Back to Journals » Clinical Interventions in Aging » Volume 17
Effect of Transcutaneous Acupoint Electrical Stimulation on Urinary Retention and Urinary ATP in Elderly Patients After Laparoscopic Cholecystectomy: A Prospective, Randomized, Controlled Clinical Trial
Authors Zhang Y, Gong L, Zhang Y, Dong S, Shi J, Li X, Guo Y, He S, Wu X, Liu S, Liu H, Zhang L, Yu J
Received 21 July 2022
Accepted for publication 21 November 2022
Published 1 December 2022 Volume 2022:17 Pages 1751—1760
DOI https://doi.org/10.2147/CIA.S382912
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Yanfang Zhang, Lirong Gong, Yuan Zhang, Shuan Dong, Jia Shi, Xiangyun Li, Yan Guo, Simeng He, Xiaoyang Wu, Shasha Liu, Huayang Liu, Lantian Zhang, Jianbo Yu
Department of Anesthesiology and Critical Care Medicine, Tianjin Nankai Hospital, Tianjin Medical University, Tianjin, People’s Republic of China
Correspondence: Jianbo Yu, Department of Anesthesiology and Critical Care Medicine, Tianjin Nankai Hospital, 6 Changjiang Road, Tianjin, 300100, People’s Republic of China, Tel +86-22-23475289, Email [email protected]
Purpose: To investigate the effect of transcutaneous electrical acupoint stimulation (TEAS) on urinary retention after laparoscopic cholecystectomy in elderly patients, and to explore the relationship between TEAS and urinary ATP.
Patients and Methods: The TEAS group was administered active TEAS at specific acupuncture points prior to induction of anesthesia and continued for 45 mins after surgery. In the control group, participants received sham stimulus at the same acupoints and no output current was delivered by disconnecting the device’s output line. Urine samples were collected and evaluated in the first spontaneous voiding after surgery. In this study, postoperative urinary retention (POUR) was the primary outcome, which was diagnosed based on clinical symptoms, ultrasound assessments, and the need for bladder catheterization. Secondary outcomes include urinary ATP, postoperative spontaneous urination, urination symptoms, catheter-related bladder discomfort (CRBD), delirium, duration and hospitalization costs.
Results: The study involved 598 patients recruited and randomized between August 2018 and June 2020. Among these patients, 547 (91.5%) completed the study and were analyzed. There were 64 cases of POUR, including 23 (8.4%, 95% confidence interval [CI]: 6.4– 9.9%) in the TEAS group and 41 (15.0%, 95% CI: 9.3– 13.4%) in the control group (p = 0.017). A significant difference was observed between the TEAS and control groups for urinary ATP concentration in the first spontaneous urine postoperatively (344 nmol/L versus 233 nmol/L, p=0.001). There was a shorter spontaneous voiding recovery time, smaller voiding threshold, less postoperative catheterization, less CRBD, and lower hospitalization costs in TEAS group compared with control group.
Conclusion: TEAS reduces the incidence of POUR in elderly patients undergoing laparoscopic cholecystectomy, which may be related to an increase in bladder ATP release.
Keywords: transcutaneous electrical acupoint stimulation, urinary retention, ATP, catheterization, laparoscopic surgery, catheter-related bladder discomfort
Introduction
Urinary retention is a common complication after anesthesia, often accompanied by painful vesical distention and cardiovascular responses, and can lead to motility and atony problems, especially in older patients.1,2 In addition, in the elderly, urinary retention is associated with restlessness, confusion, and the possibility of delirium.3
In general anesthesia, stress responses are attenuated and sympathetic nerve activity is inhibited, as well as vagus nerve activity is inhibited.4 As a result of reduced parasympathetic activity, baroreceptor function may be impaired and the recovery of spontaneous urination may be delayed.5 Aging is a physiological process associated with dysfunction of the autonomic nervous system.6,7 The physiological response to anesthesia may be unpredictable and paradoxical if the autonomic nervous system is dysfunctional. ATP, the principal messenger released from urothelial cells, is a co-transmitter together with noradrenaline in sympathetic nerves and acetylcholine in parasympathetic nerves and considered a potential therapeutic target for functional bladder functional disorders.8
In recent years, acupuncture has gained popularity as a method of improving urination control. Acupuncture and related methods have been shown to reduce the incidence of urinary retention after orthopedic, obstetric and gynecological, and gastrointestinal procedures.9–11 Transcutaneous electrical acupoint stimulation (TEAS), which applies electrical stimulation to acupuncture points instead of needles, has shown benefits in studies relating to regulating voiding, but remains controversial when used in elderly patients.12,13 In addition, the effect of TEAS on urinary ATP function in patients following surgery is unclear. Therefore, we conducted a double-blind randomized trial and hypothesized that TEAS is effective in reducing urinary retention following laparoscopic cholecystectomy and is associated with increased urinary ATP release.
