Back to Journals » Journal of Pain Research » Volume 19
Electroacupuncture Alleviates KOA-Induced Pain and Cartilage Degeneration via NGF/TrkA Pathway
Authors Fu Y, Lin L, Chen W, Shi G, Li HP, Tu JF ![]() , Liu CZ
, Liu CZ
Received 5 September 2025
Accepted for publication 16 December 2025
Published 7 January 2026 Volume 2026:19 560506
DOI https://doi.org/10.2147/JPR.S560506
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Houman Danesh
Yiming Fu,* Lulu Lin,* Wen Chen, Guangxia Shi, Hong-Ping Li, Jian-Feng Tu, Cun-Zhi Liu
International Acupuncture and Moxibustion Innovation Institute, School of Acupuncture-Moxibustion and Tuina, Beijing University of Chinese Medicine, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jian-Feng Tu; Hong-Ping Li, Email [email protected]; [email protected]
Introduction: Knee osteoarthritis (KOA) is a chronic degenerative joint disease marked by pain, cartilage degradation, and limited mobility. Existing treatments remain suboptimal due to limited efficacy and adverse effects, highlighting the urgent need for safer, mechanism-based therapies. Electroacupuncture (EA) has demonstrated clinical benefits in KOA, yet its underlying molecular mechanisms remain unclear.
Methods: A KOA rat model was established via intra-articular injection of monosodium iodoacetate (MIA). EA was applied at Dubi (ST35) and Neixiyan (EX-LE5) acupoints. We assessed the effect of EA on nociceptive behavior in rats with KOA using von Frey filament testing, weight-bearing asymmetry measurements, and spontaneous pain assays. Cartilage degeneration was analyzed via toluidine blue staining, while immunofluorescence staining quantified protein expression levels in cartilage and dorsal root ganglia (DRG). Inhibitor and agonist injections were employed to evaluate the specific involvement of the NGF/TrkA pathway in EA-mediated effects.
Results: EA significantly reduced mechanical allodynia (p < 0.001), weight-bearing asymmetry (p < 0.001), spontaneous pain (p < 0.001). EA decreased macroscopic chondropathy score (p < 0.01) and cartilage degeneration score (p < 0.001). EA inhibited MMP13 expression (p < 0.05), suppressed NGF (p < 0.001) and TrkA (p < 0.05) expression, decreased PGP9.5 overexpression (p < 0.05), and downregulated pro-inflammatory cytokines IL-1β (p < 0.01) and TNF-α (p < 0.01). Pharmacological inhibition of NGF/TrkA mimicked EA’s effects, while activation of this pathway counteracted its analgesia. EA selectively downregulated TrkA in CGRP+ (p < 0.01), but not IB4+ (p > 0.05) or NF200+ (p > 0.05) DRG neurons subtypes.
Conclusion: Our results demonstrate that EA alleviates KOA, possibly via inhibiting NGF/TrkA pathway activation in knee joints and reducing TrkA expression in CGRP+ sensory neurons, supporting the therapeutic potential of EA for KOA.
Keywords: osteoarthritis, electroacupuncture, nerve growth factor, pain, cartilage diseases
Introduction
Knee osteoarthritis (KOA) is a chronic degenerative disease primarily characterized by joint cartilage degeneration, synovial inflammation, and pain. It involves pathological changes across multiple joint structures - including cartilage, ligaments, and synovium—leading to pain, functional impairment, and reduced mobility.1 The prevalence of KOA exceeds 22.9% among individuals aged 40 years and older, with incidence rising exponentially with advancing age.2,3 With global population aging and evolving lifestyle factors, KOA has become a major cause of chronic pain, disability, and functional decline in older adults. This condition substantially diminishes patients’ quality of life and imposes a considerable burden on both healthcare systems and families,3 thereby establishing KOA as an important global public health concern. Given the chronic and recurrent nature of KOA, pain management strategies are typically categorised into conservative treatment and surgical intervention. Conservative approaches such as patient education, physiotherapy modalities, and oral or topical medications remain the cornerstone of clinical management for most patients.4 These strategies aim to alleviate pain, preserve joint function, and delay disease progression. However, the long-term use of commonly prescribed pharmacological agents such as non-steroidal anti-inflammatory drugs (NSAIDs), although effective for symptom relief, is limited by well-recognized adverse effects, including hepatotoxicity, nephrotoxicity, and elevated cardiovascular risk.5,6 Such complications highlight the need to develop or integrate safer therapeutic alternatives within conservative treatment algorithms. Notably, acupuncture emerges as a valuable adjunct therapy, offering symptomatic relief while circumventing the systemic adverse effects associated with conventional pharmacological interventions.
Acupuncture, as an integral component of traditional Chinese medicine, has gained global recognition for its efficacy in chronic pain management and is increasingly incorporated into clinical treatment strategies for KOA.7,8 Robust evidence from large-scale clinical trials has demonstrated that acupuncture effectively alleviates pain in patients with KOA.9–11 Electroacupuncture (EA), which delivers controlled electrical stimulation through acupuncture needles, differs from manual acupuncture by providing more stable, quantifiable, and adjustable stimulation parameters. Recent systematic reviews and network meta-analyses have further reported that EA outperforms conventional acupuncture in reducing pain and improving overall clinical symptoms in KOA patients.12,13 In KOA animal models, EA has been shown to attenuate synovial inflammation, inhibit cartilage degradation, and reduce pain sensitization.14 Accumulating evidence further suggests that neuroinflammatory processes and peripheral sensitisation may serve as important mediating mechanisms underlying EA’s analgesic effects.15 However, despite these advances, the molecular pathways through which EA regulates KOA-related pain and protects against cartilage degeneration remain incompletely understood.
Nerve growth factor (NGF) and its high-affinity receptor, tropomyosin receptor kinase A (TrkA), have been identified as critical mediators in KOA pathogenesis and pain transmission.16,17 Within the inflammatory microenvironment of the osteoarthritic joint, NGF is mainly produced by synovial fibroblasts and infiltrating macrophages, and its expression progressively increases during disease development.18 Elevated local NGF activates TrkA-expressing nociceptors distributed throughout the synovium, joint capsule, and periarticular tissues. This activation enhances neuronal excitability, upregulates pain-related ion channels such as transient receptor potential vanilloid (TRPV1), and promotes sensory nerve sprouting, ultimately leading to marked peripheral sensitization.19,20 NGF can also undergo retrograde transport to dorsal root ganglion (DRG) neurons, where it induces transcriptional changes that contribute to central sensitization.21 Central sensitization amplifies nociceptive input from the periphery, thereby sustaining chronic KOA pain.22,23 Although primarily implicated in pain transmission, NGF/TrkA-driven sensitization may also alter joint loading and mobility patterns, potentially exacerbating cartilage degeneration during disease progression.24
Here, the present study aimed to evaluate the effects of EA on pain behavior and cartilage degeneration in a monosodium iodoacetate (MIA)-induced rat model of KOA. In particular, we focused on whether EA exerts its therapeutic effects by regulating the NGF/TrkA signaling pathway within the synovium and sensory nervous system. Additionally, we examined TrkA expression in different DRG nociceptor subtypes to identify the neuronal populations potentially targeted by EA. These investigations were designed to clarify the cellular and molecular mechanisms through which EA modulates nociceptive signaling in KOA.
Materials and Methods
Animals
Male Sprague-Dawley rats (180–200 g) obtained from Beijing Vital River Laboratory Animal Technology Co., Ltd. All procedures in this study were approved by the Animal Care Committee of Beijing University of Chinese Medicine (Approval No.: BUCM-4-2021030101-1003) and conducted in accordance with the Regulations on the Management of Laboratory Animals of the Ministry of Science and Technology of the People’s Republic of China. This research also adheres to the Research Reporting of in vivo Experiments (ARRIVE) reporting guidelines.25 The rats were housed in specific pathogen-free conditions with a 12 h light/dark cycle and had ad libitum access to food and water.
MIA-Induced KOA Model Establishment
The KOA was induced by intra-articular (i.a.) injection of MIA solution (1.5 mg /50 μL, Sigma-Aldrich, USA) dissolved in 50 μL of sterile saline into right knee joint of rat under 1% sodium pentobarbital anesthesia (intraperitoneal injection; i.p., Sigma-Aldrich, USA). Rats in saline group were treated with 50 μL of sterile saline. Two weeks later, MIA-induced KOA rats were randomized by the random number table method into three groups to receive no treatment or EA or Sham EA.
Mechanical Allodynia
50% paw withdrawal threshold (PWT) was used to measure mechanical allodynia which was in response to a series of von Frey filaments (Ugo Basile, Italy) and determined using the “up-and-down” method. Eight von Frey filaments were chosen (0.41 g, 0.70 g, 1.20 g, 2.00 g, 3.63 g, 5.50 g, 8.50 g and 15.10 g). Each test began with a von Frey force of 2.00 g perpendicularly delivered to the plantar surface of the right hind paw for approximately 2–3 s. A positive reaction was noted when the foot abruptly withdrew either during stimulation or right after the von Frey filament was removed. Depending on whether the answer was positive or negative, the next stronger or weaker filament was used. After the initial shift was noticed, this processing was carried out for six stimuli. A value of 0.25 g was noted if a rat reacted to the lowest filament. A value of 15.0 g was given to rats that did not react to the highest filament.
