Back to Journals » Clinical Interventions in Aging » Volume 20
eGFR–ACR Risk Stratification of Rapid Kidney Function Decline Across Aging Phenotypes in Older Chinese Adults
Authors Chang H ![]() , You H, Yao Y, Zheng Y, Mao J, Yao Y, Wang M, Wang X, Chen J
, You H, Yao Y, Zheng Y, Mao J, Yao Y, Wang M, Wang X, Chen J
Received 24 June 2025
Accepted for publication 14 November 2025
Published 20 November 2025 Volume 2025:20 Pages 2105—2118
DOI https://doi.org/10.2147/CIA.S549212
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Maddalena Illario
Huaiwen Chang,1 Huaizhou You,2,3 Ye Yao,4 Yan Zheng,3,5,6 JianPing Mao,2 Yin Yao,1 Mengjing Wang,2,3 Xiaofeng Wang,3,5 Jing Chen2,3
1Department of Computational Biology, School of Life Sciences, Fudan University, Shanghai, People’s Republic of China; 2Division of Nephrology, Huashan Hospital, Fudan University, Shanghai, People’s Republic of China; 3National Clinical Research Center for Aging and Medicine, Huashan Hospital, Fudan University, Shanghai, People’s Republic of China; 4Department of Biostatistics, School of Public Health, Fudan University, Shanghai, People’s Republic of China; 5State Key Laboratory of Genetic Engineering, Human Phenome Institute, School of Life Sciences, Fudan University, Shanghai, People’s Republic of China; 6Ministry of Education Key Laboratory of Public Health Safety, School of Public Health, Institute of Nutrition, Fudan University, Shanghai, People’s Republic of China
Correspondence: Jing Chen, Division of Nephrology, Huashan Hospital, Fudan University, 12 Middle Wulumuqi Road, Shanghai, 200040, People’s Republic of China, Tel +86-21-52889387, Fax +86-21-52888304, Email [email protected] Mengjing Wang, Division of Nephrology, Huashan Hospital, Fudan University, 12 Middle Wulumuqi Road, Shanghai, 200040, People’s Republic of China, Tel +86-21-52889387, Fax +86-21-52888304, Email [email protected]
Objective: To develop an estimated glomerular filtration rate (eGFR) and urine albumin–creatinine ratio (ACR) risk stratification for rapid kidney function decline across aging phenotypes in older adults.
Methods: We included 1539 older adults (486 healthy aging, 661 aging with comorbidities, 392 aging with CKD) from the Rugao Longevity and Aging Study and Huashan Hospital. Rapid decline was defined as a ≥ 30% decrease in eGFR over 2 years. We estimated adjusted incidence of rapid decline across baseline eGFR (≥ 90, 75–< 90, 60–< 75, < 60 mL/min/1.73 m2) and ACR (< 30 vs ≥ 30 mg/g) categories within each aging phenotype. We defined adjusted incidence rate of < 5%, 5– 7.5%, 7.5– 15%, and > 15% as no risk, low risk, moderate risk, and high risk, respectively. Random forests assessed the relative contribution of pre-specified eGFR and ACR categories.
Results: Mean ages were 77.7 ± 4.4, 78.0 ± 4.1, and 77.7 ± 5.5 years in healthy, comorbidity, and CKD cohort, respectively. Among healthy participants, the adjusted incidence remained in low risk when eGFR was between 60 and 75 mL/min/1.73 m2, but increased to moderate risk when eGFR < 60 mL/min/1.73 m2. In the comorbidity cohort, a low risk classification was observed with ACR < 30 mg/g and eGFR ≥ 75 mL/min/1.73 m2, or with ACR ≥ 30 mg/g and eGFR ≥ 90 mL/min/1.73 m2, other combinations were associated with moderate risk. In the CKD cohort, moderate risk corresponded to ACR < 30 mg/g with eGFR ≥ 60 mL/min/1.73 m2 or ACR ≥ 30 mg/g with eGFR ≥ 75 mL/min/1.73 m2, while all other scenarios were classified as high risk. Random forest results corroborated that eGFR dominated discrimination in healthy aging, whereas ACR carried greater weight in comorbidity and CKD cohorts.
Conclusion: Phenotype-specific eGFR-ACR thresholds provide pragmatic risk stratification to guide targeted monitoring and earlier intervention in older adults.
Keywords: kidney function decline, glomerular filtration rate, urine albumin–creatinine ratio, healthy aging, comorbidity, chronic kidney disease
Introduction
Declines in renal functioning are associated with adverse outcomes, including end-stage renal disease (ESRD), cardiovascular events, hospitalization, and all-cause mortality.1–3 Early identification of individuals at risk for rapid kidney function decline can facilitate targeted interventions. Older adults are particularly susceptible to this risk. Epidemiological data reveal a stark age-related gradient: while chronic kidney disease (CKD) affects nearly 33% of adults aged 65 and over, its prevalence in middle-aged populations remains substantially lower, often below 10%.4–6 This underscores the urgent need for the development of a risk assessment tool to identify elderly populations at high-risk of rapid kidney function decline.7–10 To this end, a decline in eGFR of ≥30% over two years has been widely validated as a clinically meaningful surrogate endpoint for ESRD and all-cause mortality, and thus serves as the definition of rapid decline in the present study.11–14
Aging is accompanied by a reduction in renal functional reserve, meaning the kidneys have a decreased capacity to augment the glomerular filtration rate (GFR) after physiological or pathological stimuli.15 This reserve acts as the kidney’s “stress-test” capacity, and its depletion often precedes a decline in baseline eGFR, serving as an early indicator of renal frailty and vulnerability. These changes are exacerbated by prevalent comorbidities and pre-existing renal disease. Conditions such as hypertension, diabetes, and hyperuricemia accelerate the loss of renal reserve through well-established mechanisms, including microvascular injury, endothelial dysfunction, and chronic inflammation, which collectively promote glomerulosclerosis and tubulointerstitial fibrosis. Concurrently, established CKD can directly lead to nephron destruction and fibrosis via immune-mediated or inflammatory pathways.16–21 Reduced renal functional reserve thus reflects renal frailty and increased vulnerability to injury, making it a critical stratification for assessing risk for functional decline in older populations.15,22,23
Previous studies have used estimated GFR (eGFR) and/or urine albumin-creatinine ratios (ACRs) to stratify the risk of renal failure or related adverse events. Existing prediction models were largely developed in middle-aged or mixed-age populations and apply a “one-size-fits-all” approach, which fails to account for the profound heterogeneity in renal reserve and vulnerability across different aging phenotypes.24–26
The present study aims to evaluate the role of eGFR and ACR in predicting rapid renal functional decline in older adults with differing aging trajectories—which reflect disparate renal functional reserve and vulnerabilities. The study cohorts include healthy aging (older adults without CKD or concordant comorbidities), aging with comorbidities (with diabetes, hypertension, stroke, gout, chronic heart failure, or atherosclerotic coronary artery disease, but without a diagnosis of CKD), and aging with CKD (older adults with diagnoses of CKD according to KDIGO guideline).27 The present study builds on previous work, including the use of the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formula, which has been shown to be the most reliable method for estimating eGFR in the elderly.28,29
Consistent with the KDIGO risk heat map—which cross-classifies eGFR and albuminuria to stage CKD risk—we position our phenotype-specific joint eGFR–ACR matrix, anchored to the ≥30% two-year eGFR decline endpoint.30 We aimed to define cohort-level eGFR and ACR thresholds based on different aging profiles to predict rapid kidney function decline in older adults. These tailored measures may enhance risk stratification and support timely, targeted interventions to prevent progression to ESRD and improve quality of life in the elderly.
