Back to Journals » Journal of Pain Research » Volume 16
Hotspots and Trends in Research on Treating Pain with Electroacupuncture: A Bibliometric and Visualization Analysis from 1994 to 2022
Authors Hu L ![]() , Yang J, Liu T, Zhang J, Huang X, Yu H
, Yang J, Liu T, Zhang J, Huang X, Yu H
Received 1 June 2023
Accepted for publication 19 October 2023
Published 3 November 2023 Volume 2023:16 Pages 3673—3691
DOI https://doi.org/10.2147/JPR.S422614
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Houman Danesh
Liyu Hu, Jikang Yang, Ting Liu, Jinhuan Zhang, Xingxian Huang, Haibo Yu
The Fourth Clinical Medical College of Guangzhou University of Chinese Medicine, Guangzhou University of Chinese Medicine, Shenzhen, People’s Republic of China
Correspondence: Haibo Yu, The Fourth Clinical Medical College of Guangzhou University of Chinese Medicine, No. 1 Fuhua Road, Futian District, Shenzhen, 518000, People’s Republic of China, Tel +8613603066098, Email [email protected]
Purpose: Electroacupuncture is widely used to pain management. A bibliometric analysis was conducted to identify the hotspots and trends in research on electroacupuncture for pain.
Methods: We retrieved studies published from 1994– 2022 on the topic of pain relief by electroacupuncture from the Web of Science Core Collection database. We comprehensively analysed the data with VOSviewer, CiteSpace, and bibliometrix. Seven aspects of the data were analysed separately: annual publication outputs, countries, institutions, authors, journals, keywords and references.
Results: A total of 2030 papers were analysed, and the number of worldwide publications continuously increased over the period of interest. The most productive country and institution in this field were China and KyungHee University. Evidence-Based Complementary and Alternative Medicine was the most productive journal, and Pain was the most co-cited journal. Han Jisheng, Fang Jianqiao, and Lao Lixing were the most representative authors. Based on keywords and references, three active areas of research on EA for pain were mechanisms, randomized controlled trials, and perioperative applications. Three emerging trends were functional magnetic resonance imaging (fMRI), systematic reviews, and knee osteoarthritis.
Conclusion: This study comprehensively analysed the research published over the past 28 years on electroacupuncture for pain treatment, using bibliometrics and science mapping analysis. This work presents the current status and landscape of the field and may serve as a valuable resource for researchers. Chronic pain, fMRI-based mechanistic research, and the perioperative application of electroacupuncture are among the likely foci of future research in this area.
Keywords: bibliometrics, electroacupuncture, pain, VOSviewer, CiteSpace, blibliometrix
Introduction
Pain is an unpleasant sensory and emotional experience that may or may not be linked to tissue damage.1 Various methodologies are employed to categorize pain, including physiological and pathological classifications.2 Physiological pain serves a protective role, while pathological pain, such as postherpetic neuralgia and trigeminal neuralgia, predominates in medical consultations. Pain can also be anatomically classified into somatic pain, visceral pain, and referred pain. Somatic pain encompasses discomfort on the body’s surface and within joints and muscles. Treatment strategies depend on the underlying cause. Neuropathic pain often involves non-opioid analgesics, tricyclic antidepressants, and antiepileptic drugs. Nonneuropathic pain, such as osteoarthritis, is managed with nonsteroidal anti-inflammatory drugs. Acute pain management often entails opioid analgesics.3 With pain affecting more than 30% of the global population, and resulting in substantial economic burdens, it is imperative to establish a treatment modality that is not only highly effective but also safe for prolonged implementation.4,5
Electroacupuncture (EA) is an approach that combines traditional acupuncture with electrical stimulation. EA presents favorable outcomes in pain management and quality-of -life enhancement, surpassing manual acupuncture due to its added electrical stimulation at specific frequencies.6–9 The effectiveness of EA correlates with current intensity and frequency.10 Higher frequencies swiftly induce serotonin and endorphin release for short-term pain relief, while lower frequencies trigger enkephalin and dynorphin secretion, leading to prolonged analgesic effects.11 Consequently, EA has emerged as a promising adjunctive therapy for both acute and chronic pain conditions.6,12 Notably, EA also provides a more readily standardized and suitable treatment paradigm than manual acupuncture for future clinical studies.13 Despite an increasing body of mechanistic and clinical research on EA analgesia, the status, potential clinical applications and future directions of this research remain unclear. Prior research has focused on specific pain disorders such as low back pain, migraine and chronic pain.14–16 However, several systematic evaluations have suggested that current clinical studies are of poor quality. Hence, a knowledge map of the status of research is required to identify the strengths and challenges that must be addressed to facilitate the development of in-depth investigations.
The study of bibliometrics presents a valuable quantitative basis for comprehending fundamental themes and research patterns within a given discipline on a global scale. It has the advantage of identifying emerging areas of research.17 A bibliometric analysis of the global use of EA for pain has not been undertaken. Therefore, The aim of this study is to comprehensively examine the research foundation of EA in pain management by reviewing the global scientific discoveries from 1994 to 2022. Additionally, a crucial objective is to investigate the most promising research teams and potential research trends to offer guidance for future research and clinical application.
Materials and Methods
Data Collection
We conducted a literature search on the Web of Science Core Collection Database from inception to Dec. 31, 2022. We retrieved 2057 publications in January 2023, including articles, reviews, proceeding papers, early access, book chapters, and retracted publications. The search strategy included the terms “electroacupuncture” and “pain”. The search formula is shown in detail in Table 1. We included only articles or reviews published in English. For bibliometric analysis, we extracted information such as title, author, abstract, keywords, and references. After a detailed filtering process, we ultimately analysed 2030 studies.
 |
Table 1 Search Queries |
Analysis Tools
Several tools were utilized in this study for data analysis and visualization. Microsoft Office Excel 2019 was used to analyze annual publications and fit a growth function to determine the current phase of the field. VOSviewer and CiteSpace were used to explore bibliometrics, including analyses of institutions, authors, journals, keywords, and references.18–20 Citation bursts and relationships between citing and cited journals were also examined using CiteSpace.21 Bibliometrix, an R tool, was used to generate national output, collaboration networks, and strategic diagrams.22 Additionally, the H-index was utilized to evaluate academic work quality and quantity and identify important researchers and teams.23
Results
Annual Publication Outputs and Temporal Trends
A total of 2030 publications were included in our study, including 1643 (81%) articles and 387 (19%) reviews. Along with minor fluctuations, the frequency of publications demonstrates a general upward trend (Figure 1). The initial stage, spanning from 1994 to 2002, is characterized by a gradual increase in the number of publications and represents a nascent phase. Conversely, the subsequent phase, encompassing the years 2002 to 2022, can be described as a period of flourishing, evinced by exponential growth in the proliferation of publications.
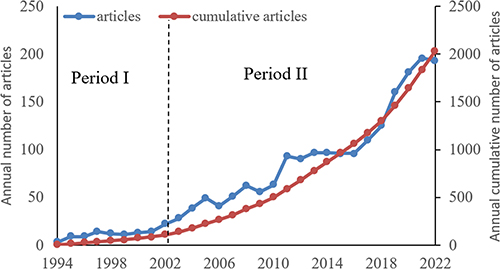 |
Figure 1 Annual publications from 1994 to 2022 and logical curve of scientific literature. |
Analysis of Countries/Regions
Fifty-two countries worldwide contributed to a total of 2030 publications on EA for pain. Figure 2a shows the annual contributions of these countries in the period from 1994 to 2022. China, the United States, Japan, and Sweden were the first to begin EA-related research, but only China and the United States have continued to explore the field. Therefore, China produced the most publications (52.71%, 1070), followed by the United States (13.69%, 278) and Korea (9.95%, 202; Table 2). The dominant countries in terms of influence appear to be the United States (H=94), China (H=82), Korea (H=53), the United Kingdom (H=47), and Australia (H=35). China, the United States, Korea, the United Kingdom and Brazil were the countries that cooperated most with other countries (Figure 2b).
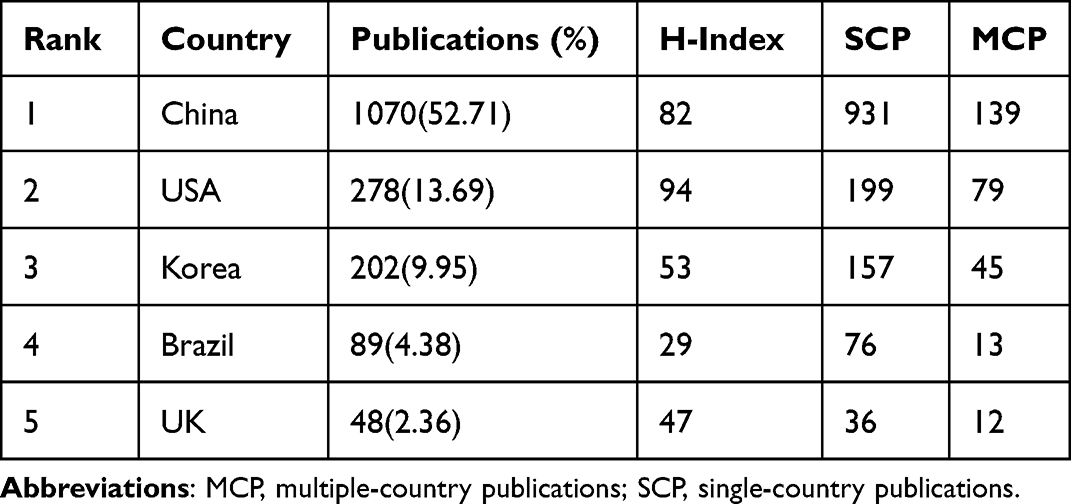 |
Table 2 The Top Five Most Productive Countries |
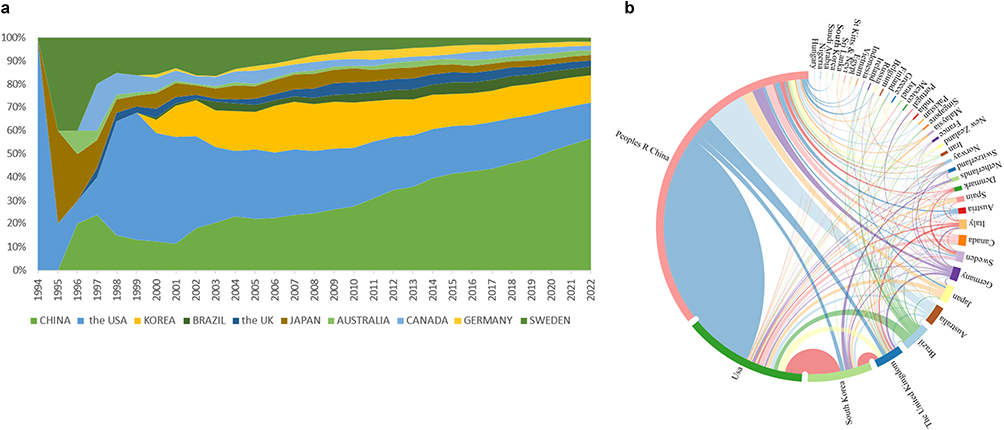 |
Figure 2 (a) Countries’ annual cumulative publication counts. (b) Collaboration network of countries/regions. |
Analysis of Institutions
The 2030 studies related to EA for pain originated from a total of 1830 institutions. Kyung Hee University (129), Chinese Academy of Medical Sciences (101), China Medical University (91), Beijing University of Chinese Medicine (85), and Zhejiang Chinese Medical University (78) ranked the top five institutions in terms of the number of publications (Table 3). A shift in highly productive institutions from Korea to China was observed (Figure 3a). A node with high betweenness centrality (BC) in CiteSpace has a strong influence on the relationship in the whole network (Figure 3b). The institutions with the top 3 BC values were Capital Medical University (0.19), Peking University (0.16) and Kyung Hee University (0.09), indicating that inter-institutional cooperation affects international cooperation and that only by breaking down academic barriers and enhancing inter-institutional cooperation can we promote the development of the discipline and improve our academic influence. Especially in China, where there are numerous institutions, it is essential to enhance the collaboration among them.
