Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Predictive Factors of Menstrual Recovery After Laparoscopic Sleeve Gastrectomy in Polycystic Ovary Syndrome Women with Obesity
Authors Cai M, Zhang Y, Gao J, Dilimulati D, Bu L, Cheng X, Du L, Zhou D, Zhu J, Qu S ![]() , Zhang M
, Zhang M
Received 9 March 2023
Accepted for publication 1 June 2023
Published 13 June 2023 Volume 2023:16 Pages 1755—1766
DOI https://doi.org/10.2147/DMSO.S411573
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Antonio Brunetti
Meili Cai,1,* Yuqin Zhang,1,* Jingyang Gao,1,* Diliqingna Dilimulati,1 Le Bu,1,2 Xiaoyun Cheng,1,2 Lei Du,2,3 Donglei Zhou,2,3 Jiangfang Zhu,2,3 Shen Qu,1,2 Manna Zhang1,2
1Department of Endocrinology and Metabolism, Shanghai Tenth People’s Hospital, School of Medicine, Tongji University, Shanghai, 200072, People’s Republic of China; 2National Metabolic Management Center, Shanghai Tenth People’s Hospital, School of Medicine, Tongji University, Shanghai, 200072, People’s Republic of China; 3Department of Gastrointestinal Surgery, Shanghai Tenth People’s Hospital, School of Medicine, Tongji University, Shanghai, 200072, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shen Qu; Manna Zhang, Department of Endocrinology and Metabolism, Shanghai Tenth People’s Hospital, School of Medicine, Tongji University, 301 Middle Yanchang Road, Shanghai, 200072, People’s Republic of China, Tel +86-021-66301004, Email [email protected]; [email protected]
Objective: To explore the predictors of menstrual recovery in polycystic ovary syndrome (PCOS) women with obesity following laparoscopic sleeve gastrectomy (LSG).
Methods: A total of 88 PCOS patients with obesity and 76 control patients with obesity aged 18– 45 years were enrolled between May 2013 and December 2020. PCOS was diagnosed using the Rotterdam diagnostic criteria (2003). Anthropometric measurements, biochemical parameters, sex hormones, and circulating fibrinogen-like protein 1 (FGL-1) levels were collected before and six-month after LSG. The data on postoperative menstrual status, body weight, and fertility were obtained through telephone follow-ups for all individuals with PCOS.
Results: Patients with PCOS were followed up for at least six months after surgery, and the mean follow-up time was 3.23 years. At 6 months after LSG, circulating total testosterone (TT), calculated free testosterone (cFT), and FGL-1 levels declined significantly. The mean percent excess weight loss (%EWL) and percent total weight loss (%TWL) in PCOS patients at the final follow-up was 97.52% ± 33.90% and 31.65% ± 10.31%, respectively. The proportion of regular menstruation in PCOS patients significantly increased within six months (75.86% vs 0.03% at baseline). In the logistic regression analysis, time from PCOS diagnosis (P=0.007), body mass index (BMI) (P=0.007), TT (P=0.038) at baseline were demonstrated to be independent predictive factors for the regular menstruation in women with PCOS and obesity within 6 months after LSG.
Conclusion: In PCOS patients with obesity, time from PCOS diagnosis, BMI, and TT levels at baseline were independently and negatively associated with menstrual recovery within 6 months after LSG, which could be applied in preoperative evaluation.
Keywords: polycystic ovary syndrome, obesity, laparoscopic sleeve gastrectomy, menstruation, fibrinogen-like protein 1
Introduction
Polycystic ovary syndrome (PCOS) is a heterogeneous disease that causes infertility and ovulatory dysfunction in women of reproductive age. The Rotterdam criteria in 2003 recommended the diagnosis of PCOS be based on at least two of three features: 1) clinical or biochemical hyperandrogenism; 2) oligo-anovulation; 3) polycystic ovaries.1 Women of reproductive age are affected by PCOS at a rate of 6–20%.1,2 Moreover, women with PCOS are predisposed to metabolic syndrome, and 38–88% of them are overweight or obese.3 Multiple studies have found that obesity amplifies and worsens all aspects of metabolic and reproductive health in PCOS.4 Bariatric surgery, which is the most effective intervention for weight loss, has become an effective therapy for PCOS patients with obesity.5,6
Regular menstruation is an important indicator of the health of the female reproductive system and endocrine conditions.7,8 Previous studies have demonstrated that menstrual irregularities and long cycles are associated with an increased risk of type 2 diabetes (T2DM), gestational diabetes mellitus (GDM), and coronary heart disease.9–11 For women with PCOS, focusing on menstruation recovery is a vital symptom of improved ovulation function and an important sign of treatment effectiveness. Thus, changes in the menstrual status of PCOS patients with obesity must be investigated after bariatric surgery. Previous studies with relatively small sample sizes studies have reported that Roux-en-Y Gastric Bypass (RYGB) can reduce menstrual irregularities, ameliorate ovulatory dysfunction, and adjust the follicular phase length in women with obesity.12–14 However, few studies have regarded menstruation recovery as the primary endpoint in PCOS patients with obesity after laparoscopic sleeve gastrectomy (LSG),15–17 which is the most common bariatric surgery in China (> 90%) and worldwide (55.4%).18,19 Furthermore, the predictive factors for menstrual recovery in PCOS patients with obesity after bariatric surgery remain unknown. Thus, we hypothesized that some clinical indices at baseline may influence the recovery of menstruation in PCOS patients with obesity after LSG.
Therefore, this study aimed to investigate the predictive factors of regular menstruation in PCOS patients with obesity post-LSG. Our results may help clinicians to assess and understand the prognosis of patients with PCOS after LSG in terms of restored menstruation.
Methods and Materials
Ethics and Trial Registration
The study protocol complied with the Declaration of Helsinki for medical studies. The Ethics Committee of the Shanghai Tenth People’s Hospital approved the clinical research protocol of the study (approval number: SHSY-IEC-BG/05-08/04.1), which was registered at ClinicalTrials.gov Protocol Registration System (registration number: NCT05536583). All subjects signed an informed consent form before their data were published.
