Back to Journals » International Journal of General Medicine » Volume 19
Elevated Red Cell Distribution Width as a Potential Marker of Acute Mountain Sickness in Chinese Young Men Upon Rapidly Ascending to 3,650 m
Authors Tang X, Tang L, Li S, Li X, Li X, Wang Q, Yang Y ![]()
Received 8 May 2026
Accepted for publication 3 July 2026
Published 10 July 2026 Volume 2026:19 620783
DOI https://doi.org/10.2147/IJGM.S620783
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Woon-Man Kung
Xugang Tang, Luxun Tang, Shuang Li, Xiuchuan Li, Xiaoyu Li, Qiang Wang, Yongjian Yang
Department of Cardiology, The General Hospital of Western Theater Command, Chengdu, 610083, People’s Republic of China
Correspondence: Yongjian Yang, Department of Cardiology, The General Hospital of Western Theater Command, 270 Tianhui Road, Rongdu Avenue, Jinniu District, Chengdu, Sichuan, 610083, People’s Republic of China, Email [email protected]
Background: Elevated red cell distribution width (RDW) has been implicated in chronic mountain sickness; however, its relationship with acute mountain sickness (AMS) remains uncertain. We aimed to evaluate the association between elevated RDW and AMS among Chinese young men undergoing high-altitude air ascent.
Methods: 157 participants (median age, 22 years) were enrolled and passively ascended primarily by air from 500 m to 3,650 m, spending approximately 3.5 hours. Participants were classified as AMS+ and AMS− based on their Lake Louise AMS score (LLS) after 24 hours at 3,650 m. Measurements included heart rate (HR), blood pressure, pulse oximeter saturation (SpO2), and complete blood count (CBC). Statistical analyses included correlation analysis, logistic regression, and receiver operating characteristic (ROC) curve analysis.
Results: The prevalence of AMS at 3,650 m was 45%. AMS+ participants had higher HR and RDW and lower SpO2 than AMS− participants. LLS was positively correlated with age, BMI, HR, and RDW, and negatively correlated with SpO2. Adjusted logistic regression revealed independent risk factors for AMS, including lower SpO2 (odds ratio [OR] = 0.809, P < 0.01), higher RDW coefficient of variation (RDW–CV) (OR = 2.790, P < 0.01), and a higher neutrophil-to-monocyte ratio (OR = 1.114, P < 0.05). ROC curve analysis demonstrated that elevated RDW–CV is a significant diagnostic indicator for AMS, with an optimal cutoff of 13.7, yielding a sensitivity of 94.37%, specificity of 45.35%, and an area under the curve (AUC) of 0.703.
Conclusion: The findings suggest that elevated RDW–CV is linked to an increased risk of AMS among Chinese young men primarily undergoing air ascent to 3,650 m.
Keywords: acute mountain sickness, blood cell count, hypobaric hypoxia, inflammation, red cell distribution width
Introduction
Rapidly ascending to altitudes above 2,500 m can lead to acute mountain sickness (AMS), a common condition that includes symptoms such as headaches, dizziness, gastrointestinal issues (like loss of appetite, nausea, or vomiting), weakness or fatigue, and insomnia.1 Although AMS typically resolves on its own, it can sometimes progress to severe complications, including high-altitude cerebral edema or pulmonary edema, which can be life-threatening.2 The diagnosis of AMS primarily relies on the patient’s self-reported nonspecific symptoms, and there are currently no gold-standard criteria, such as a diagnostic biomarker, since the underlying causes of AMS remain unknown.3 Therefore, researching a diagnostic biomarker for AMS is essential.
The biological pathways and specific molecular mechanisms underlying AMS are still not fully understood.4,5 Research suggests that AMS may involve inflammatory processes.1,6,7 Elevated levels of pro-inflammatory cytokines and other inflammatory markers, such as C-reactive protein, have been observed during high-altitude exposure8 along with cytokines like IL-1, IL-6, and TNF-α.9–12 In adult studies, several indices derived from whole blood cell counts have been introduced as prognostic markers for cancer survival and cardiovascular disease. These include the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and the systemic immune-inflammation index (SII).13 Additionally, red cell distribution width (RDW) has been suggested as a biomarker for red cell dysfunction related to high systemic inflammation and as a prognostic marker in heart failure and cardiovascular disease.14 RDW reflects the extent of red blood cell anisocytosis, a phenomenon strongly modulated by inflammatory status. Elevated RDW has also been proposed as an indicator for chronic mountain sickness in patients experiencing high-altitude polycythemia.15 Existing research demonstrates that RDW is correlated with the length of acclimatization to high altitude.16 To date, research exploring the association between RDW and AMS at high altitudes is limited.
Here, we hypothesized that RDW is associated with AMS. Therefore, this study aimed to examine whether RDW is associated with AMS in a Chinese young male population primarily undergoing air ascent to high altitude. This study provides new evidence of the involvement of inflammation in AMS.
