Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
Efficacy and Safety of Acupoint Catgut Embedding for Obesity Associated with Polycystic Ovary Syndrome: A Qualitative and Quantitative Analysis
Authors Li XX, Hu ZY, Yuan DN, Zhao JX, Ma WB ![]() , Lan L
, Lan L
Received 15 July 2025
Accepted for publication 26 January 2026
Published 21 February 2026 Volume 2026:19 553787
DOI https://doi.org/10.2147/DMSO.S553787
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Liang Wang
Xing-xian Li,1 Zhuo-ya Hu,1 Dong-ni Yuan,1 Jun-xin Zhao,1 Wen-bin Ma,2 Lei Lan1
1Acupuncture and Tuina College, Chengdu University of Traditional Chinese Medicine, Chengdu, People’s Republic of China; 2School of Health and Rehabilitation, Chengdu University of Traditional Chinese Medicine, Chengdu, People’s Republic of China
Correspondence: Lei Lan, Email [email protected]
Aim: Obesity is common in women with polycystic ovary syndrome (PCOS) and can exacerbate PCOS symptoms. Although Acupoint catgut embedding (ACE) is frequently used to treat the clinical symptoms of simple obesity, it is unclear how it will affect obesity associated with PCOS. We conducted a systematic review and meta-analysis of randomized clinical trials (RCTs) to evaluate the effectiveness of ACE in treating obesity in women with PCOS.
Methods: We searched databases from inception to January 8, 2025. Two independent reviewers extracted data and assessed the risk of bias. All meta-analyses used random effects models, and the GRADE approach was used to assess the certainty of the evidence.
Results: We included 25 RCTs (1,663 participants). Based on usual care, compared to blank treatment, ACE probably reduces body mass index (BMI), waist-to-hip ratio (WHR), and waist circumference (WC), and may enable a greater proportion of patients to achieve a weight loss no less than 5% (relative risk [RR] 1.33, 95% CI 1.15 to 1.55) and may reduce triglycerides (TG). Furthermore, when compared to active comparators, ACE probably enables a greater proportion of patients to achieve a weight loss no less than 5% (RR 1.40, 95% CI 1.11 to 1.76) and reduces WC and may also reduce BMI and TG. All effects were supported by low to moderate certainty evidence.
Conclusion: When compared to blank treatment, on the basis of usual care, ACE for obesity associated with PCOS may improve obesity-related outcomes. When compared to active comparators, it may have comparable or greater therapeutic efficacy and fewer adverse events. Such improvements in obesity-related indicators may help alleviate metabolic and reproductive symptoms in women with PCOS. As all included trials were conducted in China, further high-quality studies in diverse populations are needed to confirm the generalizability of these findings.
Keywords: obesity, polycystic ovary syndrome, acupoint catgut embedding, meta-analysis
Introduction
Polycystic Ovary Syndrome (PCOS) is a prevalent endocrine disorder that affects 10% to 13% of women of reproductive age.1 It is characterized by hyperandrogenism, ovulatory dysfunction, and polycystic ovaries.2 Obesity is highly prevalent among women with PCOS, with estimates suggesting that 50% to 80% of the affected women are overweight or obese.3 The interplay between obesity and PCOS is complex, with obesity exacerbating the symptoms of PCOS and vice versa. Insulin resistance, a key feature of both conditions, plays a central role in this relationship.4 The INSR gene, which encodes the insulin receptor, is pivotal in this relationship. Genetic variations in INSR have been associated with high insulin levels, further aggravating the metabolic and hormonal imbalances observed in PCOS. These mutations likely disrupt insulin receptor function, impairing glucose metabolism and amplifying the symptoms of both obesity and PCOS.5 Pharmacological treatment of obesity in PCOS spots the improvement of weight loss and insulin sensitivity, involving Metformin, Liraglutide, Orlistat, and combined oral contraceptives.6–9 Despite the availability of several pharmacological options, challenges remain, including side effects, cost, and patient adherence. Long-term management is essential, but frequent relapses after discontinuation of treatment are common.3,8,10–12 Further treatment has to focus on alternative therapies with fewer side effects and better long-term efficacy.
Acupoint catgut embedding (ACE), an advanced technique rooted in Traditional Chinese Medicine (TCM), involves the precise insertion of biodegradable surgical catgut into designated acupoints. This method is intended to deliver a sustained, stable, and mild form of stimulation to the body, which can persist for several weeks to months.13 Among its numerous benefits, ACE stands out for its minimal side effects, robust stimulation, long-lasting therapeutic outcomes, and cost-effectiveness.14,15 These characteristics render it especially advantageous for the management of chronic conditions like PCOS when accompanied by obesity. The mechanisms of ACE are multifaceted and include the regulation of the hypothalamic-pituitary-ovarian axis, improvement of insulin resistance, reduction of inflammation, and modulation of intestinal flora.16 Compared to pharmacological treatments, which often necessitate ongoing medication and may result in a range of side effects from mild to severe, ACE provides an alternative with minimal side effects and long-lasting therapeutic outcomes. It has the potential to regulate hormonal imbalances, enhance insulin sensitivity, and assist in weight management without the associated adverse reactions.17 Systematic reviews have demonstrated the potential of ACE in mitigating the clinical symptoms of simple obesity.18 Despite growing clinical interest, the current evidence base remains limited by several factors. Most existing studies on ACE focus primarily on simple or abdominal obesity and exhibit considerable heterogeneity in acupoint selection, embedding materials, implantation depth, and treatment duration. Additionally, the overall quality of evidence varies substantially across studies.19,20 Moreover, the pathophysiology of PCOS-related obesity—characterized by insulin resistance, hyperandrogenism, and reproductive dysfunction—differs markedly from that of simple obesity, raising concerns about whether findings from general obesity studies can be directly extrapolated to PCOS populations. To bridge this gap, this systematic review and meta-analysis aim to assess the clinical efficacy of ACE for obesity associated with PCOS. By synthesizing the available evidence, this study endeavors to provide a comprehensive understanding of the therapeutic potential of ACE, thereby informing clinical practice and guiding future research.
Methods
Our systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement,21 (Supplement Table 1) and its protocol has been registered on PROSPERO (CRD42024521230). We made two changes to our protocol: (1) we added the proportion of participants reducing their bodyweight no less than 5% because a 5% reduction in baseline weight improves obesity-related metabolic risk factors and coexisting disorder4,22 and (2) we added subgroup analyses of ACE combined with different treatments.
Literature Search
From the establishment of the databases to March 3, 2024, and updated to January 8, 2025, several studies were identified through systematic literature retrieval from eight electronic literature databases, including PubMed, Cochrane Library, Embase, Web of Science, Chinese National Knowledge Infrastructure (CNKI), VIP Database for Chinese Technical Periodicals, Wan Fang, and Sinomed. (Supplement Table 2) Additionally, Clinical Trials.gov and the WHO International Clinical Trials Registry Platform (ICTRP) were searched. The search terms included polycystic ovary syndrome, obesity, and acupoint catgut embedding.
Study Selection
All retrieved literature was independently reviewed and screened by two reviewers (Dong-ni Yuan and Zhuo-ya Hu). First, the titles and abstracts were read to identify potentially eligible studies, followed by a full-text review to determine if they met the inclusion criteria. In case of any disagreement, a third reviewer (Xing-xian Li) was consulted for evaluation.