Study Design and Participants
This study enrolled 88 PCOS patients with obesity, as well as 76 age- and body mass index (BMI)-matched participants with normal menstrual cycles who were admitted to the Department of Endocrinology, Shanghai Tenth People’s Hospital, between May 2013 and December 2020 (Figure 1). All participants were aged 18–45 and were eligible for the indication of the Guidelines for Metabolic and Bariatric Surgery of Obesity and T2DM in China.19 The inclusion criteria were as follows: 1) aged 18–45 years; 2) BMI≥32.5 kg/m2 or BMI≥27.5 kg/m2 with waist circumference≥85 cm.15 Exclusion criteria included 1) pregnancy; 2) secondary obesity caused by endocrine disorders; 3) history of hysterectomy, bilateral oophorectomy and more than one bariatric procedure; 4) severe hepatic, renal or heart dysfunction; 5) mental illnesses or intellectual disability; 6) insufficient laboratory examination and 7) use of medications (including oral contraceptives, antiandrogens, hypoglycemic, glucagon-like peptide-1 receptor agonist and orlistat) within one month before the evaluation.
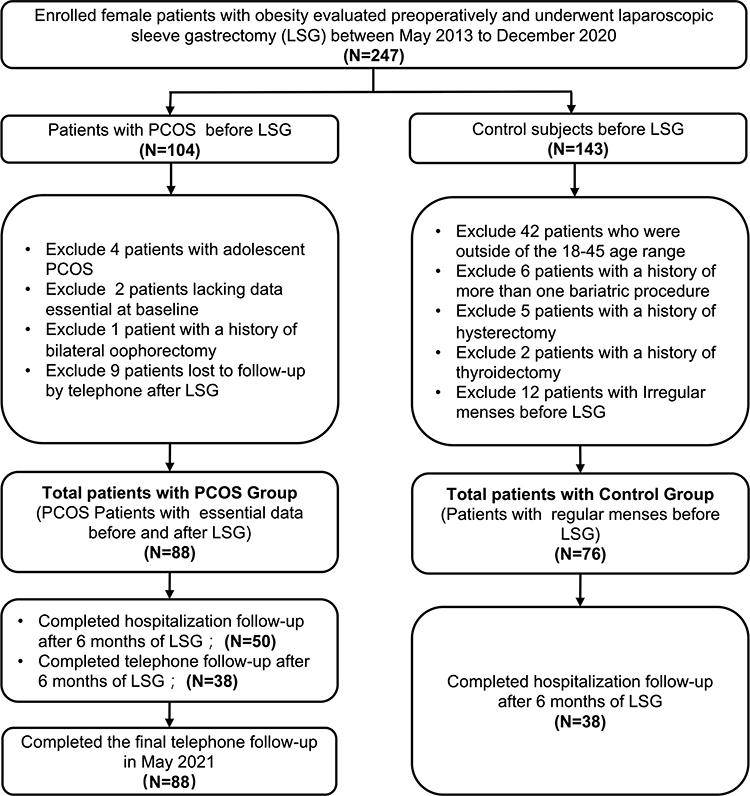 |
Figure 1 The flow diagram of patient recruitment, grouping, and follow-up process. |
PCOS was diagnosed using the Rotterdam diagnostic criteria (2003),20 which incorporate two of three characteristics: clinical or biochemical hyperandrogenism (Ferriman-Gallwey score≥8; total testosterone level>0.5 ng/mL), polycystic ovary morphology (PCOM) (≥12 ovaries with a diameter of 2–9 mm per ovary, or ovarian volume>10 cm3), and menstrual irregularities/ovulatory dysfunction. In accordance with the international evidence-based guidelines for PCOS, irregular menstrual cycles were defined as menstruation occurring outside the interval of 21 to 35 days or less than eight cycles per year.21 Among the control individuals, menstrual cycles were normal (21 days≤cycles≤35 days), there were no clinical or biochemical signs of hyperandrogenism, and gynecological ultrasound showed no signs of PCOM.
Bariatric Surgery and Follow-Up
Multidisciplinary team members (including endocrinologists, gastrointestinal surgeons, and nurses) assessed all hospitalized participants with obesity at baseline and six months after LSG. Hospitalization follow-up means that the subjects were hospitalized for face-to-face clinical and biochemical evaluation post-op follow-up. At the time of the final follow-up, telephone follow-up was conducted by trained endocrinology specialists to confirm, supplement, and track data (including postoperative menstrual status, weight loss, and fertility) in all participants with PCOS. Menstrual regularity within 6 months after LSG was defined as self-reported regular consecutive spontaneous (≥3 times) menstrual cycles (21 days≤cycles≤35 days) within 6 months, which continued to exist until the final follow-up time.22 The number of menstruations per year was defined as the absolute number of spontaneous menstruations within 12 months before the initial evaluation at the time of recruitment prior to LSG, 6 months after LSG, or the final follow-up after LSG.17
Anthropometric Parameters Evaluation
All patients underwent anthropometric measurements by trained endocrinology specialists on standard medical scales, including body weight, height, heart rate, systolic blood pressure (SBP), diastolic blood pressure (DBP), waist circumference, and hip circumference. The number of menstruations per year was defined as the absolute number of menstruations during one year. Based on the 2003 Rotterdam criteria, time from PCOS diagnosis refers to the entire disease process from the time of diagnosis in the women’s first clinical records. Preoperative hirsutism was assessed using the Ferriman-Gallwey score in each of the nine locations of the body by two trained endocrinology specialists.23 BMI was calculated by dividing the body weight (kg) by the square of the body height (m2). The waist-to-hip ratio (WHR) was calculated by dividing the waist circumference (cm) by the hip circumference (cm). After 6 months and at the final follow-up, the weight loss was measured by percent total weight loss (%TWL) and the percent excess weight loss (%EWL). The formula for %TWL was as follows: [(preoperative weight − last weight) / preoperative weight] ×100.24 The %EWL was calculated as follows: (preoperative weight–last weight) / (preoperative weight – ideal weight to produce a BMI of 25 kg/m2) × 100.25
Metabolic Parameter Measurement
Fasting morning blood samples were collected from all subjects after at least 10 h of overnight fasting, before and after surgery. Glycosylated hemoglobin (HbA1c), uric acid (UA), creatinine, alanine aminotransferase (ALT), aspartate aminotransferase (AST), total cholesterol (TC), triglyceride (TG), high-density lipoprotein cholesterol (HDL-c), and low-density lipoprotein cholesterol (LDL-c) levels were measured. Using a 75-g oral glucose tolerance test, fasting plasma glucose (FBG), fasting serum insulin (FINS), postprandial plasma glucose (PBG), and postprandial insulin (PINS) levels were measured at 0 and 120 min, respectively.26 The homeostasis model assessment of insulin resistance (HOMA-IR) was calculated as [FBG (mmol/L) × FINS (mU/L)] / 22.5.27
Hormone and Biochemical Parameters Assays
An immunochemiluminometric assay (Roche Diagnostics GmbH, Cot., Sandhofer, Mannheim, Germany) was used to determine the levels of luteinizing hormone (LH), follicle-stimulating hormone (FSH), total testosterone (TT), and sex hormone-binding globulin (SHBG). Circulating TT level was determined by the electrochemiluminescence immunoassay (Elecsys testosterone II), intra- and interassay CV≤20%, measurement range:0.025–15ng/mL. Free testosterone (cFT) was calculated according to the formula 24.00314 × [TT] / log10 [SHBG] 0.04599 × [TT]2.28 Circulating fibrinogen-like protein 1 (FGL-1) levels were determined using human FGL-1 enzyme-linked immunosorbent assay (ELISA) kits (CUSABIO, Wuhan, China; Catalog# CSB-E05071m).