Materials and Methods
Study Populations
We examined data from three distinct cohorts. A total of 1950 elderly participants from the Rugao Longevity and Aging Study (RLAS) composed the healthy and comorbidity cohorts (2017–12-31 to 2019–12-31), 3692 elderly patients with CKD from Huashan Hospital at Fudan University composed the CKD cohort (2006–12-25 to 2023–11-14). The RLAS is a longitudinal population-based study conducted in Rugao in the Jiangsu Province of China, and is designed to examine aging trajectories. This study enrolled individuals over 70 years old living in 31 villages in the Jiang’an township and has followed up with all participants every two years since 2014. Further details about the study design have been described elsewhere.31 Huashan Hospital is a general tertiary care hospital located in Shanghai, China, but 67% of the patients come from other areas in China. Electronic health records of patients over 70 years old who were treated at Huashan Hospital were used as the data source for the CKD cohort.
Based on the following criteria, we excluded 803 of the 1950 elderly participants in the RLAS cohort. A total of 600 individuals were lost to follow-up, 114 were diagnosed with CKD (and thus could not be part of the healthy aging or comorbidities cohorts), 25 were under 70 years of age, 35 had abnormal eGFR increases exceeding 20% over two years, and 28 had baseline ACR levels above 300 mg/g. After these exclusions, our final study population included 486 individuals in the healthy cohort and 661 in the comorbidity cohort. Cohort classification was based on the presence of documented comorbidities, which are detailed in the following sections.
The Huashan Hospital database included 3692 elderly patients who met the inclusion criteria (had at least two documented serum creatinine and cystatin C measurements, at least one documented ACR measurement, had an interval of at least two years between serum creatinine measurements, had their initial ACR measurement prior to their most recent serum creatinine measurement, and were aged ≥ 65 years). From this cohort, we excluded 2836 patients without serum creatinine, serum cystatin C, and ACR measurements taken within the same quarter, as well as those who did not have two-year follow-ups of serum creatinine and cystatin C levels. We also excluded 260 patients who did not have a diagnosis of CKD; 190 patients who were younger than 70 years old; and 14 patients with abnormally elevated eGFR values, as assessed by senior nephrologists. Thus, the final CKD cohort included 392 individuals.
This study was approved by the following institutional review boards: the Fudan University School of Life Sciences Human Ethics Committee (BE1815) and the Ethics Committee at Huashan Hospital, Fudan University (KY20241068). Ethical approval for the UK Biobank Study was granted by the National Information Governance Board for Health and Social Care and the NHS North West Multicenter Research Ethics Committee. All participants provided informed consent via electronic signatures at baseline.
Figure S1 describes the patient selection processes from the RLAS and the Huashan Hospital electronic medical records.
 |
Figure 1 Adjusted incidence rate of rapid kidney function decline by eGFR–ACR category in older cohorts. Blue circles/solid line denote the healthy aging cohort (slope = 0.64 percentage points per category; 95% CI 0.23–1.04). Orange squares/solid line denote the comorbidity cohort (slope = 0.65; 0.43–0.86). Red triangles/solid line denote the CKD cohort (slope = 1.27; 0.50–2.04). Rates are adjusted for age, hemoglobin, cholesterol, triglycerides, and cohort type. External validation of the ≥30% two-year endpoint in UK Biobank is summarized in the Results and detailed in Supplementary Method S1, Figure S2, and Supplementary Tables S1, S1b, and S2. |
Variable Measurement
Baseline serum creatinine, serum cystatin C, albumin, calcium, uric acid, triglycerides, low-density lipoprotein, cholesterol and hemoglobin values, demographic data including age and sex, and physical examination measures (eg, weight and systolic and diastolic blood pressures), were collected from each database. For the RLAS cohort and Huashan Hospital cohorts, biochemical measurements were collected using automated biochemistry analyzers (either the Olympus AU5811 Clinical Chemistry Analyzer or the Hitachi 7600–020 analyzer) in conjunction with standard biochemical laboratory tests conducted by experienced technicians at Jiangsu Rugao Hospital of Traditional Chinese Medicine or Huashan Hospital, respectively.
Medical diagnoses in the RLAS dataset were gathered based on medical insurance data from Rugao City and verified by at least two members of the research team. Medical diagnoses in the Huashan Hospital dataset were derived from ICD-10–codes. Participants were then stratified into three cohorts. The healthy cohort consisted of individuals who had neither concordant comorbidities nor clinical evidence of CKD. Comorbid populations were defined as individuals without CKD but with conditions that have been directly associated with pathological renal changes (eg, chronic inflammation and vascular injury) and can accelerate renal functional decline, including diabetes, hypertension, stroke, gout, chronic heart failure, and coronary atherosclerotic heart disease, collectively termed “concordant comorbidities”.32 The CKD cohort included participants with CKD and encompassed cases on the spectrum from acute kidney injury (AKI) to CKD. Causes of CKD in our cohort included primary nephritis, secondary nephropathy, hereditary nephropathy, and kidney tumors. Borderline cases, such as mildly reduced eGFR (eg, 60–75 mL/min/1.73 m2) but without any other abnormalities of kidney structure or function were assigned to the comorbidity cohort if any concordant comorbidity was present; otherwise, to the healthy cohort. This hierarchical classification enabled a comprehensive analysis of the clinical trajectories associated with renal function decline.
