")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Efficacy and Safety of Low-Dose Brexpiprazole for Acute Schizophrenia: Meta-Analysis of Randomized Placebo-Controlled Trials
Authors Zhao M, Qin B, Mao Y, Wang H, Wang A, Wang C
Received 13 May 2022
Accepted for publication 7 August 2022
Published 11 August 2022 Volume 2022:18 Pages 1705—1713
DOI https://doi.org/10.2147/NDT.S374577
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jun Chen
Mingjun Zhao,1,* Bin Qin,2,* Yage Mao,3 Hailing Wang,1 Aiqin Wang,1 Chuansheng Wang4
1Department of Pharmacy, The Second Affiliated Hospital of Xinxiang Medical University (Henan Mental Hospital), Xinxiang, Henan, People’s Republic of China; 2Department of Neurology, Liuzhou General Hospital, Liuzhou, Guangxi, People’s Republic of China; 3Department of Pharmacy, Maternal and Child Health Care Hospital of Xinxiang City, Xinxiang, Henan, People’s Republic of China; 4Department of Psychiatry, The Second Affiliated Hospital of Xinxiang Medical University (Henan Mental Hospital), Xinxiang, Henan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chuansheng Wang, Department of Psychiatry, The Second Affiliated Hospital of Xinxiang Medical University (Henan Mental Hospital), 207# QianJin Road, Xinxiang, Henan, 453000, People’s Republic of China, Tel +86-373-3388772, Fax +86-373-3374082, Email [email protected]
Purpose: The purpose of this meta-analysis was to compare the efficacy and safety profile of low-dose brexpiprazole (< 2 mg/d) compared to placebo and standard-dose brexpiprazole (2– 4 mg/d).
Patients and Methods: We identified relevant studies pertaining to the specific purpose of our meta-analysis by searching PubMed, Web of Science, Embase, Cochrane library, and PsycINFO using the search terms “schizophrenia” or “schizophrenic” AND “brexpiprazole” or “REXULTI”. We systematically reviewed all randomized controlled trials (RCTs) comparing low-dose brexpiprazole with placebo. Primary efficacy outcomes were the PANSS total score change and response rate. Primary safety outcomes were total treatment discontinuation rate, and total serious adverse events (SAEs). Risk ratios (RR) and standardized mean differences (SMDs) were pooled implementing a random effect model.
Results: Four RCTs (2178 patients) were included for effect assessment of low-dose brexpiprazole treatment on the patients with acute schizophrenia. Low-dose brexpiprazole was not superior to placebo (SMD = − 0.11, 95% CI = − 0.23, 0.02, P = 0.10, I2 = 0%), and significantly inferior to standard-dose brexpiprazole (SMD = 0.15, 95% CI = 0.03, 0.26, P = 0.01, I2 = 0%) for PANSS total score change. Low-dose brexpiprazole did not result in significant difference for response rate when compared to placebo and standard-dose brexpiprazole (RR = 1.16, 95% CI = 0.95, 1.41, P = 0.14, I2 = 25%; RR = 0.92, 95% CI = 0.76, 1.12, P = 0.40, I2 = 38%, respectively). For ratio of total discontinuation, low-dose brexpiprazole did not exhibit significant difference when compared to placebo (RR = 0.95, 95% CI = 0.81, 1.11, P = 0.53, I2 = 0%) and standard-dose brexpiprazole group (RR = 1.11, 95% CI = 0.95, 1.29, P = 0.19, I2 = 0%). Total SAEs in low-dose brexpiprazole group did not differ significantly from placebo and standard-dose brexpiprazole group (RR = 0.96, 95% CI = 0.52, 1.80, P = 0.90, I2 = 0%; RR = 1.29, 95% CI = 0.65, 2.57, P = 0.47, I2 = 26%, respectively).
Conclusion: The results indicated that low-dose brexpiprazole may be not superior for improving the efficacy and safety for acute schizophrenia compared to placebo and standard-dose brexpiprazole, and may cause additional risk of increasing body weight. Therefore, using low-dose brexpiprazole in acute schizophrenia patients may be not recommended.
Keywords: brexpiprazole, placebo, acute schizophrenia, RCTs, meta-analysis
Introduction
Schizophrenia is a life-long, frequently debilitating psychotic illness affecting approximately 1% of the world’s population. Symptom expression is highly heterogeneous, but can include positive symptoms such as delusions, hallucinations, and thought disorders, negative symptoms such as emotional withdrawal, passivity, and difficulty beginning and sustaining activities, and cognitive deficits such as impaired executive function (eg, poor response inhibition), information processing, attention, and memory.1–4 Collectively, these symptoms disrupt social and occupational functioning and negatively impact overall quality of life.3,5,6
Successful long-term treatment remains challenging due to therapeutic response heterogeneity and adverse effects.7–10 Schizophrenia is treated using two main classes of antipsychotics: first-generation, or typical, and second-generation, or atypical. Most atypical antipsychotics are antagonists of dopamine D2 and serotonin 5-HT2A receptors, and can alleviate both positive and negative symptoms11,12 with fewer or less severe adverse effects such as extrapyramidal symptoms (EPS), hyperprolactinemia, and cardiovascular abnormalities compared to typical antipsychotics.13,14 However, atypical antipsychotics are associated with other adverse effects such as weight gain, metabolic abnormalities, and QTc prolongation.10,15,16 Furthermore, one previous study of the associations of anti-psychotic dose with efficacy and adverse effects in patients with schizophrenia find that anti-psychotic efficacy appeared to show a clear dose-dependency, and adverse effects (AEs) appeared to be increased in a dose-dependent manner.17 Therefore, there is an urgent need to find new antipsychotic medications that can relieve the most common and debilitating symptoms of schizophrenia with better efficacy, safety and tolerability profiles. In addition, it is vital to define the minimum effective dose each antipsychotic agent for specific symptoms, and thereby, further reduce the risk of AEs.