We included trials that: (1) Patients diagnosed with PCOS based on the 2003 Rotterdam criteria and who met the WHO Asia-Pacific obesity standard with a BMI ≥25 kg/m2, regardless of age, race, nationality, or course of disease. (2) Participants were randomly assigned to either a treatment group or a control group, where the treatment group included ACE monotherapy or combined with usual care, and the control group included usual care (including medication or lifestyle control). (3) Follow-up was conducted for at least three months or three menstrual cycles. (4) At least one of the outcome indicators was reported: bodyweight, body mass index (BMI), waist circumference (WC), waist-to-hip ratio (WHR), testosterone (T), homeostasis model assessment for insulin resistance (HOMA-IR), triglycerides (TG), or adverse events. We excluded: (1) Comparison of ACE with other acupuncture techniques or traditional Chinese medicine, and (2) Studies that did not use internationally standardized units for outcome measures.
Data Abstraction and Risk of Bias Assessment
Two reviewers (Dong-ni Yuan and Jun-xin Zhao) independently extracted data from all eligible trials. We collected information on study characteristics (including first author name, year of publication, funding source, study location, sample size, and length of follow-up), interventions, and all patient-important outcomes. When a study reported results at multiple time points, we selected the most commonly used time point in the eligible trials. We calculated the change data by comparing baseline data with outcome data to account for within-person variability.
Two reviewers (Dong-ni Yuan and Jun-xin Zhao) independently assessed the risk of bias using the modified Cochrane Risk of Bias Tool 1.0,23,24 including random sequence generation, allocation concealment, blinding of patients, health care providers, data collectors, outcome assessors, and data analysts, incomplete outcome data (missing data ≥20% indicating high risk of bias), and other potential sources of bias. For each item, the response options were scored as “definitely or probably yes” (assigned a low risk of bias) and “definitely or probably no” (assigned a high risk of bias). If there was a disagreement between reviewers, it would be resolved through a third party (Xing-xian Li).
Data Synthesis