Weight Bearing Asymmetry
An indicator of joint discomfort in the KOA was thought to be variations in the weight distribution of the hind paws between the right (ipsilateral) and left (contralateral) limbs. A PH-200 incapacitance tester (Techman, China) was used to determine the weight distribution of the hind paws. Each hind paw of the rat was put on a different force plate. Over the course of three seconds, the force applied by each hind limb—measured in grams—is averaged. The asymmetry of weight distribution in hind paw was calculated by the difference in the amount of weight (g) between the left and right limbs.
Spontaneous Pain
Rats were placed in transparent acrylic boxes measuring 18 × 18 × 18 cm. Over the course of an hour, we recorded how many seconds the rat spent licking or flinching its ipsilateral hind paw.
EA Treatment
The most commonly used acupoints for alleviating KOA in humans are “Dubi” (ST 35) and “Neixiyan” (Ex-LE 4).11,14 In our study, rats in the EA treatment group received EA at the right ST35 and Ex-LE4 once every other day for seven sessions, from days 14 to 26 following MIA injection. ST 35 is located at the lateral cavity of the patella and patellar ligament and Ex-LE 4 lies on the medial cavity of the patella and the patellar ligament.
Previous studies have demonstrated that 2 Hz EA intervention exhibits significant analgesic effects in animal models of KOA.26,27 EA stimulation (1 mA, 2 Hz) was applied for 30 min using a pair of 0.25 × 25 mm stainless-steel needles inserted 3-5 mm into each acupoint and connected to Han’s Acupoint Nerve Stimulator (HANS-200, China). For the Sham EA group, acupuncture needles were inserted 3–5 mm at the right hypochondrium and 10-15 mm at the iliac crest for 30 min without electrical stimulation, serving as a non-therapeutic control. EA procedures were performed without anesthesia. Rats were gently restrained during stimulation to avoid interference with pain signal transmission.
Toluidine Blue Staining
Knee joints were fixed in 4% paraformaldehyde at 4 °C for 24 h and subsequently decalcified in 10% EDTA (pH 7.4), with the solution changed every week until complete decalcification. Following decalcification of the knee joint, the tissue was sectioned into 8 μm paraffin slices. Following dewaxing with xylene, staining was performed using a 0.04% toluidine blue solution (Macklin, China). Images were acquired using microscope (Olympus, Japan).
Joint Pathology
Rats were euthanized under anesthesia with 1% sodium pentobarbital (i.p., Sigma-Aldrich, USA). Transcardial perfusion was then performed with physiological saline followed by 4% paraformaldehyde. The right knee joints were collected for macroscopic evaluation of cartilage morphology.
Macroscopic cartilage lesions were graded using the Guingamp classification:28 grade 0 represents a normal appearance; grade 1, slight yellowish discoloration of the cartilage surface; grade 2, mild erosions restricted to the weight-bearing zone; grade 3, erosions extending to the subchondral bone; and grade 4, extensive erosions with exposure of subchondral bone. Five articular regions were scored: the medial femoral condyle, lateral femoral condyle, medial tibial plateau, lateral tibial plateau, and femoral trochlea. The sum of the five regional scores yielded a maximum possible score of 20.
Histological assessment of cartilage and subchondral bone (including osteophytes), demonstrated by toluidine blue staining, was conducted in accordance with the recommendations of the International Osteoarthritis Research Society.29 Cartilage degeneration was scored from 0 is “no degeneration”, 1 is “minimal degeneration” (5–10% affected), 2 is “mild degeneration” (11–25% affected), 3 is “moderate degeneration” (26–50% affected), 4 is “marked degeneration” (51–75% affected), 5 is “degeneration” (greater than 75% affected). Each score was multiplied by the number of thirds of the cartilage length involved (1, 2, or 3) to obtain the maximum possible score of 15.
Drug Administration
MNAC13, a selective TrkA antagonist (Absolute Antibody, UK), was used to inhibit NGF/TrkA signaling in the KOA model. MNAC13 (1 µg/µL stock solution) was diluted in 0.01 M phosphate-buffered saline (PBS) to prepare a working solution of 20 µg in 50 µL. Rats in the MNAC13 group received intra-articular (i.a.) injection of 50 µL into the right knee joint on days 20 and 22 after MIA injection. The remaining groups of rats received the corresponding solvent injections.
To pharmacologically enhance NGF/TrkA signaling, NGF-7S (Sigma-Aldrich, USA) was dissolved in sterile saline to obtain a working solution of 10 µg in 50 µL. Rats in the NGF-7S group received intra-articular (i.a.) injection of 50 µL into the right knee joint on days 18 and 23 post-MIA injection. The remaining groups of rats received the corresponding solvent injections.
Immunofluorescent Staining
Rats were euthanised under 1% pentobarbital anaesthesia (i.p., Sigma-Aldrich, USA), followed by cardiac perfusion with physiological saline and 4% paraformaldehyde. The detailed procedure for collecting the synovium, including the infrapatellar fat pad (IPFP), should be performed according to the previously published protocol.30 L3-L5 DRG tissue sampling method followed the previously published protocol.31
Right knee joint synovium and L3-L5 DRG tissue were fixed in 4% paraformaldehyde for 24 h, then dehydrated in a 30% sucrose solution. Tissue sections were prepared by serial cryosectioning. After blocking with 5% donkey serum, primary antibodies were incubated with them for an entire night at 4°C. Subsequently, sections were incubated with secondary antibodies. Goat anti-β-NGF antibody (3 μg/mL, R&D Systems, USA), goat anti-TrkA antibody (3 μg/mL, R&D Systems, USA), rabbit anti-PGP9.5 antibody (1:800, Abcam, UK), rabbit anti-TNF-α antibody (1:1000, Abcam, UK), rabbit anti-IL-1β antibody (1:1000, Abcam, UK), rabbit anti-CGRP antibody (1:400, Cell Signaling Technology, USA), mice anti-NF200 antibody (1:200, Cell Signaling Technology, USA), Isolectin B4 (BSI-B4, 1:1000, Sigma-Aldrich, USA). Following that, the sections were treated with secondary antibodies that matched the main ones: donkey anti-rabbit IgG conjugated with Dylight 594 (1:400, Jackson ImmunoResearch, USA), donkey anti-rabbit IgG conjugated with Dylight 488 (1:400, Jackson ImmunoResearch, USA), donkey anti-mice IgG conjugated with Dylight 488 (1:400, Jackson ImmunoResearch, USA), donkey anti-goat IgG conjugated with Dylight 594 (1:400, Jackson ImmunoResearch, USA) and Alexa Fluor 488 (1:1000, Thermo Fisher Scientific, USA). Images were acquired using microscope (Olympus, Japan). ImageJ software was employed to analyse immunofluorescence intensity using a consistent threshold configuration.
Statistical Analysis
Statistical analyses were performed using GraphPad Prism 8 (GraphPad Software, San Diego, CA, USA). Data are presented as mean ± SEM. Normality was assessed using the Shapiro–Wilk test, and homogeneity of variance using Levene’s test. When both assumptions were satisfied, group differences were evaluated using one-way or two-way ANOVA, followed by Tukey’s post-hoc test. For comparisons between two groups, the Student’s t-test was used. Non-parametric tests were applied when normality or variance assumptions were not met. The comparison is considered to be significantly different if p < 0.05.
Results
EA Intervention Alleviates Pain and Improves Cartilage Degeneration in KOA Model Rats
MIA was injected intra-articularly (i.a.) into the right knee joint of the rats to establish the KOA model,32 while the saline group was injected with saline only. The schematic diagram was shown in Figure 1A. To assess joint pain and function, Paw withdrawal threshold (PWT) and weight-bearing asymmetry (WBA) were measured at baseline and on days 7, 14, 21, and 28 following MIA injection. In comparison with the saline group, MIA injection reduced the paw withdrawal threshold in the ipsilateral hindpaw (Figure 1B).
