Back to Journals » Advances in Medical Education and Practice » Volume 17
Enhancing Medical Education: The Role of Artificial Intelligence Tools in the Teaching-Learning Process
Authors Kalhori Z ![]() , Bajoulvand R, Zahedian M, Malgard S, Aalaa M
, Bajoulvand R, Zahedian M, Malgard S, Aalaa M ![]() , Asadzandi S
, Asadzandi S ![]()
Received 30 December 2025
Accepted for publication 19 May 2026
Published 23 May 2026 Volume 2026:17 592844
DOI https://doi.org/10.2147/AMEP.S592844
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Md Anwarul Azim Majumder
Zahra Kalhori,1 Razyeh Bajoulvand,2 Mehdi Zahedian,2 Shiva Malgard,1 Maryam Aalaa,3 Shadi Asadzandi4
1Department of Medical Library and Information Science, School of Health Management and Information Sciences, Iran University of Medical Sciences, Tehran, Iran; 2Student Research Committee, Iran University of Medical Sciences, Tehran, Iran; 3Department of Medical Education, School of Medicine, Tehran University of Medical Sciences, Tehran, Iran; 4Health Management and Economics Research Center, Health Management Research Institute, Iran University of Medical Sciences, Tehran, Iran
Correspondence: Shadi Asadzandi, Email [email protected]
Objective: This study aimed to investigate the role of artificial intelligence (AI) tools in enhancing the teaching–learning process in medical education through a scoping review.
Methods: This study was conducted as a scoping review. A comprehensive search of published articles was performed across multiple databases, including Scopus, PubMed, Web of Science, Embase, ERIC, Emerald, and IEEE, covering the period from 2000 to 2024. After removing duplicate records using EndNote software, titles and abstracts were screened, followed by full-text evaluation. The quality of the included studies was assessed using the Critical Appraisal Skills Programme (CASP), and reporting was conducted in accordance with the PRISMA-ScR guidelines.
Results: The findings were categorized into four main themes: (1) domains of application of AI tools, (2) characteristics of AI tools in medical education, (3) applications and effectiveness of AI tools, and (4) challenges associated with AI use.
Conclusion: The integration of AI into the teaching–learning process in medical education offers significant opportunities for developing innovative educational approaches. While AI enhances student engagement, learning outcomes, and satisfaction, it also introduces challenges such as ethical concerns, potential biases, and issues related to data privacy. Addressing these challenges is essential for the effective and responsible implementation of AI in medical education.
Keywords: medical education, artificial intelligence, teaching, learning, students
Introduction
Artificial intelligence (AI) is a transformative technology capable of analyzing complex data, identifying patterns, and providing intelligent solutions. It encompasses machine learning algorithms, natural language processing, and advanced simulation techniques, which have been widely applied across various domains, particularly in healthcare.1 By enabling personalized solutions and the analysis of large datasets, AI has the potential to enhance the efficiency and accuracy of both educational and clinical processes.2
AI has revolutionized medical education by providing innovative tools such as intelligent educational systems and clinical simulations. These technologies personalize learning, provide immediate feedback, and allow educators to design data-driven curricula.3 The teaching–learning process in medical education is a combination of theoretical training, hands-on practice, and clinical experiences, aiming to train physicians who can diagnose and treat accurately.4 This process faces challenges, including resource constraints, differences in student abilities, and time pressures. Striking a balance between scientific knowledge and practical skills requires innovative approaches to improve the quality of education.5 AI can simulate complex clinical scenarios that enhance students’ diagnostic and therapeutic skills.6 However, integrating AI into medical education is riddled with challenges, including ethical concerns and algorithmic biases.7
AI has improved the teaching-learning process in medicine with advanced clinical simulations and large language models (LLMs). Systems such as DxR Clinician provide virtual clinical scenarios that enhance students’ diagnostic skills.8 AI-based surgical simulations also increase students’ accuracy and efficiency.9 Studies have shown that AI can improve diagnostic accuracy by up to 22% and reduce learning time.6 LLMs are employed to automatically assess student responses and provide personalized feedback.10 However, challenges such as algorithmic biases and ethical issues still require attention.7
Some disadvantages of AI in teaching and learning include ethical concerns about its use, the potential for job loss, reduced human interaction in the classroom, limitations in AI programming, additional costs imposed on educational institutions, and the potential decline of traditional teaching roles.11 However, several studies have confirmed the positive effects of AI in medical education.3,5,12,13 At Harvard Medical School, AI courses have been integrated to train researchers who can address complex healthcare problems.14 AI can reduce the burden of administrative tasks, such as clinical documentation, and allow students to focus more on interacting with patients.5 Still, more than half of medical students in a multicenter study raised concerns about AI eroding patient trust or undermining the value of the medical profession.3 Data privacy problems and algorithmic biases are other areas of concern.7,15
The present study aimed to evaluate the role of AI tools in the teaching–learning process in medical education, considering both their potential benefits and associated challenges. The findings can help researchers, educators, and policymakers identify AI tools, analyze their effects on learning, improve teaching methods, develop educational content, assess student performance, create personalized learning environments, and analyze learning data.
To achieve this aim, the study addressed the following research questions:
- What are the main domains of AI application in medical education?
- What are the characteristics of AI tools used in the teaching–learning process?
- How effective are AI tools in improving educational outcomes
- What challenges are associated with the use of AI in medical education?