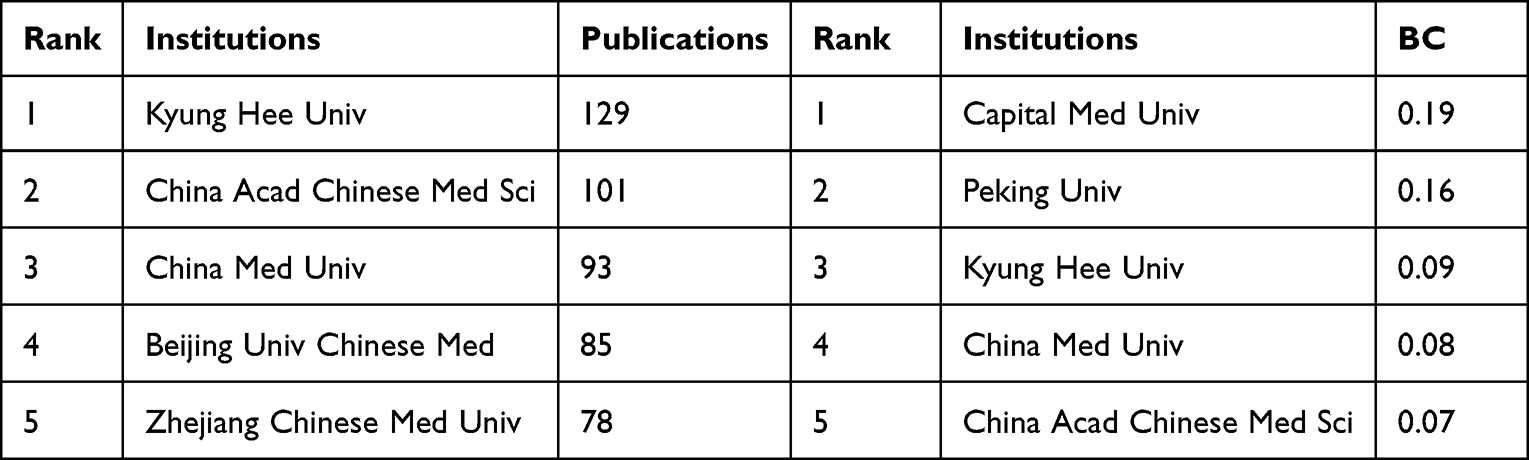 |
Table 3 The Top Five Most Productive Institutions |
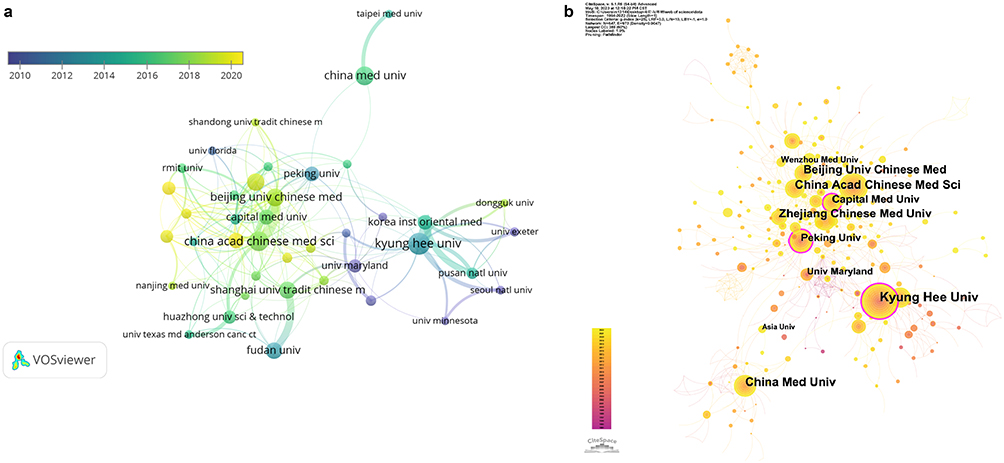 |
Figure 3 (a) Institutional collaboration network visualization map generated by VOS viewer. (b) Institutional collaboration network visualization map generated by CiteSpace. |
Analysis of Authors and Co-Cited Authors
The survey includes 8703 authors and 33941 co-cited authors. Table 4 and Table 5 present the ten most productive and co-cited authors among all authors. Figure 4 shows a visualization of the co-author network.
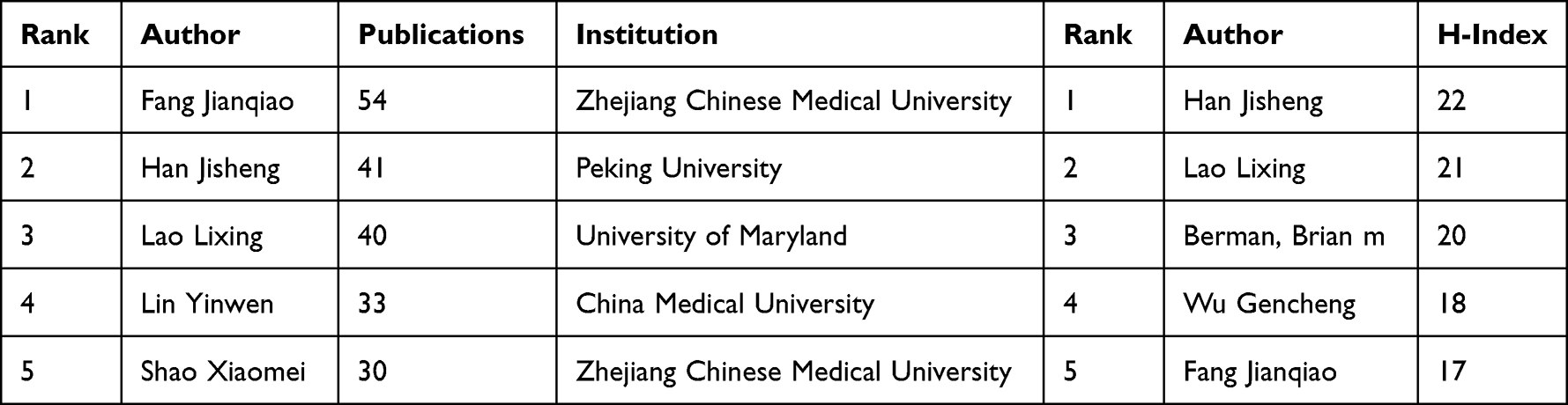 |
Table 4 Top Five Active and Influential Authors on the Topic of EA for Pain |
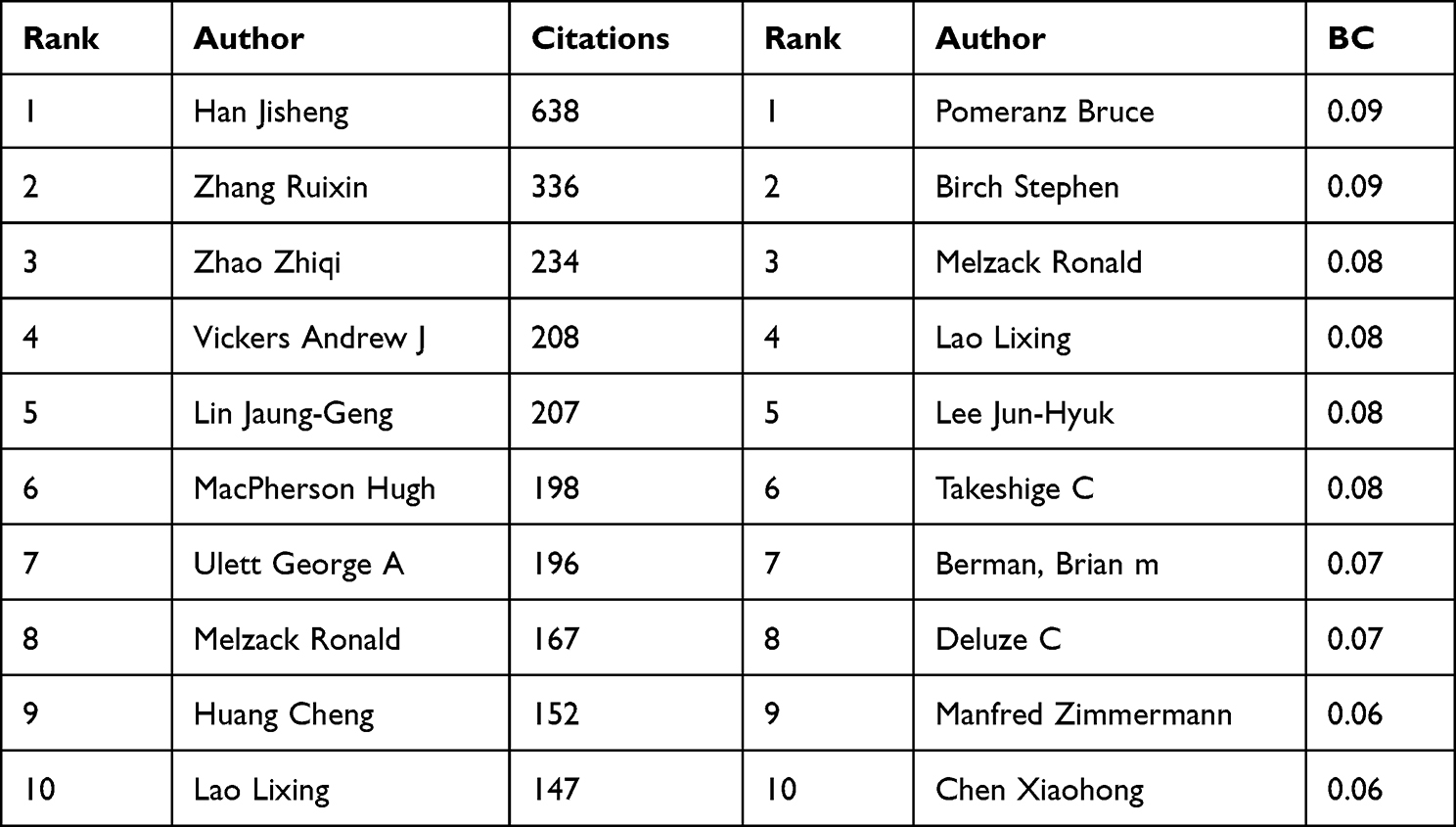 |
Table 5 Top Ten Authors on EA and Pain, Ranked by Citation Count and Co-Citation BC |
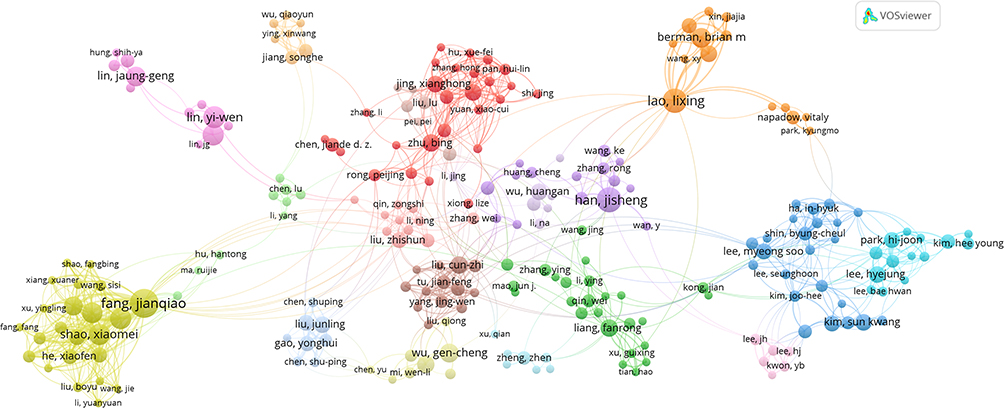 |
Figure 4 Co-authorship analyses of authors carried out with VOSviewer. |
Analysis of Authors
Highly productive and influential authors and their teams drive the development of related disciplines. The top five most productive authors are Fang Jianqiao (54), Han Jisheng (41), Lao Lixing (40), Lin Yinwen (33), and Shao Xiaomei (30; Table 4). A high H-index means that an author is an influential person who has a high number of publications and citations. The top 5 authors with the highest H-index values were Han Jisheng (H=22), Lao Lixing (H=21), Berman, Brian m (H=20), Wu Gencheng (H=18), and Fang Jianqiao (H=17; Table 4). Interestingly, most of these researchers were the same as the high-yield authors. The analysis of research teams reveals core teams (Figure 4). One team, led by Lao Lixing, Berman, Brian M, and Ren Ke, collaborates closely with Liang Fanrong and Bai Lijun’s teams. The purple and yellow clusters represent teams anchored by Han Ji Sheng and by Fang Jianqiao, Liang Yi, Shao Xiaomei, and Du Junying respectively. Comparatively, Hsieh Ching-Liang, Lin Yiwen, and Lin Jaunggeng’s teams tend to operate independently, engaging in little collaboration with others. Additionally, Wu Gencheng and Wang Yanqing lead independent teams.
