Back to Journals » Journal of Pain Research » Volume 18
Effects of Transcutaneous Electrical Acupoint Stimulation on Recovery After Gynecological Laparoscopic Surgery: A Randomized, Single-Blind, Controlled Trial
Authors Zheng J, Zhou H, Diao Y, Song P, Yi Z, Guo X, Li L ![]()
Received 29 May 2025
Accepted for publication 8 November 2025
Published 3 December 2025 Volume 2025:18 Pages 6449—6462
DOI https://doi.org/10.2147/JPR.S543574
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Jia Zheng,1 Huipeng Zhou,2 Yugang Diao,1 Pei Song,1 Zhuo Yi,1 Xuewei Guo,1 Lin Li1
1Department of Anesthesiology, General Hospital of Northern Theater Command, Shenyang, 110016, People’s Republic of China; 2Department of Anesthesiology, The 964TH Hospital of Chinese People’s Liberation Army Joint Logistics Support Force, Changchun, 130000, People’s Republic of China
Correspondence: Lin Li, Department of Anesthesiology, General Hospital of Northern Theater Command, No. 83, Wenhua Road, Shenhe District, Shenyang, 110016, People’s Republic of China, Tel +86 13304042711, Email [email protected]
Purpose: Gynecological laparoscopic surgery is a common minimally invasive procedure, but postoperative recovery quality remains an important clinical concern. This study aimed to evaluate the effects of transcutaneous electrical acupoint stimulation (TEAS) on the quality of recovery in patients undergoing gynecological laparoscopic surgery.
Patients and Methods: In this prospective, randomized, single-blind, controlled trial, patients scheduled for gynecological laparoscopic surgery under general anesthesia at a tertiary hospital in China between April and December 2022 were enrolled. Participants were randomized into the TEAS group and the control group. In the TEAS group, bilateral stimulation of Neiguan, Zusanli, and Hegu acupoints was initiated 30 minutes before anesthesia induction and maintained until the end of surgery. In the control group, electrodes were applied without electrical stimulation (sham procedure). The primary outcome was the incidence of postoperative nausea and vomiting (PONV) within 24 hours. Secondary outcomes included the Quality of Recovery-40 (QoR-40) scores, Pittsburgh Sleep Quality Index (PSQI) scores, pain intensity assessed by numerical rating scale (NRS), and patient-controlled analgesia (PCA) usage.
Results: A total of 85 patients completed the study (TEAS group, n=42; control group, n=43). The incidence of 24-hour PONV was significantly lower in the TEAS group compared to the control group (42.9% vs 67.4%, P=0.023). QoR-40 scores at 48 hours postoperatively were significantly higher in the TEAS group (P< 0.001). Additionally, the TEAS group exhibited lower blood glucose levels 30 minutes after skin incision (P=0.045), reduced intraoperative remifentanil consumption (P=0.031), fewer total and effective PCA demands (P=0.004 and P=0.039, respectively), and earlier recovery of gastrointestinal function (all P< 0.05).
Conclusion: Perioperative TEAS effectively reduces the incidence of early postoperative nausea and vomiting and enhances recovery quality in patients undergoing gynecological laparoscopic surgery, but the improvements in QoR-30 scores were statistically significant but not clinically significant. These benefits may be attributed to attenuated stress responses, improved sleep quality, and decreased analgesic requirements.
Keywords: laparoscopic surgery, gynecological surgery, transcutaneous electrical acupoint stimulation, postoperative recovery, postoperative nausea and vomiting
Introduction
Laparoscopic surgery in gynecology presents numerous advantages over traditional open surgical techniques, including smaller incisions, expedited recovery, and diminished postoperative pain.1,2 Despite its minimally invasive nature and associations with reduced blood loss and shorter hospital stays, laparoscopic surgery may induce physiological alterations in the body owing to the establishment of artificial pneumoperitoneum and intraoperative positional changes, which can lead to adverse reactions.3,4 These adverse reactions encompass pain, bleeding, infection or fever, gastrointestinal dysfunction, and anesthesia-related effects such as dizziness, headache, and drowsiness, all of which may hinder rehabilitation and prolong hospitalization.5,6 Among gynecological patients presenting with high-risk factors, the incidence of postoperative nausea and vomiting (PONV) can ascend to 70% to 80%, with postoperative pain, drowsiness, and fatigue reported in 45%, 42%, and 21% of patients, respectively.7,8 The discontinuation of analgesic treatment often arises from inadequate efficacy or the emergence of side effects, thereby increasing the demand for non-pharmacological alternative analgesic approaches.
Transcutaneous electrical acupoint stimulation (TEAS) is a technique that integrates principles of traditional Chinese acupuncture with transcutaneous nerve electrical stimulation, administering specific pulse currents through the skin at designated acupuncture points.9 TEAS is characterized by its ease of use, safety, non-invasive nature, and broad acceptance and application across various medical disciplines, including obstetrics, gynecology, gastrointestinal surgery, and oncology.10,11 The technique has demonstrated efficacy as an adjunct to perioperative sedation and analgesia, contributing to reduced anxiety, alleviation of the stress response, mitigation of PONV, and enhancement of postoperative cognitive function.11–14 A recent meta-analysis found that TEAS significantly reduced postoperative pain and opioid use, with signals toward reducing PONV, although heterogeneity was substantial.15 More recently, Szmit et al10 systematically reviewed 22 RCTs and confirmed perioperative benefits for PONV and pain reduction, but highlighted methodological variability and small sample sizes. Nevertheless, there remains a lack of high-quality evidence to evaluate the impact of TEAS on the recovery duration of patients undergoing gynecological laparoscopic surgery. Although several drugs can be used to improve the quality of recovery, non-pharmacological approaches could be useful as an adjunct to pharmacological therapy, when there are drug interaction issues, or to decrease opioid use.
Consequently, the present study aims to investigate the effect of TEAS on the quality of recovery in patients undergoing gynecologic laparoscopic surgery. The findings are expected to inform the potential role of TEAS as a non-pharmacological adjunct for improving postoperative outcomes and minimizing perioperative complications. The present trial specifically evaluates TEAS within gynecological laparoscopy and extends outcomes to validated recovery indices, addressing a gap in prior evidence.
Materials and Methods
Study Design and Participants
This prospective, randomized, single-blind, controlled trial was conducted at the Northern Theater General Hospital of the People’s Liberation Army of China between April and December 2022. Patients scheduled to undergo gynecological laparoscopic surgery under general anesthesia were screened for eligibility.
Inclusion criteria were as follows: (1) age between 18 and 65 years, (2) body mass index (BMI) between 18 and 30 kg/m2, and (3) American Society of Anesthesiologists (ASA) physical status classification I–II. Exclusion criteria included: (1) presence of rash or infection at the acupoint stimulation sites; (2) long-term use of sedatives or analgesics (ie, regular use for >3 months of any benzodiazepines, non-benzodiazepine sedatives, opioids, non-steroidal anti-inflammatory drugs (NSAIDs), or gabapentinoids); (3) history of substance abuse; (4) diabetes mellitus; (5) impaired hepatic or renal function; (6) cognitive impairment; (7) severe cardiovascular disease; (8) history of chronic pain; (9) prior experience with acupoint stimulation therapy; (10) presence of a pacemaker; and (11) participation in another clinical trial within the preceding three months. Participants were withdrawn from the study if there was a change in the surgical plan, if the duration of surgery exceeded three hours, or if postoperative transfer to the intensive care unit (ICU) was required.
The study protocol adhered to the principles outlined in the Declaration of Helsinki and Good Clinical Practice guidelines. Ethical approval was obtained from the Ethics Committee of the Northern Theater General Hospital of the People’s Liberation Army of China (Approval No. Y(2021)138). Written informed consent was obtained from all participants or their legal representatives prior to enrollment. The trial was registered with the Chinese Clinical Trial Registry (Registration No. ChiCTR2200058283), and the full trial details are publicly available at https://www.chictr.org.cn/showproj.html?proj=166185. The full study protocol is available from the corresponding author upon reasonable request.