Method
Design
We choose a scoping review method as the most appropriate method to address our research question “what is the role of AI tools in improving the teaching-learning process in medical education using a literature review”. Our review was guided by the Arksey and O’Malley framework, 2005,16 which entails the following steps: identification of the research question; identification of relevant studies; study selection; charting the data; and collating, summarizing and reporting of the results. Here, we report results of the review guided by the 2018 Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for scoping reviews guidelines (PRISMA-ScR).17
Search Study
All the published articles in Scopus, PubMed, Emerald, ERIC, Web of Science, IEEE, and Embase were searched using an advanced search to obtain scientific evidence related to the research objective. The time limit for retrieving articles was from 2000 to 2024, according to the researchers’ initial survey (scientometrics), research conducted in the field of artificial intelligence in the teaching-learning process has grown significantly since 2000, and a ten-year period was considered for a more comprehensive study. Of course, it should be noted that given that there were not many research activities focused on teaching-learning with a focus on artificial intelligence in medical education, all studies were conducted without restrictions on population or specific field. The operators included Boolean operators, parentheses, and truncation. The keywords used to retrieve articles included artificial intelligence, medical education, and teaching-learning, which were included in the search strategy along with their synonyms after reviewing the MESH. Data extraction was performed on 2024/10/12 and the total number of data retrieved from the databases was 4729 data.
The search strategy in the Web of Science is presented below as an example. A table of all database search strategies is provided in the Supplementary File.
TS=((“Artificial Intelligence” OR AI OR “AI-written” OR “AI-generated” OR chatbot* OR ChatGPT OR “ChatGPT-generated” OR “GPT3” OR “OpenAI” OR “generative artificial intelligence” OR “natural language processing” OR NLP) AND (“medical education” OR ME OR “medical instruction” OR “medical pedagog*” OR “medical teaching” OR “medical training” OR “medical tuition” OR “Medical Sciences Education” OR “Health Profession Education” OR “Biomedical Education”) AND (“teaching-learning” OR teaching AND learning OR “adult education” OR andrology OR “adult teaching” OR “adult learning”))
After searching the databases, the retrieved resources were entered into EndNote 21 software.
Eligibility for Research Question
Our research question was: what is the role of AI tools in improving the teaching-learning process in medical education using a literature review? We used the Population, Concept and Context (PCC) framework to determine the eligibility of our research question for this scoping review. Population is AI tools; Concept is teaching-learning process in medical education literatures. Context is medical education.
Inclusion and Exclusion Criteria
The inclusion criteria for articles were: relevance of the article’s subject area to the research objective and being an original article. The exclusion criteria were gray literature, theses, conference papers, review articles, languages other than English, lack of access to the full text, and being irrelevant to AI tools used in the teaching-learning process in medical education.
Study selection occurred in three stages. In the first stage, duplicate data were removed in EndNote, and then the titles and abstracts were screened (4617 literatures). Two authors independently reviewed and screened all the retrieved articles. After that, the full text of the articles was evaluated (335 literatures). In cases of consensus, the document was retained, and in cases of disagreement, a third person was asked to review the documents, and a decision was made after a discussion.
In this study, medical education was considered broadly to include bioscience education and healthcare education within medical science education (basic and clinical fields). Therefore, studies from these related domains were not excluded.
Charting of Data
We extracted data on the following: author and year of publication, objective, study design, population, field of study, AI tool charectristic and key results.
Collating, Summarizing and Reporting of the Results
We employed thematic content analysis to examine results from the selected articles (44 literatures). We utilized the maxqda24 package to identify the themes from the included articles. The data was evaluated by two reviewers. Initially, the reviewers acquainted themselves with the articles’ content. Secondly, the findings presented in the articles were classified into categories according to the study context and subsequently organized into nodes.
Quality Appraisal of Included Primary Studies
In this way, information on AI tools used in the teaching-learning process was extracted. CASP was employed to assess the quality of the retrieved studies, and PRISMA was followed in drawing up the report, which included the process of searching, screening, and selecting articles (Figure 1).
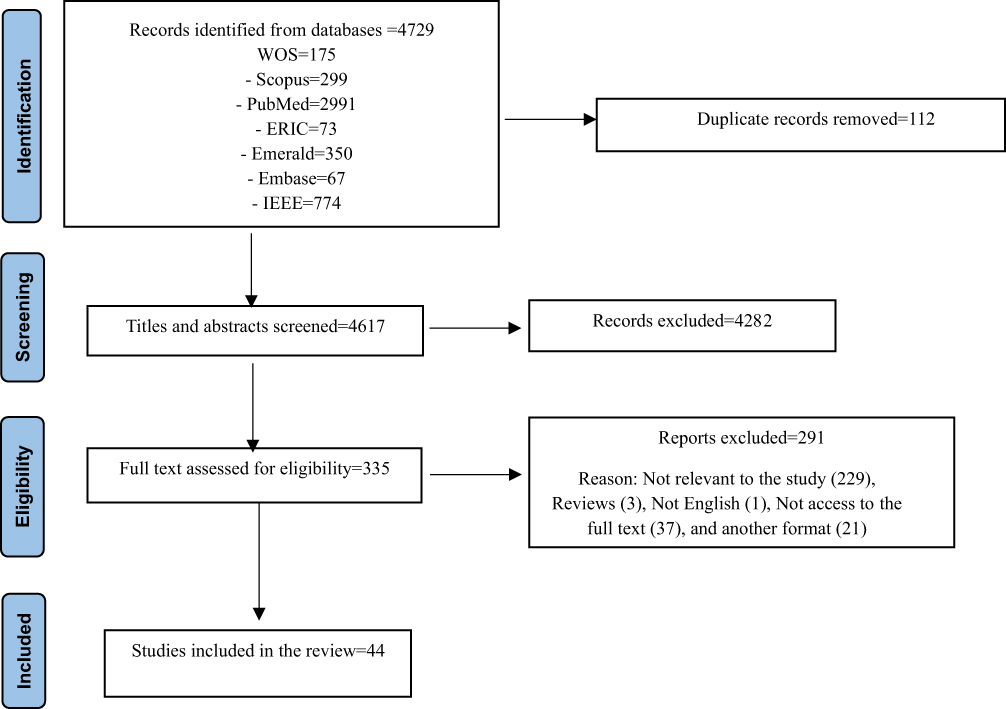 |
Figure 1 The process of searching, screening, and selecting articles on AI tools in the teaching-learning process in medical science education. |
Results
This scoping review identified 4729 studies from 2000 to 2024. After removing 112 duplicates, 4617 studies were screened. Title and abstract screening excluded 4282 studies, and 335 studies remained for full-text evaluation. Finally, 44 original studies related to the application of AI in the teaching-learning process in medicine were analyzed. Table 1 presents the bibliographic information of the articles, objective, method, population, AI tool used, and a summary of the effect of this tool on the teaching-learning process.