Analysis of Co-Cited Authors
The most cited author was Han Jisheng (638), followed by Zhang Ruixin (336) and Zhao Zhiqi (234). Vickers Andrew J (208), Lin Jaung-Geng (207; Table 4). The top 5 authors in terms of BC were Pomeranz Bruce (0.09), Birch Stephen (0.09), Melzack Ronald (0.08), Lao Lixing (0.08), and Lee Jun-Hyuk (0.08; Table 5). Based on analysis of these results, it can be seen that Lao Lixing’s team is a very influential team, devoting themselves to mechanistic research from a neuro-immuno-endocrine perspective and improving the quality of randomized controlled trials in acupuncture.24–26
Analysis of Journals
Evidence-Based Complementary and Alternative Medicine (n =194), Acupuncture in Medicine (n =110), and Medicine (n =56) are the top 3 academic publications out of 493 journals (Table 6). These three journals’ publications made up 28.54% of all publications. Half of the ten journals in the quartile category fell into Q4, (the last 25% of the impact factor (IF) distribution). More than half of the journals’ IFs were below 3 and the average IF of these 10 journals was 2.9835. Table 7 demonstrates that Pain was the most influential journal in EA for pain. In terms of JCR, ten journals belonged almost evenly to all quartiles. More than half of the journals’ IFs were higher than 3 and the average IF of these 10 journals was 5.2955.
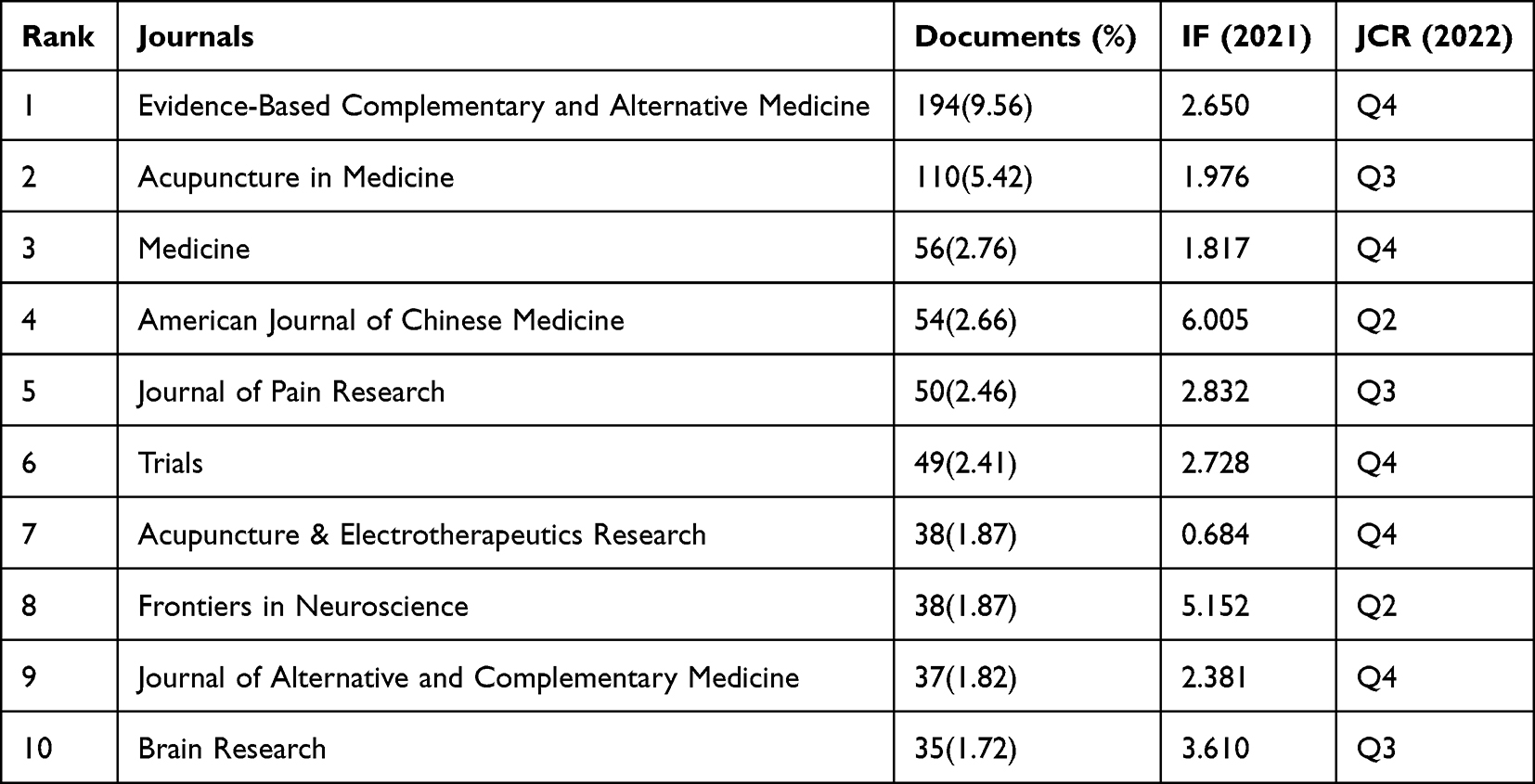 |
Table 6 Distribution of the Top Ten Journals on EA for Pain |
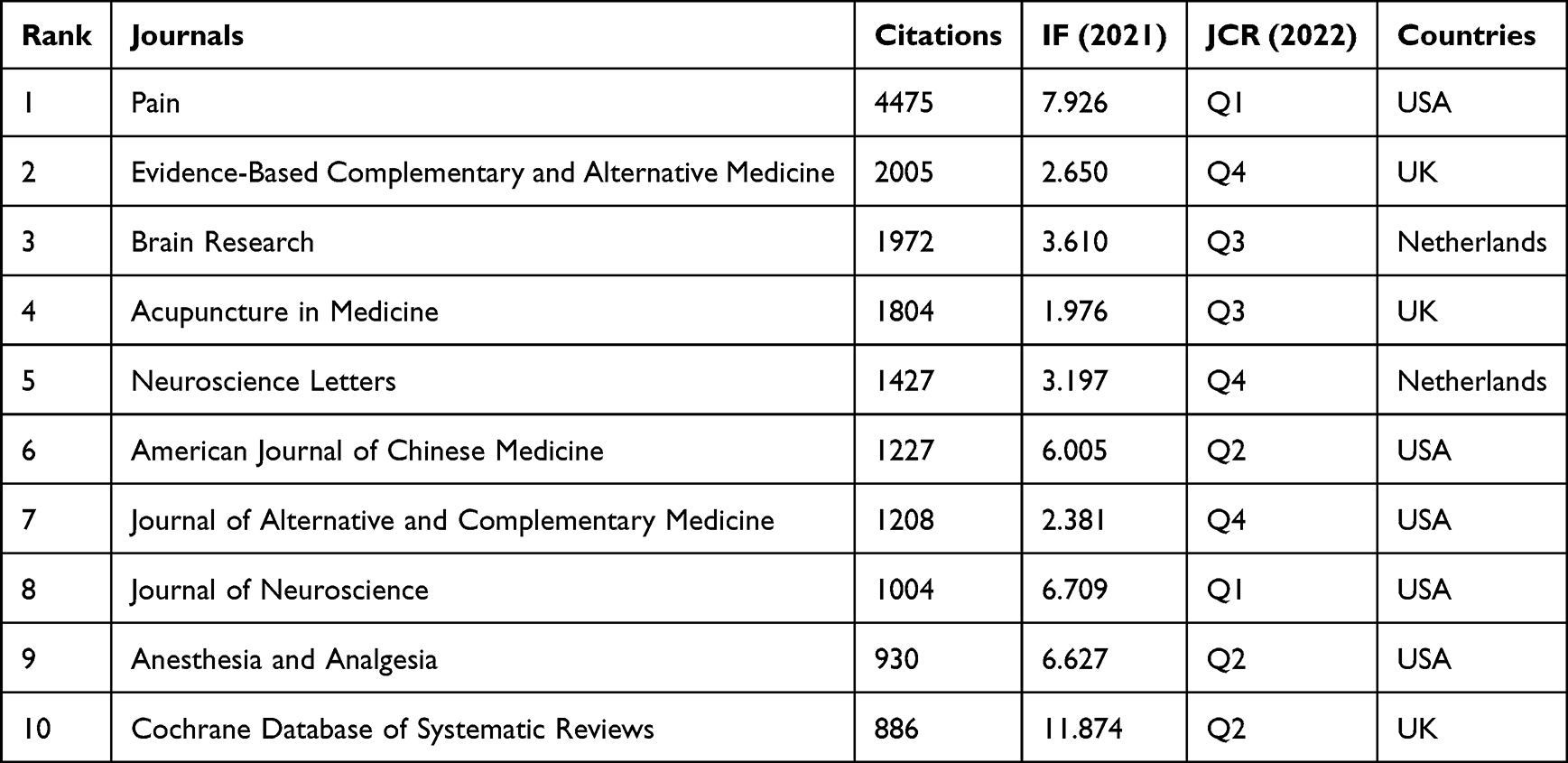 |
Table 7 Top Ten Co-Cited Journals on EA for Pain |
A Dual map of journals can facilitate analysis in terms of patterns emerging from the distributions of citation threads and the dynamics of trajectories as a function of space and time.27 The left side of the map refers to citing journals, and the right side of the map denotes the corresponding cited journals (Figure 5). As shown in Figure 5, the cited journals are mainly from disciplines “Molecular/Biology/Immunology”, “Medicine/Medical/Clinical” and “Neurology/Sports/Ophthalmology”. The citing journals are from multiple fields, such as “Health/Nursing/Medicine” and “Molecular/Biology/Genetics”.
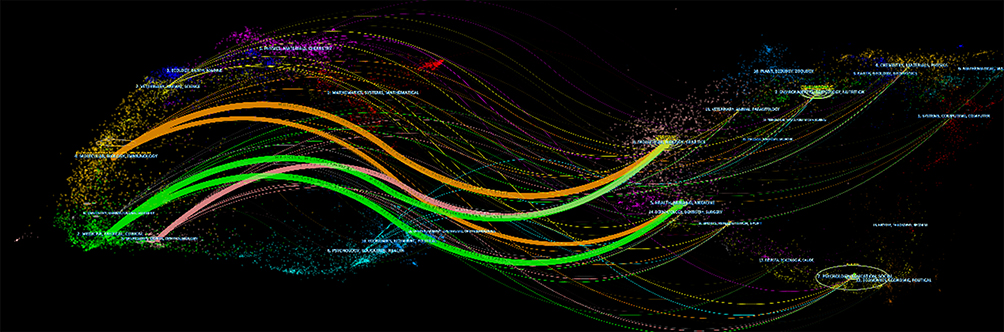 |
Figure 5 Dual-map of the overlay of journals. |
Analysis of Co-Cited References
Co-Cited Reference Networks and Co-Cited Papers
Co-citation analysis was performed to assess the correlation between articles.28 The cross-reference of publications shows the structure and trend of the corresponding scientific field.29 In our study, 52,074 cited publications were our knowledge base. By the logarithmic likelihood ratio (LLR) algorithm, we found the largest 20 clusters and clusters labelled by the titles of the citing publications (Figure 6). The total Q-value was 0.6861, and each cluster had a weighted mean silhouette of 0.8512, suggesting that the clusters had high quality. Based on the association between clusters, four major research trends were uncovered. We present clusters ranked from the largest (#0) to the smallest (#19).
 |
Figure 6 Network map of co-citation of references. |
The first and largest trend started in 1994 with 8 research clusters. These clusters, with specific information such as the label, size, silhouette score, and the average year of publication of the articles included in the cluster were as follows: cluster #10 (“fibromyalgia syndrome”; 42; S=0.972; 1996), which shared hots topics with cluster #7 (“low back pain”; 64; S =0.898; 1995), and cluster #17 (“clinical applications”; 12; S =0.998; 1987). These clusters further evolved into cluster #11 (“controlled trial”; 41; S =0.933; 1997) and cluster #8 (“visceral pain”; 59; S =0.826; 2005). The findings of the above clusters promote the research in cluster #5 (“systematic review”; 81; S =0.799; 2010), which further branches into #6(“knee osteoarthritis”; 69; S =0.847; 2010).
