Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Elevated LECT2 and PEDF in Pediatric MAFLD: Diagnostic Performance and Metabolic Correlations
Authors Yang L, Ni H, Deng M, Guo T, Zhang J, Sun B, Yang W ![]()
Received 30 July 2025
Accepted for publication 8 October 2025
Published 28 October 2025 Volume 2025:18 Pages 3999—4008
DOI https://doi.org/10.2147/DMSO.S555108
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Jae Woong Sull
Lanshu Yang,1– 3,* Hongbing Ni,4,* Meiling Deng,1,2 Tuo Guo,1 Jie Zhang,1,5 Baolan Sun,6 Weixia Yang1
1Department of Pediatrics, Affiliated Hospital of Nantong University, Medical School of Nantong University, Nantong, Jiangsu, People’s Republic of China; 2Dalian Medical University, Dalian, Liaoning, People’s Republic of China; 3Department of Pediatrics, Chongzhou Maternal and Child Health Care Hospital, Chengdu, Sichuan, People’s Republic of China; 4Department of Public Health, Affiliated Hospital of Nantong University, Nantong, Jiangsu, People’s Republic of China; 5Department of Pediatrics, Zhongda Hospital Southeast University, Nanjing, Jiangsu, People’s Republic of China; 6Department of Laboratory, Affiliated Hospital of Nantong University, Nantong, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Weixia Yang; Baolan Sun, Email [email protected]; [email protected]
Purpose: To evaluate the diagnostic value of serum hepatokines, leucocyte cell-derived chemotaxin 2 (LECT2) and pigment epithelium-derived factor (PEDF), for pediatric metabolic-associated fatty liver disease (MAFLD), and to assess their correlations with metabolic/liver injury indices and diagnostic utility.
Patients and methods: A total of 198 patients were included in the study (78 in the MAFLD group, 60 in the obese non-MAFLD and 60 in the control group). Serum LECT2 and PEDF levels were measured in all three groups. Group comparisons were performed, and LECT2/PEDF levels were correlated with metabolic parameters, and liver injury markers. ROC curve analyses and logistic regression were also conducted.
Results: Serum LECT2 and PEDF levels exhibited stepwise elevations (control < obese non-MAFLD < MAFLD; both P < 0.001), with significant correlations in MAFLD patients to BMI, insulin resistance (HOMA-IR), and liver injury markers (ALT/AST). For MAFLD versus controls, PEDF showed superior diagnostic accuracy (AUC = 0.804, 95% CI: 0.731– 0.877) to LECT2 (AUC = 0.734, 0.651– 0.817), while combined PEDF with LECT2 further improved discrimination (AUC = 0.849; sensitivity 79.5%, specificity 78.3%). For MAFLD versus obese non-MAFLD, both hepatokines had modest utility (LECT2 AUC = 0.623; PEDF AUC = 0.668), though their combination enhanced performance (AUC = 0.712; sensitivity 60.3%, specificity 73.9%). Multivariable analysis confirmed LECT2 and PEDF as independent MAFLD predictors.
Conclusion: LECT2 and PEDF are elevated in pediatric MAFLD and correlate with metabolic dysfunction. While their combination effectively distinguishes MAFLD from healthy controls, it shows moderate efficacy in differentiating MAFLD from simple obesity. Nevertheless, the LECT2/PEDF panel represents a promising risk-stratification tool to identify high-risk obese children for further diagnostic evaluation.Plain Language Summary
Metabolic-associated fatty liver disease (MAFLD) is the most common long-term liver problem in children, especially those who are obese. Diagnosing it can be hard—doctors usually need invasive tests like liver biopsies or expensive scans. So, researchers wanted to find simple blood tests that could help diagnose MAFLD in kids.
The team studied 198 children, split into three groups: 78 with MAFLD, 60 who were obese but did not have MAFLD, and 60 healthy kids. They measured two substances in the children’s blood—LECT2 (a factor linked to inflammation) and PEDF (a factor linked to fat regulation).
They found:Levels of both LECT2 and PEDF rose step by step: lowest in healthy kids, higher in obese kids without MAFLD, and highest in kids with MAFLD.Higher levels of these substances correlated with bigger weight problems, worse insulin resistance (when the body does not use insulin well), and more liver damage.PEDF was better at telling MAFLD apart from healthy kids than LECT2. Using both together worked even better—catching 79.5% of MAFLD cases and correctly ruling out 78.3% of healthy kids.
These results mean LECT2 and PEDF could become simple, non-invasive blood markers to help doctors spot MAFLD in children early, especially before the disease gets serious.
Keywords: children, obesity, MAFLD, LECT2, PEDF
Introduction
Nonalcoholic fatty liver disease (NAFLD), recently redefined as metabolic-associated fatty liver disease (MAFLD) by international consensus, represents a clinicopathologic spectrum characterized by hepatic steatosis (>5% hepatocytes) in the absence of significant alcohol consumption or other liver diseases.1–3 This entity encompasses nonalcoholic fatty liver (NAFL), non-alcoholic steatohepatitis (NASH), and associated sequelae including cirrhosis and hepatocellular carcinoma.2 Critically, MAFLD is intrinsically linked to metabolic dysfunction, serving as the hepatic manifestation of multisystem disorders including obesity, insulin resistance, and type 2 diabetes mellitus (T2DM).4 MAFLD has emerged as the most prevalent chronic liver disease in children, with studies reporting a prevalence exceeding 68% among obese pediatric populations.5
The pathogenesis of MAFLD involves complex metabolic interactions, conceptualized by evolving theories such as the “multiple hit” hypothesis, which integrates insulin resistance, lipotoxicity, and inflammatory cascades.6,7 The liver functions as a key endocrine organ, secreting hepatokines (hepatic factors) that systemically regulate metabolism.8 Over 560 hepatokines have been identified, with evidence suggesting that hepatic steatosis alters their secretion profile, subsequently promoting inflammation and insulin resistance in peripheral tissues.9
Two hepatokines of particular interest are leucocyte cell-derived chemotaxin 2 (LECT2)10 and pigment epithelium-derived factor (PEDF).11 Primarily secreted by hepatocytes, LECT2 induces skeletal muscle insulin resistance via JNK-mediated impairment of IRS-1 tyrosine phosphorylation and insulin signaling.12 Similarly, PEDF—expressed in liver and adipose tissue—disrupts insulin action in liver and muscle through JNK and ERK1/2 activation, while also promoting ectopic fat deposition via ATGL interaction.13,14 These mechanisms position LECT2 and PEDF as potential mediators of metabolic crosstalk in MAFLD.