 |
Table 1 Characteristics of the Articles and AI Tools Affecting the Teaching-Learning Process of Medical Education |
Bibliographic Information of Articles
Research methods included quantitative, qualitative, and mixed methods. Quasi-experimental designs1,18 compared AI groups with traditional groups, such as cardiovascular disease training with AI simulation. Randomized controlled trials12,13,39–56,59 were common in surgery, nursing, and anesthesiology and measured the effectiveness of AI. Qualitative phenomenological studies21,34,37,38 examined students’ emotional experiences, such as nurses’ feelings in clinical simulations. Mixed-methods studies1,19,23,26 combined quantitative (eg., test scores) and qualitative data (eg., student opinions). Descriptive studies20,27,31,35,36,59 analyzed the performance of AI tools, such as ChatGPT, in tests. Cross-sectional35 and pilot studies39,40 evaluated the feasibility of integrating AI. This diversity of methods demonstrated multiple approaches, and heterogeneity made direct comparisons difficult.
The target population included diverse groups of learners. Medical students included 66 first-year clinical students at Nantong University,1 41 clinical students at Qiqihar University,18 and 52 third-year undergraduate and first-year MSc students at the University of Zurich.3 In addition, 728 pediatric residents and 196 faculty members from 15 universities in Indonesia participated in a cross-sectional study.36 Other groups included 77 medical interns (42 men and 35 women) at Sun Yat-sen University,25 nursing students in several studies on project-based learning,34,37,38,45,50 radiology technicians in imaging training,35 and dental students in dental morphology training.49,52 Smaller, more specialized populations included 26 neurosurgery students56 and 8 healthy adults in neurological rehabilitation.41 Lack of sex-related information in most studies limited sex-related analyses.
The fields of study were mostly general medicine.1,12,18,19,21,24–28,30,31,36,39–41,44,45,53,54,59 Sub-disciplines of medicine included radiology29,35,46,47 for image interpretation training, ophthalmology14,15 for identifying pathological myopia, psychiatry (23) for designing educational tests, neurosurgery22,56,57 for practicing surgical techniques, and pharmacology20 for identifying learning objectives. Nonmedical disciplines included nursing34,37,38,50 for project-based training, dentistry49,52 for learning dental morphology, anesthesiology13,51 for ultrasound-guided nerve blocks, cardiology1,13,18 for educational simulations, antimicrobial training,37 trans-esophageal echocardiography,39 neurological rehabilitation,41 and hemodialysis training.45 This diversity demonstrates AI’s ability to cover specialized and interdisciplinary fields, but general medicine remained dominant.
Overall, research conducted on AI and medical education pursued broad and common goals focusing on improving students’ learning experience and capabilities. A central objective was to strengthen self-efficacy and develop self-directed learning among students; in other words, AI tools were designed and used in a way that allowed students to learn with greater confidence and independence.18 In addition, special attention was paid to the impact of these technologies on students’ mental and motivational state; research shows intelligent systems, when used correctly, can increase motivation and reduce anxiety in educational processes.24 Ultimately, all these efforts were aimed at comprehensively improving students’ clinical skills; AI, as a powerful auxiliary tool, played a significant role in improving the practical and clinical abilities of the future generation of physicians.25 A review of the selected studies suggests that using AI in medical education can be explained in terms of several main factors, including domains of use, tools used, application and effectiveness, and challenges associated with AI use.
Domains of Use of AI Tools
The scope of application of AI tools in medical education is very wide, covering various domains. In cardiovascular diseases, simulation approaches aided by AI have helped improve students’ performance and clinical thinking.1 Similarly, in medical imaging, AI-assisted diagnostic software (AISD) has facilitated understanding of 3D images and image interpretation skills.18 AI-based training in radiology has also received positive feedback.29 In other fields, such as pharmacy, AI platforms have been utilized to identify learning objectives and generate questions related to medications and antihypertensive treatments.20 This technology has also been employed in clinical and hospital settings to address medical knowledge gaps, aid decision-making, and manage complex care.21
At a more specialized level, neurosurgery has been using ChatGPT for board exam preparation.22 In addition, in psychiatry, the tool has been used to generate training scenarios and compare them with human scenarios.23 Ophthalmology has utilized AI systems for disease diagnosis32 and AI-guided problem-based learning modules.33 Finally, pediatric education has focused on the assessment of clinical skills and readiness for AI integration.25,36
AI Tools in Medical Education (Specifications)
Among the various AI technologies, ChatGPT has been recognized as one of the most prominent and widely used tools.19,25,30 It has shown great potential in facilitating learning, improving communication and clinical skills, and even competing with students in specialized exams. Other LLMs have also been considered as powerful tools to support learning and clinical processes.21,26 In addition, a wide range of other innovative tools has been investigated. These include AI-powered scenario-based simulation software1 used for cardiovascular disease education; AI-assisted image recognition (AISD) software using advanced algorithms such as ResU-net for 3D image analysis;18 various AI platforms such as Sage Poe and Claude-Instant used as AI search engines or information retrieval in pharmacy education;20 AI-enhanced serious games for teaching critical appraisal skills;41 robot-based adaptive learning systems to train specific motor patterns;42 self-learning software to enhance clinical skills in specialized areas;43 virtual simulator-based tools and virtual patients improving clinical reasoning and problem-based learning;44,45 smart classrooms combined with PACS simulators and electronic content;47 and interactive educational modules and 3D software significantly assisting student learning in areas such as neurology and anatomy.48,50,51
Application and Effectiveness of AI Tools
A wide range of AI tools has been used in medical education, each with its unique advantages. For example, LLMs such as ChatGP have been effective in bridging knowledge gaps, aiding differential diagnosis, and content creation.19,21,25–27,36 Furthermore, AI-based simulations and scenarios are effective tools for teaching surgical techniques and clinical diagnosis, as well as understanding physiological concepts.1,38,40,44,45,54,59 In addition, image analysis and diagnosis software, such as those using advanced algorithms18 and smart classrooms,47 have helped improve students’ diagnostic and practical skills. Besides, interactive tools, simulators, and educational games28,41,48–51,54 have been increasingly incorporated into the educational process and have demonstrated their effectiveness in learning. Overall, the findings of this section are divided into two subgroups: (a) improving students’ performance and skills, and (b) increasing their satisfaction, motivation, and learning experience.