The atypical antipsychotic brexpiprazole (OPC-34712, branded as Rexulti) is a serotonin–dopamine activity modulator18 approved for the treatment of adult schizophrenia patients in the EU,19 the USA,20 and several other countries, including Japan.21 The recommended target dosage is 2–4 mg once daily, and is achieved by administering a starting dosage of 1 mg once daily on days 1–4, titrating to 2 mg once daily on days 5–7, and if necessary, increasing to 4 mg once daily starting on day 8.22 Thus, the low-dose was defined as <2 mg/d and standard dose as 2–4 mg/d in our present study. Recently, one Phase II/III study23 comparing brexpiprazole at 1 mg/day (fixed), 2 mg/day (fixed), and 4 mg/day (fixed) to placebo, two Phase III studies24,25 comparing fixed-dose brexpiprazole at 0.25 mg/day (Correll study), 1 mg/day (Kane study), 2 mg/day, and 4 mg/day to placebo, and one Phase II, multicenter, six-arm, flexible-dose double-blind, randomized placebo-controlled trial (DBRCT) study26 comparing brexpiprazole at 0.25, 1, 2.5, and 5 mg/day showed discrepancies in outcomes of efficacy and safety for low-dose brexpiprazole. Combined with the previous research for antipsychotics’ dose-dependent effects on efficacy and adverse effects in schizophrenia,17 further studies are urgently needed to evaluate the effect of low dose brexpiprazole for specific symptoms of acute schizophrenia.
The present study addresses two clinical questions not clear answered in the above mentioned studies: 1) Does low dose brexpiprazole have any benefit for the treatment of acute schizophrenia? 2) Are there differences in efficacy (ie, the PANSS scores, response rate), and safety (ie, the discontinuation rate, the incidence of individual adverse events, weight gain and metabolic parameters) between low dose and standard dose brexpiprazole for the treatment of acute schizophrenia?
Treatment with some antipsychotic medications is associated with clinically significant reductions in non-high density lipoprotein cholesterol (non-HDL-C), and unfavorable changes in the triglyceride: HDL-C ratio.27 One previous study find that brexpiprazole may be one of the few available antipsychotic medications with moderate adverse metabolic.28 Therefore, we used total cholesterol, HDL cholesterol, and low density lipoprotein (LDL) cholesterol as the metabolic parameters, and performed the following meta-analysis comparing the efficacy and safety of low-dose brexpiprazole compared to placebo standard-dose brexpiprazole for the treatment of acute schizophrenia.
Materials and Methods
All steps of this review were performed in strict accordance with the Cochrane Handbook for Systematic Reviews of Interventions29 and the results are reported according to the Preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement guidelines.30
Search Strategy
We searched for articles in PubMed, Web of Science, Embase, ClinicalTrials, Cochrane library, and PsycINFO without language restrictions using the search terms “schizophrenia” or “schizophrenic” AND “brexpiprazole” or “REXULTI” from database inception to March 29, 2022 (Supplementary Table 1). Additionally, the bibliographies of included randomized controlled trials (RCTs), relevant reviews, or meta-analyses were manually searched for further relevant published and unpublished studies that may have been missed in the initial electronic search. The authors also searched ClinicalTrials.gov and conference summaries to ensure that the search was as comprehensive as possible and minimize the possibility of publication bias.
Eligibility Criteria and Study Selection
We included all DBRCTs meeting the following criteria: (a) all study patients were in the acute phase of schizophrenia according to any standard diagnostic criteria (DSM-III, DSM-III-R, DSM-IV, DSM-IV-TR, DSM-5, or ICD-10); and (b) studies compared low-dose brexpiprazole (<2 mg/d) monotherapy to placebo or standard-dose brexpiprazole (2–4 mg/d). We excluded (a) duplicate publications, (b) pooled analyses, (c) Non-double blinded studies, (e) no relevant interventions, and (f) studies lacking quantitative data on efficacy, and safety. Eligibility screening was performed in two steps. First, both independent reviewers screened titles and abstracts for relevance to the study objective, and then performed full-text screening for eligibility. Conflicts were resolved by discussions with a third reviewer. We included articles in peer-reviewed journals, abstracts submitted to conferences, and available results at ClinicalTrials.gov, with no restrictions regarding schizophrenia severity, demographic factors, or study location. In order to reduce the heterogeneity due to treatment duration, as the previous study,31 only DBRCTs involving patients experiencing an acute exacerbation of symptoms and prescribed brexpiprazole were included.