For dichotomous outcomes, we calculated the relative risk (RR) and its corresponding 95% confidence interval (CI): the proportion of participants achieving a bodyweight reduction no less than 5% and adverse effects. In cases where the percentage change in body weight was not provided by the authors of the randomized controlled trials (RCTs), this information was approximated based on the reported data.25 For continuous outcomes, we calculated the weighted mean difference (WMD) and its corresponding 95% CI: (1) BMI, higher score indicated worse outcome; (2) WC, higher score indicated worse outcome; (3) WHR, higher score indicated worse outcome; (4) T, higher score indicated worse outcome; (5) TG, higher scores indicate worse outcomes; (6) HOMA-IR, higher score indicated worse outcome.
For all meta-analyses, we used a DerSimonian-Laird random effects model. The statistical heterogeneity across pooled estimates was evaluated using the Cochrane Q test and the I2 statistic, while subgroup analyses were conducted to explore potential sources of heterogeneity. In line with Cochrane guidelines, we interpreted I2 values as follows: 0% to 40% as “possibly not important”, 30% to 60% as “moderate heterogeneity”, 50% to 90% as “substantial heterogeneity”, and 75% to 100% as “considerable heterogeneity”.26 Data analysis was conducted using STATA software version 17 (Stata Corp, College Station, TX, USA). All comparisons were two-tailed using a threshold of p≤0.05.
Certainty of Evidence
We applied the GRADE (Grading of Recommendations, Assessment, Development, and Evaluation) method to assess the certainty of evidence for each outcome. Evidence can be downgraded from high to moderate, low, or very low certainty due to the risk of bias, consistency, directness, precision, and potential publication bias.27 We assessed publication bias through a visual assessment of funnel plot asymmetry only when a meta-analysis included at least 10 contributing studies.
Results
Search Results and Study Characteristics
We screened 3022 citations, and 25 trials involving a total of 1663 participants met the eligibility criteria.28–52 (Figure 1) All studies were conducted in China, and they were all single-center trials. Nine studies were funded by government,28,31–33,35,36,40,47,49 and sixteen without funding.29,30,34,37–39,41–46,48,50–52 Among 23 trials that reported age, the average age median of the patients was 26.09 years (IQR 23.02 to 29.40). The median of the average duration of condition was 35.52 months (IQR 22.01 to 56.70) among 22 trials reporting this information. Twenty-two trials compared ACE to blank treatment, on the basis of usual care,28–40,42–44,46,47,49–52 and five compared ACE to pharmacotherapy (including metformin,32,41,48 metformin and ethinylestradiol and cyproterone acetate tablets (EE/CPA),45 and drospirenone and ethinylestradiol tablets(II) (DRSP/EE(II))40 (Table 1).
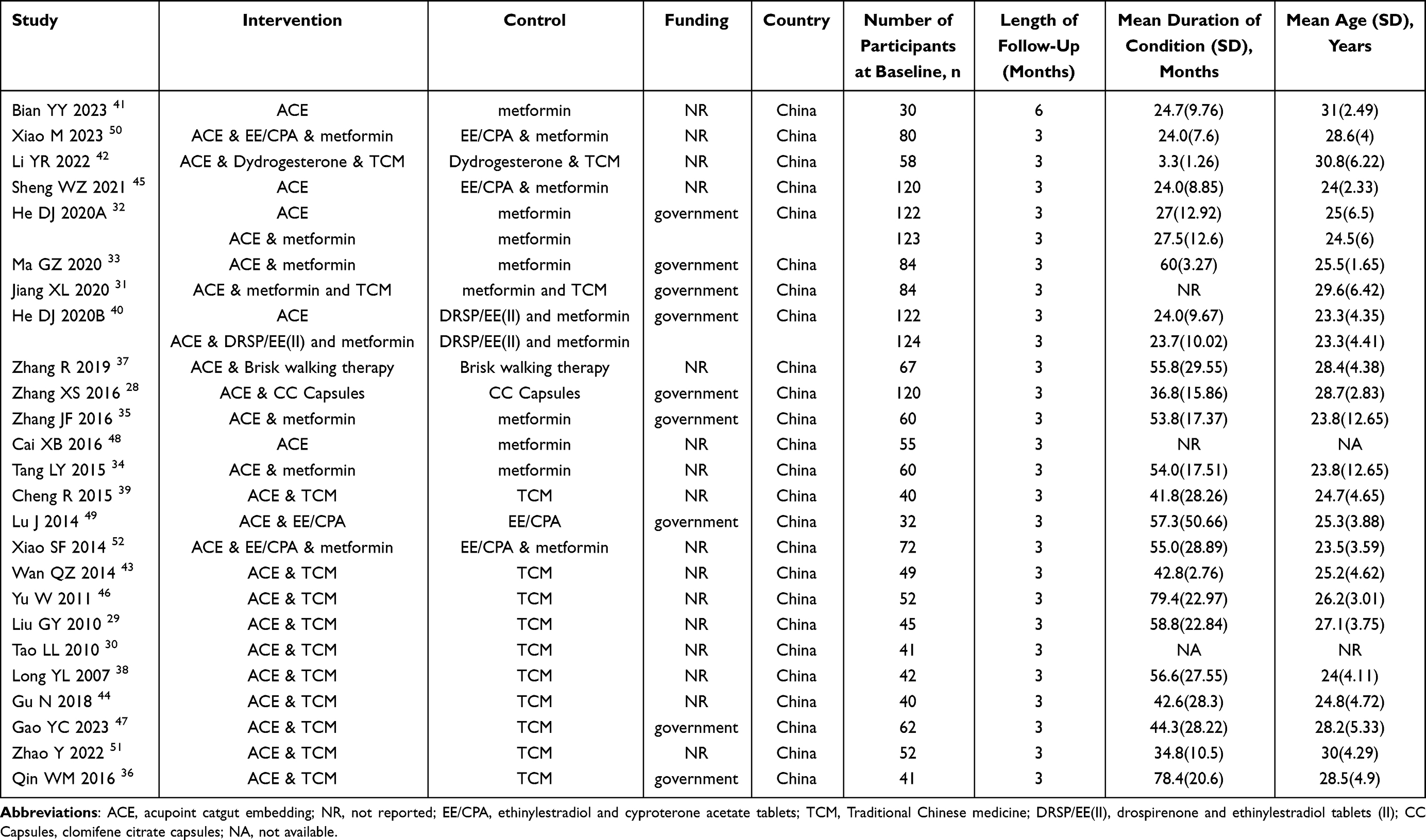 |
Table 1 Baseline Characteristics of Included Studies |
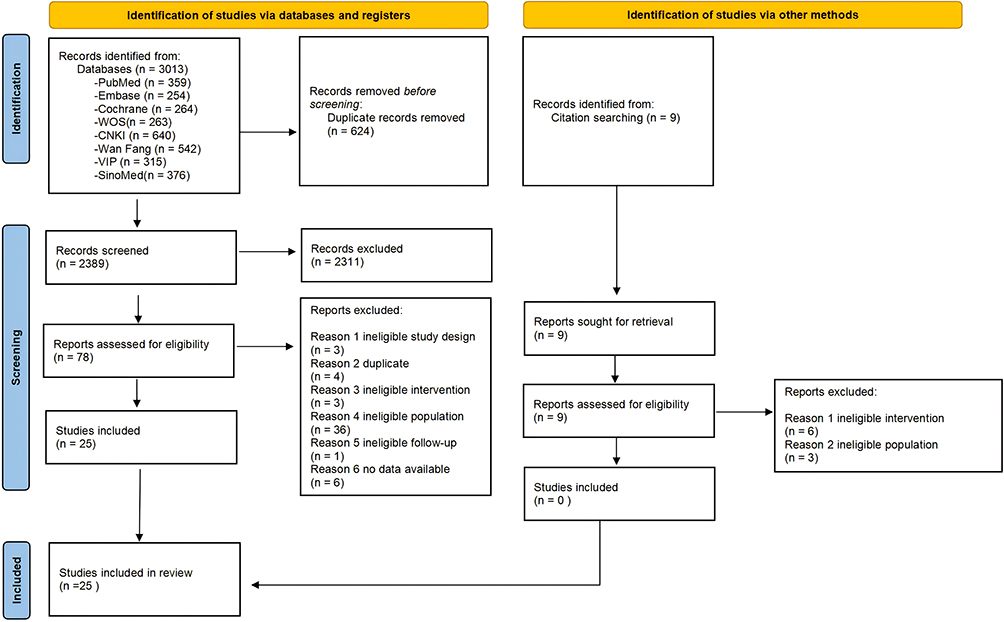 |
Figure 1 Flowchart of the search results and the selection details. |
