Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Effects on Exercise Tolerance and Functional Outcomes of Eccentric versus Concentric Aerobic Exercise in People with COPD: A Systematic Review and Meta-Analysis
Authors Magunagoikoetxea-Comins G, Jiménez- García ME, Pérez-Ferreiro M, Fernandez-Pardo TE ![]()
Received 9 August 2025
Accepted for publication 14 November 2025
Published 18 December 2025 Volume 2025:20 Pages 4061—4078
DOI https://doi.org/10.2147/COPD.S558167
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Vanesa Bellou
Garbiñe Magunagoikoetxea-Comins,1 María Encarnación Jiménez- García,1 Monica Pérez-Ferreiro,1 Teresa E Fernandez-Pardo1,2
1Physiotherapy Department, Ramón y Cajal University Hospital, Madrid, Spain; 2Faculty of Medicine, Health and Sports, Department of Physiotherapy, Villaviciosa de Odón, Madrid, 28670, Spain
Correspondence: María Encarnación Jiménez- García, Email [email protected]
Introduction and Objectives: Chronic obstructive pulmonary disease (COPD) is associated with peripheral muscle weakness, dyspnoea and decreased exercise tolerance. Eccentric aerobic exercise (ECC), characterised by contractions during muscle stretching, is becoming an alternative to concentric aerobic exercise (CON) in this population, due to its reduced cardiorespiratory demand. The main objective of this systematic review, following the PRISMA criteria, is to determine the benefits of ECC versus CON on exercise tolerance in people with COPD.
Methods: A literature search was conducted in PubMed, Cochrane, Google Scholar and PEDro databases until March 2025. Only randomised controlled trials published in the last 10 years and with exercise tolerance and functional outcomes analysed were included.
Results: Six randomised controlled trials were included (n=154), with good methodological quality (PEDro 6– 7) and moderate certainty of evidence. The ECC showed benefits compared to CON in improvement of quadriceps strength (− 0.15 [− 0.51, 0.22] p=0.43); reduction of dyspnoea (− 0.74 [− 1.15, − 0.34] p < 0.001) and lower limb fatigue (− 2.29, p < 0.001), a higher work rate (− 0.48 [− 1.07, 0.12] p =0.12), improvements in Timed Up and Go (TUG) (− 2.03 [− 2.90, − 0.16] p< 0.001) and decrease heart rate (− 14.37 [− 18.24, − 10.50] p < 0.01), suggesting increased cardiorespiratory efficiency. In contrast, the CON showed an improvement in endurance time (1.05 [0.45, 1.64] p< 0.01) and oxygen saturation (1.79 [0.62, − 2.97] p < 0.01) (IC 95%).
Conclusion: ECC is presented as an effective and safe strategy to improve exercise tolerance in people with COPD in terms of saturation, dyspnoea, fatigue and heart rate, while CON improves endurance time. However, further studies are required to confirm its long-term functional benefits and its applicability in other pathologies and also treatment protocols are needed to standardize the use of eccentric exercise.
Keywords: aerobic exercise, eccentric, COPD, downhill
A Letter to the Editor has been published for this article.
Introduction
Chronic obstructive pulmonary disease (COPD) is a respiratory condition characterized by persistent symptoms such as dyspnoea, cough, and sputum production, along with clinical events such as exacerbations, caused by alterations in the airways and alveoli, resulting in progressive airflow obstruction.1 This disease not only impacts lung function, but also is associated with extrapulmonary comorbidities, such as peripheral muscle dysfunction, which contribute to a poorer prognosis.2 In particular, muscle weakness in the lower limbs limits mobility and promotes sedentary behavior, aggravating functional performance and quality of life. This deterioration perpetuates a negative spiral of functional decline that can culminate in severe disability.3–5
COPD also represents a significant challenge for healthcare systems. In the European Union, COPD-related costs amount to €38.6 billion annually, equivalent to 56% of the budget allocated to respiratory diseases.6 The prevalence and morbidity of COPD continue to increase due to smoking, population ageing, and environmental pollution.7 In fact, it is estimated that by 2030 COPD will be one of the leading causes of death worldwide.8
Pulmonary rehabilitation is the cornerstone of non-pharmacological management of COPD and has been shown to improve dyspnoea, exercise capacity, and quality of life across all severity stages.5,9,10 However, the high intensity required to induce muscular adaptations with traditional concentric exercise (CON), such as cycling on a regular bicycle or walking uphill, may not be tolerated by people with severe COPD due to dyspnoea and early lower limb fatigue, thus limiting its effectiveness.11 This limitation highlights the need for modalities that can induce peripheral muscle adaptations with lower ventilatory and metabolic demands,5,12 a role in which eccentric exercise (ECC) may be particularly advantageous.13,14
Considering these limitations, ECC, characterized by muscle lengthening during contraction,15 emerges as a promising alternative. In clinical practice, ECC can be implemented through different strategies, such as downhill walking15–17 or specialized ECC bicycles, where the pedals are moved in reverse by an electric motor while the person applies resistance to maintain a predetermined pedaling cadence.18–20
Thanks to its higher efficiency, ECC allows for significant improvements in muscle power with a metabolic and cardiorespiratory demand four to five times lower than that of CON.13,14 Furthermore, it has the potential to increase muscle strength and mass without exacerbating dyspnoea, making it an attractive option for people with severe COPD.14 However, although its safety and tolerability have been demonstrated in preliminary studies, there is still limited evidence regarding its effectiveness compared with conventional exercise in pulmonary rehabilitation programs.13,14,21,22
Beyond COPD, ECC has been shown to improve muscle strength and functional performance in older adults,23 in people with neurological conditions,24,25 and in individuals with coronary artery disease, inducing improvements in maximal capacity similar to CON, but with lower cardiorespiratory demands.26,27 This reflects greater energy efficiency, which may be particularly relevant for individuals with reduced energetic reserves. Taken together, these findings suggest a potential for translating ECC into COPD rehabilitation programs.
The aim of this systematic review is to analyze the effects of eccentric aerobic exercise compared with traditional concentric exercise on muscle strength, functional capacity, maximal aerobic capacity, lung function, and quality of life in adults with COPD. Additionally, the potential benefits of ECC in terms of exercise tolerance, lower limb fatigue, and dyspnoea will be assessed, providing a solid evidence base to inform the development of more effective therapeutic guidelines, optimizing interventions for people with COPD, improving their quality of life, and reducing the burden on healthcare systems.
Materials and Methods
This review followed the preferred reporting guidelines for systematic reviews and meta-analyses (PRISMA).28 The protocol was registered with PROSPERO (CRD420251007647).
Eligibility Criteria
The PICO (Population, Intervention, Comparator and Outcome) framework was used to establish eligibility criteria. The population included human subjects of either sex, aged 18 years or older and diagnosed with COPD, recruited at any time since disease diagnosis and with any degree of disease. The intervention had to comprise eccentric aerobic exercise, with or without additional elements; the physical exercise programme had to be administered under the supervision of health professionals and its parameters (intensity, duration, frequency, etc) specified. The comparison had to involve a similar exercise programme whose aerobic training phase was based on concentric exercise (control group). Studies had to include outcome measures in relation to quadriceps muscle strength, exercise tolerance, maximal aerobic capacity, perceived degree of dyspnoea and/or lower limb fatigue. Muscle strength was considered a relevant outcome despite the aerobic focus of the intervention, given the well-documented capacity of ECC to induce peripheral muscle adaptations in addition to its aerobic benefits, which are clinically relevant in COPD rehabilitation.13,14 Only original randomised controlled trials published in peer-reviewed journals were included.
The exclusion criteria were: studies including people with respiratory pathologies other than COPD or with severe comorbidities that may significantly affect the response to training; studies in which the main intervention does not include eccentric aerobic training as part of the experimental treatment; studies that do not include a structured training programme but are limited to a single session with the performance of a stress test and studies that do not specify the parameters of the physical exercise administered. Conference abstracts were excluded due to the limited methodological details and outcome data provided, which make it difficult to assess study quality.
