Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Effects of Virtual Reality Interventions on Anxiety and Depression in Patients with Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis
Authors Chen S, Liu Z, Luo Y, Gong F, Wen H ![]()
Received 17 March 2026
Accepted for publication 25 June 2026
Published 13 July 2026 Volume 2026:21 605739
DOI https://doi.org/10.2147/COPD.S605739
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Zijing Zhou
Siling Chen,1,2,* Zhiqun Liu,3,* Yanqi Luo,1,2 Fanghua Gong,4 Hui Wen3
1School of Nursing, Hunan Normal University, Changsha, Hunan, 410013, People’s Republic of China; 2Kiang Wu Nursing College of Macau, Macau, People’s Republic of China; 3Department of Emergency Medicine, Hunan Provincial People’s Hospital (The First Affiliated Hospital of Hunan Normal University), Changsha, Hunan, 410005, People’s Republic of China; 4Department of Administration, Hunan Tuberculosis Prevention and Control Institute (Hunan Chest Hospital), Changsha, Hunan, 410013, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Fanghua Gong, Department of Administration, Hunan Tuberculosis Prevention and Control Institute (Hunan Chest Hospital), 519 Xianjiahu Road, Yuelu District, Changsha, Hunan, 410013, People’s Republic of China, Tel +86 13787189163, Email [email protected]
Background: The effectiveness of virtual reality (VR) technology in reducing anxiety and depression among patients with chronic obstructive pulmonary disease (COPD) remains uncertain. This study aimed to evaluate the impact of VR-based interventions on psychological outcomes in patients with COPD through a systematic review and meta-analysis.
Methods: A systematic search was conducted in 11 databases, including PubMed, Embase, Web of Science, the Cochrane Library, CINAHL, PsycINFO, China National Knowledge Infrastructure (CNKI), Wanfang Database, VIP Database, the Chinese Medical Journal Full-text Database (CMJD), and SinoMed, from database inception to February 11, 2026. Randomized controlled trials (RCTs) assessing the effects of VR interventions on anxiety or depression in patients with COPD were included. Two reviewers independently performed study screening, data extraction, and quality assessment, and the risk of bias was evaluated using the revised Cochrane risk-of-bias tool for randomized trials (RoB 2). Standardized mean differences (SMDs) with 95% confidence intervals (CIs) were calculated using a random-effects model in RevMan 5.4, and the certainty of evidence was assessed using the GRADE approach. The primary outcomes were changes in anxiety and depression symptoms.
Results: A total of 1,767 records were identified, of which 10 studies involving 673 patients with COPD met the inclusion criteria, and 9 studies were included in the meta-analysis. Because of substantial between-study heterogeneity, a random-effects model was used. Meta-analysis showed that, compared with control groups, VR interventions significantly reduced anxiety levels in patients with COPD [SMD = − 1.63, 95% CI (− 2.49, − 0.78), P = 0.0002, I2 = 95%] and reduced depressive symptoms [SMD = − 0.90, 95% CI (− 1.28, − 0.53), P < 0.00001, I2 = 77%].
Conclusion: VR-based interventions show potential for improving anxiety and depressive symptoms in patients with COPD and may serve as a valuable adjunct to conventional pulmonary rehabilitation. Nevertheless, the substantial heterogeneity observed across studies limits the certainty of the available evidence. Consequently, the findings should be interpreted with caution, and further rigorously designed, large-scale RCTs are needed to verify the long-term effectiveness of VR interventions and inform their optimal clinical implementation.
Keywords: virtual reality, COPD, anxiety, depression, systematic review, meta-analysis
Introduction
Chronic obstructive pulmonary disease (COPD) is a heterogeneous respiratory disorder characterized by persistent and usually progressive airflow limitation resulting from airway and/or alveolar abnormalities, leading to chronic respiratory symptoms such as dyspnea, cough, sputum production, and recurrent exacerbations.1 COPD is associated with high prevalence, disability, and mortality, imposing a substantial economic and societal burden worldwide. As the third leading cause of death globally, COPD affects more than 380 million people living with the disease.2,3 Global epidemiological studies estimate that the prevalence of COPD among individuals aged ≥40 years is approximately 10.3%, corresponding to nearly 391 million cases worldwide, of which more than 25% are classified as severe. The prevalence increases markedly with advancing age.1 Patients commonly experience persistent breathlessness, reduced exercise capacity, and recurrent acute exacerbations, which substantially impair quality of life and increase healthcare and financial burden.
As physiological function declines, mental health problems become increasingly prominent in patients with COPD.4 Psychological distress is closely associated with poorer clinical outcomes. Compared with patients without these comorbidities, those with anxiety or depression experience more frequent acute exacerbations, higher rehospitalization rates, and an increased risk of mortality.5–7 Through both neuroimmune dysregulation and maladaptive behavioral responses, anxiety and depression may increase healthcare utilization and all-cause mortality and serve as independent predictors of poor prognosis.8,9 The global prevalence of comorbid anxiety and depression in patients with COPD is estimated to reach up to 40%,1 which is substantially higher than that observed in the general population.10
Effective interventions are needed to address symptoms of anxiety and depression in patients with COPD. Current clinical guidelines recommend a multimodal approach, including pharmacological treatment, cognitive behavioral therapy, and traditional pulmonary rehabilitation (PR) combined with psychological support.5,11,12 As a cornerstone of comprehensive COPD management, PR improves exercise capacity and quality of life, relieves dyspnea, and, when combined with psychological or behavioral strategies, has also been shown to reduce symptoms of anxiety and depression.10,13 However, access to and completion of center-based PR are frequently limited by high costs, geographic and logistical barriers, and low referral rates, and its psychological benefits remain modest for some patients, highlighting the need for innovative and engaging therapeutic approaches.14 In recent years, virtual reality (VR)-based interventions have emerged as a novel approach in the management and rehabilitation of patients with COPD. VR has increasingly been incorporated into PR as a complementary tool and has also been applied in usual care, breathing or relaxation training, and home-based rehabilitation.15,16
VR technology is a computer-generated interactive environment that provides users with immersive multisensory experiences. It has been increasingly applied in medical rehabilitation, with its core function involving the simulation of real or virtual scenarios through multimodal stimuli, including visual, auditory, and tactile feedback. Such features may enhance patient engagement and motivation, thereby improving adherence to rehabilitation programs.15 In the rehabilitation of patients with COPD, VR technology can not only deliver conventional exercise and breathing training but also incorporate psychological interventions, such as relaxation training and mindfulness-based practices, to help alleviate anxiety and depression. Through gamified design and scenario-based simulation, VR may strengthen psychological support and emotional regulation, potentially reducing anxiety and depressive symptoms while simultaneously promoting physiological recovery.
VR technology can be classified into three categories according to the level of immersion: immersive, semi-immersive, and non-immersive systems. Among these, immersive VR is currently regarded as the most representative form.17 Immersive VR isolates users from the real environment through head-mounted displays and integrates visual, auditory, and kinesthetic feedback to create highly realistic multisensory experiences. It can simulate exercise environments such as forests, beaches, or urban parks, allowing patients to perform walking, running, or upper-limb training in virtual settings, which may improve exercise tolerance and respiratory function.18,19 In addition, immersive environments may reduce external distractions and negative emotional triggers, thereby helping to interrupt anxiety cycles. Through social interaction features and goal-oriented feedback, VR may enhance patients’ sense of achievement and provide potential benefits in alleviating depressive symptoms.20 Non-immersive VR primarily relies on computer or screen-based interfaces to present virtual environments while users remain aware of their real surroundings. Although the level of immersion is lower, it still allows a degree of interactivity. When combined with breathing exercises, real-time feedback on respiratory rate and patterns may help patients develop more effective breathing strategies and relieve dyspnea.21 However, limited situational engagement and social interaction, together with environmental distractions, may restrict its psychological benefits.22 In recent years, motion-based interactive games have become an important application of VR technology, enabling physical participation through motion capture, and they are now widely used in PR for patients with COPD.23 Common VR systems include Kinect, Nintendo Wii, HTC Vive headsets, and the BioMaster virtual scenario training platform.24 With the development of telemedicine, home-based rehabilitation models integrating artificial intelligence and VR have gradually emerged. Related clinical practices have been initiated in the United States, and a non-inferiority study of remote VR PR has been completed in the Ningxia region of China, suggesting a potential low-cost implementation pathway.16 Therefore, a systematic evaluation of the effectiveness of VR in managing anxiety and depression among patients with COPD is of considerable clinical importance.
To date, research on VR in patients with COPD has focused predominantly on physical outcomes, with systematic reviews indicating that VR-assisted rehabilitation may improve exercise tolerance, relieve dyspnea, and enhance treatment adherence and health-related quality of life.25 Beyond its physical effects, VR may also positively influence anxiety and depression, which are common comorbidities in patients with COPD, through mechanisms such as attentional redirection, situational exposure, and emotional regulation. However, evidence regarding these psychological benefits remains comparatively limited and inconsistent. Several studies have reported significant improvements in anxiety and depression following VR interventions,18,19,21,26,27 whereas others have found no significant between-group differences in anxiety outcomes.28 Moreover, existing reviews have largely examined anxiety and depression as secondary rather than primary endpoints, and no meta-analysis has yet specifically synthesized the psychological effects of VR in patients with COPD.15,25 Differences in the level of immersion, intervention content, and comparator conditions across studies may further contribute to these inconsistent findings and have not been systematically evaluated. Therefore, synthesizing the available evidence through a systematic review and meta-analysis is necessary to better evaluate the effectiveness and stability of VR-based interventions for anxiety and depression in patients with COPD.
Therefore, this study conducted a systematic review and meta-analysis to evaluate the effects of VR technology on anxiety and depression in patients with COPD, synthesizing current evidence and quantitatively assessing the psychological outcomes reported in existing studies.
Materials and Methods
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines and prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO) on March 11, 2025 (registration number: CRD420251001032). Following the completion of the study selection process, only a limited number of studies meeting the inclusion criteria were identified. Consequently, the protocol was revised on February 4, 2026, with the following amendments: (1) the addition of disease staging and intervention setting to the data extraction items; (2) removal of the restriction that the control group receive PR only, to allow for usual care or other comparators; and (3) an updated literature search extended to February 11, 2026, with the addition of PsycINFO to the database list and the inclusion of grey literature sources such as CNKI dissertations.
Literature Search
To identify relevant studies, two researchers (SC and YL) independently searched PubMed, Embase, Web of Science, the Cochrane Library, CINAHL, PsycINFO, China National Knowledge Infrastructure (CNKI), Wanfang Database, VIP Database, the Chinese Medical Journal Full-text Database (CMJD), and SinoMed. Studies published in English and Chinese from database inception to February 11, 2026 were considered eligible. The search strategy included the following terms and their related variants: “virtual reality”, “VR”, “digital therapy”, “interactive videogame”, “chronic obstructive pulmonary disease”, “chronic obstructive lung disease”, “COPD”, “anxiety”, “depression”, and “negative emotions”. The detailed search strategy is provided in Supplementary Material. To ensure comprehensive coverage, grey literature sources, including the World Health Organization International Clinical Trials Registry Platform (WHO ICTRP) and CNKI dissertations, were also searched. EndNote X9 was used for literature management and duplicate removal. Literature searching and study screening were conducted independently by two researchers according to predefined criteria. Inter-rater agreement between the two reviewers (SC and YL) for the title and abstract screening was assessed using Cohen’s κ coefficient. Any disagreements were resolved through discussion until consensus was reached, or by consultation with a third reviewer (HW).