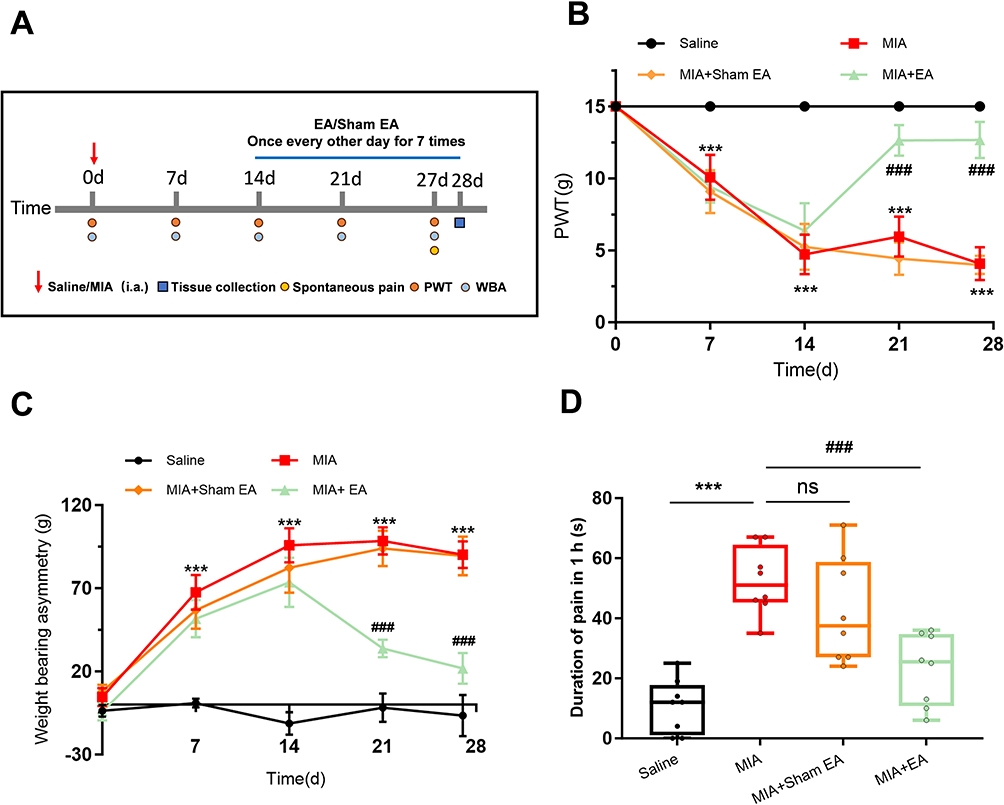 |
Figure 1 EA alleviates mechanical allodynia, weight-bearing asymmetry and spontaneous pain induced by KOA. (A) Schematic illustration of model establishment, electroacupuncture (EA) intervention, behavioral testing, and tissue collection. Arrows in the schematic indicate the time points for model induction. (B and C) Time course of EA intervention at ST35 and Ex-LE4 acupoints on mechanical allodynia and weight-bearing asymmetry in the saline, MIA, MIA + sham EA, and MIA + EA groups (per group, n = 8). ***p < 0.001 vs saline group; ###p < 0.001 vs MIA group. (D) Assessment of spontaneous pain behavior across the saline, MIA, MIA + sham EA, and MIA + EA groups (per group, n = 8). ***p < 0.001, ###p < 0.001. Abbreviations: ns, not significant; WBA, weight-bearing asymmetry; PWT, Paw withdrawal threshold. |
In the KOA model group, WBA was significantly increased compared with the saline group (Figure 1C). Moreover, rats in the MIA group exhibited markedly increased spontaneous pain behaviors compared with those in the saline group on days 27 (Figure 1D). Our observation indicated impaired joint function and increased pain in KOA model rats.
We then observed the interventional effect of EA on pain of KOA model rat. From previous research, it was found that 2 Hz EA is an effective intervention frequency for controlling the symptoms of KOA animal models.33 Here, we continued to use the KOA model rats right Dubi (ST35) and Neixiyan (EX-LE5) with 2 Hz frequency EA. We found that PWT significantly increased, WBA significantly decreased, and spontaneous pain significantly decreased after EA intervention compared with the MIA group. In contrast, sham EA did not show this effect (Figure 1B - D).
KOA induces degeneration of knee joint cartilage, which significantly impairs lower limb mobility and compromises daily functioning.34 We investigated whether EA improved cartilage damage in KOA model rats. Morphological examination of knee joint tissues revealed that KOA rats exhibited pronounced cartilage discoloration and erosion compared to the saline group, accompanied by a significant increase in the macroscopic chondropathy score (Figure 2A and B). A hallmark feature of cartilage degeneration is the degradation and subsequent loss of proteoglycans.35 Toluidine blue staining of knee joint sections revealed that, KOA rats exhibited visibly lighter or absent cartilage staining, indicative of proteoglycan depletion and exacerbated cartilage damage. Superficial staining defects and structural discontinuities were observed, accompanied by a significant increase in cartilage degeneration score, compared with the saline group (Figure 2C and D). EA intervention attenuated cartilage degeneration, resulting in a significant reduction in both the macroscopic joint cartilage lesion score and the cartilage degeneration score (Figure 2A–D).
Figure 2 Continued. Figure 2 EA alleviates cartilage degeneration and reduces MMP13 expression in the synovium induced by KOA. (A) Representative images of cartilage morphology from saline group, MIA group, MIA + sham EA group and EA group. Arrows indicate areas of cartilage erosion. (B) Summary of macroscopic chondropathy score of four groups (per group, n = 5). **p < 0.01, ***p < 0.001; ns: not significant. (C) Representative images of cartilage toluidine blue staining from saline group, MIA group, MIA + sham EA group and EA group, scale bar = 500 µm. Arrows indicate areas of cartilage matrix depletion. (D) Summary of OARSI Osteoarthritis Cartilage Histopathology Score of four groups (per group, n = 4). ***p < 0.001; ns: not significant. Scale bar = 100 µm. (E) Representative immunofluorescence images of MMP13 expression in synovial tissue from saline group, MIA group, MIA + sham EA group and EA group, scale bar = 100 µm. (F) Summary of MMP3 fluorescence intensity in synovial of 4 groups (per group, n = 4). *p < 0.05, ***p < 0.001. Abbreviation: ns, not significant.
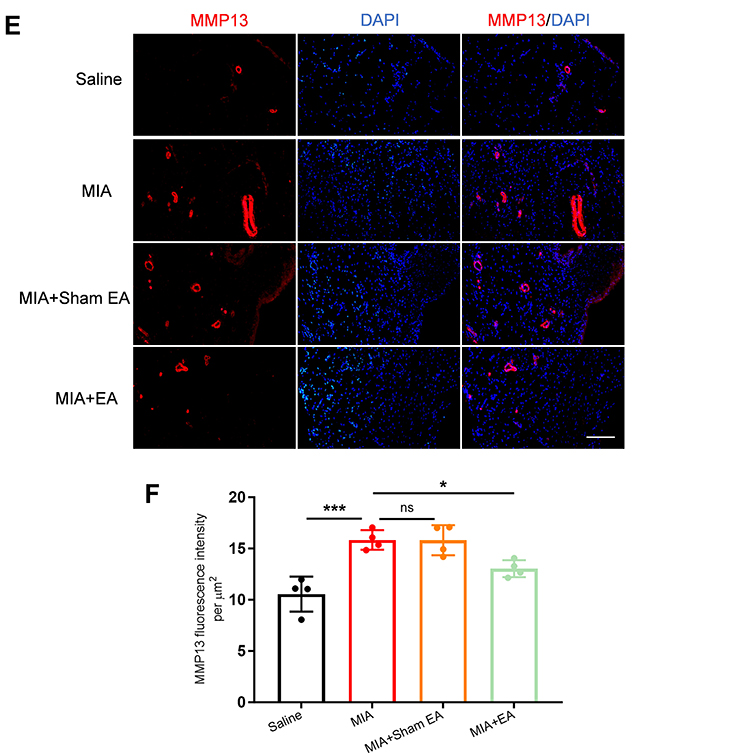
Matrix metalloproteinase 13 (MMP13) was further utilized to evaluate the degradation activity of type II collagen within the cartilage matrix, thereby indicating the severity and progression of KOA-associated lesions.36 The immunofluorescence intensity of MMP13 was markedly increased in knee joint sections from KOA model rats, whereas EA intervention significantly attenuated MMP13 expression levels. However, sham EA did not exert such beneficial effects (Figure 2E and F). These findings suggest that EA significantly inhibited the expression or activity of MMP13, mitigated type II collagen degradation, and consequently contributed to cartilage preservation. Therefore, these results indicate that EA exerts pain and significantly attenuates joint cartilage degeneration in KOA model rats.
EA Intervention Inhibits Abnormal Activation of the NGF/TrkA Pathway, Overproduction of Pro-Inflammatory Cytokines, and Abnormal Proliferation of Nerve Fibers in the Synovial Tissue of KOA Model Rats
NGF/TrkA signaling pathway plays a critical role in the transmission of KOA-related pain by inducing peripheral and central sensitization, ultimately leading to hyperalgesia.37 Therefore, we planned to explore whether EA could interfere with NGF/TrkA signaling. The expression of NGF and TrkA was significantly increased in the MIA group (Figure 3A–D). EA significantly reduced the elevated NGF and TrkA expression in the knee synovium, compared with the MIA group (Figure 3A–D). In contrast, sham EA did not show any such effect (Figure 3A–D). These results indicate that EA can inhibit the activation of NGF/TrkA signaling in the injured knee joints of KOA model rats.