Materials and Methods
Design
The study was approved by the ethics committee of Tianjin Nankai Hospital and is in accordance with the Helsinki Declaration. The trial was registered at ClinicalTrials.gov (registration number: NCT03631160). Written informed consent was obtained from all participating patients prior to randomization.
Patients
Inclusion criteria were: (1) age above 65 years; (2) elective laparoscopic cholecystectomy under general anesthesia; (3) no preventive or intraoperative indwelling catheter. The criteria for exclusion were: (1) urinary tract obstruction or infection, such as moderate or severe benign prostatic hyperplasia (International Prostate Symptom Score (I-PSS) greater than 7), urinary tract infections in the last 3 months; (2) contraindications for TEAS such as skin allergy, infections, itching or pacemaker wear; (3) previous experience with multiple acupuncture sessions; (4) preoperative American Society of Anaesthetists (ASA) grade ≥ IV; (5) severe impairment requiring kidney replacement therapy; and (6) participation in other clinical investigations within 3 months.
Eligible participants were randomly assigned to the TEAS and control groups at a 1:1 ratio using block randomization. Random numbers were then sealed in sequentially numbered, opaque envelopes which were revealed by the acupuncture before administration. Participants, outcome assessors and statisticians were blinded to the treatment allocation.
TEAS Administration
Four acupoints were selected as the stimulation points: Ciliao (BL32, bilateral), Sanyinjiao (SP6, bilateral), Zhongji (CV3), and Guanyuan (CV4). The above acupoints are located in lower back, lower leg and lower abdomen. Their positioning is based on the National Standard of the People’s Republic of China: acupoint position (Figure 1). TEAS was administered by a licensed acupuncturist with ≥8 years of clinical acupuncture experience. A low-frequency pulse electroacupuncture stimulator (Hwato brand model no. SDZ---IV, Suzhou Medical Appliances Co., Ltd, Suzhou, China) was attached to the selected acupoints. Stimulus started 30 mins before induction of anesthesia and lasted 45 mins after surgery. The frequency of stimulation was 4 / 20 Hz, and the intensity was determined by the patient’s tolerance until the local skin twitches slightly and the pain was tolerable.14
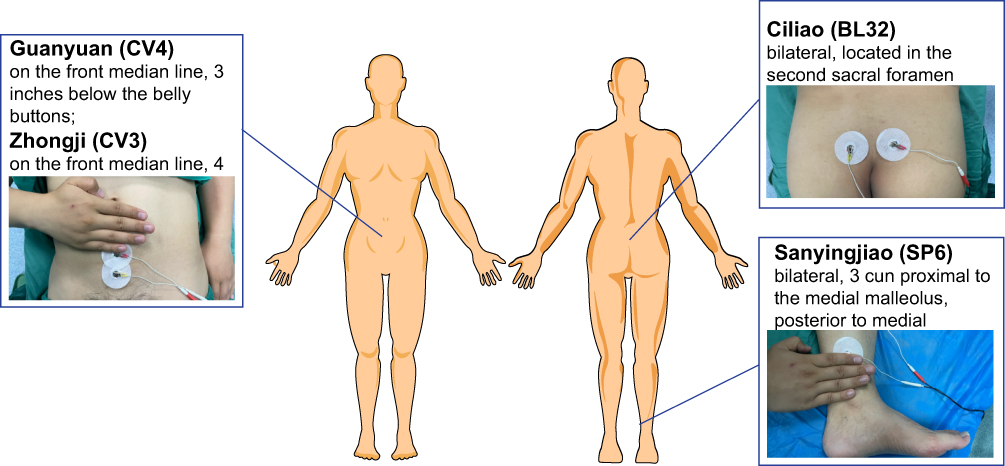 |
Figure 1 Location of acupoints in the trial. |
Participants in the control group received sham stimulus at the same points with sham electrode lines, cutting off output wires, causing no current output to pass to the patient, despite being connected. We also informed each patient that they may not feel tingling in their lower extremities and lower back when the stimulator works prior to stimulation. In addition, in order to make the simulation as realistic as possible, the stimulator with sham electrode lines had the same working power indicator and sound as the normal electrode lines, indicating that the stimulator was effective even if it does not actually have an electrical current output.
Anesthetic and Surgical Procedure
All patients were completely emptied before entering the operating room. The method of anesthesia was standard for the two groups. Anesthesia was induced with 0.2–0.6 mg/kg etomidate and 0.2–0.5 μg/kg sufentanil and maintained with remifentanil and propofol infusion. Intraoperative monitoring included an electrocardiogram, noninvasive blood pressure, peripheral capillary oxygen saturation, carbon dioxide division at the end of breathing, and the bispectral index. Intra-abdominal pressure was maintained between 8–12 mmHg. Patients were treated with Ringer’s lactate solution infusion at a rate of 10 mL/kg/h before and during the procedure. This was continued after surgery until oral fluid intake was allowed. Patient controlled intravenous analgesia (PCIA) with sufentanil combined with flurbiprofen was administered for 24–48 h postoperatively, as necessary.