Each participant’s eGFR was computed using the CKD-EPI 2012 creatinine-cystatin C equation.28 Percentage change in eGFR was calculated as follows: (last estimated eGFR – first estimated eGFR)/(first estimated eGFR) × 100%. Rapid kidney function decline was defined as a ≥ 30% change in eGFR over a two-year period and served as a surrogate endpoint for ESRD and all-cause mortality.11–14 Additionally, we validated this surrogate endpoint for mortality in an independent UK Biobank subcohort (see Supplementary Method S1, Figure S2, Supplementary Tables S1, S1b, and S2). In multivariable Cox models, a ≥30% two-year eGFR decline was strongly associated with all-cause mortality (adjusted HR 6.37, 95% CI 2.33–17.38), and sensitivity thresholds showed consistent directionality (≥35%: HR 4.93, 95% CI 1.20–20.21; ≥50%: HR 8.26, 95% CI 1.14–59.71). A margin of 0.5 years was allowed before and after the baseline period to determine the most recent available eGFR for calculation.
Statistical Analysis
Continuous variables are expressed as means ± standard deviations, and categorical variables are presented as counts (percentages). Missing data were handled per protocol: complete-case analysis for the outcome and key stratifiers (baseline eGFR/ACR and the follow-up eGFR); for adjustment covariates with low missingness (<5%), single imputation using cohort-specific medians was applied. For exploratory pairwise comparisons, p-values were adjusted using the Benjamini–Hochberg false discovery rate at 5%.
Adjusted incidence rate of rapid kidney function decline served as the primary metric for quantifying risk across different eGFR and ACR categories. To obtain the adjusted incidence rate, we constructed a logistic regression adjustment model—detailed in Supplementary Method S2—to control for age, hemoglobin, cholesterol, triglycerides and aging classifications (Healthy, Comorbidity and CKD), variables have been strongly associated with dysfunction in renal reserve, and alter the relationships between baseline eGFR, ACR, and incidence rate of rapid kidney function decline.33–36 A summary table was also constructed to present adjusted incidence rate of rapid kidney function decline for various baseline eGFR and ACR combinations. Risk levels were categorized into four tiers: no risk (incidence rate <5%, green), low risk (incidence rate 5–7.5%, yellow), moderate risk (incidence rate 7.5–15%, orange), and high risk (incidence rate >15%, red). This stratification framework provides a clinically interpretable assessment of risk, enabling targeted interventions for populations at greatest risk.
Adjusted incidence rate trendlines for eGFR and ACR categories were calculated for the three study cohorts using least squares linear regression. Model fit was evaluated using various statistical parameters, including P-values, R2, and adjusted R2, to assess each models’ explanatory power and reliability.
To identify the most influential predictors of rapid kidney function decline, the relative importance of eGFR and ACR categories was evaluated with a Random Forest (RF) model. The RF algorithm calculates the mean decrease in impurity (MDI) to rank feature importance,37 and quantifies each variable’s contribution to the model’s predictive performance. This non-parametric method is particularly suited for clinical datasets with complex variable interactions and provides robust insights into the relative predictive values of various eGFR and ACR categories.
In parallel, we computed odds ratios (ORs) for each eGFR and ACR category to quantify their direct association with rapid kidney function decline. An OR > 1 indicates increased risk, while ORs < 1 indicate protective effects. The dual analysis framework, combining both RF and logistic regression, allowed for a comprehensive analysis of the predictive roles of eGFR and ACR categories across our three study cohorts.
Statistical significance was set at a two-tailed P < 0.01. For multivariable inference, model parsimony respected an events-per-variable (EPV) ≥10. All analyses were conducted using Python 3.9 and the Scikit-learn toolkit, with the exception of hypothesis testing (continuous variables: ANOVA, categorical variables: chi-square tests), which were completed in R (version 4.1.2).
Results
Baseline Characteristics
Table 1 presents the baseline participant characteristics in the three cohorts—the healthy aging cohort, the aging with comorbidities cohort, and aging with CKD cohort. The mean (SD) ages in these cohorts were 77.7 (4.4), 78.0 (4.1), 77.7 (5.5), respectively, and the percentages of male participants in each cohort were 54.7%, 42.7%, and 54.3%, respectively. Thus, the average age was similar across all three cohorts, but participants in the comorbidity cohort were more likely to be female than in the other cohorts. Diagnoses in the comorbidity cohort included diabetes (70 cases), hypertension (417 cases), stroke (66 cases), heart disease (55 cases), gout (113 cases), and heart failure (39 cases). In the CKD cohort, patients had to have been diagnosed with CKD as their primary medical condition including CKD stages 2 through 5. Sequentially higher baseline levels of serum creatinine (61.5 vs 64.9 vs 100.7 μmol/L), serum cystatin C (1.1 vs 1.1 vs 1.4 mg/L), ACR (6.0 vs 10.9 vs 62.8 mg/g), and unadjusted two-year eGFR decline percentages (30% vs 35% vs 50%) were observed across the healthy, comorbidities, and CKD cohorts, respectively, with statistically significant differences found between all three cohorts (P < 0.01). The eGFR distributions for different cohorts are presented in Figure S3.