Randomization and Blinding
Prior to surgery, a research staff member not involved in the trial’s implementation generated the randomization sequence using a computer-based random number generator. The random allocation in this study was performed using a computerized random number generator. A third-party statistician not involved in participant enrollment used the random number generation function of SPSS. A fixed seed number (eg, 12345) was preset to generate random numbers ranging between 0 and 1. Participants with a random number ≤0.5 were assigned to the experimental group, while those with a random number >0.5 were allocated to the control group, ensuring a 1:1 ratio between the two groups. The group assignments were concealed in sequentially numbered, opaque, sealed envelopes, which were opened only at the time of anesthesia induction. At that point, the designated operators were informed of the group allocation and administered the corresponding interventions. All participants and outcome assessors remained blinded to group assignments throughout the study. The anesthesiologists performing the intervention were not involved in data collection or analysis. Although the anesthesiologists were unblinded due to the nature of the intervention, all outcome assessors and data analysts remained blinded to minimize performance and detection bias.
Intervention
All interventions were performed by a licensed acupuncturist with internationally recognized certification and 5–10 years of clinical experience. In accordance with traditional Chinese medicine principles and anatomical landmarks, bilateral Neiguan, Zusanli, and Hegu acupoints were selected for TEAS. Stimulation was administered for 30 minutes prior to anesthesia induction using disposable silicone electrodes. TEAS was delivered with a Huatuo electronic acupuncture device (SDZ-V model, Suzhou Medical Devices Co., Ltd., Suzhou, China). The device was set to a frequency of 2/100 Hz for sparse and dense wave stimulation, with the intensity gradually increased from 6 mA to the maximum tolerable level for the participant, not exceeding 15 mA. The stimulation aimed to induce slight muscle twitching, achieving the optimal “De Qi” sensation. Electrical stimulation was terminated at the end of anesthesia.
In the control group, identical electrodes were applied and connected to the device, but no electrical stimulation was delivered. After 30 minutes, anesthesia induction proceeded as planned. To maintain blinding, participants were informed preoperatively that they might or might not experience electrical stimulation. Regardless of group assignment, all participants were asked three times if they tolerated the stimulation, ensuring that they remained unaware of their group allocation and were blinded to the intervention.
Anesthesia and Perioperative Management
All participants fasted for 8 hours and refrained from liquid intake for 4 hours prior to surgery. Standard intraoperative monitoring included electrocardiogram (ECG), heart rate (HR), pulse oximetry (SpO2), invasive blood pressure (IBP), bispectral index (BIS), and body temperature. Following a 5-minute rest period, the mean arterial pressure (MAP) was recorded as the baseline (MAP0).
After anesthesia induction, bilateral TAP blocks were performed under ultrasound guidance. The patients were positioned supine with abdominal skin disinfected. The ultrasound transducer was placed between the iliac crest and subcostal margin along the midaxillary line for axial scanning to identify the external oblique, internal oblique, and transversus abdominis muscles. Using an in-plane ultrasound technique, the needle was advanced to the fascial plane between the internal oblique and transversus abdominis muscles, with 15 mL of 0.375% ropivacaine injected on each side.
Anesthesia induction was performed using sufentanil 0.15 µg/kg, rocuronium 0.6 mg/kg, and propofol 2.0 mg/kg. Anesthesia maintenance was performed using propofol infusion at 4–8 mg/kg/h, remifentanil at 0.6–1.0 µg/kg/h, and sevoflurane inhalation. Sevoflurane is a risk factor for PONV;16 therefore, the MAC was set at 0.3 with a concentration of 1%-2%. This balanced anesthesia technique was employed to minimize sevoflurane exposure and thereby reduce the risk of PONV, while ensuring adequate depth of anesthesia as monitored by BIS. The infusion rate of propofol was adjusted to ensure the depth of anesthesia at BIS of 40–60. If the anesthesia was too deep or too shallow during the operation, the participant exited the trial. The remifentanil infusion rate was adjusted to maintain MAP within 20% of MAP0. When MAP was <25% of MAP0, 40 µg of phenylephrine (HR ≥50 bpm) or 3 mg of ephedrine (HR <50 bpm) was administered. When MAP was ≥25% of MAP0, 5 mg of urapidil was administered. When HR was ≤40 bpm, 0.5 mg of atropine was administered. If the surgery duration exceeded 1 hour, an additional 0.15 mg/kg of rocuronium bromide was administered. At the beginning of suturing, an intravenous infusion of ondansetron 8 mg and flurbiprofen ester 50 mg was given for prophylactic antiemetic and analgesic purposes. At the end of suturing, a patient-controlled intravenous analgesia (PCIA) pump (sufentanil 2 µg/kg + 0.9% sodium chloride) was established. The flow rate was 2 mL/h, with a single additional dose of 0.5 mL after pressing and a lock time of 15 minutes. The participant was transferred to the post-anesthesia care unit (PACU) for observation after tracheal tube removal.
The opioid-sparing regimen was deliberately designed based on three key pharmacological principles. (1) Synergistic effects of multimodal anesthesia: Remifentanil was combined with sevoflurane (1–2%) and propofol (4–8 mg/kg/h), allowing significant opioid reduction. Volatile anesthetics reduce remifentanil EC50 by >40%.17,18 (2) Procedure-specific requirements: Gynecologic laparoscopy involves moderate surgical stress (compared to open surgery). The dose aligns with enhanced recovery after surgery (ERAS) guidelines for minimally invasive procedures. (3) Adjunct regional analgesia: All patients received bilateral TAP blocks with 0.375% ropivacaine, providing somatic analgesia that further reduced opioid demand.
Outcomes
The primary outcome was the incidence of PONV within the first 24 hours after surgery. PONV events were further categorized based on postoperative periods: 0–2 hours, 2–4 hours, 4–6 hours, and 6–24 hours. Secondary outcomes included the Quality of Recovery-40 (QoR-40) score, Pittsburgh Sleep Quality Index (PSQI), postoperative pain assessed via the Numeric Rating Scale (NRS), total and effective patient-controlled intravenous analgesia (PCIA) usage, incidence of gastrointestinal function recovery, adverse events, time to first flatus, and length of hospital stay.
Nausea was defined as a subjective unpleasant sensation in the epigastrium accompanied by an involuntary urge to vomit. Vomiting was defined as sustained, forceful contraction of abdominal muscles with either expulsion of gastric contents or retching (without content expulsion) occurring ≥2 times within 5 minutes. It was clarified in the Methods.
The QoR-40, a well-established tool in clinical research, was used to assess recovery quality due to its reliability, validity, and responsiveness.19 The QoR-40 consists of 40 items across five dimensions, each rated on a 1–5 scale, yielding a total score range of 40–200, with higher scores indicating better recovery quality.20 The NRS, an 11-point scale ranging from 0 (no pain) to 10 (worst pain imaginable), was utilized to assess pain intensity. The PSQI, which evaluates sleep quality, consists of seven components, each rated on a scale from 0 to 3, yielding a total score range of 0–21, with higher scores indicating poorer sleep quality.
Additional perioperative parameters were recorded, including MAP and HR at the following time points: preoperatively (T0), at intubation (T1), at skin incision (T2), after pneumoperitoneum establishment (T3), at the end of surgery (T4), and 5 minutes post-extubation (T5). Other perioperative factors, such as anesthesia duration, recovery time, PACU stay, blood loss, and anesthesia drug consumption, were also documented. Biochemical measures included glycemia 30 minutes post-skin incision. The time to first flatus was the time between the end of surgery and the first stools passed by the participants.
Sample Size
Based on the literature, the incidence of PONV in patients undergoing gynecological laparoscopic surgery within the first 24 hours is approximately 66.7%,21 which was used as the reference value for the control group. It was hypothesized that TEAS could lead to an absolute reduction in the incidence of PONV by 30%, with a clinically significant reduction of 20%.22 The assumed 30% absolute reduction in PONV incidence was based on a previous RCT showing that non-pharmacologic interventions combined with antiemetics can achieve such an effect in a similar patient population.22 Assuming a two-sided confidence level of 95% (α = 0.05) and a statistical power of 80% (β = 0.2), the required sample size was calculated using G*Power software. The results indicated 40 participants per group (80 in total). To account for a 10% dropout rate, 4 additional participants were added to each group, resulting in a final target enrollment of 44 participants per group (88 in total).