Sources of Information
Searches were conducted until March 2025 using the online electronic databases PubMed, The Cochrane Library for Clinical Trials (CENTRAL), Google Scholar and PEDro. In addition, the reference lists of selected articles and relevant systematic reviews were manually screened to identify other potentially eligible studies.
Search Strategy
The search strategy was designed based on the PICO framework to identify all relevant studies on eccentric aerobic exercise-based training in people with COPD.
To ensure the relevance of the evidence to current clinical practice and training technologies, the search was limited to studies published in the last 10 years (2015–2025). In 2015, the first article on the effect of ECC on the quality of life in a patient with COPD was published29 (case report), so it has been considered as the starting point for this review.
PubMed
Search terms used: (“eccentric” OR “downhill”) AND (“exercise” OR “rehabilitation” OR “training” OR “practice” OR “workout” OR “contraction” OR “pulmonary rehabilitation”) AND (“lung disease” OR “COPD”). Filters applied: humans, randomized controlled trials (RCTs), publications from 2015 to 2025, and languages English, Spanish, or French.
Cochrane CENTRAL
Search terms used: (“eccentric” OR “downhill”) AND (“exercise” OR “rehabilitation” OR “training” OR “practice” OR “workout” OR “contraction”) AND “COPD”. Search fields: title, abstract, and keywords. Filters applied: Trials published between 2015 and 2025. No language filters were available; eligible RCTs were identified through manual screening.
Google Scholar
Search terms used: (eccentric OR downhill) AND COPD. Filters applied: publications from 2015 to 2025, all languages, all study types. Due to database limitations, no filters for study design or population were available, and eligible RCTs were selected manually.
PEDro
Search terms used: “COPD” AND “eccentric” in the Title and Abstract fields. Filters applied: publications from 2015 onwards and “Match all search terms (AND)” to ensure that all terms appeared in each record. Only studies meeting the eligibility criteria for RCTs were included after manual screening.
Study Selection Process
Two members of the research team (G.M.C and T.F.P) conducted the initial search. After elimination of duplicates, the titles and abstracts were examined, discarding records that did not fit the scope of this review. Subsequently, the full texts of abstracts that did not provide sufficient information for exclusion or that appeared potentially suitable for inclusion were obtained. Both authors (G.M.C and T.F.P) then independently assessed the full texts and selected studies for inclusion based on the information available. Discrepancies between reviewers were resolved by discussion.
Data Extraction Process
Data from each study included in this review were extracted independently by two authors (G.M.C. and T.F.P.) into an Excel spreadsheet. The two authors then compared the two spreadsheets and resolved inconsistencies through discussion in order to achieve a consensus data extraction table.
List of Data
Information on several key variables was collected from the included studies. With respect to publication details, data on the authors, year of publication, and journal were recorded.
Regarding study design, the type of randomisation, the level of blinding (single, double, etc), and the experimental design (parallel group, cross-over, or other) were documented.
Regarding the population, data on sample size and demographic characteristics, including gender, age, and body mass index (BMI), were documented. Baseline functional status was also recorded, measured by forced expiratory volume in 1 second (FEV1) and COPD grade according to the Global initiative for chronic obstructive lung disease (GOLD) scale. Additionally, the homogeneity of the sample in terms of baseline characteristics was assessed.
For the intervention, detailed information was collected on the duration of the training programme, the frequency of the sessions (number of sessions per week), the duration and intensity of the sessions, the type of exercise performed (such as cycloergometer, treadmill, or strength exercises), the progression of the exercise and the existence of familiarisation and follow-up sessions. For the comparator, the same data were recorded as for the intervention.
For the outcomes, primary and secondary outcome variables were distinguished. Primary variables included means and standard deviations (SD) of indicators such as muscle strength, exercise tolerance, maximal aerobic capacity, dyspnoea and lower limb fatigue, assessed both before and after the training period. Secondary variables comprised the inferential statistical parameters used to assess differences between groups. In addition, all outcomes consistent with each outcome domain were collected, regardless of the measurement scales or time points used. If some outcomes were not comparable, notes were made to justify their exclusion. For those that used different measurement scales, the standardized mean difference was applied.
Finally, other relevant variables were collected, such as programme adherence, exercise tolerance and any reported adverse events. For missing or uncertain data, the intention-to-treat principle was assumed in analyses where indicated. If critical information was missing, it was explicitly recorded, and where possible, authors were contacted for clarification.
Assessment of Risk of Bias of Individual Studies
PEDro Scale
The risk of bias of individual studies was assessed using the Physiotherapy Evidence Database (PEDro) scale,30,31 a validated tool for evaluating the methodological quality of randomized controlled trials in rehabilitation research. The PEDro scale evaluates internal validity and statistical reporting, assigning one point per criterion met (maximum score: 10), with the first item related to external validity excluded from the total score. Higher scores indicate higher methodological quality. Methodological quality was classified as: ≥9 points = excellent, 6–8 = good, 4–5 = moderate, <4 = low.31
Two independent reviewers (G.M.C. and T.F.P.) assessed each study, resolving discrepancies through discussion. The PEDro scale was selected because it is widely recognized in physiotherapy and exercise-based interventions, ensuring standardized evaluation of methodological rigor.
RoB 2.0
The risk of bias was also assessed using the Cochrane Risk-of-Bias Tool for Randomized Trials (RoB 2.0),32 which complements the PEDro scale by evaluating five domains: bias arising from the randomization process, deviations from intended interventions, missing outcome data, outcome measurement, and selection of reported results.
Two independent reviewers (G.M.C. and T.F.P.) applied the RoB 2.0 tool to each study, with disagreements resolved by discussion. Risk of bias judgments were categorized as low, some concerns, or high, following Sterne et al.32
Assessment of the Certainty of the Evidence
The certainty of the evidence for each outcome was assessed using the GRADE (Grading of recommendations, assessment, development, and evaluation) system.33,34 This system classifies evidence into four categories: high, moderate, low, and very low, based on the following domains:
Risk of Bias
Evaluated using PEDro scores and RoB 2.0 assessments, considering limitations such as lack of participant and therapist blinding inherent to exercise interventions.
Inconsistency (Heterogeneity)
Examined using I² statistics across studies for each outcome. Outcomes with I² > 50% were considered to have substantial heterogeneity.
Imprecision
Evaluated by examining confidence intervals (CIs). Outcomes with wide CIs or CIs including the null value were downgraded.
Indirectness
Considered applicability of interventions and populations to the review question.
Publication Bias
Assessed qualitatively by examining study reporting and comprehensiveness of included trials.
Decisions on downgrading or maintaining evidence certainty were made collectively by two independent reviewers (G.M.C. and T.F.P.), with discrepancies resolved through discussion. Random-effects models were used in meta-analyses where substantial heterogeneity was detected, and fixed-effects models were applied when heterogeneity was low.
Data Synthesis
Review Manager software (RevMan 5.4) was used to perform the meta-analysis (The Cochrane Collaboration, 2020). For those variables that were measured on the same scale in the included studies, the mean difference was used.To determine the overall effect, the p-value of the Z-statistic was interpreted. If p < 0.05, the null hypothesis is rejected and the alternative hypothesis is accepted, demonstrating that the overall effect is not produced by chance. A 95% confidence interval was determined. Heterogeneity among included studies was calculated using the I² statistic, which describes the percentage of variability due to heterogeneity rather than chance.
Results
Study Selection
The literature search yielded a total of 83 results. After removing 29 duplicates using the Zotero bibliographic manager, the titles and abstracts of the remaining 54 articles were screened, leading to the exclusion of 42 studies that did not meet the scope of this review. The full texts of the remaining 12 articles were then assessed for eligibility, resulting in the inclusion of six studies in this review (Figure 1).
