulthood betrayal trauma and conviction of erroneous thought. Further studies with well-controlled comparisons and longer prospective follow-up are needed to explore the precise links between factors, and even the causality.
Disclosure
This study was supported by a grant from the Kaohsiung Municipal Kai-Syuan Psychiatric Hospital (104-01). The authors alone are responsible for the content and writing of this paper, and all authors declare that they have no conflicts of interest.
References
1. Kessler RC, Ustun TB. The World Mental Health (WMH) Survey Initiative Version of the World Health Organization (WHO) Composite International Diagnostic Interview (CIDI). Int J Methods Psychiatr Res. 2004;13(2):93–121. doi:10.1002/mpr.168
2. Baker DE, Hill M, Chamberlain K, et al. Interpersonal vs. Non-Interpersonal Cumulative Traumas and Psychiatric Symptoms in Treatment-Seeking Incarcerated Women. J Trauma Dissociation. 2021;22(3):249–264. doi:10.1080/15299732.2020.1760172
3. Fowler JC, Allen JG, Oldham JM, Frueh BC. Exposure to interpersonal trauma, attachment insecurity, and depression severity. J Affect Disord. 2013;149(1–3):313–318. doi:10.1016/j.jad.2013.01.045
4. Mikolajewski AJ, Scheeringa MS. Links between Oppositional Defiant Disorder Dimensions, Psychophysiology, and Interpersonal versus Non-interpersonal Trauma. J Psychopathol Behav Assess. 2022;44(1):261–275. doi:10.1007/s10862-021-09930-y
5. Varese F, Smeets F, Drukker M, et al. Childhood adversities increase the risk of psychosis: a meta-analysis of patient-control, prospective- and cross-sectional cohort studies. Schizophr Bull. 2012;38(4):661–671. doi:10.1093/schbul/sbs050
6. Kraan T, Velthorst E, Smit F, de Haan L, van der Gaag M. Trauma and recent life events in individuals at ultra high risk for psychosis: review and meta-analysis. Schizophr Res. 2015;161(2–3):143–149. doi:10.1016/j.schres.2014.11.026
7. Janssen I, Krabbendam L, Bak M, et al. Childhood abuse as a risk factor for psychotic experiences. Acta Psychiatr Scand. 2004;109(1):38–45. doi:10.1046/j.0001-690X.2003.00217.x
8. Schreier A, Wolke D, Thomas K, et al. Prospective study of peer victimization in childhood and psychotic symptoms in a nonclinical population at age 12 years. Arch Gen Psychiatry. 2009;66(5):527–536. doi:10.1001/archgenpsychiatry.2009.23
9. Rubin DC. Remembering Our Past: Studies in Autobiographical Memory. Cambridge; New York, NY, USA: Cambridge University Press; 1996:448.
10. Rubin DC, Schrauf RW, Greenberg DL. Belief and recollection of autobiographical memories. Mem Cognit. 2003;31(6):887–901. doi:10.3758/BF03196443
11. Oyebode F. Sims’ Symptoms in the Mind: Textbook of Descriptive Psychopathology.
12. Na EJ, Choi KW, Hong JP, et al. Paranoid Ideation Without Psychosis Is Associated With Depression, Anxiety, and Suicide Attempts in General Population. J Nerv Ment Dis. 2019;207(10):826–831. doi:10.1097/NMD.0000000000001050
13. van Os J, Hanssen M, Bijl RV, Ravelli A. Strauss (1969) revisited: a psychosis continuum in the general population? Schizophr Res. 2000;45(1–2):11–20. doi:10.1016/S0920-9964(99)00224-8
14. Verdoux H, van Os J. Psychotic symptoms in non-clinical populations and the continuum of psychosis. Schizophr Res. 2002;54(1):59–65. doi:10.1016/S0920-9964(01)00352-8
15. Peters E, Joseph S, Day S, Garety P. Measuring delusional ideation: the 21-item Peters et al. Delusions Inventory (PDI). Schizophr Bull. 2004;30(4):1005–1022. doi:10.1093/oxfordjournals.schbul.a007116
16. Peters ER, Joseph SA, Garety PA. Measurement of delusional ideation in the normal population: introducing the PDI (Peters et al. Delusions Inventory). Schizophr Bull. 1999;25(3):553–576. doi:10.1093/oxfordjournals.schbul.a033401
17. Hardy A, Fowler D, Freeman D, et al. Trauma and hallucinatory experience in psychosis. J Nerv Ment Dis. 2005;193(8):501–507. doi:10.1097/01.nmd.0000172480.56308.21