Body Fat Distribution Measurement
Dual-energy X-ray absorptiometry (APEX 4.5.0.2, Hologic, USA) measurements offer a quick non-invasive estimation of the percentage of total body fat (%TBF), android fat mass, and visceral adipose tissue (VAT) mass. Abdominal subcutaneous adipose tissue (SAT) mass was determined by subtracting the VAT mass from the android fat mass.29
Statistical Analysis
SPSS (version 25.0) and GraphPad Prism (version 8.0) were used to perform all statistical analyses. Continuous data were presented as means and 95% confidence intervals (CI). Categorical variables were presented as percentages. Continuous data were compared between the two groups using an independent sample t-test. Qualitative variables were assessed using the chi-squared test. Spearman correlation test was used to analyze the association between the two indices. Logistic regression analysis was performed in the PCOS group to explore prognostic factors for predicting the recovery of regular menstrual cycles within 6 months after LSG. The logistic regression analyses included variables with P<0.05 in the correlation analysis. Statistical significance was set at P<0.05.
Results
Comparison of Baseline Characteristics in PCOS Patients and Controls
A flow diagram of the patient’s selection process is shown in Figure 1. Although age, BMI, and %TBF were comparable between patients with PCOS and controls, patients in the PCOS group had higher waist circumference, WHR, and VAT mass than those of patients in the control group (P<0.05). The mean number of menstruations per year and the HDL-c levels in the PCOS group were significantly lower than those in the control group (P<0.05). Moreover, patients in the PCOS group had higher HOMA-IR, FINS, PINS, UA, ALT, AST, TG, TT, and cFT levels than those in the control group (P<0.05). The LH/FSH and SHBG levels did not differ significantly between the two groups. PCOS patients had significantly higher circulating FGL-1 levels than control individuals at baseline (P<0.05) (Table 1).
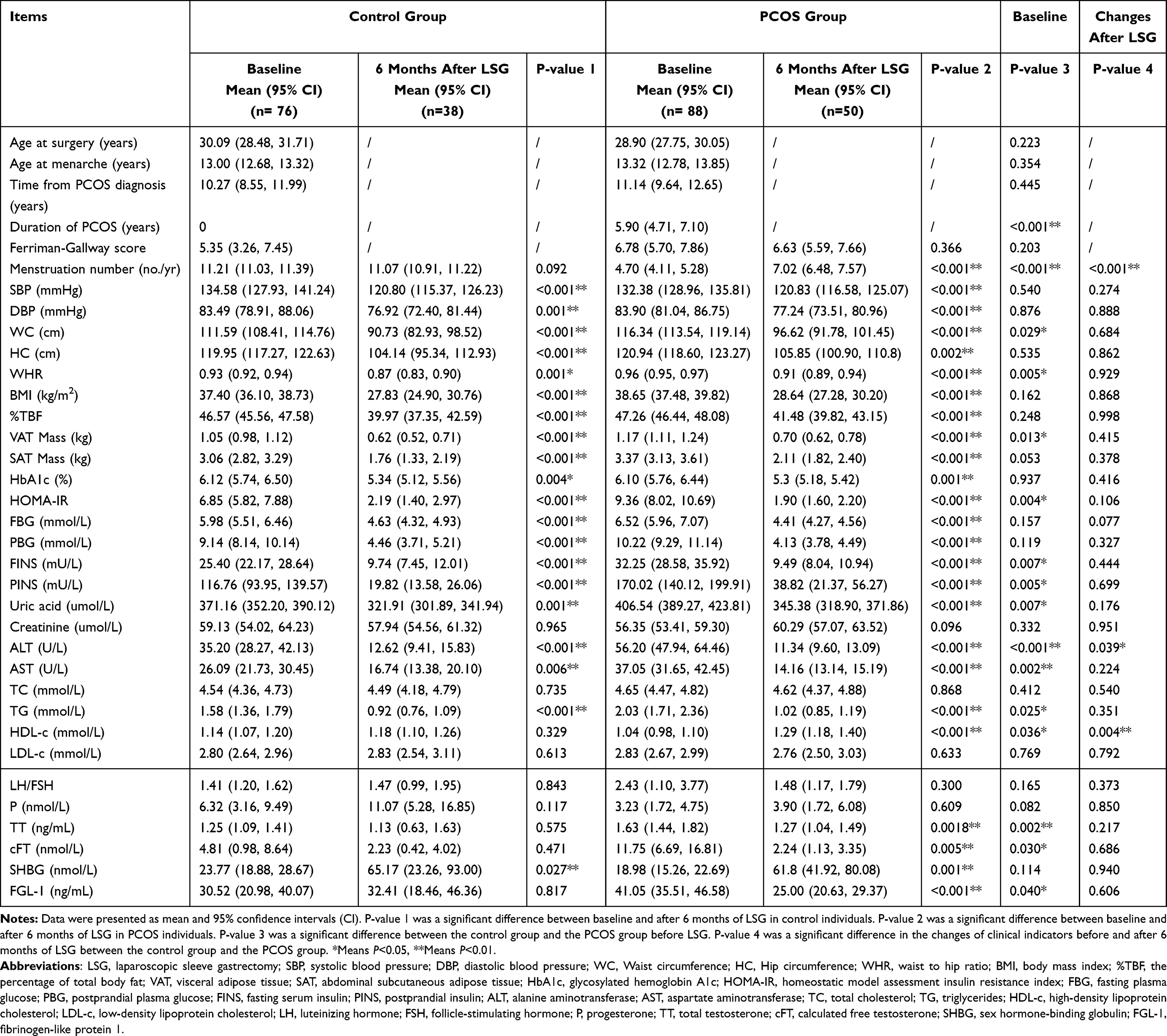 |
Table 1 Clinical and Biochemical Characteristics at Baseline and 6 Months Follow Up After LSG |
Comparison of Follow-Up Characteristics in Hospitalized Participants at 6 Months After LSG
At 6 months postoperatively (Table 1), significant improvements in SBP, DBP, waist circumference, hip circumference, WHR, BMI, %TBF, VAT Mass, SAT Mass, HbA1c, HOMA-IR, FPG, PBG, FINS, PINS, UA, ALT, AST, TG, and SHBG were observed both in PCOS and control individuals (P<0.05). In PCOS patients, the number of menstruations per year increased significantly from [4.70 (4.11, 5.28) to 7.02 (6.48, 7.57), P<0.001] after 6 months of LSG. Moreover, the circulating TT and cFT levels declined significantly from 1.63 (1.44, 1.82) ng/mL to 1.27 (1.04, 1.49) ng/mL and from 11.75 (6.69, 16.81) ng/mL to 2.24 (1.13, 3.35) ng/mL in patients with