Outcome Measures
Both dichotomous and continuous measures of schizophrenia outcomes were included in this meta-analysis. Total score and sub-scores on the PANSS are used routinely as outcome measures in treatment efficacy studies32 during treatment. Primary efficacy outcomes were changes in PANSS total score33,34 from baseline to endpoint, response rate at week 6. Primary safety outcomes were total treatment discontinuation rate, and total serious adverse events (SAEs). The response rate was defined as a ≥30% reduction in PANSS total score from baseline or a score of 1 (very much improved) or 2 (much improved) on the Clinical Global Impression-Improvement (CGI-I) scale.35 Secondary efficacy outcomes were changes in PANSS positive and negative subscale scores on week 6 compared to baseline. Secondary safety outcomes were discontinuation due to AEs, total treatment-emergent adverse events (TEAEs), and metabolic parameters (eg, the proportions of patients demonstrating a ≥ 7% increase in body weight, level changes in total cholesterol, HDL cholesterol, and LDL cholesterol).
Data Extraction
The recommended target REXULTI dosage is 2 mg to 4 mg once daily for treatment of schizophrenia according to FDA instructions.22 The standard dose was defined as 2–4 mg/d and low-dose as <2 mg/d in our present study according to the information from FDA.22 Two independent investigators individually identified the articles according to inclusion and exclusion criteria, and extracted data separately for low-dose brexpiprazole, standard-dose brexpiprazole, and placebo groups. All data were extracted using a standardized form to ensure consistency. Data were summarized by one investigator and checked by a second reviewer. Any discrepancies were resolved by discussion or involvement of a third author.
Risk of Bias Assessment
Two independent researchers assessed the methodological quality of each study using Risk of Bias Assessment Tool from the Cochrane Handbook for Systematic Reviews of Intervention, and the risk of bias table containing seven dimensions of Random sequence generation (selection bias); Allocation concealment (selection bias); Blinding of participants and personnel (performance bias); Blinding of outcome assessment (detection bias); Incomplete outcome data (attrition bias); Selective reporting (reporting bias); Other bias was generated using Review Manager (Rev-Man) version 5.3 (http://www.cochrane.org). To reduce reporting biases, we also searched and evaluated unpublished literature and accessed online trial registries. Each risk of bias domain was rated as “high risk”, “unclear risk” or “low risk”.29
Data Analysis
The meta-analysis was performed using RevMan 5.3. We only included outcomes for which ≥2 datasets were available. The random-effects model of DerSimonian and Laird36 was used for data pooling as it is more conservative than typical fixed-effects models, and thus, is more appropriate when there is potential heterogeneity across studies. We estimated the effect sizes and pooled estimates of effect across studies using Risks Ratios (RR) for dichotomous measures and standardized mean differences (SMDs) for continuous measures (with corresponding 95% confidence intervals (CIs). We also assessed heterogeneity using the Q statistic and the I2 statistic, with Q test P value <0.1 or I2 ≥ 50% indicating significant heterogeneity, and I2 values of 25%, 50%, and 75%, signifying mild, moderate and high heterogeneity, respectively.37,38
Results
Search Results
A total of 696 records were identified through database searches (PubMed:144; Cochrane Library:86; Embase:240; Web of Science:121; ClinicalTrials:76; PsycINFO:29). After excluding 272 reduplicate records, we initially retrieved 424 potentially relevant studies. Of these, 359 were excluded for not meeting inclusion criteria after reading the title or abstract. A total of 61 studies were further excluded after two reviewers independently read the full texts. Finally, four studies23–26 with a total of 2178 patients met our inclusion criteria were included in this meta-analysis (Figure 1).