Risk of Bias
Among the 25 eligible trials, 16 (64%) adequately generated randomization sequences. All trials were at high risk in at least one domain involving allocation concealment or blinding. One trial (4%) reported ≥20% missing outcome data (Supplement Table 3).
ACE vs Blank Treatment on the Basis of Usual Care
Bodyweight Reduction No Less Than 5%
Low certainty evidence from 5 trials (381 patients) shows that on the basis of usual care, compared to blank treatment, a greater proportion of patients who received ACE may reduce their bodyweight no less than 5% (RR 1.33, 95% CI 1.15 to 1.55; Table 2, Figure 2).37,40,42,46,50
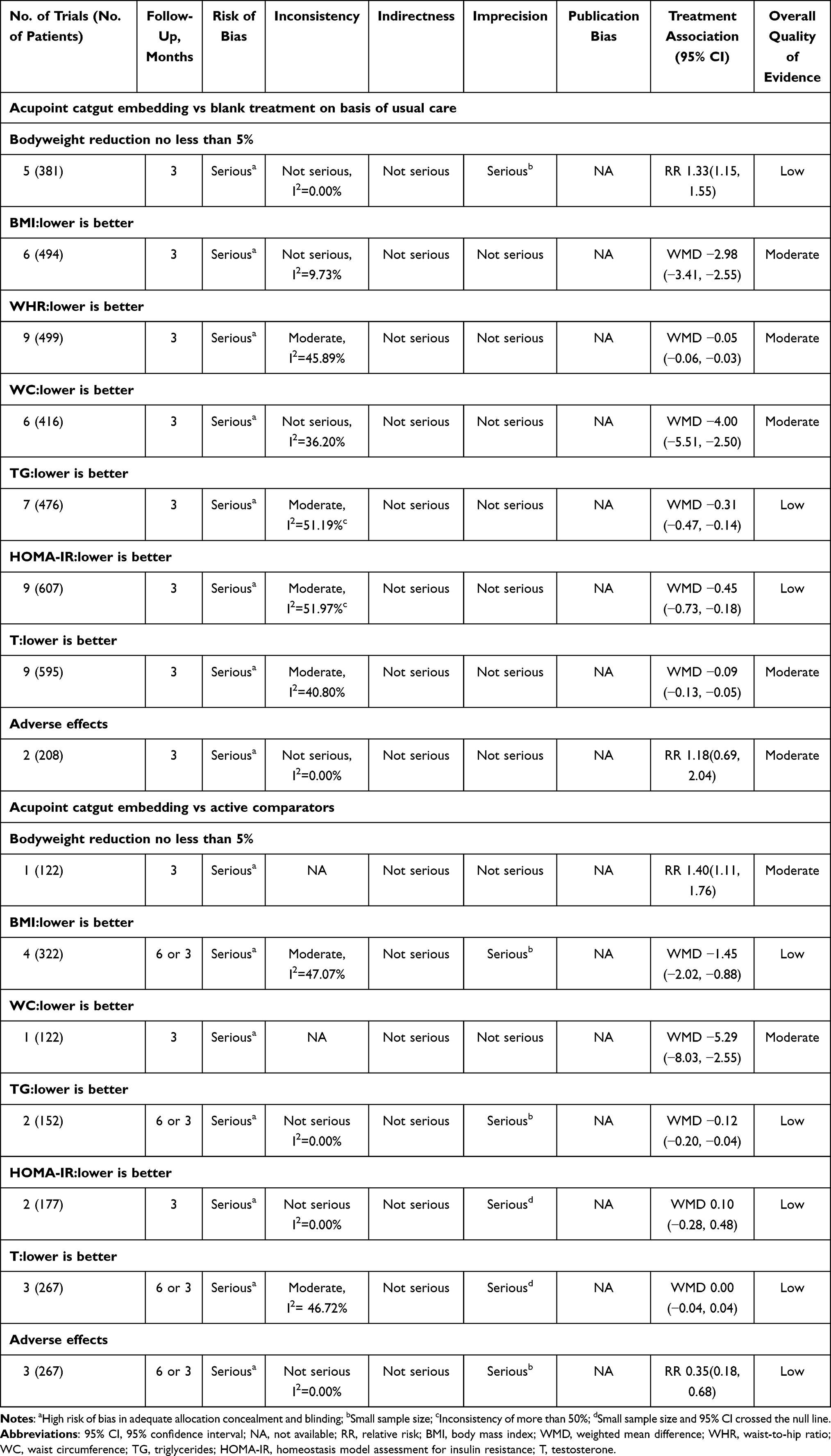 |
Table 2 Grade Evidence Profile of Acupoint Catgut Embedding for Obesity Associated with Polycystic Ovary Syndrome |
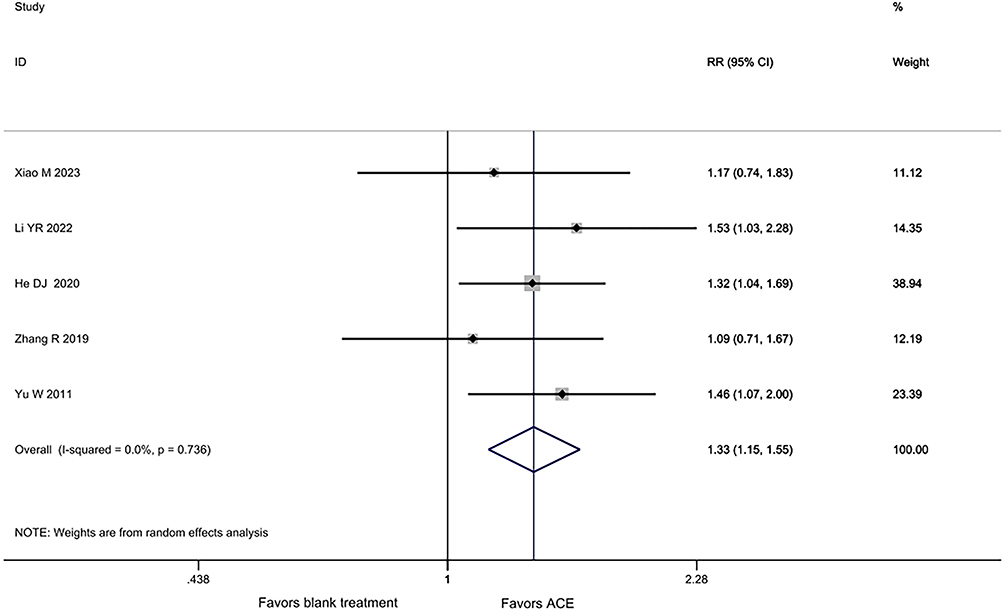 |
Figure 2 Bodyweight reduction no less than 5% among patients who received acupoint catgut embedding compared to blank treatment, on the basis of usual care. |
BMI
Moderate certainty evidence shows that compared to no treatment, patients who received ACE probably experience a greater BMI reduction on the basis of pharmacotherapy (6 trials, 494 patients, WMD −2.98, 95% CI −3.41 to −2.55),28,33,35,40,49,50 traditional Chinese herbs (10 trials, 443 patients, WMD −1.43, 95% CI −1.98 to −0.89),29,30,36,38,39,43,44,46,47,51 and the combination of pharmacotherapy, traditional Chinese herbs, and health instruction (1 trial, 58 patients, WMD −3.13, 95% CI −4.22 to −2.04).42 (Table 2, Figure 3).
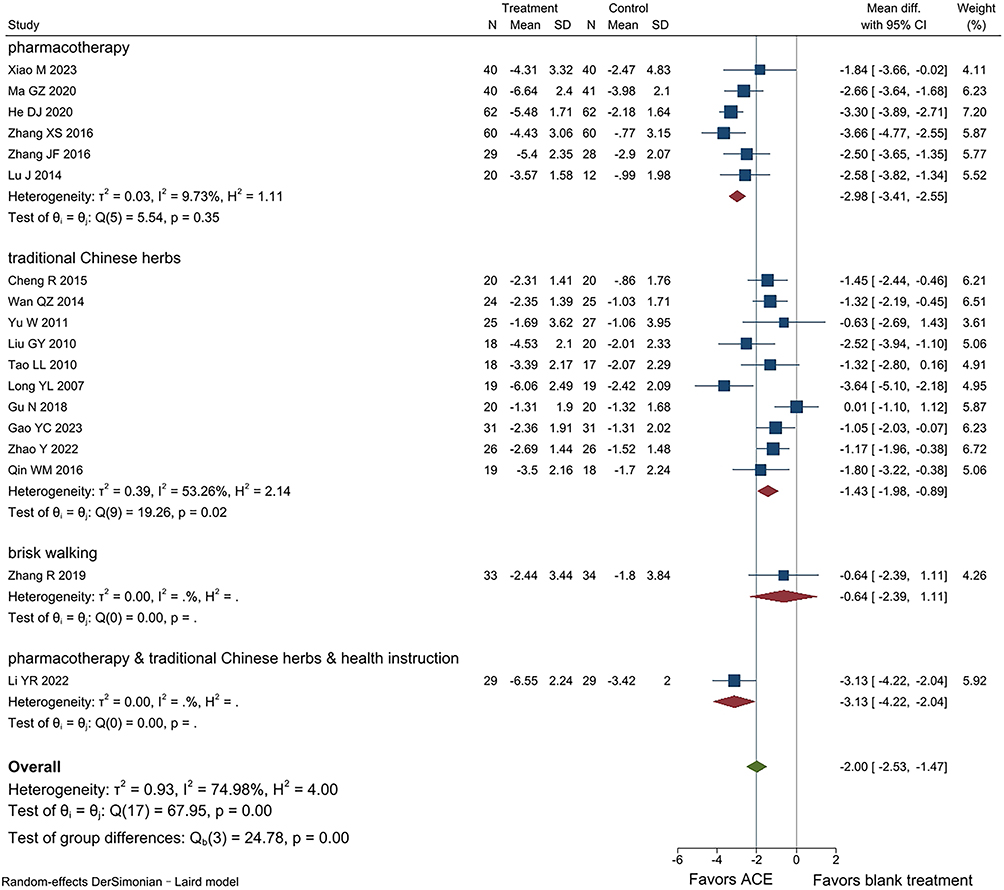 |
Figure 3 BMI among patients who received acupoint catgut embedding compared to blank treatment, on the basis of usual care. |
WHR
Moderate certainty evidence from 9 trials (499 patients) shows that on the basis of usual care, compared to blank treatment, patients who received ACE probably reduce WHR (WMD −0.05, 95% CI −0.06 to −0.03; Table 2, Figure 4). 36,37,39,40,42–44,49,51
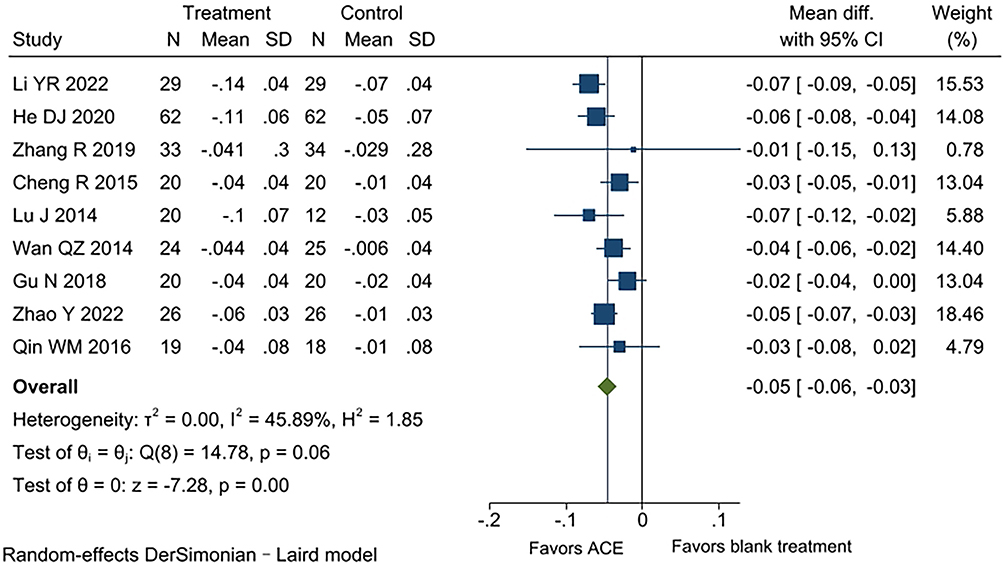 |
Figure 4 WHR among patients who received acupoint catgut embedding compared to blank treatment, on the basis of usual care. |
WC
Evidence from 7 trials (497 patients) shows that on the basis of usual care, compared to blank treatment, patients who received ACE may experience a greater WC reduction (I2= 63.58%).30,33,37,40,42,46,50 To explore the sources of heterogeneity, a sensitivity analysis was conducted using a stepwise exclusion approach. When Ma GZ 202033 was excluded, the heterogeneity significantly decreased (I2= 36.20%). This suggests that Ma GZ 202033 may be a source of heterogeneity. The study included participants under the age of 18, which may have contributed to the increased heterogeneity.