PCOS, respectively. The circulating FGL-1 levels declined significantly from 41.05 (35.51, 46.58) ng/mL to 25.00 (20.63, 29.37) ng/mL in PCOS patients. Serum HDL-c levels increased significantly in PCOS patients after 6 months of LSG (P<0.05). The changes in menstruation number and serum ALT and HDL-c levels differed significantly between the PCOS and control groups (P<0.05). However, no significant difference was observed in the changes in circulating TT, cFT, and FGL-1 levels between the PCOS and control subjects.
Changes in Menstrual Status, Fertility and Weight Loss in PCOS Patients with Obesity After LSG
All PCOS patients were followed-up at least six months after surgery, and the mean follow-up time was 3.23 years (range, 0.61–7.95 years). In the PCOS group, the number of menstruations per year improved significantly (4.70 [4.11, 5.28) vs 10.59 [10.13, 11.06], P<0.001) at the final follow-up after LSG (Figure 2A). The proportion of regular menstruation in PCOS patients with obesity significantly increased within six months (75.86%) and at the final follow-up (79.52%) after LSG (P<0.05) (Figure 2B). At the 6-month postoperative follow-up, no significant difference was observed in the number of menstruations per year in control subjects (11.21 [11.03, 11.39] to 11.07 [10.91, 11.22], P=0.092) (Table 1). Strikingly, 16.49% of individuals with PCOS had experienced menstruation within 7 days postoperatively. At the final follow-up, the spontaneous pregnancy, live birth, and miscarriage rates of PCOS patients were 19.31%, 17.04%, and 2.27%, respectively (data not shown).
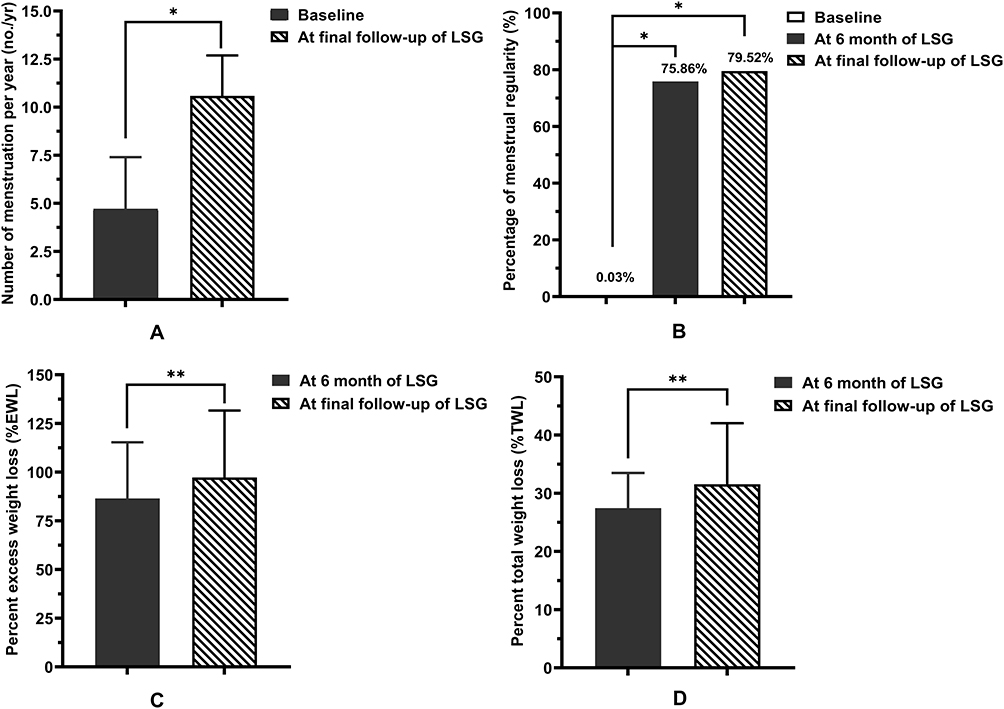 |
Figure 2 Menstrual status and weight loss in PCOS patients with obesity before and after LSG. (A) The number of menstrual cycles per year, (B) the percentage of menstrual regularity, (C) the percent excess weight loss (%EWL), and (D) the percent total weight loss (%TWL) levels at baseline and after LSG. Calculation of percent excess weight loss (%EWL) was done as follows: (preoperative weight–last weight) / (preoperative weight – ideal weight to produce BMI 25 kg/m2) × 100. ;Percent total weight loss (%TWL) was defined by the formula: (preoperative weight − last weight) / preoperative weight × 100. *means P<0.05, **means P<0.01. Abbreviation: LSG, Laparoscopic sleeve gastrectomy. |
At the 6-month postoperative follow-up, 88 PCOS patients with obesity retained a mean loss of 85.13±28.02% of their excess weight and 27.55± 6.21% of their total weight. Additionally, the mean %EWL and %TWL were 97.52±33.90% and 31.65± 10.31%, at the final follow-up (Figure 2C and D). In the Control group, patients with obesity retained mean %EWL and %TWL of 79.64±7.28% and 24.86± 1.76% at the 6-month follow-up postoperatively, respectively. The weight loss did not differ significantly between women with PCOS and controls at the 6-month follow-up (P>0.05) (data not shown).