Improving Students’ Performance and Skills
Several studies have demonstrated significant positive effects of AI-based tools and approaches on improving students’ academic performance and clinical skills.1,12,13,18,25,28,38,40–51,56,59 These improvements include increased scores on diagnostic tests, improved academic self-efficacy, enhanced self-directed learning, and improved clinical reasoning.18,54 Compared with traditional methods, combining AI-based approaches such as PPT+AI has resulted in higher scores on challenging tests.28 Tools such as eCREST have also been effective in improving clinical reasoning and reducing diagnostic errors.44 Besides, web-based virtual patients (D-PBL) outperformed linear PBL on exams.45 Reducing side effects and increasing self-assessment scores are the other benefits of using AI.13
Increasing Student Satisfaction, Motivation, and Learning Experience
Many studies have emphasized increasing student satisfaction and motivation by integrating AI technologies. In general, AI tools have increased student satisfaction, improved learning experience, and even reduced anxiety.13,19,21,26,27,29,36,37,47,48,51,53,56,57 For example, LLMs such as ChatGPT have been widely utilized in content creation, ideation, and simplification of concepts to enhance the learning experience.26,27 Interactive and 3D tools and new approaches, such as AI-RADS29 and smart classrooms, can also enhance student satisfaction and enjoyment in the learning process.47,48,51
Challenges of AI Use
Besides numerous benefits, studies have highlighted key challenges and considerations in using AI in medical education. One of the most important challenges is the accuracy and validity of AI-generated content, which highlights the need for expert review.20,22,27,36 Concerns have also been raised about biases, misinformation, and ethical issues in the use of these technologies.21 Some studies have emphasized the need for initial guidance and training for students.53,57 Student preferences can also influence the adoption of different tools; for instance, some students’ preference for traditional simulations over web-based simulations suggests the importance of considering diversity in learning styles.55
Discussion
The present study conducted a scoping review to examine the role of AI tools in improving the teaching–learning process in medical education and to discuss the challenges of using AI in this field. In this section, the main findings are discussed in four categories: (1) domains of use of AI tools, (2) characteristics of AI tools in medical education, (3) application and effectiveness of AI tools, and (4) challenges of using AI.
Domains of Use of AI Tools
AI tools have been used in teaching–learning processes in medical education across various disciplines, including cardiology, medical imaging, psychiatry, pediatrics, ophthalmology, and pharmacy. Their application spans theoretical training, preclinical education, and clinical practice,60 This broad integration reflects the increasing need to bridge the gap between theoretical knowledge and clinical application. AI enables students to engage in clinical decision-making within controlled and simulated environments,61 which is particularly valuable given the ethical and practical limitations of training with real patients.
AI-based virtual reality and simulation platforms allow learners to interact with virtual patients in realistic scenarios, enabling repeated practice in a safe environment.62 This repeated exposure is likely to strengthen clinical reasoning through pattern recognition and experiential learning. Supporting this, immersive AI-driven platforms such as medical tr.AI.ning provide interactive, context-rich training environments that facilitate clinical decision-making and enhance experiential learning.62
While AI-driven tools, particularly generative AI (GenAI), have demonstrated strong potential in supporting cognitive and decision-making skills, their effectiveness in developing hands-on clinical and procedural skills remains limited. AI-based environments cannot fully replicate the complexity, unpredictability, and nuanced interpersonal dynamics of real patient interactions. Therefore, AI should be considered a complementary tool rather than a replacement for real clinical experience.
Characteristics of AI Tools in Medical Education
AI tools can be broadly categorized into (a) generative language models, such as chatbots, and (b) AI-driven tools designed to facilitate teaching–learning processes. This distinction highlights two complementary dimensions of AI in education: cognitive support and experiential training. Evidence suggests that the future of medical education will be significantly influenced by the integration of these technologies.63 Generative models, such as ChatGPT, extend beyond information retrieval by enabling interactive reasoning and supporting knowledge synthesis.21 In contrast, AI-driven systems, including simulation platforms and diagnostic tools, enhance procedural and applied skills. The combined use of these tools contributes to improvements in both knowledge acquisition and clinical competence.