Inclusion and Exclusion Criteria
Randomized controlled trials(RCTs) minimize selection bias and control for confounding through random allocation and are considered the gold standard for evaluating intervention efficacy. Therefore, only RCTs were included to ensure the validity and quality of the evidence in this meta-analysis.
Studies were included according to the PICOS framework if they met the following inclusion criteria:
- Population (P): patients diagnosed with COPD;
- Intervention (I): the intervention group received VR-based training (eg, immersive or non-immersive VR, exergaming, or interactive video games);
- Comparison (C): the control group received conventional PR or usual care (eg, routine pharmacological management or health education);
- Outcomes (O): at least one outcome measure of anxiety or depression assessed using a validated scale;
- Study design (S): RCTs.
In addition, only studies published in English or Chinese were included.
The exclusion criteria were as follows:
- studies that did not report outcomes related to anxiety or depression in patients with COPD following VR intervention;
- irrelevant publications, conference abstracts, letters, or commentaries;
- studies for which the full text was unavailable;
- duplicate publications or studies with incomplete data; and
- studies with missing essential information for which the authors could not be contacted.
Data Extraction
The primary objective of this systematic review and meta-analysis was to evaluate the effects of VR interventions on anxiety and depression in patients with COPD, with primary outcomes defined as changes in anxiety and depressive symptoms. Two researchers independently extracted data and assessed the methodological quality of the included studies as well as the accuracy of the extracted information. Any disagreements were resolved through discussion with a third researcher(HW). Extracted data included the first author, publication year, country, participant characteristics (patient source, age, disease stage, and sample size), intervention characteristics (implementation setting, control condition, intervention group, platform, content, and frequency), and outcome assessment measures.
Quality Assessment of Included Studies
Two researchers independently assessed the risk of bias in the included studies using the revised Cochrane risk-of-bias tool for randomized trials (RoB 2),29 in accordance with the latest recommendations of the Cochrane Handbook. The assessment evaluated potential bias arising from the randomization process, deviations from intended interventions, missing outcome data, outcome measurement, and selective reporting of results. Each study was categorized as having a low risk of bias, some concerns, or a high risk of bias. The assessment results were cross-checked by the two reviewers. Any disagreements were resolved through discussion or consultation with a third researcher.
Statistical Analysis
The primary outcomes of this systematic review and meta-analysis were the effects of VR technology on anxiety and depression in patients with COPD. Heterogeneity among studies was evaluated using the χ2 test and the I2 statistic. Significant heterogeneity was considered present when P ≤ 0.10 and I2 ≥ 50%, in which case a random-effects model was applied. Pooled effect sizes with 95% confidence intervals (CIs) were calculated, and standardized mean differences (SMDs) were used to combine outcomes measured using different assessment scales. Effect sizes were calculated based on the differences in outcome measures between the intervention and control groups at the end of the trials. An SMD ≥ 0.8 was interpreted as a large effect, 0.5–0.79 as a moderate effect, and 0.2–0.49 as a weak effect.30 Meta-analysis was performed using RevMan 5.4 software. All statistical tests were two-sided, and P < 0.05 was considered statistically significant. Sensitivity analyses were conducted to assess the robustness of the results. The certainty of the evidence was assessed using GRADE. Subgroup analyses were conducted to explore potential sources of clinical heterogeneity according to VR immersion type (immersive vs non-immersive), control-group type (PR vs usual care or health education), intervention content (exercise-based, breathing/relaxation-based, or mixed), and study region (China vs non-China). These subgroup variables were selected a priori based on clinical relevance and plausible mechanisms that might influence intervention effectiveness. Subgroup analyses were performed only when at least two studies were available within each subgroup. Differences between subgroups were assessed using the test for subgroup interaction. Given the limited number of included studies and the absence of adjustment for multiple comparisons, all subgroup findings were considered exploratory and interpreted with caution.