Materials and Methods
Research Design
This cross-sectional study was conducted from August 12–17, 2025, at a site located 3,650 m above sea level in Tibet, China. Firstly, the subjects underwent chest radiography, echocardiography, and electrocardiography to verify their good physical health at 500 m. All subjects were divided into groups of 30 each. They took a flight of approximately 2.5 hours from Chengdu, Sichuan (500 m above sea level), to Gonggar, Tibet (3,569 m above sea level), followed by a roughly 1-hour car ride to barracks at an altitude of 3,650 m. High-altitude assessments were conducted following 24 hours of altitude exposure for the subjects. During the research process, the subjects maintained the same daily routine and refrained from strenuous physical activity, with standardized and uniform dietary and living conditions.
Subjects
Male subjects residing at sea level were recruited if they met all of the following criteria: first, no exposure to high altitude (land with an elevation exceeding 2,500 m above sea level)1 within the preceding six months; second, no history of respiratory or cardiovascular disease; third, no use of any drugs, including both prescription and over-the-counter drugs. Subjects of Chinese Tibetan heritage were excluded. Additional exclusion criteria included any infectious disease within the previous two weeks (such as upper respiratory tract infection, pneumonia, or enteritis), as well as a history of respiratory disease, cerebrovascular or cardiovascular disease, renal or hepatic disease, or malignant tumor.
All subjects signed informed written consent and were entitled to withdraw from the research at any stage. The research was conducted in strict accordance with the Declaration of Helsinki and approved by the Ethics Committee of the General Hospital of Western Theater Command, Chinese People’s Liberation Army (Ethics Approval No.: 2022EC3-ky062). Furthermore, baseline demographic data of all subjects, such as age, body mass index (BMI), ethnicity, educational background, as well as smoking and alcohol consumption habits, were collected using standardized questionnaires.
Diagnosis of AMS
After 24 h at 3,650 m, all subjects finished the revised Lake Louise Acute Mountain Sickness (AMS) score questionnaire. It covers four symptoms: headache, dizziness, gastrointestinal issues, and fatigue/weakness.17 Each item is scored on a 4-point scale ranging from 0 (no symptoms) to 3 (severe symptoms). AMS was confirmed in subjects with headache and a total Lake Louise score (LLS) ≥ 3. The LLS system is a well-recognized and standard tool for AMS diagnosis in high-altitude studies.18 Subjects were finally divided into AMS-positive (AMS+) and AMS-negative (AMS−) groups according to their LLS results.
Heart Rate (HR), Blood Pressure (BP), and Pulse Oximeter Saturation (SpO2)
Following 24 h of exposure at 3,650 m, resting HR, BP, and SpO2 of all participants were assessed indoors. It should be pointed out that no diffuse oxygen supplementation was available in the room. HR and BP were measured via the OMRON HEM-6200 (Omron Health Care, Inc., Bannockburn, IL, USA), and SpO2 was detected using the Onyx 9500 (Nonin Medical, Inc., Plymouth, MN, USA). Prior to SpO2 testing, subjects warmed their fingers by keeping their hands in their pockets. To guarantee measurement reliability, all indicators were collected three times in succession at roughly 30-second intervals, with the mean values adopted for subsequent analysis.
Red Cell Distribution Width (RDW)
Blood samples were collected from the median cubital vein using EDTA tubes after subjects were exposed to 3,650 m for 24 h. The samples were analyzed with standard automated hematology analyzers (XN-9100, Sysmex Co., Saitama, Japan) to determine the RDW and other composite inflammatory markers derived from the complete blood count (CBC), including the neutrophil-to-lymphocyte ratio (NLR), the platelet-to-lymphocyte ratio (PLR), and the neutrophil-to-monocyte ratio (NMR), among others.
Statistical Analysis
Data were expressed as mean ± standard deviation, median (interquartile range), or percentages as applicable. All statistical analyses were conducted using SPSS 22.0, with a two-sided P < 0.05 defined as statistically significant. The Kolmogorov–Smirnov test was applied for normality testing. Continuous variables were compared by the t-test or Mann–Whitney U-test, and categorical variables by the chi-square test. Pearson or Spearman correlation analysis was adopted to explore variable correlations according to data distribution. Factors with P < 0.10 in univariate analysis were enrolled in multivariable logistic regression, with AMS as the dependent variable. Independent variables included age, BMI, ethnicity, smoking, drinking, education, HR, SpO2, BP, RDW, and NMR. Ethnicity, smoking, and drinking were analyzed as binary variables, whereas other indicators were treated as continuous variables to screen independent risk factors for AMS. Additionally, ROC curve analysis was performed to evaluate the diagnostic value of RDW for AMS.