Predictive Factors for Regular Menstruation in PCOS Patients with Obesity After LSG
Spearman correlation analysis indicated that time from PCOS diagnosis, duration of obesity, number of menstruations per year, BMI, HOMA-IR, and TT were significantly associated with the recovery of menstruation within 6 months after LSG (Supplementary Table 1). In the logistic regression analysis, time from PCOS diagnosis (odds ratios [OR]=0.811; 95% CI: 0.696–0.944, P=0.007), BMI (OR=0.839; 95% CI: 0.738–0.953, P=0.007), and TT (OR=0.377; 95% CI: 0.150–0.947, P=0.038) at baseline were independent predictive factors for recovery of menstruation within 6 months after LSG (Table 2). Even after adjusting for related confounders (including age, SBP, heart rate, AST, Fertility, and marital status), these indicators were still significantly associated with menstruation recovery 6 months postoperatively (Table 2). However, no association was observed between other clinical indicators (including Age, HbA1c, TC, TG, LDL-c, HDL-c, UA, LH/FSH, SHBG, FGL-1, and body fat composition) at baseline and regular menstruation status within six months after LSG.
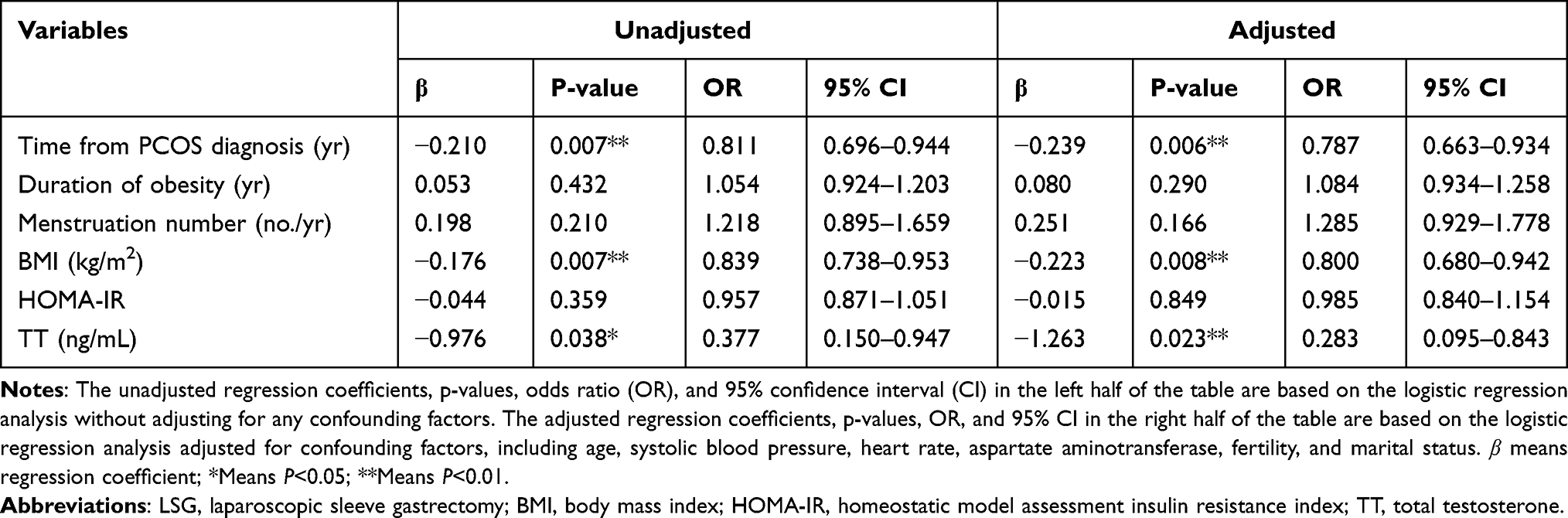 |
Table 2 Binary Logistic Regression Analysis of Variables at Baseline and Menstrual Status of PCOS Patients with Obesity Within 6 Months After LSG |
Discussion
PCOS is a common reproductive endocrine disease, and most PCOS patients have different degrees of insulin resistance, chronic inflammation, T2DM, and lipid dysfunction,1,30 all of which are exacerbated by obesity. As a specific manifestation of ovarian dysfunction, the recovery of the menstrual cycle is the primary goal of PCOS management.31 However, few studies have reported on the prognosis of menstrual status in patients with PCOS and obesity after LSG. To our knowledge, our study is the first to explore the predictive factors for regular menstruation in women with PCOS and obesity after LSG.
In our study, despite similar ages and BMIs between the PCOS and control groups, the PCOS group had a higher waist circumference, WHR, and VAT mass. The results generally corroborated those of previous studies revealing that PCOS patients tend to be more centrally obese than are patients without PCOS.32,33 In addition, PCOS patients with obesity had higher UA, severer insulin resistance, and lipid dysfunction than those of patients with regular menstruation and obesity at baseline, which is consistent with previous studies showing that PCOS patients with obesity demonstrate more severe metabolic abnormalities.34–36 FGL-1, as a hepatokine and adipokine, has an undeniably robust relationship with nonalcoholic fatty liver disease, obesity, insulin resistance, and T2DM.37,38 In line with our previous study, PCOS patients with obesity had significantly higher FGL-1 levels than those of patients without PCOS.39 Additionally, this study is the first to report that circulating FGL-1 levels in PCOS patients with obesity significantly decreased 6 months after LSG, although the changes in FGL-1 levels did not differ significantly in obese patients without PCOS. However, the underlying mechanism of this phenomenon remains unclear, which may be attributed to the close relationship between the circulating FGL-1 and obesity-related insulin resistance, and glucose and lipid metabolism dysfunction in patients with PCOS.37,39 Our results suggest that higher circulating FGL-1 levels in PCOS patients were associated with higher insulin resistance based on HOMA-IR, higher UA levels, higher TG levels, and lower HDL levels at baseline in this group compared with those in controls.