18. Raune D, Bebbington P, Dunn G, Kuipers E. Event attributes and the content of psychotic experiences in first-episode psychosis. Psychol Med. 2006;36(2):221–230. doi:10.1017/S003329170500615X
19. Koyanagi A, Oh H, Stickley A, Haro JM, DeVylder J. Risk and functional significance of psychotic experiences among individuals with depression in 44 low- and middle-income countries. Psychol Med. 2016;46(12):2655–2665. doi:10.1017/S0033291716001422
20. van Os J, Verdoux H, Maurice-Tison S, et al. Self-reported psychosis-like symptoms and the continuum of psychosis. Soc Psychiatry Psychiatr Epidemiol. 1999;34(9):459–463. doi:10.1007/s001270050220
21. Stefanis NC, Hanssen M, Smirnis NK, et al. Evidence that three dimensions of psychosis have a distribution in the general population. Psychol Med. 2002;32(2):347–358. doi:10.1017/S0033291701005141
22. Cole PM, Putnam FW. Effect of incest on self and social functioning: a developmental psychopathology perspective. J Consult Clin Psychol. 1992;60(2):174–184. doi:10.1037/0022-006X.60.2.174
23. Terr LC. Childhood traumas: an outline and overview. Am J Psychiatry. 1991;148(1):10–20.
24. Heim C, Binder EB. Current research trends in early life stress and depression: review of human studies on sensitive periods, gene-environment interactions, and epigenetics. Exp Neurol. 2012;233(1):102–111. doi:10.1016/j.expneurol.2011.10.032
25. Heim C, Shugart M, Craighead WE, Nemeroff CB. Neurobiological and psychiatric consequences of child abuse and neglect. Dev Psychobiol. 2010;52(7):671–690. doi:10.1002/dev.20494
26. Chiu GR, Lutfey KE, Litman HJ, et al. Prevalence and overlap of childhood and adult physical, sexual, and emotional abuse: a descriptive analysis of results from the Boston Area Community Health (BACH) survey. Violence Vict. 2013;28(3):381–402. doi:10.1891/0886-6708.11-043
27. de Vries B, van Busschbach JT, van der Stouwe ECD, et al. Prevalence Rate and Risk Factors of Victimization in Adult Patients With a Psychotic Disorder: a Systematic Review and Meta-analysis. Schizophr Bull. 2019;45(1):114–126. doi:10.1093/schbul/sby020
28. Parker G, Roussos J, Hadzi-Pavlovic D, et al. The development of a refined measure of dysfunctional parenting and assessment of its relevance in patients with affective disorders. Psychol Med. 1997;27(5):1193–1203. doi:10.1017/S003329179700545X
29. Bousha DM, Twentyman CT. Mother-child interactional style in abuse, neglect, and control groups: naturalistic observations in the home. J Abnorm Psychol. 1984;93(1):106–114. doi:10.1037/0021-843X.93.1.106
30. Li DJ, Hsieh YC, Chiu CD, Lin CH, Chou LS. The moderation of maternal parenting on the association of trauma, dissociation, and psychosis in depressive inpatients. Eur J Psychotraumatol. 2022;13(1):2024974. doi:10.1080/20008198.2021.2024974
31. American Psychiatric Association., American Psychiatric Association. Task Force on DSM-IV. Diagnostic and Statistical Manual of Mental Disorders: DSM-IV-TR.
32. Goldberg LR, Freyd JJ. Self-reports of potentially traumatic experiences in an adult community sample: gender differences and test-retest stabilities of the items in a brief betrayal-trauma survey. J Trauma Dissociation. 2006;7(3):39–63. doi:10.1300/J229v07n03_04
33. Williams JB. A structured interview guide for the Hamilton Depression Rating Scale. Arch Gen Psychiatry. 1988;45(8):742–747. doi:10.1001/archpsyc.1988.01800320058007
34. Vandenberg RJ, Lance CE. A review and synthesis of the measurement invariance literature: suggestions, practices, and recommendations for organizational research. Org Res Methods. 2000;3(1):4–70. doi:10.1177/109442810031002
35. Hayes AF. An Index and Test of Linear Moderated Mediation. Multivariate Behavioral Research. 2015;50(1):1–22. doi:10.1080/00273171.2014.962683