Moderate certainty evidence shows that, on the basis of usual care, compared to blank treatment, patients who received ACE probably experience a greater WC reduction (WMD −4.00 cm, 95% CI −5.51 to −2.50 cm; Table 2, Figure 5).
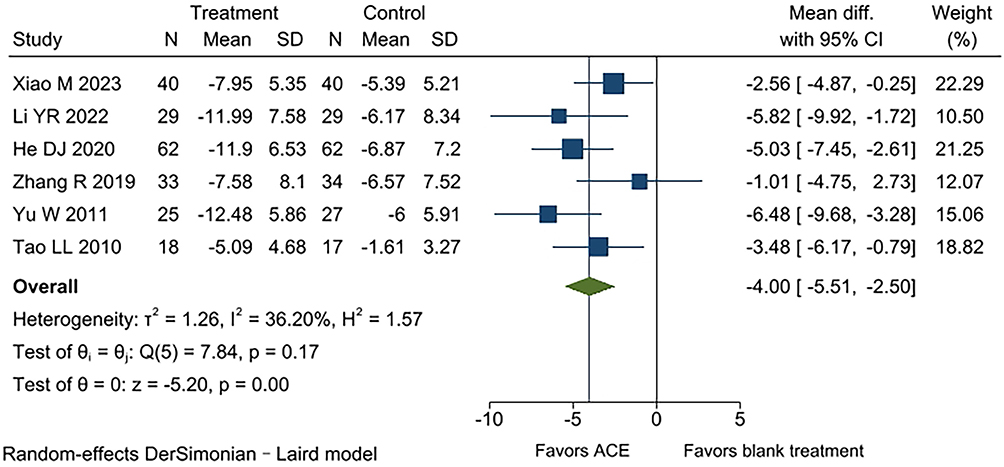 |
Figure 5 WC among patients who received acupoint catgut embedding compared to blank treatment, on the basis of usual care. |
TG
Low certainty evidence from 7 trials (476 patients) shows that on the basis of usual care, compared to blank treatment, patients who received ACE may experience a greater reduction in TG (WMD −0.31 mmol/L, 95% CI −0.47 to −0.14 mmol/L; Table 2, Supplement Figure 1).30,32,33,36,42,47,50
HOMA-IR
Low certainty evidence from 9 trials (607 patients) shows that, on the basis of usual care, compared to blank treatment, patients who received ACE may obtain a greater reduction in HOMA-IR (WMD −0.45, 95% CI −0.73 to −0.18; Supplement Figure 2).30–33,35,36,42,46,50
T
Moderate certainty evidence from 9 trials (595 patients) shows that on the basis of usual care, compared to blank treatment, patients who received ACE probably obtain a greater reduction in T (WMD −0.09 ng/mL, 95% CI −0.13 to −0.05 ng/mL; Table 2, Supplement Figure 3).28,29,38,40,43,46,47,49,50
Adverse Effects
Moderate certainty evidence from 2 trials (208 patients) shows that there is probably little to no difference in adverse effects between ACE and blank treatment on the basis of usual care. (RR 1.18, 95% CI 0.69 to 2.04 Table 2, Supplement Figure 4).31,40
ACE vs Active Comparators
The active comparators include metformin, metformin combined with EE/CPA, or DRSP/EE(II).
Bodyweight Reduction No Less Than 5%
Moderate certainty evidence from one trial (122 patients) suggests that compared to metformin and DRSP/EE(II), a greater proportion of patients who received ACE probably reduce their bodyweight no less than 5% (RR 1.40, 95% CI 1.11 to 1.76; Table 2). 40
BMI
Low certainty evidence from 4 trials (322 patients) suggests that, compared to active comparators, patients who received ACE may experience a greater reduction in BMI (WMD −1.45, 95% CI −2.02 to −0.88; Table 2, Figure 6). 40,41,45,48
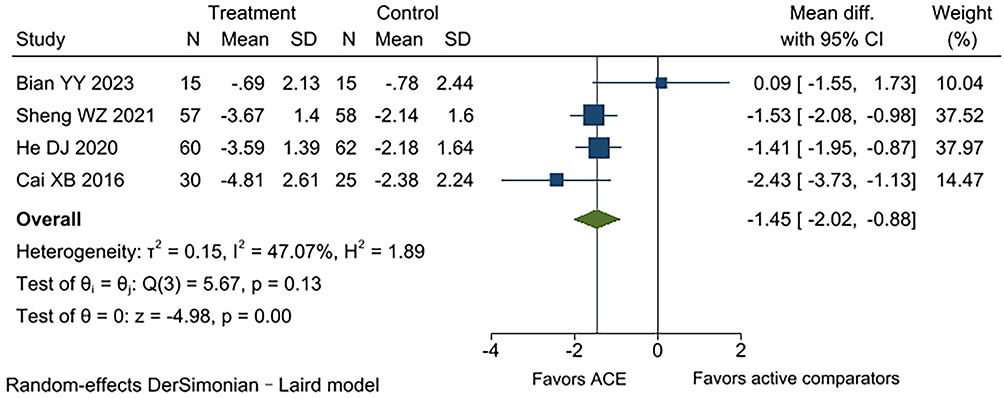 |
Figure 6 BMI among patients who received acupoint catgut embedding compared to active comparators. |
WHR
From one trial (122 patients) suggests that, compared to DRSP/EE(II) and metformin at 3 months of treatment, patients who received ACE may reduce WHR (WMD −0.04, 95% CI −0.06 to −0.02).40 From one trial (55 patients) suggests that, compared to metformin at 3 months of treatment, patients who received ACE may experience a greater reduction in WHR (WMD −0.11, 95% CI −0.14 to −0.08).48 From one trial (30 patients) suggests that, compared to metformin at 6 months of treatment, patients who received ACE may experience little to no difference in WHR (WMD 0.01, 95% CI −0.00 to 0.02).41
WC
Moderate certainty evidence from one trial (122 patients) suggests that compared to DRSP/EE(II) and metformin, patients who received ACE probably experience a greater reduction in WC (WMD −5.29 cm, 95% CI −8.03 to −2.55 cm; Table 2). 40
TG
Low certainty evidence from 2 trials (152 patients) suggests that, compared to metformin, patients who received ACE may obtain a reduction in TG (WMD −0.12 mmol/L, 95% CI −0.20 to −0.04 mmol/L; Table 2, Supplement Figure 5).32,41
HOMA-IR
Low certainty evidence from 2 trials (177 patients) suggests that, compared to metformin, patients who received ACE may experience little to no difference in HOMA-IR reduction (WMD 0.10, 95% CI −0.28 to 0.48; Table 2, Supplement Figure 6).32,48
T
Low certainty evidence from 3 trials (267 patients) suggests that, compared to active comparators, patients who received ACE may experience little to no difference in T reduction (WMD 0.00 ng/mL, 95% CI −0.04 to 0.04 ng/mL; Table 2, Supplement Figure 7).40,41,45
Adverse Effects
Low certainty evidence from 3 trials (267 patients) suggests that there may be fewer adverse effects when applying ACE compared to active comparators (RR 0.35, 95% CI 0.18 to 0.68; Table 2, Supplement Figure 8).40,41,45
Discussion
Overall Findings
On the basis of usual care, compared to blank treatment, patients who received ACE probably experience greater reductions in BMI, WHR, WC and T; and may experience a greater proportion of reducing their bodyweight no less than 5%, as well as reductions in TG and HOMA-IR. Compared to active comparators, patients who received ACE probably experience a greater proportion of reducing their bodyweight no less than 5% and a reduction in WC; in addition, these patients may experience reductions in BMI and TG, as well as fewer adverse effects, but may have little to no difference in reductions in HOMA-IR and T. All effects were supported by low to moderate certainty evidence.