Statistical Analysis
Data analysis was performed using SPSS version 26.0 (Armonk, NY, USA). Continuous variables were assessed for normality using the Shapiro–Wilk test. For normally distributed continuous variables, data were expressed as means ± standard deviations (SDs), while non-normally distributed variables were presented as medians with interquartile ranges (IQRs). Comparisons between groups for normally distributed continuous variables were conducted using the two-sample t-test, assuming equal variance. Welch’s t-test was applied for comparisons when variances were unequal. For non-normally distributed continuous variables, the Wilcoxon rank-sum test was employed. Categorical variables were presented as frequencies (n) and percentages (%). Differences between categorical variables in the two groups were analyzed using the chi-squared test or Fisher’s exact test, as appropriate.
The primary outcome was assessed using generalized estimating equations (GEE), with the identification number as the clustering variable, time as the within-subject variable, and the occurrence of PONV as the dependent variable. The interaction between the intervention and time was evaluated to determine whether the effect of the intervention varied over time. P-values were calculated for the interaction effect, with main effects of time and intervention excluded in the analysis to isolate the interaction.
Two-way analysis of variance (ANOVA) was utilized to compare the postoperative recovery scale scores, HR, and MAP between the two groups at each time point during the perioperative period. Sidak’s multiple comparisons test was employed to adjust for multiple comparisons. The analysis was performed following the modified intent-to-treat (mITT) principle.
Results
Participants Characteristics
A total of 112 patients scheduled for gynecological laparoscopic surgery were screened for eligibility. Fourteen patients were excluded as they did not meet the inclusion criteria, and ten declined to participate. The remaining 88 patients were randomly assigned to either the TEAS or the control group. Three patients were subsequently excluded from the mITT analysis due to a change in procedure (n=2) or a procedure time exceeding 3 hours (n=1). Thus, a final total of 85 patients were included in the analysis, and therefore, a modified intention-to-treat (mITT) analysis was employed (Figure 1). No significant differences in baseline characteristics were observed between the two groups (Table 1).
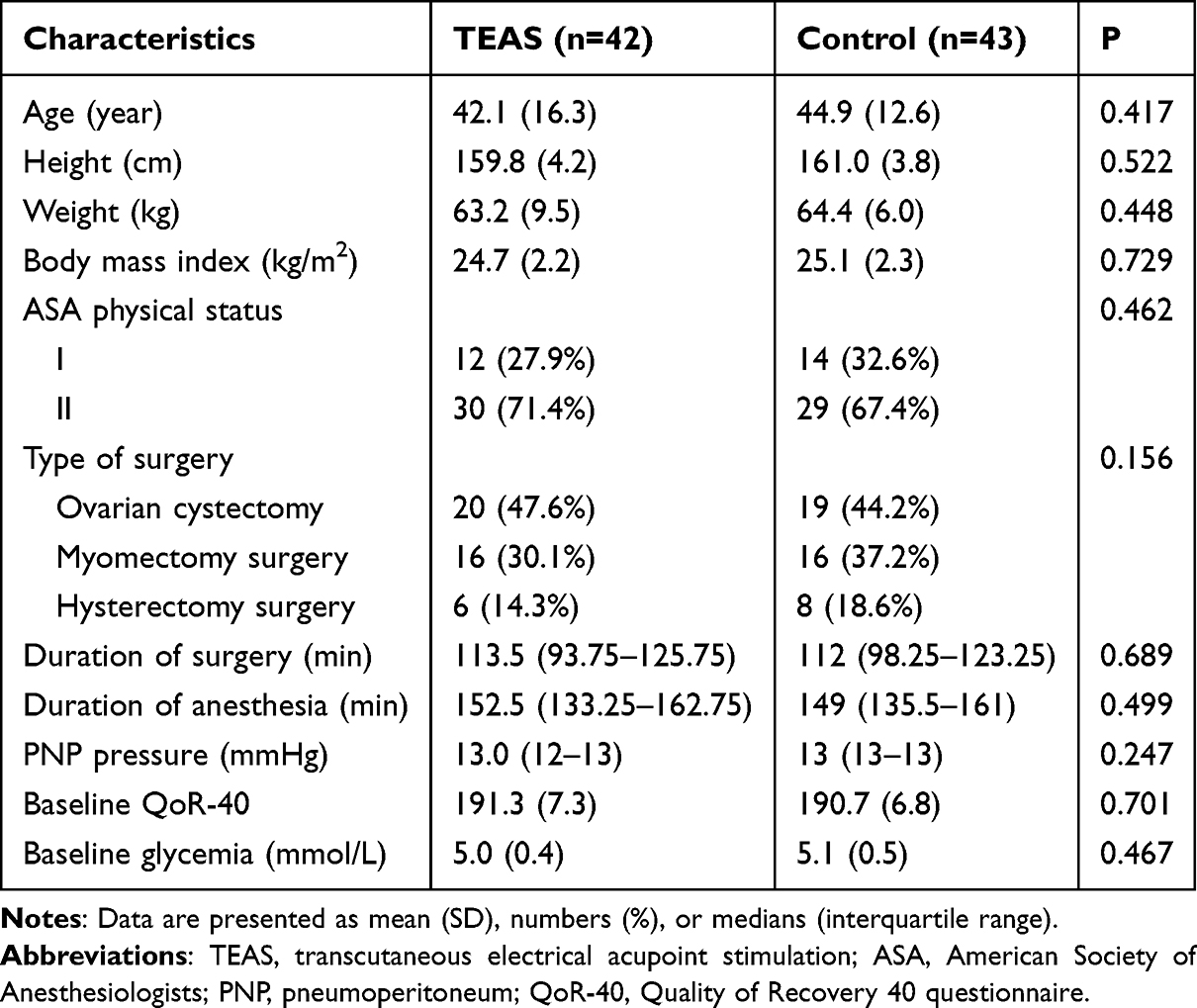 |
Table 1 Baseline Characteristics of the Participants in the Modified Intention-to-Treat Analysis |
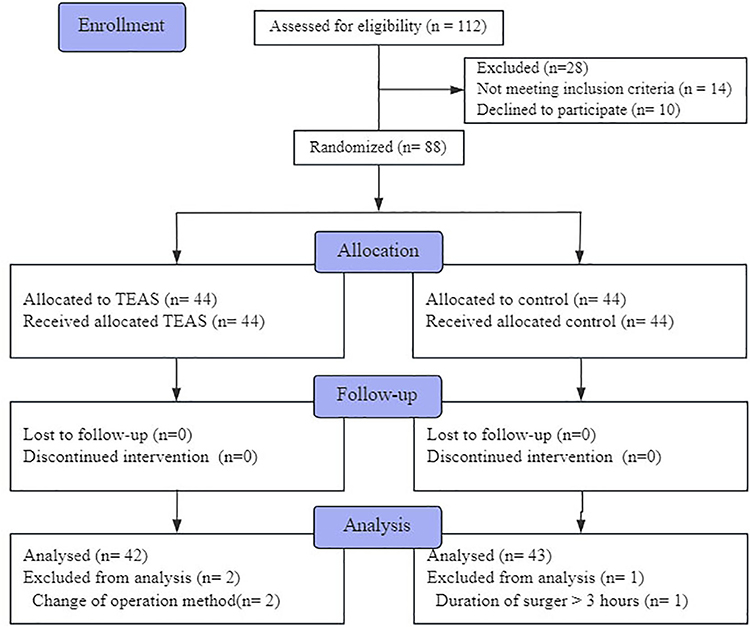 |
Figure 1 Flow diagram of the study. |
Primary Outcome
The incidence of PONV within the 24-hour postoperative period differed significantly between the two groups. The TEAS group had an incidence of 42.9%, while the control group had a significantly higher incidence of 67.4% (P=0.023; odds ratio [OR] = 2.762; 95% confidence interval [CI]: 1.142, 6.681). When considering nausea and vomiting separately, no significant differences were observed in the incidence of vomiting between the two groups at various postoperative follow-up intervals.