36. Hayes AF. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach.
37. Hayes AF, Matthes J. Computational procedures for probing interactions in OLS and logistic regression: SPSS and SAS implementations. Behav Res Methods. 2009;41(3):924–936. doi:10.3758/BRM.41.3.924
38. Chiu C-D, Ho HL, Tollenaar MS, Elzinga BM, Zhang T. Early relational trauma and self representations: misattributing externally derived representations as internally generated Psychological Trauma: Theory, Research, Practice, and Policy. 2019;11(1):64–72. doi:10.1037/tra0000369
39. Calkins ME, Moore TM, Merikangas KR, et al. The psychosis spectrum in a young U.S. community sample: findings from the Philadelphia Neurodevelopmental Cohort. World Psychiatry. 2014;13(3):296–305. doi:10.1002/wps.20152
40. Dolphin L, Dooley B, Fitzgerald A. Prevalence and correlates of psychotic like experiences in a nationally representative community sample of adolescents in Ireland. Schizophr Res. 2015;169(1–3):241–247. doi:10.1016/j.schres.2015.09.005
41. Kelleher I, Connor D, Clarke MC, et al. Prevalence of psychotic symptoms in childhood and adolescence: a systematic review and meta-analysis of population-based studies. Psychol Med. 2012;42(9):1857–1863. doi:10.1017/S0033291711002960
42. Claridge G. Single indicator of risk for schizophrenia: probable fact or likely myth? Schizophr Bull. 1994;20(1):151–168. doi:10.1093/schbul/20.1.151
43. Linscott RJ, van Os J. Systematic reviews of categorical versus continuum models in psychosis: evidence for discontinuous subpopulations underlying a psychometric continuum. Implications for DSM-V, DSM-VI, and DSM-VII. Annual Review of Clinical Psychology. 2010;6(1):391–419. doi:10.1146/annurev.clinpsy.032408.153506
44. Linscott RJ, van Os J. An updated and conservative systematic review and meta-analysis of epidemiological evidence on psychotic experiences in children and adults: on the pathway from proneness to persistence to dimensional expression across mental disorders. Psychol Med. 2013;43(6):1133–1149. doi:10.1017/S0033291712001626
45. Caldieraro MA, Baeza FLC, Pinheiro DO, et al. Prevalence of psychotic symptoms in those with melancholic and nonmelancholic depression. J Nerv Ment Dis. 2013;201(10):855–859. doi:10.1097/NMD.0b013e3182a5c06e
46. McCarthy JB, Dobroshi Z. Major Depression, Bipolar Disorder and Psychosis in Children. J Infant Child Adolescent Psychotherapy. 2014;13(3):249–261. doi:10.1080/15289168.2014.937984
47. Souery D, Zaninotto L, Calati R, et al. Phenomenology of psychotic mood disorders: lifetime and major depressive episode features. J Affect Disord. 2011;135(1–3):241–250. doi:10.1016/j.jad.2011.07.027
48. Lincoln TM. Relevant dimensions of delusions: continuing the continuum versus category debate. Schizophr Res. 2007;93(1–3):211–220. doi:10.1016/j.schres.2007.02.013
49. Sisti D, Rocchi MBL, Siddi S, et al. Preoccupation and distress are relevant dimensions in delusional beliefs. Compr Psychiatry. 2012;53(7):1039–1043. doi:10.1016/j.comppsych.2012.02.005
50. Spinhoven P, Elzinga BM, Hovens JGFM, et al. The specificity of childhood adversities and negative life events across the life span to anxiety and depressive disorders. J Affect Disord. 2010;126(1–2):103–112. doi:10.1016/j.jad.2010.02.132
51. Isvoranu A-M, van Borkulo CD, Boyette -L-L, et al. A Network Approach to Psychosis: pathways Between Childhood Trauma and Psychotic Symptoms. Schizophr Bull. 2017;43(1):187–196. doi:10.1093/schbul/sbw055
52. van der Kolk BA, van der Hart O. Pierre Janet and the breakdown of adaptation in psychological trauma. Am J Psychiatry. 1989;146(12):1530–1540.
53. Alexander PC. Childhood trauma, attachment, and abuse by multiple partners. Psychol Trauma. 2009;1(1):78–88. doi:10.1037/a0015254
54. Coid J, Petruckevitch A, Feder G, et al. Relation between childhood sexual and physical abuse and risk of revictimisation in women: a cross-sectional survey. Lancet. 2001;358(9280):450–454. doi:10.1016/S0140-6736(01)05622-7
55. Irwin HJ. Violent and Nonviolent Revictimization of Women Abused in Childhood. J Interpers Violence. 1999;14(10):1095–1110. doi:10.1177/088626099014010006
56. Usami S, Sato M, Matsumoto K, et al. [Histology and immunopathology of colonic carcinoma]. Nihon Geka Gakkai Zasshi. 1990;91(6):667–676.