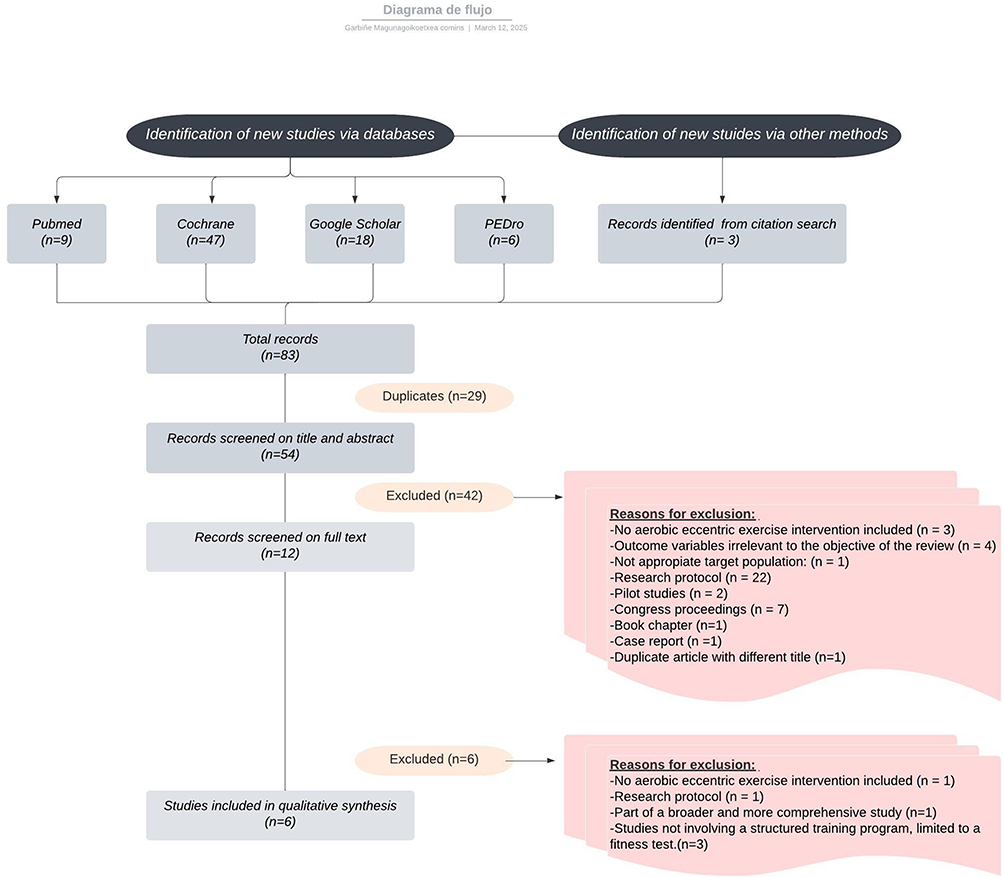 |
Figure 1 Flow chart of the process of selecting eligible studies. |
Characteristics of the Studies
All included studies are parallel-group randomised clinical trials, with an experimental group performing ECC and a control group performing CON. The total final sample size was 154 patients, with variability between studies ranging from 15 to 35 participants, and group sizes ranging from 7 to 18 individuals. All studies calculated their samples from previous power analyses; however, in two of them, the final size did not reach the initial estimate.15,17 The distribution between ECC and CON training groups was balanced in all studies. Characteristics of the studies, including population, intervention, and outcomes, are summarized in Table 1. All studies reported outcome measures at baseline (pre-intervention) and immediately post-intervention. Only one study16 included an additional follow-up assessment at 3 months post-intervention.
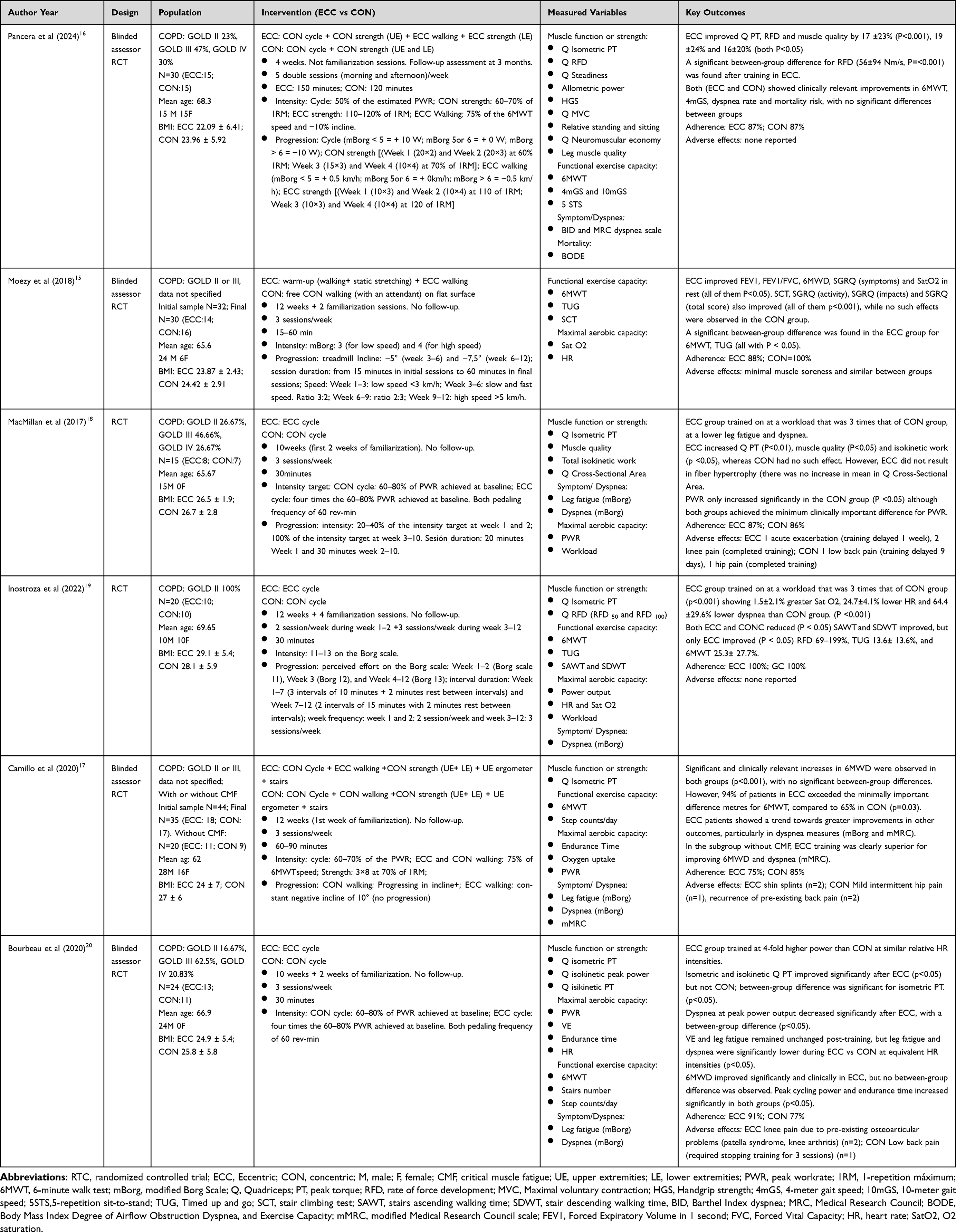 |
Table 1 Characteristics of Included Studies |
In terms of population characteristics, all studies enrolled people with COPD, but with different degrees of severity according to the GOLD classification (from II to IV). The most frequent severity grade in three of the studies was GOLD III (severe), with prevalences of 47%, 46.66% and 62.5% in each study.16,18,20 However, two studies did not specify the exact percentages of GOLD II and III patients,15,17 while another included exclusively GOLD II patients.19 The mean age of the patients varied slightly, ranging from 62 to 69.65 years.
In terms of gender distribution, most studies included more men than women. Two studies had all-male samples,18,20 while two others had male predominance.15,17 Only two of the six studies included an equal distribution between men and women.16,19 BMI was reported in all included studies. The mean BMI for participants in the ECC groups ranged from 22.1 to 29.1 kg/m², while in the CON groups it ranged from 23.0 to 28.1 kg/m². Overall, baseline BMI values were similar between groups across studies, indicating comparable body composition at baseline.
Regarding the intervention, the duration of training ranged from 4 to 12 weeks, with a mode of 12 weeks. The frequency ranged from 2 to 5 sessions per week, with 3 sessions per week being the most common. Except for one study that included double sessions (morning and afternoon),16 all other studies implemented single sessions. The duration of each session ranged from 15 to 150 minutes, with a mode of 30 minutes.