Among the plethora of hepatokines implicated in NAFLD/MAFLD pathogenesis, LECT2 and PEDF were prioritized due to their distinct and complementary roles in core disease mechanisms. LECT2 has emerged as a key regulator of insulin resistance and inflammation, directly linking adipose tissue dysfunction to hepatic steatosis.10,12 Conversely, PEDF is a potent mediator of lipotoxicity and hepatic metabolic stress, with levels rising early in the disease process.11,13,14 Importantly, both factors have shown promise in preliminary pediatric studies,10–14 suggesting their relevance in the early pathogenesis of MAFLD. While other hepatokines exist, the selection of LECT2 and PEDF was driven by their strong pathophysiological rationale in metabolic dysfunction and the critical need to evaluate their combined diagnostic potential in a pediatric cohort, an area that remains underexplored.
Non-invasive diagnosis of pediatric MAFLD remains challenging. While liver biopsy is the diagnostic gold standard, its invasiveness limits utility.15 Ultrasonography, though widely used, lacks sensitivity in mild steatosis (<30%) and obese patients, and cannot stage disease severity.15 Advanced techniques like MRI-PDFF offer quantitative accuracy but face cost and accessibility barriers.16 Consequently, reliable serum biomarkers are urgently needed.
This study investigates serum LECT2 and PEDF levels in MAFLD children, evaluating their individual and combined diagnostic utility as invasive biomarkers reflective of underlying metabolic dysregulation.
Methods
Participants
This study was conducted by the Pediatrics Department of Nantong University Affiliated Hospital. A total 198 children were enrolled, including 60 healthy controls (normal weight, no MAFLD) and 138 obese children (BMI ≥ 95th percentile for age/sex per Chinese growth standards). The obese group was further stratified into obese non-MAFLD (n = 60) and MAFLD (n = 78). ALL groups were age-matched. The study complied with the Declaration of Helsinki and was approved by the institutional ethics committee of the Affiliated Hospital of Nantong University (Approval No: 2022-K029-01). Written informed consent was obtained from all participants and their parents or guardians.
Diagnostic criteria include the following sections: according to the Standardized Growth Curve for Height and Weight for Children and Adolescents 0 to 18 Years of Age in China, BMI exceeding the 95th percentile of Chinese children of the same age and sex is used as a diagnostic criterion for childhood obesity.17 The Definition of Metabolic (Dysfunction)-Associated Fatty Liver Disease in Pediatrics: An International Expert Consensus Statement (2021) suggests that hepatocellular steatosis based on histologic, imaging, or blood biomarker findings in combination with one of three conditions: overweight/obesity, type 2 diabetes mellitus, and metabolic dysfunction can be used as a diagnostic criterion for MAFLD.3 Diagnostic criteria for fatty liver imaging are the presence of two of the following three abdominal ultrasound findings: (1) diffuse enhancement of near-field echoes in the liver (bright liver), with stronger echoes than the kidneys; (2) poorly visualized intrahepatic ductal structures; and (3) gradual attenuation of far-field echoes in the liver.
The inclusion criteria were (1) age: ≤14 years; (2) availability of complete clinical data such as gender, age, BMI, fasting blood glucose, insulin series, liver function, renal function, blood lipids, blood routine, and liver ultrasound.
The exclusion criteria were (1) recent application of drugs affecting glucose, lipid metabolism or liver function indexes; (2) diabetes mellitus; (3) abnormal liver and kidney function other than MAFLD; (4) obesity caused by abnormal thyroid, pituitary or hypothalamus function; (5) history of alcohol consumption or malignant tumor; (6) history of hormone therapy in the past 3 months; (7) Those who have incomplete clinical data.
Collection of Clinical Data and Calculation of Relevant Indices
All clinical information of the children were collected and analyzed for gender, age, Body Mass Index (BMI), fasting blood glucose (FBG), fasting insulin (FINS), C-peptide, alanine aminotransferase (ALT), aspartate aminotransferase (AST), γ-glutamyl transferase (GGT), triglycerides (TG), total cholesterol (TC), low density lipoprotein (LDL-C), high density lipoprotein (HDL-C), serum uric acid (SUA). HOMA‐IR = FPG (mmol/L) × FINS (μU/mL)/22.5.
Collection and Processing of Blood Specimens
5mL of peripheral venous blood was collected in the early morning on an empty stomach in a procoagulant biochemical tube. After centrifugation at 3500r/min for 10min, the serum was aspirated and divided into 2 EP tubes, which were sealed and labeled with the corresponding information of the child. The samples should be stored in a refrigerator at −80°C and protected from repeated freezing and thawing. Serum concentrations of LECT2 and PEDF were quantified using commercially available enzyme-linked immunosorbent assay (ELISA) kits (Shuolian Biotechnology Co., Shanghai, China), strictly adhering to manufacturer protocols. All assays were performed in duplicate.