For nausea, the differences in incidence between the two groups were as follows: 0.25 (CI: 0.05, −0.45, P=0.013) within the first 0–2 hours, 0.09 (CI: −0.10, 0.27, P=0.351) within 2–4 hours, and 0.04 (CI: −0.10, 0.19, P=0.561) within 4–6 hours (Table 2).
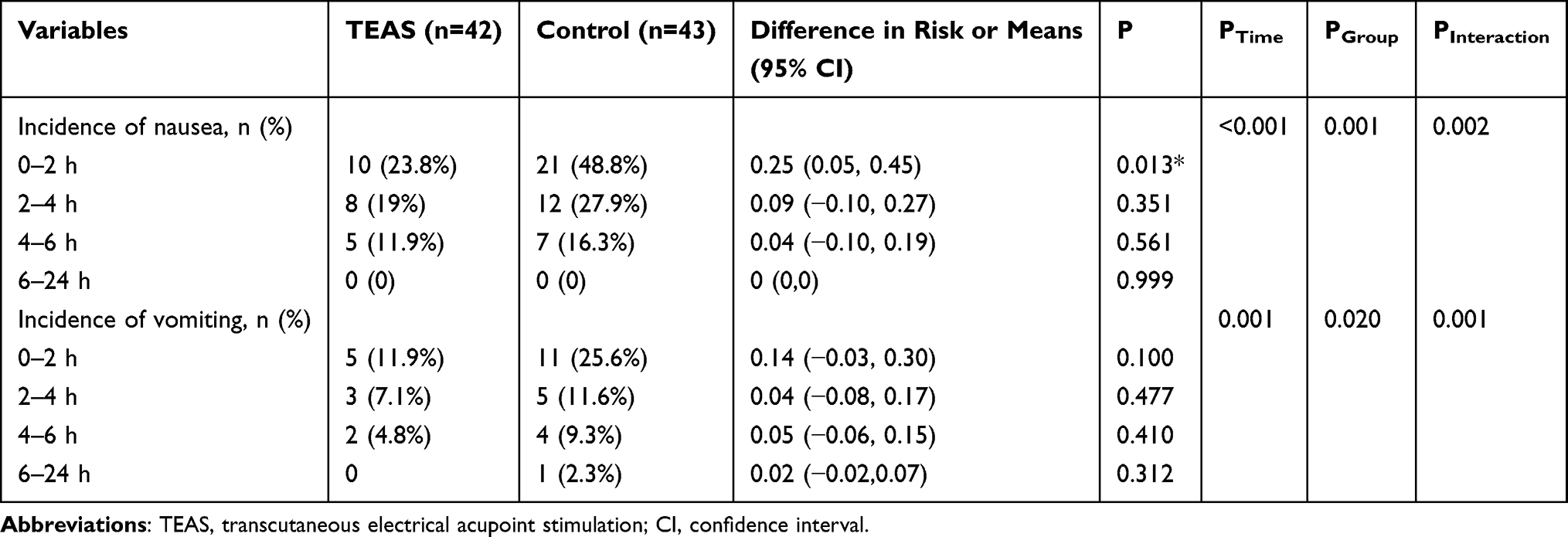 |
Table 2 Comparison of the Incidence of PONV Between Two Groups at Different Time Points |
Secondary Outcomes
ANOVA conducted on the QoR-40 scores at 48 hours postoperatively revealed that the TEAS group had a significantly higher total score (184.0) compared to the control group (181.0), with a difference of −2.9% (95% CI: −4.07, −1.78, P<0.001). Additionally, the scores across all five dimensions were significantly higher in the TEAS group than in the control group at the same time point (P<0.001).
Multiple comparisons of the QoR-40 scores at different postoperative time points demonstrated that, prior to surgery, the quality of recovery scores were similar between the two groups. However, the TEAS group exhibited significantly better recovery at 24 and 48 hours postoperatively, with differences of −7.0% (95% CI: −9.05, −4.95, P<0.0001) and −2.0% (95% CI: −3.63, −0.37, P=0.010), respectively. The difference in QoR-40 scores at 6 hours postoperatively was −0.02% (95% CI: −1.23, 1.17, P=0.068), which was not statistically significant. The specific differences in the five dimensions of the QoR-40 scores are presented in Figure 2.
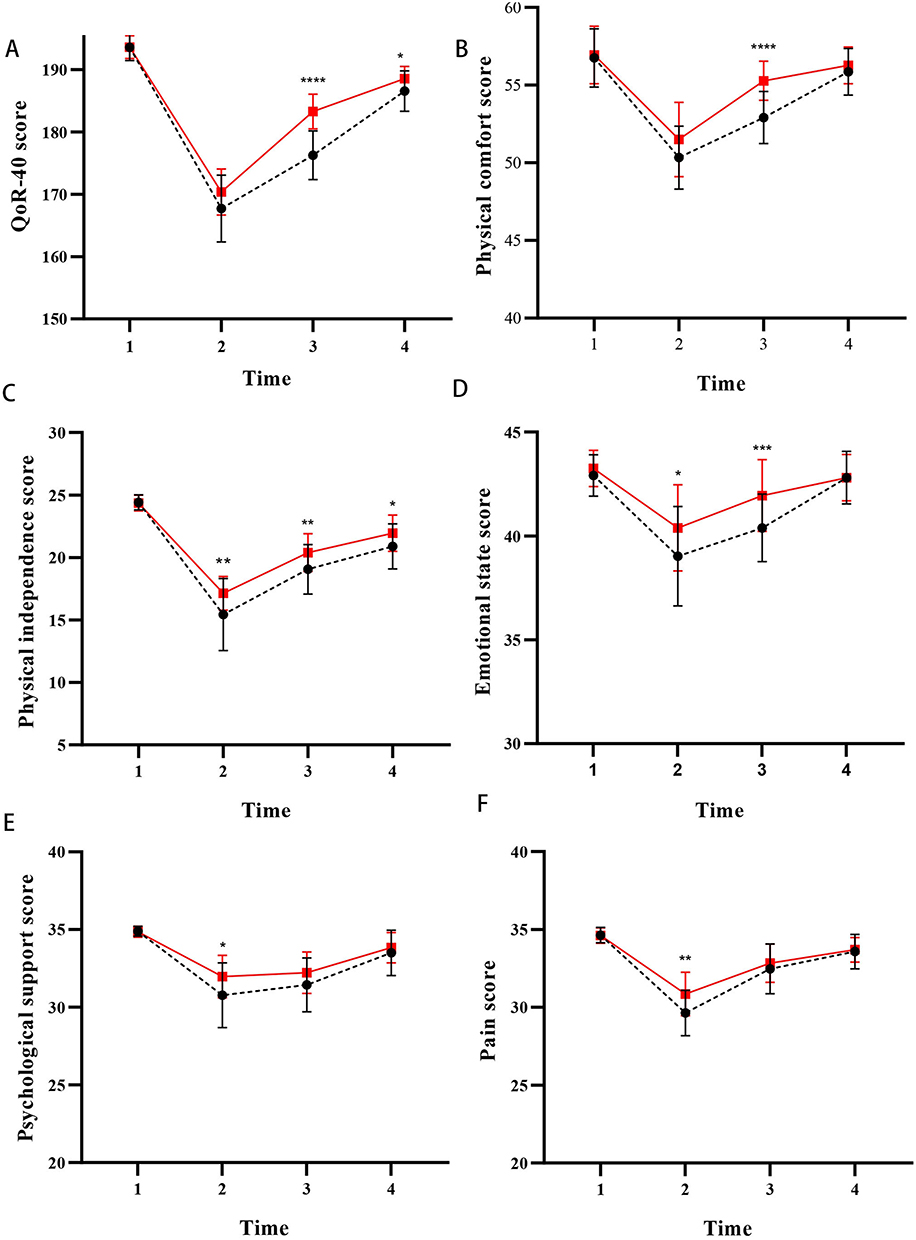 |
Figure 2 Scores of QoR-40 and scores of the five dimensions. X-axis 1, 2, 3, and 4 represent baseline and postoperative 6, 24, and 48 h, respectively. The solid red line represents the transcutaneous electrical acupoint stimulation (TEAS) group, and the dotted black line represents the control. Data are presented as means ± standard deviations. *P<0.05. |
There were no significant differences in HR between the two groups (P>0.05). However, MAP was significantly higher in the TEAS group compared to the control group (86.3 vs 84.2 mmHg, P<0.0001). MAP levels were comparable at baseline (T0); however, following the initiation of surgery, MAP decreased significantly more in the control group than in the TEAS group at T1, T2, and T4, with the most pronounced difference occurring at the time of skin incision (P<0.0001) (Figure 3). Although HR varied across time points, there were no significant differences between the groups (P>0.05).