Data Collection and Urinary ATP Measurements
The primary outcome was the incidence of POUR after surgery in this study. Based on clinical symptoms, ultrasound assessments, and bladder catheterization requirements, postoperative urinary retention (POUR) was diagnosed by the attending surgeon (Supplementary Table S1).2
The secondary outcomes included urinary ATP concentration, spontaneous voiding ability, urination symptoms (such as voiding difficulty, oliguria, or nocturia), Catheter-related bladder discomfort (CRBD), delirium, early ambulation, length of hospital stay, and hospital costs. CRBD was evaluated by the anesthesiology resident: none = no complaints of CRBD symptoms, mild = reported only upon direct inquiry, moderate = spontaneous complaints by the patient without behavioral responses (eg, pulling out the catheter, flailing limbs, or a loud vocal response), and severe = spontaneous complaints by the patient with behavioral responses.15 An assessment of postoperative delirium was made by trained personnel using the Confusion Assessment Method for the Intensive Care Unit (CAM–ICU) and the Richmond Agitation-Sedation Scale (RASS) from the first to the third postoperative day.16 A patient was considered delirious if he or she was awake (RASS of 3 or greater) and positive for CAM-ICU on either of the CAM–ICU assessments. Early ambulation was defined as any partial or full weight-bearing activity conducted two to three times outside the ward, with a total walking distance of 250 to 500 m.17