Statistical Analysis
Data analysis was performed using SPSS 26.0 (IBM Corp.) and GraphPad Prism 10.4 (GraphPad Software). Continuous variables were assessed for normality with Shapiro–Wilk testing; normally distributed data are expressed as mean ± standard deviation (sd), non-normally distributed data as median (interquartile range, IQR), and categorical variables as frequencies (%). Group comparisons employed: one-way ANOVA with LSD post-hoc testing for normally distributed variables across Control, obese non-MAFLD, and MAFLD groups; Kruskal–Wallis H-test with Dunn-Bonferroni post-hoc analysis for non-normally distributed variables; and Chi-square or Fisher’s exact tests for categorical data. Diagnostic performance of LECT2, PEDF, and their combination for MAFLD detection was evaluated using ROC curve analysis, with AUC calculation, sensitivity/specificity (95% CIs), and optimal cutoffs determined by Youden index maximization. All tests were two-tailed with statistical significance defined as P < 0.05.
Results
Participant Characteristics
The mean age of participants was comparable across groups: 11.04 years (95% CI: 9.58–12.52) in the MAFLD group, 10.67 years (9.04–11.83) in the obese non-MAFLD group, and 10.33 years (9.19–11.90) in the control group (P = 0.390). Gender distribution also showed no significant difference (P = 0.134) (Table 1).
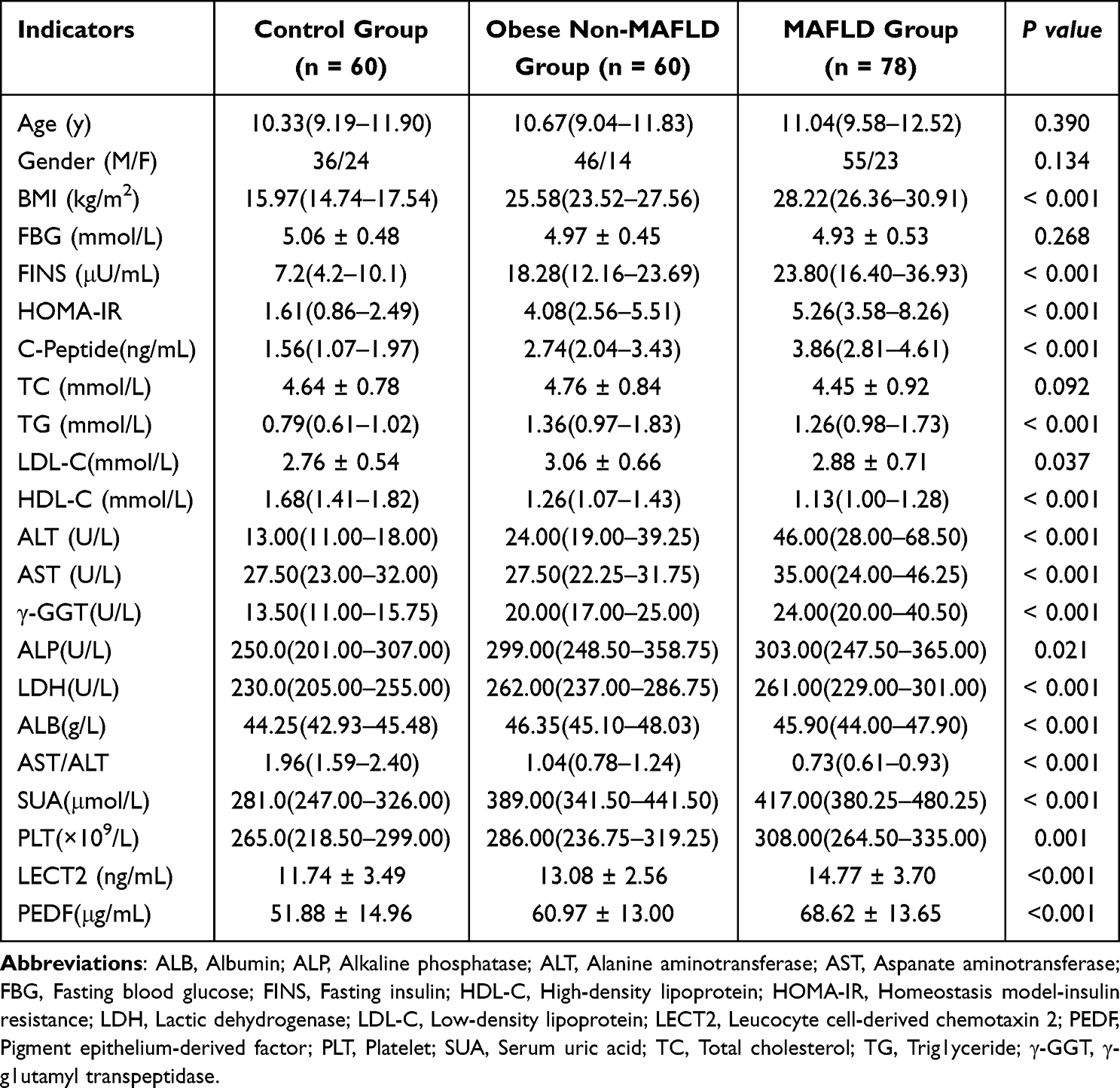 |
Table 1 Clinical and Serological Characteristics of the Subjects |
BMI was significantly higher in both the MAFLD and obese non-MAFLD groups versus controls (P < 0.0001). Significant intergroup differences (P < 0.0001) were observed for FINS, HOMA-IR, HDL-C, ALT, AST, γ-GGT, AST/ALT ratio, SUA, TG, LDH and ALB. No significant differences were detected in FBG, TC, or LDL-C levels (P > 0.05).