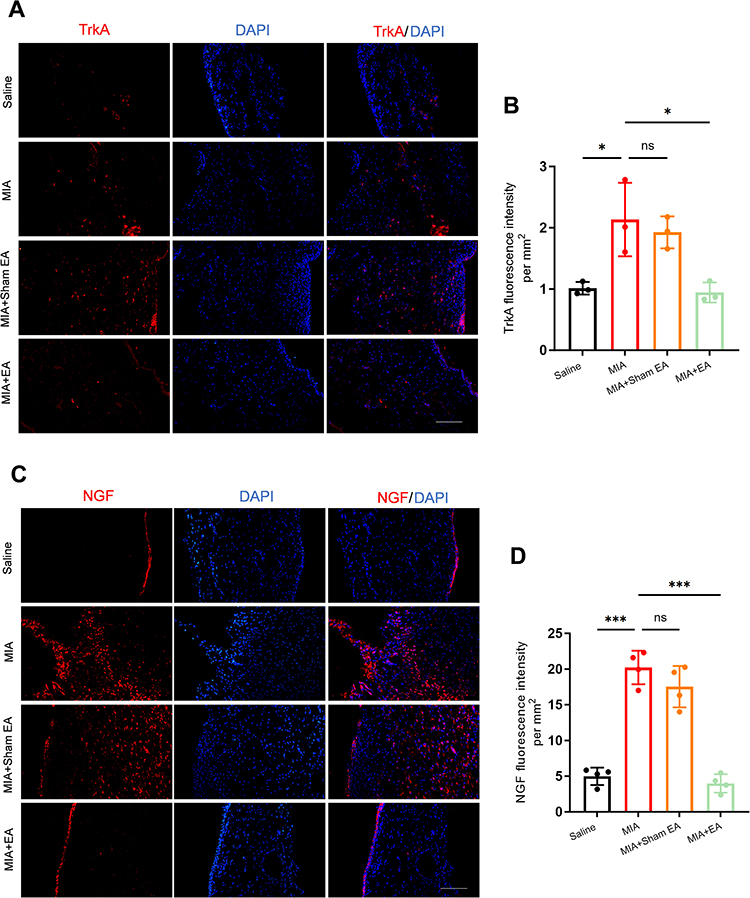 |
Figure 3 EA inhibits NGF/TrkA activation in synovial tissue of KOA model rats. (A) Representative immunofluorescence images showing NGF expression in the synovial tissue from the saline, MIA, MIA + sham EA, and MIA + EA groups. Scale bar = 100 µm. (B) Quantification of NGF fluorescence intensity in the synovium across the four groups (per group, n = 3). *p < 0.05; ns: not significant. (C) Representative immunofluorescence images showing TrkA expression in the synovial tissue from the saline, MIA, MIA + sham EA, and MIA + EA groups. Scale bar = 100 µm. (D) Quantification of TrkA fluorescence intensity in the synovium across the four groups (per group, n = 4). ***p < 0.001. Abbreviation: ns, not significant. |
Previous studies have demonstrated that NGF/TrkA signaling pathway primarily contributes to pain exacerbation by promoting IL-1β expression and the proliferation of sensory nerve fibers, while also forming a positive feedback loop with TNF-α to amplify inflammatory responses in the KOA model.16 We planned to explore whether EA could suppress the release of pro-inflammatory cytokines and relieve pain. Following MIA induction, the expression of IL-1β and TNF-α in the knee joint was significantly enhanced (Figure 4A–D). EA treatment inhibited the expression of IL-1β and TNF-α (Figure 4A–D), while sham EA treatment did not produce such effect (Figure 4A–D).
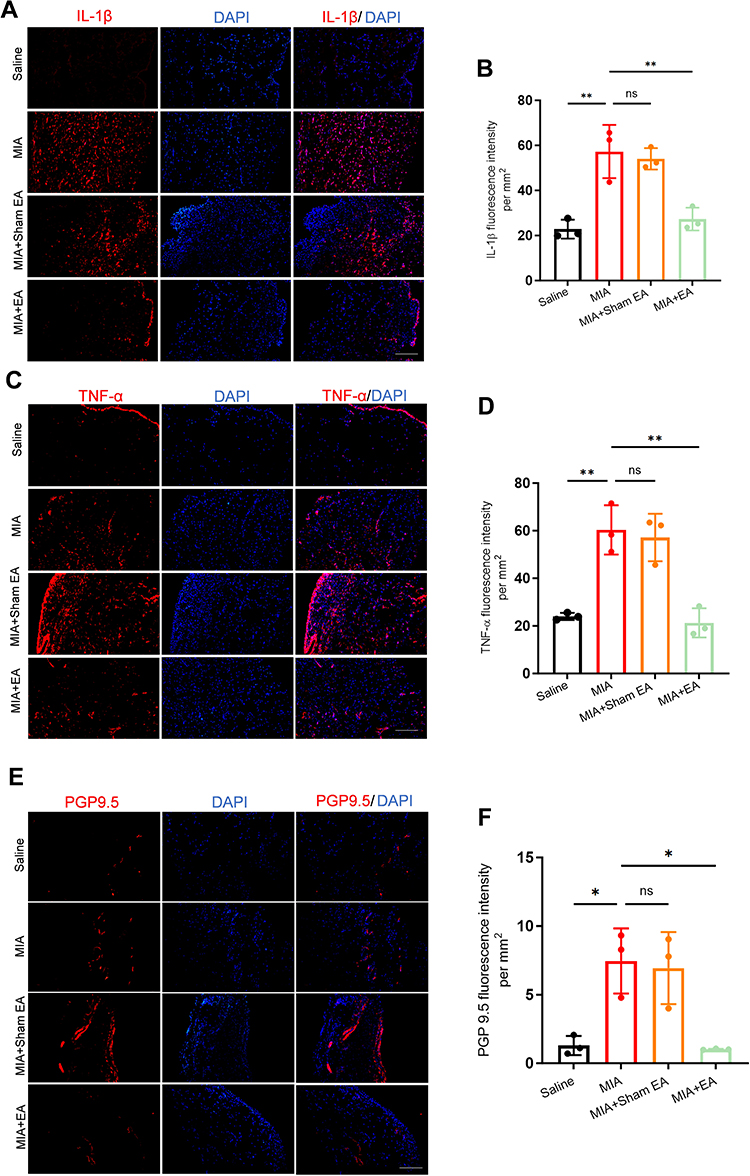 |
Figure 4 EA inhibits IL-1β, TNF-α and PGP9.5 expression in synovial tissue of KOA model rats. (A) Representative immunofluorescence images showing IL-1β expression in the synovial tissue from the saline, MIA, MIA + sham EA, and MIA + EA groups. Scale bar = 100 µm. (B) Quantification of IL-1β fluorescence intensity in the synovium across the four groups (per group, n = 3). **p < 0.01; ns: not significant. (C) Representative immunofluorescence images showing TNF-α expression in the synovial tissue from the saline, MIA, MIA + sham EA, and MIA + EA groups. Scale bar = 100 µm. (D) Quantification of TNF-α fluorescence intensity in the synovium across the four groups (per group, n = 3). **p < 0.01; ns: not significant. (E) Representative immunofluorescence images showing PGP9.5 expression in the synovial tissue from the saline, MIA, MIA + sham EA, and MIA + EA groups. Scale bar = 100 µm. (F) Quantification of PGP9.5 fluorescence intensity in the synovium across the four groups (per group, n = 3). *p < 0.05. Abbreviation: ns, not significant. |
Protein Gene Product 9.5 (PGP9.5) was highly expressed in sensory nerve endings.38 During the progression of KOA, the inflammatory microenvironment and joint structural damage can induce abnormal regeneration or sensitization of nerve fibers, thereby exacerbating pain symptoms.39,40 Therefore, we planned to explore whether EA could suppress abnormal sensory nerve fiber proliferation. PGP9.5 expression was significantly increased in the synovial tissue (Figure 4E and F), suggesting an increase in the density of nerve fibers within the synovium or exacerbated neural remodeling in KOA model rat. EA significantly reduced PGP9.5 expression (Figure 4E and F), suggesting that EA may alleviate KOA-related peripheral nerve sensitization and chronic pain by inhibiting abnormal nerve fiber proliferation or activity within the synovium. In contrastt, sham EA did not have any such effect (Figure 4E and F). Therefore, these results indicate that EA can inhibit the excessive activation of the NGF/TrkA pathway in KOA knees and alleviate pain by further reducing the expression of pro-inflammatory cytokines and nerve fiber hyperinnervation.
EA Intervention Is Mimicked by Pharmacological Inhibition of the NGF/TrkA Signaling Pathway and Reversed Through Its Activation
MNAC13 has been identified as a selective inhibitor that prevents the binding of NGF to TrkA.41 We proceeded to investigate further whether pharmacological inhibition of NGF/TrkA signaling using MNAC13 (20 µg/50 µL, i.a.) could replicate the anti-hyperalgesic effects of EA. The schematic diagram was shown in Figure 5A. Compared with saline group, the MNAC13 treatment significantly improved mechanical hyperalgesia and reduced WBA (Figure 5B–E), which mimics the antinociceptive effect achieved by EA treatment (Figure 5B–E). This demonstrated the key contribution of the NGF/TrkA pathway to pain in KOA model rats.