During the first spontaneous void after surgery, urine samples were collected from thirsty patients in each group and tested for urinary ATP levels. The urine samples were centrifuged at 2500 x g for 5 minutes and stored at-80°C. Measurement of urine ATP concentrations was performed using a luminometer and a luciferin-luciferase assay (Sigma–Aldrich). In brief, the colorimetric reaction absorbance was measured using a spectrophotometer at 460 nm, and the ATP concentration was estimated by applying the luminescence value to a standard curve of known ATP concentrations.
Statistical Analysis
We conducted all analyses using IBM SPSS 22.0 (IBM Corp., Armonk, NY, USA). Kolmogorov–Smirnov was used to test the normality of continuous data (p < 0.05: reject normality), with the mean and SD reported for normal data, and the median (IQR) for non-normal data. As appropriate, t-tests or Mann–Whitney U-tests were used to compare the two groups. Categorical variables were analyzed through the chi-squared test or Fisher’s exact probability test and summarized as numbers (%). Statistical significance was set at p < 0.05.
Results
The study assessed 712 patients who underwent elective laparoscopic cholecystectomy, of whom 598 met the inclusion/exclusion criteria. The 598 patients were enrolled and randomly assigned to two groups, the TEAS group (n = 298) and the control group (n = 300). There were 22 subjects who did not receive allocated intervention due to cancellation of surgery or preventive indwelling catheter (10 subjects from the TEAS group and 12 subjects from the control group); 29 subjects discontinued interventions due to another surgery or an intraoperative indwelling catheter (15 subjects from the TEAS group and 14 subjects from the control group). This resulted in the analysis of data on 547 subjects, including 273 patients in the TEAS group and 274 patients in the control group. A detailed patient flowchart is shown in Figure 2.