The second major trend of research concerns the mechanisms of acupuncture. It starts with research on EA frequency with cluster #14 (“intensity frequency”; 25; S=0.966; 1985), which develops research on the rat model with cluster #16 (“ventriculocisternal perfusate”; 13; S=0.994; 1988), #12 (“electroacupuncture-produced anti-hyperalgesia”; 35; S=0.881; 1997) and #2 (“zusanli point”; 111; S=0.774; 1989). More recently, these clusters became cluster#1 (“neuropathic pain”; 134; S=0.793; 2004) and cluster#3 (“fMRI study”; 106; S=0.835; 2004), with strong links to #0 (“signaling pathway”; 139; S=0.869; 2004), which is mainly dedicated to exploring the mechanisms of acupuncture analgesia, not only central mechanisms but also peripheral mechanisms such as local changes at acupoints.
The third major research trend concerns perioperative acupuncture. These trends began in 1995, with the first cluster on EA anesthesia for hysterectomy, cluster #9 (“abdominal hysterectomy”; 44; S=0.924; 1998) and cluster #19 (“analgesia”; 5; S=1; 1997), which evolved into cluster #4 (“postoperative pain”; 93; S=0.782; 2005) and has currently evolved into cluster #8 with EA in pain after abdominal surgery (“visceral pain”; 59; S=0.826; 2005). In addition, there are some clinical studies of EA for dysmenorrhea and perimenopausal syndrome in cluster #9.
The fourth trend concerns ethical issues, and starts with a cluster on “ethical issue”, #15 (S=0.998; 13; 1988). This topic was picked up again approximately 2000 on neuroinflammatory responses, #13 (S=0.928; 25; 2000). This cluster is proximal to “postoperative pain”, cluster #4, into which it merges.
The top five studies that received the most attention from researchers are included in Table 8. All publications were reviews. Examining this table, it becomes evident that the majority of scholars devoted considerable attention to investigating the mechanism underlying EA for pain.
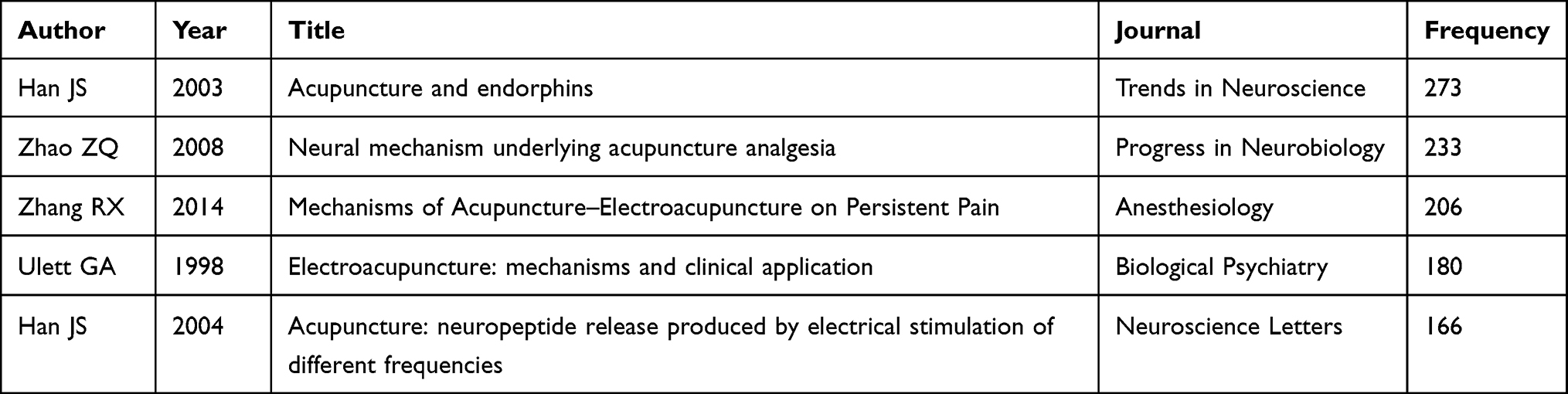 |
Table 8 Top Five Co-Cited Publications on EA for Pain |
Turning-Point Papers
Furthermore, we conducted a structural variation analysis, and identified the top 10 intellectual “turning-point” papers (Table 9). ΔBC measures the structural variation caused by an article in terms of BC in the baseline network.30 The BC is potentially valuable for detecting interdisciplinary activities. These 10 articles are not the most cited, even with fewer than 20 citations, but they are playing a key role in setting new research trends. They all influenced the structure of at least two clusters. The top 5 studies mainly focused on the verified effectiveness and safety of EA for menopausal symptoms, postoperative analgesia and low back pain.11,31,32 One of the papers calls for urgent improvement in the quality of acupuncture clinical trial design and notes that sham acupuncture has a greater effect than drugs and other placebos.33 Additionally, a new animal model of external ankle joint pain was established.34
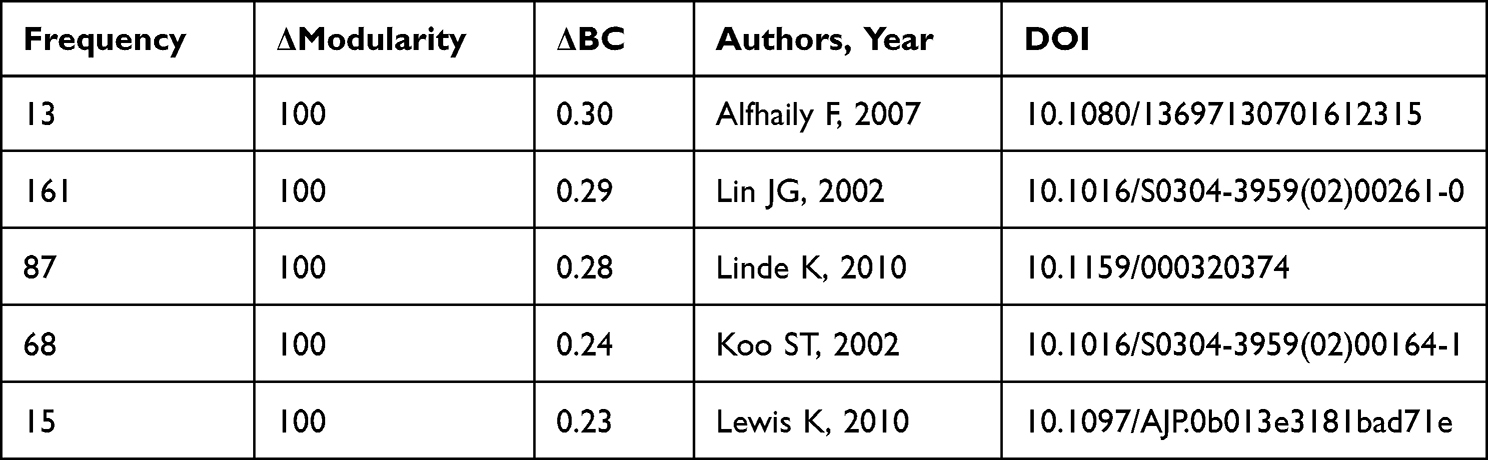 |
Table 9 Top Five Publications with the Strongest BC Divergency in the Co-Citation Network |
Analysis of Keywords
Theme Evolution Analysis
Theme evolution analysis can be used to detect, quantify and visualize areas of hotspots of research interest.35 Based on the previous description, we used 2002 as a cut-off point in the strategy map, and the horizontal axis and vertical axis represent the centrality and density of the keywords respectively. The strategy map can be divided into four quadrants based on centrality and density. Quadrant one comprises clusters that possess strong centrality and high density and are crucial to the knowledge base structure. Quadrant two includes well-developed clusters that are not currently significant to the research field. Quadrant three features themes that are not yet fully developed but may be new and emerging. Quadrant four hosts basic, important themes to the research field.
“Acupuncture/pain/nociception”, “electroacupuncture/analgesia/spinal cord/chronic pain”, “physical therapy/tennis elbow”, and “met-enkephalin/immunocytochemistry” were motor themes from 1994 to 2002. Mechanisms of “orphan fibropeptide” are also well explored. “Chronic pain” and “central nervous system” were emerging. (Figure 7a).
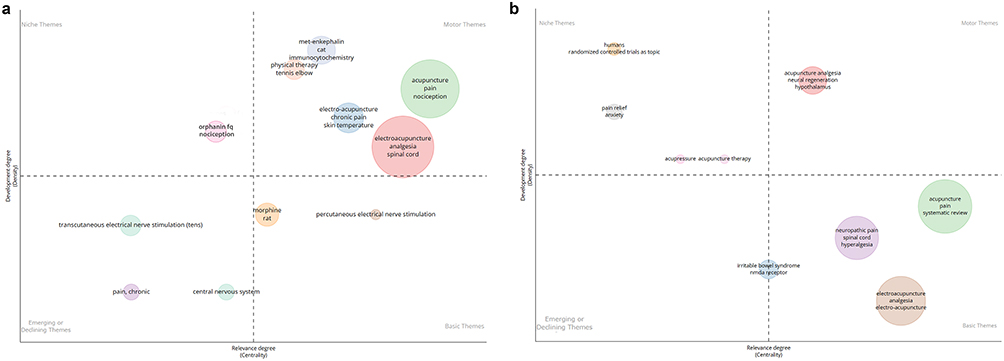 |
Figure 7 (a) Strategic diagrams of EA for pain research (1994–2002). (b) Strategic diagrams of EA for pain research (2002–2022). |
From 2002 to 2022, motor themes in the previous stage were developed into basic themes. Notably, “randomized controlled trials”, “pain relief”, and “anxiety” have been niche themes. “Acupuncture analgesia” remained a motor theme. Additionally, “neural generation” and “hypothalamus” could be related to “central nervous system” (Figure 7b).
Co-Occurrence Analysis
Co-occurrence network analysis of keywords was conducted by VOSviewer.36 Keywords were divided into 5 clusters (Figure 8) and the largest red cluster included 82 keywords, among which the keywords “analgesia” and “neuropathic pain” received the most attention (Table 10). The second is the green cluster, which consists of EA clinical applications, such as “electroacupuncture”, “pain”, “management”, and “randomized controlled trail”. The blue cluster focused on the use of perioperative acupuncture named acupuncture anesthesia, and the yellow cluster focused on human brain fMRI studies of acupuncture analgesia.