Results
Search Results
A total of 1,767 records were identified through searches across 11 databases (Figure 1). After removing duplicates and screening titles and abstracts, 1,734 records were excluded for not meeting the study objectives, leaving 33 articles for full-text assessment. The inter-rater agreement for title and abstract screening yielded a Cohen’s κ value of 0.88. Following full-text review, 23 articles were excluded for the following reasons: 2 did not meet the study design criteria, 4 did not meet the study type criteria, 6 did not involve VR interventions, 9 were unavailable in full text, and 2 had inaccessible data. Ultimately, 10 studies were included in this review. Among the 10 included studies, 6 were conducted in China and 4 were conducted in other countries. One study demonstrated a skewed distribution of post-intervention data and was therefore included only in the systematic review, whereas data from the remaining 9 studies were included in the meta-analysis.
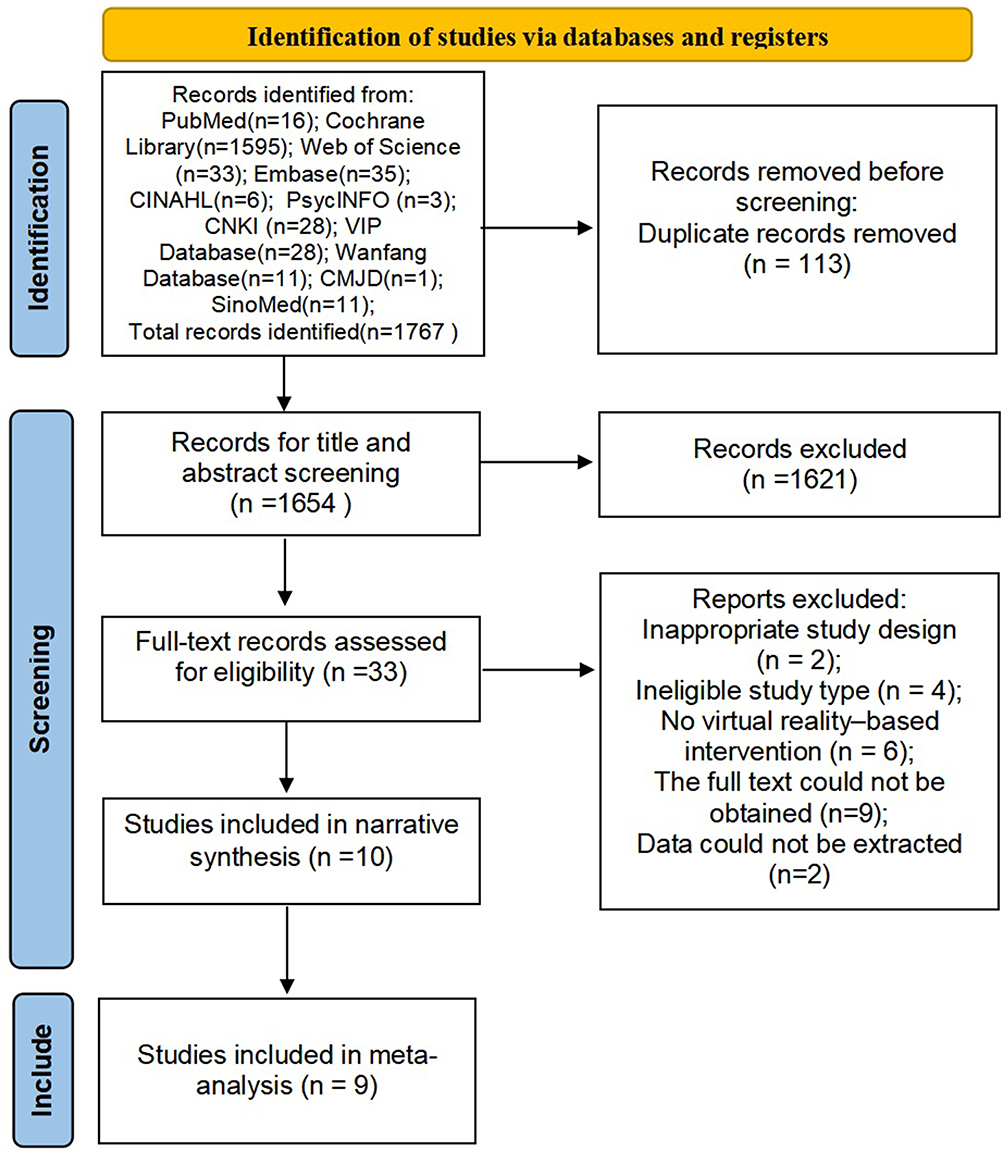 |
Figure 1 PRISMA flowchart of study selection. |
Study Characteristics
The basic characteristics of the included studies are summarized in Table 1. A total of 10 studies,18,19,21,23,26–28,31–33 involving 673 patients with COPD, were included in this review. Extracted data included the first author, publication year, country, participant age, intervention setting, disease stage, sample size, study design, intervention characteristics, and outcome measures. All studies were published between 2014 and 2025. Geographically, the included studies were conducted in four countries: China (n = 6), Turkey (n = 2), Poland (n = 1), and Italy (n = 1) (Figure 2). According to intervention format, five studies employed immersive VR technology,18,19,27,32,33 whereas the remaining five used non-immersive VR technology.21,23,26,28,31 Nine studies evaluated the effects of VR on anxiety outcomes.18,19,21,23,26–28,31,33 Among these, five studies assessed anxiety using the Hospital Anxiety and Depression Scale (HADS),18,19,23,26,31 while the others used the HADS-anxiety subscale (HADS-A),27 the Self-Rating Anxiety Scale (SAS),21 the State–Trait Anxiety Inventory (STAI),28 and the COPD Quality of Life Scale (COPD-QOL).33 In addition, nine studies reported depression outcomes.18,19,21,23,26,28,31–33 Most studies used HADS to assess depression,18,19,23,26,31 whereas the remaining studies applied the Self-Rating Depression Scale (SDS),21 the Beck Depression Inventory (BDI),28 the Hamilton Depression Rating Scale (HAMD-17),32 and the COPD-QOL.33
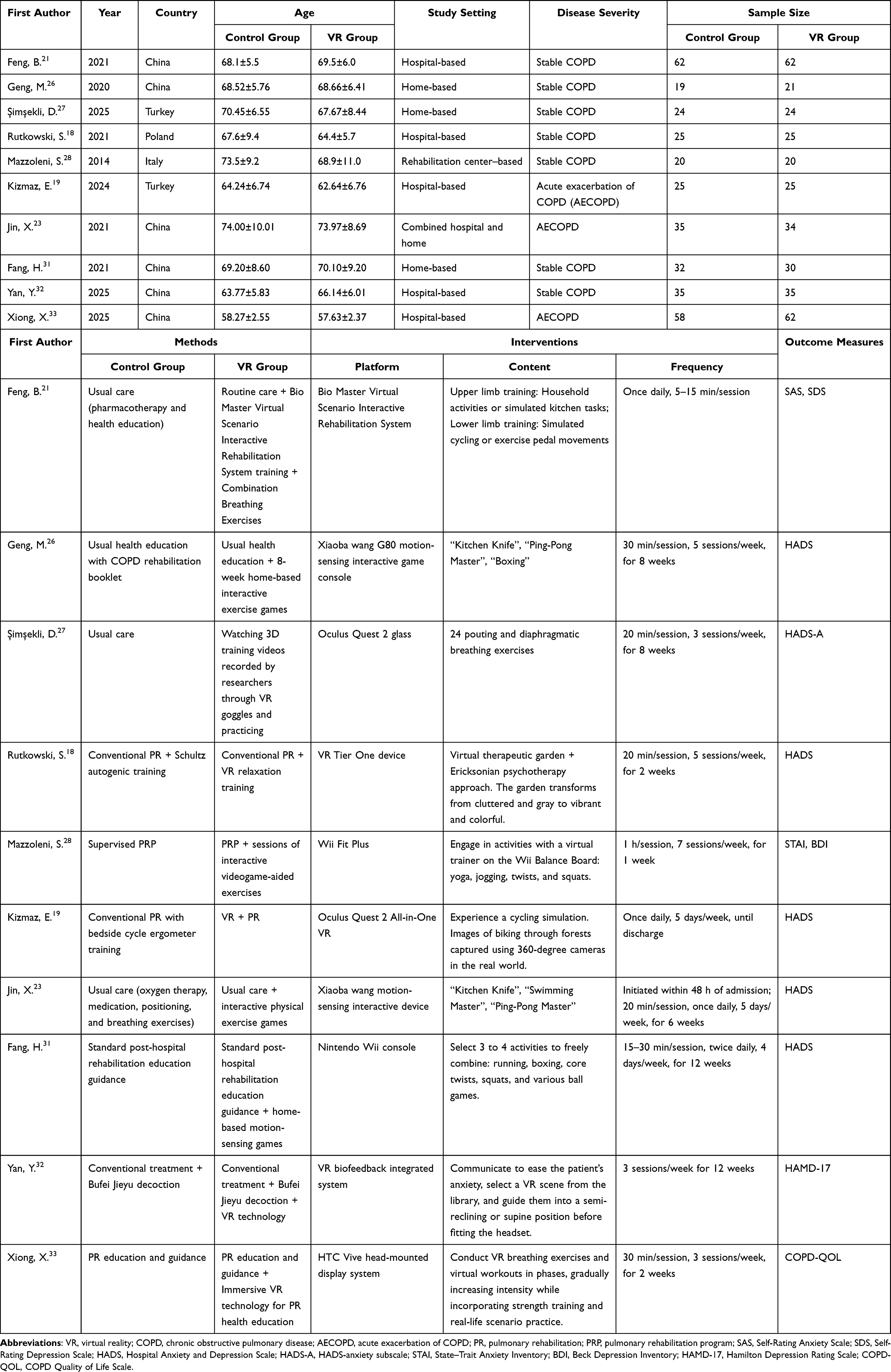 |
Table 1 Characteristics of All Studies Included |
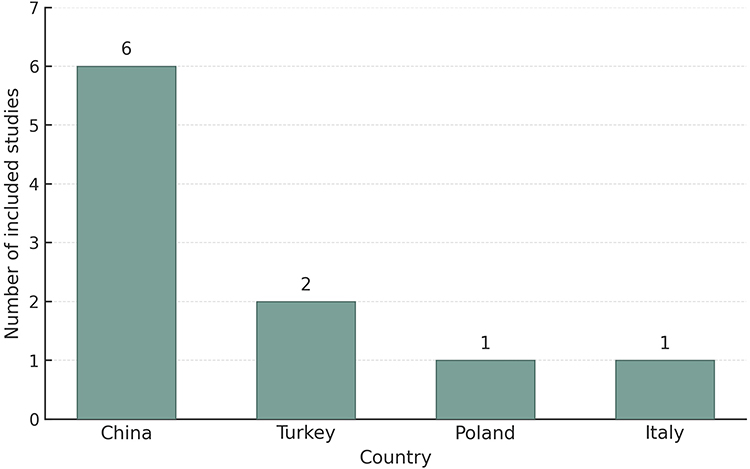 |
Figure 2 Geographic distribution of the included studies by country. |
Quality Assessment
The methodological quality of the included studies was assessed using the RoB 2. The results of the risk-of-bias assessment are presented in Table 2 and are further illustrated in the risk of bias summary (Figure 3) and risk of bias traffic light plot (Figure 4).
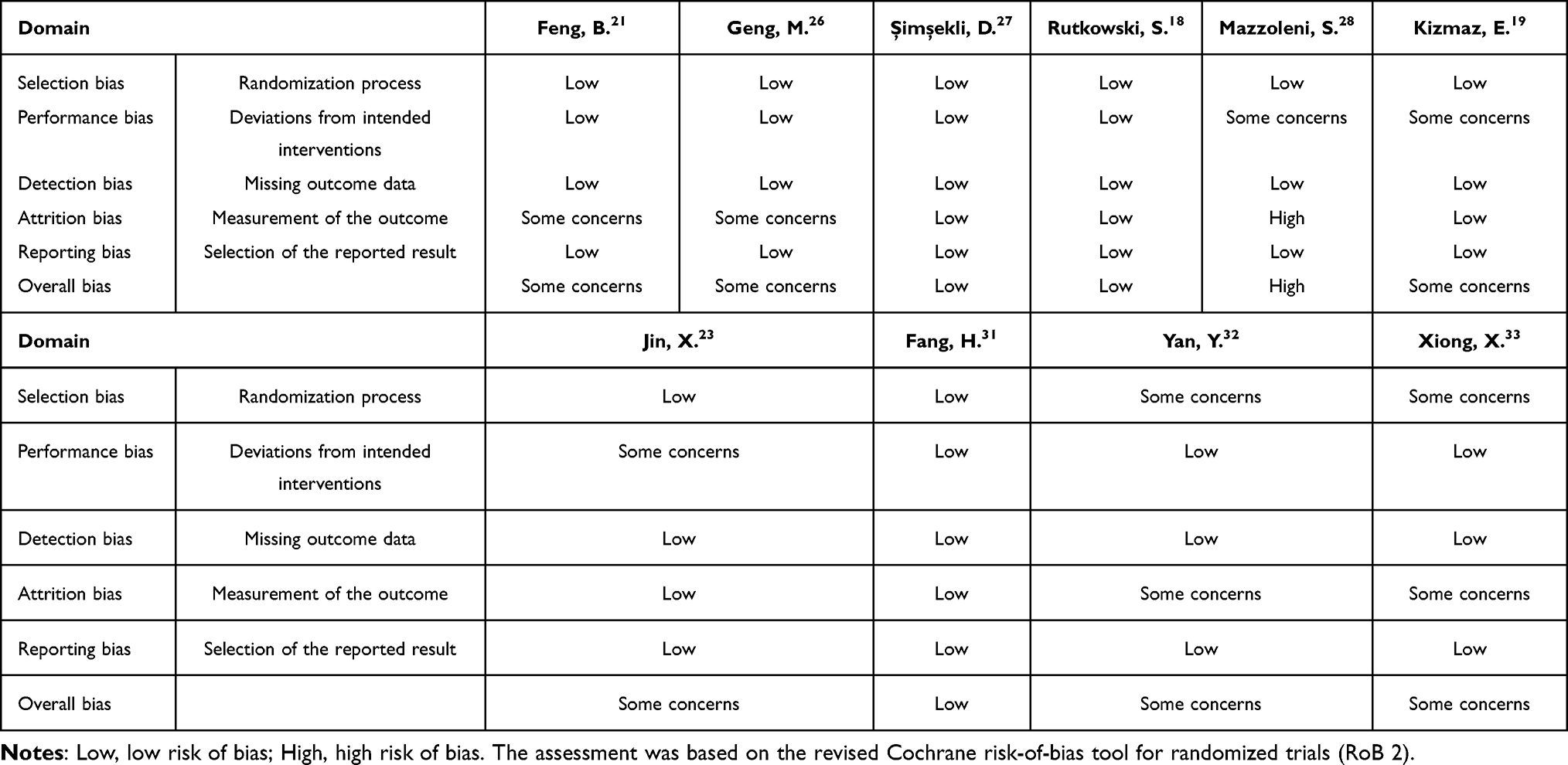 |
Table 2 Methodological Quality Assessment of the Included Studies Based on the Cochrane Risk of Bias Tool |
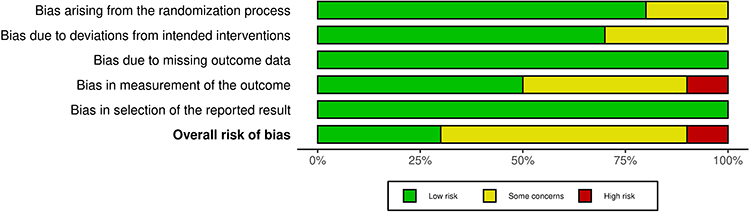 |
Figure 3 Risk-of-bias summary of the included studies assessed using the RoB 2. |
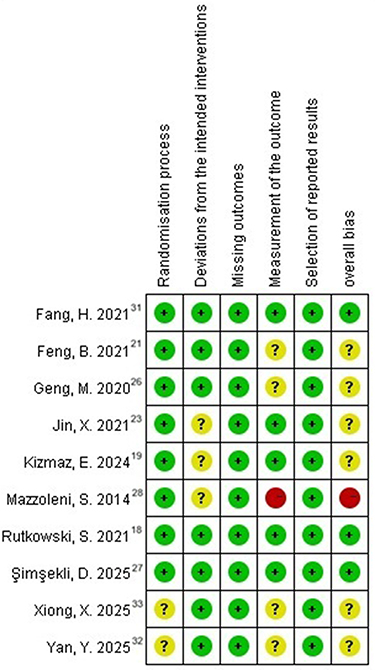 |
Figure 4 Risk-of-bias traffic light plot of the included studies assessed using the RoB 2. |
Overall, the included studies demonstrated acceptable methodological quality. All studies were rated as having a low risk of bias for missing outcome data and selection of reported results. Most studies were also judged as having a low risk of bias in the domains of the randomization process and deviations from intended interventions, although some concerns were identified in a minority of studies. The domain of outcome measurement showed the greatest risk of bias, with four studies rated as having some concerns and one study rated as high risk. Overall, three studies were judged as having a low risk of bias, six as having some concerns, and one as having a high risk of bias.
The quality of evidence for the included outcomes was assessed using the GRADE approach, and the results are presented in Table 3.