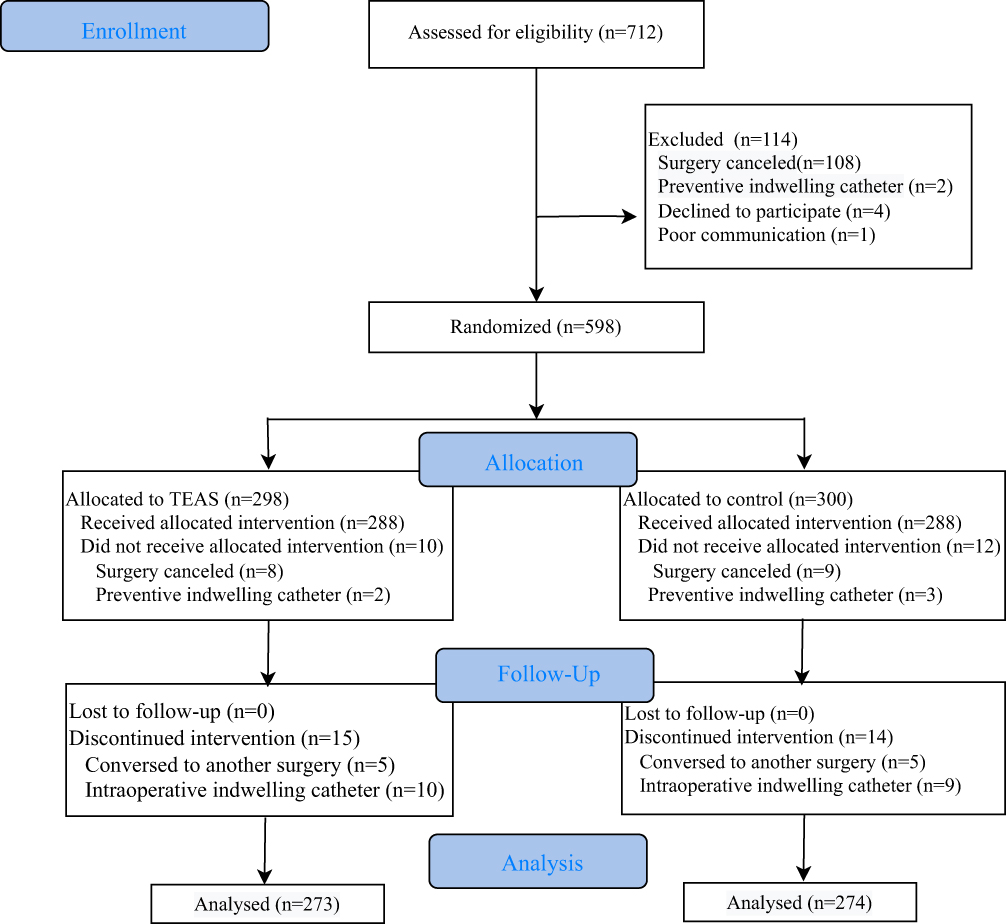 |
Figure 2 Patient flow chart. |
As can be seen in Table 1, the demographics and baseline characteristics of the patients were similar between the two groups and no significant differences were observed between the two groups (p >0.05).
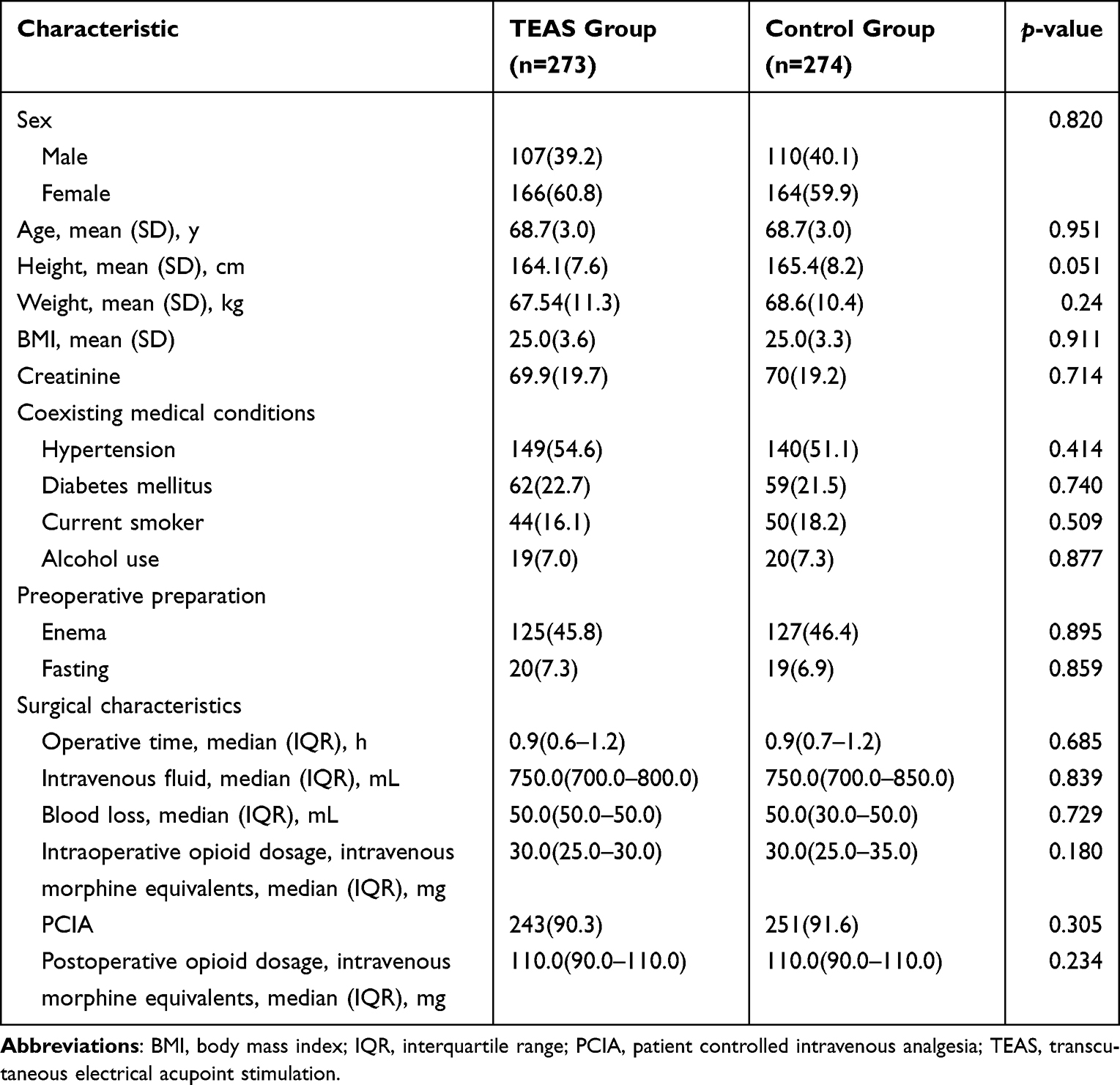 |
Table 1 Baseline Participant Characteristics |
Sixty-four patients were diagnosed with POUR, including 23 (8.4%, 95% confidence interval [CI]: 6.4–9.9%) in the TEAS group and 41 (15.0%, 95% CI: 9.3–13.4%) in the control group with a statistically significant difference (p = 0.017, Table 2). As compared to the control group, patients in the TEAS group had a shorter recovery time from spontaneous voiding (5.1 h versus 8.1 h, p =0.005) and smaller voiding threshold (414.9 mL versus 504.8 mL, p =0.048). The concentration of urinary ATP was measured in the first spontaneous urine postoperatively, and the results showed that patients in the TEAS group had a significantly higher level of ATP concentration (387.6 nmol/L versus 244.5 nmol/L, p =0.001) than those in the control group (Figure 3).
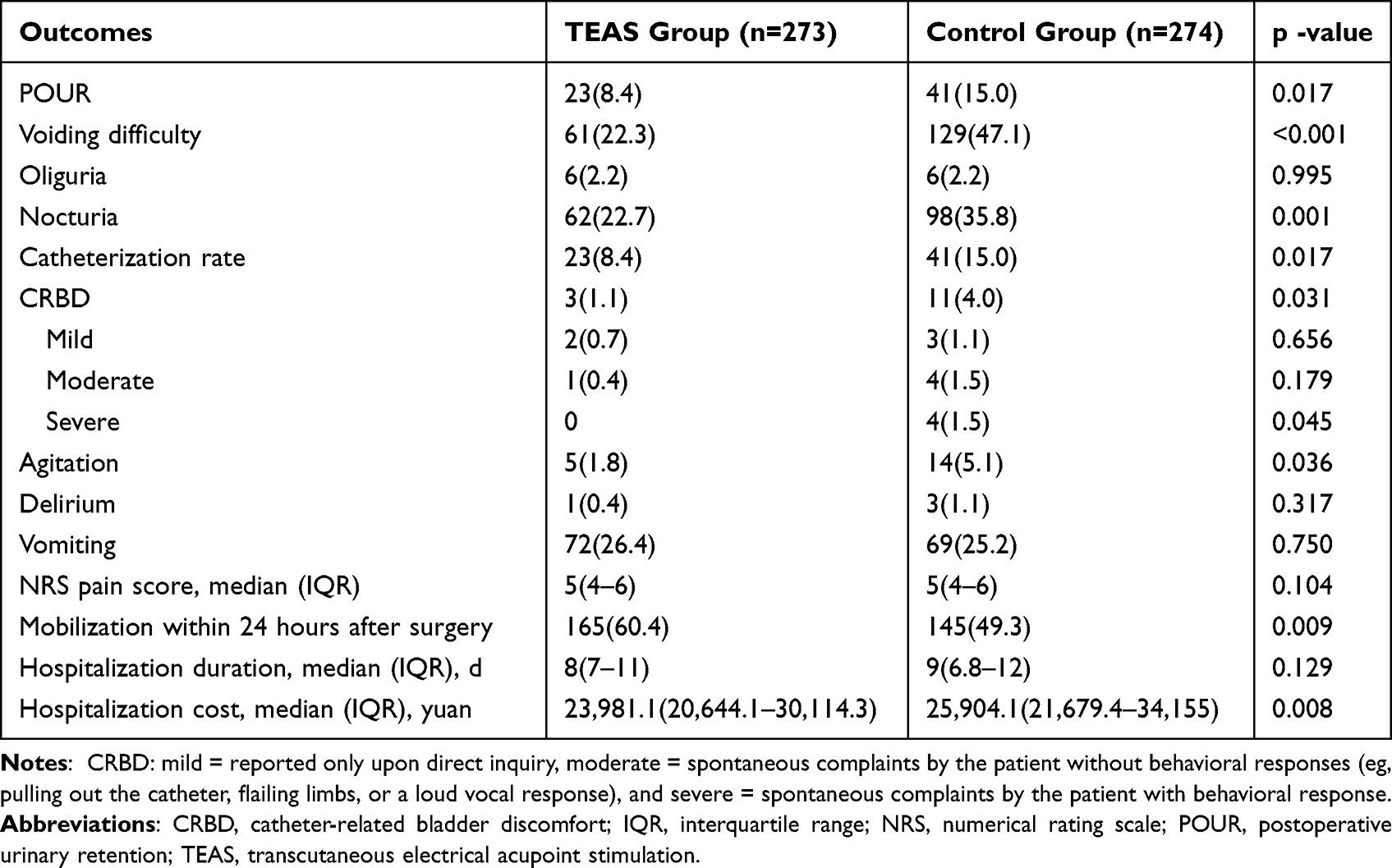 |
Table 2 Postoperative Voiding and Recovery Indicators |
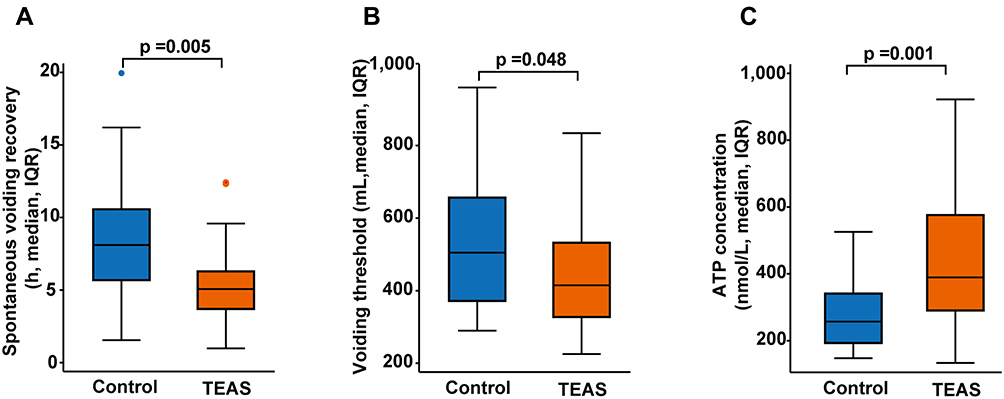 |
Figure 3 Postoperative spontaneous voiding recovery and urinary ATP. (A) spontaneous voiding recovery, (B) Voiding threshold, (C) ATP concentrations (n=30 in the TEAS group; n=30 in the control group). |