Regarding the type of exercise, four studies used exclusively aerobic exercise,15,18–20 while two included strength exercises.16,17 Three studies used a cycloergometer,18–20 one a treadmill,15 and two combined both,16,17 although the comparison between ECC and CON was made only with the treadmill. In the cycloergometer studies, one set the initial intensity based on the Borg scale,19 while the others were based on the maximal work rate in the stress test.16–18,20 In the treadmill studies, one set the intensity based on the Borg scale,15 while the other two based it on the speed achieved in the 6-minute walk test.16,17
Since ECC is perceived as less demanding, two studies matched the intensity of the two groups based on relative heart rate,18,20 three matched the intensity based on perceived exertion on the Borg scale,15,16,19 and one study did not establish matching criteria.17 In addition, four studies used continuous training16–18,20 and two used intervallic training.15,19
The main outcomes assessed were aerobic capacity, muscle strength and functional capacity. All studies, except one,16 analysed measures of aerobic ability such as heart rate, oxygen saturation, and peak power rating (PWR), among others, although with considerable heterogeneity in the variables used. The same was true for the assessment of muscle strength: although all studies measuring muscle strength included isometric maximal quadriceps torque (isometric PT), there was great variability in the other strength measures used.
In contrast, variables related to patient symptoms were more homogeneous. Four of the five studies that assessed symptoms used the modified Borg scale to measure dyspnoea and lower limb fatigue.17–20 Of these, three measured both variables,17,18,20 while one focused only on dyspnoea.19
Exercise tolerance was assessed in all but one study,18 using tests such as walking, getting up from a chair or going up and down stairs. The 6-minute walk test (6MWT) was the most commonly used test, appearing in all studies, followed by the Timed Up and Go test (TUG), used in two.15,19 Three studies included functional measures related to stair climbing and descending, although with different methodologies,15,19,20 and two studies counted total daily steps.17,20
Adherence and adverse events were generally favorable across the included studies. Adherence to the training programs was high, with ECC groups ranging from 75% to 100% and CON groups ranging from 77% to 100%, indicating that both exercise modalities were feasible and well tolerated by people with COPD. Adverse events were minimal and mostly mild. Two studies reported no adverse effects.16,19 Moezy et al15 observed only minor muscle soreness, similar between groups; in Mac Millan et al18 the ECC group experienced one acute exacerbation and two cases of knee pain, while the CON group reported one episode of low back pain and one case of hip pain and Camillo et al17 reported ECC-related shin splints in two participants, and in the CON group mild intermittent hip pain (n=1) and recurrence of pre-existing back pain (n=2). Finally, Bourbeau et al20 described knee pain due to pre-existing osteoarticular conditions in two ECC participants, and low back pain in one CON participant that required pausing training for three sessions. Overall, the data suggest that ECC is feasible, well tolerated, and associated with a low incidence of mild, transient adverse events, comparable to CON.
Risk of Bias in Individual Studies
PEDro Scores
PEDro scores for the included studies ranged from 6 to 7 points (mean 6), indicating overall “good” methodological quality (6–8 points) (Table 2). All studies were randomized clinical trials. Blinding of participants and therapists was largely unfeasible due to the nature of the interventions, which represents an inherent limitation and explains why criteria 5 and 6 of the PEDro scale were not met. Assessor blinding was reported in four studies,15–17,20 while the remaining two did not specify whether this procedure was applied.18,19
 |
Table 2 PEDro Scale Scores of the Studies |
RoB 2.0 Assessments
The RoB 2.0 tool provided complementary evaluation across five bias domains. Among the included RCTs, Bourbeau et al20 presented the lowest risk of bias, with low risk across all domains. The remaining studies had unclear overall risk: Moezy et al,15 MacMillan et al,18 and Inostroza et al19 had two domains classified as some concerns, whereas Pancera et al16 and Camillo et al17 had only one domain with some concerns (Figure 2).
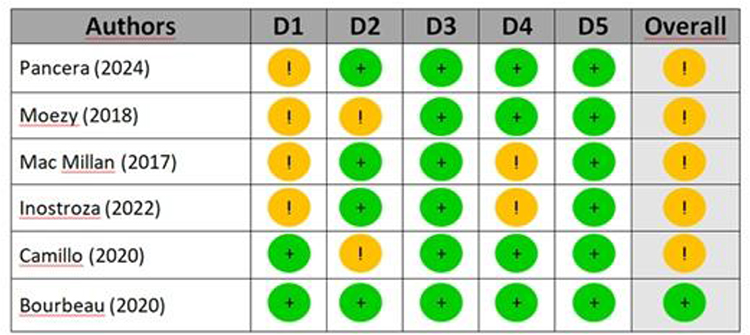 |
Figure 2 Risk of bias assessment. |
Results of Individual Studies
Table 1 summarises the main characteristics of the included studies.
Synthesis Results
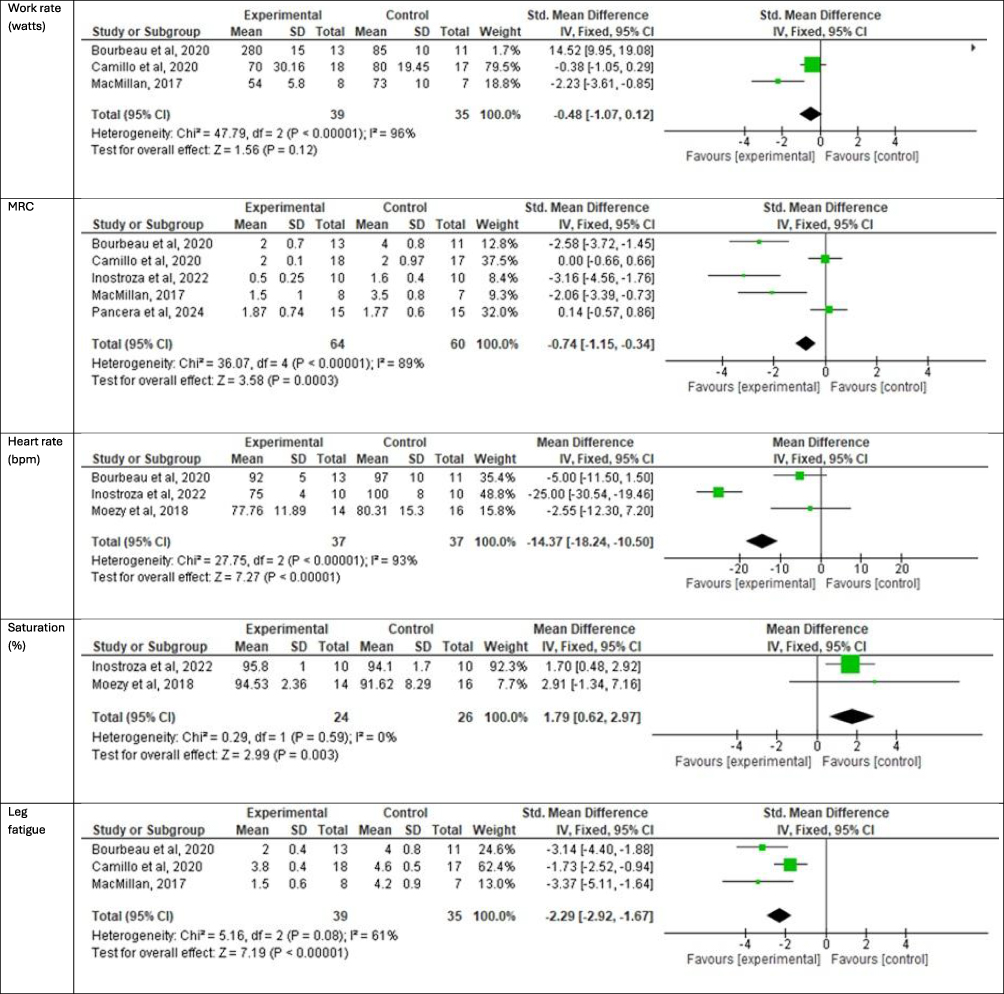
Quantitative results shown in (Figure 3).