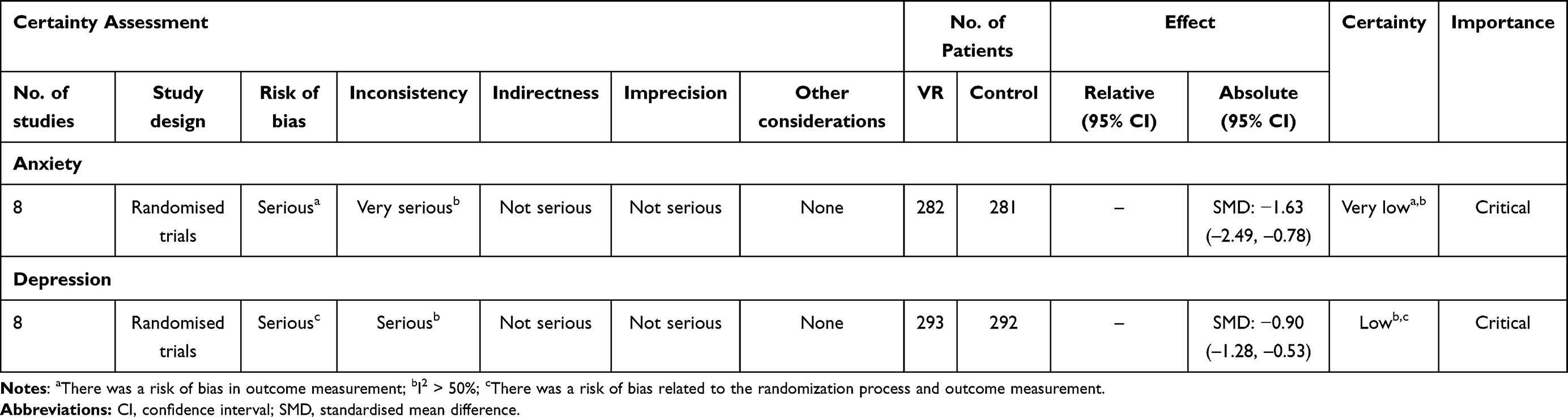 |
Table 3 GRADE Evaluation Results |
Results of Systematic Review and Meta-Analysis
Anxiety
Figure 5 presents the meta-analysis results of VR interventions on anxiety outcomes in patients with COPD. A total of nine studies assessed anxiety outcomes,18,19,21,23,26–28,31,33 of which eight were included in the meta-analysis. The pooled analysis showed that VR intervention significantly reduced anxiety levels compared with the control group [SMD = −1.63, 95% CI (−2.49, −0.78), P = 0.0002]. Given the substantial heterogeneity among studies (I2 = 95%), a random-effects model was applied. Among the five studies using the HADS,18,19,23,26,31 the study by Geng et al26 was excluded from the meta-analysis because of a skewed post-intervention data distribution and was included only in the systematic review. That study reported significantly lower anxiety scores after intervention compared with both baseline and the control group (P < 0.05). Meta-analysis of the remaining four studies showed significant heterogeneity (I2 = 86%, P < 0.0001). The random-effects model indicated that VR intervention significantly reduced anxiety [SMD = −0.79, 95% CI (−1.54, −0.04), P=0.04]. The remaining studies used different assessment instruments. Studies employing the HADS-A27 and the SAS21 reported significant pre–post improvements following intervention. The study using the STAI28 demonstrated only slight improvement in state anxiety in the control group, with no improvement observed in the intervention group. The study using the COPD-QOL33 also reported lower anxiety scores in the VR group compared with both pre-intervention levels and the control group.
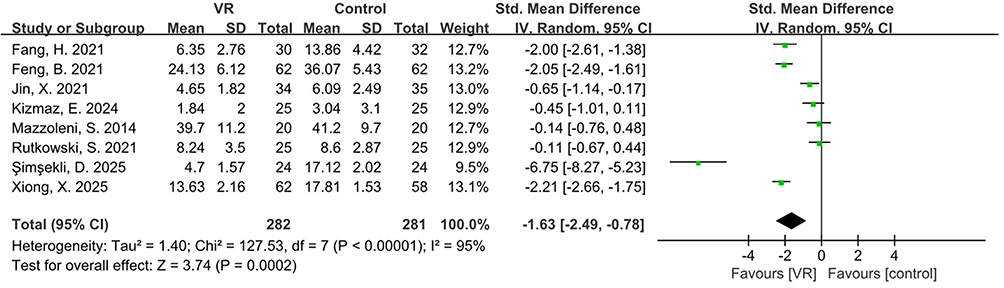 |
Figure 5 Forest plot of the effects of VR interventions on anxiety in patients with COPD. |
Depression
Figure 6 presents the meta-analysis results of VR interventions on depressive outcomes in patients with COPD. A total of nine studies assessed depressive outcomes,18,19,21,23,26,28,31–33 of which eight were included in the meta-analysis. The pooled analysis showed that VR intervention significantly reduced depression levels compared with the control group [SMD = −0.90, 95% CI (−1.28, −0.53), P<0.00001]. Moderate to high heterogeneity was observed among studies (I2 = 77%); therefore, a random-effects model was applied. Among the five studies using the HADS,18,19,23,26,31 the study by Geng et al26 was excluded from the meta-analysis because of a skewed post-intervention data distribution and was included only in the systematic review. That study reported significantly lower depression scores after intervention compared with both baseline and the control group (P<0.05). Meta-analysis of the remaining four studies continued to show heterogeneity (I2=76%, P = 0.005). The random-effects model indicated that VR intervention significantly reduced depressive symptoms [SMD=−0.79, 95% CI (−1.35, −0.23), P=0.006]. The remaining studies used different assessment instruments. The study using the SDS21 reported significant reductions in depressive symptoms after intervention. The study using the BDI28 demonstrated improvement in both groups, although between-group differences were not statistically significant. Studies employing the HAMD-1732 and the COPD-QOL33 both reported lower depression scores in the VR group compared with pre-intervention levels and the control group.
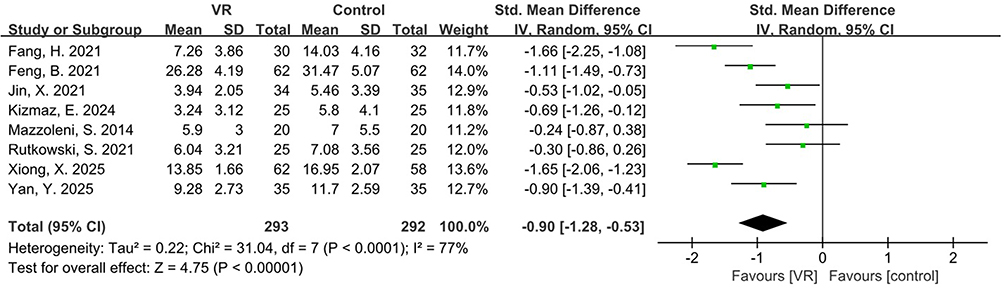 |
Figure 6 Forest plot of the effects of VR interventions on depression in patients with COPD. |
Subgroup Analysis
Subgroup Analysis Based on VR Modality (Immersive vs Non-Immersive VR) for Anxiety Outcomes
Figure 7 presents a subgroup analysis comparing the effects of immersive versus non-immersive VR on anxiety levels in patients with COPD. Overall, VR intervention, combining immersive and non-immersive formats, significantly reduced anxiety [SMD=−1.63, 95% CI (−2.49, −0.78), P=0.0002, I2 =95%]. Subgroup analysis suggested a trend toward greater efficacy for immersive VR [SMD = −2.21, 95% CI (−3.94, −0.49), P=0.01, I2=97%] compared with non-immersive VR [SMD = −1.22, 95% CI (−2.14, −0.29), P=0.01, I2=92%]. Although the pooled effect estimate appeared larger for immersive VR than for non-immersive VR, the between-subgroup difference was not statistically significant (P = 0.32).
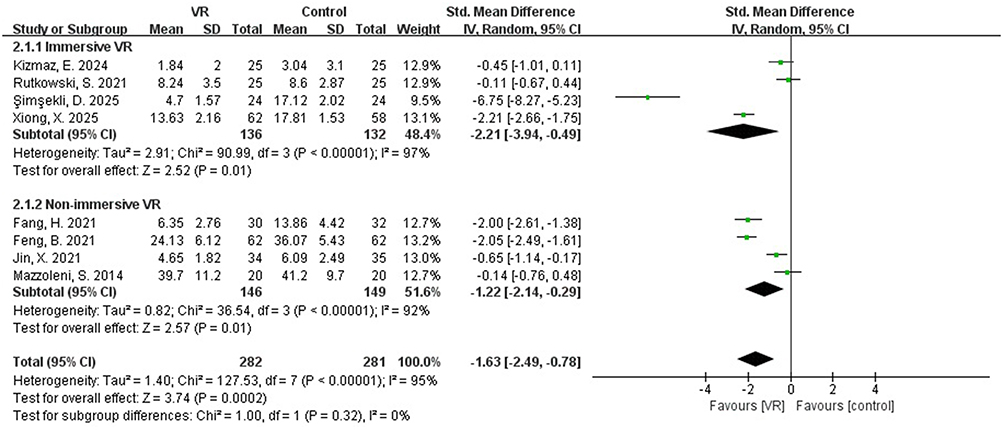 |
Figure 7 Forest plot of subgroup analysis comparing immersive and non-immersive VR interventions on anxiety in patients with COPD. |
Subgroup Analysis Based on VR Modality (Immersive vs Non-Immersive VR) for Depression Outcomes
Figure 8 presents a subgroup analysis comparing the effects of immersive versus non-immersive VR on depressive status in patients with COPD. Overall, VR intervention combining immersive and non-immersive approaches significantly reduced depressive symptoms [SMD = −0.90, 95% CI (−1.28, −0.53), P < 0.00001, I2 = 77%]. Subgroup analysis suggested that immersive VR showed significant benefits compared with the control group [SMD = −0.91,95% CI (−1.50,-0.31), P = 0.003], although high between-study heterogeneity was observed (I2 = 82%). Non-immersive VR also significantly improved depressive symptoms [SMD=−0.89, 95% CI (−1.44,-0.34), P=0.001], with substantial heterogeneity (I2=79%). No statistically significant difference was found between immersive and non-immersive VR (P = 0.98), indicating that VR interventions with different levels of immersion showed comparable efficacy in alleviating depressive symptoms in patients with COPD.