Serum Hepatokine Levels
Serum LECT2 and PEDF concentrations differed significantly among groups (both P < 0.001). Pairwise comparisons revealed progressively increasing concentrations from controls to obese non-MAFLD to MAFLD groups. LECT2 levels were higher in MAFLD versus obese non-MAFLD (P = 0.0092), which in turn exceeded the control group (P = 0.0178). Similarly, PEDF levels were elevated in MAFLD compared to obese non-MAFLD (P = 0.0044), and obese non-MAFLD surpassed controls (P = 0.012) (Figure 1).
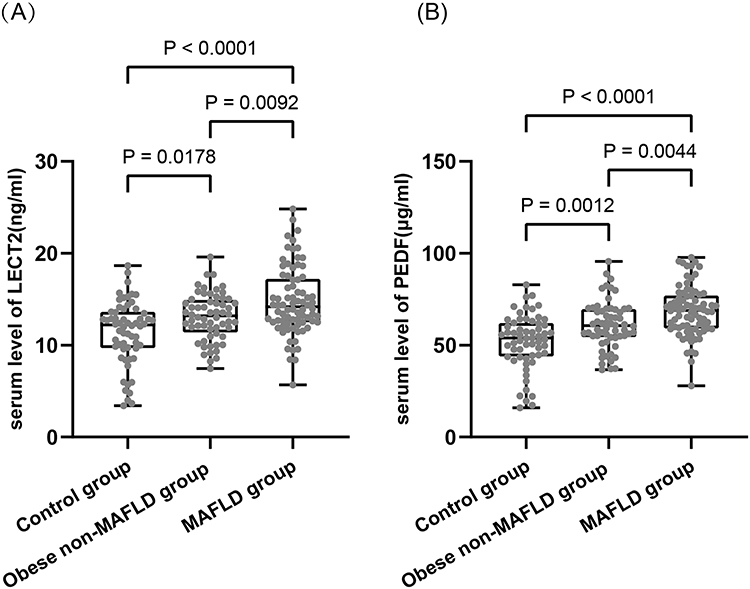 |
Figure 1 Serum levels of LECT2 and PEDF in the MAFLD, obese non-MAFLD, and control groups. (A) ELISA analysis of serum LECT2 levels across the three groups. (B) ELISA analysis of serum PEDF levels across the three groups. |
Correlation Analysis in MAFLD Group
LECT2 correlated positively with BMI (r= 0.245, P = 0.030), FBG (r= 0.241, P = 0.033), FINS (r= 0.321, P = 0.004), HOMA-IR (r= 0.343, P = 0.002), TG (r= 0.318, P = 0.004), ALT (r= 0.286, P = 0.011), and AST (r= 0.308, P = 0.006) values (Figure 2). Figure 2 Contiune. Figure 2 Correlation analysis types between hepatokines (LECT2 and PEDF) and metabolic/liver injury parameters. (A-F, L) Scatter plots of LECT2 (ng/mL) vs indicators: ALT (U/L, (A)), AST (U/L, (B)), BMI (kg/m2, (C)), FPG (mmol/L, (D)), FINS (μU/mL, (E)), HOMA-IR (F), and TG (mmol/L, (L)). (G–K) Scatter plots of PEDF (μg/mL) vs indicators: BMI (kg/m2, G), FPG (mmol/L, (H)), FINS (μU/mL, (I)), HOMA-IR (J), and PLT (×109/L, (K)). All include correlation coefficient (r), significance level (P), black linear regression line with 95% CI.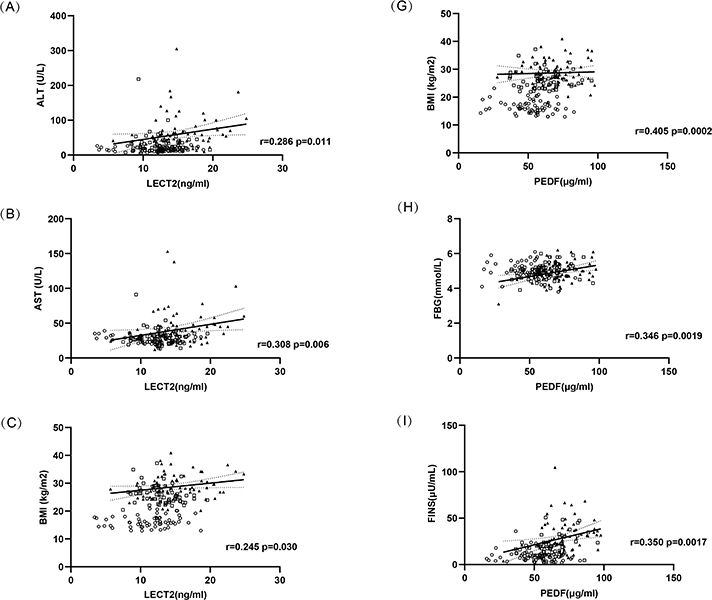

PEDF correlated positively with BMI (r= 0.405, P = 0.0002), FBG (r= 0.346, P = 0.0019), FINS (r= 0.350, P = 0.0017), HOMA-IR (r= 0.393, P = 0.0004), ALT (r= 0.224, P = 0.048), and platelet count (PLT) (r= 0.270, P = 0.017) values (Figure 2).