Figure 3 Continued. Figure 3 Quantitative results.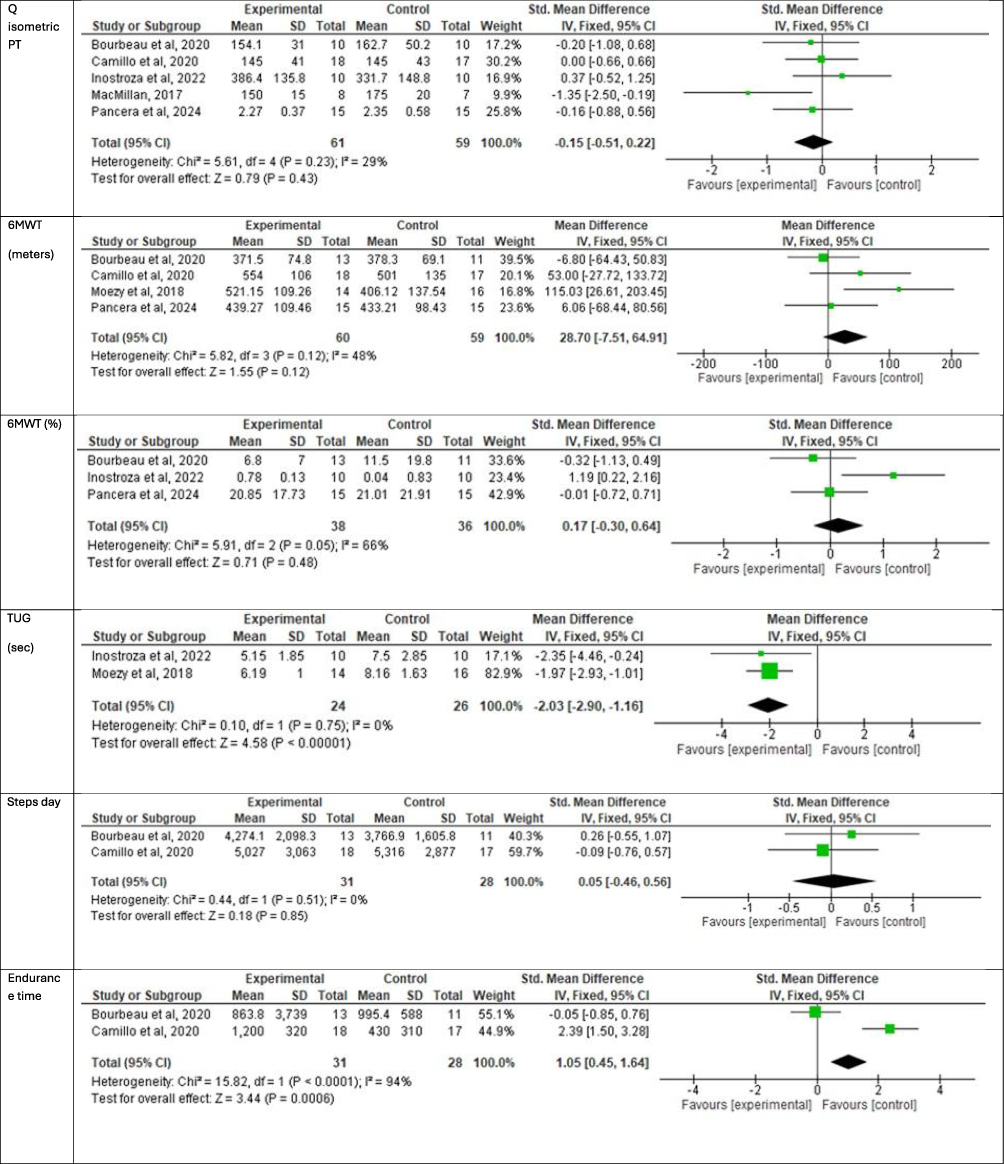
Quadriceps Muscle Strength
Five studies assessed quadriceps isometric peak torque (Q isometric PT) in Newton, with a total sample of 120 subjects.16–20 The results indicate an improvement in quadriceps muscle strength in the experimental group compared to the control group (−0.15 [−0.51, 0.22] p=0.43). Heterogeneity between studies was low (I² = 29%) and d= 0.43 who is a medium effect.
Exercise Tolerance
Four studies measured exercise tolerance through the six-minute walk test (6MWT) in metres, with a total of 119 subjects.15–17,20 An improvement in distance covered was observed in the control group compared to the experimental group (28.70 [−7.51, 64.91] p=0.12). Heterogeneity between studies was low (I² = 48%) and small effect (d=0.35).
Three studies (n=74) measured exercise tolerance as the percentage improvement in metres from baseline.16,19,20 The results favoured the control group (0.17 [−0.30, 0.64] p=0.48), with medium heterogeneity (I² = 67%) and small effect (d=0.36).
Two studies (n=50) assessed exercise tolerance using the TUG in seconds.15,19 The results showed an improvement in the experimental group compared to the control (−2.03 [−2.90, −0.16] p< 0.001), with homogeneous studies (I² = 0%) and a large effect (d=1.15).
Activity Level and Aerobic Ability
The studies by Bourbeau et al and Camillo et al17,20 (n=59), measured the total number of daily steps, finding similar results in both groups (−0.05 [−0.46, 0.56] p=0.85), with homogeneous studies (I² = 0%) and a null effect (d=0).
These same studies also assessed endurance time, where a significant improvement was observed in the control group compared to the experimental group (1.05 [0.45, 1.64] p<0.01), with high between-study heterogeneity (I² = 94%) and a large effect (d=0.9).
Three studies (n=74) analysed work rate in watts,17,18,20 showing a higher work rate in the experimental group (−0.48 [−1.07, 0.12] p =0.12), with high heterogeneity (I² = 96%) and d= 0.7 who is a medium effect.
Regarding exercise adaptations, two studies (n=50) analysed oxygen saturation,15,19 finding an increase in oxygen saturation in the control group compared to the experimental (1.79 [0.62, −2.97] p < 0.01), with loss heterogeneity (I² =0%) and small effect (d=0.47).
Regarding heart rate, in addition to these two studies, Bourbeau et al20 also analysed this variable. With a total of 74 participants, a reduction was observed in the experimental group compared to the control (−14.37 [−18.24, −10.50] p < 0.01), despite high heterogeneity (I²= 93%) and d= 0.66 who is a medium effect.
Dyspnoea and Lower Limb Fatigue
Five studies (n= 124) assessed dyspnoea and its evolution over weeks of training,16–20 finding a reduction in the experimental group (−0.74 [−1.15, −0.34] p <0.001), despite high heterogeneity between studies (I² = 89%) and medium effect (d=0.77).
Three of these articles (n= 74) also analysed lower limb fatigue after training,17,18,20 reporting lower values in the experimental group (−2.29 [−2.92, −1.67] p<0.001), with moderate heterogeneity (I² = 61%) and a large effect (d=1.6).
Certainty of Evidence
Table 3 summarizes the certainty of evidence across outcomes. Overall, all outcomes were rated as moderate certainty.