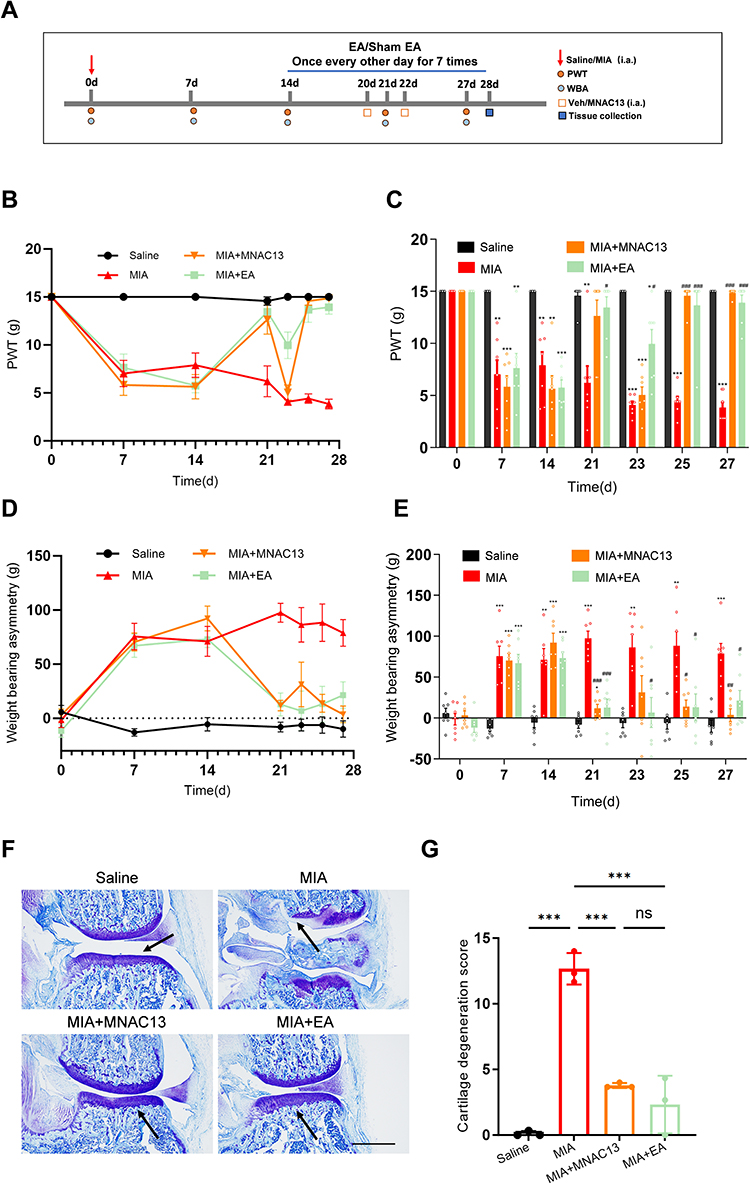 |
Figure 5 Specific blockade of NGF/TrkA signaling ameliorates pain and cartilage degeneration in KOA model rats. (A) Schematic illustration of model establishment, MNAC13 administration, behavioral testing, and tissue collection. Arrows in the schematic indicate the time points for model induction. (B and C) Changes in paw withdrawal threshold (PWT) in the saline, MIA, MIA + MNAC13, and MIA + EA groups (per group, n = 7). *p < 0.05, **p < 0.01, ***p < 0.001 vs saline group; #p < 0.05, ###p < 0.001 vs MIA group. (D and E) Changes in weight-bearing asymmetry (WBA) in the saline, MIA, MIA + MNAC13, and MIA + EA groups (per group, n = 7). **p < 0.01, ***p < 0.001 vs saline group; #p < 0.05, ##p < 0.01, ###p < 0.001 vs MIA group. (F) Representative toluidine blue-stained images of cartilage from the saline, MIA, MIA + MNAC13, and MIA + EA groups. Scale bar = 500 µm. (G) Quantification of cartilage degeneration scores in the four groups (per group, n = 3). ***p < 0.001. Abbreviation: ns, not significant. |
In parallel, the potential of MNAC13-mediated pharmacological blockade of NGF/TrkA signaling to attenuate cartilage degeneration in KOA model rats was assessed through histological evaluation of cartilage sections. Toluidine blue staining showed thatthe MNAC13 treatment significantly improved cartilage degeneration in KOA model rats, compared with saline group (Figure 5F and G). Moreover, its therapeutic effect was similar to that of EA (Figure 5F and G).
Subsequently, we examined whether activation of the NGF/TrkA signaling pathway could counteract the EA-induced anti-hyperalgesic effects and chondroprotective effects in KOA model rats. To achieve this, NGF-7S solution (10 µg/50 µL)42 was intra-articularly administered on days 18 and 23. The schematic diagram was shown in Figure 6A. Combined treatment of NGF-7S injection and EA effectively reversed the analgesic effect of EA, as evidenced by an increased weight-bearing difference between the hind limbs, compared with the EA group (Figure 6B–E). However, NGF-7S administration failed to completely abolish the protective effect of EA on cartilage degeneration (Figure 6F and G). Notably, while intra-articular NGF-7S administration effectively reversed the analgesic effect of EA, it did not completely abolish EA-induced protection against cartilage degeneration. The persistence of partial chondroprotection despite NGF activation suggests that EA may also exert cartilage-protective actions through additional mechanisms beyond NGF/TrkA signaling. These results indicate that pharmacological antagonism of NGF/TrkA signaling mimics the anti-hyperalgesic and cartilage-protective effects of EA in KOA model rats, whereas pharmacological activation of NGF/TrkA signaling reverses the EA-induced analgesic effects.
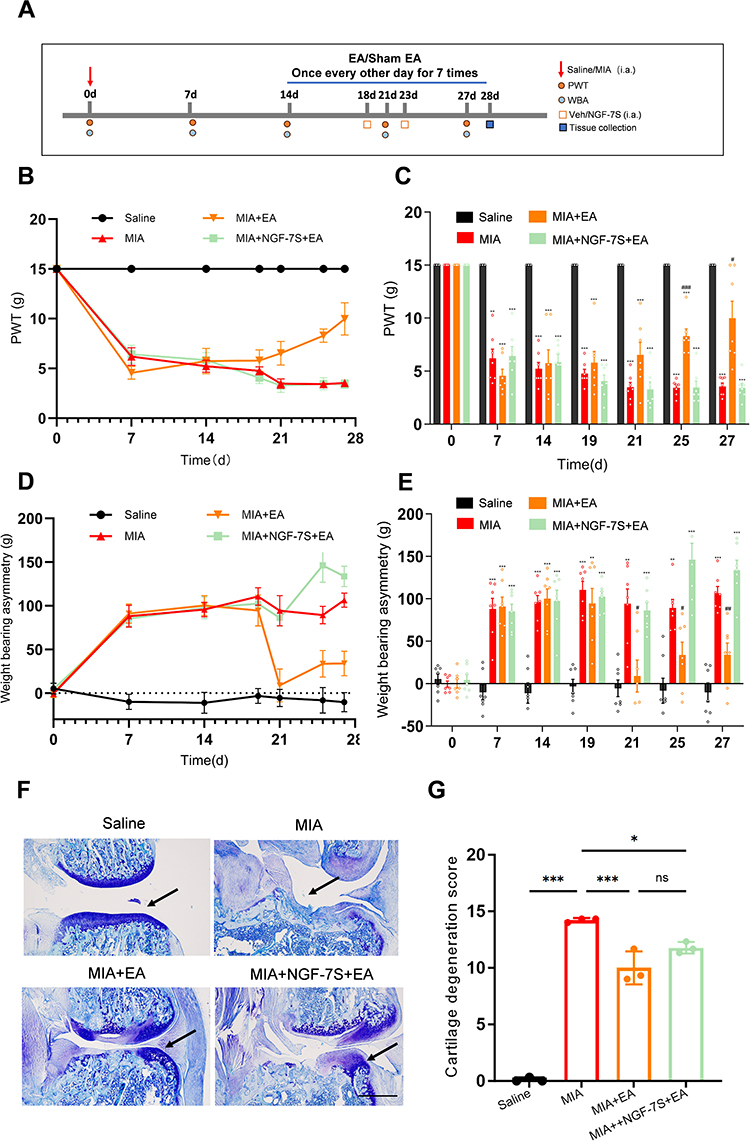 |
Figure 6 Pharmacological activation of NGF reverses EA-induced antiabnormal pain in KOA model rats. (A) Schematic timeline illustrating model establishment, NGF-7S administration, behavioral testing, and tissue collection. Arrows in the schematic indicate the time points for model induction. (B and C) Changes in paw withdrawal threshold (PWT) in the saline, MIA, MIA + EA, and MIA + NGF-7S + EA groups (per group, n = 7). **p < 0.01, ***p < 0.001 vs saline group; #p < 0.05, ###p < 0.001 vs MIA group. (D and E) Changes in weight-bearing asymmetry (WBA) among the saline, MIA, MIA + EA, and MIA + NGF-7S + EA groups (per group, n = 7). **p < 0.01, ***p < 0.001 vs saline group, #p < 0.05, ##p < 0.01 vs MIA group. (F) Representative toluidine blue-stained images of cartilage from the saline, MIA, MIA + EA, and MIA + NGF-7S + EA groups. Scale bar = 500 µm. Arrows indicate areas of cartilage matrix depletion. (G) Quantitative analysis of cartilage degeneration scores among the four groups (per group, n = 3). *p < 0.05, ***p < 0.001. Abbreviation: ns, not significant. |
EA Intervention Inhibits TrkA Overexpression in DRG of KOA Model Rats
Next, we hypothesized that the increase in NGF in the knee joints of KOA model rats may cause pain through its high-affinity receptor TrkA expressed on peripheral sensory neurons, while EA alleviates KOA symptoms by inhibiting this pathway. We used immunofluorescence to detect whether the expression of TrkA in the ipsilateral L3-L5 DRG of KOA model rats induced by MIA injection was affected. Compared with the saline group, significantly increased TrkA expression was observed in the L3-L5 DRG of KOA model rats (Figure 7A and B). Additionally, TrkA was significantly reduced in the L3-L5 DRG in the EA group. No significant effect was observed in the sham EA group (Figure 7A and B). These results indicate that TrkA in the DRG is involved in the inflammatory pain process, and that EA inhibits the overexpression of TrkA, thereby alleviating KOA symptoms.