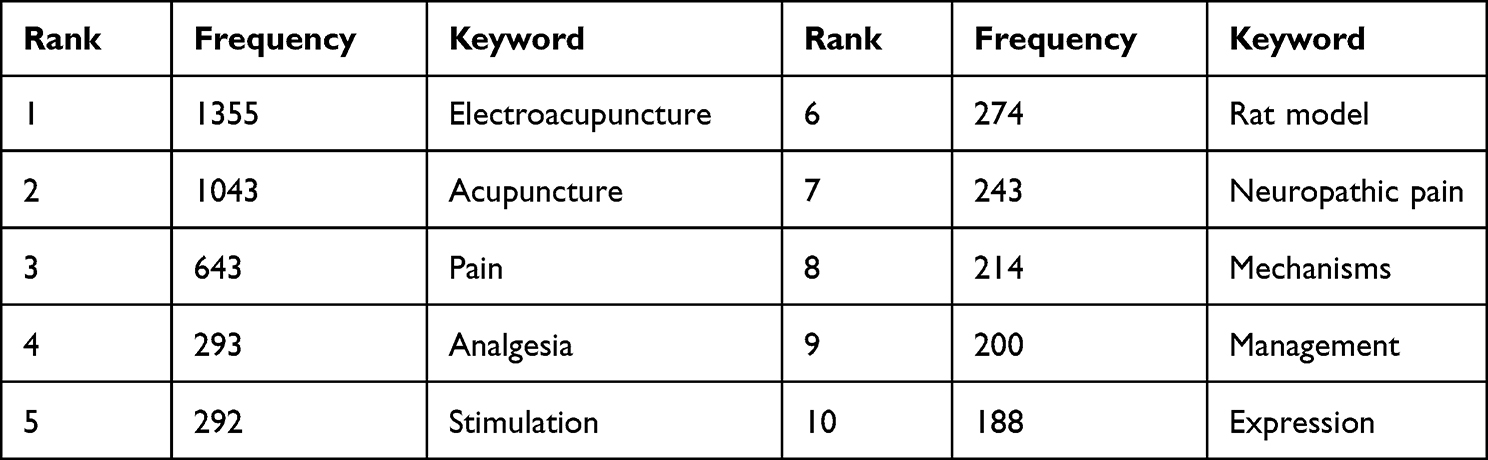 |
Table 10 Top 10 Keywords Ranked by Frequency |
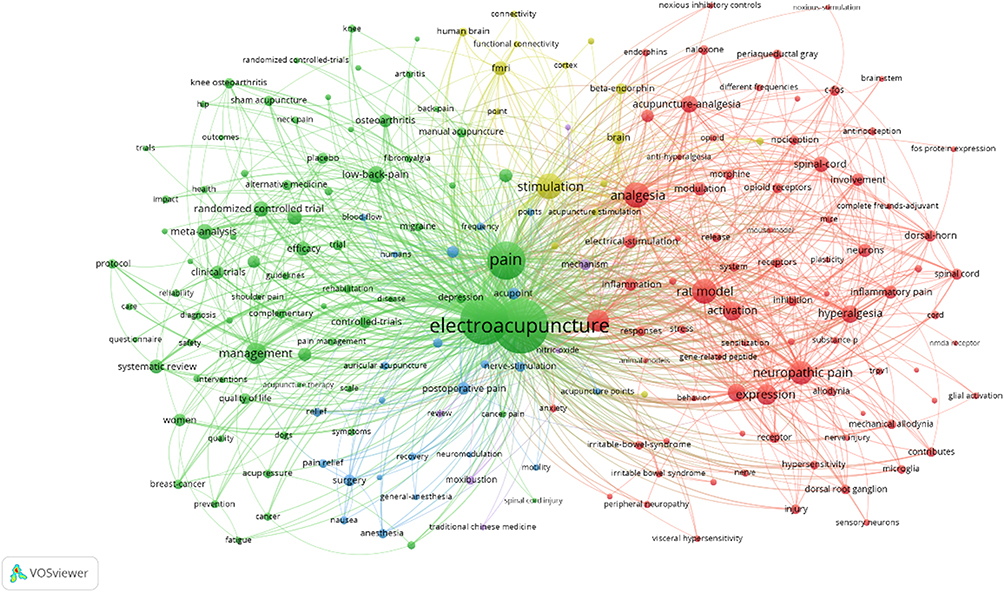 |
Figure 8 Co-occurrence network map of keywords. |
Keywords Burst Detection Analysis
A total of 74 keywords were detected in the keyword co-occurrence network for EA and pain, and the top 25 keywords are shown in Table 11. Based on the chronological order, the earliest keyword cited in the outbreak was “acupuncture analgesia” (15.66), and this keyword was focused on for 20 years (1994–2014). It was followed by “electroacupuncture analgesia” (1995–2003) and “analgesia”, but there are differences in their scope. With the deepening of research, the keywords “knee osteoarthritis”, “systematic review”, “depression”, “guideline”, “surgery”, and “validation” have received attention in recent years. It is clear that recent studies have focused more on clinical efficacy. Besides, we performed keyword bursting for each cluster individually, and the results are consistent with the trend of the results above, as detailed in the Supplementary File. The top 5 keywords are drawn from distinct clusters, with some being unique to a single cluster. For instance, the first two keywords originated from Cluster 1 (Supplementary Figure 1) and the third keyword from Cluster 3 (Supplementary Figure 2). While the fourth keyword recurs in Cluster 0 (Supplementary Figure 3), Cluster 1, and Cluster 4 (Supplementary Figure 4), and the fifth keyword is repeatedly found in Cluster 3, Cluster 2 (Supplementary Figure 5), and Cluster 0.
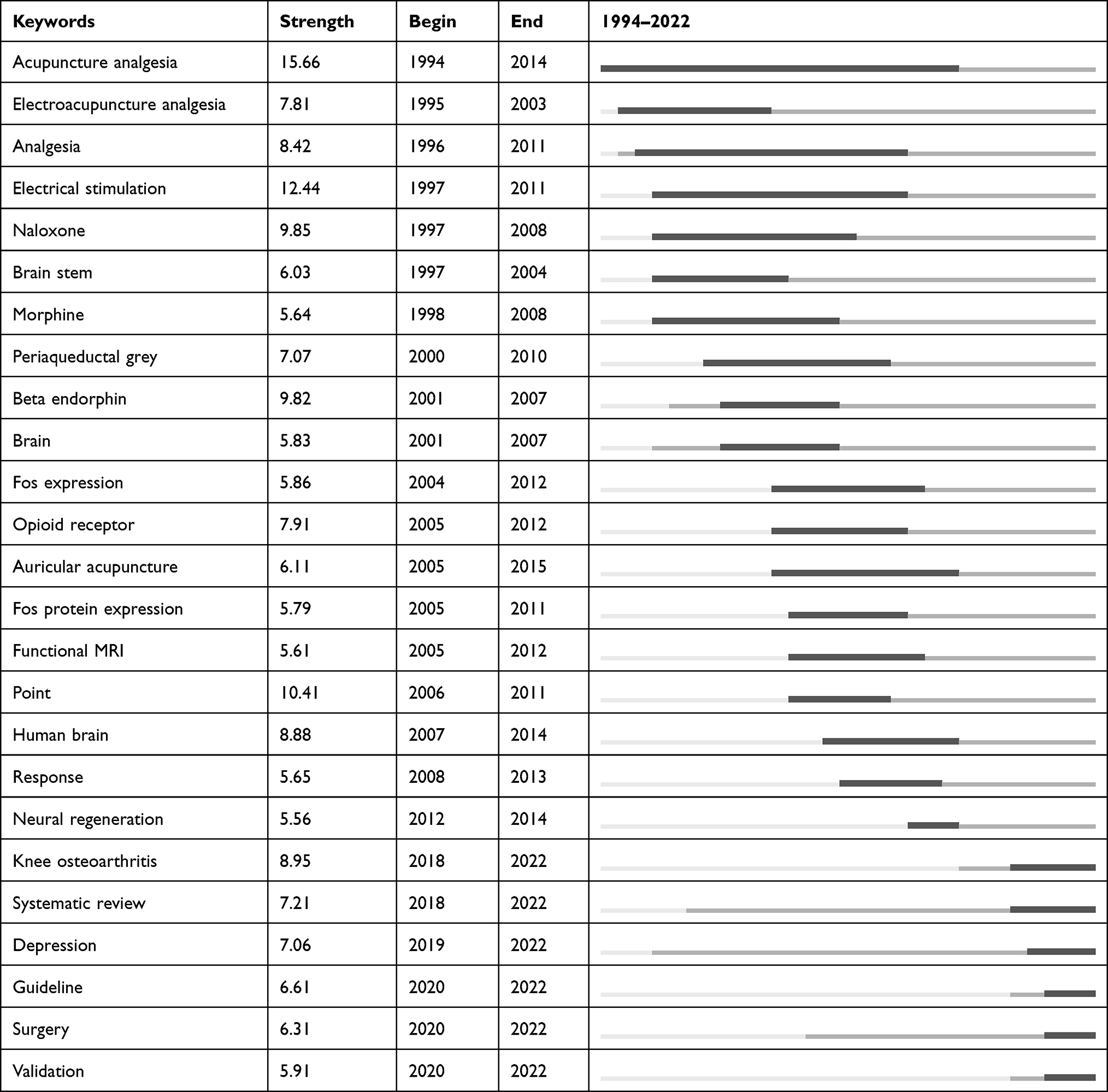 |
Table 11 Top 25 Keywords with the Beginning Year of Burst |
Discussion
Summary of the Main Findings
We present a comprehensive overview of the development of EA and pain research over the past 28 years using three software programs (CiteSpace, VOSviewer, Bibliometrix R package).
Outputs of Publications
We identified an exponential growth of publications on EA for pain since 2002, and the number of studies published per year thus far is still on an upward trend. This means that there is considerable potential for research in this area. On the other hand, the growing trend in the literature shows that there has not been breakthrough for the time being, which may be related to the complexity of the acupuncture effect.
China was the country with the most publications, followed by the USA. Over the past 20 years, China has shown explosive growth in relevant publications, gradually overtaking the original leader, the United States. Since 2016, China has enacted legislation to determine the status of traditional Chinese medicine and provided strong support for its development, inspiring numerous scholars. This may also be the reason for the increase in the number of publications in China. The top 10 output institutions originated from South Korea and China. Kyung Hee University is the most prolific institution, followed by several Chinese medicine schools in China. The top three high-yield authors are Fang Jianqiao, Han Jisheng, and Lao Lixing. Correspondingly, they come from China and the United States.
From countries to institutions and authors, the findings of this survey indicate that China, the United States, and South Korea are leading the trend in EA for pain.
Status of Journals
Evidence-Based Complementary and Alternative Medicine, Acupuncture in Medicine, and Medicine were the top three journals. Their IF are all below 3 for two reasons in particular. First, research quality may need improvement. Second, the effects of acupuncture are quite complex and the mechanisms underlying its efficacy are difficult to elucidate. The aforementioned issues constitute the challenges that we must confront in future research endeavors. Evidence-Based Complementary and Alternative Medicine, Cochrane Database Systematic Reviews, and Pain were the most influential journals, which may be related to the type and scope of literature in the journals. The high self-citation rate in the field may be attributed to the fact that Evidence-Based Complementary and Alternative Medicine boasts the highest number of publications and H-index in the field.
We can see that the journal sources of the citing papers are more abundant, and the cited journals are relatively concentrated (Figure 5). EA and pain research presents a trend of interdisciplinary research, and EA is increasingly widely used clinically.
In future research, it is imperative that we enhance interdisciplinary collaboration to modernize acupuncture. We must place equal emphasis on both the quantity and quality of research results while striving for publication in high-level journals.
Status of Cooperation
China, the United States, and South Korea are recognized as highly influential and possess extensive collaborative relationships with other nations. Capital Medical University, Peking University, and Kyung Hee University are the most influential institutions. Kyung Hee University also has the largest amount of literature, while Capital Medical University and Peking University have temporarily fallen behind in this regard. However, through their collaborative efforts with other academic institutions, it is anticipated that both the quantity and quality of their literature will improve in the future.
As the discipline has evolved, several core author teams have gradually formed. From diverse perspectives, the mechanisms of EA analgesia were investigated by various research teams. The investigation was conducted by Lao Lixing’s team and emphasized neuro-immuno-endocrine interactions, whereas Liang FanRong’s team used fMRI to observe how EA modulates brain networks.24,37–40 Han Jisheng’s team focused on frequency-dependent mechanisms, and Wu Gencheng delved into orphan fibropeptides.41,42 Furthermore, researchers have probed various chronic pain types; for example, Liang focused on osteoarthritis in the knee, neck pain, primary dysmenorrhea, and migraine. Fang Jianqiao’s team examined complex regional pain syndrome, diabetic neuropathic pain and trigeminal neuralgia, whereas Hsieh Ching-Liang’s team concentrated on fibromyalgia. The function of EA within the emotional dimension of pain and its utility for mitigating lower abdominal pain and chronic pain induced anxiety and depression were also scrutinized.9 Additionally, studies were conducted on chemotherapy-induced side effects in cancer patients and irritable bowel syndrome. The research conducted in this domain has substantially augmented our comprehension of EA and its prospective benefits for pain management.