Regular menstruation is determined on the basis of the dynamic reproductive endocrine system, including ovarian events, hypothalamic-pituitary interactions, and changes in the endometrium and myometrium.40 Therefore, menstrual recovery is an easily ascertainable external parameter to improve ovarian function. Therefore, the menstrual status of women with PCOS and obesity must be determined after LSG. The menstrual status in the PCOS group after LSG was tracked via hospitalization and telephone interviews in the present study, the median follow-up time was 3.23 years. Our data revealed that 75.86% of PCOS patients with obesity recovered from regular menstrual cycles within 6 months after LSG, which was comparable to the data reported by previous studies.15,41 Notably, 24.66% of patients in the PCOS group experienced their first menstruation within 7 days after LSG. However, the underlying mechanism of this phenomenon is unclear, which may be attributed to changes in gastrointestinal hormones, insulin resistance, and the hypothalamic-pituitary-adrenal axis immediately after LSG.42,43 A systematic review and Meta-analysis revealed that pregnancy rates ranged from 95.2% to 100% after bariatric surgery in PCOS patients with obesity, which is inconsistent with our studies (the spontaneous pregnancy and live birth rates of PCOS subjects were 19.31% and 17.04%, respectively).44 This may be due to the different marital statuses and fertility intentions of women with PCOS and obesity.
Further analyses were performed to explore the predictive factors for the regularity of menstrual cycles in PCOS patients with obesity after LSG. Our data revealed that time from PCOS diagnosis and BMI were independent predictors for recovering regular menstrual cycles within 6 months after LSG. These findings suggest that a shorter time from PCOS diagnosis or lower BMI at baseline is associated with a greater likelihood of resumption of menses in PCOS patients with obesity after LSG. Growing evidence has demonstrated that hyperandrogenemia is significantly associated with long and irregular menstruation in women with PCOS,45,46 and ovarian hyperandrogenism can inhibit folliculogenesis and lead to polyfollicular morphology.47,48 In accordance with previous studies, our findings indicate that a high circulating TT level was an independent risk factor for the restoration of menstrual regularity in PCOS patients with obesity after LSG. This phenomenon may be explained by the fact that hyperandrogenism greatly improves after LSG in PCOS patients with obesity, which contributes to menstrual recovery in these patients. Large-sample multicenter studies are needed to verify this relationship in women with PCOS and obesity after LSG.
Although the correlation analysis indicated that the duration of obesity and the number of menstruations per year were associated with recovery of menstruation within 6 months following LSG, the association vanished after adjustment for other confounding factors. There was no correlation between other clinical features (age, HbA1c, TC, TG, LDL-c, HDL-c, UA, LH/FSH, SHBG, FGL-1, and body fat composition) and the recovery of menstrual cycles in PCOS patients with obesity after LSG. These results suggest that these clinical indicators may have a limited effect on menstruation recovery after LSG. The %TWL and %EWL of PCOS patients with obesity had no significant correlation with menstruation recovery at 6 months after LSG in the present study (data not shown), which was consistent with the results of a previous prospective study.15 This clinical study observed the complete PCOS remission rate (requiring six consecutive regular menstruation cycles or spring pregnancy) in 45 PCOS patients with obesity (mean age=28.7 years, mean BMI=35.6 kg/m2) after 12 months of LSG. The results revealed that the %TWL in the complete remission group showed no significant difference in the non-remission group (34.3 [27.5–39.8] vs 30.1 [26.3–38.7], P>0.05) after 12 months of LSG.
This study had some limitations: Firstly, for non-hospitalized participants with PCOS, menstrual status and body weight were self-reported, which might have resulted in a recall bias. Telephone follow-up to assess menstrual recovery may lack accuracy. Secondly, the measurement of circulating TT level using immunochemiluminometric assay instead of high-performance liquid chromatography-mass spectrometry (HPLC-MS) may lack sensitivity. Lastly, the predictive factors identified in this study have not been verified in other populations, and future studies need to involve larger populations of PCOS patients with obesity to confirm the accuracy and generalizability of our findings.
Conclusions
In a Chinese population of PCOS patients with obesity, the frequency of regular menstrual cycles could be greatly improved after LSG. Time from PCOS diagnosis, BMI, and TT at baseline were independent predictive factors for recovering menstrual cycles in PCOS patients with obesity within 6 months after LSG, which will help clinicians to assess the prognosis of PCOS patients after LSG in terms of restored menstruation.
Data Sharing Statement
All data supporting the conclusions of this article in this study are included in this article without undue reservation.
Acknowledgments
The study could not have been conducted without the participation of these patients. It is supported by grants from the National Key R&D Program of China (No.2018YFC1314100), the National Nature Science Foundation of China (No. 82170861 and No.81970677), and the Clinical Research Plan of SHDC (No. SHDC2020CR1017B).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Escobar-Morreale HF. Polycystic ovary syndrome: definition, aetiology, diagnosis and treatment. Nat Rev Endocrinol. 2018;14(5):270–284. doi:10.1038/nrendo.2018.24