Through subgroup analysis, we found that in reducing BMI, ACE may have varying effects in combination with different treatments, with the benefits of ACE being greater in the group combined with pharmacotherapy than in the group combined with traditional Chinese herbs.
Relation to Other Studies
There have been three previous systematic reviews of ACE for PCOS.53–55 We reviewed all the included studies, evaluated whether they were initially included, and the reasons to exclude them can be found in Supplement Table 4. However, their focus was solely on patients with PCOS, rather than those with obesity associated with PCOS. Therefore, there is still insufficient evidence to confirm the effectiveness of ACE in treating obesity associated with PCOS.
We evaluated the practical significance of ACE in managing obesity associated with PCOS and assessed the quality of evidence. Additionally, we included obesity-related outcomes such as bodyweight reduction no less than 5%, BMI, WHR, WC, and TG to objectively evaluate the clinical significance of ACE in treating obesity associated with PCOS.
Strengths and Limitations
Due to individual weight heterogeneity, the weight loss cannot explain the magnitude of clinical efficacy. Therefore, we converted the absolute value of bodyweight to the proportion of bodyweight reduction of no less than 5% as the primary outcome.
There are several limitations in this review. First, many of the studies only used the term “random” without specifying the allocation concealment or blinding, which may introduce the risk of bias. Second, we were unable to objectively assess the long-term effects of ACE, as only one study in the eligible literature had a follow-up period longer than three months, resulting in a lack of observation and tracking of long-term efficacy. Third, all of the included studies were conducted in China, which may limit the generalizability of the findings to other populations or regions.
Implications
Low to moderate certainty evidence suggests that, compared to blank treatment and active comparators, ACE may enable a greater proportion of patients to achieve a weight loss of 5% or more and may result in reductions in BMI, WC, and TG. Additionally, compared to active comparators, ACE may offer comparable therapeutic efficacy in terms of HOMA-IR, and T, while leading to fewer adverse effects. This suggests that ACE may provide better improvement in obesity, as well as obesity-related metabolic risk factors and coexisting diseases. PCOS and obesity form a vicious cycle; weight reduction can help alleviate metabolic and reproductive symptoms in women with PCOS. Reducing TG helps lower cardiometabolic risk in patients with obesity-related PCOS, while decreasing T is especially significant due to its impact on reproductive, metabolic, and dermatologic symptoms. Additionally, improved HOMA-IR reflects enhanced insulin sensitivity, which is crucial for reducing the risk of long-term metabolic complications like type 2 diabetes. And ACE may have varying effects in combination with different treatments. Therefore, attention should be paid not only to the efficacy of ACE as a standalone treatment but also to its role in different combination therapies, further optimizing clinical treatment protocols. However, these conclusions are based on moderate or low certainty evidence. Additionally, well-designed randomized controlled trials are necessary to clarify the role of ACE in managing obesity associated with PCOS. Trials should incorporate methodological safeguards to prevent bias, including rigorous scientific randomization methods, allocation concealment, and blinding, and patients should be followed up for at least 6 months (and ideally for 1 year). Future studies should also ensure adequate sample sizes, employ multicenter designs to improve the generalizability of findings, and adopt standardized outcome measures to facilitate comparability across trials.
Conclusion
In this systematic review and meta-analysis of RCTs of patients with obesity associated with PCOS, ACE probably reduces BMI, WHR, WC and T, and may enable a greater proportion of patients to achieve a weight loss no less than 5% and reduce TG and HOMA-IR, when compared with blank treatment, on the basis of usual care. Comparisons with active comparators suggest that ACE probably enables a greater proportion of patients to achieve a weight loss no less than 5% and reduces WC and may reduce BMI and TG and result in fewer adverse effects. However, as all findings are based on evidence of low to moderate certainty, these results should be interpreted with caution. Further large-scale, high-quality randomized controlled trials are needed to validate these findings.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, Lei Lan, upon reasonable request.
Acknowledgments
The authors especially thank the editors and reviewers for their valuable feedback, which significantly improved the quality of the paper.
Author Contributions
Xing-xian Li: Data curation, Formal analysis, Writing – original draft, Writing – review and editing. Lei Lan: Formal analysis, Writing – review and editing. Zhuo-ya Hu: Writing – original draft, Data curation. Dong-ni Yuan: Writing–original draft, Data curation. Jun-xin Zhao: Writing–original draft, Data curation. Wen-bin Ma: Writing–original draft, Data curation.
All authors gave final approval for the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This work was supported by the Sichuan provincial project (Grant No. 2022YFS0401) and Chengdu University of Traditional Chinese Medicine University-Institute Joint Innovation Fund (Grant No. LH202402049).
Disclosure
The authors declare that they have no conflict of interest.