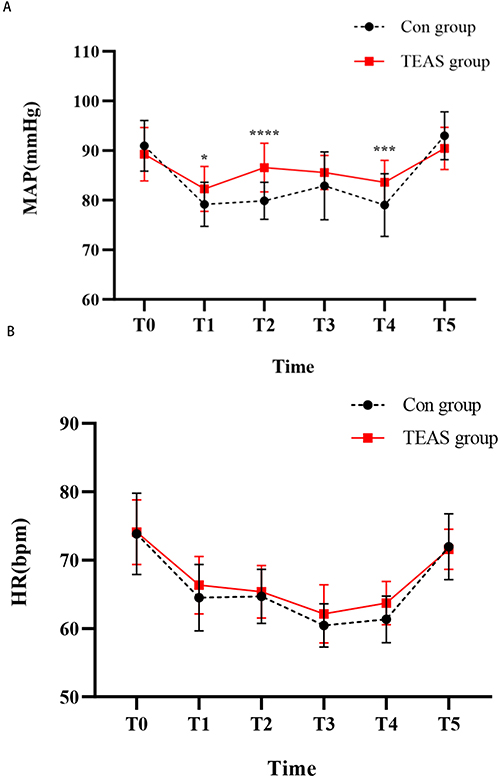 |
Figure 3 Intraoperative hemodynamic outcomes. (A) MAP at different time points in the two groups. (B) HR at different time points in the two groups. Data are presented as means ± standard deviations. *P<0.05, ***P<0.001,****P<0.0001. Abbreviations: MAP, mean arterial pressure; HR, heart rate. |
The TEAS group also demonstrated lower blood glucose levels 30 minutes after skin incision compared to the control group (P=0.045), reduced remifentanil consumption during surgery (P=0.031), fewer total and effective patient-controlled intravenous analgesia (PCIA) presses (P=0.004 and P=0.039, respectively), and faster recovery of gastrointestinal function (P<0.05) (Table 3). No significant differences were observed between the two groups with respect to propofol and sevoflurane usage during surgery, the number of emergency rescue analgesia events, the occurrence of adverse events, awakening time, PACU stay, or hospital length of stay (all P>0.05) (Table 3).
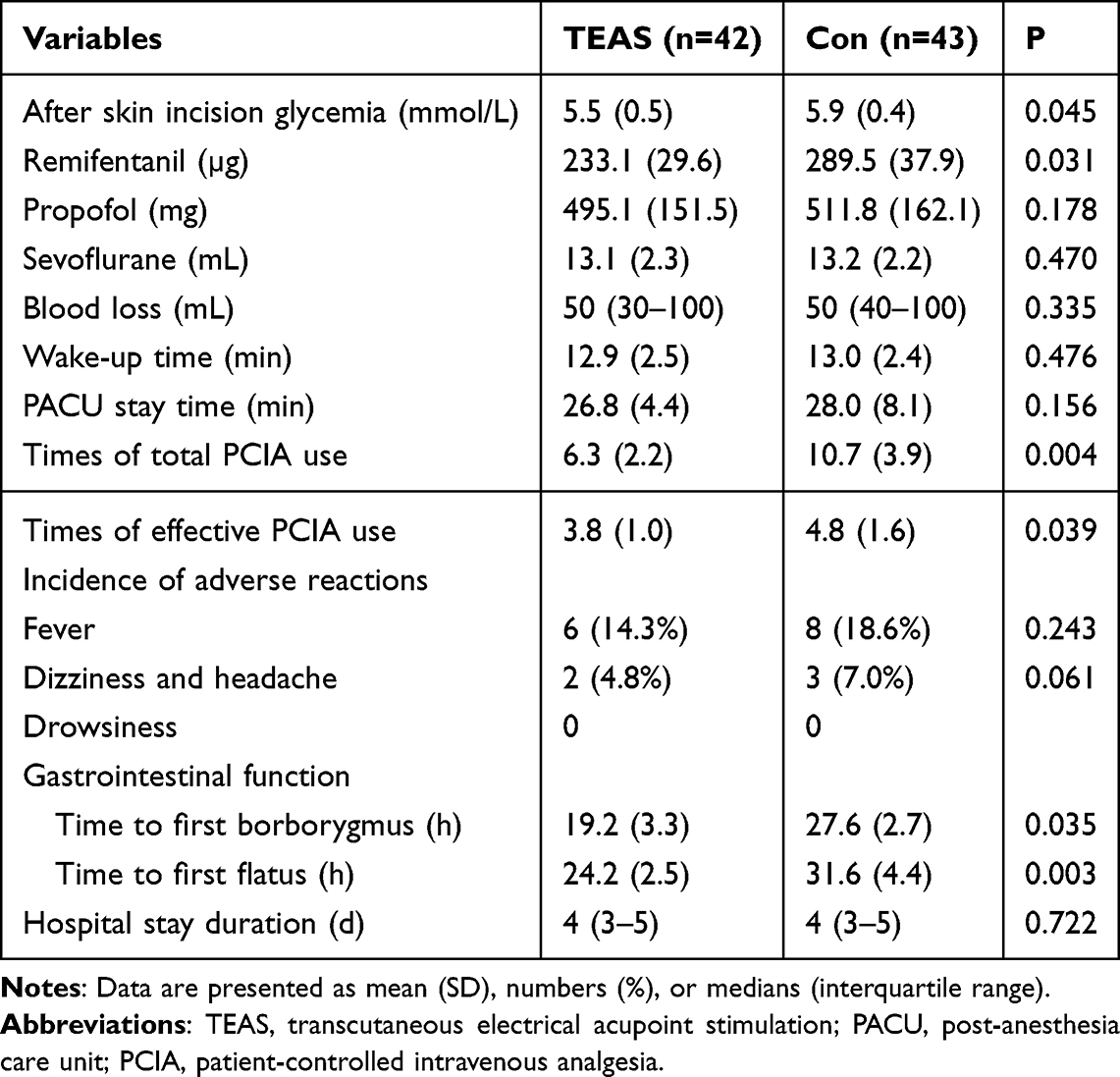 |
Table 3 Perioperative Data Between the Two Groups |
Although the two groups had similar preoperative sleep quality, the TEAS group reported significantly better sleep quality on the first and second postoperative days, as indicated by higher PSQI scores (P=0.015 and P=0.024, respectively). Furthermore, the TEAS group had lower NRS pain scores at 6 and 24 hours postoperatively (P=0.022 and P=0.042, respectively) (Table 4).
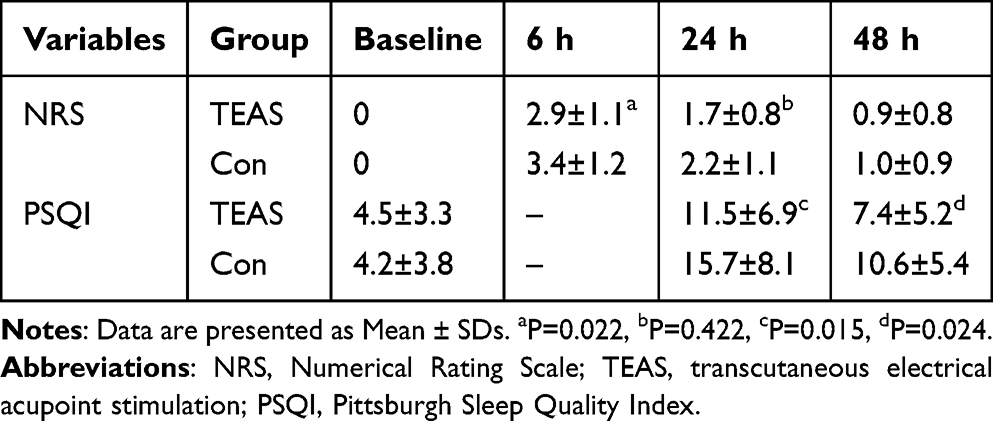 |
Table 4 NRS and PSQI Scores Were Compared at Different Points in Time |
Discussion
This randomized, single-blind, controlled trial evaluated the effects of TEAS on the quality of recovery in patients undergoing gynecological laparoscopic surgery. The findings demonstrate that preoperative and intraoperative TEAS significantly reduce the incidence of early PONV, enhance recovery outcomes, alleviate stress responses, improve sleep quality, and reduce the occurrence of adverse events. Nevertheless, it is important to note that the improvements in QoR-30 scores were statistically significant but not clinically significant.