Results
Clinical Characteristics of the Study Subjects
At 500 m, 182 young Chinese males were enrolled. Incomplete data excluded 25 subjects from the final data analysis. Table 1 presents the clinical characteristics of the sample. The age, BMI, ethnicity, education level, alcohol consumption, and smoking patterns of the AMS+ group and the AMS− group did not differ significantly.
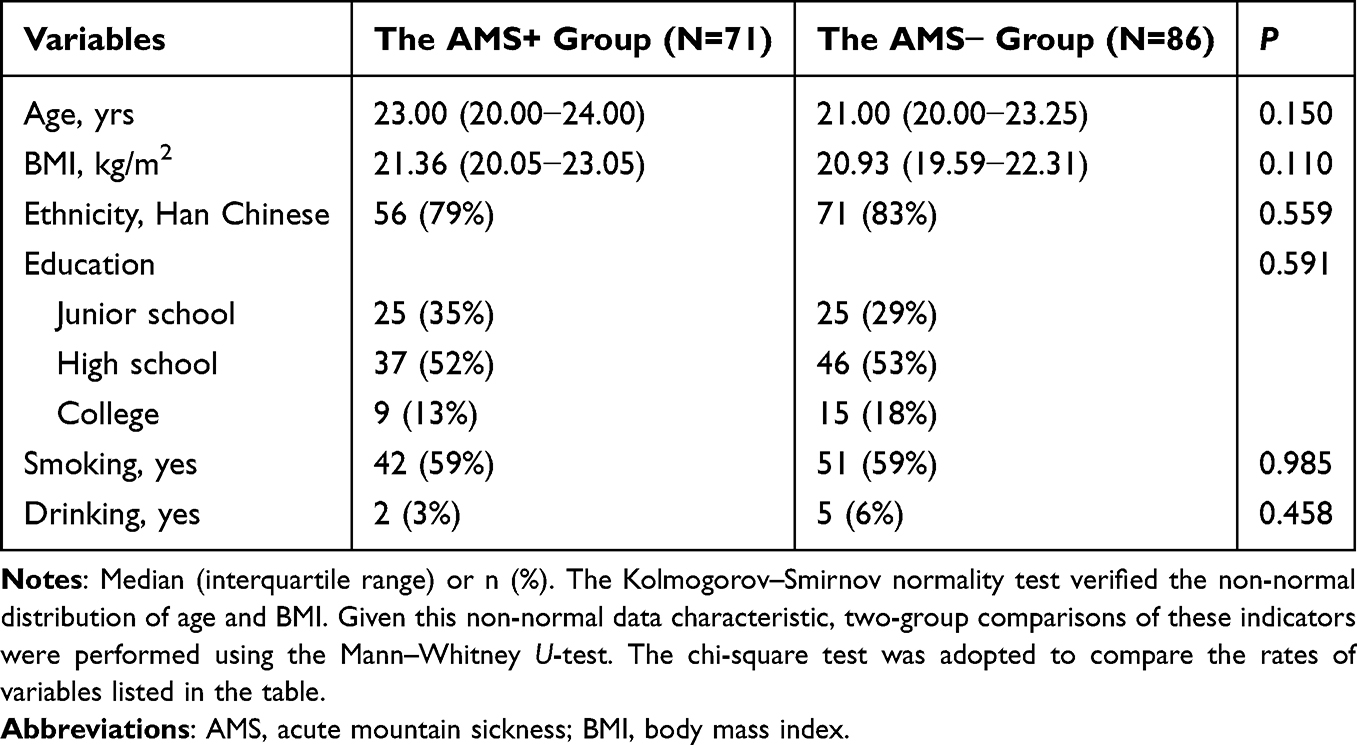 |
Table 1 Characteristics of the Sample |
Prevalence and Clinical Characteristics of AMS Following 24-Hour Exposure at 3,650 M
After 24-hour exposure at 3,650 m, the median LLS was 3 (3–4) in the AMS+ group and 2 (1–2) in the AMS− group, with a significant intergroup difference (P < 0.01).
In the present study, the prevalence of AMS was 45% (71/157) following rapid aerial ascent to 3,650 m. The most prevalent symptoms were dizziness (73%, 115/157), headache (69%, 108/157), fatigue and weakness (61%, 96/157), and gastrointestinal discomfort (16%, 25/157). Moreover, the AMS+ group exhibited markedly higher symptomatic prevalence than the AMS− group (data not shown).
Higher HR but Lower SpO2 in AMS+ Subjects at 3,650 M After 24 Hours
As shown in Table 2, following 24-hour high-altitude exposure at 3,650 m, the AMS+ group showed significantly lower SpO2 and higher HR than the AMS− group. There was no statistically significant difference in BP between the two cohorts.
 |
Table 2 Comparisons of HR, SpO2, BP, NMR, and RDW Between the AMS+ and AMS− Groups |
Higher RDW−CV and RDW−SD in AMS+ Subjects at 3,650 M After 24 Hours
As indicated in Table 2, after 24 hours at an altitude of 3,650 m, the AMS+ group exhibited significantly higher RDW−CV and RDW−SD values compared to the AMS− group. There was no statistically significant difference in NMR between the AMS+ and AMS− groups.