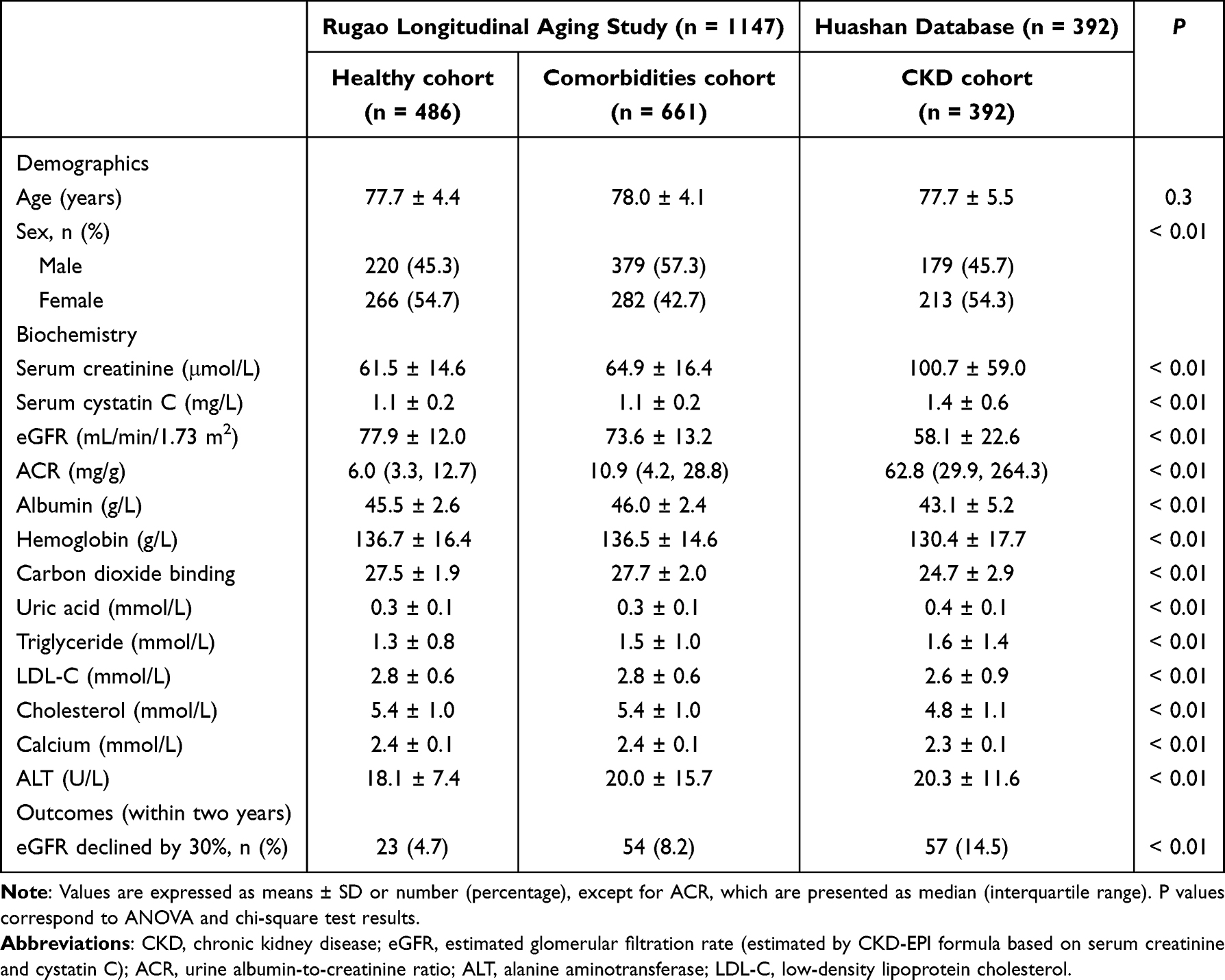 |
Table 1 Baseline Demographic and Clinical Characteristics of Participants in the Three Elderly Populations |
Risk Assessment of Rapid Kidney Function Decline in Three Elderly Aging Cohorts
We conducted an early-warning analysis of rapid kidney function decline (≥ 30% eGFR reduction over two years) across three distinct elderly cohorts: Healthy, Comorbidity, and CKD. External validation in the UK Biobank further supported the face validity of this surrogate endpoint: a ≥30% two-year eGFR decline was associated with higher all-cause mortality (adjusted HR 6.37, 95% CI 2.33–17.38), with a similar pattern for ≥35% and ≥50% thresholds (Supplementary Method S1 and Supplementary Table S2). Table 2 summarizes the adjusted incidence rate for each baseline combination of eGFR (≥ 90, 75–90, 60–75, < 60 mL/min/1.73 m2) and ACR (< 30 vs ≥ 30 mg/g).
 |
Table 2 Adjusted Incidence Rate Based on Baseline eGFR and ACR Categories for Three Elderly Populations |
Across all cohorts, adjusted incidence rate rose as eGFR declined and as ACR increased. However, the slope of the increase in incidence rate differed by cohort (Figure 1 and Table 3). In the Healthy aging cohort, the slope of the linear fit was 0.64 percentage points per eGFR and ACR category (95% CI 0.23–1.04; P = 0.054; R2 = 0.895, adjusted R2 = 0.843), indicating a relatively gradual increase in adjusted incidence rate as one moves through worsening eGFR/ACR levels. In the Aging with comorbidities cohort, the slope was 0.65 (95% CI 0.43–0.86; P < 0.001; R2 = 0.970, adjusted R2 = 0.965), reflecting a steeper rise in rate. The steepest increase occurred in the CKD cohort, with a slope of 1.27 (95% CI 0.50–2.04; P = 0.003; R2 = 0.858, adjusted R2 = 0.830). In every cohort, combinations with ACR ≥ 30 mg/g carried higher adjusted incidence rate than their counterpart categories with ACR < 30 mg/g, regardless of eGFR.
 |
Table 3 Linear Fit Coefficients and Model Performance for Adjusted Incidence Rate by eGFR/ACR Category in Elderly Cohorts |
Evaluation metrics were used to describe the adjusted incidence rate and corresponding risk across diverse combinations of eGFR and ACR for all three cohorts (Figure 2). In the healthy cohort (all ACR < 30 mg/g), risk remained in the no‐risk tier (< 5%) at eGFR ≥ 75 mL/min/1.73 m2, rose to low risk (5–7.5%) at 60–75 mL/min/1.73 m2, and to moderate risk (7.5–15%) at eGFR < 60 mL/min/1.73 m2. In the comorbidity cohort, only those with ACR < 30 mg/g and eGFR ≥ 75 mL/min/1.73 m2 or with ACR ≥ 30 mg/g and eGFR ≥ 90 mL/min/1.73 m2 had low risk; all other combinations fell into the moderate‐risk tier. In the CKD cohort, ACR < 30 mg/g with eGFR ≥ 60 mL/min/1.73 m2 or ACR ≥ 30 mg/g with eGFR ≥ 75 mL/min/1.73 m2 had moderate risk, while every other combination fell into the high-risk tier (> 15%). These findings demonstrate that the precise eGFR/ACR thresholds warranting intervention differ substantially by underlying health status. Complementary univariate analyses demonstrated monotonic, phenotype-dependent risk gradients when stratifying by eGFR alone (Figure S4) or ACR alone (Figure S5), reinforcing the joint eGFR–ACR matrix.
 |
Figure 2 Adjusted incidence rate of rapid kidney function decline by eGFR and ACR categories in older cohorts. Color scale: green <5% (no risk); yellow 5–7.5% (low); Orange 7.5–15% (moderate); red >15% (high). Rates are derived from logistic models adjusted for age, hemoglobin, cholesterol, triglycerides, and phenotype. eGFR was estimated using the CKD-EPI creatinine–cystatin C equation; ACR denotes urine albumin–creatinine ratio. Blank cells indicate n < 10 in the corresponding eGFR-by-ACR stratum. |
Understanding the Relative Importance of eGFR and ACR Categories for Predicting Rapid Kidney Function Decline
Previous analyses have demonstrated the utility of the combination of eGFR and ACR for risk stratification. However, further investigation is needed to determine the specific contributions of these markers within healthy aging, comorbidities, and CKD populations. Here, we sought to understand population-specific priorities for risk prediction by quantifying the relative predictive strength of eGFR and ACR and evaluating the associated odds ratios for rapid kidney function decline.