As compared with the control group, there were fewer patients in the TEAS group who experienced voiding difficulty (22.3% versus 47.1%, p <0.001) and nocturia (22.7% vs 35.8%, p =0.001). Postoperative catheterization was less common in the TEAS group (8.4% versus 15.0%, p =0.017) and CRBD was less prevalent (0.7% versus 3.3%, p =0.031) in comparison to the control group, and fewer patients in the TEAS group demonstrated agitated behavior including attempts to pull out the catheter, flailing limbs, or loud vocalizations (0 versus 1.5%, p =0.045). The TEAS group had lower hospitalization costs compared to the control group (23,981.1 yuan [IQR: 20,644.1–30,114.3 yuan] versus 25,904.1 yuan [IQR: 21,679.4–34,155 yuan], p =0.008). While no significant differences were observed between the two groups in terms of delirium (p =0.317), vomiting (p =0.750), or hospitalization duration (p =0.129).
During the study, six patients experienced adverse events, including four cases of gross hematuria or lower urinary tract infection and two cases of localized acupuncture point redness or pruritus, and no statistically significant difference was found between the TEAS and control groups in terms of the above adverse events (Table 3). There were no serious adverse events reported in either group. And all adverse events occurring during the trial were mild and resolved within a short period of time.
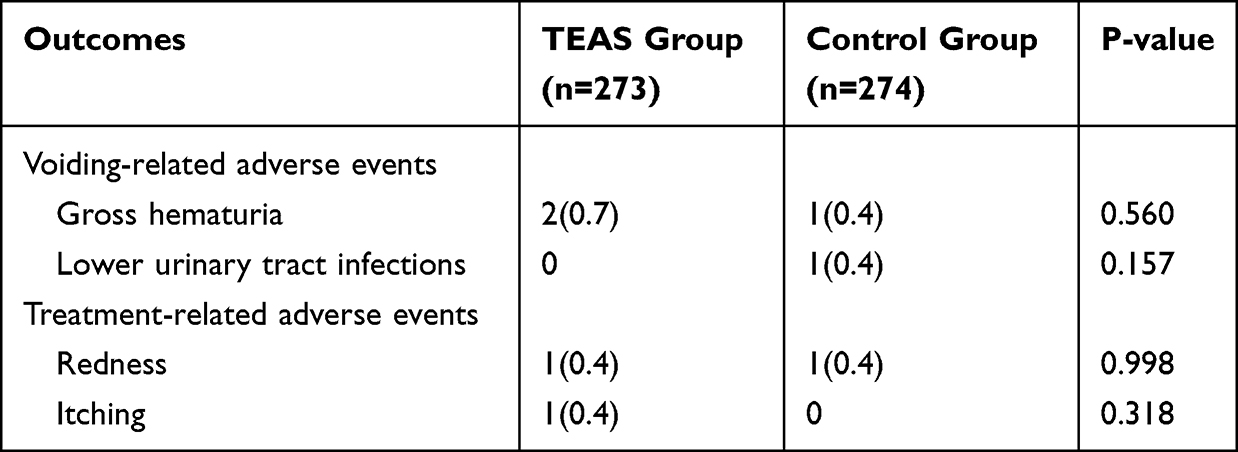 |
Table 3 Adverse Events |
Discussion
According to our findings, TEAS can reduce the incidence of urinary retention in elderly patients following laparoscopic surgery. This mechanism may be related to the improvement of spontaneous urination reflex recovery by increasing ATP release, which is consistent with the hypothesis we presented.