Diagnostic Performance of Hepatokines
PEDF demonstrated significantly higher diagnostic accuracy than LECT2 for distinguishing MAFLD patients from healthy, normal-weight controls (AUC [95% CI]: 0.804 [0.731–0.877] vs 0.734 [0.651–0.817]; both P < 0.0001). Notably, this “high accuracy” is specific to this comparison and does not extend to the clinically more relevant distinction of MAFLD from obese non-MAFLD children. At optimal cutoff values (>57.53 μg/mL for PEDF and >12.90 ng/mL for LECT2), PEDF showed 82.1% sensitivity and 66.7% specificity, while LECT2 showed 66.7% sensitivity and 71.7% specificity. The combined model significantly improved diagnostic performance (AUC: 0.849 [0.785–0.914], P < 0.0001), achieving 79.5% sensitivity and 78.3% specificity (Figure 3A).
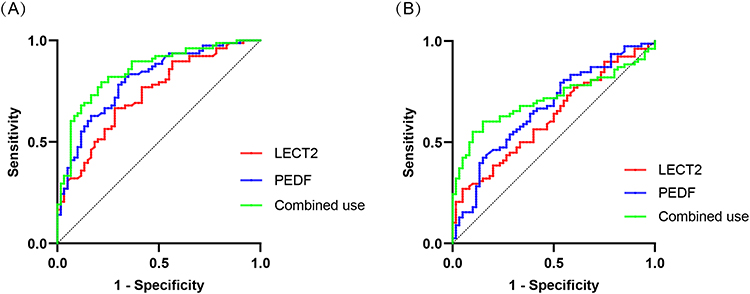 |
Figure 3 Receiver operating characteristic (ROC) analysis of serum LECT2 and PEDF for MAFLD diagnosis. (A) Discrimination between MAFLD patients (n = 78) and healthy controls (n = 60). (B) Discrimination between MAFLD patients (n = 78) and obese non-MAFLD individuals (n = 60). AUC values with 95% confidence intervals: LECT2 (0.734, 95% CI 0.651–0.817; P < 0.0001), PEDF (0.804, 95% CI 0.731–0.877; P < 0.0001), combined model (0.849, 95% CI 0.785–0.914) in A; LECT2 (0.623, 95% CI 0.531–0.716; P = 0.0128), PEDF (0.668, 95% CI 0.577–0.759; P < 0.0001), combined model (0.712, 95% CI 0.626–0.799) in B. Optimal cut-off values yielded sensitivities of 79.5% (combined (A) and 60.3% (combined (B), with specificities of 78.3% and 73.9%, respectively. |
In the comparison between MAFLD and obese non-MAFLD individuals — the scenario where clinicians most often face diagnostic uncertainty — both hepatokines exhibited only moderate diagnostic performance: LECT2 demonstrated an AUC of 0.623 (95% CI: 0.531–0.716; P = 0.0128) and PEDF showed an AUC of 0.668 (95% CI: 0.577–0.759; P = 0.0008). Using optimal cutoff values (>16.85 ng/mL for LECT2 and >70.64 μg/mL for PEDF), LECT2 exhibited relatively low sensitivity (26.9%) but high specificity (95.0%), while PEDF showed balanced performance with 42.3% sensitivity and 73.9% specificity. The combination of both markers resulted in significantly improved diagnostic accuracy (AUC: 0.712, 95% CI: 0.626–0.799; P < 0.0001), achieving 60.3% sensitivity while maintaining 73.9% specificity (Figure 3B).
Logistic Regression Analysis
Univariable and multivariable analyses confirmed LECT2 and PEDF as significant independent predictors of MAFLD (R2= 0.247 and R2= 0.351, respectively; both P < 0.001) (Table 2).
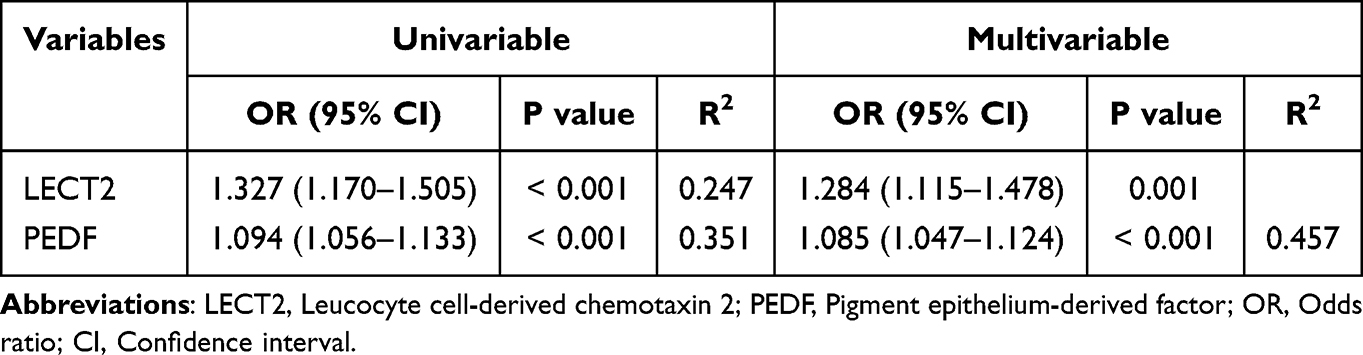 |
Table 2 Univariable and Multivariable Regression Analysis for Predicting MAFLD |
Discussion
The principal finding of this study is that serum LECT2 and PEDF concentrations demonstrated significant stepwise elevations across metabolic phenotypes, progressing from healthy controls to obese non-MAFLD subjects and further to MAFLD patients. This graded pattern suggests these hepatokines may reflect advancing metabolic dysregulation associated with hepatic steatosis.18
Also, ROC analyses revealed compelling diagnostic potential for both hepatokines. PEDF outperformed LECT2 in distinguishing MAFLD from healthy controls (AUC 0.804 vs 0.734). Critically, their combination synergistically enhanced accuracy (AUC 0.849; sensitivity 79.5%, specificity 78.3%), suggesting complementary pathophysiological roles. However, efficacy declined when differentiating MAFLD from obese non-MAFLD subjects (combined AUC 0.712). This attenuation may reflect progressive pathophysiological changes of metabolic dysfunction advances from obesity to established MAFLD, the relative contribution of these hepatokines to disease pathogenesis likely intensifies, thereby enhancing their discriminative capacity against healthy states but diminishing contrast between metabolic disease subgroups. This observation aligns with the biomarkers’ concentration gradients and suggests their diagnostic utility is stage-dependent. The stage-dependent diagnostic utility implies greatest value for early detection of metabolic liver derangements prior to overt MAFLD.