The meso-institutional cooperation network and micro-author cooperation network indicate insufficient cooperation due to low density. Moreover, domestic cooperation frequently occurred, while international cooperation was lacking and needed to be strengthened. In particularly, collaboration should be strengthened between China, the United States, and South Korea.
Research Hotspots of EA for Pain
We investigated hotspots of EA for pain from three prospectives, namely, co-cited authors, keywords, and cited references.43
In terms of co-cited authors, Han Jisheng and Zhang Ruixing belonged to the core author teams mentioned above. Zhao Zhiqi mainly focused on the cellular and molecular mechanisms of nociception modulation by EA.44 Vickers Andrew J focused on clinical decision models and chronic pain.45–47 Similarly, Lin JaungGeng focused on the clinical application and mechanism of EA in patients with perioperative pain and cancer pain.48,49 From this, it can be seen that mechanisms and clinical application are the focus of research.
Keyword co-occurrence analysis showed that the top ten recurring keywords (Table 8) were related to the mechanisms of acupuncture analgesia. Depending on the underlying cause, pain is classified into two types: inflammation due to tissue damage and neuropathy due to nerve damage. The mechanisms of pain can be further divided into three levels: peripheral, spinal and supraspinal. In terms of inflammatory pain, in the periphery, EA promotes the release of opioids from peripheral inflammatory cells and reduces the expression of proinflammatory factors in local areas of inflammation.50–52 At the spinal level, EA inhibits the transmission of noxious stimuli through the involvement of spinal opioids, 5-HT, norepinephrine, glutamate, spinal glial cells, cytokines and signalling molecules.53–55 However, it should be emphasized that these pathways do not act individually and their combined efficacy in pain management is not fully understood. In neuropathic pain, the mechanisms have been studied more intensively in the spine, and opioids, serotonin, norepinephrine, excitatory amino acids, inhibitory amino acids, and glial cell/cytokines all play key roles.56
Our clustering analysis of keywords revealed four focus areas of EA for pain. In addition to the molecular biological mechanisms mentioned earlier, clinical randomized controlled trials are also hot topics in EA for pain. Furthermore, The multimodal analgesia approach has propelled EA’s role as a perioperative adjunct. Preoperative EA at Zusanli (ST36) prior to anesthesia has reduced morphine use by 61%, delaying postoperative pain onset by 18 minutes.11 Post anesthesia EA has significantly lowered analgesic doses and postoperative pain in knee joint replacement and radical prostatectomy.57,58 The application of EA in post cardiac surgery pain management is also effective.59 Owing to its proven efficacy with minimal side effects, the integration of EA has been proposed by researchers as an adjunct modality for analgesia in obstetric and pediatric populations, with the aim of minimizing analgesic drug administration.60,61 A meta-analysis has shown a role for EA in postoperative pain management and better results with bilateral EA.48,62 However, some are hesitant to endorse EA as an adjunct for analgesia due to concerns about its efficacy being contingent on surgical type and the perceived lower quality of evidence.63,64 As far as disease types are concerned, the most studied are mainly chronic pain, including low back pain, knee osteoarthritis, migraine, shoulder pain, fibromyalgia, and dysmenorrhea. EA is endorsed as an adjuvant therapy for chronic pain and nonspecific low back pain in the United Kingdom and the United States, respectively.65–67 It is noted that EA offers significant benefits in pain reduction and improvement in quality of life without any associated harm. It is important to highlight that acupuncture is currently not recommended in NICE’s 2022 guidelines for the management of osteoarthritis, low back pain, and migraine. However, this recommendation is not due to its lack of effectiveness, but primarily because of the limited availability of high-quality literature. The guidelines explicitly state that experts consider the use of EA and recommend further research to identify the characteristics of patients with osteoarthritis who would benefit from EA. At the same time, EA has shown marked effectiveness in managing acute pain. Meta-analyses suggest that EA yields more pronounced alleviation of acute lumbar pain when contrasted with medication and basic manual acupuncture.12 Furthermore, EA therapy for acute herpes zoster-associated pain also surpasses conventional approaches such as oral antiviral medications.68
The top five most co-cited references indicated that EA is more effective than manual acupuncture and suggested combining EA with low-dose traditional analgesic medication to reduce drug side effects.9,56 Endogenous opioid peptides play a crucial role in mediating the analgesic effects of EA in the central nervous system and have frequency-dependent properties.10,69,70
Therefore, according to the findings of this study, EA is mainly used to treat pain during the perioperative period and chronic pain, especially musculoskeletal pain.47 The analgesic effect of EA is essentially a manifestation of the integration process of impulse inputs from the pain area and acupuncture points at different levels of the central nervous system.69 However, this is a complex process and different signalling pathways can influence each other. Among these pathways, the role of endogenous opioids is crucial.
Global Trends in EA and Pain Research
The global trend in EA and pain research was investigated from the burst analysis of keywords, turning point papers and clusters of references.
Burst means that certain keywords are heavily cited in a short period, indicating that these topics have received more attention. In Table 10, the top five keywords in terms of strength among the ten latest keywords are point, human brain, knee osteoarthritis, systematic review, and depression. Similarly, according to the clustering of references, the two latest clusters were #5 (“systematic review”; 81; S =0.799; 2010) and #6(“knee osteoarthritis”; 69; S =0.847; 2010).
The top five turning point papers were all focused on the theme of clinical efficacy, with two reviews, one a meta-analysis, and two clinical trials.11,31–34 Knee osteoarthritis is just one type of chronic pain, but it has received more attention due to negative results published in JAMA.71 There is increasing discussion about the efficacy of acupuncture for pain, leading to an increase in both clinical trials and systematic reviews.
With the development of neuroimaging technology, fMRI is widely used to study the mechanism of acupuncture. In the context of EA treatment for acute pain, its primary effect involves the inhibition of activity in central pain perception and processing-related regions. Optimal intensity yields superior outcomes compared to minimal intensity.72 Similarly, different frequencies mediate distinct analgesic mechanisms. At 2 Hz, stimulation activates the primary motor and supplementary motor areas, along with the temporal gyrus, while inhibiting both hippocampi. At 100 Hz, stimulation activates the inferior parietal lobule, anterior cingulate cortex, hypothalamus, and pons, while inhibiting the contralateral amygdala. EA’s impact on neuropathic pain has been extensively researched.73 In animal experiments, models of brachial plexus and sciatic nerve injuries have consistently demonstrated definitive therapeutic effects after three months of EA treatment. fMRI findings indicate that compared to sham acupuncture, EA effects manifest as synchronized activation patterns in regions tied to somatosensory perception and pain, alongside fluctuations in the limbic/paralimbic system.74 The effect of EA is linked to the reversal of maladaptive plasticity associated with neuropathic pain.75 EA stimulation prompts spontaneous activity coupling in brain areas involved in pain perception modulation.76 The specific activation of the medial prefrontal cortex implies that EA’s analgesic action may encompass emotional regulation. Changes in the insula and thalamus may also play a pivotal role.77,78 In the treatment of migraines using EA, changes in the insula and thalamus are also pivotal.79 Clinical trials suggest that EA’s mechanism for carpal tunnel syndrome potentially involves reshaping the white matter microstructure in the primary somatosensory cortex, concurrently enhancing functional connectivity between the primary somatosensory area and regions associated with emotional processing.80,81 For chronic pain conditions such as fibromyalgia, EA can regulate primary somatosensory function linked with insular neurochemistry, thereby alleviating pain severity.82 In summary, the limbic system may be the key area where acupuncture works.83 fMRI is also often used for acupoint-specific studies, such as KI 3, LI 4, and KI 4.84–86 Compared to sham acupuncture, genuine acupuncture can cause different responses of mu-opioid receptors and significantly reduce periaqueductal grey matter activity.76,87 In addition, the mechanisms of different treatment paradigms have been explored, such as the combination of Ting Points and Gathering Points, EA versus acupressure, and contralateral and ipsilateral selection of points at the affected site.88–90 Notably, it has been suggested that manual acupuncture should be studied separately from EA, which produces a more extensive increase in signal than manual acupuncture, especially in the anterior middle cingulate layer.83,91
In addition to attention to pain symptoms, negative emotions such as anxiety or depression due to pain also received attention.92,93 The dopamine system, amygdala and anterior cingulate gyrus are involved in the regulation of negative emotions associated with pain.94
In summary, the trend of EA for pain focuses on the brain response to EA, especially in patients with chronic pain. When evaluating the efficacy, both pain relief and emotional improvement of the patient were considered. Meanwhile, in the clinical application and efficacy evaluation of EA, emphasis has increasingly been placed on quality, in addition to the continuously increasing quantity.
Future Outlook
It is important to pay more attention to the design of clinical trials on EA than before, distinguishing between EA and manual acupuncture, exploring appropriate EA parameters to improve clinical efficacy, and standardizing EA patterns to reduce variability and increase reproducibility.91,95 A greater proportion of patients suffering from chronic pain were female but the models were mostly male rats, which may overlook the crucial influence of gender on the therapeutic effect of pain.96–98 Future researchers should improve the quality and completeness of data reporting to publish more high-quality and influential papers.
Limitations
There are still some limitations in this study that need to be addressed. First, due to the limitations of the data format, we only analyze English articles from the Web of Science database, which might lead to language and publication bias. Second, our co-citation network is only based on first authors, which does not adequately reflect the authors’ influence; however, we also considered the impact of the author’s team in our subsequent analysis. Third, because there may be a delay in new articles being cited after publication, this may lead to an underestimation of the impact of the article, but the way we assess impact is not just in the number of citations but is also reflected in the names of the clusters.
Conclusion
The present results have provided the basis and reference for research topic selection. Chronic pain and related negative emotions, as well as perioperative pain, have become key points of clinical research. In particular, the mechanisms underlying the brain’s response to EA represent a key focus for ongoing inquiry. In addition, China, the United States, and South Korea should take a leading role in enhancing international cooperation. This may involve efforts to enhance the quality and rigor of experiments, to adhere to widely accepted consensus guidelines and to publish findings in high-impact journals to foster broader dissemination of results.
Funding
This work was supported by Shenzhen’s Sanming Project (SZSM201612001).
Disclosure
The authors declare no conflicts of interest in this study.