A notable shift in the relative contribution of eGFR and ACR to risk prediction was observed across the cohorts (Figure 3, Supplementary Tables S3 and S4). In healthy older adults, eGFR < 60 mL/min/1.73 m2 emerged as the strongest predictor of rapid kidney function decline (OR 6.15; P < 0.01). Among individuals with comorbidities, ACR demonstrated greater predictive value than partial eGFR categories—albuminuria (ACR ≥30 mg/g) conferred higher risk, while ACR <30 mg/g was protective (OR 0.40; P<0.01). In the CKD cohort, the predictive value of ACR was even more prominent, with both ACR ≥ 30 mg/g and ACR < 30 mg/g ranking as the second and third most influential predictors, respectively. Despite these variations, eGFR < 60 mL/min/1.73 m2 remained the most significant predictor of rapid decline across all three cohorts. It should be noted that the marginal ORs for the same eGFR/ACR classification vary across different phenotypes, as they are influenced by phenotype-specific baseline risks and differences in the distribution and co-occurrence of eGFR and proteinuria.
 |
Figure 3 Random Forest feature importance for eGFR and ACR categories predicting rapid kidney function decline. Random forest feature importance (mean decrease in Gini) for predicting ≥30% eGFR decline within 2 years across the three cohorts. Very low importance for certain eGFR/ACR categories reflects cohort-specific distributions (eg, near-constant or low-variance categories), overlap with related features, and weaker separability. Feature importance reflects predictive contribution, not causal effect. |
Discussion
Here, we used a categorical analysis of several different cohorts of aging individuals (all 70+, and including a healthy cohort, a comorbidity cohort, and a CKD cohort) to establish cohort-leveled eGFR and ACR thresholds for early warning of rapid kidney function decline. In healthy older adults, risk remains <5% when eGFR ≥75 mL/min/1.73 m2; values of 60–75 indicate a low-risk early-warning state that merits routine surveillance, whereas eGFR <60 denotes moderate risk and closer follow-up. In older adults with concordant comorbidities, low risk is confined to ACR <30 with eGFR ≥75 or ACR ≥30 with eGFR ≥90; all other combinations are moderate risk, supporting tighter risk-factor management and earlier review. In CKD, ACR <30 with eGFR ≥60 or ACR ≥30 with eGFR ≥75 corresponds to moderate risk, while all remaining cells are high risk (>15%), justifying intensified follow-up and timely nephrology referral. Applied upstream of KDIGO, our phenotype-aware eGFR–ACR matrix operationalizes heterogeneity in renal functional reserve and—consistent with the KDIGO risk heat map30—demonstrates higher ACR confers greater risk at any eGFR, yielding actionable, phenotype-specific thresholds for geriatric care.
Relative to established frameworks, our approach complements the CKD Prognosis Consortium (CKD-PC) and the Kidney Failure Risk Equation (KFRE).38–41 CKD-PC established the continuous prognostic value of eGFR and albuminuria for kidney failure, cardiovascular events, and mortality, while KFRE (4-/8-variable) quantifies 2–5-year kidney-failure risk in patients with established CKD. In contrast, our phenotype-aware matrix targets adults ≥70 years and a short-term early-warning endpoint (≥30% eGFR decline over 2 years) across healthy, comorbidity, and CKD phenotypes, yielding actionable thresholds that can be layered upstream of KDIGO, CKD-PC, and KFRE to prioritize monitoring and referral.
Our findings are directionally consistent with prior work in predominantly non-elderly cohorts validating a ≥30% two-year eGFR decline as a clinically meaningful endpoint,12,13 but they recalibrate risk gradients and decision thresholds for geriatric care. Compared with mixed-age or trial populations, older adults—especially those with concordant comorbidities or CKD—exhibited steeper absolute rate increases per eGFR/ACR category and a greater marginal prognostic yield of albuminuria, whereas healthy older adults showed flatter gradients. These differences likely reflect age-related depletion of renal functional reserve and a higher burden of microvascular/proteinuric injury. Our phenotype-tailored joint eGFR–ACR matrix recalibrates early-warning risk gradients in older adults. Given the higher prevalence and adverse consequences of rapid kidney function decline in the elderly,26,42 and in light of the increasing economic and public health burden of population aging, our preliminary findings—if validated—may inform earlier screening and more proactive interventions. These efforts could meaningfully improve outcomes in older individuals. The risk chart derived from our cohort (Figure 2) offers a practical tool for identifying elderly patients most likely to benefit from targeted therapeutic strategies.
The risk of rapid kidney function decline remained very low (< 5%) for healthy older adults with baseline eGFR ≥75 mL/min/1.73 m2. Within this group, risk rose to low (5–7.5%) at eGFR 60–75 mL/min/1.73 m2 and to moderate (7.5–15%) at eGFR <60 mL/min/1.73 m2. Among older adults with comorbidities, risk was low only when ACR <30 mg/g with eGFR ≥75 mL/min/1.73 m2 or when ACR ≥30 mg/g with eGFR ≥90 mL/min/1.73 m2; all other eGFR–ACR combinations were moderate. In the CKD cohort, ACR <30 mg/g with eGFR ≥60 mL/min/1.73 m2 or ACR ≥30 mg/g with eGFR ≥75 mL/min/1.73 m2 corresponded to moderate risk, whereas all remaining cells were high (>15%). When ACR ≥30 mg/g, maintaining eGFR ≥75 mL/min/1.73 m2 appears important to mitigate risk. These between-cohort differences of risk stratification are expected and likely reflect differences in baseline functional reserve, phenotype-specific pathobiology (greater microvascular injury/inflammation in comorbidity/CKD),43,44 and differences in exposure distributions like that people with kidney disease or comorbid conditions are typically exposed to multiple medications and undergo more frequent clinical monitoring, factors that may influence renal-function trajectories (steeper absolute rate increase per category in CKD/comorbidity vs healthy; Table 3). Accordingly, a pre-specified joint eGFR–ACR risk matrix provides more granular risk characterization than either dimension alone, while the relative weights of eGFR and ACR appropriately differ by aging phenotype.