LECT2 is primarily expressed in hepatocytes and secreted into systemic circulation. Initially identified as a neutrophil chemotactic factor,19 it has been recharacterized as an energy-sensing hepatokine linking obesity to insulin resistance.20,21 Our data demonstrate a stepwise elevation in serum LECT2 across metabolic phenotypes: controls (8.2 ± 2.1 ng/mL), obese non-MAFLD (12.1 ± 3.4 ng/mL), and MAFLD (18.6 ± 5.2 ng/mL; P < 0.001). This gradient exceeds levels aligned with Lan et al’s demonstration of LECT2 as a hepatic lipid sensor upregulated prior to weight gain.21 Mechanistically, LECT2 impairs skeletal muscle insulin signaling through phosphorylation cascades: it suppresses insulin-stimulated Akt phosphorylation while activating c-JNK. This dual action enhances IRS-1 serine phosphorylation and attenuates tyrosine phosphorylation,12,22 thereby disrupting downstream insulin signaling.
Clinically, we observed significant correlations between serum LECT2 levels and key indicators of metabolic/liver injury markers including insulin resistance (HOMA-IR) and hepatocellular damage (ALT, AST).23,24 These associations confirm LECT2’s dual pathophysiological roles in perpetuating metabolic dysfunction through insulin signaling impairment25 and directly promoting liver fibrogenesis through hepatic stellate cell activation.26 Notably, serum LECT2 levels in MAFLD patients approached the established pathological threshold associated with systemic amyloidogenic risk (>20 ng/mL).27 This suggests potential long-term multi-organ damage beyond metabolic sequelae. Therapeutic targeting via AAV9-LECT2-shRNA demonstrates antifibrotic potential in experimental studies, supporting its translational relevance.27
PEDF, a 50 kDa protein originally identified in retinal pigment epithelium,28 is robustly expressed in hepatocytes and adipose tissue (hepatocytes and adipose). Elevated circulating serum PEDF correlates with obesity and insulin resistance in preclinical models, declining after metabolic interventions,29 yet exhibits functionally divergent effects (metabolic duality). Mechanistically, this duality manifests through: (1) Systemic insulin desensitization via JNK/ERK1/2 activation in liver and muscle, impairing insulin signaling;13 and (2) Ectopic lipid accumulation through adipose triglyceride lipase (ATGL) suppression, exacerbating hepatic steatosis and insulin resistance, reducing insulin sensitivity.30
In pediatric MAFLD, elevated serum PEDF concentrations correlate with a cluster of metabolic disturbances—including adiposity, dysglycemia, insulin resistance, and transaminase elevations—mechanistically aligning with its dual pathophysiological roles as a systemic instigator of insulin resistance and context-dependent hepatic lipid modulator.31 This functional duality is governed by spatially distinct signaling: endocrine pathways mediate circulating PEDF’s disease-promoting effects, whereas autocrine/paracrine mechanisms underlie intrahepatic PEDF’s metabolic-stabilizing functions.32,33 This spatial dichotomy not only establishes PEDF as a biomarker reflecting metabolic stress severity but also reveals therapeutic targeting potential, necessitating future studies to delineate tissue-specific receptor interactions and signaling cascades.
The superior performance of the LECT2-PEDF panel suggests that these two biomarkers may capture distinct yet complementary pathophysiological aspects of MAFLD—LECT2 potentially reflecting inflammatory/metabolic stress and PEDF reflecting lipotoxicity and insulin resistance. This synergy makes their combination particularly powerful for screening.
When distinguishing obese non-MAFLD children from those with MAFLD, individual LECT2 and PEDF testing shows only modest diagnostic utility, while their combination significantly enhances discriminative performance—addressing a key clinical need for early risk stratification in obese children. As shown in the study’s ROC curve analysis (Figure 3B), individual hepatokines exhibit limited ability to differentiate obese non-MAFLD from MAFLD. In contrast, the combination of LECT2 and PEDF markedly improves diagnostic accuracy. For clinical practice, this improvement is vital: obese non-MAFLD children are already at elevated metabolic risk, and missed MAFLD cases (due to poor sensitivity of individual tests) could delay early intervention. Combined testing reduces this risk by enhancing the detection of incipient MAFLD in the obese non-MAFLD subgroup.
Several limitations warrant consideration in this study. First, hepatic steatosis was diagnosed using ultrasonography rather than histology or MRI-PDFF. Ultrasound has limited sensitivity for detecting mild steatosis (<30% fat infiltration), potentially leading to underdiagnosis of early MAFLD (which requires ≥5% steatosis). This misclassification may have affected both the observed MAFLD prevalence and the accuracy of LECT2/PEDF correlations. Furthermore, in children with severe obesity, subcutaneous and visceral adipose tissue can attenuate ultrasound waves, further reducing image quality and diagnostic accuracy. Additionally, the subjective nature of ultrasonographic interpretation, without established quantitative criteria for children, introduces the possibility of inter-observer variability. Second, our cohort lacked stratification by fibrosis stage, limiting assessment of hepatokine-fibrosis relationships. Third, although we employed stringent ALT thresholds to minimize the risk, the possibility of undetected subclinical liver damage cannot be entirely ruled out in the absence of liver biopsy, the diagnostic gold standard. Finally, the single-center recruitment restricts generalizability to diverse ethnic populations. Future longitudinal studies incorporating histopathological endpoints and multi-omics approaches are needed to validate these hepatokines as clinical tools.