References
1. Raja SN, Carr DB, Cohen M, et al. The revised International Association for the Study of Pain definition of pain: concepts, challenges, and compromises. Pain. 2020;161(9):1976–1982. doi:10.1097/j.pain.0000000000001939
2. Orr PM, Shank BC, Black AC. The role of pain classification systems in pain management. Crit Care Nurs Clin North Am. 2017;29(4):407–418. doi:10.1016/j.cnc.2017.08.002
3. Schwenk ES, Viscusi ER, Buvanendran A, et al. Consensus guidelines on the use of intravenous ketamine infusions for acute pain management from the American Society of Regional Anesthesia and Pain Medicine, the American Academy of Pain Medicine, and the American Society of Anesthesiologists. Reg Anesth Pain Med. 2018;43(5):456–466. doi:10.1097/AAP.0000000000000806
4. Steglitz J, Buscemi J, Ferguson MJ. The future of pain research, education, and treatment: a summary of the IOM report “Relieving pain in America: a blueprint for transforming prevention, care, education, and research”. Transl Behav Med. 2012;2(1):6–8. doi:10.1007/s13142-012-0110-2
5. Cohen SP, Vase L, Hooten WM. Chronic pain: an update on burden, best practices, and new advances. Lancet. 2021;397(10289):2082–2097. doi:10.1016/S0140-6736(21)00393-7
6. Mao JJ, Liou KT, Baser RE, et al. Effectiveness of electroacupuncture or auricular acupuncture vs usual care for chronic musculoskeletal pain among cancer survivors: the PEACE randomized clinical trial. JAMA Oncol. 2021;7(5):720–727. doi:10.1001/jamaoncol.2021.0310
7. Onuora S. Intensive electroacupuncture reduces OA pain. Nat Rev Rheumatol. 2021;17(1):2.
8. Seo SY, Lee K-B, Shin J-S, et al. Effectiveness of acupuncture and electroacupuncture for chronic neck pain: a systematic review and meta-analysis. Am J Chin Med. 2017;45(8):1573–1595. doi:10.1142/S0192415X17500859
9. Ulett GA, Han S, J-s H. Electroacupuncture: mechanisms and clinical application. Biol Psychiatry. 1998;44(2):129–138. doi:10.1016/S0006-3223(97)00394-6
10. Han J-S. Acupuncture and endorphins. Neurosci Lett. 2004;361(1–3):258–261. doi:10.1016/j.neulet.2003.12.019
11. Lin J-G, M-W L, Wen Y-R, Hsieh C-L, Tsai S-K, Sun W-Z. The effect of high and low frequency electroacupuncture in pain after lower abdominal surgery. Pain. 2002;99(3):509–514. doi:10.1016/S0304-3959(02)00261-0
12. Wu B, Yang L, Fu C, et al. Efficacy and safety of acupuncture in treating acute low back pain: a systematic review and Bayesian network meta-analysis. Ann Palliat Med. 2021;10(6):6156–6167. doi:10.21037/apm-21-551
13. Kong J, Gollub RL, Webb JM, Kong J-T, Vangel MG, Kwong K. Test-retest study of fMRI signal change evoked by electro-acupuncture stimulation. NeuroImage. 2007;34(3):1171–1181. doi:10.1016/j.neuroimage.2006.10.019
14. Liang Y-D, Li Y, Zhao J, Wang X-Y, Zhu H-Z, Chen X-H. Study of acupuncture for low back pain in recent 20 years: a bibliometric analysis via CiteSpace. J Pain Res. 2017;10:951–964. doi:10.2147/JPR.S132808
15. He K, Zhan M, Li X, Wu L, Liang K, Ma R. A bibliometric of trends on acupuncture research about migraine: quantitative and qualitative analyses. J Pain Res. 2022;15:1257–1269. doi:10.2147/JPR.S361652
16. Huang L, Xu G, Sun M, et al. Recent trends in acupuncture for chronic pain: a bibliometric analysis and review of the literature. Complement Ther Med. 2023;72:102915. doi:10.1016/j.ctim.2023.102915
17. Ugolini D, Puntoni R, Perera FP, Schulte PA, Bonassi S. A bibliometric analysis of scientific production in cancer molecular epidemiology. Carcinogenesis. 2007;28(8):1774–1779. doi:10.1093/carcin/bgm129
18. van Eck NJ, Waltman L. Software survey: VOSviewer, a computer program for bibliometric mapping. Scientometrics. 2010;84(2):523–538. doi:10.1007/s11192-009-0146-3
19. Chen C. Searching for intellectual turning points: progressive knowledge domain visualization. Proc Natl Acad Sci U S A. 2004;1(Suppl 1):5303–5310. doi:10.1073/pnas.0307513100
20. Mao N, Wang M-H, Ho Y-S. A bibliometric study of the trend in articles related to risk assessment published in Science Citation Index. Hum Ecological Risk Assessment. 2010;16(4):801–824. doi:10.1080/10807039.2010.501248
21. Chen C. CiteSpace II: detecting and visualizing emerging trends and transient patterns in scientific literature. J Am Soc Inform Sci Technol. 2006;57(3):359–377. doi:10.1002/asi.20317
22. Aria M, Cuccurullo C. bibliometrix: an R-tool for comprehensive science mapping analysis. J Informetr. 2017;11(4):959–975. doi:10.1016/j.joi.2017.08.007
23. Ioannidis JPA, Baas J, Klavans R, Boyack KW. A standardized citation metrics author database annotated for scientific field. PLoS Biol. 2019;17(8):e3000384. doi:10.1371/journal.pbio.3000384
24. Li Y, Yang M, Wu F, et al. Mechanism of electroacupuncture on inflammatory pain: neural-immune-endocrine interactions. J Trad Chin Med. 2019;39(5):740–749.
25. Fei Y-T, Cao H-J, Xia R-Y, et al. Methodological challenges in design and conduct of randomised controlled trials in acupuncture. BMJ. 2022;376:e064345. doi:10.1136/bmj-2021-064345
26. Zhang Y-Q, Jiao R-M, Witt CM, et al. How to design high quality acupuncture trials-a consensus informed by evidence. BMJ. 2022;376:e067476. doi:10.1136/bmj-2021-067476
27. Chen C, Leydesdorff L. Patterns of connections and movements in dual-map overlays: a new method of publication portfolio analysis. J Assoc Inform Sci Technol. 2014;65(2):334–351. doi:10.1002/asi.22968
28. Small H. Co-citation in the scientific literature: a new measure of the relationship between two documents. J Am Soc Inf Sci. 1973;24(4):265–269. doi:10.1002/asi.4630240406
29. Leydesdorff L, Comins JA, Sorensen AA, Bornmann L, Hellsten I. Cited references and Medical Subject Headings (MeSH) as two different knowledge representations: clustering and mappings at the paper level. Scientometrics. 2016;109(3):2077–2091. doi:10.1007/s11192-016-2119-7
30. Chen C. A glimpse of the first eight months of the COVID-19 literature on Microsoft academic graph: themes, citation contexts, and uncertainties. Front Res Metr Anal. 2020;5:607286. doi:10.3389/frma.2020.607286
31. Alfhaily F, Ewies Aa A. Acupuncture in managing menopausal symptoms: hope or mirage? Climacteric. 2007;10(5):371–380. doi:10.1080/13697130701612315
32. Lewis K, Abdi S. Acupuncture for lower back pain: a review. Clin J Pain. 2010;26(1):60–69. doi:10.1097/AJP.0b013e3181bad71e
33. Linde K, Niemann K, Meissner K. Are sham acupuncture interventions more effective than (other) placebos? A re-analysis of data from the Cochrane review on placebo effects. Forsch Komplementarmed. 2010;17(5):259–264. doi:10.1159/000320374
34. Koo ST, Park YI, Lim KS, Chung K, Chung JM. Acupuncture analgesia in a new rat model of ankle sprain pain. Pain. 2002;99(3):423–431. doi:10.1016/S0304-3959(02)00164-1
35. Cobo MJ, López-Herrera AG, Herrera-Viedma E, Herrera F. An approach for detecting, quantifying, and visualizing the evolution of a research field: a practical application to the Fuzzy Sets Theory field. J Informetr. 2011;5(1):146–166. doi:10.1016/j.joi.2010.10.002
36. Yu D, Xu Z, Pedrycz W. Bibliometric analysis of rough sets research. Appl Soft Comput. 2020;94:106467. doi:10.1016/j.asoc.2020.106467
37. Niu X, Zhang M, Liu Z, et al. Interaction of acupuncture treatment and manipulation laterality modulated by the default mode network. Mol Pain. 2017;13:1744806916683684. doi:10.1177/1744806916683684
38. Liu P, Qin W, Zhang Y, et al. Combining spatial and temporal information to explore function-guide action of acupuncture using fMRI. J Magn Reson Imaging. 2009;30(1):41–46. doi:10.1002/jmri.21805
39. Zhang Y, Liang J, Qin W, et al. Comparison of visual cortical activations induced by electro-acupuncture at vision and nonvision-related acupoints. Neurosci Lett. 2009;458(1):6–10. doi:10.1016/j.neulet.2009.04.027
40. Jiang Y, Wang H, Liu Z, et al. Manipulation of and sustained effects on the human brain induced by different modalities of acupuncture: an fMRI study. PLoS One. 2013;8(6):e66815. doi:10.1371/journal.pone.0066815
41. Ma F, Xie H, Dong Z-Q, Wang Y-Q, Wu G-C. Effects of electroacupuncture on orphanin FQ immunoreactivity and preproorphanin FQ mRNA in nucleus of raphe magnus in the neuropathic pain rats. Brain Res Bull. 2004;63(6):509–513. doi:10.1016/j.brainresbull.2004.04.011
42. Fu X, Wang Y-Q, Wu G-C. Involvement of nociceptin/orphanin FQ and its receptor in electroacupuncture-produced anti-hyperalgesia in rats with peripheral inflammation. Brain Res. 2006;1078(1):212–218. doi:10.1016/j.brainres.2006.01.026
43. Zhou H, Tan W, Qiu Z, Song Y, Gao S. A bibliometric analysis in gene research of myocardial infarction from 2001 to 2015. PeerJ. 2018;6:e4354. doi:10.7717/peerj.4354
44. Dai W-J, Sun J-L, Li C, et al. Involvement of Interleukin-10 in analgesia of electroacupuncture on incision pain. Evid Based Complement Alternat Med. 2019;2019:8413576. doi:10.1155/2019/8413576
45. Vickers AJ, van Calster B, Steyerberg EW. A simple, step-by-step guide to interpreting decision curve analysis. Diagnos Prognos Res. 2019;3:18. doi:10.1186/s41512-019-0064-7
46. Vickers AJ, Cronin AM, Maschino AC, et al. Acupuncture for chronic pain: individual patient data meta-analysis. Arch Intern Med. 2012;172(19):1444. doi:10.1001/archinternmed.2012.3654
47. Vickers AJ, Vertosick EA, Lewith G, et al. Acupuncture for chronic pain: update of an individual patient data meta-analysis. J Pain. 2018;19(5):455–474. doi:10.1016/j.jpain.2017.11.005
48. M-S W, Chen K-H, Chen IF, et al. The efficacy of acupuncture in post-operative pain management: a systematic review and meta-analysis. PLoS One. 2016;11(3):e0150367. doi:10.1371/journal.pone.0150367
49. Lin J-G, Chen Y-H. The role of acupuncture in cancer supportive care. Am J Chin Med. 2012;40(2):219–229. doi:10.1142/S0192415X12500176
50. Li A, Zhang R-X, Wang Y, et al. Corticosterone mediates electroacupuncture-produced anti-edema in a rat model of inflammation. BMC Complement Altern Med. 2007;7(1):27. doi:10.1186/1472-6882-7-27
51. J-g S, H-h L, Y-f C, et al. Electroacupuncture improves survival in rats with lethal endotoxemia via the autonomic nervous system. Anesthesiology. 2012;116(2):406–414. doi:10.1097/ALN.0b013e3182426ebd
52. Su TF, Zhao YQ, Zhang LH, et al. Electroacupuncture reduces the expression of proinflammatory cytokines in inflamed skin tissues through activation of cannabinoid CB2 receptors. Eur J Pain. 2012;16(5):624–635. doi:10.1002/j.1532-2149.2011.00055.x
53. Kim HY, Wang J, Lee I, Kim HK, Chung K, Chung JM. Electroacupuncture suppresses capsaicin-induced secondary hyperalgesia through an endogenous spinal opioid mechanism. Pain. 2009;145(3):332–340. doi:10.1016/j.pain.2009.06.035
54. Silva JRT, Silva ML, Prado WA. Analgesia induced by 2- or 100-Hz electroacupuncture in the rat tail-flick test depends on the activation of different descending pain inhibitory mechanisms. J Pain. 2011;12(1):51–60. doi:10.1016/j.jpain.2010.04.008
55. Shan S, Qi-Liang MY, Hong C, et al. Is functional state of spinal microglia involved in the anti-allodynic and anti-hyperalgesic effects of electroacupuncture in rat model of monoarthritis? Neurobiol Dis. 2007;26(3):558–568. doi:10.1016/j.nbd.2007.02.007
56. Zhang R, Lao L, Ren K, Berman BM. Mechanisms of Acupuncture–Electroacupuncture on Persistent Pain. Anesthesiology. 2014;120(2):482–503. doi:10.1097/ALN.0000000000000101
57. Cheng SI, Kelleher DC, DeMeo D, Zhong H, Birch G, Ast MP. Intraoperative acupuncture as part of a multimodal analgesic regimen to reduce opioid usage after total knee arthroplasty: a prospective cohort trial. Med Acupunct. 2022;34(1):49–57. doi:10.1089/acu.2021.0072
58. Ntritsou V, Mavrommatis C, Kostoglou C, et al. Effect of perioperative electroacupuncture as an adjunctive therapy on postoperative analgesia with tramadol and ketamine in prostatectomy: a randomised sham-controlled single-blind trial. Acupunct Med. 2014;32(3):215–222. doi:10.1136/acupmed-2013-010498
59. Bigeleisen PE, Goehner N. Novel approaches in pain management in cardiac surgery. Curr Opin Anaesthesiol. 2015;28(1):89–94. doi:10.1097/ACO.0000000000000147
60. Yaster M. Multimodal analgesia in children. Eur J Anaesthesiol. 2010;27(10):851–857. doi:10.1097/EJA.0b013e328338c4af
61. Usichenko TI. Acupuncture as part of multimodal analgesia after caesarean section. Acupunct Med. 2014;32(3):297–298. doi:10.1136/acupmed-2014-010584
62. Cassu RN, Luna SPL, Clark RMO, Kronka SN. Electroacupuncture analgesia in dogs: is there a difference between uni- and bi-lateral stimulation? Vet Anaesth Analg. 2008;35(1):52–61. doi:10.1111/j.1467-2995.2007.00347.x
63. Mitra S, Carlyle D, Kodumudi G, Kodumudi V, Vadivelu N. New Advances in Acute Postoperative Pain Management. Curr Pain Headache Rep. 2018;22(5):35. doi:10.1007/s11916-018-0690-8
64. Shah S, Godhardt L, Spofford C. Acupuncture and postoperative pain reduction. Curr Pain Headache Rep. 2022;26(6):453–458. doi:10.1007/s11916-022-01048-4
65. American Society of Anesthesiologists Task Force on Chronic Pain M, American Society of Regional A, Pain M. Practice guidelines for chronic pain management: an updated report by the American Society of Anesthesiologists Task Force on Chronic Pain Management and the American Society of Regional Anesthesia and Pain Medicine. Anesthesiology. 2010;112(4):810–833. doi:10.1097/ALN.0b013e3181c43103
66. National Institute for Health and Care Excellence: Guidelines. Chronic Pain (Primary and Secondary) in Over 16s: Assessment of All Chronic Pain and Management of Chronic Primary Pain. London: National Institute for Health and Care Excellence (NICE) 2021; 2021.