Positive Correlations of Total LLS with Age, BMI, HR, RDW−CV, RDW−SD, and Negative Correlation with SpO2
To screen for potential AMS risk factors, we carried out a correlation analysis of total LLS in relation to multiple clinical and demographic parameters. Significant positive correlations were observed between total LLS and age, BMI, HR, RDW−CV, and RDW−SD, whereas SpO2 was inversely associated with LLS (Figure 1). A borderline positive correlation was detected between AMS severity scores and NMR (ρ = 0.135, P = 0.092). By contrast, educational background, ethnic origin, smoking and drinking behaviors, as well as BP, showed no obvious correlation with LLS (data not shown). Further correlation analysis indicated that SpO2 was significantly negatively correlated with both RDW−CV (ρ = −0.202, P < 0.05) and RDW−SD (ρ = −0.206, P < 0.05) (Figure 1).
 |
Figure 1 The Lake Louise AMS score relates to various parameters, including (A) age, (B) BMI (body mass index), (C) heart rate (HR), (D) pulse oximeter saturation (SpO2), (E) RDW−SD, and (F) RDW−CV. Furthermore, SpO2 is associated with (G) RDW−SD and (H) RDW−CV. AMS, acute mountain sickness; BMI, body mass index; HR, heart rate; RDW−CV, red cell distribution width coefficient of variation; RDW−SD, red cell distribution width standard deviation; SpO2, pulse oximeter saturation. The Kolmogorov–Smirnov normality test indicated non-normal distribution for all plotted parameters. Given this finding, Spearman correlation analysis was performed to investigate correlational relationships across study variables. |
Univariable and Adjusted Logistic Regression Analysis of Risk Factors for AMS
Univariable logistic regression analysis of all participants revealed that lower SpO2 was significantly and negatively correlated with AMS. By comparison, higher BMI, RDW−CV, RDW−SD, and NMR were positively associated with AMS (Table 3). No significant correlations were observed between AMS and other variables, including age, ethnicity, educational level, smoking, alcohol consumption, and blood pressure (Table 3). Further multivariable adjusted logistic regression analysis demonstrated that reduced SpO2, as well as elevated NMR and RDW−CV, were independent risk factors for AMS (Table 3).
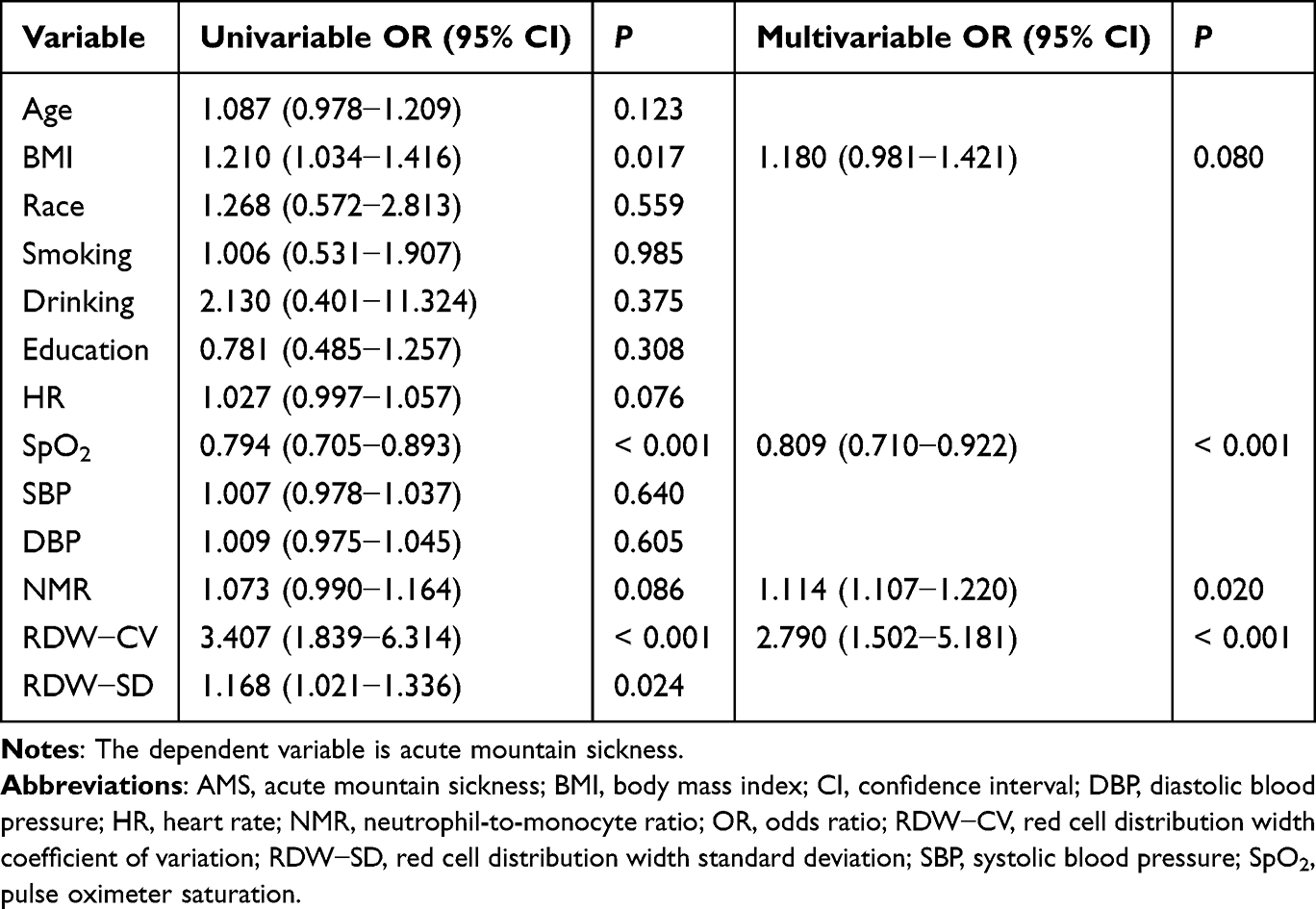 |
Table 3 Risk Factors for AMS Among All Participants After Rapid Exposure to 3,650 m for Twenty-Four Hours |