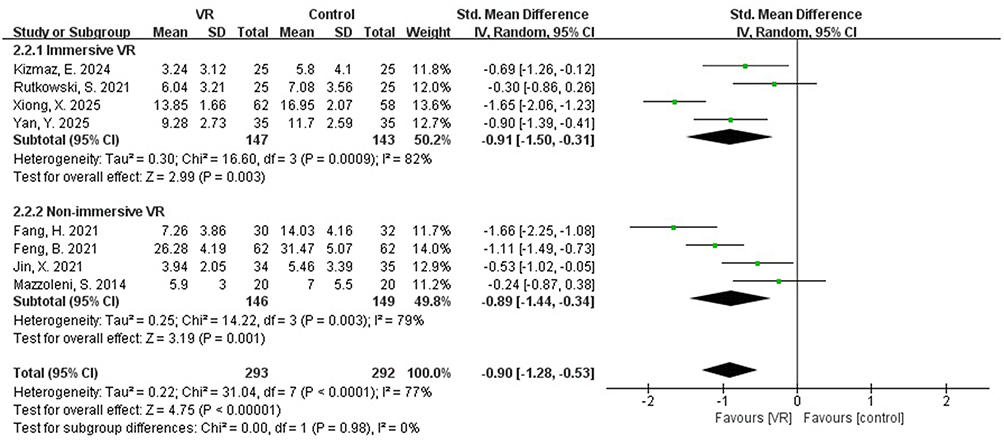 |
Figure 8 Forest plot of subgroup analysis comparing immersive and non-immersive VR interventions on depression in patients with COPD. |
Subgroup Analysis Based on Control Group Type for Anxiety Outcomes
Figure 9 shows the subgroup analysis examining the influence of control group settings on anxiety outcomes in patients with COPD. In studies in which the control group received conventional PR, no statistically significant difference in anxiety improvement was observed between the VR and control groups [SMD = −0.74, 95% CI (−1.82, 0.34), P=0.18], and considerable heterogeneity was identified (I2 = 94%). In contrast, when the control group received only routine care or health education, VR produced a significant and large improvement in anxiety symptoms [SMD=−2.64, 95% CI (−4.05, −1.23), P=0.0002], although substantial heterogeneity remained (I2 = 95%). The subgroup comparison was statistically significant (P = 0.04), indicating that differences in control group design may represent an important source of heterogeneity across studies.
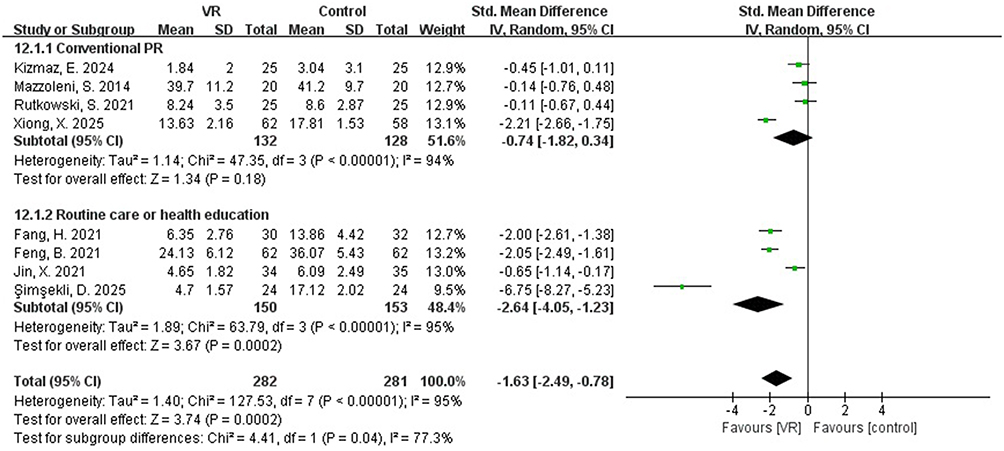 |
Figure 9 Forest plot of subgroup analysis based on control group type for anxiety outcomes in patients with COPD. |
Subgroup Analysis Based on Intervention Content for Anxiety Outcomes
Figure 10 shows a subgroup analysis examining the influence of intervention content (exercise-based, breathing or relaxation training-based, and mixed interventions) on anxiety outcomes in patients with COPD. Exercise-based VR interventions demonstrated significantly greater improvement in anxiety symptoms compared with the control group [SMD = −0.81, 95% CI (−1.55, −0.06), P = 0.03], although substantial heterogeneity was observed (I2 = 85%). For breathing or relaxation training-based interventions, the pooled effect size was large but did not reach statistical significance [SMD = −3.39, 95% CI (−9.90, 3.12), P = 0.31], with considerable heterogeneity (I2 = 98%). Mixed interventions combining exercise with breathing or relaxation training showed significant improvements in anxiety symptoms with large effect sizes [SMD=−2.13, 95% CI (−2.44, −1.81), P<0.00001] and no detected heterogeneity (I2 = 0%). The subgroup comparison indicated significant differences among intervention types (P = 0.005), suggesting that intervention content may represent an important source of heterogeneity, with the combined intervention model demonstrating the most consistent and pronounced effects.
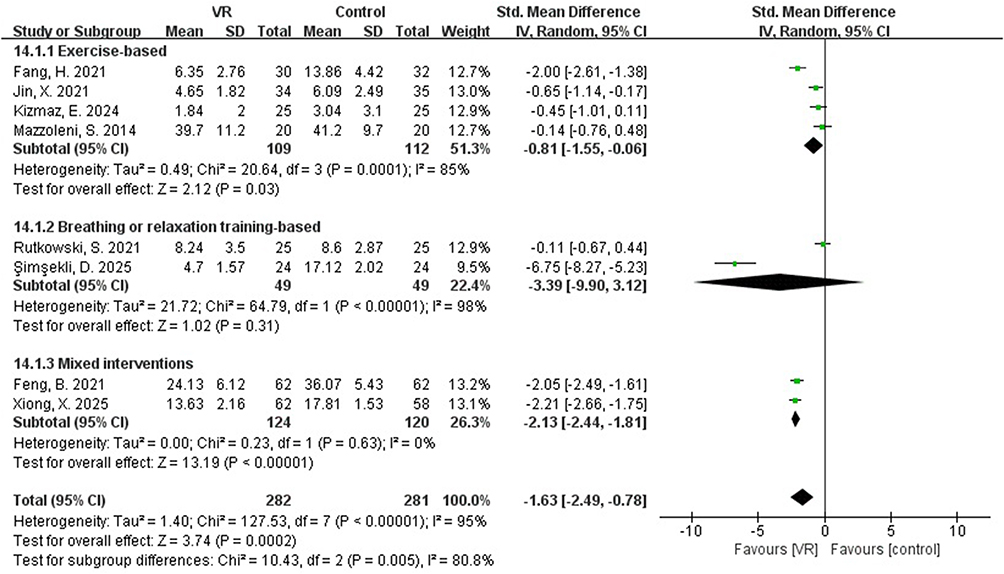 |
Figure 10 Forest plot of subgroup analysis based on intervention content for anxiety outcomes in patients with COPD. |
Subgroup Analysis Based on Study Region for Depression Outcomes
Figure 11 shows a subgroup analysis evaluating regional differences (China versus non-China) in the effects of VR on depressive status among patients with COPD. In studies conducted in China, VR demonstrated significantly greater improvement in depressive symptoms compared with control interventions [SMD = −1.17, 95% CI (−1.58, −0.76), P<0.00001], although substantial heterogeneity was observed (I2 = 75%). In non-China studies, VR interventions also significantly improved depressive symptoms [SMD = −0.42, 95% CI (−0.76, −0.08), P = 0.01], with no evident heterogeneity (I2 = 0%). Subgroup comparison indicated significant differences in effect sizes between regions (P = 0.006), suggesting that study region may represent an important source of heterogeneity. Overall, studies conducted in China showed relatively larger intervention effects.
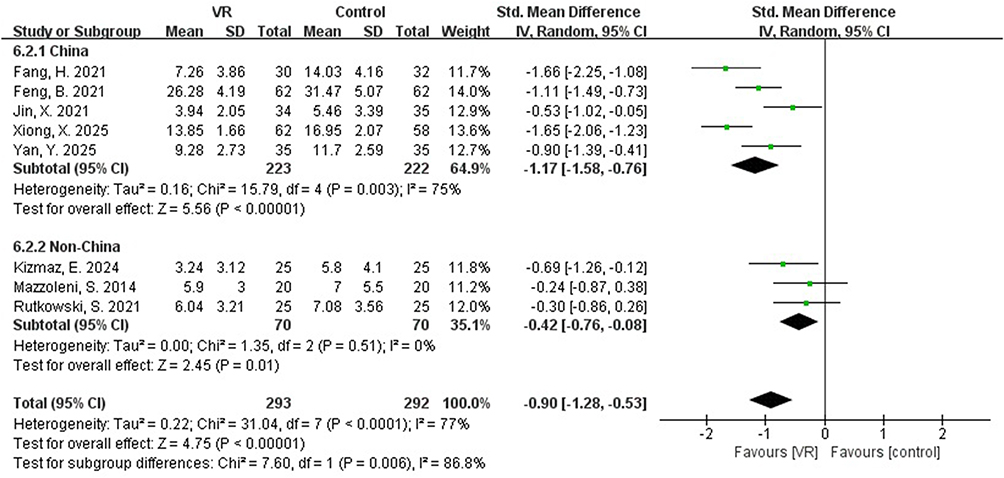 |
Figure 11 Forest plot of subgroup analysis based on study region for depression outcomes in patients with COPD. |
Overall Results of Subgroup Analyses for Anxiety and Depression Outcomes
To facilitate comparison across outcomes, the main findings of the subgroup analyses are summarized in Table 4. In the forest plot, estimates located to the left of the line of no effect favor the VR group, whereas those to the right favor the control group.