POUR is defined as the inability to void when the bladder is full, along with pain and discomfort in the lower abdomen.2 The incidence of POUR in the general surgical population varies widely. It is estimated to be 6–10% in laparoscopic cholecystectomy.18,19 In older patients, changes resulting from physiological aging, as well as comorbidities and multiple drug therapies, may result in lower urinary tract symptoms, such as urinary retention and incontinence. The risk of POUR increases with age, with patients over 60 years of age being at double the risk.20 In this population of elderly patients with poor mobility and cognitive impairment, combined with susceptibility to both infection and urinary bacterial overgrowth, a high rate of urinary tract infections is prevalent.21 According to a three-year surveillance study of 134,637 patients, urinary tract infections are the second most common healthcare-associated infections among the elderly, and catheter-associated urinary tract infections are more prevalent among the needy.22 In the present study, a significant reduction in the incidence of POUR after TEAS treatment was observed as compared to the baseline incidence of 15% in the elderly, which was consistent with previous research. Furthermore, no urinary tract infections occurred in patients treated with TEAS, indicating that TEAS has a protective effect on urinary tract susceptibility in older adults.
The storage and elimination of urine are essential aspects of daily life and involve intricate neural signaling pathways that require coordination between the urinary bladder and the urethra.23 It is necessary for both continence and micturition that the autonomic nerves and somatic nerves cooperate to control the bladder and urethra. During the storage phase of the micturition cycle, the sympathetic nervous system inhibits the contraction of the smooth muscle in the detrusor. As a result, the bladder is able to relax and expand. As the urinary bladder empties, ATP and acetylcholine act on smooth muscle P2X purinoceptor 1 (P2X1) and muscarinic receptors (M2 and M3) to mediate contractions. A switch from the filling phase to the emptying phase occurs when tension in the bladder stimulates stretch receptors (which are slowly adapting mechanoreceptors).24 Inhibition of the parasympathetic nerves that innervate the bladder is the mechanism by which anticholinergics, opioids, and anesthetics cause urinary retention.25,26 There are numerous signaling molecules secreted by the urinary epithelium (including acetylcholine, nitric oxide, neuropeptides, neurotrophins, and prostaglandins) which form the “uroepithelium-associated sensory network”, with ATP serving as the main messenger for the voiding reflex and pain.27 In experiments, administration of intravesical ATP increased afferent firing induced by bladder distension, decreased the voltage threshold for electrical stimulation, and increased the area of action potentials.28 In rats with bladder dysfunction caused by AUR, ATP-sensitive potassium channel openers prevent the need for catheterizations as a result of the dysfunctional bladder.29 The present study found elevated urinary ATP levels in TEAS of laparoscopic cholecystectomy patients, which may be associated with lower urinary retention rates.
An elderly person’s ability to adapt to environmental or intrinsic visceral stimuli is compromised due to significant changes in autonomic nervous system function as they age. There is evidence that the elderly has altered peripheral and central nervous system activity, as well as reduced neurotransmitter receptor function. As a result, bladder capacity is reduced and bladder volume sensation is lost.30 In order to increase sympathetic, parasympathetic, and central cholinergic activity, simple strategies can be implemented to enhance autonomic function and increase cortical blood flow. By inhibiting ATP release from the urothelium and attenuating bladder afferent nerve firing, OnabotulinumtoxinA is able to exert its clinical effects on urinary urgency in cases of overactive bladder syndrome.31 Alternatively, acupuncture-like stimulation of specific body areas causes an increase in bladder tone and a decrease in periurethral electromyogram activity when the bladder is full and contracting.32 This response is mediated through the pelvic efferent (parasympathetic) nerve that drives the bladder and depends on the state of the bladder’s filling.33 Adenosine A1 receptors and local anti-nociceptive effects of acupuncture have been shown in research to increase ATP concentration in the body, as well as adenosine levels.34 As a result of the present study, patients receiving TEAS treatment had higher urinary ATP levels and significantly faster recovery from voluntary voiding after surgery. Thus, increasing urinary ATP levels are related to the regulation of TEAS during urination.