Evidence certainty was primarily downgraded due to:
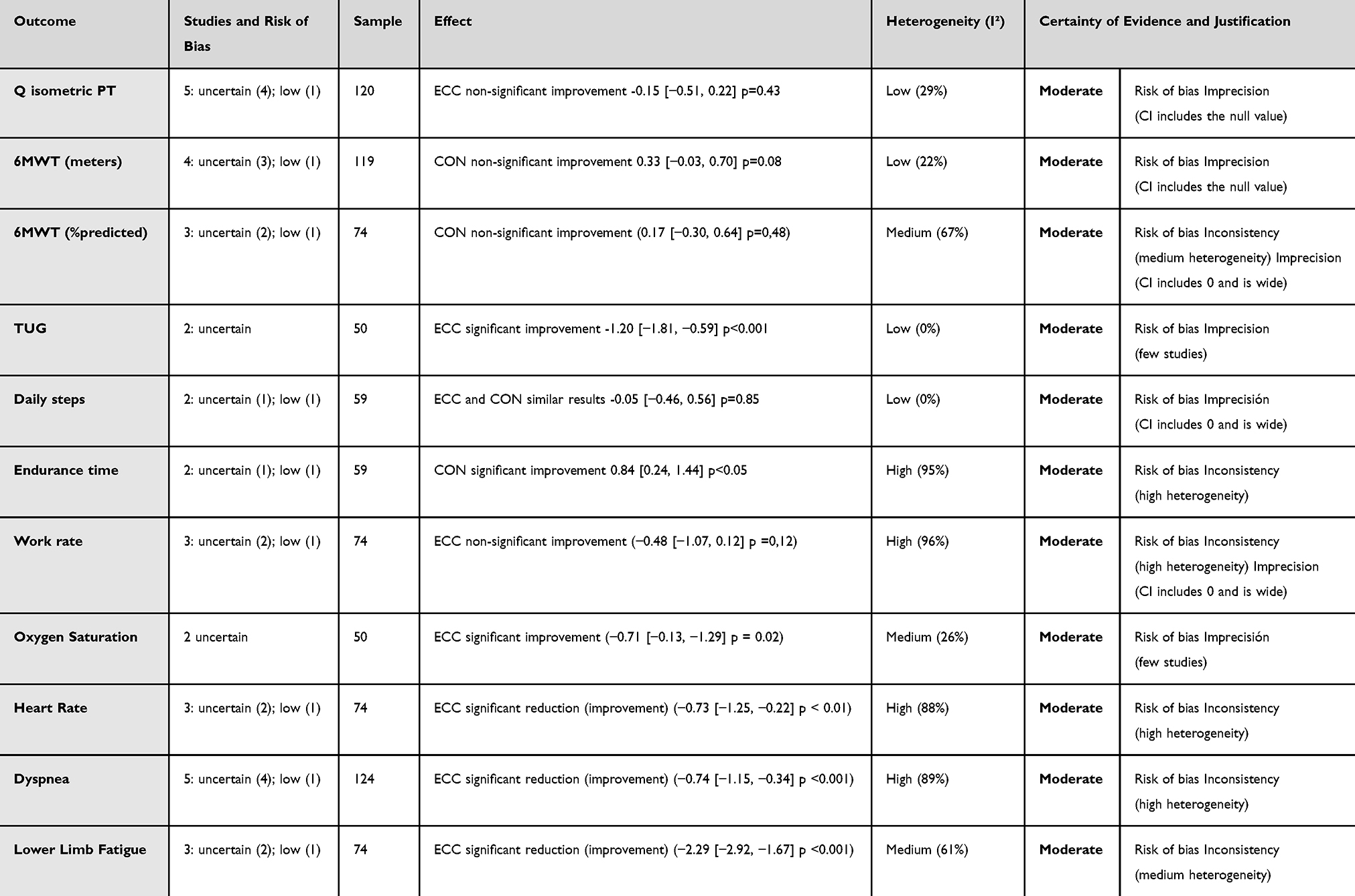 |
Table 3 Level of Evidence of the Articles |
Risk of Bias
Limitations in participant and therapist blinding inherent to exercise interventions, and small sample sizes.
Inconsistency
Moderate to high heterogeneity across studies (I² 26–96%).
Imprecision
Confidence intervals were wide or included the null effect.
Discussion
The objective of this review was to compare the effects on exercise tolerance and functional outcomes of eccentric aerobic exercise (ECC) versus concentric exercise (CON) in people with COPD. Improvements, with a large or medium effect (d>0.6) were observed in quadriceps strength, functionality (measured with the Timed Up and Go test), work rate, dyspnoea, leg fatigue, and resting heart rate in the experimental group.
The demographics of the participants were similar in all studies: a predominance of men, with a mean age between 62 and 62.9 years and a diagnosis of COPD stages GOLD II–III. The duration of the pulmonary rehabilitation programmes ranged from 4–12 weeks, with 12 weeks being the most common, as recommended by the American Thoracic Society clinical practice guideline.35 Sessions ranged from 15–150 minutes, with an average duration of 30 minutes.36 Traditionally, the aerobic exercises used in pulmonary rehabilitation are mainly the updown treadmill and the cycloergometer, but the emergence of new training methods in the general population, such as ECC, makes it necessary to review these traditional methods.
The outcomes analyzed in this review — including endurance time, Timed Up and Go test (TUG) time, 6-minute walk test (6MWT) distance, daily step count, as well as symptoms of dyspnoea and lower-limb fatigue — are widely recognized as indicators of exercise tolerance and functional capacity in people with COPD. Therefore, the evidence synthesized supports framing our results within these patient-centered domains. However, the differences in sample size between the studies and the exercise protocol followed mean that the endurance time, work rate, heart rate, and dyspnoea outcomes are highly heterogeneous (I > 75%), making their results more questionable.
The most analysed variable in the studies of this meta-analysis was quadriceps muscle strength. All studies, except Moezy et al,15 included it among their objectives. A recent review published in 202337 already confirmed that ECC increases quadriceps strength, measured during both isometric and eccentric contraction. Several studies have analysed the effects of ECC on the quadriceps,38–40 obtaining improvements in peak torque, thickness and hypertrophy, respectively. Although all of them were performed in healthy subjects, they support the strength improvement associated with ECC, in line with the articles included in this review.
The fact that this variable is the most commonly used is not irrelevant, since in people with COPD quadriceps weakness is associated with reduced exercise tolerance, poorer functional performance, poorer quality of life and reduced physical activity.41
People with more severe COPD have been found to have greater quadriceps fatigue and dyspnoea both at rest and during exercise,42 the latter being the most limiting symptom of the disease.43 Likewise, studies such as that by Rodio et al have linked increased quadriceps strength through ECC to lower levels of pain and fatigue in healthy subjects,44 which could explain the decrease in dyspnoea, assessed using the Medical Research Council (MRC) scale and improvement in muscle fatigability observed in the articles in this review.
In general, a reduction in dyspnoea should translate into an increase in functional ability.45 In the articles reviewed, functionality was assessed using 6MWT and TUG, with mixed results. While times in the TUG test were better in subjects who performed ECC, in the 6MWT it was the participants who followed a CON programme who covered more distance, although without statistically significant differences. This difference could be attributed to the nature of the tests: the 6MWT is a linear test that measures the distance walked in 6 minutes,46 whereas the TUG involves getting up from a chair, walking 3 metres and sitting down again.47
Traditionally, the TUG test has been the most widely used test in the elderly population for its reliability in predicting the risk of falls and frailty,47 especially because it includes functional transfers. Eccentric quadriceps exercise training has been associated with improved functionality48 and a reduction in the number of falls in older people,49 as well as improving gait pattern, symmetry50 and shock absorption.51 Activities such as getting up or sitting down from a chair involve eccentric contractions of the quadriceps,52 as does walking downhill, which could explain the good results of the experimental group in this test.
On the other hand, the 6MWT is linear and of longer duration (6 minutes compared to approximately 10 seconds for the TUG,53 which could explain the better results of the group in terms of endurance time.
Regarding the steps per day variable, no differences were observed between the two groups, with a homogeneity of 0% between the two groups and a null effect, so it would not be a variable that provides significant information in this review.
Finally, one of the main advantages of ECC over CON is that it allows greater tolerance to effort (measured in terms of absolute power).54 This means a lower maximum heart rate during exercise, as observed in this review, as well as a lower ventilatory demand55 and an improvement in oxygen saturation, as demonstrated by Har-NIr et al56 in their study on multiple sclerosis and ECC. However, these results differ from those obtained in this review. Perhaps because in patients with obstructive respiratory pathology, it would be more interesting to study the effects on hypercapnia than the effects on oxygen saturation.57
Limitations
This review has certain limitations. Firstly, the number of articles included, despite presenting a significant clinical effect, is still too small to extrapolate the data to the general population.
The protocols followed in the studies were not similar. There is a lot of variability between the type of exercise (walking or cycling), session time, and training duration among the selected articles, making it difficult to determine the benefits of eccentric versus concentric training. Therefore, it would be interesting to first establish a treatment protocol that unifies criteria before conducting new studies.