Conclusion
In conclusion, this study demonstrates that LECT2 and PEDF are elevated in pediatric MAFLD and correlate with metabolic dysfunction. While the combination of these biomarkers shows high accuracy in distinguishing MAFLD from healthy controls, it exhibits moderate performance in differentiating MAFLD from obesity alone. Nevertheless, the LECT2/PEDF panel shows promise as a screening tool for risk stratification in children with obesity, potentially enabling earlier intervention and optimized allocation of definitive diagnostic resources.
Data Sharing Statement
Study data are available from the corresponding author upon reasonable request to protect participant privacy.
Author Contributions
Lanshu Yang and Hongbing Ni: Writing – original draft, Conceptualization, Methodology. Meiling Deng: Writing – review & editing, Investigation. Tuo Guo: Writing – review & editing, Resources, Validation, Project Administration. Jie Zhang: Writing – review & editing, Resources, Data Curation, Formal analysis. Baolan Sun: Supervision, Conceptualization, Writing – review & editing. Weixia Yang: Supervision, Funding acquisition, Conceptualization, Resources, Writing – review & editing.
All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was funded by Nantong Bureau of Science and Technology (MS22022016), Health Commission of Nantong (MA2021002), Priority Academic Program Development of Nantong Talent Center (2022-III-609) and Jiangsu Provincial Research Hospital (YJXYY202204).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rinella ME, Lazarus JV, Ratziu V, et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. Ann Hepatol. 2024;29(1):101133. doi:10.1016/j.aohep.2023.101133
2. Yki-Jarvinen H. Nutritional modulation of non-alcoholic fatty liver disease and insulin resistance. Nutrients. 2015;7(11):9127–9138. doi:10.3390/nu7115454
3. Eslam M, Alkhouri N, Vajro P, et al. Defining paediatric metabolic (dysfunction)-associated fatty liver disease: an international expert consensus statement. Lancet Gastroenterol Hepatol. 2021;6(10):864–873. doi:10.1016/S2468-1253(21)00183-7
4. Fabbrini E, Magkos F. Hepatic steatosis as a marker of metabolic dysfunction. Nutrients. 2015;7(6):4995–5019. doi:10.3390/nu7064995
5. Zhang L, El-Shabrawi M, Baur LA, et al. An international multidisciplinary consensus on pediatric metabolic dysfunction-associated fatty liver disease. Med. 2024;5(7):797–815. doi:10.1016/j.medj.2024.03.017
6. Argenziano ME, Kim MN, Montori M, et al. Epidemiology, pathophysiology and clinical aspects of Hepatocellular Carcinoma in MAFLD patients. Hepatol Int. 2024;18(Suppl 2):922–940. doi:10.1007/s12072-024-10692-4
7. Fang YL, Chen H, Wang CL, et al. Pathogenesis of non-alcoholic fatty liver disease in children and adolescence: from “two hit theory” to “multiple hit model”. World J Gastroenterol. 2018;24(27):2974–2983. doi:10.3748/wjg.v24.i27.2974
8. Vinnakota KC, Pannala VR, Wall ML, et al. Network modeling of liver metabolism to predict plasma metabolite changes during short-term fasting in the laboratory rat. Front Physiol. 2019;10:161. doi:10.3389/fphys.2019.00161
9. Jensen-Cody SO, Potthoff MJ. Hepatokines and metabolism: deciphering communication from the liver. Mol Metab. 2021;44:101138. doi:10.1016/j.molmet.2020.101138
10. Yamagoe S, Yamakawa Y, Matsuo Y, et al. Purification and primary amino acid sequence of a novel neutrophil chemotactic factor LECT2. Immunol Lett. 1996;52(1):9–13. doi:10.1016/0165-2478(96)02572-2
11. Tombran-Tink J, Mazuruk K, Rodriguez IR, et al. Organization, evolutionary conservation, expression and unusual Alu density of the human gene for pigment epithelium-derived factor, a unique neurotrophic serpin. Mol Vis. 1996;2:11.