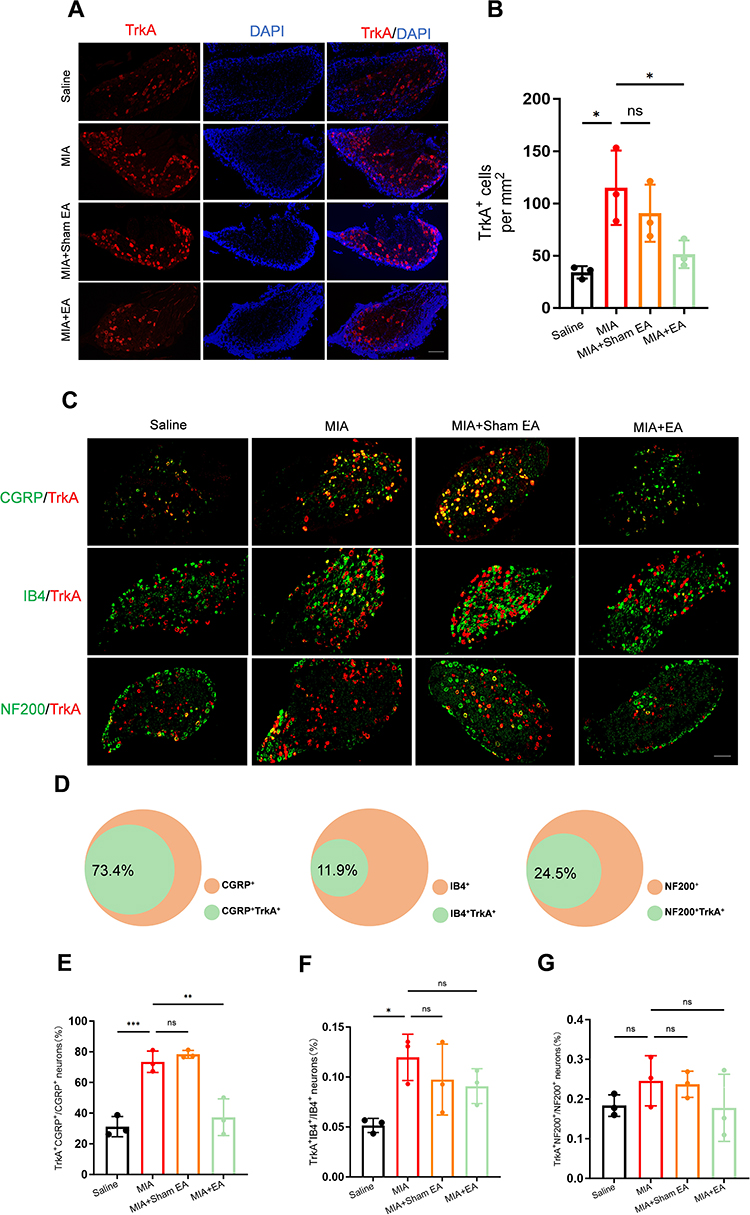 |
Figure 7 EA intervention inhibits TrkA expression in CGRP+ neurons in DRG of KOA model rats. (A) Representative immunofluorescence images of TrkA in DRG from saline group, MIA group, MIA + sham EA group and EA group. Scale bar = 200 µm. (B) Quantification of the number of TrkA+ cells in DRG across the four groups (per group, n = 3). *p < 0.05; ns: not significant. (C) Representative images of double-labelling immunostaining of TrkA+ with CGRP+, IB4+, NF200+ in DRG sections from the saline, MIA, MIA + sham EA, and MIA + EA groups, scale bars = 200 µm. (D) Pie chart summarizing the proportion of TrkA co-localization in IB4+, CGRP+, and NF200+ neurons in KOA model rats. Three sections were analyzed per rat, and the results were averaged. (E) Quantification of the percentage of CGRP+ neurons co-expressing TrkA in the DRG across the four groups (per group, n = 3). **p < 0.01, ***p < 0.001; ns: ns: not significant. (F) Quantification of the percentage of IB4+ neurons co-expressing TrkA in the DRG across the four groups (per group, n = 3). *p < 0.05; ns: not significant. (G) Quantification of the percentage of NF200+ neurons co-expressing TrkA in the DRG across the four groups (per group, n = 3). Abbreviation: ns, not significant. |
EA Intervention Inhibits the Overexpression of TrkA in CGRP+ DRG Neurons of KOA Rats
To further explore whether EA acts on specific neurons in the KOA model DRG, we detected TrkA expression in rat DRG neurons and labeled neurons in the DRG with CGRP, IB4, and NF200. Using double-labeled immunofluorescence, Figure 7C and D show that TrkA is expressed in 73.4%, 11.9%, and 24.5% of CGRP, IB4, and NF 200 nociceptive neurons, respectively. These data indicate that TrkA is expressed in nociceptive neurons of the ipsilateral L3–L5 DRG, predominantly in CGRP+ peptidergic neurons, followed by NF200+ large-sized A fiber neurons and IB4+ non-peptidergic neurons.
Then, our result showed that EA significantly reduced TrkA expression in CGRP+ neurons (Figure 7E). TrkA expression in IB4+ and NF200+ neurons was not significantly altered following EA intervention (Figure 7F and G). These findings indicate that EA alleviates KOA by specifically downregulating TrkA expression in CGRP+ DRG neurons..
Discussion
KOA is now recognized as a whole-joint disease involving not only cartilage degeneration but also pathological changes in the synovium, subchondral bone, meniscus, ligaments, and periarticular innervation. These structural alterations, together with local inflammatory and neurobiological processes, collectively contribute to the development of chronic joint pain and functional impairment.43,44 Intra-articular injection of MIA is a commonly used method for constructing KOA models.42 This model not only reliably induces peripheral hyperalgesia but also causes characteristic cartilage damage by inducing matrix degradation.45 Local NGF upregulation in the knee joint is a key driver of nociceptive transmission, and pharmacological or genetic suppression of NGF/TrkA signaling consistently alleviates pain in KOA models.23,46–48 EA has been reported to downregulate NGF and TrkA expression in peripheral tissues, DRG, and the spinal cord,49 but the causal link between NGF/TrkA signaling inhibition and EA-induced analgesia in KOA remained unclear. Here, we found that EA markedly reduced NGF and TrkA expression in KOA joints. NGF/TrkA signaling blockade mimicked EA’s analgesic effect, whereas exogenous NGF activation attenuated it, suggesting that modulation of the NGF/TrkA signaling contributes substantially to EA-induced analgesia.
Previous study showed that activation of the NGF/TrkA signaling pathway in KOA markedly upregulates both the mRNA and protein expression of PGP9.5, enhances sensory nerve fiber innervation in the synovium, and thereby exacerbates peripheral hyperalgesia.22 Consistent with this, our study assessed whether EA regulates pathological innervation via NGF/TrkA signaling. Our data demonstrated that EA significantly reduced PGP9.5 expression and aberrant nerve fiber sprouting, a change that correlated with pain relief and is likely associated with NGF/TrkA signaling modulation.
NGF binding to the TrkA receptor has been strongly implicated in the transmission of pain signals.50 Previous work reported that DRG neurons with high TrkA expression, particularly small- and medium-diameter neurons, exhibit distinct electrophysiological properties associated with nociceptive signaling.51,52 Increased TrkA expression in the DRG was directly linked to various experimental models of pain. Inhibition of the TrkA signaling pathway—such as through intrathecal administration of anti-NGF antibodies or TrkA inhibitors—was shown to alleviate pain-related behaviors.53 Following these prior studies, we investigated whether EA could affect TrkA expression in DRG of KOA model rat. We found that EA significantly suppressed TrkA expression. CGRP+ neurons represent a crucial population involved in nociception, whose activity is strongly regulated by the NGF/TrkA signaling pathway.
Subsequently, TrkA expression was detected in IB4+, CGRP+ and NF200+ DRG neurons in the KOA rat model. Moreover, EA treatment primarily altered TrkA expression in CGRP+ neurons. It has been reported that 92% of TrkA-positive neurons co-express CGRP, a neuropeptide critically involved in pain transmission.54 Furthermore, research indicates that approximately 85% of TrkA+ bone pain receptors co-express CGRP, and that NGF directly upregulates CGRP synthesis through TrkA activation. In inflammatory or nerve injury models, NGF binding to TrkA activates downstream signaling pathways, including phosphoinositide 3-kinase (PI3K) and protein kinase C (PKC), which resulted in increased CGRP release and enhanced peripheral sensitization.55 But it should be noted that, in the MIA-induced KOA model, both TrkA and CGRP were co-upregulated within DRGs, whereas post-traumatic OA showed elevated CGRP expression alone, indicating model-specific variations.56
Previous studies have shown that MMP-13 is the major collagenase responsible for degrading type II collagen, the principal structural component of articular cartilage, and its upregulation is a hallmark of cartilage degeneration in KOA.57 The degradation fragments generated from type II collagen breakdown can further activate type A synoviocytes, leading to the release of pro-inflammatory cytokines and additional matrix metalloproteinases, including TNF-α, IL-1β, and MMP-13, thereby amplifying synovial inflammation and cartilage catabolism.58 Moreover, the IPFP, an integral anatomical and functional component of the knee joint, secretes multiple inflammatory mediators. These act upon periarticular tissues including the synovium, cartilage, and menisci, thereby exacerbating the inflammatory microenvironment and accelerating cartilage degeneration.59 Together, these molecular and cellular events drive the progressive deterioration observed in KOA.57 Therefore, our study aimed to determine whether EA could modulate cartilage degeneration and its associated inflammatory pathways in the KOA condition. Our data showed that EA reduced the levels of MMP13 in the synovium of the model knee joint while inhibiting pro-inflammatory cytokine levels, suggesting a significant inhibition of cartilage damage and degeneration in KOA model rats, along with reduced inflammatory responses and suppression of inflammatory amplification effects.