References
1. Saadati S, Mason T, Godini R, et al. Metformin use in women with polycystic ovary syndrome (PCOS): opportunities, benefits, and clinical challenges. J Diabetes Obes Metab. 2025;27(Suppl 3):31–15. doi:10.1111/dom.16422
2. Legro RS, Arslanian SA, Ehrmann DA, et al. Diagnosis and treatment of polycystic ovary syndrome: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2013;98(12):4565–4592. doi:10.1210/jc.2013-2350
3. Hoeger KM, Dokras A, Piltonen T. Update on PCOS: consequences, challenges, and guiding treatment. J Clin Endocrinol Metab. 2021;106(3):e1071–e1083. doi:10.1210/clinem/dgaa839
4. Moran LJ, Pasquali R, Teede HJ, Hoeger KM, Norman RJ. Treatment of obesity in polycystic ovary syndrome: a position statement of the Androgen Excess and Polycystic Ovary Syndrome Society. Fertil Steril. 2009;92(6):1966–1982. doi:10.1016/j.fertnstert.2008.09.018
5. Rasheed RA, Rasheed PH, Ali AM. Metabolic and hormonal profiling in polycystic ovarian syndrome: insights into INSR gene variations. Mol Biol Rep. 2024;51(1):989. doi:10.1007/s11033-024-09924-5
6. Zeng X, Xie YJ, Liu YT, Long SL, Mo ZC. Polycystic ovarian syndrome: correlation between hyperandrogenism, insulin resistance and obesity. Clin Chim Acta. 2020;502:214–221. doi:10.1016/j.cca.2019.11.003
7. Yali Z. Efficacy analysis of da Diane-35 combined with metformin in the treatment of obese patients with polycystic ovary syndrome. Clin Res. 2021;29(08):95–97.
8. Glueck CJ, Goldenberg N. Characteristics of obesity in polycystic ovary syndrome: etiology, treatment, and genetics. Metabolism. 2019;92:108–120. doi:10.1016/j.metabol.2018.11.002
9. Goldberg A, Graca S, Liu J, et al. Anti-obesity pharmacological agents for polycystic ovary syndrome: a systematic review and meta-analysis to inform the 2023 international evidence-based guideline. Obes Rev. 2024;25(5):e13704. doi:10.1111/obr.13704
10. Xianying Z, Li Z, Zuyue S. Progress in the study of pharmacological mechanism of action of traditional Chinese medicines used in the treatment of polycystic ovary syndrome. China J Chinese Materia Medica. 2016;41(20):3715–3720. doi:10.4268/cjcmm20162003
11. Rashid R, Mir SA, Kareem O, et al. Polycystic ovarian syndrome-current pharmacotherapy and clinical implications. Taiwan J Obstet Gynecol. 2022;61(1):40–50. doi:10.1016/j.tjog.2021.11.009
12. Morley LC, Tang T, Yasmin E, Norman RJ, Balen AH. Insulin-sensitising drugs (metformin, rosiglitazone, pioglitazone, D-chiro-inositol) for women with polycystic ovary syndrome, oligo amenorrhoea and subfertility. Cochrane Database Syst Rev. 2017;11(11):Cd003053. doi:10.1002/14651858.CD003053.pub6
13. Yufan W, Hongyu Y. Research progress of weight loss in obesity-related polycystic ovary syndrome treated with traditional Chinese medicine. Xinjiang J Trad Chin Med. 2019;37(02):116–119.
14. Li Y, Zhou J, Wei Z, He X, Liang L, Sunzi K. The efficacy and safety of acupoint catgut embedding therapy for depression: a protocol for systematic review and meta-analysis. Front Psychiatry. 2023;14:1331780. doi:10.3389/fpsyt.2023.1331780
15. Zhang X, Li Q, Yi R, et al. Effect of acupoint catgut embedding for abdominally obese female with strong appetite: mixed analysis of a randomized clinical trial. Diabetes Metab Syndr Obes. 2022;15:3387–3395. doi:10.2147/dmso.S388485
16. Haoyu Z, Xuen L, Nenggui X, et al. Clinical application and mechanistic investigation of acupoint catgut embedding for obesity-type polycystic ovary syndrome. J Li-shizhen Trad Chin Med. 2022;33(03):359–661.
17. Wenjuan S, Taotao J, Guorong Y, Yang Z. Research progress on acupoint catgut embedding theory for obesity-related polycystic ovarian syndrome. World Chin Med. 2024;19(03):432–436.
18. JianQiong L, Xiang S, Ying C, LiChang L, ShengXu W. Clinical randomized controlled trials of acupoint catgut-embedding for simple obesity:a Meta-analysis. Chin Acupuncture Moxibustion. 2014;34(06):621–626. doi:10.13703/j.0255-2930.2014.06.033
19. Qifeng Z, Yuqiu L, Xiaoling W, et al. Research progress of acupoint catgut embedding in treating simple obesity in recent five years. J Clin Acupuncture Moxibustion. 2021;37(10):96–100.
20. Limei W, Binghe G, Wenxia G, et al. Overview of acupoint catgut embedding in the treatment of simple obesity. Chin Med Modern Distance Educ China. 2022;20(22):205–208.
21. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol. 2009;62(10):1006–1012. doi:10.1016/j.jclinepi.2009.06.005
22. Heymsfield SB, Wadden TA. Mechanisms, pathophysiology, and management of obesity. N Engl J Med. 2017;376(3):254–266. doi:10.1056/NEJMra1514009
23. Akl EA, Sun X, Busse JW, et al. Specific instructions for estimating unclearly reported blinding status in randomized trials were reliable and valid. J Clin Epidemiol. 2012;65(3):262–267. doi:10.1016/j.jclinepi.2011.04.015
24. Higgins JP, Altman DG, Gøtzsche PC, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011:
25. Shi Q, Wang Y, Hao Q, et al. Pharmacotherapy for adults with overweight and obesity: a systematic review and network meta-analysis of randomised controlled trials. Lancet. 2024;403(10434):e21–e31. doi:10.1016/s0140-6736(24)00351-9
26. Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions.
27. Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924–926. doi:10.1136/bmj.39489.470347.AD
28. Xueshu Z, Wenfang C, Hui Y. Treatment of polycystic ovary syndrome with clomiphene combined with water hole embedded wire: a randomized controlled study. J Chengdu Univ Trad Chin Med. 2016;39(01):67–70. doi:10.13593/j.cnki.51-1501/r.2016.01.067
29. Guiying L, Lili T, Jun X, Pengpeng X. The impact of thread-embedding and Chinese medicine on hyperandrogenism of obese patients with polycystic ovary syndrome. Liaoning J Trad Chin Med. 2010;37(10):2026–2028. doi:10.13192/j.ljtcm.2010.10.174.liugy.065
30. Lili T, Huiying W, Xiaoping C, et al. Effect of point thread-embedding plus herbal decoction for strengthening the spleen to dissolve Phlegm on the glucolipide metabolism of the obese patients with polycystic ovary syndrome. J Tradit Chin Med. 2010;51(03):239–242. doi:10.13288/j.11-2166/r.2010.03.019
31. Xiaolin J, Jing L, Yang Z, Chunli Z, Xiaoqian D, Lide Z. Effect of Cangfu Daotan decoction combined with point thread-embedding on immunity and intestinal Flo-ra in obese polycystic ovary syndrome. Clin Misdiagnosis Misther. 2020;33(08):51–56.
32. Danjuan H, Shaorong L, Man G, Lu W, Yaqin Y, Xiaotao H. Effect of acupoint thread-embedding combined with metformin on glucose and lipid metabolism in patients with obese polycystic ovary syndrome. Shanghai J Acupuncture Moxibustion. 2020;39(12):1516–1520. doi:10.13460/j.issn.1005-0957.2020.12.1516
33. Guizhi M, Zhihai H, Yin S, et al. Effect of acupoint thread-embedding combined with metformin on glucose and lipid metabolism in obese polycystic ovary syndrome patients. Shanghai J Acupuncture Moxibustion. 2020;39(09):1123–1127. doi:10.13460/j.issn.1005-0957.2020.09.1123
34. Liangying T, Ruicong H, Jianfeng Z. Effect of acupoint catgut embedding therapy on obesity type polycystic ovarian syndrome patients with sex hormone. Clin J Chinese Med. 2015;7(21):60–62.