2. Stener-Victorin E, Deng Q. Epigenetic inheritance of polycystic ovary syndrome - challenges and opportunities for treatment. Nat Rev Endocrinol. 2021;17(9):521–533. doi:10.1038/s41574-021-00517-x
3. Barber TM, Franks S. Obesity and polycystic ovary syndrome. Clin Endocrino. 2021;95(4):531–541. doi:10.1111/cen.14421
4. Glueck CJ, Goldenberg N. Characteristics of obesity in polycystic ovary syndrome: etiology, treatment, and genetics. Metabolism. 2019;92:108–120. doi:10.1016/j.metabol.2018.11.002
5. Christ JP, Falcone T. Bariatric surgery improves hyperandrogenism, menstrual irregularities, and metabolic dysfunction among women with polycystic ovary syndrome (PCOS). Obes Surg. 2018;28(8):2171–2177. doi:10.1007/s11695-018-3155-6
6. Tian Z, Zhang YC, Wang Y, Chang XH, Zhu HL, Zhao Y. Effects of bariatric surgery on patients with obesity and polycystic ovary syndrome: a meta-analysis. Surg Obes Relat Dis. 2021;17(8):1399–1408. doi:10.1016/j.soard.2021.04.009
7. Mihm M, Gangooly S, Muttukrishna S. The normal menstrual cycle in women. Anim Reprod Sci. 2011;124(3–4):229–236. doi:10.1016/j.anireprosci.2010.08.030
8. Messinis IE, Messini CI, Dafopoulos K. Novel aspects of the endocrinology of the menstrual cycle. Reprod Biomed Online. 2014;28(6):714–722. doi:10.1016/j.rbmo.2014.02.003
9. Rostami Dovom M, Ramezani Tehrani F, Djalalinia S, Cheraghi L, Behboudi Gandavani S, Azizi F. Menstrual cycle irregularity and metabolic disorders: a population-based prospective study. PLoS One. 2016;11(12):e0168402. doi:10.1371/journal.pone.0168402
10. Wang YX, Wang S, Mitsunami M, et al. Pre-pregnancy menstrual cycle regularity and length and the risk of gestational diabetes mellitus: prospective cohort study. Diabetologia. 2021;64(11):2415–2424. doi:10.1007/s00125-021-05531-2
11. Thong EP, Codner E, Laven JSE, Teede H. Diabetes: a metabolic and reproductive disorder in women. Lancet Diabetes Endocrinol. 2020;8(2):134–149. doi:10.1016/S2213-8587(19)30345-6
12. Jamal M, Gunay Y, Capper A, Eid A, Heitshusen D, Samuel I. Roux-en-Y gastric bypass ameliorates polycystic ovary syndrome and dramatically improves conception rates: a 9-year analysis. Surg Obes Relat Dis. 2012;8(4):440–444. doi:10.1016/j.soard.2011.09.022
13. Turkmen S, Ahangari A, Bäckstrom T. Roux-en-Y gastric bypass surgery in patients with polycystic ovary syndrome and metabolic syndrome. Obes Surg. 2016;26(1):111–118. doi:10.1007/s11695-015-1729-0
14. Eid GM, Cottam DR, Velcu LM, et al. Effective treatment of polycystic ovarian syndrome with Roux-en-Y gastric bypass. Surg Obes Relat Dis. 2005;1(2):77–80. doi:10.1016/j.soard.2005.02.008
15. Hu L, Ma L, Xia X, et al. Efficacy of bariatric surgery in the treatment of women with obesity and polycystic ovary syndrome. J Clin Endocrinol Metab. 2022;107(8):e3217–e3229. doi:10.1210/clinem/dgac294
16. Lv B, Xing C, He B. Effects of bariatric surgery on the menstruation- and reproductive-related hormones of women with obesity without polycystic ovary syndrome: a systematic review and meta-analysis. Surg Obes Relat Dis. 2022;18(1):148–160. doi:10.1016/j.soard.2021.09.008
17. Różańska-Walędziak A, Bartnik P, Kacperczyk-Bartnik J, Czajkowski K, Walędziak M. The impact of bariatric surgery on menstrual abnormalities-a cross-sectional study. Obes Surg. 2020;30(11):4505–4509. doi:10.1007/s11695-020-04840-6
18. Wilson R, Aminian A, Tahrani AA. Metabolic surgery: a clinical update. Diabetes Obes Metab. 2021;23:63–83. doi:10.1111/dom.14235
19. Du Y, Zhang J, Chen G, Sun Z. Formulation and interpretation of the Chinese guidelines for surgical treatment of obesity and type 2 diabetes mellitus. Biosci Trends. 2021;15(5):299–304. doi:10.5582/bst.2021.01287
20. The Rotterdam ESHRE/ASRM-sponsored PCOS consensus workshop group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Hum Reprod. 2004;19(1):41–47. doi:10.1093/humrep/deh098
21. Teede HJ, Misso ML, Costello MF, et al. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Fertil Steril. 2018;110(3):364–379. doi:10.1016/j.fertnstert.2018.05.004
22. Misra M, Prabhakaran R, Miller KK, et al. Weight gain and restoration of menses as predictors of bone mineral density change in adolescent girls with anorexia nervosa-1. J Clin Endocrinol Metab. 2008;93(4):1231–1237. doi:10.1210/jc.2007-1434
23. Rosenfield RL. Hirsutism. N Engl J Med. 2011;353:2578–2588. doi:10.1056/NEJMcp033496
24. Carandina S, Soprani A, Zulian V, Cady J. Long-term results of one anastomosis gastric bypass: a single center experience with a minimum follow-up of 10 years. Obes Surg. 2021;31(8):3468–3475. doi:10.1007/s11695-021-05455-1
25. O’Brien PE, Hindle A, Brennan L, et al. Long-Term outcomes after bariatric surgery: a systematic review and meta-analysis of weight loss at 10 or more years for all bariatric procedures and a single-centre review of 20-year outcomes after adjustable gastric banding. Obes Surg. 2019;29(1):3–14. doi:10.1007/s11695-018-3525-0
26. Yang W, Liu J, Shan Z, et al. Acarbose compared with metformin as initial therapy in patients with newly diagnosed type 2 diabetes: an open-label, non-inferiority randomized trial. Lancet Diabetes. 2014;2:46–55. doi:10.1016/S2213-8587(13)70021-4
27. Lin SY, Li WC, Yang TA, et al. Optimal threshold of homeostasis model assessment of insulin resistance to identify metabolic syndrome in a Chinese population aged 45 years or younger. Front Endocrinol (Lausanne). 2022;12:746747. doi:10.3389/fendo.2021.746747
28. Keelan JA, Mattes E, Tan H, et al. Androgen concentrations in umbilical cord blood and their association with maternal, fetal and obstetric factors. PLoS One. 2012;7(8):e42827. doi:10.1371/journal.pone.0042827