Previous studies have shown that NGF activates downstream signals by binding to the TrkA receptor, inducing the expression of transcription factors Etv4 and Etv5, thereby promoting the transcription and expression of MMP13.60 Next, we found that specific inhibition of NGF-TrkA binding alleviated cartilage degeneration, and this effect was similar to that of EA. Previous studies have shown that in KOA models, MMP13 activity is directly related to joint destruction and does not completely depend on the NGF/TrkA pathway.23 Our data showed that activation of NGF did not completely offset the inhibitory effect of EA on cartilage degeneration. This may be related to the direct effect of EA on MMP13, or EA may inhibit cartilage degeneration through mechanisms other than NGF.
Several limitations warrant consideration. First, the present work focused on peripheral and DRG-level mechanisms and did not examine potential central regulatory processes, such as spinal or supraspinal modulation of nociception. Second, the inability of NGF activation to fully counteract the chondroprotective effects of EA implies the involvement of other regulatory mechanisms beyond the NGF/TrkA axis. Third, the study did not employ genetic approaches to directly validate the causal role of NGF/TrkA signaling, and future investigations using conditional or cell-type-specific manipulations will be essential to strengthen these conclusions.
Conclusions
This study demonstrated that EA intervention significantly alleviated pain and cartilage degeneration in a rat model of KOA. The effects of EA may be mediated through inhibition of the NGF/TrkA signaling pathway in joint tissues, accompanied by downregulation of TrkA expression in CGRP-positive nociceptive neurons. These findings further support the therapeutic potential of EA as an alternative approach for the management of KOA.
Data Sharing Statement
All data in the current findings are attainable from the corresponding author (Jian-feng Tu).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (to Jianfeng Tu (grant number: 82305418)), the National Science Fund for Distinguished Young Scholars (to Cunzhi Liu (grant number: 81825024)) and the Fundamental Research Funds for the Central Universities (to Hongping Li (grant number: 2020-JYB-XJSJJ-014)).
Disclosure
The authors declare no conflicts of interest.
References
1. Pettenuzzo S, Berardo A, Belluzzi E, et al. Mechanical insights into fat pads: a comparative study of infrapatellar and suprapatellar fat pads in osteoarthritis. Connect Tissue Res. 2025;66(4):272–18. doi:10.1080/03008207.2025.2502591
2. GBD 2021 Osteoarthritis Collaborators. Global, regional, and national burden of osteoarthritis, 1990-2020 and projections to 2050: a systematic analysis for the Global Burden of Disease Study 2021. Lancet Rheumatol. 2023;5(9):e508–e522. doi:10.1016/S2665-9913(23)00163-7
3. Cross M, Smith E, Hoy D, et al. The global burden of Hip and knee osteoarthritis: estimates from the global burden of disease 2010 study. Ann Rheum Dis. 2014;73(7):1323–1330. doi:10.1136/annrheumdis-2013-204763
4. Poenaru D, Sandulescu MI, Potcovaru CG, et al. High-Intensity Laser Therapy in Pain Management of Knee Osteoarthritis. Biomedicines. 2024;12(8):1679. doi:10.3390/biomedicines12081679
5. Geng R, Li J, Yu C, et al. Knee osteoarthritis: current status and research progress in treatment (Review). Exp Ther Med. 2023;26(4):481. doi:10.3892/etm.2023.12180
6. Pradelli L, Sinigaglia T, Migliore A, et al. Non-Surgical Treatment of Knee Osteoarthritis: multidisciplinary Italian Consensus on Best Practice. Ther Clin Risk Manag. 2021;17:507–530. doi:10.2147/TCRM.S288196
7. Kolasinski SL, Neogi T, Hochberg MC, et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Care Res. 2020;72(2):149–162. doi:10.1002/acr.24131
8. Brophy RH, Fillingham YA. AAOS Clinical Practice Guideline Summary: management of Osteoarthritis of the Knee (Nonarthroplasty. Third Edition J Am Acad Orthop Surg. 2022;30(9):e721–e729. doi:10.5435/JAAOS-D-21-01233
9. Witt C, Brinkhaus B, Jena S, et al. Acupuncture in patients with osteoarthritis of the knee: a randomised trial. Lancet. 2005;366(9480):136–143. doi:10.1016/S01406736(05)66871-7
10. Scharf HP, Mansmann U, Streitberger K, et al. Acupuncture and knee osteoarthritis: a three-armed randomized trial. Ann Intern Med. 2006;145(1):12–20. doi:10.7326/0003-4819-145-1-200607040-00005
11. Tu JF, Yang JW, Shi GX, et al. Efficacy of Intensive Acupuncture Versus Sham Acupuncture in Knee Osteoarthritis: a Randomized Controlled Trial. Arthritis Rheumatol. 2021;73(3):448–458. doi:10.1002/art.41584
12. Liu W, Fan Y, Wu Y, et al. Efficacy of Acupuncture-Related Therapy in the Treatment of Knee Osteoarthritis: a Network Meta-Analysis of Randomized Controlled Trials. J Pain Res. 2021;14:2209–2228. doi:10.2147/JPR.S315956
13. Liu CY, Duan YS, Zhou H, et al. Clinical effect and contributing factors of acupuncture for knee osteoarthritis: a systematic review and pairwise and exploratory network meta-analysis. BMJ Evid Based Med. 2024;29(6):374–384. doi:10.1136/bmjebm-2023-112626
14. Zhang W, Zhang L, Yang S, et al. Electroacupuncture ameliorates knee osteoarthritis in rats via inhibiting NLRP3 inflammasome and reducing pyroptosis. Mol Pain. 2023;19:17448069221147792. doi:10.1177/17448069221147792
15. Li Y, Yang M, Wu F, et al. Mechanism of electroacupuncture on inflammatory pain: neural-immune-endocrine interactions. J Tradit Chin Med. 2019;39(5):740–749 doi:10.19852/j.cnki.jtcm.2019.05.01.
16. Cañada-García D, Calvo-Enrique L, Lisa S, et al. Gene expression analyses in mouse sensory ganglia determine a crucial role of NGF/TrkA in knee osteoarthritis chronification. Osteoarthritis Cartilage. 2025. doi:10.1016/j.joca.2025.06.004
17. Wangzhou A, Price TJ. Reinvigorating drug development around NGF signaling for pain. J Clin Invest. 2025;135(4):e189029. doi:10.1172/JCI189029
18. Takano S, Uchida K, Miyagi M, et al. Nerve Growth Factor Regulation by TNF-α and IL-1β in Synovial Macrophages and Fibroblasts in Osteoarthritic Mice. J Immunol Res. 2016;2016:5706359. doi:10.1155/2016/5706359
19. Lee S, Hwang C, Marini S, et al. NGF-TrkA signaling dictates neural ingrowth and aberrant osteochondral differentiation after soft tissue trauma. Nat Commun. 2021;12(1):4939. doi:10.1038/s41467-021-25143-z
20. Omerbašić D, Smith ES, Moroni M, et al. Hypofunctional TrkA Accounts for the Absence of Pain Sensitization in the African Naked Mole-Rat. Cell Rep. 2016;17(3):748–758. doi:10.1016/j.celrep.2016.09.035
21. Kumar V, Mahal BA. NGF - the TrkA to successful pain treatment. J Pain Res. 2012;5:279–287. doi:10.2147/JPR.S33408
22. Liu Z, Li M, Zhang L, et al. NGF Signaling Exacerbates KOA Peripheral Hyperalgesia via the Increased TRPV1-Labeled Synovial Sensory Innervation in KOA Rats. Pain Res Manag. 2024;2024:1552594. doi:10.1155/2024/1552594
23. O-Sullivan I, Kc R, Singh G, et al. Sensory Neuron-Specific Deletion of Tropomyosin Receptor Kinase A (TrkA) in Mice Abolishes Osteoarthritis (OA) Pain via NGF/TrkA Intervention of Peripheral Sensitization. Int. J Mol Sci. 2022;23(20):12076. doi:10.3390/ijms232012076
24. Ohashi Y, Uchida K, Fukushima K, et al. NGF Expression and Elevation in Hip Osteoarthritis Patients with Pain and Central Sensitization. Biomed Res Int. 2021;2021:9212585. doi:10.1155/2021/9212585
25. Percie du Sert N, Hurst V, Ahluwalia A, et al. The ARRIVE guidelines 2.0: updated guidelines for reporting animal research. Br J Pharmacol. 2020;177(16):3617–3624. doi:10.1111/bph.15193
26. Seo BK, Sung WS, Park YC, et al. The electroacupuncture-induced analgesic effect mediated by 5-HT1, 5-HT3 receptor and muscarinic cholinergic receptors in rat model of collagenase-induced osteoarthritis. BMC Complementary and Alternative Medicine. 2016;16(212):1 doi:10.1186/s12906-016-1204-z.
27. Yuan XC, Wang Q, Su W, et al. Electroacupuncture potentiates peripheral CB2 receptor-inhibited chronic pain in a mouse model of knee osteoarthritis. J Pain Res. 2018;11:2797–2808. doi:10.2147/JPR.S171664
28. Guingamp C, Gegout-Pottie P, Philippe L, et al. Mono-iodoacetate-induced experimental osteoarthritis: a dose-response study of loss of mobility, morphology, and biochemistry. Arthritis Rheum. 1997;40(9):1670–1679. doi:10.1002/art.1780400917
29. Gerwin N, Bendele AM, Glasson S, et al. The OARSI histopathology initiative— recommendations for histological assessments of osteoarthritis in the rat. Osteoarthritis Cartilage. 2010;18(Suppl 3):S24–34 doi:10.1016/j.joca.2010.05.030.