35. Jianfeng Z, Ruicong H, Liangying T, Guangxian Z. Effect of acupoint catgut embedding therapy on blood glucose and insulin related index of patients with polycystic ovary syndrome. Guangming J Chin Med. 2016;31(06):831–833.
36. Qin W, Zhao K, Yang H. Effect of acupoint catgut embedding therapy combined with Chinese medicine for nourishing the kidneys and promoting blood circulation and improving blood glucose and lipid levels as well as the pregnancy rate in obese PCOS patients with infertility. Exp Ther Med. 2016;12(5):2909–2914. doi:10.3892/etm.2016.3715
37. Rui Z. Effect of Acupoint Catgut Embedding Combined with Aerobic Exercise on Body Weight in Patients with Phlegm-Damp Type Polycystic Ovary Syndrome (PCOS). Heilongjiang University of Chinese Medicine; 2019. doi:10.27127/d.cnki.ghlzu.2019.000094.
38. Yongling L. Effects of Acupuncture Therapy Combined Chinese Medicinal Herb on Insulin Resistance and Serum Adiponectin in Obese Polycystic Ovary Syndrome. Guangzhou University of Chinese Medicine; 2007.
39. Ru C, Qingzhi W, Jing O, Xiaosu Z. Curative observation on the effect of Chinese medicine combined with point embedding therapy in treating the women with polycystic ovary syndrome. J Liaoning Univ Traditional Chin Med. 2015;17(05):219–221. doi:10.13194/j.issn.1673-842x.2015.05.078
40. Danjuan H, Shaorong L, Xiaotao H. Clinical study on catgut embedding at acupoint in treatment of obese polycystic ovary syndrome. Hubei J Trad Chin Med. 2020;42(02):12–16.
41. Yunying B. Clinical Study of Chinese Medicine Combined with Acupoint Catgut Embedding in the Treatment of Obese Polycystic Ovary Syndrome. China Academy of Chinese Medical Sciences; 2023. doi:10.27658/d.cnki.gzzyy.2023.000267.
42. Yarui L. Clinical Study of Chinese and Western Medicine Combined with Acupoint Embedding Line for Obese PCOS with IR. Heilongjiang University of Chinese Medicine; 2022. doi:10.27127/d.cnki.ghlzu.2022.000512.
43. Qingzhi W. Clinical Research on Chinese Medicine of Eliminating Phlegm and Dampness Combined with Point Embedding Therapy in Treating Insulin Resistance of Obese Women with Polycystic Ovary Syndrome. Nanjing University of Chinese Medicine; 2014.
44. Na G, Xiaobin J. Clinical observation on treatment of obese polycystic ovary syndrome with catgut embedding at the waist and abdomen combined with tonifying kidney and resolving phlegm. Clin Lab J. 2018;7(03):410–412.
45. Whenzhen S. Clinical observation on Gua position combined with acupoint embedding in the treatment of obese polycystic ovary syndrome. Chin Med Modern Distance Educ China. 2021;19(04):87–90.
46. Wen Y. Clinical Observation of the Therapeutic Effect of Acupuncture Combined with Medicine on Polycystic Ovary Syndrome. Heilongjiang University of Chinese Medicine; 2011.
47. Yingchun G. Clinical observation of spleen-strengthening, kidney-tonifying, and turbidity-resolving formula combined with acupoint catgut embedding for treating obese polycystic ovary syndrome. New Mom New Born. 2023;64–66.
48. Xianbing C, Ya L, Junling W, Jian C. Clinical observation of electro-acupuncture and acupoint catgut-embedding therapy in the treatment of obese polycystic ovary syndrome. Guangming J Chin Med. 2016;31(04):538–541.
49. Jin L, Xiaosu Z, Xue Z, Huifen Z, Jing L, Cairong Z. Clinical observation of 20 cases of obese polycystic ovary syndrome treated with minimally invasive acupoint thread embedding combined with Diane-35. Jiangsu J Trad Chin Med. 2014;46(07):55–56.
50. Min X. Clinical Efficacy Analysis of Acupoint Embedding Combined with metformin in the Treatment of Phlegm-Damp Polycystic Ovary Syndrome Leading to Infertility. Shandong University of Traditional Chinese Medicine; 2023. doi:10.27282/d.cnki.gsdzu.2023.000057.
51. Yu Z. The clinical effectiveness of traditional Chinese medicine combined with acupuncture point thread embedding therapy in the treatment of polycystic ovary syndrome. Med Health. 2022;(2):82–84.
52. Shaofang X, Yiyong X, Lijuan Z, Julan H. Acupoint thread embedding combined with Diane and metformin in the treatment of 36 cases of obese polycystic ovary syndrome. Jiangxi J Trad Chin Med. 2014;45(04):53–55.
53. Min L, Qi C. Meta-analysis of acupoint catgut embedding combined with Diane-35 in the treatment of polycystic ovary syndrome. Maternal Child Health Care China. 2018;33(03):702–707.
54. Chaochao Y, Chaoyang M, Yuan X, et al. Effectiveness of acupoint catgut embedding therapy for polycystic ovary syndrome: a systematic review and meta-analysis. World J Acupuncture-Moxibustion. 2017;27(04):41–51. doi:10.1016/S1003-5257(18)30010-2
55. Kewei Q, Dongyun G, Chuyi Y. Meta-analysis of acupoint catgut embedding therapy for insulin resistance in polycystic ovary syndrome. Electronic J Practl Gynecol Endocrinol. 2020;7(34):51–52. doi:10.16484/j.cnki.issn2095-8803.2020.34.037
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Predictive Factors of Menstrual Recovery After Laparoscopic Sleeve Gastrectomy in Polycystic Ovary Syndrome Women with Obesity
Cai M, Zhang Y, Gao J, Dilimulati D, Bu L, Cheng X, Du L, Zhou D, Zhu J, Qu S, Zhang M
Diabetes, Metabolic Syndrome and Obesity 2023, 16:1755-1766
Published Date: 13 June 2023
Thyroid Hormones and Cardiometabolic Risk Factors in Saudi Women with Polycystic Ovary Syndrome: A Cross-Sectional Study
Saeed WM, Alsehli F
International Journal of Women's Health 2023, 15:1197-1203
Published Date: 26 July 2023
Effect of Consultation Number on the Assessment and Treatment of Polycystic Ovary Syndrome
Wang Y, Chen J, Dong H, Ma RL, Zou Y, Wang W, Zheng Q, Feng Y, Tan Z, Zeng X, Zhao Y, Deng Y, Wang Y, Gu B, Sun A
International Journal of Women's Health 2024, 16:527-541
Published Date: 25 March 2024
Association Between rs2278426 Polymorphism of the ANGPTL8 Gene and Polycystic Ovary Syndrome
Wu H, Wang H, Sun L, Liu M, Wang H, Sun X, Zhang W
Diabetes, Metabolic Syndrome and Obesity 2024, 17:1749-1760
Published Date: 16 April 2024
PCOS and Obesity: Contraception Challenges
Meczekalski B, Rasi M, Battipaglia C, Fidecicchi T, Bala G, Szeliga A, Luisi S, Genazzani AD
Open Access Journal of Contraception 2025, 16:43-58
Published Date: 5 May 2025