12. Hirosumi J, Tuncman G, Chang LF, et al. A central role for JNK in obesity and insulin resistance. Nature. 2002;420(6913):333–336. doi:10.1038/nature01137
13. Yoshida T, Akiba J, Matsui T, et al. Pigment Epithelium-Derived Factor (PEDF) prevents hepatic fat storage, inflammation, and fibrosis in dietary steatohepatitis of mice. Dig Dis Sci. 2017;62(6):1527–1536. doi:10.1007/s10620-017-4550-x
14. Tsai TH, Shih SC, Ho TC, et al. Pigment epithelium-derived factor 34-mer peptide prevents liver fibrosis and hepatic stellate cell activation through down-regulation of the PDGF receptor. PLoS One. 2014;9(4):e95443. doi:10.1371/journal.pone.0095443
15. Pasanta D, Tungjai M, Chancharunee S, et al. Body mass index and its effects on liver fat content in overweight and obese young adults by proton magnetic resonance spectroscopy technique. World J Hepatol. 2018;10(12):924–933. doi:10.4254/wjh.v10.i12.924
16. Stine JG, Munaganuru N, Barnard A, et al. Change in MRI-PDFF and histologic response in patients with nonalcoholic steatohepatitis: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2021;19(11):2274–2283.e5. doi:10.1016/j.cgh.2020.08.061
17. Blond E, Disse E, Cuerq C, et al. EASL-EASD-EASO clinical practice guidelines for the management of non-alcoholic fatty liver disease in severely obese people: do they lead to over-referral? Diabetologia. 2017;60(7):1218–1222. doi:10.1007/s00125-017-4264-9
18. Jung TW, Chung YH, Kim HC, Abd El-Aty AM, Jeong JH. LECT2 promotes inflammation and insulin resistance in adipocytes via P38 pathways. J Mol Endocrinol. 2018;61(1):37–45. doi:10.1530/JME-17-0267
19. Lan F, Misu H, Chikamoto K, et al. LECT2 functions as a hepatokine that links obesity to skeletal muscle insulin resistance. Diabetes. 2014;63(5):1649–1664. doi:10.2337/db13-0728
20. Xie Y, Fan KM, Guan SX, Hu Y, Gao Y, Zhou W-J. LECT2: a pleiotropic and promising hepatokine, from bench to bedside. J Cell Mol Med. 2022;26(13):3598–3607. doi:10.1111/jcmm.17407
21. Takata N, Ishii KA, Takayama H, et al. LECT2 as a hepatokine links liver steatosis to inflammation via activating tissue macrophages in NASH. Sci Rep. 2021;11(1):555. doi:10.1038/s41598-020-80689-0
22. Kikuchi A, Takayama H, Tsugane H, et al. Plasma half-life and tissue distribution of leukocyte cell-derived chemotaxin 2 in mice. Sci Rep. 2020;10(1):13260. doi:10.1038/s41598-020-70192-x
23. Paine-Cabrera D, Harvey LK, Robarts DR, et al. Leukocyte cell-derived chemotaxin 2 correlates with pediatric non-alcoholic fatty liver disease. Clin Transl Sci. 2023;16(12):2719–2728. doi:10.1111/cts.13666
24. Suzuki K, Tsujiguchi H, Hara A, et al. Hepatokine leukocyte cell-derived chemotaxin 2 as a biomarker of insulin resistance, liver enzymes, and metabolic dysfunction-associated steatotic liver disease in the general population. J Diabetes Investig. 2025;16(2):298–308. doi:10.1111/jdi.14351
25. Kim J, Lee SK, Kim D, et al. Adipose tissue LECT2 expression is associated with obesity and insulin resistance in Korean women. Obesity. 2022;30(7):1430–1441. doi:10.1002/oby.23445
26. Xu M, Xu HH, Lin Y, et al. LECT2, a ligand for Tie1, plays a crucial role in liver fibrogenesis. Cell. 2019;178(6):1478–1492.e20. doi:10.1016/j.cell.2019.07.021
27. Lin Y, Dong MQ, Liu ZM, et al. A strategy of vascular-targeted therapy for liver fibrosis. Hepatology. 2022;76(3):660–675. doi:10.1002/hep.32299
28. Crowe S, Wu LE, Economou C, et al. Pigment epithelium-derived factor contributes to insulin resistance in obesity. Cell Metab. 2009;10(1):40–47. doi:10.1016/j.cmet.2009.06.001
29. Reinehr T. Inflammatory markers in children and adolescents with type 2 diabetes mellitus. Clin Chim Acta. 2019;496:100–107. doi:10.1016/j.cca.2019.07.006
30. Jones IC, Carnagarin R, Armstrong J, et al. Pigment epithelium-derived factor: inhibition of phosphorylation of Insulin Receptor (IR)/IR Substrate (IRS), osteogeneration from adipocytes, and increased levels due to doxorubicin exposure. Pharmaceutics. 2023;15(7):1960. doi:10.3390/pharmaceutics15071960
31. Mao T, Wang Y. PEDF overexpression ameliorates cardiac lipotoxicity in diabetic cardiomyopathy via regulation of energy metabolism. Diabetes Metab Syndr Obes. 2025;18:217–231. doi:10.2147/DMSO.S482346
32. Li XH, Wang HP, Wu YD, et al. A novel mouse model of PEDF-associated serious liver inflammation, hepatic tumorigenesis and cardiovascular injury mimics human nonalcoholic steatohepatitis. Genes Dis. 2024;11(1):11–14. doi:10.1016/j.gendis.2023.01.011
33. Abooshahab R, Hooshmand K, Salami HA, Dass CR. The impact of pigment-epithelium-derived factor on MCF-7 cell metabolism in the context of glycaemic condition. Pharmaceutics. 2023;15(8):2140. doi:10.3390/pharmaceutics15082140
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Title: A Qualitative Systematic Review of Parental Perceptions, Motivators, and Barriers to Management of Childhood Obesity
Musa S, Al-Dahshan A, Kehyayan V
Diabetes, Metabolic Syndrome and Obesity 2024, 17:4749-4765
Published Date: 11 December 2024
Serum Vitamin D Profiles of Children with Asthma in Southwest Saudi: A Comparative Cross-Sectional Study
Asseri AA
International Journal of General Medicine 2024, 17:6323-6333
Published Date: 17 December 2024
Sleep Restriction and Weekend Sleep Compensation Relate to Eating Behavior in School-Aged Children
Chamorro R, Garrido-González M, Gutierrez M, Santos JL, Weisstaub G
Nature and Science of Sleep 2025, 17:1671-1681
Published Date: 22 July 2025
Glucagon-Like Peptide-2 as a Potential Biomarker for Nonalcoholic Fatty Liver Disease in Children with Obesity: Preliminary Assessment of Metabolic Associations and Underlying Mechanisms
Zhang SJ, Xu K, Zhu F, Teng YQ, Tang YF, Xu HW
Diabetes, Metabolic Syndrome and Obesity 2025, 18:3515-3525
Published Date: 18 September 2025