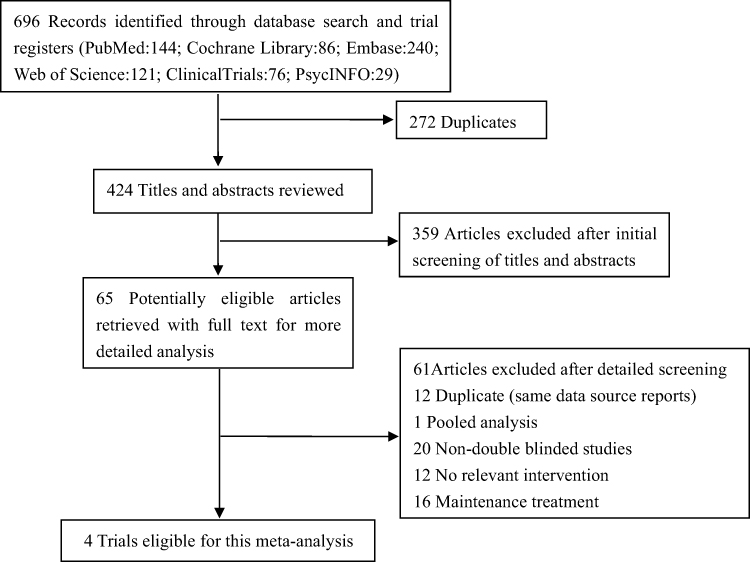 |
Figure 1 Prisma flow chart of study selection. Notes: PRISMA figure adapted from Liberati A, Altman D, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Journal of clinical epidemiology. 2009;62(10). Creative Commons |
Characteristics of Included Studies
Patient characteristics and the design features of the included trials are summarized in Table 1. Four of the included trials were published between 2015 and 2018, and the results of one unpublished trial were last updated on October 20, 2015. Across the 4 DBRCTs, 2085 patients with acute schizophrenia were randomized to receive low-dose brexpiprazole (n = 456), standard dose brexpiprazole (n = 1050) or placebo (n = 579). Single-study sample sizes ranged from 316 to 674 patients, with a mean sample size of 521.3. Single-study age group ranged from 37.4 to 45, and did not differ in the low-dose group compared to the corresponding placebo, and standard-dose group (P = 0.72 and P = 0.07, respectively). The overall ratio of males was 59.5% (ranging from 47.5% to 63.1%) and did not differ in the low-dose group compared to the corresponding placebo, and standard-dose group (P = 0.45 and P = 0.90, respectively). Patients ranged in age from 18 to 65 years, and mean age did not differ in the low-dose group compared to either the corresponding placebo group or standard-dose group (P = 0.72 and P = 0.07, respectively). Finally, mean baseline PANSS total score ranged from 93.3 to 98.8, and there were no statistically significant differences when low-dose brexpiprazole compared to placebo groups and standard-dose brexpiprazole (P = 0.32; P = 0.41). All the duration of studies was 6 weeks.
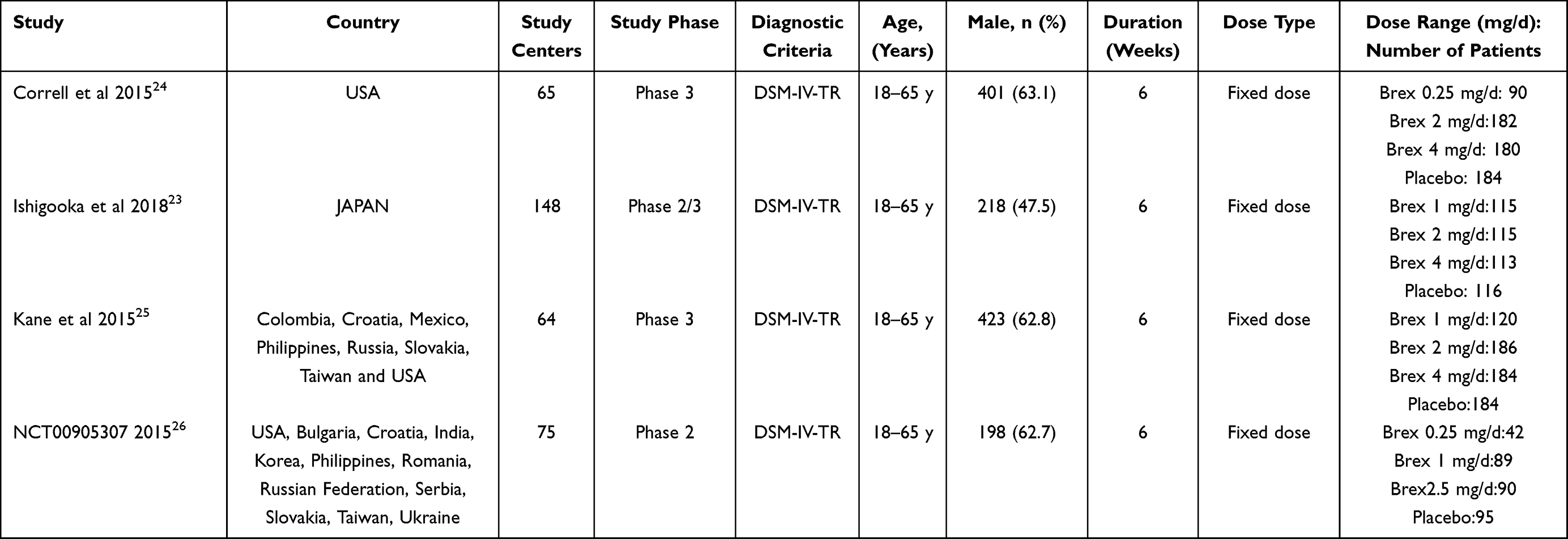 |
Table 1 Characteristics of the Studies Included in the Meta-Analysis |
Study Quality
The risks of bias for each individual DBRTC and the proportions with low risk, unclear risk, and high risk of bias for each domain are shown in Supplementary Figure 1. The overall quality of studies was moderate: three described the method of random sequence generation for group allocation, and allocation concealment was low for three trials. Four studies reported the blinding of participants and assessors. Four trials reported completeness of follow-up for the outcome. No selective reporting was found in either of the studies.