Receiver operating characteristic (ROC) curve analysis was subsequently conducted to assess the diagnostic efficacy of RDW−CV for AMS. The results validated that increased RDW−CV served as a promising biomarker for AMS identification. The optimal RDW−CV cut-off value was 13.7, with a sensitivity of 94.37%, a specificity of 45.35%, and an area under the curve (AUC) of 0.703 (95% confidence interval (CI): 0.625–0.774). Moreover, NMR (AUC = 0.575, 95% CI: 0.493–0.653) and SpO2 (AUC = 0.661, 95% CI: 0.581–0.735) also exhibited critical diagnostic values for AMS.
Discussion
The present study constitutes one of the earliest works investigating the relationship between RDW and AMS. The results of this study indicate that elevated RDW−CV may serve as a potential marker of AMS among Chinese young men upon rapidly ascending to 3,650 m. In addition, higher NMR and reduced SpO2 were also closely correlated with AMS. Therefore, RDW−CV, an objective and readily available biomarker, is recommended for testing in subjects with symptoms of AMS upon rapid exposure to plateaus above 3,650 m to facilitate the diagnosis of AMS.
With the ongoing development of western China, a growing number of individuals, particularly young male residents, travel to high-altitude areas for work, tourism, and other activities.19 AMS has therefore become a critical health issue for populations exposed to high-altitude environments. The rate of ascent and the absolute altitude reached significantly affect the prevalence of AMS.1 In the present study, 45% of the 157 enrolled participants developed AMS following air ascent to 3,650 m and 24 hours of sustained high-altitude exposure. This prevalence was notably lower than the 84% reported in Murdoch’s research, in which subjects flew directly to 3,740 m and resided at 3,860 m overnight.20 The discrepancy in AMS prevalence between the two studies may be largely attributed to the distinct altitude reached, as rapid altitude gain is a well-recognized risk factor for AMS.21 Variations in the diagnostic criteria for AMS may also exert a certain influence. Furthermore, our previously published study observed an AMS rate of 31% among 375 participants who reached 4,086 m by train within 43 hours.22 Combined with the present findings, these data further validate that ascent rate modulates the prevalence of AMS.