Future Lines of Research
None of the review articles indicated whether any musculoskeletal injury occurred, despite evidence that poorly executed eccentric exercise can cause muscle damage.58 The need for standardized, multicenter, and long-term protocols could emphasize the emergence of possible injuries. This information would be useful in determining which types of patients with comorbidities might or might not benefit from this type of training.
Given that all participants in this review were people diagnosed with COPD, it would be interesting to research the effect of eccentric aerobic exercise training on other respiratory or cardiac pathologies.
Conclusions
Eccentric aerobic exercise is a valid alternative to concentric aerobic exercise in the training of people with COPD, contributing to improved exercise tolerance in terms of heart rate, fatigue and dyspnoea and functionality, while CON improves endurance time. However, further studies are required to determine with greater certainty its impact on functionality.
Acknowledgments
The authors thank everyone who contributed to this study. Author contributions: All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Ilustre Colegio Oficial de Fisioterapeutas de la Comunidad de Madrid.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Celli B, Fabbri L, Criner G, et al. Definition and nomenclature of chronic obstructive pulmonary disease: time for its revision. Am J Respir Crit Care Med. 2022;206(11):1317–1325. doi:10.1164/rccm.202204-0671PP
2. Bui KL, Nyberg A, Rabinovich R, Saey D, Maltais F. The relevance of limb muscle dysfunction in chronic obstructive pulmonary disease: a review for clinicians. Clin Respir Physiol. 2019;40(2):367–383.
3. Barreiro E, Sieck G. Muscle dysfunction in COPD. J Appl Physiol. 2013;114(9):1220–1221. doi:10.1152/japplphysiol.00162.2013
4. Geidl W, Carl J, Cassar S, et al. Physical activity and sedentary behaviour patterns in 326 persons with COPD before starting a pulmonary rehabilitation: a cluster analysis. J Clin Med. 2019;8(9):1346. doi:10.3390/jcm8091346
5. Li P, Li J, Wang Y, Xia J, Liu X. Effects of exercise intervention on peripheral skeletal muscle in stable patients with COPD: a systematic review and meta-analysis. Front Med. 2021;8:766841. doi:10.3389/fmed.2021.766841
6. Forum of International Respiratory Societies. The Global Impact of Respiratory Disease.
7. Soriano JB, Abajobir AA, Abate KH, et al. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir Med. 2017;5(9):691–706. doi:10.1016/S2213-2600(17)30293-X
8. Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3(11):e442. doi:10.1371/journal.pmed.0030442
9. McCarthy B, Casey D, Devane D, Murphy K, Murphy E, Lacasse Y. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2015;2015(2):CD003793. doi:10.1002/14651858.CD003793.pub3
10. Moecke DP, Zhu K, Gill J, et al. Safety and efficacy of inpatient pulmonary rehabilitation for patients hospitalized with an acute exacerbation of chronic obstructive pulmonary disease: systematic review and meta-analyses. Ann Am Thorac Soc. 2023;20(2):307–319. doi:10.1513/AnnalsATS.202206-545OC
11. Troosters T. Chronic obstructive pulmonary disease: exercise training on the edge. Exp Physiol. 2013;98(6):1079–1080. doi:10.1113/expphysiol.2013.072066
12. Zainuldin R, Mackey MG, Alison JA. Optimal intensity and type of leg exercise training for people with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2011;2011(11):CD008008. doi:10.1002/14651858.CD008008.pub2
13. Isner-Horobeti ME, Dufour SP, Vautravers P, Geny B, Coudeyre E, Richard R. Eccentric exercise training: modalities, applications and perspectives. Sports Med. 2013;43(6):483–512. doi:10.1007/s40279-013-0052-y
14. LaStayo P, Marcus R, Dibble L, Frajacomo F, Lindstedt S. Eccentric exercise in rehabilitation: safety, feasibility, and application. J Appl Physiol. 2014;116(11):1426–1434. doi:10.1152/japplphysiol.00008.2013
15. Moezy A, Erfani A, Mazaherinezhad A, Mousavi SAJ. Downhill walking influence on physical condition and quality of life in patients with COPD: a randomized controlled trial. Med J Islam Repub Iran. 2018;32:49. doi:10.14196/mjiri.32.49
16. Pancera S, Lopomo NF, Porta R, Sanniti A, Buraschi R, Bianchi LNC. Effects of combined endurance and resistance eccentric training on muscle function and functional performance in patients with chronic obstructivepulmonary disease: randomized controlled trial. Arch Phys Med Rehabil. 2024;105(3):470–479. doi:10.1016/j.apmr.2023.09.004
17. Camillo CA, Osadnik CR, Burtin C, et al. Effects of downhill walking in pulmonary rehabilitation for patients with COPD: a randomised controlled trial. Eur Respir J. 2020;56(3):2000639. doi:10.1183/13993003.00639-2020
18. MacMillan N, Kapchinsky S, Konokhova Y, et al. Eccentric ergometer training promotes locomotor muscle strength but not mitochondrial adaptation in patients with severe chronic obstructive pulmonary disease. Front Physiol. 2017;8. doi:10.1002/central/CN-01369640/full
19. Inostroza M, Valdés O, Tapia G, et al. Effects of eccentric vs concentric cycling training on patients with moderate COPD. Eur J Appl Physiol. 2022;122(2):489–502. doi:10.1007/s00421-021-04850-x
20. Bourbeau J, De Sousa Sena R, Taivassalo T, et al. Eccentric versus conventional cycle training to improve muscle strength in advanced COPD: a randomized clinical trial. Respir Physiol Neurobiol. 2020;276:103414. doi:10.1016/j.resp.2020.103414
21. Valladares-Ide D, Bravo MJ, Carvajal A, et al. Changes in pulmonary and plasma oxidative stress and inflammation following eccentric and concentric cycling in stable COPD patients. Eur J Appl Physiol. 2021;121(6):1677–1688. doi:10.1007/s00421-021-04652-1
22. Ward TJC, Lindley MR, Ferguson RA, et al. Submaximal eccentric cycling in people with COPD: acute whole-body cardiopulmonary and muscle metabolic responses. Chest. 2021;159(2):564–574. doi:10.1016/j.chest.2020.08.2082
23. Kulkarni D, Gregory S, Evans M. Effectiveness of eccentric-biased exercise interventions in reducing the incidence of falls and improving functional performance in older adults: a systematic review. Eur Geriatr Med. 2022;13(2):367–380. doi:10.1007/s41999-021-00571-8
24. Kim Y, Oh S, Kim DY, Lim JY. Effects of eccentric contraction-based resistance exercise on physical performance in chronic stroke patients: a randomized controlled trial. Medicine. 2025;104(32):e43491. doi:10.1097/MD.0000000000043491
25. Lattouf NA, Tomb R, Assi A, Maynard L, Mesure S. Eccentric training effects for patients with post-stroke hemiparesis on strength and speed gait: a randomized controlled trial. NeuroRehabilitation. 2021;48(4):513–522. doi:10.3233/NRE-201601
26. Besson D, Sow AK, Fournel I, et al. Impact of eccentric cycling in coronary rehabilitation program: a pragmatic randomized controlled trial versus conventional rehabilitation. Eur J Phys Rehabil Med. 2024;60(5):878–888. doi:10.23736/S1973-9087.24.08364-3
27. Casillas JM, Besson D, Hannequin A, et al. Effects of an eccentric training personalized by a low rate of perceived exertion on the maximal capacities in chronic heart failure: a randomized controlledtrial. Eur J Phys Rehabil Med. 2016;52(2):159–168.
28. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
29. Erfani A, Moezy A, Mazaherinezhad A, Mousavi SAJ. Does downhill walking on treadmill improve physical status and quality of life of a patient with COPD? Asian J Sports Med. 2015;6(4):e25821. doi:10.5812/asjsm.25821
30. Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther. 2003;83(8):713–721. doi:10.1093/ptj/83.8.713
31. Cashin AG, McAuley JH. Clinimetrics: Physiotherapy Evidence Database (PEDro) Scale. J Physiother. 2020;66(1):59. doi:10.1016/j.jphys.2019.08.005
32. Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. doi:10.1136/bmj.l4898
33. Aguayo-Albasini JL, Flores-Pastor B, Soria-Aledo V. [GRADE system: classification of quality of evidence and strength of recommendation]. Cirugia Espanola. 2014;92(2):82–88. Spanish. doi:10.1016/j.ciresp.2013.08.002
34. Sanabria AJ, Rigau D, Rotaeche R, Selva A, Marzo-Castillejo M, Alonso-Coello P. Sistema GRADE: metodología para la realización de recomendaciones para la práctica clínica. Aten Primaria. 2015;47(1):48–55. doi:10.1016/j.aprim.2013.12.013
35. Rochester CL, Alison JA, Carlin B, et al. Pulmonary rehabilitation for adults with chronic respiratory disease: an official American thoracic society clinical practice guideline. Am J Respir Crit Care Med. 2023;208(4):e7–26. doi:10.1164/rccm.202306-1066ST
36. Cosío BG, Hernández C, Chiner E, et al. Actualización 2021 de la Guía Española de la EPOC (GesEPOC). Tratamiento no farmacológico. Arch Bronconeumol. 2022;58(4):345–351. doi:10.1016/j.arbres.2021.08.010
37. Ansari M, Hardcastle S, Myers S, Williams AD. The health and functional benefits of eccentric versus concentric exercise training: a systematic review and meta-analysis. J Sports Sci Med. 2023;22(2):288–309. doi:10.52082/jssm.2023.288
38. Anwer S, Jeelani SI, Khan SA, Quddus N, Kalra S, Alghadir AH. Effects of TheraBand and theratube eccentric exercises on quadriceps muscle strength and muscle mass in young adults. BioMed Res Int. 2021;2021:5560144. doi:10.1155/2021/5560144
39. Kojic F, Mandic D, Duric S. The effects of eccentric phase tempo in squats on hypertrophy, strength, and contractile properties of the quadriceps femoris muscle. Front Physiol. 2024;15:1531926. doi:10.3389/fphys.2024.1531926
40. Leong CH, McDermott WJ, Elmer SJ, Martin JC. Chronic eccentric cycling improves quadriceps muscle structure and maximum cycling power. Int J Sports Med. 2014;35(7):559–565. doi:10.1055/s-0033-1358471
41. Jenkins TO, Patel S, Edwards GD, et al. Longitudinal change in ultrasound-derived rectus femoris cross-sectional area in COPD. ERJ Open Res. 2024;10(4):00123–2024. doi:10.1183/23120541.00123-2024
42. Paneroni M, Cavicchia A, Beatrice S, Bertacchini L, Venturelli M, Vitacca M. The influence of lung function and respiratory muscle strength on quadriceps muscle fatigability in COPD patients under long-term oxygen therapy. Arch Bronconeumol. 2024;60(7):410–416. doi:10.1016/j.arbres.2024.04.004
43. Lamberton CE, Mosher CL. Review of the evidence for pulmonary rehabilitation in COPD: clinical benefits and cost-effectiveness. Respir Care. 2024;69(6):686–696. doi:10.4187/respcare.11541
44. Rodio A, Fattorini L. Downhill walking to improve lower limb strength in healthy young adults. Eur J Sport Sci. 2014;14(8):806–812. doi:10.1080/17461391.2014.908958
45. Martins RDL, Monteiro EDSS, de Lima AMJ, Santos ADC, Brasileiro-Santos MDS. Effect of telerehabilitation on pulmonary function, functional capacity, physical fitness, dyspnea, fatigue, and quality of Life in COVID-19 patients: a systematic review and metanalysis. Telemed J E-Health. 2024;30(8):e2256–86. doi:10.1089/tmj.2023.0653
46. Ngueleu AM, Barrette S, Buteau C, et al. Impact of pathway shape and length on the validity of the 6-minute walking test: a systematic review and meta-analysis. Sensors. 2024;25(1):17. doi:10.3390/s25010017
47. Podsiadlo D, Richardson S. The timed «Up & Go»: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. 1991;39(2):142–148. doi:10.1111/j.1532-5415.1991.tb01616.x
48. Arab F, Quddus N, Khan SA, Alghadir AH, Khan M. Association of eccentric quadriceps torque with pain, physical function, and extension lag in women with grade ≤ II knee osteoarthritis: an observational study. Medicine. 2022;101(31):e29923. doi:10.1097/MD.0000000000029923
49. Kim J, Choi S. Association of timed up and go test results with future injurious falls among older adults by sex: a population-based cohort study. BMC Geriatr. 2024;24(1):1035. doi:10.1186/s12877-024-05588-9
50. Xie H, Chien JH. Walking on different inclines affects gait symmetry differently in the anterior-posterior and vertical directions: implication for future sensorimotor training. PeerJ. 2024;12:e18096. doi:10.7717/peerj.18096
51. Papachatzis N, Takahashi KZ. Mechanics of the human foot during walking on different slopes. PLoS One. 2023;18(9):e0286521. doi:10.1371/journal.pone.0286521
52. Wang H, Simpson KJ, Chamnongkich S, Kinsey T, Mahoney OM. A biomechanical comparison between the single-axis and multi-axis total knee arthroplasty systems for the stand-to-sit movement. Clin Biomech. 2005;20(4):428–433. doi:10.1016/j.clinbiomech.2004.12.003
53. Bohannon RW. Reference values for the timed up and go test: a descriptive meta-analysis. J Geriatr Phys Ther. 2006;29(2):64–68. doi:10.1519/00139143-200608000-00004
54. Barreto RV, Lima LC, Borszcz FK, de Lucas RD, Denadai BS. Acute physiological responses to eccentric cycling: a systematic review and meta-analysis. J Sports Med Phys Fitness. 2023;63(10):1051–1068. doi:10.23736/S0022-4707.23.14971-1
55. Kammerlander A, Schneider SR, Furian M, et al. Effect of eccentric cycling on oxygen uptake and hemodynamics in patients with chronic obstructive pulmonary disease: a randomized controlled crossover trial. Respir Int Rev Thorac Dis. 2025:1–11.
56. Har-Nir I, Frid L, Kalron A. Energy expenditure and perceived effort during uphill and downhill walking in people with multiple sclerosis. Eur J Phys Rehabil Med. 2023;59(1):25–31. doi:10.23736/S1973-9087.22.07682-1
57. Corbellini C, Tavella S, Gugliotta E, Zampese S, Sanchez Romero EA, Villafane J. Hypercapnia and functional improvements during pulmonary rehabilitation. Eur Respir J. 2021;58(suppl 65):PA1827.
58. Maeo S, Yamamoto M, Kanehisa H, Nosaka K. Prevention of downhill walking-induced muscle damage by non-damaging downhill walking. PLoS One. 2017;12(3):e0173909. doi:10.1371/journal.pone.0173909
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Listen to Me! – A Mixed-Methods Study of Thoughts and Attitudes Towards Participation in Pulmonary Telerehabilitation Among People with Severe and Very Severe COPD Who Declined Participation in Pulmonary Rehabilitation
Skibdal KM, Emme C, Hansen H
Patient Preference and Adherence 2022, 16:2781-2798
Published Date: 18 October 2022
Effect of Singing on Symptoms in Stable COPD: A Systematic Review and Meta-Analysis
Fang X, Qiao Z, Yu X, Tian R, Liu K, Han W
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2893-2904
Published Date: 14 November 2022
Exploring the Presence of Implicit Bias Amongst Healthcare Professionals Who Refer Individuals Living with COPD to Pulmonary Rehabilitation with a Specific Focus Upon Smoking and Exercise
Barradell AC, Robertson N, Houchen-Wolloff L, Singh SJ
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1287-1299
Published Date: 21 June 2023
Can Blood Biomarkers Be Used to Assess Oxidative Stress in COPD Patients After Pulmonary Rehabilitation
Beykumül A, Ersoy Y, Gülbaş G, Neselioglu S
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2179-2186
Published Date: 5 October 2023
Advocating for Action: Exploring the Potential of Virtual Reality in Breathing Exercise – A Review of The Clinical Applications
Alhammad SA
Patient Preference and Adherence 2024, 18:695-707
Published Date: 19 March 2024