30. Ozeki N, Muneta T, Mizuno M, et al. Preparation of Synovial Mesenchymal Stem Cells from a Rat Knee Joint. Bio-Protocol. 2016;6(9):e1799. doi:10.21769/BioProtoc.1799
31. Sleigh JN, Weir GA, Schiavo G. A simple, step-by-step dissection protocol for the rapid isolation of mouse dorsal root ganglia. BMC Res Notes. 2016;9:82. doi:10.1186/s13104-016-1915-8
32. Pitcher T, Sousa-Valente J, Malcangio M. The Monoiodoacetate Model of Osteoarthritis Pain in the Mouse. J Vis Exp. 2016;2016(111):53746. doi:10.3791/53746
33. Cai FH, Li FL, Zhang YC, et al. Research on electroacupuncture parameters for knee osteoarthritis based on data mining. Eur J Med Res. 2022;27(1):162. doi:10.1186/s40001-022-00795-9
34. Vongsirinavarat M, Nilmart P, Somprasong S, et al. Identification of knee osteoarthritis disability phenotypes regarding activity limitation: a cluster analysis. BMC Musculoskelet Disord. 2020;21(1):237. doi:10.1186/s12891-020-03260-y
35. Yasuda T. Cartilage destruction by matrix degradation products. Mod Rheumatol. 2006;16(4):197–205. doi:10.1007/s10165-006-0490-6
36. Bedingfield SK, Fang Y, Liu DD, et al. Matrix-targeted Nanoparticles for MMP13 RNA Interference Blocks Post-Traumatic Osteoarthritis. bioRxiv. 2020;01(30):925321. doi:10.1101/2020.01.30.925321
37. Yu H, Huang T, Lu WW, et al. Osteoarthritis Pain. Int J Mol Sci. 2022;23(9):4642. doi:10.3390/ijms23094642
38. Romeo HE, Weihe E, Müller S, et al. Protein gene product (PGP) 9.5 immunoreactivity in nerve fibres and pinealocytes of Guinea-pig pineal gland: interrelationship with tyrosine- hydroxylase- and neuropeptide-Y-immunoreactive nerve fibres. Cell Tissue Res. 1993;271(3):477–484. doi:10.1007/BF02913730
39. Walsh DA, McWilliams DF, Turley MJ, et al. Angiogenesis and nerve growth factor at the osteochondral junction in rheumatoid arthritis and osteoarthritis. Rheumatology. 2010;49(10):1852–1861. doi:10.1093/rheumatology/keq188
40. Tong L, Yu H, Huang X, et al. Current understanding of osteoarthritis pathogenesis and relevant new approaches. Bone Res. 2022;10(1):60 doi:10.1038/s41413-022-00226-9.
41. Malerba F, Bruni Ercole B, Florio R, et al. A Quantitative Bioassay to Determine the Inhibitory Potency of NGF-TrkA Antagonists. SLAS Discov. 2021;26(6):823–830. doi:10.1177/24725552211000672
42. Guzman RE, Evans MG, Bove S, et al. Mono-iodoacetate-induced histologic changes in subchondral bone and articular cartilage of rat femorotibial joints: an animal model of osteoarthritis. Toxicol Pathol. 2003;31(6):619–624. doi:10.1080/01926230390241800
43. Wang M, Tan G, Jiang H, et al. Molecular crosstalk between articular cartilage, meniscus, synovium, and subchondral bone in osteoarthritis. Bone Joint Res. 2022;11(12):862–872. doi:10.1302/2046-3758.1112.BJR-2022-0215.R1
44. Ozeki N, Koga H, Sekiya I. Degenerative Meniscus in Knee Osteoarthritis: from Pathology to Treatment. Life. 2022;12(4):603. doi:10.3390/life12040603
45. von Loga IS, El-Turabi A, Jostins L, et al. Active immunisation targeting nerve growth factor attenuates chronic pain behaviour in murine osteoarthritis. Ann Rheum Dis. 2019;78(5):672–675. doi:10.1136/annrheumdis-2018-214489
46. Kc R, Li X, Kroin JS, et al. PKCδ null mutations in a mouse model of osteoarthritis alter osteoarthritic pain independently of joint pathology by augmenting NGF/TrkA induced axonal outgrowth. Ann Rheum Dis. 2024;83(7):e17. doi:10.1136/annrheumdis-2015-208444
47. Nocchi L, Portulano C, Franciosa F, et al. Nerve growth factor-mediated photoablation of nociceptors reduces pain behavior in mice. Pain. 2019;160(10):2305–2315. doi:10.1097/j.pain.0000000000001620
48. Nwosu LN, Mapp PI, Chapman V, et al. Blocking the tropomyosin receptor kinase A (TrkA) receptor inhibits pain behaviour in two rat models of osteoarthritis. Ann Rheum Dis. 2016;75(6):1246–1254. doi:10.1136/annrheumdis-2014-20720
49. Zhao YX, Yao MJ, Shen JW, et al. Electroacupuncture attenuates nociceptive behaviors in a mouse model of cancer pain. Mol Pain. 2024;20:17448069241240692. doi:10.1177/17448069241240692
50. Rowan A. Keeping Trk of Pain. Nat Rev Neurosci. 2005;6:496. doi:10.1038/nrn1707
51. Tomotsuka N, Kaku R, Obata N, et al. Up-regulation of brain-derived neurotrophic factor in the dorsal root ganglion of the rat bone cancer pain model. J Pain Res. 2014;7:415–423. doi:10.2147/JPR.S63527
52. Obata K, Katsura H, Sakurai J, et al. Suppression of the p75 neurotrophin receptor in uninjured sensory neurons reduces neuropathic pain after nerve injury. J Neurosci. 2006;26(46):11974–11986. doi:10.1523/JNEUROSCI.3188-06.2006
53. Yu T, Calvo L, Anta B, et al. In vivo regulation of NGF-mediated functions by Nedd4-2 ubiquitination of TrkA. J Neurosci. 2014;34(17):6098–6106. doi:10.1523/JNEUROSCI.4271-13.2014
54. Averill S, McMahon SB, Clary DO, et al. Immunocytochemical localization of trkA receptors in chemically identified subgroups of adult rat sensory neurons. Eur J Neurosci. 1995;7(7):1484–1494. doi:10.1111/j.1460-9568.1995.tb01143.x
55. Nencini S, Ringuet M, Kim DH, et al. Mechanisms of nerve growth factor signaling in bone nociceptors and in an animal model of inflammatory bone pain. Mol Pain. 2017;13:1744806917697011. doi:10.1038/s41598-020-72227-9
56. Alves CJ, Couto M, Sousa DM, et al. Nociceptive mechanisms driving pain in a post traumatic osteoarthritis mouse model. Sci Rep. 2020;10(1):15271. doi:10.1038/s41598-020-72227-9
57. Hu Q, Ecker M. Overview of MMP-13 as a Promising Target for the Treatment of Osteoarthritis. Int J Mol Sci. 2021;22(4):1742. doi:10.3390/ijms22041742
58. Sengprasert P, Kamenkit O, Tanavalee A, et al. The Immunological Facets of Chondrocytes in Osteoarthritis. J Rheumatol. 2024;51(1):13–25 doi:10.3899/jrheum.2023-0816.
59. Wang MG, Seale P, Furman D. The infrapatellar fat pad in inflammaging, knee joint health, and osteoarthritis. Npj Aging. 2024;10(34):1 doi:10.1038/s41514-024-00159-z.
60. Fontanet P, Irala D, Alsina FC, et al. Pea3 transcription factor family members Etv4 and Etv5 mediate retrograde signaling and axonal growth of DRG sensory neurons 32 644–650 in response to NGF. J Neurosci. 2013;33(40):15940–15951. doi:10.1523/JNEUROSCI.0928-13.2013
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Pain Empathy and Its Association with the Clinical Pain in Knee Osteoarthritis Patients
Zhao R, Ji Y, Li J, Li X, Wu T, Wu H, Liu C
Journal of Pain Research 2022, 15:4017-4027
Published Date: 19 December 2022
Modulation of Brain Network Topological Properties in Knee Osteoarthritis by Electroacupuncture in Rats
Zhang JP, Shen J, Xiang YT, Xing XX, Kang BX, Zhao C, Wu JJ, Zheng MX, Hua XY, Xiao LB, Xu JG
Journal of Pain Research 2023, 16:1595-1605
Published Date: 17 May 2023
Hotspots and Trends in Research on Treating Pain with Electroacupuncture: A Bibliometric and Visualization Analysis from 1994 to 2022
Hu L, Yang J, Liu T, Zhang J, Huang X, Yu H
Journal of Pain Research 2023, 16:3673-3691
Published Date: 3 November 2023
The Impact of Fu’s Subcutaneous Needling on Lower Limb Muscle Stiffness in Knee Osteoarthritis Patients: Study Protocol for a Pilot Randomized Controlled Trial
Li H, Yang CC, Bai T, Sun J, Fu Z, Mi J, Chou LW
Journal of Pain Research 2024, 17:3315-3326
Published Date: 9 October 2024
Combination Treatment with Thread-Embedding Acupuncture and Electroacupuncture for Knee Osteoarthritis Patients with Postoperative Pain: A Randomized Controlled Feasibility Study
Lee YJ, Han CH, Jeon JH, Kim E, Park KH, Kim AR, Kim YI
Journal of Pain Research 2025, 18:89-103
Published Date: 8 January 2025