The RDW is a routine complete blood count (CBC) indicator that is inexpensive, rapidly detectable, and readily accessible. It reflects the degree of anisocytosis, namely the variation in erythrocyte size. Accumulated evidence has demonstrated that elevated RDW reflects disrupted erythrocyte homeostasis and is closely correlated with hypoxic status.23,24 Clinically, increased RDW is positively linked to disease severity in patients with obstructive sleep apnea.25 Likewise, in children with pulmonary arterial hypertension secondary to congenital heart disease, higher RDW levels are significantly associated with hypoxia, right ventricular fractional area change, and left ventricular ejection fraction.26
Hypoxia is well recognized as the core initiating factor of AMS, and inflammatory responses also participate in its pathological progression.1,6,7 Notably, RDW serves as a biomarker of low-grade inflammation and can mirror the severity of inflammatory activation.27,28 Consistent with our primary observations at 24 h post-exposure to 3,650 m, individuals presenting AMS exhibited higher RDW−CV and RDW−SD levels relative to those without AMS. The positive linear association between LLS and the two RDW indices further supports their close linkage to AMS severity. More importantly, multivariate logistic regression identified elevated RDW−CV as an independent predictor of AMS onset, implying its potential value in risk stratification for AMS. At present, relevant studies focusing on RDW and high-altitude disorders remain scarce. Only one previous study has reported elevated RDW in patients with chronic mountain sickness complicated by high-altitude polycythemia.15 Another study reported an association between RDW and the duration of high-altitude acclimatization.16 The current study is among the earliest investigations exploring the association between RDW and AMS. Elevated levels of pro-inflammatory mediators triggered by high-altitude hypoxia impair the body’s anti-inflammatory defense, culminating in the development of AMS.7 Considering the critical role of inflammation induced by high-altitude hypoxia in AMS pathogenesis and the close connection between RDW and inflammatory status, we hypothesize that inflammation induced by high-altitude hypoxia may be a key contributor to RDW elevation in AMS patients. However, restricted by research funding, this study failed to measure classic inflammatory markers such as interleukin-1 and interleukin-6 in our study population.
In addition, our results indicated that elevated NMR was significantly correlated with AMS. As a CBC-derived inflammatory biomarker, NMR has been widely investigated in multiple diseases. Existing studies have validated the prognostic potential of NMR for evaluating inflammatory status in patients with pancreatic cancer and locally advanced gastric cancer.29 Similarly, increased NMR has been recognized as an independent risk factor for severe COVID-19, with satisfactory sensitivity and specificity for clinical prediction.30 Collectively, these findings further support the essential involvement of inflammation in the pathogenesis of AMS. Of note, no significant correlations were found between AMS and other CBC-related inflammatory indices in the present cohort (data not shown). Such negative results may be attributable to the short-term acute hypoxic exposure in this high-altitude setting.
Previous studies have identified elevated BMI as a risk factor for AMS.31,32 Consistent with these reports, our study also found a positive correlation between BMI and AMS. Nevertheless, this association disappeared in the multivariable regression model. A plausible explanation is that all enrolled participants were young males, and the number of subjects with high BMI was relatively limited in this cohort.
Hypobaric hypoxia serves as the predominant pathogenic etiology of AMS. Owing to its non-invasive property and operational simplicity, SpO2 monitoring is regarded as a critical auxiliary biomarker for the early prediction and clinical diagnosis of AMS.33–35 Heterogeneity in high-altitude exposure regimens and pulse oximetry detection modalities across different studies contributes to substantial discrepancies in relevant research conclusions.36 In our study, all participants experienced a controlled high-altitude environment using the same passive exposure method. Our results confirm that lower SpO2 levels are a significant risk factor for AMS. Furthermore, our recently published clinical evidence further consolidates the above conclusion.22
Limitations
This study presents several strengths, including a consistent ascent profile, alongside notable limitations. Firstly, the participant cohort was exclusively male, which may introduce a potential sex bias. Secondly, with a median age of 22 years, the generalizability of the findings to older populations is limited. Additionally, due to funding constraints, inflammatory markers such as interleukin-1 and interleukin-6 could not be measured. Fourthly, hematological characteristics were not assessed before ascent, leaving uncertainty regarding any potential effects of altitude. Finally, the study focused on a single altitude level and a single observation point; these aspects warrant further investigation in future research.
Conclusion
The current study suggests that elevated RDW−CV is associated with AMS in Chinese young men primarily undergoing air ascent to 3,650 m. Furthermore, elevated NMR and decreased SpO2 were strongly associated with AMS. Additional research involving women, older adults, higher altitudes, and longer observation periods is needed to confirm these findings.
Data Sharing Statement
Data will be made available on reasonable request from the corresponding author.
Ethics Approval Statement
The study was conducted in accordance with the Declaration of Helsinki and received approval from the General Hospital of Western Theater Command of the People’s Liberation Army (2022EC3-ky062). All participants provided written informed consent and were free to withdraw from the study at any time.
Acknowledgments
The authors express their gratitude to all participants and investigators for their valuable contributions to this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Key R&D Program of China (grant no. 2024YFC3016400).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gatterer H, Villafuerte FC, Ulrich S, Bhandari SS, Keyes LE, Burtscher M. Altitude illnesses. Nat. Rev. Dis. Primers. 2024;10(1):43. doi:10.1038/s41572-024-00526-w
2. Burtscher J, Swenson ER, Hackett PH, Millet GP, Burtscher M. Flying to high-altitude destinations: is the risk of acute mountain sickness greater? J Travel Med. 2023;30(4):taad011. doi:10.1093/jtm/taad011
3. Yang J, Jia ZL, Song XY, et al. Proteomic and clinical biomarkers for acute mountain sickness in a longitudinal cohort. Commun Biol. 2022;5(1):548. doi:10.1038/s42003-022-03514-6
4. Cobb AB, Levett DZH, Mitchell K, et al. Physiological responses during ascent to high altitude and the incidence of acute mountain sickness. Physiol. Rep. 2021;9(7). doi:10.14814/phy2.14809.