29. Dhaliwal R, Shepherd JA, El Ghormli L, et al. Changes in visceral and subcutaneous fat in youth with type 2 diabetes in the TODAY study. Diabetes Care. 2019;42(8):1549–1559. doi:10.2337/dc18-1935
30. Dabravolski SA, Nikiforov NG, Eid AH, et al. Mitochondrial dysfunction and chronic inflammation in polycystic ovary syndrome. Int J Mol Sci. 2021;22(8):3923. doi:10.3390/ijms22083923
31. Balen AH, Morley LC, Misso M, et al. The management of anovulatory infertility in women with polycystic ovary syndrome: an analysis of the evidence to support the development of global WHO guidance. Hum Reprod Update. 2016;22(6):687–708. doi:10.1093/humupd/dmw025
32. Pazderska A, Kyaw Tun T, Phelan N, et al. In women with PCOS, waist circumference is a better surrogate of glucose and lipid metabolism than disease status per se. Clin Endocrinol. 2018;88(4):565–574. doi:10.1111/cen.13542
33. Cai M, Gao J, Du L, et al. The changes in body composition in obese patients with polycystic ovary syndrome after laparoscopic sleeve gastrectomy: a 12-month follow-up. Obes Surg. 2021;31(9):4055–4063. doi:10.1007/s11695-021-05496-6
34. Mu L, Pan J, Yang L, et al. Association between the prevalence of hyperuricemia and reproductive hormones in polycystic ovary syndrome. Reprod Biol Endocrinol. 2018;16(1):104. doi:10.1186/s12958-018-0419-x
35. Wekker V, van Dammen L, Koning A, et al. Long-term cardiometabolic disease risk in women with PCOS: a systematic review and meta-analysis. Hum Reprod Update. 2020;26(6):942–960. doi:10.1093/humupd/dmaa029
36. Zhuang C, Luo X, Wang W, Sun R, Qi M, Yu J. Cardiovascular risk according to body mass index in women of reproductive age with polycystic ovary syndrome: a systematic review and meta-analysis. Front Cardiovasc Med. 2022;9:822079. doi:10.3389/fcvm.2022.822079
37. Liu XH, Qi LW, Alolga RN, Liu Q. Implication of the hepatokine, fibrinogen-like protein 1 in liver diseases, metabolic disorders and cancer: the need to harness its full potential. Int J Biol Sci. 2022;18(1):292–300. doi:10.7150/ijbs.66834
38. Dilimulati D, Du L, Huang X, et al. Serum fibrinogen-like protein 1 levels in obese patients before and after laparoscopic sleeve gastrectomy: a six-month longitudinal study. Diabetes Metab Syndr Obes. 2022;15:2511–2520. doi:10.2147/DMSO.S374011
39. Zhang Y, Dilimulati D, Chen D, et al. Serum fibrinogen-like protein 1 as a novel biomarker in polycystic ovary syndrome: a case-control study. J Endocrinol Invest. 2022;45(11):2123–2130. doi:10.1007/s40618-022-01844-0
40. Richards JS. The ovarian cycle. Vitam Horm. 2018;107:1–25. doi:10.1016/bs.vh.2018.01.009
41. Li YJ, Han Y, He B. Effects of bariatric surgery on obese polycystic ovary syndrome: a systematic review and meta-analysis. Surg Obes Relat Dis. 2019;15(6):942–950. doi:10.1016/j.soard.2019.03.032
42. Martinou E, Stefanova I, Iosif E, Angelidi AM. Neurohormonal Changes in the Gut-Brain Axis and Underlying Neuroendocrine Mechanisms following Bariatric Surgery. Int J Mol Sci. 2022;23(6):3339. doi:10.3390/ijms23063339
43. Moffett RC, Naughton V. Emerging role of GIP and related gut hormones in fertility and PCOS. Peptides. 2020;125:170233. doi:10.1016/j.peptides.2019.170233
44. Yue W, Huang X, Zhang W, et al. Metabolic Surgery on Patients with Polycystic Ovary Syndrome: a Systematic Review and Meta-Analysis. Front Endocrinol (Lausanne). 2022;13:848947. doi:10.3389/fendo.2022.848947
45. Goodman NF, Cobin RH, Futterweit W, et al. American Association of Clinical Endocrinologists, American College of Endocrinology, and Androgen Excess and Pcos Society Disease State Clinical Review: Guide to the Best Practices in the Evaluation and Treatment of Polycystic Ovary Syndrome--Part 1. Endocr Pract. 2015;21(11):1291–1300. doi:10.4158/EP15748.DSC
46. Zhang D, Gao J, Liu X, Qin H, Wu X. Effect of three androgen indexes (FAI, FT, and TT) on clinical, biochemical, and fertility outcomes in women with polycystic ovary syndrome. Reprod Sci. 2021;28(3):775–784. doi:10.1007/s43032-020-00316-1
47. Rosenfield RL, Ehrmann DA. The pathogenesis of polycystic ovary syndrome (PCOS): the hypothesis of PCOS as functional ovarian hyperandrogenism revisited. Endocr Rev. 2016;37(5):467–520. doi:10.1210/er.2015-1104
48. Yang Z, Zhou W, Zhou C, et al. Steroid metabolome profiling of follicular fluid in normo- and hyperandrogenic women with polycystic ovary syndrome. J Steroid Biochem Mol Biol. 2021;206:105806. doi:10.1016/j.jsbmb.2020.105806
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Long-Term Weight Loss Outcome of Laparoscopic Sleeve Gastrectomy Predicted by the Percentage of Excess Weight Loss at 6 Months in Chinese Patients with Body Mass Index ≥ 32.5 Kg/m2
Wang L, Tian C, Xu G, Sang Q, Chen G, Yu C, Wuyun Q, Wang Z, Chen W, Amin B, Wang D, Lian D, Zhang N
Diabetes, Metabolic Syndrome and Obesity 2022, 15:2235-2247
Published Date: 29 July 2022
Serum Fibrinogen-Like Protein 1 Levels in Obese Patients Before and After Laparoscopic Sleeve Gastrectomy: A Six-Month Longitudinal Study
Dilimulati D, Du L, Huang X, Jayachandran M, Cai M, Zhang Y, Zhou D, Zhu J, Su L, Zhang M, Qu S
Diabetes, Metabolic Syndrome and Obesity 2022, 15:2511-2520
Published Date: 17 August 2022
Thyroid Hormones and Cardiometabolic Risk Factors in Saudi Women with Polycystic Ovary Syndrome: A Cross-Sectional Study
Saeed WM, Alsehli F
International Journal of Women's Health 2023, 15:1197-1203
Published Date: 26 July 2023
Association Between rs2278426 Polymorphism of the ANGPTL8 Gene and Polycystic Ovary Syndrome
Wu H, Wang H, Sun L, Liu M, Wang H, Sun X, Zhang W
Diabetes, Metabolic Syndrome and Obesity 2024, 17:1749-1760
Published Date: 16 April 2024
PCOS and Obesity: Contraception Challenges
Meczekalski B, Rasi M, Battipaglia C, Fidecicchi T, Bala G, Szeliga A, Luisi S, Genazzani AD
Open Access Journal of Contraception 2025, 16:43-58
Published Date: 5 May 2025