Efficacy Outcomes
In our meta-analyses, low-dose brexpiprazole was not superior to placebo for PANSS total score change (SMD = −0.11, 95% CI = −0.23, 0.02, P = 0.10, I2 = 0%) (Figure 2A) and PANSS positive subscale score change (SMD = −0.02, 95% CI = −0.18, 0.13, P = 0.76, I2 = 36%) (Supplementary Table 2), while was significantly inferior to standard-dose brexpiprazole (SMD = 0.15, 95% CI = 0.03, 0.26, P = 0.01, I2 = 0%), with no heterogeneity for PANSS total score change (Figure 2B), and PANSS positive subscale score change (SMD = 0.12, 95% CI = 0.00, 0.23, P = 0.05, I2 = 0%) (Supplementary Table 2). While, for the change of PANSS negative subscale score, low-dose brexpiprazole exhibited superiority over placebo (SMD = −0.14, 95% CI = −0.26,-0.01, P = 0.03, I2 = 0%) with no substantial heterogeneity, and inferiority to standard-dose brexpiprazole (SMD = 0.11, 95% CI = −0.00, 0.23, P = 0.05, I2 = 0%) (Supplementary Table 2).
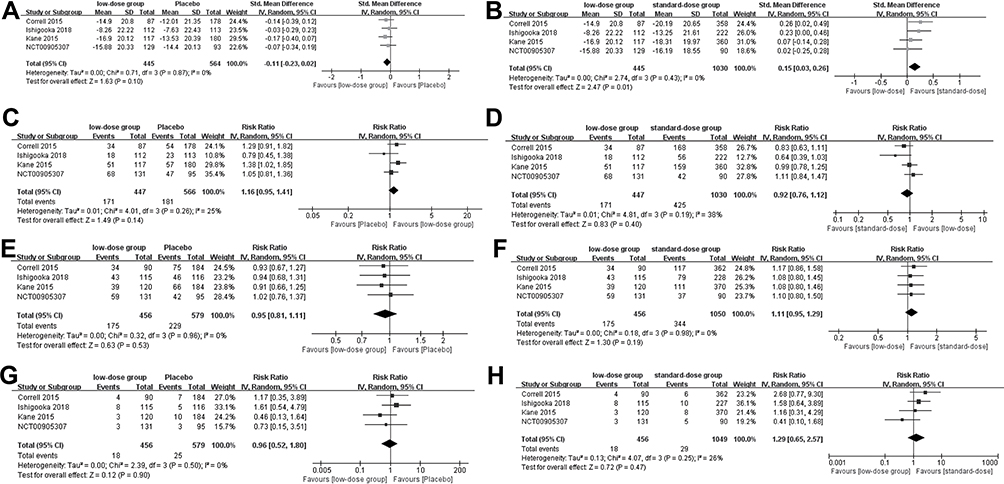 |
Figure 2 Forest plot for the primary outcomes, (A) PANSS total score change between low-dose brexpiprazole and placebo, (B) PANSS total score change between low-dose and standard-dose brexpiprazole, (C) response rate between low-dose brexpiprazole and placebo, (D) response rate between low-dose and standard-dose brexpiprazole, (E) total discontinuation between low-dose brexpiprazole and placebo, (F) total discontinuation between low-dose and standard-dose brexpiprazole, (G) total SAEs between low-dose brexpiprazole and placebo, (H) total SAEs between low-dose and standard-dose brexpiprazole. |
Low-dose brexpiprazole did not result in significant difference for response rate when compared to placebo (Figure 2C) and standard-dose brexpiprazole (Figure 2D) (RR = 1.16, 95% CI = 0.95, 1.41, P = 0.14, I2 = 25%; RR = 0.92, 95% CI = 0.76, 1.12, P = 0.40, I2 = 38%, respectively) at week 6.
Safety Outcomes
For the ratio of total discontinuation, low-dose brexpiprazole did not show significant difference when compared to placebo (RR = 0.95, 95% CI = 0.81, 1.11, P = 0.53, I2 = 0%) (Figure 2E) and standard-dose brexpiprazole groups (RR = 1.11, 95% CI = 0.95, 1.29, P = 0.19, I2 = 0%) (Figure 2F). Results of discontinuation due to AEs were similar (low-dose brexpiprazole vs placebo: RR = 0.84, 95% CI = 0.60, 1.18, P = 0.31, I2 = 0%; low-dose brexpiprazole vs standard-dose brexpiprazole group: RR = 1.33, 95% CI = 0.95, 1.85, P = 0.09, I2 = 0%) (Supplementary Table 2).
Total SAEs in low-dose brexpiprazole group did not differ significantly from placebo (RR = 0.96, 95% CI = 0.52, 1.80, P = 0.90, I2 = 0%) (Figure 2G) and standard-dose brexpiprazole group (RR = 1.29, 95% CI = 0.65, 2.57, P = 0.47, I2 = 26%) (Figure 2H). Similarly, low-dose brexpiprazole group did not exhibit significant difference when compared to placebo (RR = 0.94, 95% CI = 0.83, 1.07, P = 0.38, I2 = 30%) and standard-dose brexpiprazole group (RR = 0.98, 95% CI = 0.89, 1.09, P = 0.77, I2 = 10%) for total TEAEs in (Supplementary Table 2). Potentially clinically relevant increases in body weight (≥7%) were higher in low-dose brexpiprazole group than in the placebo group (RR = 2.90, 95% CI = 1.26, 6.67, P = 0.01, I2 = 0%) with no significant heterogeneity. While there was no significant difference between low-dose and standard-dose brexpiprazole (RR = 0.9, 95% CI = 0.53, 1.52, P = 0.68, I2 = 0%) with no significant heterogeneity (Supplementary Table 2).