5. Li YH, Zhang YJ, Zhang Y. Research advances in pathogenesis and prophylactic measures of acute high altitude illness. RESP MED. 2018;145:145–9. doi:10.1016/j.rmed.2018.11.004
6. Nourkami-Tutdibi N, Küllmer J, Dietrich S, Monz D, Zemlin M, Tutdibi E. Serum vascular endothelial growth factor is a potential biomarker for acute mountain sickness. Front Physiol. 2023;14.
7. Pham K, Parikh K, Heinrich EC. Hypoxia and inflammation: insights from high-altitude physiology. Front Physiol. 2021;12:676782. doi:10.3389/fphys.2021.676782
8. Malacrida S, Giannella A, Ceolotto G, et al. Transcription factors regulation in human peripheral white blood cells during hypobaric hypoxia exposure: an in-vivo experimental study. Sci Rep. 2019;9(1). doi:10.1038/s41598-019-46391-6.
9. Kammerer T, Faihs V, Hulde N, et al. Hypoxic-Inflammatory responses under acute hypoxia: in vitro experiments and prospective observational expedition trial. Int J Mol Sci. 2020;21(3):1034. doi:10.3390/ijms21031034
10. Lundeberg J, Feiner JR, Schober A, Sall JW, Eilers H, Bickler PE. Increased cytokines at high altitude: lack of effect of ibuprofen on acute mountain sickness, physiological variables, or cytokine levels. High Alt Med Biol. 2018;19(3):249–258. doi:10.1089/ham.2017.0144
11. Liu B, Chen J, Zhang L, et al. IL-10 dysregulation in acute mountain sickness revealed by transcriptome analysis. Front Immunol. 2017;8(8):628. doi:10.3389/fimmu.2017.00628
12. Wang C, Jiang H, Duan J, et al. Exploration of acute phase proteins and inflammatory cytokines in early stage diagnosis of acute mountain sickness. High Alt Med Biol. 2018;19(2):170–177. doi:10.1089/ham.2017.0126
13. Fest J, Ruiter R, Ikram MA, Voortman T, van Eijck CHJ, Stricker BH. Reference values for white blood-cell-based inflammatory markers in the Rotterdam Study: a population-based prospective cohort study. Sci Rep. 2018;8(1). doi:10.1038/s41598-018-28646-w
14. García-Escobar A, Lázaro-García R, Goicolea-Ruigómez J, et al. Red blood cell distribution width is a biomarker of red cell dysfunction associated with high systemic inflammation and a prognostic marker in heart failure and cardiovascular disease: a potential predictor of atrial fibrillation recurrence. High Blood Pressure Cardiovasc Prev. 2024;31(5):437–449. doi:10.1007/s40292-024-00662-0
15. Wu WT, Ni YN, Sun WJ, et al. Elevated red cell distribution width is an indicator for chronic mountain sickness in high altitude polycythemia patients: a retrospective study. Respir Med. 2026;251:108588. doi:10.1016/j.rmed.2025.108588
16. Chen L, He XF, Wang H, et al. Physiological and molecular dynamic changes during 23-day high-altitude exposure reveal novel biomarkers for acclimatization. Front Physiol. 2026;17:1763837. doi:10.3389/fphys.2026.1763837
17. Roach RC, Hackett PH, Oelz O, et al. The 2018 Lake Louise Acute Mountain Sickness Score. High Alt Med Biol. 2018;19(1):4–6. doi:10.1089/ham.2017.0164
18. Meier D, Collet T-H, Locatelli I, et al. Does this patient have acute mountain sickness?: the rational clinical examination systematic review. JAMA. 2017;318(18):1810–1819. doi:10.1001/jama.2017.16192
19. Huang L. High altitude medicine in China in the 21st century: opportunities and challenges. Mil Med Res. 2014(1):17.
20. Murdoch DR. Altitude illness among tourists flying to 3740 meters elevation in the Nepal Himalayas. J Travel Med. 1995;2:255–256. doi:10.1111/j.1708-8305.1995.tb00671.x
21. Bärtsch P, Swenson ER. Acute high-altitude illnesses. N Engl J Med. 2013;368(24):2294–2302. doi:10.1056/NEJMcp1214870
22. Tang XG, Li XC, Song BM, Li S, Wang Q, Yang YJ. Association between decreased pulse oximetry and acute mountain sickness upon rapid ascent to 4,086 m among young chinese men. High Alt Med Biol. 2025;26:102–103. doi:10.1089/ham.2024.0093
23. Yčas JW. Toward a Blood-Borne Biomarker of Chronic Hypoxemia: red Cell Distribution Width and Respiratory Disease. Adv Clin Chem. 2017;82:105–197.