However, these tools should be used as adjuncts rather than replacements for traditional education. Concerns regarding bias, misinformation, and reliability in AI-generated outputs require careful supervision and alignment with evidence-based medical resources.21,64 Furthermore, the future development of AI tools depends on effective multidisciplinary collaboration among clinicians, educators, and technical experts. Without appropriate guidance, there is also a risk that students may become overly reliant on AI tools, potentially weakening independent clinical reasoning.
Application and Effectiveness of AI Tools
The functions of AI in medical education can be categorized into (a) improving students’ performance and skills and (b) enhancing satisfaction, motivation, and learning experience. The findings of this review indicate that AI-based approaches consistently improve clinical performance, diagnostic accuracy, and self-directed learning. These effects are largely driven by personalized learning pathways and immediate feedback mechanisms, which promote deeper engagement.21
Empirical evidence further supports these findings. AI-based simulation approaches significantly improve clinical thinking and practical skills compared to traditional methods.1 Similarly, AI-assisted diagnostic tools, such as AISD software, enhance image interpretation skills, self-efficacy, and learner autonomy through real-time feedback and 3D visualization.18
The effectiveness of GenAI is highly dependent on instructional design. AI tools are most beneficial when integrated into structured learning environments with clear objectives, guided interaction, and opportunities for critical evaluation of outputs. In contrast, unstructured use may result in passive learning and superficial understanding. Consistent with previous evidence,24,65 AI integration is also associated with increased motivation and reduced anxiety, reflecting a shift toward more learner-centered educational models.
Challenges of Using AI
While AI offers substantial benefits, its implementation in medical education is associated with several ethical, technical, and organizational challenges.65–67 Ethical concerns include algorithmic bias, lack of transparency, and potential inaccuracies in AI-generated content, which may affect learning quality and clinical decision-making.21
Information security is another critical issue, particularly in the context of sensitive medical data. Although some AI platforms claim to provide enterprise-level data protection, concerns remain regarding data storage, unauthorized access, and potential misuse of user inputs.65–67
In addition, although some AI tools are freely available, the large-scale implementation of AI in educational institutions often requires significant investment in infrastructure, integration, training, and maintenance. These hidden costs may limit accessibility, especially in resource-constrained settings.
From a pedagogical perspective, overreliance on AI tools may reduce critical thinking and independent problem-solving skills. Furthermore, variability in study designs and outcomes highlights the lack of standardized evaluation frameworks for AI in medical education. Addressing these challenges requires clear policies, ethical guidelines, and the promotion of AI literacy to ensure safe and effective integration.
Conclusion
The findings of this scoping review demonstrate that artificial intelligence plays a transformative role in enhancing the teaching–learning process in medical education. A wide range of AI tools—including large language models such as ChatGPT, AI-driven virtual patient platforms, immersive simulation systems (eg., medical tr.AI.ning), and AI-assisted diagnostic tools such as AISD software—have shown significant potential in improving clinical reasoning, diagnostic accuracy, and student engagement.
These technologies support personalized learning, provide immediate feedback, and facilitate the integration of theoretical knowledge with practical clinical skills. In particular, simulation-based and AI-driven interactive tools enable safe, repetitive practice in complex clinical scenarios, thereby enhancing experiential learning and competency development.
However, despite these benefits, challenges such as algorithmic bias, data privacy concerns, lack of transparency, and the risk of overreliance on AI remain critical issues that must be addressed. Therefore, the effective implementation of AI in medical education requires the development of clear guidelines, ethical frameworks, and robust evaluation systems.
Future efforts should focus on integrating AI literacy into medical curricula, strengthening infrastructure, and conducting longitudinal and comparative studies to better understand the long-term impact of AI on clinical competence and professional development. A balanced and evidence-based approach will be essential to ensure that AI serves as a complementary tool that enhances, rather than replaces, the role of educators in medical training.
Future research may also focus on specific learner populations, such as undergraduate students, postgraduate trainees, or residents, to better understand how AI-based educational tools influence teaching–learning processes within each group.
To maximize the effectiveness of AI tools in medical education, educators should integrate them within structured learning designs that include clear objectives, guided interaction, and opportunities for critical evaluation of AI-generated outputs. AI tools are most effective when used to support active learning, clinical reasoning, and personalized feedback rather than passive information retrieval. Conversely, uncritical reliance on AI outputs, lack of supervision, and substituting AI for real clinical experience should be avoided, as these practices may hinder the development of independent thinking and practical skills.
Implications for Stakeholders and Policymakers
The findings of this study suggest that policymakers and educational stakeholders should develop clear guidelines for the ethical and effective integration of AI in medical education. Investment in infrastructure, faculty training, and AI literacy programs is essential to support implementation. In addition, regulatory frameworks should be established to address data privacy, transparency, and algorithmic bias. Collaboration between educators, clinicians, and technology developers is also recommended to ensure that AI tools align with educational needs and standards.
AI Declaration
Artificial intelligence was not used in this article.
Data Sharing Statement
The data can be requested from the corresponding author.
Ethical Considerations
This research received ethical approval (IR.IUMS.REC.1403.695) from Iran University of Medical Sciences.
Acknowledgment
This article is a part of a research project approved by Iran University of Medical Sciences in 2023, with the research code 1403-2-37-30887.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The present research was conducted with the support of Iran University of Medical Sciences. The funder had no role in data collection, analysis, or manuscript preparation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zheng K, Shen Z, Chen Z, Che C, Zhu H. Application of AI-empowered scenario-based simulation teaching mode in cardiovascular disease education. BMC Medical Education. 2024;24(1):1003. doi:10.1186/s12909-024-05977-z
2. Goodfellow I, Bengio Y, Courville A. Deep Learning. Cambridge: MIT Press; 2016.
3. Civaner MM, Uncu Y, Bulut F, Chalil EG, Tatli A. Artificial intelligence in medical education: a cross-sectional needs assessment. BMC Medical Education. 2022;22(1):772. doi:10.1186/s12909-022-03852-3
4. Frenk J, Chen L, Bhutta ZA, Cohen J, Crisp N, Evans T. Health professionals for a new century: transforming education to strengthen health systems in an interdependent world. The Lancet. 2010;376(9756):
5. Savage TR. Artificial intelligence in medical education. Academic Medicine. 2021; 96(9):1229–21.
6. Chan KS, Zary N. Applications and challenges of implementing artificial intelligence in medical education: integrative review. JMIR Med Educ. 2019;5(1):e13930.