We found that the overall risk of rapid kidney function decline was higher in older adults with comorbidities compared to healthy older adults. Conditions such as hypertension and diabetes may contribute to kidney injury, which manifests as vascular sclerosis, glomerular ischemia, and impaired podocyte function.45,46 Thus, our study suggests that, in older adults with comorbidities known to impact kidney function, clinicians should aim to maintain eGFR ≥90 mL/min/1.73 m2, or ACR <30 mg/g with eGFR ≥75 mL/min/1.73 m2, to help slow disease progression.
In our study, findings suggested that tailored eGFR targets should be established based on individual health status, the presence of comorbidities or CKD, and ACR levels. Random forest analysis (Supplementary Method S3) showed that, although eGFR remained a key predictor of kidney function decline among healthy older adults, its relative significance diminished in individuals with comorbidities or CKD, whereas ACR became increasingly important. In healthy older adults, vascular changes such as arterial sclerosis—which reduces kidney filtration efficacy—are the main underlying drivers of changes in eGFR.47 However, conditions such as diabetic nephropathy, hypertensive nephropathy, hyperuricemic nephropathy, and heart failure tend to affect the glomerulus, damaging podocytes and endothelial cells and leading to protein leakage (albuminuria).48–51 As these conditions progress, they can also induce structural and functional kidney damage, making ACR a more sensitive marker of early kidney injury than eGFR in these populations.52 Similarly, in elderly patients with CKD, conditions such as glomerulonephritis can lead to significant glomerular damage, which manifests as proteinuria.53 It therefore makes sense that ACR offered additional prognostic value in the CKD cohort.
This study provides a comprehensive assessment of eGFR, albuminuria, and the risk of rapid kidney function decline in elderly Chinese populations, but several limitations merit consideration. Our cohorts were geographically concentrated, and diagnoses largely relied on medical insurance records and ICD-10 coding, which may have missed subclinical CKD and introduced selection bias. Primary analyses used a complete-case approach; for a small proportion of covariates with missing values, we applied single median imputation. This approach may slightly attenuate variance and between-group differences but is unlikely to change overall patterns or interpretations of the phenotype-specific risk profiles. We adjusted for key confounders,33 yet residual or unmeasured confounding remains possible (eg, exposure to ACE inhibitors, ARBs, or SGLT2 inhibitors). Event counts for harder renal endpoints (≥40% or ≥50% eGFR decline, or renal replacement therapy) were low over two years, limiting precision, and cardiovascular outcomes (3-/4-point MACE) were incompletely ascertained in this time frame.34–36 Spot ACR can vary with timing, hydration, and assay differences; such random variation tends to dilute true associations rather than create false risk gradients. Finally, our primary cohorts comprised 100% Han Chinese, whereas UK Biobank participants are predominantly White British; while use of the CKD-EPI creatinine–cystatin C equation mitigates some race-related estimation differences, population heterogeneity may still influence surrogate endpoint for ESRD and intervention thresholds. Future studies should externally validate these phenotype-specific thresholds in independent, multi-center cohorts—including non-Chinese populations—and, where needed, recalibrate them for local practice. Future studies should also extend follow-up to assess hard outcomes (ESRD, 3-/4-point MACE and mortality) to test transportability and clinical utility.
Our pre-specified joint eGFR–ACR risk matrix is designed to complement—not replace—KDIGO. After routine eGFR and ACR testing, clinicians can apply the matrix to provide an early-warning estimate of ≥30% decline over two years, tailored by aging phenotype. This supports tailored monitoring and timely nephrology referral within existing KDIGO pathways without redefining CKD.
Conclusions
In summary, our findings indicate that a pre-specified joint eGFR–ACR risk matrix tailored by aging phenotype provides earlier risk characterization, complementing KDIGO-based staging to prioritize monitoring and timely referral in older adults.
Data Sharing Statement
The materials underlying the published results are included in the article and Supplementary Information. Due to participant privacy and institutional policies, individual-level data are not publicly available. De-identified data from the Huashan Hospital cohort are available upon reasonable request from the corresponding authors, Dr Jing Chen or Dr Mengjing Wang. De-identified data from the Rugao Longevity and Aging Study (RLAS) cohort are available upon reasonable request from the data custodian, Dr Xiaofeng Wang; requests can be coordinated via the corresponding authors.
Ethics Approval and Consent to Participate
The study was approved by the Human Ethics Committee of the School of Life Sciences, Fudan University, and Medical Ethics Committee of Huashan Hospital, Fudan University. Written informed consent was obtained from all participants. All methods were performed in accordance with relevant guidelines and regulations.
Acknowledgments
The authors are grateful to all those who participated in this study and wish to acknowledge the valuable advice and assistance obtained from the Ministry of Education Key Laboratory of Contemporary Anthropology, Human Phenome Institute, Fudan University, and all specialist physicians at Huashan Hospital, Fudan University. The funders had no role in the study design, data collection or analysis, the decision to publish, or the preparation of the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by grants from the National Natural Science Foundation of China (W2411077, 81730017, 82470765); the National Key R&D Program of China (2020YFC2005000, 2018YFC2000400); the Shanghai Municipal Health Commission Clinical Research Project (202540108); the Shanghai Shenkang Municipal Hospital Joint Research Project (SHDC12025117); the Fudan University medical engineering project (yg2023-05, yg2023-18); and the Shanghai Municipal Health Commission (ZHYYZXYYD-202510).
Disclosure
None of the authors have any conflicts of interest in relation to this report.