This randomized controlled trial demonstrated that TEAS enhanced postoperative recovery quality in patients undergoing gynecological laparoscopic surgery by modulating early PONV and multiple recovery parameters. The results revealed a 24.5% reduction in 24-hour PONV incidence in the TEAS group compared with controls (42.9% vs 67.4%). This finding aligns with the mechanistic study by Cheong et al,23 which demonstrated that acupoint stimulation suppresses 5-HT3 receptor activity through the vagal nucleus tractus solitarius pathway. The 5-HT3 receptor plays a crucial role in nausea and vomiting. Serotonin, when released, can activate 5-HT3 receptors in the gastrointestinal tract and the central nervous system, ultimately triggering nausea and vomiting. Antagonizing the 5-HT3 receptor is a strategy used to treat PONV by blocking the effects of serotonin at these receptors.24,25 The TEAS group had a shorter recovery time for gastrointestinal functions and a significantly lower incidence of PONV, similar to previous studies.26–28 TEAS exhibited a distinct time-dependent antiemetic effect: the absolute risk reduction for nausea reached 25% during the critical 0–2 hour postoperative window, while its efficacy gradually attenuated in the subsequent 2–6 hour period. This temporal kinetic profile suggests that TEAS may primarily exert its effects through transient modulation of enterochromaffin cell signaling rather than sustained alteration of neurotransmitter levels, which shows intrinsic consistency with the multiphase regulatory model of postoperative nausea proposed by Gan et al.29
The TEAS group demonstrated a statistically significant improvement in recovery quality assessment, as shown by higher QoR-40 total scores compared with controls at 48 hours postoperatively (184.0 vs 181.0, p<0.001), representing 47.6% of the established minimal clinically important difference (MCID=6.3 points).20 The concurrent improvement across all five subdomains (physical comfort, emotional state, physical independence, psychological support, and pain control) suggests that TEAS likely exerts its therapeutic effects through multiple interconnected physiological pathways. Yao et al30 reported higher QoR-40 scores in the TEAS group after gynecological laparoscopic surgery. Notably, TEAS demonstrated a characteristic delayed-enhancement pattern in overall recovery quality improvement: while no significant difference was observed in QoR-40 scores at 6 hours postoperatively (P=0.068), the treatment effect peaked at 24 hours (P<0.0001). This temporal pattern likely reflects the requisite time window for hypothalamic-pituitary-adrenal (HPA) axis recalibration, which aligns precisely with the postoperative recovery phase model,31,32 featuring initial physiological stabilization (<6 h), followed by functional recovery (6–24 h), and ultimately psychosocial adaptation (>24 h). Therefore, TEAS, as a non-pharmacological intervention, appears clinically important in reducing the incidence of PONV after gynecological laparoscopy and promoting the early recovery of the patients.
Poor quality of postoperative recovery in patients undergoing gynecological laparoscopic surgery can be due to several factors. CO2 inflation increases intra-thoracic and intra-abdominal pressures, leading to a decrease in cardiac output and an increase in sympathetic activity.33,34 In addition, excessive CO2 in the blood predisposes to hypercapnia and stimulates the release of humoral factors such as catecholamines and cortisol from aortic body chemoreceptors.35,36 These changes initiate the stress response through the sympathetic-adrenomedullary and hypothalamic-pituitary-adrenocortical dual systems, causing fluctuations in blood flow and damage to target organs, affecting the perfusion of vital organs.37,38 TEAS can make the perioperative blood pressure and HR smoother, and by regulating the levels of plasma cortisol and adrenocorticotropic hormone, it can alleviate the stress response to a certain degree, preventing damage to the body caused by overstress. It can also reduce the secondary damage caused by stress, enhance the body’s ability to resist damage and repair trauma, promote postoperative recovery, and improve prognosis.14
Elevated glycemia is a common sign of stress induced by surgical trauma.37 In a study of hysterectomies, it was found that the simultaneous preoperative stimulation of the Sanyinjiao and the Foot Sanli had a significant inhibitory effect on intraoperative glycemia and insulin tolerance.39 In another study of craniotomy in elderly patients, TEAS was found to reduce the stress response during extubation, and hemodynamic parameters and plasma concentrations of epinephrine, norepinephrine, and cortisol decreased during extubation in the TEAS group.40 The results of this trial also found that the glycemia in the TEAS group was significantly lower than in the control group at 30 min after skin incision, while MAP and HR fluctuated less compared with basal values after intubation, but MAP and HR fluctuated quite a bit at other moments, which might be related to the regulation of the depth of anesthesia after intubation.
Perioperative pain is one of the main aspects affecting the quality of postoperative recovery, not only affecting the patient’s emotional state but also associated with postoperative sleep disturbances.41,42 Pain leads to prolonged sleep latency and reduced total sleep time, whereas sleep disturbances also increase pain sensitivity and decrease pain threshold.43,44 TEAS analgesia acts as a complex network of regulatory mechanisms, from the peripheral to the central nervous system, involving multiple molecular pathways, inflammatory factors, neurotransmitters, and the properties of the acupoints themselves.45 A growing number of clinical trials15,46–48 demonstrated that TEAS can increase anesthesia effect, effectively reduce the need for perioperative analgesia, produce organ protection, and promote the recovery of gastrointestinal function. Acupuncture on LI4 and PC6 can stimulate the release of endogenous opioid peptides from the center, impede the upward transmission of pain messages, and enhance postoperative analgesia.49 TEAS not only significantly relieves acute pain up to 24 hours after surgery50 but also alleviates chronic pain up to half a year after radical mastectomy for breast cancer.46 The present study showed that the TEAS group consumed less intraoperative remifentanil and had a lower number of PCIA uses. Kjolhede et al51 concluded that sleep quality after gynecological surgery is an important factor influencing postoperative recovery, with a PSQI score of ≥6 defined as the presence of a sleep disorder.52 Here, the study showed lower PSQI scores in the TEAS group within 2 days after surgery, concluding that TEAS may improve postoperative sleep quality.
Limitations of the Study
This study presents several limitations. Firstly, the inclusion criteria encompassed only ASAI-II patients, necessitating further confirmation of the generalizability of the findings. Secondly, this trial implemented preoperative and intraoperative TEAS, which may limit compatibility with other studies that utilized different protocols. Thirdly, the duration of follow-up was relatively short, and the data collected were limited in scope. Fourth, the single-blind design may introduce performance bias, as the anesthesiologists administering TEAS were not blinded. However, outcome assessors and data analysts were blinded to minimize bias. Fifth, this was a single-center study, which may limit the generalizability of the findings. Future multicenter trials are warranted to confirm these results. Lastly, improvements in QoR-40 scores were statistically significant but below the minimal clinically important difference, limiting clinical relevance. Consequently, the effects of TEAS on the long-term postoperative recovery of patients warrant further investigation.