7. Zarei M, Mamaghani HE, Abbasi A, Hosseini M-S. Application of artificial intelligence in medical education: a review of benefits, challenges, and solutions. Medicina Clínica Práctica. 2024;7(2):100422. doi:10.1016/j.mcpsp.2023.100422
8. Mir MM, Mir GM, Raina NT, et al. Application of artificial intelligence in medical education: current scenario and future perspectives. J Advanc Med Educ Professional. 2023;11(3):133.
9. Sun L, Yin C, Xu Q, Zhao W. Artificial intelligence for healthcare and medical education: a systematic review. Am J Translat Res. 2023;15(7):4820.
10. Feigerlova E, Hani H, Hothersall-Davies E. A systematic review of the impact of artificial intelligence on educational outcomes in health professions education. BMC Med Educ. 2025;25(1):129. doi:10.1186/s12909-025-06719-5
11. Al-Tkhayneh KM, Alghazo EM, Tahat D. The advantages and disadvantages of using artificial intelligence in education. J Educ Soc Res. 2023;13(4):105. doi:10.36941/jesr-2023-0094
12. Barthelemy FX, Segard J, Fradin P, Hourdin N, Batard E, Pottier P. ECG interpretation in Emergency Department residents: an update and e-learning as a resource to improve skills. Eur J Emerg Med. 2017;24(2):149–156. doi:10.1097/MEJ.0000000000000312
13. Cai N, Wang G, Xu L, Zhou Y, Chong H, Zhao Y. Examining the impact perceptual learning artificial-intelligence-based on the incidence of paresthesia when performing the ultrasound-guided popliteal sciatic block: simulation-based randomized study. BMC Anesthesiol. 2022;22(1):392. doi:10.1186/s12871-022-01937-6
14. Gehrman E. How Generative AI Is Transforming Medical Education. Harvardedu; 2024.
15. Obermeyer Z, Powers B, Vogeli C, Mullainathan S. Dissecting racial bias in an algorithm used to manage the health of populations. Science. 2019;366(6464):447–453. doi:10.1126/science.aax2342
16. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. doi:10.1080/1364557032000119616
17. Tricco AC, Lillie E, Zarin W, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
18. Wang D, Huai B, Ma X, et al. Application of artificial intelligence-assisted image diagnosis software based on volume data reconstruction technique in medical imaging practice teaching. BMC Med Educ. 2024;24(1):405. doi:10.1186/s12909-024-05382-6
19. Thomae AV, Witt CM, Barth JJJME. Integration of ChatGPT into a course for medical students: explorative study on teaching scenarios, students’ perception, and applications. JMIR Med Educ. 2024;10(1):e50545. doi:10.2196/50545
20. Sridharan K, Sequeira R. Artificial intelligence and medical education: application in classroom instruction and student assessment using a pharmacology & therapeutics case study. BMC Med Educ. 2024;24(1):431. doi:10.1186/s12909-024-05365-7
21. Skryd A, Lawrence K. ChatGPT as a tool for medical education and clinical decision-making on the wards: case study. JMIR Format Res. 2024;8:e51346. doi:10.2196/51346
22. Powers AY, McCandless MG, Taussky P, Vega RA, Shutran MS, Moses ZBJC. Educational limitations of ChatGPT in neurosurgery board preparation. Cureus. 2024;16(4).
23. Hudon A, Kiepura B, Pelletier M, Phan V. Using ChatGPT in psychiatry to design script concordance tests in undergraduate medical education: mixed methods study. JMIR Med Educ. 2024;10:e54067. doi:10.2196/54067
24. Beketov V, Lebedeva M, Taranova MJCP. The use of artificial intelligence in teaching medical students to increase motivation and reduce anxiety during academic practice. Curr Psychol. 2024;43(16):14367–14377.
25. Ba H, Zhang L, Yi Z. Enhancing clinical skills in pediatric trainees: a comparative study of ChatGPT-assisted and traditional teaching methods. BMC Med Educ. 2024;24(1):558. doi:10.1186/s12909-024-05565-1
26. Magalhães S, Cruz-Correia R. Incorporating ChatGPT in medical informatics education: mixed methods study on student perceptions and experiential integration proposals. JMIR Med Educ. 2024;10;e51151.
27. Alfertshofer M, Knoedler S, Hoch CC, et al. Analyzing question characteristics influencing ChatGPT’s performance in 3000 USMLE®-style questions. Med Sci Educ. 2025;35(1):257–267. doi:10.1007/s40670-024-02176-9
28. Sanchez-Gonzalez M, Terrell MJC. Flipped classroom with artificial intelligence: educational effectiveness of combining voice-over presentations and AI. Cureus. 2023;15(11).
29. Lindqwister AL, Hassanpour S, Levy J, JMJFiMT S. AI-RADS: successes and challenges of a novel artificial intelligence curriculum for radiologists across different delivery formats. Front Med Technol. 2023;4:1007708. doi:10.3389/fmedt.2022.1007708
30. Ghosh A, Jindal NM, Gupta VK, Bansal E, Bajwa NK, Sett AJC. Is ChatGPT’s knowledge and interpretative ability comparable to first professional MBBS (Bachelor of medicine, bachelor of surgery) students of India in taking a medical biochemistry examination? Cureus. 2023;15(10).