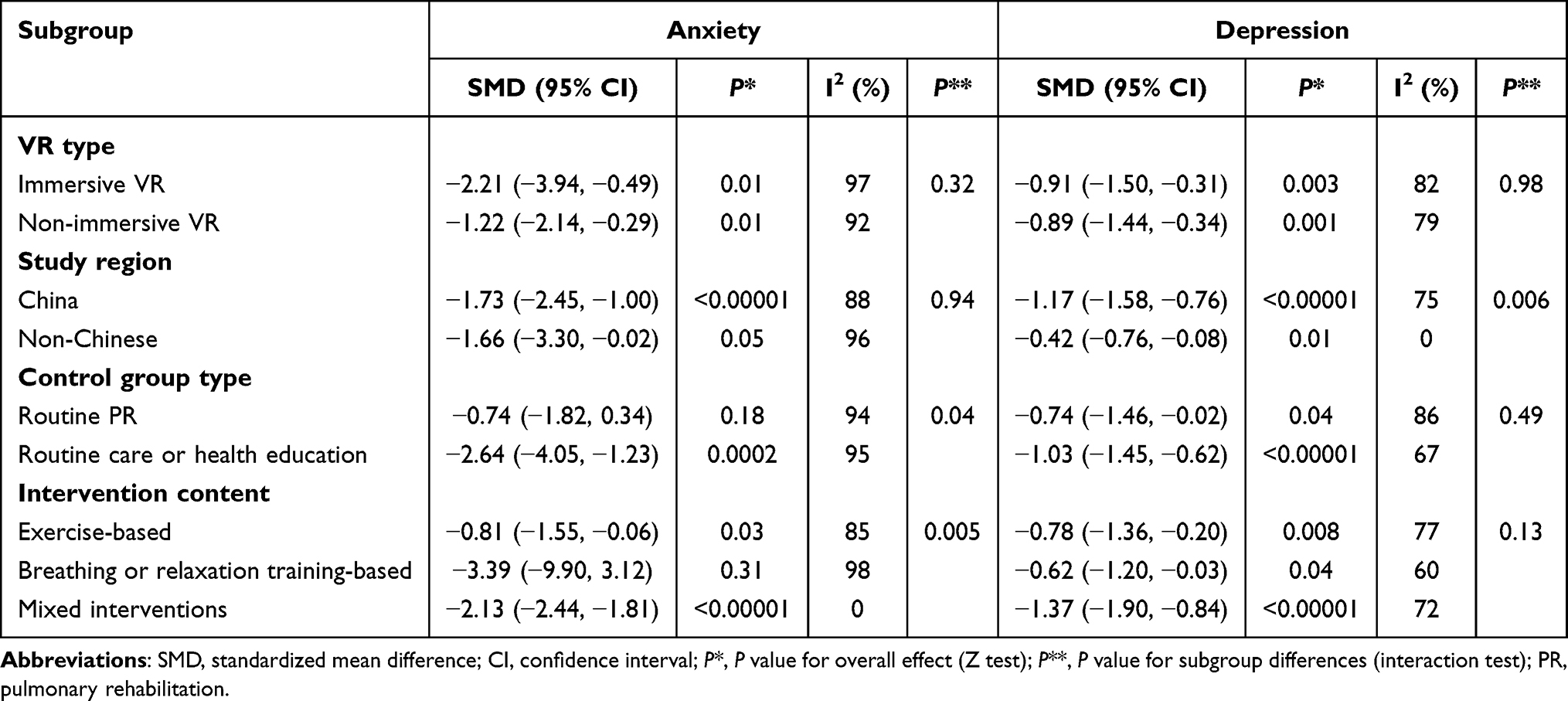 |
Table 4 Subgroup Analyses of the Effects of VR–Based Interventions on Anxiety and Depression in Patients with COPD |
Sensitivity Analysis and Publication Bias
Given the high heterogeneity (I2 ≥ 50%) observed in the pooled analyses of both anxiety and depression outcomes, sensitivity analyses were performed using a stepwise exclusion approach to explore potential sources of heterogeneity. For anxiety outcomes, the direction of the pooled effect size remained unchanged after sequential exclusion of individual studies, indicating overall robustness of the findings. Exclusion of the study by Şimşekli et al resulted in relatively large changes in both heterogeneity and effect size (I2 = 92%, P < 0.00001), with a pooled estimate of [SMD = −1.10, 95% CI (−1.81, −0.38), P = 0.003], suggesting that this study may have substantially influenced the overall results. Sensitivity analysis for depressive outcomes showed consistent findings, with the overall effect direction remaining stable after sequential exclusion. When the study by Xiong et al was removed, heterogeneity decreased markedly (I2 = 68%, P = 0.005), yielding a pooled effect size of [SMD = −0.79, 95% CI (−1.13, −0.45), P < 0.00001], indicating that this study may represent a potential source of heterogeneity. According to methodological recommendations for meta-analyses, funnel plots are generally used to assess publication bias when at least 10 studies are included.34 As fewer than 10 studies were available for each outcome in the present meta-analysis, funnel plot analysis was not conducted.
Discussion
This systematic review and meta-analysis suggests that VR-based interventions may reduce symptoms of anxiety and depression in patients with COPD compared with conventional PR or standard care. Subgroup analyses revealed no significant difference between immersive and non-immersive formats, whereas comparator type and intervention content emerged as potential effect modifiers. However, given the substantial heterogeneity, the variability in intervention characteristics, and the small number of included studies, these findings should be interpreted with caution and require confirmation in adequately powered RCTs.
The findings of this study are consistent with previous RCTs and systematic reviews,35–37 suggesting that VR interventions may alleviate anxiety through multiple interacting mechanisms. Immersive VR appears to promote emotional regulation through multisensory engagement; visual, auditory, and interactive feedback can redirect attention away from dyspnea and disease-related stimuli and reduce anxiety-related cognitive burden,38 helping to interrupt the cycle linking dyspnea, fear, and anxiety.24 Integrating VR with diaphragmatic and pursed-lip breathing training may further reduce hypoxia-related anxiety at the physiological level,39 while exposure to relaxing natural scenes may add mind-body benefits through parasympathetic activation and reduced cortisol.40,41 By contrast, non-immersive VR may rely more on cognitive and behavioral mechanisms, as real-time visualization of respiratory parameters and immediate feedback can strengthen self-efficacy and reduce the anxiety associated with a perceived loss of control.42 More broadly, VR of either type may improve engagement and adherence through interactive tasks and encourage a shift from avoidance to active participation, contributing to a regulatory pathway that combines attentional redirection, behavioral activation, and a restored sense of control.21,27,37
The findings of this study suggest that VR interventions may be associated with greater reductions in depressive symptoms than conventional PR and usual care.43 Immersive VR may enhance engagement through situational immersion and progressively challenging tasks, and repeated successful experiences may help reduce the learned helplessness common in chronic disease,44 while virtual social or multiplayer environments may alleviate disease-related social isolation and provide emotional support.45 Non-immersive VR appears to act mainly through behavioral reinforcement and reward-based mechanisms.46 Home-based or remotely delivered training can reduce time- and location-related barriers and improve continuity, and phased goals and reward systems may activate neural reward pathways that help restore motivation and counter the behavioral withdrawal associated with low mood.42 Compared with conventional care, which often lacks immediate feedback, the continuous positive reinforcement and enhanced self-efficacy afforded by VR may serve as key psychological mediators of improvement in depression.47
Subgroup analyses showed that both immersive and non-immersive VR produced significant therapeutic effects, with no statistically significant difference between subgroups. The slightly larger effect of immersive VR was accompanied by markedly higher heterogeneity (I2 > 90%), suggesting that differences in intervention duration, setting, and disease stage, rather than the level of immersion, drove the variability. The consistent effects across formats suggest that behavioral activation and enhanced self-efficacy may be key underlying mechanisms.46 Because the number of studies was limited and the training content and assessment tools varied, the power to detect true subgroup differences was reduced; current evidence therefore does not establish the superiority of either format, and the apparent subgroup differences should be regarded as exploratory.48
When compared with conventional care or health education as control conditions, VR showed a greater effect in reducing anxiety, whereas this advantage was attenuated when compared with PR. This pattern is plausible because PR itself improves psychological status through exercise, breathing regulation, and group support,49,50 so its therapeutic pathways overlap with those of VR, whereas usual care offers little targeted psychological support. Therefore, VR is more likely to function as a complementary or alternative approach to PR rather than replacing established rehabilitation models. For patients with COPD who are unable to participate in center-based PR because of geographic barriers, limited mobility, or low motivation, VR may represent an engaging home-based alternative. In the included studies, VR interventions were associated with greater reductions in anxiety and depressive symptoms than conventional health education alone.
Intervention content was a further source of heterogeneity. Hybrid programs combining exercise with breathing or psychological training produced the largest and most consistent effects; exercise-based VR showed moderate benefits; and breathing or relaxation training alone produced variable outcomes. Exercise may reduce anxiety indirectly by improving exercise tolerance, relieving dyspnea, and enhancing self-efficacy, with psychological engagement and behavioral activation as key mechanisms of emotional improvement.51,52 Integrating task-oriented movement and multimodal feedback within VR may further enhance attentional shifting and emotional regulation, generating synergistic benefits.53 Future VR programs should therefore move beyond single-symptom training toward an integrated motor, cognitive, and emotional framework.
Subgroup analysis by region showed that studies conducted in China reported larger effect sizes for depression improvement. This difference may be related to variations in baseline accessibility to PR resources and intervention intensity rather than true regional differences in VR efficacy.54–57 The included evidence was geographically concentrated, as six of the ten studies were conducted in China and the remaining four in Turkey, Poland, and Italy. The geographic concentration of the available evidence may limit the generalizability of the findings, because differences in healthcare systems, cultural context, and intervention implementation may affect both the magnitude of treatment effects and the comparability of outcomes across regions.58 First, baseline access to PR differs markedly. Structured outpatient PR is a routine part of COPD care in high-income European settings,59 and three of the four non-Chinese trials used rehabilitation comparators that themselves confer psychological benefits.54,57 In contrast, PR services in China remain predominantly concentrated in tertiary hospitals, while community- and home-based rehabilitation programs are still under development.60 Most Chinese control groups therefore received only routine care or health education, against which the incremental benefit of VR is correspondingly larger. Variations in reimbursement coverage, the availability of respiratory therapists, and the integration of psychological support into routine respiratory care therefore plausibly account for a substantial portion of the regional difference observed in our subgroup analysis.61 Second, cultural and measurement factors may contribute, including the somatic expression of distress in some East Asian populations, stronger family involvement, unevenly distributed digital health literacy, and the limited cross-cultural equivalence of scales such as the HADS, all of which can affect symptom reporting and engagement.62–65 Third, platforms and adjunctive therapies varied; Chinese trials more often used motion-sensing or scenario-based systems,21,23,26,31 in one case combined with herbal medicine, whereas European trials used head-mounted or balance-board devices19,27,28 that differ in immersion level and carry a higher risk of cybersickness.66 A single pooled estimate may therefore not fully represent the same intervention across settings,67 and generalization across health systems warrants caution.58 Multinational trials using standardized comparators, harmonized protocols,68 culturally validated measures,62 and pre-specified stratification by region are needed to separate the true efficacy of VR from contextual modifiers.
Sensitivity analysis indicated that the overall results were stable, although individual studies exerted a notable influence on heterogeneity. For anxiety outcomes, heterogeneity decreased after exclusion of the study by Şimşekli et al Their intervention consisted solely of viewing pre-recorded three-dimensional breathing training videos, including pursed-lip and diaphragmatic breathing, through VR goggles, without scenario simulation or motor interaction. This limited level of immersion may have weakened emotional engagement and regulation effects, thereby influencing the estimated effect size. In the analysis of depression outcomes, the pooled results changed substantially after exclusion of the study by Xiong et al This study implemented phased reinforcement through VR-based breathing and virtual exercise training and assessed outcomes using the COPD-QOL rather than dedicated psychological assessment scales. Differences in both intervention protocols and measurement instruments are therefore likely to represent major sources of heterogeneity. These findings suggest that future studies should standardize VR hardware and software parameters and harmonize intervention frequency, session duration, and overall treatment course. In addition, individual characteristics such as cultural background and disease severity should be carefully considered. The use of standardized and validated psychological assessment scales for anxiety and depression is also recommended to improve comparability across studies.62
Both approaches demonstrate potential therapeutic value. From a clinical and feasibility standpoint, device selection should consider the intervention goals, the core training components, and patient characteristics. Complex interactive operations may add burden for older adults and reduce adherence,28 and immersive head-mounted systems may provoke cybersickness in some users.66 In contrast, non-immersive VR may achieve comparable effects with lower cost and easier deployment, which could make it a practical option for PR centers and home-based settings. However, given the limited number of studies and the substantial clinical heterogeneity across interventions, these observations should be interpreted cautiously and require confirmation in larger, methodologically rigorous trials before firm conclusions can be drawn.