References
1. Buyadaa O, Magliano DJ, Salim A, Koye DN, Shaw JE. Risk of rapid kidney function decline, all-cause mortality, and major cardiovascular events in nonalbuminuric chronic kidney disease in type 2 diabetes. Diabetes Care. 2020;43(1):122–129. doi:10.2337/dc19-1438
2. Rifkin DE, Shlipak MG, Katz R, et al. Rapid kidney function decline and mortality risk in older adults. Arch Intern Med. 2008;168(20):2212–2218. doi:10.1001/archinte.168.20.2212
3. Guo Y, Cui L, Ye P, Li J, Wu S, Luo Y. Change of kidney function is associated with all-cause mortality and cardiovascular diseases: results from the kailuan study. J Am Heart Assoc. 2018;7(21):e010596. doi:10.1161/JAHA.118.010596
4. Flaherty CM, Surapaneni A, Seegmiller JC, Coresh J, Grams ME, Ballew SH. CKD prevalence and incidence in older adults using estimated GFR with different filtration markers: the atherosclerosis risk in communities study. Kidney Med. 2024;6(10):100893. doi:10.1016/j.xkme.2024.100893
5. Stevens LA, Li S, Wang C, et al. Prevalence of CKD and comorbid illness in elderly patients in the United States: results from the Kidney Early Evaluation Program (KEEP). Am J Kidney Dis. 2010;55(3 Suppl 2):S23–33. doi:10.1053/j.ajkd.2009.09.035
6. Zhang QL, Rothenbacher D. Prevalence of chronic kidney disease in population-based studies: systematic review. BMC Public Health. 2008;8:117. doi:10.1186/1471-2458-8-117
7. Kellum JA, Romagnani P, Ashuntantang G, Ronco C, Zarbock A, Anders HJ. Acute kidney injury. Nat Rev Dis Primers. 2021;7(1):52. doi:10.1038/s41572-021-00284-z
8. Akbar S, Moss AH. The ethics of offering dialysis for AKI to the older patient: time to re-evaluate? Clin J Am Soc Nephrol. 2014;9(9):1652–1656. doi:10.2215/CJN.01630214
9. Feest TG, Round A, Hamad S. Incidence of severe acute renal failure in adults: results of a community based study. BMJ. 1993;306(6876):4813. doi:10.1136/bmj.306.6876.481
10. Schmitt R, Coca S, Kanbay M, Tinetti ME, Cantley LG, Parikh CR. Recovery of kidney function after acute kidney injury in the elderly: a systematic review and meta-analysis. Am J Kidney Dis. 2008;52(2):262–271. doi:10.1053/j.ajkd.2008.03.005
11. Coresh J, Turin TC, Matsushita K, et al. Decline in estimated glomerular filtration rate and subsequent risk of end-stage renal disease and mortality. JAMA. 2014;311(24):2518–2531. doi:10.1001/jama.2014.6634
12. Lambers Heerspink HJ, Tighiouart H, Sang Y, et al. GFR decline and subsequent risk of established kidney outcomes: a meta-analysis of 37 randomized controlled trials. Am J Kidney Dis. 2014;64(6):860–866. doi:10.1053/j.ajkd.2014.08.018
13. Levey AS, Inker LA, Matsushita K, et al. GFR decline as an end point for clinical trials in CKD: a scientific workshop sponsored by the national kidney foundation and the US food and drug administration. Am J Kidney Dis. 2014;64(6):821–835. doi:10.1053/j.ajkd.2014.07.030
14. Kovesdy CP, Coresh J, Ballew SH, et al. Past decline versus current eGFR and subsequent ESRD risk. J Am Soc Nephrol. 2016;27(8):2447–2455. doi:10.1681/ASN.2015060687
15. Sharma A, Mucino MJ, Ronco C. Renal functional reserve and renal recovery after acute kidney injury. Nephron Clin Pract. 2014;127(1–4):94–100. doi:10.1159/000363721
16. Chowdhury SR, Chandra Das D, Sunna TC, Beyene J, Hossain A. Global and regional prevalence of multimorbidity in the adult population in community settings: a systematic review and meta-analysis. EClinicalMedicine. 2023;57:101860. doi:10.1016/j.eclinm.2023.101860
17. Perkowska-Ptasinska A, Deborska-Materkowska D, Bartczak A, et al. Kidney disease in the elderly: biopsy based data from 14 renal centers in Poland. BMC Nephrol. 2016;17(1):194. doi:10.1186/s12882-016-0410-8
18. Russo GT, De Cosmo S, Viazzi F, et al. Diabetic kidney disease in the elderly: prevalence and clinical correlates. BMC Geriatr. 2018;18(1):38. doi:10.1186/s12877-018-0732-4
19. Ronco P, Beck L, Debiec H, et al. Membranous nephropathy. Nat Rev Dis Primers. 2021;7(1):69. doi:10.1038/s41572-021-00303-z
20. Wang M, Ding D, Zhao Q, et al. Kidney function and dementia risk in community-dwelling older adults: the Shanghai Aging Study. Alzheimers Res Ther. 2021;13(1):21. doi:10.1186/s13195-020-00729-9
21. Wang M, Sun X, Zhang W, et al. Frailty and the risk of kidney function decline in the elderly population: the Rugao longevity and ageing study. Nephrol Dial Transplant. 2021;36(12):2274–2281. doi:10.1093/ndt/gfaa323
22. Armenta A, Madero M, Rodriguez-Iturbe B. Functional reserve of the kidney. Clin J Am Soc Nephrol. 2022;17(3):458–466. doi:10.2215/CJN.11070821
23. Noel S, Parikh CR. Kidney functional reserve helps early detection of subclinical chronic kidney disease. Am J Physiol Renal Physiol. 2023;325(6):F885–F887. doi:10.1152/ajprenal.00327.2023
24. Levey AS, de Jong PE, Coresh J, et al. The definition, classification, and prognosis of chronic kidney disease: a KDIGO controversies conference report. Kidney Int. 2011;80(1):17–28. doi:10.1038/ki.2010.483
25. Gansevoort RT, Matsushita K, van der Velde M, et al. Lower estimated GFR and higher albuminuria are associated with adverse kidney outcomes. A collaborative meta-analysis of general and high-risk population cohorts. Kidney Int. 2011;80(1):93–104. doi:10.1038/ki.2010.531
26. Hussain J, Grubic N, Akbari A, et al. Associations between modest reductions in kidney function and adverse outcomes in young adults: retrospective, population based cohort study. BMJ. 2023:381:e075062. doi:10.1136/bmj-2023-075062
27. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group, Summary of Recommendation Statements. Kidney Int Suppl. 2013;3(1):5–14. doi:10.1038/kisup.2012.77
28. Inker LA, Schmid CH, Tighiouart H, et al. Estimating glomerular filtration rate from serum creatinine and cystatin C. N Engl J Med. 2012;367(1):20–29. doi:10.1056/NEJMoa1114248