Conclusion
This trial indicates that TEAS was associated with improvements in the quality of postoperative recovery in patients undergoing gynecological laparoscopic surgery. Still, the improvements in QoR-30 scores were statistically significant but fell short of being clinically significant. TEAS appears to mitigate perioperative blood flow fluctuations by diminishing the stress response, reducing the incidence of PONV, and lowering the requirement for perioperative analgesia. Additionally, it may facilitate a quicker return of gastrointestinal function, improve sleep quality, and contribute to a more rapid recovery during the postoperative period.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
The study was approved by the Ethics Committee of the General Hospital of the Northern Theatre Command of the Chinese People’s Liberation Army (Approval No. Y (2021)138). All participants were informed about the study protocol and provided written informed consent to participate in the study. I confirm that all methods were performed in accordance with the relevant guidelines. All procedures were performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Liaoning Provincial Joint Science and Technology Program (2024JH2/102600283).
Disclosure
The authors declare that they have no competing interests.
References
1. Levy L, Tsaltas J. Recent advances in benign gynecological laparoscopic surgery. Fac Rev. 2021;10:60. doi:10.12703/r/10-60
2. Tica VI, Tica AA, De Wilde RL. The Future in Standards of Care for Gynecologic Laparoscopic Surgery to Improve Training and Education. J Clin Med. 2022;11(8):2192. doi:10.3390/jcm11082192
3. Ferrari F, Forte S, Sbalzer N, et al. Validation of an enhanced recovery after surgery protocol in gynecologic surgery: an Italian randomized study. Am J Clin Exp Obstet Gynecol. 2020;223(4):543.e1–543.e14. doi:10.1016/j.ajog.2020.07.003
4. Stone R, Carey E, Fader AN, et al. Enhanced Recovery and Surgical Optimization Protocol for Minimally Invasive Gynecologic Surgery: an AAGL White Paper. J Minimally Invasive Gynecol. 2021;28(2):179–203. doi:10.1016/j.jmig.2020.08.006
5. Philosophe R. Avoiding complications of laparoscopic surgery. Fertil Steril. 2003;80(4):30–39. doi:10.1016/s0015-0282(03)01189-0
6. Atkinson TM, Giraud GD, Togioka BM, Jones DB, Cigarroa JE. Cardiovascular and Ventilatory Consequences of Laparoscopic Surgery. Circulation. 2017;135(7):700–710. doi:10.1161/CIRCULATIONAHA.116.023262
7. Gan TJ, Belani KG, Bergese S, et al. Fourth Consensus Guidelines for the Management of Postoperative Nausea and Vomiting. Anesthesia Analg. 2020;131(2):411–448. doi:10.1213/ane.0000000000004833
8. Wu CL, Berenholtz SM, Pronovost PJ, Fleisher LA. Systematic review and analysis of postdischarge symptoms after outpatient surgery. Anesthesiology. 2002;96(4):994–1003. doi:10.1097/00000542-200204000-00030
9. Yuan W, Wang Q. Perioperative acupuncture medicine: a novel concept instead of acupuncture anesthesia. Chinese Med J. 2019;132(6):707–715. doi:10.1097/cm9.0000000000000123
10. Szmit M, Krajewski R, Rudnicki J, Agrawal S. Application and efficacy of transcutaneous electrical acupoint stimulation (TEAS) in clinical practice: a systematic review. Adv Clin Exp Med. 2023;32(9):1063–1074. doi:10.17219/acem/159703
11. Yu X, Zhang F, Chen B. The effect of TEAS on the quality of early recovery in patients undergoing gynecological laparoscopic surgery: a prospective, randomized, placebo-controlled trial. Trials. 2020;21(1):43. doi:10.1186/s13063-019-3892-4
12. Chen J, Zhang Y, Li X, et al. Efficacy of transcutaneous electrical acupoint stimulation combined with general anesthesia for sedation and postoperative analgesia in minimally invasive lung cancer surgery: a randomized, double-blind, placebo-controlled trial. Thoracic Cancer. 2020;11(4):928–934. doi:10.1111/1759-7714.13343
13. Li WJ, Gao C, An LX, Ji YW, Xue FS, Du Y. Perioperative transcutaneous electrical acupoint stimulation for improving postoperative gastrointestinal function: a randomized controlled trial. J Integr Med. 2021;19(3):211–218. doi:10.1016/j.joim.2021.01.005
14. Chi YL, Zhang WL, Yang F, Su F, Zhou YK. Transcutaneous Electrical Acupoint Stimulation for Improving Postoperative Recovery, Reducing Stress and Inflammatory Responses in Elderly Patient Undergoing Knee Surgery. Am J Chin Med. 2019;47(7):1445–1458. doi:10.1142/s0192415x19500745
15. Wang D, Shi H, Yang Z, et al. Efficacy and Safety of Transcutaneous Electrical Acupoint Stimulation for Postoperative Pain: a Meta-Analysis of Randomized Controlled Trials. Pain Res Manag. 2022;2022:7570533. doi:10.1155/2022/7570533
16. Hoshijima H, Miyazaki T, Mitsui Y, Omachi S, Yamauchi M, Mizuta K. Machine learning-based identification of the risk factors for postoperative nausea and vomiting in adults. PLoS One. 2024;19(8):e0308755. doi:10.1371/journal.pone.0308755
17. Nöst R, Thiel-Ritter A, Scholz S, Hempelmann G, Müller M. Balanced anesthesia with remifentanil and desflurane: clinical considerations for dose adjustment in adults. J Opioid Manag Sep-Oct. 2008;4(5):305–309. doi:10.5055/jom.2008.0034
18. Lang E, Kapila A, Shlugman D, Hoke JF, Sebel PS, Glass PS. Reduction of isoflurane minimal alveolar concentration by remifentanil. Anesthesiology. 1996;85(4):721–728. doi:10.1097/00000542-199610000-00006
19. Gornall BF, Myles PS, Smith CL, et al. Measurement of quality of recovery using the QoR-40: a quantitative systematic review. Br J Anaesth. 2013;111(2):161–169. doi:10.1093/bja/aet014
20. Wessels E, Perrie H, Scribante J, Jooma Z. Quality of recovery in the perioperative setting: a narrative review. J Clini Anesthesia. 2022;78:110685. doi:10.1016/j.jclinane.2022.110685
21. Echeverria-Villalobos M, Fiorda-Diaz J, Uribe A, Bergese SD. Postoperative Nausea and Vomiting in Female Patients Undergoing Breast and Gynecological Surgery: a Narrative Review of Risk Factors and Prophylaxis. Front Med Lausanne. 2022;9:909982. doi:10.3389/fmed.2022.909982
22. Yan S, Xu M, Zou X, et al. Acupuncture combined with ondansetron for prevention of postoperative nausea and vomiting in high-risk patients undergoing laparoscopic gynaecological surgery: a randomised controlled trial. United Eur Gastroenterol J. 2023;11(6):564–575. doi:10.1002/ueg2.12421
23. Cheong K. Neuromodulatory Effects of Acupoint Stimulation on 5-HT3 Receptor Signaling in the Solitary Tract Nucleus. J Neurogastroenterol Motility. 2021;2021:1.
24. Theriot J, Wermuth HR, Ashurst JV. Antiemetics, Selective 5-HT3 Antagonists. StatPearls. 2025;2025:1.
25. Smith HS, Cox LR, Smith EJ. 5-HT3 receptor antagonists for the treatment of nausea/vomiting. Ann Palliative Med. 2012;1(2):2.
26. Gao W, Li W, Yan Y, et al. Transcutaneous electrical acupoint stimulation applied in lower limbs decreases the incidence of paralytic ileus after colorectal surgery: a multicenter randomized controlled trial. Surgery. 2021;170(6):1618–1626. doi:10.1016/j.surg.2021.08.007
27. Wang N, Ding P, Zheng DY, et al. Wearable transcutaneous electrical acupoint stimulation bracelet for prevention of postoperative nausea and vomiting in patients undergoing hysteroscopic surgery: a randomised controlled trial. Br J Anaesth. 2022;129(4):e85–e87. doi:10.1016/j.bja.2022.06.028
28. Li S, Zheng M, Wu W, Guo J, Ji F, Zheng Z. Effects of Electroacupuncture Administered 24hours Prior to Surgery on Postoperative Nausea and Vomiting and Pain in Patients Undergoing Gynecologic Laparoscopic Surgery: a Feasibility Study. Explore. 2017;13(5):313–318. doi:10.1016/j.explore.2017.06.002
29. Gan T. Mechanisms and Management of Postoperative Nausea: a Comprehensive Review. Anesthesiology. 2023;138(2):280–295.