This study has several limitations. First, the relatively small number of included studies limited the precision of the pooled estimates and precluded formal assessment of publication bias. Second, substantial clinical and methodological heterogeneity existed across studies, including differences in intervention content, intervention dose, and outcome assessment tools, which may have contributed to the observed between-study variability. Third, although subgroup analyses were performed to explore potential sources of heterogeneity, the small number of studies within individual subgroups limited the reliability of these findings. Consequently, subgroup results should be considered exploratory and interpreted cautiously. Finally, the available evidence was geographically concentrated, with most studies conducted in China, which may limit the generalizability of the findings to other healthcare systems and cultural contexts. Future large-scale, multicenter RCTs conducted across diverse settings are needed to strengthen the evidence base and improve the applicability of the findings.
Conclusions
In summary, this systematic review and meta-analysis suggests that VR-based interventions may offer potential benefits for improving anxiety and depressive symptoms in patients with COPD and may represent a promising adjunct to conventional PR. Subgroup analyses suggested broadly comparable effects across different levels of immersion, although this observation remains exploratory. However, the certainty of the current evidence is limited by substantial between-study heterogeneity, variability in intervention characteristics and outcome measures, and the relatively small number of available studies. Therefore, the findings should be interpreted with caution. Rather than being considered an established effective intervention, VR should currently be viewed as a promising approach whose benefits require further validation. Future multicenter, adequately powered RCTs using standardized intervention protocols and harmonized outcome measures are needed to establish the long-term effectiveness, safety, and optimal implementation of VR interventions in COPD rehabilitation.
Abbreviations
COPD, Chronic obstructive pulmonary disease; PR, Pulmonary rehabilitation; VR, Virtual reality; PROSPERO, Prospective Register of Systematic Reviews; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; CNKI, China National Knowledge Infrastructure; CMJD, Chinese Medical Journal Full-text Database; RCTs, Randomized controlled trials; WHO, World Health Organization; ICTRP, International Clinical Trials Registry Platform; RoB 2, revised Cochrane risk-of-bias tool for randomized trials; CI, Confidence interval; SMD, Standardized mean difference; HADS, Hospital Anxiety and Depression Scale; HADS-A, HADS-anxiety subscale; SAS Self-Rating Anxiety Scale; COPD-QOL, COPD Quality of Life Scale; SDS, Self-Rating Depression Scale; BDI, Beck Depression Inventory; HAMD-17, Hamilton Depression Rating Scale; PRP, Pulmonary rehabilitation program; AECOPD, Acute exacerbation of COPD.
Data Sharing Statement
The data included in this study were derived from previously published studies and publicly available datasets, all of which are cited in the reference list. The results generated during the current study are presented in this article and are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
Ethical approval was not required for this study, as it was a systematic review and meta-analysis based on secondary analyses of previously published data. All included studies were publicly available and had obtained ethical approval in their original investigations.
Acknowledgments
The authors gratefully acknowledge all contributors who supported this research.
Author Contributions
All authors made substantial contributions to the work reported, including the conception and study design, data acquisition, analysis and interpretation. All authors participated in drafting, revising, or critically reviewing the article, approved the final version to be published, agreed on the journal to which the article was submitted, and accept responsibility for all aspects of the work.
Funding
This research was supported by Natural Science Foundation of Hunan Province (Grant No. 2026JJ81446) and Hunan Nursing Association (Grant No. HNKYP202404).
Disclosure
The authors declare that they have no competing interests for this work.
References
1. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for prevention, diagnosis, and management of COPD: 2025 report. Available from: https://goldcopd.org/2025-gold-report/.
2. World Health Organization. Chronic obstructive pulmonary disease (COPD). Available from: https://www.who.int/zh/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd).
3. Institute for Health Metrics and Evaluation (IHME). Global Burden of Disease 2021: findings from the GBD 2021 Study. Available from: https://www.healthdata.org/research-analysis/library/global-burden-disease-2021-findings-gbd-2021-study.
4. Wang JG, Bose S, Holbrook JT, et al. Clinical Characteristics of Patients With COPD and Comorbid Depression and Anxiety: data From a National Multicenter Cohort Study. Chronic Obstr Pulm Dis. 2025;12(1):33–23. doi:10.15326/jcopdf.2024.0534
5. Rahi MS, Thilagar B, Balaji S, et al. The impact of anxiety and depression in chronic obstructive pulmonary disease. Adv Respir Med. 2023;91(2):123–134. doi:10.3390/arm91020011
6. Wu K, Lu L, Chen Y, et al. Associations of anxiety and depression with prognosis in chronic obstructive pulmonary disease: a systematic review and meta-analysis. Pulmonology. 2025;31(1):2438553. doi:10.1080/25310429.2024.2438553
7. Zou W, Ou J, Wu F, et al. Association of mild chronic obstructive pulmonary disease with all-cause mortality: a systematic review and meta-analysis. Pulmonology. 2025;31(1):2416813. doi:10.1016/j.pulmoe.2023.09.002
8. Ouellette DR, Lavoie KL. Recognition, diagnosis, and treatment of cognitive and psychiatric disorders in patients with COPD. Int J Chronic Obstr. 2017;12,639–650. doi:10.2147/COPD.S123994
9. Gado OM, Basiony LA, Ibrahim MM, Shady IM, Affara NK. Anxiety-depressive Symptoms in Patients with Chronic Obstructive Pulmonary Disease (COPD) and Impact on Outcome. J Depress. Anxiety. 2015;4(2):181. doi:10.4172/2167-1044.1000181
10. Gordon CS, Waller JW, Cook RM, Cavalera SL, Lim WT, Osadnik CR. Effect of Pulmonary Rehabilitation on Symptoms of Anxiety and Depression in COPD: a Systematic Review and Meta-Analysis. Chest. 2019;156(1):80–91. doi:10.1016/j.chest.2019.04.009
11. Yohannes AM, Alexopoulos GS. Depression and anxiety in patients with COPD. Eur Respir Rev. 2014;23(133):345–349. doi:10.1183/09059180.00007813
12. Hansen H, Bieler T, Beyer N, et al. Supervised pulmonary tele-rehabilitation versus pulmonary rehabilitation in severe COPD: a randomised multicentre trial. Thorax. 2020;75(5):413–421. doi:10.1136/thoraxjnl-2019-214246
13. Armstrong M, Hume E, McNeillie L, et al. Cognitive behavioural therapy combined with physical activity behavioural modification strategies during pulmonary rehabilitation in patients with COPD. ERJ Open Res. 2023;9(5):00074–2023. doi:10.1183/23120541.00074-2023
14. Augustine A, Bhat A, Vaishali K, Magazine R. Barriers to pulmonary rehabilitation - A narrative review and perspectives from a few stakeholders. Lung India. 2021;38(1):59–63. doi:10.4103/lungindia.lungindia_116_20
15. Chen Y, Zhang Y, Long X, Tu H, Chen J. Effectiveness of virtual reality-complemented pulmonary rehabilitation on lung function, exercise capacity, dyspnea, and health status in chronic obstructive pulmonary disease: systematic review and meta-analysis. J Med Internet Res. 2025;27:e64742. doi:10.2196/64742
16. Xin H, Wei S, Zheng H, et al. Comparison of a Supervised Home-Based Tele-Rehabilitation with Center-Based Pulmonary Rehabilitation: protocol for a Randomized Non-Inferiority Multicenter Study in Ningxia. Int J Chron Obstruct Pulmon Dis. 2024;19:1707–1719. doi:10.2147/COPD.S467945
17. Zhang L, Liu F, Zhao J, Liu Y, Zhou Q. Research progress of telerehabilitation in pulmonary rehabilitation for patients with chronic obstructive pulmonary disease. Chin J Lung Dis. 2023;16(4):601–604.
18. Rutkowski S, Szczegielniak J, Szczepańska-Gieracha J. Evaluation of the efficacy of immersive virtual reality therapy as a method supporting pulmonary rehabilitation: a randomized controlled trial. J Clin Med. 2021;10(2):352. doi:10.3390/jcm10020352
19. Kizmaz E, Telli Atalay O, Çetin N, Uğurlu E. Virtual reality for COPD exacerbation: a randomized controlled trial. Respir Med. 2024;230:107696. doi:10.1016/j.rmed.2024.107696
20. Chen X, Chen L, Chen X, Ye Q, Cai G, Zeng Y. Assessing the impact of immersive virtual reality technology on the psychological recovery of patients with Parkinson’s disease depression: study protocol of a randomized controlled trial. Trials. 2024;25(1):715. doi:10.1186/s13063-024-08552-5
21. Feng B, Shi J, Yang B, Pan J, Song Z. Effects of Bio Master virtual scenario interactive rehabilitation combined with integrated breathing training on pulmonary function recovery in elderly patients with chronic obstructive pulmonary disease. J Pract Med. 2021;37(5):681–685.
22. Colombo V, Aliverti A, Sacco M. Virtual reality for COPD rehabilitation: a technological perspective. Pulmonology. 2022;28(2):119–133. doi:10.1016/j.pulmoe.2020.11.010
23. Jin XL. Application and effect evaluation of somatosensory interactive games in exercise intervention for hospitalized patients with acute exacerbation of chronic obstructive pulmonary disease [dissertation]. Suzhou: Suzhou University; 2021.
24. Zhu YL, Cao LJ, Zhou LX. Research progress on the application of virtual reality technology in pulmonary rehabilitation for patients with chronic obstructive pulmonary disease. Evid Based Nurs. 2024;9(8):1378–1384.
25. Chai X, Wu L, He Z. Effects of virtual reality-based pulmonary rehabilitation in patients with chronic obstructive pulmonary disease: a meta-analysis. Medicine. 2023;102(52):e36702. doi:10.1097/MD.0000000000036702
26. Geng M, Niu ME, Han YX, et al. Effects of home-based somatosensory interactive game exercise on fatigue and negative emotions in patients with stable chronic obstructive pulmonary disease. Nurs Pract Res. 2020;17(13):68–71.
27. Şimşekli D, Tan M. Effects of breathing exercises performed with virtual reality on dyspnea, anxiety and quality of life in COPD patients: a randomized controlled trial. Heart Lung. 2025;71:7–13. doi:10.1016/j.hrtlng.2025.01.014
28. Mazzoleni S, Montagnani G, Vagheggini G, et al. Interactive videogame as rehabilitation tool of patients with chronic respiratory diseases: preliminary results of a feasibility study. Respir Med. 2014;108(10):1516–1524. doi:10.1016/j.rmed.2014.07.004
29. Zhu T, Liu JC, Liu C, et al. Interpretation of the revised Cochrane risk-of-bias tool for randomized trials (RoB 2.0, 2021 version) for cluster randomized and crossover trials. Chin J Evid Based Med. 2022;22(7):842–852.
30. Cohen J. Statistical power analysis for the behavioral sciences. United States of America: lawrence Erlbaum Associates. 1988.