24. Salvagno GL, Sanchis-Gomar F, Picanza A, Lippi G. Red blood cell distribution width: a simple parameter with multiple clinical applications. Crit Rev Clin Lab Sci. 2015;52(2):86–105. doi:10.3109/10408363.2014.992064
25. León Subías E, de la Cal S G, Marin Trigo JM. Red cell distribution width in obstructive sleep apnea. Arch Bronconeumol. 2017;53(3):114–119. doi:10.1016/j.arbres.2016.05.014
26. Hassan H, Elmeazawy R, Hodeib H, Amrousy D. Value of Red Cell Distribution Width in Children with Congenital Heart Disease Associated. Pulmonary Arterial Hypertension AJPR. 2024;14(1):35–41.
27. Fujita B, Strodthoff D, Fritzenwanger M, et al. Altered red blood cell distribution width in overweight adolescents and its association with markers of inflammation. Pediatr Obes. 2013;8(5):385–391. doi:10.1111/j.2047-6310.2012.00111.x
28. Fornal M, Wizner B, Cwynar M, et al. Association of red blood cell distribution width, inflammation markers and morphological as well as rheological erythrocyte parameters with target organ damage in hypertension. Clin Hemorheol Microcirc. 2014;56(4):325–335. doi:10.3233/CH-131745
29. Tang F, Dai PH, Wei QQ, et al. The neutrophil-to-monocyte ratio and platelet-to-white blood cell ratio represent novel prognostic markers in patients with pancreatic cancer. Gastroenterol Res Pract. 2021;2021:6693028. doi:10.1155/2021/6693028
30. Rizo-Téllez SA, Méndez-García LA, Flores-Rebollo C, et al. The Neutrophil-to-Monocyte Ratio and Lymphocyte-to-Neutrophil Ratio at Admission Predict In-Hospital Mortality in Mexican Patients with Severe SARS-CoV-2 Infection (Covid-19). Microorganisms. 2020;8(10):1560. doi:10.3390/microorganisms8101560
31. Cameron H, McDevitt M, Kayser B, Kutz C, Dawadi S, Hawley A. Risk determinants of acute mountain sickness in trekkers in the nepali himalaya: a 36-year follow-up. High Alt Med Biol. 2025.
32. Wu S, Lin YC, Weng YM, et al. The impact of physical fitness and body mass index in children on the development of acute mountain sickness: a prospective observational study. BMC Pediatr. 2015;15:55. doi:10.1186/s12887-015-0373-0
33. Roach RC, Greene ER, Schoene RB, Hackett PH. Arterial oxygen saturation for prediction of acute mountain sickness. Aviat Space Environ Med. 1998;69(12):1182–1185.
34. Collier DJ, Wolff CB, Hedges AM, et al. Benzolamide improves oxygenation and reduces acute mountain sickness during a high-altitude trek and has fewer side effects than Acetazolamide at sea level. Pharmacol Res Perspect. 2016;4(3):e00203. doi:10.1002/prp2.203
35. Luks AM, Swenson ER. Pulse oximetry at high altitude. High Alt Med Biol. 2011;12(2):109–119. doi:10.1089/ham.2011.0013
36. Schiefer LM, Treff G, Treff F, et al. Validity of peripheral oxygen saturation measurements with the garmin fēnix® 5x plus wearable device at 4559 m. Sensors. 2021;21(19):6363. doi:10.3390/s21196363
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Systemic Immune Inflammatory Response Index Can Predict the Clinical Prognosis of Patients with Initially Diagnosed Coronary Artery Disease
Li Y, Bai G, Gao Y, Guo Z, Chen X, Liu T, Li G
Journal of Inflammation Research 2023, 16:5069-5082
Published Date: 2 November 2023
Systemic Inflammatory Response Index, a Potential Inflammatory Biomarker in Disease Severity of Myasthenia Gravis: A Pilot Retrospective Study
Huang S, Wang Y, Zhu J, Li S, Lin S, Xie W, Chen S, Wang Y, Wang L, Jin Q, Weng Y, Yang D
Journal of Inflammation Research 2024, 17:2563-2574
Published Date: 25 April 2024
Association of Complete Blood Count-Derived Inflammatory Markers with Trouble Sleeping: Evidence from Population Data and Experimental Sleep Deprivation
Duan C, Zhang Y, Fang P, Wang R, Wu Y, Wang Y, Fan H, Jing Y, Feng L, Yang J, Zhuang R
Nature and Science of Sleep 2026, 18:587638
Published Date: 9 April 2026