Low-dose brexpiprazole did not result in significant difference for total cholesterol (SMD = −0.00, 95% CI = −0.15, 0.15, P = 1.00, I2 = 0%), HDL cholesterol (SMD = 0.10, 95% CI = −0.07, 0.27, P = 0.24, I2 = 25%), or LDL cholesterol (SMD = 0.00, 95% CI = −0.15, 0.15, P = 0.98, I2 = 0%) with mild substantial heterogeneity when compared to placebo. Similarly, there were no significant differences between low-dose and standard-dose brexpiprazole groups for all the metabolic parameters above mentioned with the exception of HDL cholesterol, which was lower in the low-dose group (SMD = −0.17, 95% CI = −0.31,-0.04, P = 0.01, I2 = 0%) (Supplementary Table 2).
Discussion
We performed meta-analyses of efficacy and safety of low-dose brexpiprazole for the treatment of acute schizophrenia based on four DBRCTs. We performed two sets of meta-analyses comparing low-dose brexpiprazole with placebo and standard-dose brexpiprazole. According to this meta-analysis, low-dose brexpiprazole may not exhibit significant differences in improving the symptoms of schizophrenia compared to placebo (with the exception of PNASS negative subscale score change) and standard-dose brexpiprazole, further, may exhibit higher increase in body weight compared to placebo.
Second-generation antipsychotics can reduce positive and negative symptoms of schizophrenia without the severe motor side effects of first generation antipsychotics, but may also induce a distinct set of adverse reactions, including cognitive impairment.39 In large-scale studies of schizophrenia patients, cognitive dysfunction is frequently estimated by the cognitive component of the PANSS.40 Despite low-dose brexpiprazole significantly reduced the PANSS negative subscale score compared to placebo, however, it did not show superiority in the PANSS total and PANSS positive subscale score. Moreover, low-dose brexpiprazole showed the inferiority compared to standard-dose brexpiprazole for all of the PANSS total score, positive and negative subscale score change. The meta-analysis also showed that low-dose brexpiprazole was not superior to placebo for improving the patients’ response rates. Although it is difficult to draw conclusions regarding dose-response relationship from the results obtained in this study due to the brexpiprazole low-dose arm not being fully powered, low-dose brexpiprazole may not exhibit superiority for efficacy, furthermore, the standard dose may appear more appropriate for cognitive deficits associated with acute schizophrenia.
For safety, there was a high completion rate for low-dose brexpiprazole treatment groups with similar incidences of total and AEs related discontinuations across the low-dose brexpiprazole group, standard-dose brexpiprazole group and placebo group. SAEs and TEAEs of low-dose brexpiprazole group observed in this study did not differ significantly from placebo and standard-dose brexpiprazole group. However, our study showed that low-dose brexpiprazole increased the risk of body weight gain ≥7% compared to placebo treatment, consistent with product warnings by the FDA.22
Brexpiprazole and other currently available antipsychotic medications also frequently induce adverse metabolic effects such as increased blood glucose and maladaptive changes in lipid fractions, although magnitudes vary widely among specific drugs and patients.10,41 In our study, patients receiving low-dose brexpiprazole did not exhibited a significantly greater risk of elevated total cholesterol, HDL cholesterol, and LDL cholesterol compared to placebo, but those receiving the standard dose also demonstrated significant higher HDL cholesterol compared to low-dose brexpiprazole. Thus, the low-dose brexpiprazole may not show superiority for safety indicators compared to both placebo and standard-dose brexpiprazole, even may produce a significant rise in body weight.
This study has several limitations. First, just 4 DBRTCs involving only 2178 patients were included, and the treatment duration was relatively brief (up to 6 weeks). Second, the study population was restricted to patients experiencing acute exacerbation.
Conclusion
This meta-analysis suggests that low-dose brexpiprazole may be not superior for improving the efficacy and safety for acute schizophrenia compared to placebo and standard-dose brexpiprazole, and may cause additional risk of increasing body weight. Clinicians should interpret and translate our data with caution, as the meta-analysis was based on a limited number of randomized controlled trials. Further head-to-head studies comparing the relative efficacy and safety of different brexpiprazole doses for acute schizophrenia are warranted to better define the risk-to-benefit relationship for individual symptom.
Acknowledgments
We thank International Science Editing (http://www.internationalscienceediting.com) for editing and proofreading the manuscript.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests.