57. Bhavsar V, Boydell J, McGuire P, et al. Childhood abuse and psychotic experiences - evidence for mediation by adulthood adverse life events. Epidemiol Psychiatr Sci. 2017;1:1–10.
58. Lee M-A. Emotional abuse in childhood and suicidality: the mediating roles of re-victimization and depressive symptoms in adulthood. Child Abuse Negl. 2015;44:130–139. doi:10.1016/j.chiabu.2015.03.016
59. Jacobson NC. Current evolutionary adaptiveness of psychiatric disorders: fertility rates, parent−child relationship quality, and psychiatric disorders across the lifespan. J Abnorm Psychol. 2016;125(6):824–839. doi:10.1037/abn0000185
60. Hugill M, Fletcher I, Berry K. Investigation of associations between attachment, parenting and schizotypy during the postnatal period. J Affect Disord. 2017;220:86–94. doi:10.1016/j.jad.2017.05.040
61. Catalan A, Angosto V, Diaz A, et al. Relation between psychotic symptoms, parental care and childhood trauma in severe mental disorders. Psychiatry Res. 2017;251:78–84. doi:10.1016/j.psychres.2017.02.017
62. Monteleone AM, Ruzzi V, Patriciello G, et al. Parental bonding, childhood maltreatment and eating disorder psychopathology: an investigation of their interactions. Eating and Weight Disorders - Studies on Anorexia, Bulimia and Obesity. 2020;25(3):577–589. doi:10.1007/s40519-019-00649-0
63. Tohen M, Khalsa H-MK, Salvatore P, et al. Two-year outcomes in first-episode psychotic depression the McLean-Harvard First-Episode Project. J Affect Disord. 2012;136(1–2):1–8. doi:10.1016/j.jad.2011.08.028
64. Coryell W. Affective syndromes, psychotic features, and prognosis. I. Depression. Arch Gen Psychiatry. 1990;47(7):651–657. doi:10.1001/archpsyc.1990.01810190051007
65. Jager M, Bottlender R, Strauss A, Moller H-J. Fifteen-year follow-up of Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition depressive disorders: the prognostic significance of psychotic features. Compr Psychiatry. 2005;46(5):322–327. doi:10.1016/j.comppsych.2005.02.001
66. Monteiro S, Roque S, de Sá-calçada D, et al. An efficient chronic unpredictable stress protocol to induce stress-related responses in C57BL/6 mice. Front Psychiatry. 2015;6:6. doi:10.3389/fpsyt.2015.00006
67. Khazaal Y, Favrod J, Azoulay S, et al. “Michael’s Game,” a card game for the treatment of psychotic symptoms. Patient Educ Couns. 2011;83(2):210–216. doi:10.1016/j.pec.2010.05.017
68. Jones SR, Fernyhough C. Reliability of factorial structure of the Peters et al. delusions inventory (PDI-21). Pers Individ Dif. 2007;43(4):647–656. doi:10.1016/j.paid.2007.01.018
69. Geraerts E, Schooler JW, Merckelbach H, et al. The reality of recovered memories: corroborating continuous and discontinuous memories of childhood sexual abuse. Psychol Sci. 2007;18(7):564–568. doi:10.1111/j.1467-9280.2007.01940.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Abnormal Serum BDNF and p-mTOR in MDD in Adolescents with Childhood Trauma
Zhao X, Jie H, Wang J, Liu Y, Liu Y, Qin F, Long Q, Hou X, Zhang XW, Wu W, Wu X, Li J, Zeng Y
Neuropsychiatric Disease and Treatment 2024, 20:1513-1522
Published Date: 2 August 2024
Childhood Traumas and Depressive Symptoms: The Moderating Role of Anxiety Sensitivity
Şenyaşar Meterelliyoz K, Baş Uluyol Ö
Neuropsychiatric Disease and Treatment 2024, 20:1889-1900
Published Date: 7 October 2024
The Association Between Childhood Trauma and Prodromal Psychotic Symptoms in Nursing Undergraduates: Mediating Roles of Depression and Anxiety
Wang Y, Cai Q, Xu X, Gu J
Journal of Multidisciplinary Healthcare 2026, 19:617713
Published Date: 3 June 2026