31. Friederichs H, Friederichs WJ, März M. ChatGPT in medical school: how successful is AI in progress testing? Med Educ Online. 2023;28(1):2220920. doi:10.1080/10872981.2023.2220920
32. Fang Z, Xu Z, He X, Han W; Biology D. Artificial intelligence-based pathologic myopia identification system in the ophthalmology residency training program. Front Cell Develop Biol. 2022;10:1053079. doi:10.3389/fcell.2022.1053079
33. Wu D, Xiang Y, Wu X, et al. Artificial intelligence-tutoring problem-based learning in ophthalmology clerkship. Ann Transla Med. 2020;8(11):700. doi:10.21037/atm.2019.12.15
34. Kong W, Ning Y, Ma T, et al. Experience of undergraduate nursing students participating in artificial intelligence+ project task driven learning at different stages: a qualitative study. BMC Nurs. 2024;23(1):314. doi:10.1186/s12912-024-01982-1
35. Stogiannos N, Jennings M, St George C, et al. The American Society of Radiologic Technologists (ASRT) AI Educator Survey: a cross-sectional study to explore knowledge, experience, and use of AI within education. J Med Imag Radiat Sci. 2024;55(4):101449. doi:10.1016/j.jmir.2024.101449
36. Pudjiadi AH, Alatas FS, Faizi M, et al. Integration of artificial intelligence in pediatric education: perspectives from pediatric medical educators and residents. Healthcare Informatics Res. 2024;30(3):244–252.
37. Driesnack S, Rücker F, Dietze-Jergus N, Bondarenko A, Pletz MW, Viehweger -AJJ-AR. A practice-based approach to teaching antimicrobial therapy using artificial intelligence and gamified learning. JAC-Antimicrob Resist. 2024;6(4):dlae099. doi:10.1093/jacamr/dlae099
38. Leon C, Mano LY, Fernandes D, Paula RAP, Brasil G, Ribeiro L. Artificial intelligence in the analysis of emotions of nursing students undergoing clinical simulation. Revista brasileira de enfermagem. 2023;76:e20210909.
39. Linganna RE, Patel SJ, Al Ghofaily L, et al. Pilot study suggests smartphone application knowledge improves resident transesophageal echocardiography knowledge: a randomized controlled trial. J Cardiothoracic Vascular Anesthesia. 2020;34(8):2126–2132. doi:10.1053/j.jvca.2019.12.051
40. Malpani A, Vedula SS, Lin HC, Hager GD, Taylor RH. Effect of real-time virtual reality-based teaching cues on learning needle passing for robot-assisted minimally invasive surgery: a randomized controlled trial. Int J Comput AssistRadiol Surg. 2020;15(7):1187–1194. doi:10.1007/s11548-020-02156-5
41. Mlika M, Dziri C, Mezni FJLTM. About the efficacy of a serious game in critical appraisal learning: a cluster randomized controlled trial. La Tunisie Medicale. 2022;100(8):578.
42. Patton JL, Mussa-Ivaldi F. Robot-assisted adaptive training: custom force fields for teaching movement patterns. IEEE Transact Bio Med Engineer. 2004;51(4):636–646. doi:10.1109/TBME.2003.821035
43. Pioche M, Rivory J, Nishizawa T, et al. Randomized comparative evaluation of endoscopic submucosal dissection self-learning software in France and Japan. Endoscopy. 2016;48(12):1076–1083. doi:10.1055/s-0042-116946
44. Plackett R, Kassianos AP, Kambouri M, et al. Online patient simulation training to improve clinical reasoning: a feasibility randomised controlled trial. BMC Med Educ. 2020;20(1):245. doi:10.1186/s12909-020-02168-4
45. Poulton T, Ellaway RH, Round J, Jivram T, Kavia S, Hilton S. Exploring the efficacy of replacing linear paper-based patient cases in problem-based learning with dynamic Web-based virtual patients: randomized controlled trial. J Med Internet Res. 2014;16(11):e240. doi:10.2196/jmir.3748
46. Pun S-K, Chiang VC-L, Choi K-SJCC. A computer-based method for teaching catheter-access hemodialysis management. Comput Informat, Nurs. 2016;34(10):476–483. doi:10.1097/CIN.0000000000000262
47. Qin Y, Huang Z, Yu J, et al. Practice-based learning using smart class: a competency-based model in undergraduate radiology education. Academic Radiol. 2022;29(1):150–157. doi:10.1016/j.acra.2020.09.028
48. Rajan KK, Pandit ASJBME. Comparing computer-assisted learning activities for learning clinical neuroscience: a randomized control trial. BMC Med Educ. 2022;22(1):522. doi:10.1186/s12909-022-03578-2
49. Randell T, Hall M, Bizo L, Remington B. DTkid: interactive simulation software for training tutors of children with autism. J Autism Develop Disord. 2007;37(4):637–647. doi:10.1007/s10803-006-0193-z
50. Reich S, Simon JF, Ruedinger D, Shortall A, Wichmann M, Frankenberger R. Evaluation of two different teaching concepts in dentistry using computer technology. Advanc Health Sci Educ. 2007;12(3):321–329. doi:10.1007/s10459-006-9004-8
51. Rodríguez-López ES, Calvo-Moreno SO, Fernández-Pola EC, Fernández-Rodríguez T, Guodemar-Pérez J, Ruiz-López M-A. Learning musculoskeletal anatomy through new technologies: a randomized clinical trial. Revista latino-americana de enfermagem. 2020;28:e3281. doi:10.1590/1518-8345.3237.3281
52. Bateman J, Allen ME, Kidd J, Parsons N, Davies D. Virtual patients design and its effect on clinical reasoning and student experience: a protocol for a randomised factorial multi-centre study. BMC Med Educ. 2012;12(62). doi:10.1186/1472-6920-12-62