References
1. Messias E, Chen C, Eaton W. Epidemiology of schizophrenia: review of findings and myths. Psychiatr Clin North Am. 2007;30(3):323–338. doi:10.1016/j.psc.2007.04.007
2. McGrath J, Saha S, Chant D, Welham J. Schizophrenia: a concise overview of incidence, prevalence, and mortality. Epidemiol Rev. 2008;30:67–76. doi:10.1093/epirev/mxn001
3. Volavka J, Citrome L. Oral antipsychotics for the treatment of schizophrenia: heterogeneity in efficacy and tolerability should drive decision-making. Expert Opin Pharmacother. 2009;10(12):1917–1928. doi:10.1517/14656560903061309
4. Rössler W, Salize H, van Os J, Riecher-Rössler A. Size of burden of schizophrenia and psychotic disorders. Eur neuropsychopharmacol. 2005;15(4):399–409. doi:10.1016/j.euroneuro.2005.04.009
5. Browne S, Clarke M, Gervin M, Waddington J, Larkin C, O’Callaghan E. Determinants of quality of life at first presentation with schizophrenia. Br J Psychiatr. 2000;176:173–176. doi:10.1192/bjp.176.2.173
6. Hayhurst K, Massie J, Dunn G, Lewis S, Drake R. Validity of subjective versus objective quality of life assessment in people with schizophrenia. BMC Psychiatr. 2014;14:365. doi:10.1186/s12888-014-0365-x
7. Citrome L. A review of the pharmacology, efficacy and tolerability of recently approved and upcoming oral antipsychotics: an evidence-based medicine approach. CNS Drugs. 2013;27(11):879–911. doi:10.1007/s40263-013-0105-7
8. Correll C. From receptor pharmacology to improved outcomes: individualising the selection, dosing, and switching of antipsychotics. Eur Psychiatr. 2010;25:S12–S21. doi:10.1016/s0924-9338(10)71701-6
9. De Hert M, Yu W, Detraux J, Sweers K, van Winkel R, Correll C. Body weight and metabolic adverse effects of asenapine, iloperidone, lurasidone and paliperidone in the treatment of schizophrenia and bipolar disorder: a systematic review and exploratory meta-analysis. CNS Drugs. 2012;26(9):733–759. doi:10.2165/11634500-000000000-00000
10. Leucht S, Cipriani A, Spineli L, et al. Comparative efficacy and tolerability of 15 antipsychotic drugs in schizophrenia: a multiple-treatments meta-analysis. Lancet. 2013;382(9896):951–962. doi:10.1016/s0140-6736(13)60733-3
11. Mauri M, Paletta S, Maffini M, et al. Clinical pharmacology of atypical antipsychotics: an update. EXCLI J. 2014;13:1163–1191.
12. Miyamoto S, Duncan G, Marx C, Lieberman J. Treatments for schizophrenia: a critical review of pharmacology and mechanisms of action of antipsychotic drugs. Mol Psychiatry. 2005;10(1):79–104. doi:10.1038/sj.mp.4001556
13. Miyamoto S, Miyake N, Jarskog L, Fleischhacker W, Lieberman J. Pharmacological treatment of schizophrenia: a critical review of the pharmacology and clinical effects of current and future therapeutic agents. Mol Psychiatry. 2012;17(12):1206–1227. doi:10.1038/mp.2012.47
14. Uçok A, Gaebel W. Side effects of atypical antipsychotics: a brief overview. World Psychiatr. 2008;7(1):58–62. doi:10.1002/j.2051-5545.2008.tb00154.x
15. De Hert M, Detraux J, van Winkel R, Yu W, Correll C. Metabolic and cardiovascular adverse effects associated with antipsychotic drugs. Nat Rev Endocrinol. 2011;8(2):114–126. doi:10.1038/nrendo.2011.156
16. Kane J, Barnes T, Correll C, et al. Evaluation of akathisia in patients with schizophrenia, schizoaffective disorder, or bipolar I disorder: a post hoc analysis of pooled data from short- and long-term aripiprazole trials. J Psychopharmacol. 2010;24(7):1019–1029. doi:10.1177/0269881109348157
17. Yoshida K, Takeuchi H. Dose-dependent effects of antipsychotics on efficacy and adverse effects in schizophrenia. Behav Brain Res. 2021;402:113098. doi:10.1016/j.bbr.2020.113098
18. Maeda K, Lerdrup L, Sugino H, et al. Brexpiprazole II: antipsychotic-like and procognitive effects of a novel serotonin-dopamine activity modulator. J Pharmacol Exp Ther. 2014;350(3):605–614. doi:10.1124/jpet.114.213819
19. European Medicines Agency. RXULTI 0.24-4 mg film coated tablets: EU summary of product characteristics; 2018. Available from: https://www.ema.europa.eu.
20. Otsuka Pharmaceutical Co Ltd. REXULTI® (brexpiprazole) tablets, for oral use: US prescribing information; 2015. Available from: https://www.accessdata.fda.gov.
21. Otsuka Pharmaceutical Co., Ltd. REXULTI® 1 mg, 2 mg tablets: Japanese prescribing information; 2018. Available from: http://www.pmda.go.jp.
22. Rexulti® (brexpiprazole) [full prescribing information]; 2020. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/205422s005lbl.pdf.