29. Wang M, Sun X, Ni L, et al. Comparative performance of creatinine-based GFR estimation equations in exceptional longevity: the rugao longevity and ageing study. Clin Interv Aging. 2020;15:733–742. doi:10.2147/CIA.S250535
30. de Boer IH, Khunti K, Sadusky T, et al. Diabetes management in chronic kidney disease: a consensus report by the American Diabetes Association (ADA) and Kidney Disease: improving Global Outcomes (KDIGO). Kidney Int. 2022;102(5):974–989. doi:10.1016/j.kint.2022.08.012
31. Liu Z, Wang Y, Zhang Y, et al. Cohort profile: the Rugao Longevity and Ageing Study (RuLAS). Int J Epidemiol. 2016;45(4):1064–1073. doi:10.1093/ije/dyv101
32. Tonelli M, Wiebe N, Guthrie B, et al. Comorbidity as a driver of adverse outcomes in people with chronic kidney disease. Kidney Int. 2015;88(4):859–866. doi:10.1038/ki.2015.228
33. Cohen E, Nardi Y, Krause I, et al. A longitudinal assessment of the natural rate of decline in renal function with age. J Nephrol. 2014;27(6):635–641. doi:10.1007/s40620-014-0077-9
34. Ronco C, Bellomo R, Kellum J. Understanding renal functional reserve. Intensive Care Med. 2017;43(6):917–920. doi:10.1007/s00134-017-4691-6
35. Perschinka F, Boyer N, Forni LG, Joannidis M. Renal function in very old critically ill patients. Curr Opin Crit Care. 2023;29(6):534–541. doi:10.1097/MCC.0000000000001088
36. Palsson R, Waikar SS. Renal functional reserve revisited. Adv Chronic Kidney Dis. 2018;25(3):e1–e8. doi:10.1053/j.ackd.2018.03.001
37. Wang J, Sourlos N, Heuvelmans M, Prokop M, Vliegenthart R, van Ooijen P. Explainable machine learning model based on clinical factors for predicting the disappearance of indeterminate pulmonary nodules. Comput Biol Med. 2024;169:107871. doi:10.1016/j.compbiomed.2023.107871
38. Tangri N, Grams ME, Levey AS, et al. Multinational assessment of accuracy of equations for predicting risk of kidney failure: a meta-analysis. JAMA. 2016;315(2):164–174. doi:10.1001/jama.2015.18202
39. Mahmoodi BK, Matsushita K, Woodward M, et al. Associations of kidney disease measures with mortality and end-stage renal disease in individuals with and without hypertension: a meta-analysis. Lancet. 2012;380(9854):1649–1661. doi:10.1016/S0140-6736(12)61272-0
40. Matsushita K, Coresh J, Sang Y, et al. Estimated glomerular filtration rate and albuminuria for prediction of cardiovascular outcomes: a collaborative meta-analysis of individual participant data. Lancet Diabetes Endocrinol. 2015;3(7):514–525. doi:10.1016/S2213-8587(15)00040-6
41. Tangri N, Stevens LA, Griffith J, et al. A predictive model for progression of chronic kidney disease to kidney failure. JAMA. 2011;305(15):1553–1559. doi:10.1001/jama.2011.451
42. Shlipak MG, Katz R, Kestenbaum B, et al. Rapid decline of kidney function increases cardiovascular risk in the elderly. J Am Soc Nephrol. 2009;20(12):2625–2630. doi:10.1681/ASN.2009050546
43. Balakumar P, Chakkarwar VA, Singh M. Ameliorative effect of combination of benfotiamine and fenofibrate in diabetes-induced vascular endothelial dysfunction and nephropathy in the rat. Mol Cell Biochem. 2009;320(1–2):149–162. doi:10.1007/s11010-008-9917-z
44. Balakumar P, Chakkarwar VA, Kumar V, Jain A, Reddy J, Singh M. Experimental models for nephropathy. J Renin Angiotensin Aldosterone Syst. 2008;9(4):189–195. doi:10.1177/1470320308098343
45. Hu S, Hang X, Wei Y, Wang H, Zhang L, Zhao L. Crosstalk among podocytes, glomerular endothelial cells and mesangial cells in diabetic kidney disease: an updated review. Cell Commun Signal. 2024;22(1):136. doi:10.1186/s12964-024-01502-3
46. Wu T, Ding L, Andoh V, Zhang J, Chen L. The mechanism of hyperglycemia-induced renal cell injury in diabetic nephropathy disease: an update. Life. 2023;13(2):539. doi:10.3390/life13020539
47. Hommos MS, Glassock RJ, Rule AD. Structural and functional changes in human kidneys with healthy aging. J Am Soc Nephrol. 2017;28(10):2838–2844. doi:10.1681/ASN.2017040421
48. Huang Z, Hong Q, Zhang X, et al. Aldose reductase mediates endothelial cell dysfunction induced by high uric acid concentrations. Cell Commun Signal. 2017;15(1):3. doi:10.1186/s12964-016-0158-6
49. Jung SW, Kim SM, Kim YG, Lee SH, Moon JY. Uric acid and inflammation in kidney disease. Am J Physiol Renal Physiol. 2020;318(6):F1327–F1340. doi:10.1152/ajprenal.00272.2019
50. Cimmino G, Conte S, Marra L, et al. Uric acid induces a proatherothrombotic phenotype in human endothelial cells by imbalancing the tissue factor/tissue factor pathway inhibitor pathway. Thromb Haemost. 2023;123(1):64–75. doi:10.1055/a-1947-7716
51. Tsigkou V, Oikonomou E, Anastasiou A, et al. Molecular mechanisms and therapeutic implications of endothelial dysfunction in patients with heart failure. Int J Mol Sci. 2023;24(5). doi:10.3390/ijms24054321
52. Levey AS, Coresh J. Chronic kidney disease. Lancet. 2012;379(9811):165–180. doi:10.1016/S0140-6736(11)60178-5
53. Liang J, Hao W, Xia F, et al. Clinicopathological features and outcome in elderly patients with idiopathic membranous nephropathy. Ren Fail. 2023;45(1):2212081. doi:10.1080/0886022X.2023.2212081
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Elevated Serum Osteoprotegerin is Associated with Reduced Risks of Albuminuria and CKD Progression in Patients with Type 2 Diabetes
Lou X, Yang Z, Wu K, Li W, Hu W, Nie R, Tu P, Duan P
Diabetes, Metabolic Syndrome and Obesity 2022, 15:3831-3841
Published Date: 12 December 2022
A 5-Year Follow-Up Study to Explore Factors Associated with Rapid Kidney Function Decline Among Bus Drivers
Wu Y, Chen Q, Zhang Q, Wu Y, Zheng X
International Journal of General Medicine 2023, 16:3193-3201
Published Date: 28 July 2023