53. Bock A, Elvers D, Goloborodko E, et al; Oral Medicine, Oral Pathology, Radiology O. An innovative PantoDict program for reporting panoramic radiographs using automatic speech recognition in dental education: a randomized observer-blinded study. Oral Surg Oral Med Oral Pathol Oral Radiol. 2021;132(1):104–111. doi:10.1016/j.oooo.2020.10.002
54. Boet S, Bould MD, Schaeffer R, et al. Learning fibreoptic intubation with a virtual computer program transfers to ‘hands on’improvement. Eur J Anaesthesiol. 2010;27(1):31–35. doi:10.1097/EJA.0b013e3283312725
55. Cendan JC, Johnson T. Enhancing learning through optimal sequencing of web-based and manikin simulators to teach shock physiology in the medical curriculum. Advanc Physiol Educ. 2011;35(4):402–407. doi:10.1152/advan.00061.2011
56. Fernández-Alemán JL, López-González L, González-Sequeros O, Jayne C, López-Jiménez JJ, Toval A. The evaluation of i-SIDRA - a tool for intelligent feedback - in a course on the anatomy of the locomotor system. Int J Med Inform. 2016;94:172–181. doi:10.1016/j.ijmedinf.2016.07.008
57. Gasco J, Patel A, Ortega-Barnett J, et al. Virtual reality spine surgery simulation: an empirical study of its usefulness. Neurol Res. 2014;36(11):968–973. doi:10.1179/1743132814Y.0000000388
58. Guha P, Lawson J, Minty I, Kinross J, Martin G. Can mixed reality technologies teach surgical skills better than traditional methods? A prospective randomised feasibility study. BMC Med Educ. 2023;23(1):144. doi:10.1186/s12909-023-04122-6
59. Fergusson SJ, Aka JJ, Hennessy CM, Wilson AJ, Parson SH, Harrison EM. Examining the impact of audience response systems on student performance in anatomy education: a randomised controlled trial. Scottish Med J. 2018;63(1):16–21. doi:10.1177/0036933017741409
60. Roveta A, Castello LM, Massarino C, Francese A, Ugo F, Maconi A. Artificial intelligence in medical education: a narrative review on implementation, evaluation, and methodological challenges. Ai. 2025;6(9):227. doi:10.3390/ai6090227
61. Pohn B, Mehnen L, Fitzek S, Choi KE, Braun RJ, Hatamikia S. Integrating artificial intelligence into pre-clinical medical education: challenges, opportunities, and recommendations. In: Frontiers in Education. edn: Frontiers Media SA; 2025.
62. Mergen M, Junga A, Risse B, Valkov D, Graf N, Marschall B. Immersive training of clinical decision making with AI driven virtual patients–a new VR platform called medical training. GMS J Med Educ. 2023; 40(2):Doc18.
63. Karabacak M, Ozkara BB, Margetis K, Wintermark M, Bisdas S. The advent of generative language models in medical education. JMIR Med Educ. 2023;9:e48163. doi:10.2196/48163
64. Ghorashi N, Ismail A, Ghosh P, Sidawy A, Javan R, Ghorashi NS. AI-powered chatbots in medical education: potential applications and implications. Cureus. 2023;15(8).
65. Rabie RM. The role of artificial intelligence and personalized education in medical curriculum: a systematic review of applications and challenges. Facul Educ J Alexandria Univer. 2023;33(4):365–384.
66. Grunhut J, Marques O, Wyatt AT. Needs, challenges, and applications of artificial intelligence in medical education curriculum. JMIR Med Educ. 2022;8(2):e35587. doi:10.2196/35587
67. Khakpaki A. Advancements in artificial intelligence transforming medical education: a comprehensive overview. Med Educ Online. 2025;30(1):2542807. doi:10.1080/10872981.2025.2542807
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Implementation of Learning Communities at Khalifa University College of Medicine and Health Sciences, Abu Dhabi, United Arab Emirates
Hernandez Jr R, Lou J, Al-Omari B, Aloum L, Kanj S, Ismaiel S, Rock J
Advances in Medical Education and Practice 2022, 13:577-583
Published Date: 28 May 2022
Impact of COVID-19 Pandemic on Medical Education: A Cross-Sectional Study in the Western Region of Saudi Arabia
Samannodi M, Bulkhi A, Alwafi H, Bukhari R, Salawati E, Hafiz B, Minshawi F, Dahlawi M, Kamfar S, Halawani H, Naser AY, Mandora R, Alshekh Ali M, Almatrafi MA
Advances in Medical Education and Practice 2022, 13:741-754
Published Date: 21 July 2022
Clinicians’ and Students’ Perceptions and Attitudes Regarding the Anatomical Knowledge of Medical Students
Almizani MS, Alotaibi MA, Bin Askar MF, Albaqami NM, Alobaishi RS, Arafa MA, Jumaa MI
Advances in Medical Education and Practice 2022, 13:1251-1259
Published Date: 4 October 2022
Comparing Knowledge Acquisition and Retention Between Mobile Learning and Traditional Learning in Teaching Respiratory Therapy Students: A Randomized Control Trial
Alhamad BR, Agha S
Advances in Medical Education and Practice 2023, 14:333-342
Published Date: 6 April 2023
Delving into the Practical Applications and Pitfalls of Large Language Models in Medical Education: Narrative Review
Li R, Wu T
Advances in Medical Education and Practice 2025, 16:625-636
Published Date: 18 April 2025