23. Ishigooka J, Iwashita S, Tadori Y. Efficacy and safety of brexpiprazole for the treatment of acute schizophrenia in Japan: a 6-week, randomized, double-blind, placebo-controlled study. Psychiatry Clin Neurosci. 2018;72(9):692–700. doi:10.1111/pcn.12682
24. Correll C, Skuban A, Ouyang J, et al. Efficacy and safety of brexpiprazole for the treatment of acute schizophrenia: a 6-week randomized, double-blind, placebo-controlled trial. Am J Psychiatry. 2015;172(9):870–880. doi:10.1176/appi.ajp.2015.14101275
25. Kane J, Skuban A, Ouyang J, et al. A multicenter, randomized, double-blind, controlled Phase 3 trial of fixed-dose brexpiprazole for the treatment of adults with acute schizophrenia. Schizophr Res. 2015;164:127–135. doi:10.1016/j.schres.2015.01.038
26. Study to evaluate the efficacy, safety, and tolerability of oral OPC-34712 and aripiprazole for treatment of acute schizophrenia (STEP 203); 2015. Available from: https://www.clinicaltrials.gov/ct2/show/results/NCT00905307?term=NCT00905307.
27. Newcomer J, Meyer J, Baker R, et al. Changes in non-high-density lipoprotein cholesterol levels and triglyceride/high-density lipoprotein cholesterol ratios among patients randomized to aripiprazole versus olanzapine. Schizophr Res. 2008;106:300–307. doi:10.1016/j.schres.2008.09.002
28. Newcomer J, Eriksson H, Zhang P, Weiller E, Weiss C. Changes in metabolic parameters and body weight in brexpiprazole-treated patients with acute schizophrenia: pooled analyses of phase 3 clinical studies. Curr Med Res Opin. 2018;34(12):2197–2205. doi:10.1080/03007995.2018.1498779
29. Higgins J, Green S. Cochrane handbook for systematic reviews of interventions Version 5.1. 0 [updated March 2011]; 2012. Available from: http://wwwcochrane-handbookorg.
30. Moher D, Liberati A, Tetzlaff J, Altman D. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535. doi:10.1136/bmj.b2535
31. Kishi T, Oya K, Matsui Y, et al. Comparison of the efficacy and safety of 4 and 2 mg/day brexpiprazole for acute schizophrenia: a meta-analysis of double-blind, randomized placebo-controlled trials. Neuropsychiatr Dis Treat. 2018;14:2519–2530. doi:10.2147/ndt.s176676
32. Fleischhacker W, Kemmler G. The clinical relevance of percentage improvements on the PANSS score. Neuropsychopharmacology. 2007;32(11):2435–2436. doi:10.1038/sj.npp.1301391
33. Morosini P, Magliano L, Brambilla L, Ugolini S, Pioli R. Development, reliability and acceptability of a new version of the DSM-IV Social and Occupational Functioning Assessment Scale (SOFAS) to assess routine social functioning. Acta Psychiatr Scand. 2000;101(4):323–329. doi:10.1111/j.1600-0447.2000.tb10933.x
34. Gharabawi G, Bossie C, Turkoz I, Kujawa M, Mahmoud R, Simpson G. The impact of insight on functioning in patients with schizophrenia or schizoaffective disorder receiving risperidone long-acting injectable. J Nerv Ment Dis. 2007;195(12):976–982. doi:10.1097/NMD.0b013e31815c1982
35. Guy W. Manual for the ECDEU Assessment Battery.
36. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7(3):177–188. doi:10.1016/0197-2456(86)90046-2
37. Higgins J, Thompson S, Deeks J, Altman D. Statistical heterogeneity in systematic reviews of clinical trials: a critical appraisal of guidelines and practice. J Health Serv Res Policy. 2002;7(1):51–61. doi:10.1258/1355819021927674
38. Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539–1558. doi:10.1002/sim.1186
39. MacKenzie N, Kowalchuk C, Agarwal S, et al. Antipsychotics, metabolic adverse effects, and cognitive function in schizophrenia. Front psychiatr. 2018;9:622. doi:10.3389/fpsyt.2018.00622
40. Kao Y, Liu Y. Effects of age of onset on clinical characteristics in schizophrenia spectrum disorders. BMC psychiatr. 2010;10:63. doi:10.1186/1471-244x-10-63
41. Newcomer J. Metabolic considerations in the use of antipsychotic medications: a review of recent evidence. J Clin Psychiatry. 2007;4:20–27.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy of Vitamin C Supplementation on Chronic Obstructive Pulmonary Disease (COPD): A Systematic Review and Meta-Analysis
Lei T, Lu T, Yu H, Su X, Zhang C, Zhu L, Yang K, Liu J
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2201-2216
Published Date: 10 September 2022
Clinical Utility of Deucravacitinib for the Management of Moderate to Severe Plaque Psoriasis
Jin JQ, Spencer RK, Reddy V, Bhutani T, Liao W
Therapeutics and Clinical Risk Management 2023, 19:413-423
Published Date: 18 May 2023