31. Fang HQ. Application of family-based somatosensory interactive game intervention in post-discharge rehabilitation of patients with chronic obstructive pulmonary disease. Integr Nurs Chin West Med. 2021;7(1):97–102. doi:10.12209/j.issn2709-1961.202012078
32. Yan YQ, Zhang JM, Xiang LH, et al. Clinical observation of virtual reality technology combined with Bufei Jieyu decoction in the treatment of chronic obstructive pulmonary disease with depressive state. J Clin Tradit Chin Med. 2025;37(8):1600–1604. doi:10.16448/j.cjtcm.2025.0824
33. Xiong XP, Jiang X, Gu SS. Effects of immersive virtual reality–based pulmonary rehabilitation health education on exercise capacity and cardiopulmonary function in patients with acute exacerbation of chronic obstructive pulmonary disease. J Hunan Norm Univ. 2024;21(6):69–73.
34. Hu Y. Evidence-Based Nursing. Beijing: People’s Medical Publishing House; 2012:73–99.
35. Qi W, Song F, Li M, et al. Synergistic effects of virtual reality and traditional treatment methods in the management of chronic obstructive pulmonary disease: a systematic review and meta-analysis of randomized controlled trials. PeerJ. 2025;13:e20047. doi:10.7717/peerj.20047
36. Pancini E, Fumagalli A, Maggiolini S, et al. Promoting emotional and psychological well-being of patients with chronic obstructive pulmonary disease: a feasibility study combining virtual reality and savoring. Annu Rev Cybertherapy Telemed. 2023;21:234–239.
37. Chiu PL, Li H, Yap KY, Lam KC, Yip PR, Wong CL. Virtual reality–based intervention to reduce preoperative anxiety in adults undergoing elective surgery: a randomized clinical trial. JAMA Netw Open. 2023;6(10):e2340588. doi:10.1001/jamanetworkopen.2023.40588
38. McGhee WRG, Doherty CJ, Graham-Wisener L, et al. Immersive virtual reality and psychological well-being in adult chronic physical illness: systematic review. BMJ Support Palliat Care. 2024;14(1):14–24. doi:10.1136/spcare-2023-004502
39. Yang Y, Wei L, Wang S, et al. The effects of pursed lip breathing combined with diaphragmatic breathing on pulmonary function and exercise capacity in patients with COPD: a systematic review and meta-analysis. Physiother Theory Pract. 2022;38(7):847–857. doi:10.1080/09593985.2020.1805834
40. Nerini C, Burk S, Andretta E, Chirico A, Giordano A. The effects of virtual reality on pain and anxiety in pediatric oncology patients. Ann. Res. Oncol. 2024;4(1):29–39. doi:10.48286/aro.2024.81
41. Mazgelytė E, Rekienė V, Dereškevičiūtė E, et al. Effects of Virtual reality-based relaxation techniques on psychological, physiological, and biochemical Stress Indicators. Healthcare. 2021;9(12):1729. doi:10.3390/healthcare9121729
42. Wormser J, Romanet C, Cachanado M, et al. Virtual reality in adults with respiratory diseases experiencing dyspnoea: a systematic review and meta-analysis. BMJ Open Respir Res. 2025;12(1):e002722. doi:10.1136/bmjresp-2024-002722
43. Yang M, Lin WT, Ma HX, et al. Research progress on the application of virtual reality technology in pulmonary rehabilitation for patients with chronic obstructive pulmonary disease. Chin Nurs Manag. 2022;22(5):796–800.
44. Xie QR, Lin WQ, Zhang Q, et al. Research progress in intelligent assessment and virtual reality training for upper limb rehabilitation after stroke. Rehabil Med J. 2023;33(3):271–279.
45. Patsaki I, Avgeri V, Rigoulia T, Zekis T, Koumantakis GA, Grammatopoulou E. Benefits from incorporating virtual reality in pulmonary rehabilitation of COPD patients: a systematic review and meta-analysis. Adv Respir Med. 2023;91(4):324–336. doi:10.3390/arm91040026
46. Jia E, Macon J, Doering M, Abraham J. Effectiveness of digital behavioral activation interventions for depression and anxiety: systematic review and meta-analysis. J Med Internet Res. 2025;27:e68054. doi:10.2196/68054
47. Rutkowski S, Rutkowska A, Kiper P, et al. Virtual reality rehabilitation in patients with chronic obstructive pulmonary disease: a randomized controlled trial. Int J Chron Obstruct Pulmon Dis. 2020;15:3271–3283. doi:10.2147/COPD.S223592
48. Schandelmaier S, Briel M, Varadhan R, et al. Development of the Instrument to assess the Credibility of Effect Modification Analyses (ICEMAN) in randomized controlled trials and meta-analyses. CMAJ. 2020;192(32):E901–E906. doi:10.1503/cmaj.200077
49. Coventry PA. Does pulmonary rehabilitation reduce anxiety and depression in chronic obstructive pulmonary disease. Curr Opin Pulm Med. 2009;15(2):143–149. doi:10.1097/MCP.0b013e3283218318
50. Tselebis A, Bratis D, Pachi A, et al. A pulmonary rehabilitation program reduces levels of anxiety and depression in COPD patients. Multidiscip Respir Med. 2013;8(1):41. doi:10.1186/2049-6958-8-41
51. Spruit MA, Singh SJ, Garvey C, et al. An official American Thoracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. 2013;188(8):e13–e64. doi:10.1164/rccm.201309-1634ST
52. Puhan MA, Gimeno-Santos E, Cates CJ, Troosters T. Pulmonary rehabilitation following exacerbations of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2016;12(12):CD005305. doi:10.1002/14651858.CD005305.pub4
53. Maples-Keller JL, Bunnell BE, Kim SJ, Rothbaum BO. The use of virtual reality technology in the treatment of anxiety and other psychiatric Disorders. Harv Rev Psychiatry. 2017;25(3):103–113. doi:10.1097/HRP.0000000000000138
54. McCarthy B, Casey D, Devane D, Murphy K, Murphy E, Lacasse Y. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2015;2015(2):CD003793. doi:10.1002/14651858.CD003793.pub3
55. Torous J, Bucci S, Bell IH, et al. The growing field of digital psychiatry: current evidence and the future of apps, social media, chatbots, and virtual reality. World Psychiatry. 2021;20(3):318–335. doi:10.1002/wps.20883
56. Riva G, Wiederhold BK, Mantovani F. Neuroscience of virtual reality: from virtual exposure to embodied medicine. Cyberpsychol Behav Soc Netw. 2019;22(1):82–96. doi:10.1089/cyber.2017.29099.gri
57. Patel S, Palmer MD, Nolan CM, et al. Supervised pulmonary rehabilitation using minimal or specialist exercise equipment in COPD: a propensity-matched analysis. Thorax. 2021;76(3):264–271. doi:10.1136/thoraxjnl-2020-215281
58. Weise A, Büchter R, Pieper D, Mathes T. Assessing context suitability (generalizability, external validity, applicability or transferability) of findings in evidence syntheses in healthcare—An integrative review of methodological guidance. Res Synth Methods. 2020;11(6):760–779. doi:10.1002/jrsm.1453
59. Rochester CL, Alison JA, Carlin B, et al. Pulmonary rehabilitation for adults with chronic respiratory disease: an official American Thoracic Society clinical practice guideline. Am J Respir Crit Care Med. 2023;208(4):e7–e26. doi:10.1164/rccm.202306-1066ST
60. Sun YC. Chronic obstructive pulmonary disease in primary healthcare institutions in China: challenges and solutions. Chronic Dis Transl Med. 2020;6(4):219–223. doi:10.1016/j.cdtm.2020.05.007
61. Yao X, Li J, He J, et al. A Kano model-based demand analysis and perceived barriers of pulmonary rehabilitation interventions for patients with chronic obstructive pulmonary disease in China. PLoS One. 2023;18(12):e0290828. doi:10.1371/journal.pone.0290828
62. Maters GA, Sanderman R, Kim AY, Coyne JC. Problems in cross-cultural use of the Hospital Anxiety and Depression Scale: “no butterflies in the desert”. PLoS One. 2013;8(8):e70975. doi:10.1371/journal.pone.0070975
63. Tang L, Zhong J, Zeng M, et al. Construction and verification of a predictive model for depression risk of patients with somatization symptoms. Front Psychiatry. 2025;16:1555513. doi:10.3389/fpsyt.2025.1555513
64. Cai Y, Zhang Z, Ren X, Chen O. Coping with chronic obstructive pulmonary disease together: a dyadic study of self-care and quality of life in patients and their caregivers. J Clin Nurs. 2025;34(8):3297–3306. doi:10.1111/jocn.17513
65. Zhang X, Yuan Y, Jiang J. Digital health literacy among older adults in China: a cross-sectional study on prevalence and influencing factors. Front Public Health. 2025;13:1661177. doi:10.3389/fpubh.2025.1661177
66. Drazich BF, McPherson R, Gorman EF, et al. In too deep? A systematic literature review of fully-immersive virtual reality and cybersickness among older adults. J Am Geriatr Soc. 2023;71(12):3906–3915. doi:10.1111/jgs.18553
67. Skivington K, Matthews L, Simpson SA, et al. A new framework for developing and evaluating complex interventions: update of Medical Research Council guidance. BMJ. 2021;374:n2061. doi:10.1136/bmj.n2061
68. Souto-Miranda S, Rodrigues G, Spruit MA, Marques A. Pulmonary rehabilitation outcomes in individuals with chronic obstructive pulmonary disease: a systematic review. Ann Phys Rehabil Med. 2022;65(3):101564. doi:10.1016/j.rehab.2021.101564
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Anxiety and Depression Among US Nursing Home Residents with Chronic Obstructive Pulmonary Disease
Osundolire S, Goldberg RJ, Lapane KL
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1867-1882
Published Date: 28 August 2023
Exploring Patterns of COPD Exacerbations and Comorbid Flare-Ups
van Dijk SHB, Brusse-Keizer MGJ, Effing T, van der Valk PDLPM, Ploumen EH, van der Palen J, Doggen CJM, Lenferink A
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2633-2644
Published Date: 16 November 2023
Advocating for Action: Exploring the Potential of Virtual Reality in Breathing Exercise – A Review of The Clinical Applications
Alhammad SA
Patient Preference and Adherence 2024, 18:695-707
Published Date: 19 March 2024
Efficacy and Safety of Escitalopram in Alleviating Depression and Anxiety Symptoms in COPD Patients: A Randomized Double-Blind Placebo-Controlled Trial
Gao Z, Tang S, Zhang W, Zhang M, Wei Z, Long Z, Wang B, Qin H, Qian H, Yin Y, Wang G, He B
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:572465
Published Date: 7 February 2026
Exercise Training Improves Depression and Anxiety in Patients with COPD: A Dose-Response Meta-Analysis of Randomized Controlled Trials
Chen S, Shang B, Bi Y, Xu R, Li Q, Zhang W, Yang Y, Hu S
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:578054
Published Date: 6 May 2026