67. NICE Evidence Reviews Collection. Evidence Review for the Clinical and Cost Effectiveness of Devices for the Management of Osteoarthritis: Osteoarthritis in Over 16s: Diagnosis and Management: Evidence Review H. London: National Institute for Health and Care Excellence (NICE) 2022; 2022.
68. He K, Ni F, Huang Y, et al. Efficacy and safety of electroacupuncture for pain control in Herpes Zoster: a systematic review and meta-analysis. Evid Based Complement Alternat Med. 2022;2022:4478444. doi:10.1155/2022/4478444
69. Zhao Z-Q. Neural mechanism underlying acupuncture analgesia. Prog Neurobiol. 2008;85(4):355–375. doi:10.1016/j.pneurobio.2008.05.004
70. Han JS. Acupuncture: neuropeptide release produced by electrical stimulation of different frequencies. Trends Neurosci. 2003;26(1):17–22. doi:10.1016/S0166-2236(02)00006-1
71. Hinman RS, McCrory P, Pirotta M, et al. Acupuncture for chronic knee pain: a randomized clinical trial. JAMA. 2014;312(13):1313–1322. doi:10.1001/jama.2014.12660
72. Shukla S, Torossian A, Duann JR, Leung A. The analgesic effect of electroacupuncture on acute thermal pain perception--a central neural correlate study with fMRI. Mol Pain. 2011;7:45. doi:10.1186/1744-8069-7-45
73. Zhang WT, Jin Z, Cui GH, et al. Relations between brain network activation and analgesic effect induced by low vs. high frequency electrical acupoint stimulation in different subjects: a functional magnetic resonance imaging study. Brain Res. 2003;982(2):168–178. doi:10.1016/S0006-8993(03)02983-4
74. Wu JJ, Lu YC, Hua XY, Ma SJ, Xu JG. A longitudinal mapping study on cortical plasticity of peripheral nerve injury treated by direct anastomosis and electroacupuncture in rats. World Neurosurg. 2018;114:e267–e282. doi:10.1016/j.wneu.2018.02.173
75. Wu JJ, Lu YC, Hua XY, Ma SJ, Shan CL, Xu JG. Cortical remodeling after electroacupuncture therapy in peripheral nerve repairing model. Brain Res. 2018;1690:61–73. doi:10.1016/j.brainres.2018.04.009
76. Zyloney CE, Jensen K, Polich G, et al. Imaging the functional connectivity of the Periaqueductal Gray during genuine and sham electroacupuncture treatment. Mol Pain. 2010;6:80. doi:10.1186/1744-8069-6-80
77. Chu WC, Wu JC, Yew DT, et al. Does acupuncture therapy alter activation of neural pathway for pain perception in irritable bowel syndrome? A comparative study of true and sham acupuncture using functional magnetic resonance imaging. J Neurogastroenterol Motil. 2012;18(3):305–316. doi:10.5056/jnm.2012.18.3.305
78. Wu J, Wang S, Lu Y, Zheng M, Hua X, Xu J. Shifted hub regions in the brain network of rat neuropathic pain model after electroacupuncture therapy. J Integr Neurosci. 2020;19(1):65–75.
79. Ishiyama S, Shibata Y, Ayuzawa S, Matsushita A, Matsumura A, Ishikawa E. The modifying of functional connectivity induced by peripheral nerve field stimulation using electroacupuncture for migraine: a prospective clinical study. Pain Med. 2022;23(9):1560–1569. doi:10.1093/pm/pnac048
80. Fisher H, Sclocco R, Maeda Y, et al. S1 brain connectivity in carpal tunnel syndrome underlies median nerve and functional improvement following electro-acupuncture. Front Neurol. 2021;12:754670. doi:10.3389/fneur.2021.754670
81. Maeda Y, Kim H, Kettner N, et al. Rewiring the primary somatosensory cortex in carpal tunnel syndrome with acupuncture. Brain. 2017;140(4):914–927. doi:10.1093/brain/awx015
82. Mawla I, Ichesco E, Zöllner HJ, et al. Greater somatosensory afference with acupuncture increases primary somatosensory connectivity and alleviates fibromyalgia pain via insular γ-aminobutyric acid: a randomized neuroimaging trial. Arthritis Rheumatol. 2021;73(7):1318–1328. doi:10.1002/art.41620
83. Napadow V, Makris N, Liu J, Kettner NW, Kwong KK, Hui KKS. Effects of electroacupuncture versus manual acupuncture on the human brain as measured by fMRI. Hum Brain Mapp. 2004;24(3):193–205. doi:10.1002/hbm.20081
84. Zhu B, Wang Y, Zhang G, et al. Acupuncture at KI3 in healthy volunteers induces specific cortical functional activity: an fMRI study. BMC Complement Altern Med. 2015;15(1):361. doi:10.1186/s12906-015-0881-3
85. Zhang Y, Glielmi CB, Jiang Y, et al. Simultaneous CBF and BOLD mapping of high frequency acupuncture induced brain activity. Neurosci Lett. 2012;530(1):12–17. doi:10.1016/j.neulet.2012.09.050
86. Zhang Q, Li A, Yue J, Zhang F, Sun Z, Li X. Using functional magnetic resonance imaging to explore the possible mechanism of the action of acupuncture at Dazhong (KI 4) on the functional cerebral regions of healthy volunteers. Intern Med J. 2015;45(6):669–671. doi:10.1111/imj.12767
87. Harris RE, Zubieta J-K, Scott DJ, Napadow V, Gracely RH, Clauw DJ. Traditional Chinese acupuncture and placebo (sham) acupuncture are differentiated by their effects on mu-opioid receptors (MORs). NeuroImage. 2009;47(3):1077–1085. doi:10.1016/j.neuroimage.2009.05.083
88. Leung A, Zhao Y, Shukla S. The effect of acupuncture needle combination on central pain processing--an fMRI study. Mol Pain. 2014;10:23. doi:10.1186/1744-8069-10-23
89. Witzel T, Napadow V, Kettner NW, Vangel MG, Hämäläinen MS, Dhond RP. Differences in cortical response to acupressure and electroacupuncture stimuli. BMC Neurosci. 2011;12(1):73. doi:10.1186/1471-2202-12-73
90. Yi M, Zhang H, Lao L, Xing -G-G, Wan Y. Anterior cingulate cortex is crucial for contra- but not ipsi-lateral electro-acupuncture in the formalin-induced inflammatory pain model of rats. Mol Pain. 2011;7:61. doi:10.1186/1744-8069-7-61
91. Langevin HM, Schnyer R, MacPherson H, et al. Manual and electrical needle stimulation in acupuncture research: pitfalls and challenges of heterogeneity. J Alternat Complement Med. 2015;21(3):113–128. doi:10.1089/acm.2014.0186
92. Du J, Fang J, Xu Z, et al. Electroacupuncture suppresses the pain and pain-related anxiety of chronic inflammation in rats by increasing the expression of the NPS/NPSR system in the ACC. Brain Res. 2020;1733:146719. doi:10.1016/j.brainres.2020.146719
93. Fangtham M, Kasturi S, Bannuru RR, Nash JL, Wang C. Non-pharmacologic therapies for systemic lupus erythematosus. Lupus. 2019;28(6):703–712. doi:10.1177/0961203319841435
94. Zhang X-H, Feng -C-C, Pei L-J, et al. Electroacupuncture attenuates neuropathic pain and comorbid negative behavior: the involvement of the dopamine system in the amygdala. Front Neurosci. 2021;15:657507. doi:10.3389/fnins.2021.657507
95. Ouyang H, Chen JDZ. Therapeutic roles of acupuncture in functional gastrointestinal disorders. Aliment Pharmacol Ther. 2004;20(8):831–841. doi:10.1111/j.1365-2036.2004.02196.x
96. Ning Z, Gu P, Zhang J, et al. Adiponectin regulates electroacupuncture-produced analgesic effects in association with a crosstalk between the peripheral circulation and the spinal cord. Brain Behav Immun. 2022;99:43–52. doi:10.1016/j.bbi.2021.09.010
97. Hashmi JA, Davis KD. Deconstructing sex differences in pain sensitivity. Pain. 2014;155(1):10–13. doi:10.1016/j.pain.2013.07.039
98. Fillingim RB, King CD, Ribeiro-Dasilva MC, Rahim-Williams B, Riley JL. Sex, gender, and pain: a review of recent clinical and experimental findings. J Pain. 2009;10(5):447–485. doi:10.1016/j.jpain.2008.12.001
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Knowledge Atlas of the Co-Occurrence of Epilepsy and Autism: A Bibliometric Analysis and Visualization Using VOSviewer and CiteSpace
Wang Y, Huo X, Li W, Xiao L, Li M, Wang C, Sun Y, Sun T
Neuropsychiatric Disease and Treatment 2022, 18:2107-2119
Published Date: 19 September 2022
Bibliometric Analysis of Research Themes and Trends of the Co-Occurrence of Autism and ADHD
Liu A, Lu Y, Gong C, Sun J, Wang B, Jiang Z
Neuropsychiatric Disease and Treatment 2023, 19:985-1002
Published Date: 24 April 2023
Bibliometric Analysis of Global Research on Transient Receptor Potential Vanilloid 1 in the Field of Pain
Wang S, Wang W, Ye X
Journal of Pain Research 2023, 16:1517-1532
Published Date: 9 May 2023
Studies on Pain Associated with Anxiety or Depression in the Last 10 Years: A Bibliometric Analysis
Zhang Q, Sun H, Xin Y, Li X, Shao X
Journal of Pain Research 2024, 17:133-149
Published Date: 5 January 2024
Global Research Status of Maca (Lepidium Meyenii Walp.): A Bibliometric Analysis of Hotspots, Bursts, and Trends
Li K, Zhao C, Dang M, Ren R, Fu M, Bai Y, Wang J, Zhang Q, Luan F
Drug Design, Development and Therapy 2025, 19:2329-2349
Published Date: 27 March 2025