30. Yao Y, Zhao Q, Gong C, et al. Transcutaneous Electrical Acupoint Stimulation Improves the Postoperative Quality of Recovery and Analgesia after Gynecological Laparoscopic Surgery: a Randomized Controlled Trial. eCAM. 2015;2015:324360. doi:10.1155/2015/324360
31. Lee L, Tran T, Mayo NE, Carli F, Feldman LS. What does it really mean to “recover” from an operation? Surgery. 2014;155(2):211–216. doi:10.1016/j.surg.2013.10.002
32. Bowyer AJ, Royse CF. Postoperative recovery and outcomes – what are we measuring and for whom? Anaesthesia. 2016;71(S1):72–77. doi:10.1111/anae.13312
33. Gutt CN, Oniu T, Mehrabi A, et al. Circulatory and Respiratory Complications of Carbon Dioxide Insufflation. Digestive Surgery. 2004;21(2):95–105. doi:10.1159/000077038
34. Popowicz P, Newman RK, Dominique E. Abdominal Compartment Syndrome. StatPearls. 2025;2025:1.
35. Henny CP, Hofland J. Laparoscopic surgery: pitfalls due to anesthesia, positioning, and pneumoperitoneum. Surg Endosc. 2005;19(9):1163–1171. doi:10.1007/s00464-004-2250-z
36. Andersson LE, Bååth M, Thörne A, Aspelin P, Odeberg-Wernerman S. Effect of carbon dioxide pneumoperitoneum on development of atelectasis during anesthesia, examined by spiral computed tomography. Anesthesiology. 2005;102(2):293–299. doi:10.1097/00000542-200502000-00009
37. Finnerty CC, Mabvuure NT, Ali A, Kozar RA, Herndon DN. The surgically induced stress response. JPEN J Parenter Enteral Nutr. 2013;37(5 Suppl):21s–9s. doi:10.1177/0148607113496117
38. Chen L, Shen Y, Liu S, Cao Y. Transcutaneous Electrical Acupoint Stimulation Improved Preoperative Blood Pressure in Gynecological Malignant Tumor Patients With Hypertension: a Randomized, Controlled Trial. Front Oncol. 2022;12:906528. doi:10.3389/fonc.2022.906528
39. Man KM, Man SS, Shen JL, et al. Transcutaneous electrical nerve stimulation on ST36 and SP6 acupoints prevents hyperglycaemic response during anaesthesia: a randomised controlled trial. Eur J Anaesthesiol. 2011;28(6):420–426. doi:10.1097/EJA.0b013e32833fad52
40. Bai WY, Yang YC, Teng XF, Wan YX, Wei W, Zhu JC. Effects of Transcutaneous Electrical Acupoint Stimulation on the Stress Response During Extubation After General Anesthesia in Elderly Patients Undergoing Elective Supratentorial Craniotomy: a Prospective Randomized Controlled Trial. J Neurosurg Anesthesiol. 2018;30(4):337–346. doi:10.1097/ana.0000000000000460
41. Li Q, Zhu ZY, Lu J, et al. Sleep deprivation of rats increases postsurgical expression and activity of L-type calcium channel in the dorsal root ganglion and slows recovery from postsurgical pain. Acta Neuropathol Commun. 2019;7(1):217. doi:10.1186/s40478-019-0868-2
42. Song B, Luo M, Zhu J. The efficacy of acupuncture in postoperative sleep quality: a literature review. Sleep Breathing. 2021;25(2):571–577. doi:10.1007/s11325-020-02187-x
43. Haack M, Simpson N, Sethna N, Kaur S, Mullington J. Sleep deficiency and chronic pain: potential underlying mechanisms and clinical implications. Neuropsychopharmacology. 2020;45(1):205–216. doi:10.1038/s41386-019-0439-z
44. Letzen JE, Remeniuk B, Smith MT, Irwin MR, Finan PH, Seminowicz DA. Individual differences in pain sensitivity are associated with cognitive network functional connectivity following one night of experimental sleep disruption. Human Brain Mapp. 2020;41(3):581–593. doi:10.1002/hbm.24824
45. Shah S, Godhardt L, Spofford C. Acupuncture and Postoperative Pain Reduction. Current Pain Headache Rep. 2022;26(6):453–458. doi:10.1007/s11916-022-01048-4
46. Lu Z, Wang Q, Sun X, et al. Transcutaneous electrical acupoint stimulation before surgery reduces chronic pain after mastectomy: a randomized clinical trial. J Clini Anesthesia. 2021;74:110453. doi:10.1016/j.jclinane.2021.110453
47. Li H, Du C, Lu L, et al. Transcutaneous electrical acupoint stimulation combined with electroacupuncture promotes rapid recovery after abdominal surgery: study protocol for a randomized controlled trial. Front Public Health. 2022;10:1017375. doi:10.3389/fpubh.2022.1017375
48. Pan P, Zhang X, Qian H, et al. Effects of electro-acupuncture on endothelium-derived endothelin-1 and endothelial nitric oxide synthase of rats with hypoxia-induced pulmonary hypertension. Experiment Biol Med. 2010;235(5):642–648. doi:10.1258/ebm.2010.009353
49. Chen J, Tu Q, Miao S, Zhou Z, Hu S. Transcutaneous electrical acupoint stimulation for preventing postoperative nausea and vomiting after general anesthesia: a meta-analysis of randomized controlled trials. Int J Surg. 2020;73:57–64. doi:10.1016/j.ijsu.2019.10.036
50. Liu X, Li S, Wang B, An L, Ren X, Wu H. Intraoperative and postoperative anaesthetic and analgesic effect of multipoint transcutaneous electrical acupuncture stimulation combined with sufentanil anaesthesia in patients undergoing supratentorial craniotomy. Acupuncture Med. 2015;33(4):270–276. doi:10.1136/acupmed-2014-010749
51. Kjølhede P, Langström P, Nilsson P, Wodlin NB, Nilsson L. The impact of quality of sleep on recovery from fast-track abdominal hysterectomy. J Clin Sleep Med. 2012;8(4):395–402. doi:10.5664/jcsm.2032
52. Tsai PS, Wang SY, Wang MY, et al. Psychometric evaluation of the Chinese version of the Pittsburgh Sleep Quality Index (CPSQI) in primary insomnia and control subjects. Qual Life Res. 2005;14(8):1943–1952. doi:10.1007/s11136-005-4346-x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Transcutaneous Acupoint Electrical Stimulation on Urinary Retention and Urinary ATP in Elderly Patients After Laparoscopic Cholecystectomy: A Prospective, Randomized, Controlled Clinical Trial
Zhang Y, Gong L, Zhang Y, Dong S, Shi J, Li X, Guo Y, He S, Wu X, Liu S, Liu H, Zhang L, Yu J
Clinical Interventions in Aging 2022, 17:1751-1760
Published Date: 1 December 2022
Acupuncture and Moxibustion in the Treatment of Gynecological Perioperative Anxiety: A Systematic Review and Meta-Analysis
Wang X, Yu Q, Zhu J, Liu J, Gao X, Wang X, Wang L, Xu X
Journal of Pain Research 2024, 17:3515-3538
Published Date: 31 October 2024
The Effect of Transcutaneous Electrical Acupuncture Stimulation on Postoperative Pain Control and Mobility in Patients Undergoing Percutaneous Endoscopic Lumbar Discectomy: Study Protocol for a Prospective Randomized Trial
Hu CF, Meng FX, Luo X, Chen BY
Journal of Pain Research 2025, 18:6345-6357
Published Date: 26 November 2025
Effect of Continuous Perioperative Transcutaneous Electrical Acupoint Stimulation on Postoperative Delirium in Elderly Patients Undergoing Laparoscopic Gastrointestinal Surgery: A Randomized Controlled Trial
Gao L, Chu J, Liu YS, Zhang H, Chen Y, Li Z, Deng K
Clinical Interventions in Aging 2026, 21:581811
Published Date: 23 February 2026