This study has several limitations. First, we evaluated only the incidence of urinary retention following laparoscopic cholecystectomy and short-term after catheter removal, without long-term follow-up of voiding relief and functional outcomes. Second, despite the careful blinding procedure, there may be a potential placebo effect. Third, this study demonstrated that people with elevated ATP concentrations had a reduced bladder voiding threshold, although the specific mechanism remains to be determined.
Conclusion
TEAS can reduce the incidence of POUR and increase ATP release in elderly patients who have undergone laparoscopic cholecystectomy. Future studies should examine specific mechanisms by which ATP participates in TEAS to reduce bladder dysfunction caused by urinary retention.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study will be available upon reasonable request from the corresponding author. Email: [email protected].
Ethical Approval
The study was approved by Tianjin Nankai Hospital Ethics Committee (ethical register number: NKYY_YX_IRB_2017_032_01). Trial Registration: NCT03631160.
Acknowledgments
The authors would like to thank the medical and nursing staff at Tianjin Nankai Hospital as well as all patients who participated in the trial. Both of these individuals did not receive any compensation for their contributions.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Keita H, Diouf E, Tubach F, et al. Predictive factors of early postoperative urinary retention in the postanesthesia care unit. Anesth Analg. 2005;101(2):592–596. doi:10.1213/01.ANE.0000159165.90094.40
2. Baldini G, Bagry H, Aprikian A, Carli F, Warner D, Warner M. Postoperative urinary retention: anesthetic and perioperative considerations. Anesthesiology. 2009;110(5):1139–1157. doi:10.1097/ALN.0b013e31819f7aea
3. Serlin DC, Heidelbaugh JJ, Stoffel JT. Urinary retention in adults: evaluation and initial management. Am Fam Physician. 2018;98(8):496–503.
4. Heid F, Kauff DW, Lang H, Kneist W. Impact of inhalation vs. intravenous anaesthesia on autonomic nerves and internal anal sphincter tone. Acta Anaesthesiol Scand. 2015;59(9):1119–1125. doi:10.1111/aas.12535
5. McGrane S, Atria NP, Barwise JA. Perioperative implications of the patient with autonomic dysfunction. Curr Opin Anaesthesiol. 2014;27(3):365–370. doi:10.1097/ACO.0000000000000072
6. Lee UJ, Ward JB, Feinstein L, et al. National trends in neuromodulation for urinary incontinence among insured adult women and men, 2004–2013: the urologic diseases in America project. Urology. 2021;150:86–91. doi:10.1016/j.urology.2020.11.043
7. Yang PS, Chen CL, Hou CP, Lin YH, Tsui KH. An open-label, prospective interventional study of the tolerability and efficacy of 0.4 mg oral tamsulosin oral controlled absorption system in men with lower urinary tract symptoms associated with benign prostatic hyperplasia who are unsatisfied with treatment with 0.2 mg tamsulosin. Clin Interv Aging. 2018;13:235–242. doi:10.2147/CIA.S152701
8. Burnstock G. Physiology and pathophysiology of purinergic neurotransmission. Physiol Rev. 2007;87(2):659–797. doi:10.1152/physrev.00043.2006
9. Lauterbach R, Ferrer Sokolovski C, Rozenberg J, Weissman A. Acupuncture for the treatment of post-partum urinary retention. Eur J Obstet Gynecol Reprod Biol. 2018;223:35–38. doi:10.1016/j.ejogrb.2018.01.029
10. Gao Y, Zhou X, Dong X, Jia Q, Xie S, Pang R. Electroacupuncture for bladder function recovery in patients undergoing spinal anesthesia. Evid Based Complement Alternat Med. 2014;2014:892619. doi:10.1155/2014/892619
11. Bian XM, Lv L, Lin WB, Liang HH, Zhang Y, Wang LC. Moxibustion therapy at CV4 prevents postoperative dysuria after procedure for prolapse and hemorrhoids. Evid Based Complement Alternat Med. 2013;2013:756095. doi:10.1155/2013/756095
12. Yang L, Wang Y, Mo Q, Liu Z. A comparative study of electroacupuncture at Zhongliao (BL33) and other acupoints for overactive bladder symptoms. Front Med. 2017;11(1):129–136. doi:10.1007/s11684-016-0491-6
13. Chen WY, Li ZC, Xi SP, Zhang LX. 经皮穴位电刺激对接受硬膜外分娩镇痛的产妇发热的影响 [Effect of transcutaneous electrical acupoint stimulation on epidural-related maternal fever in parturients undergoing epidural labor analgesia]. Zhen Ci Yan Jiu. 2021;46(7):586–591. Chinese. doi:10.13702/j.1000-0607.200616
14. Yang XY, Xiao J, Chen YH, et al. Dexamethasone alone vs in combination with transcutaneous electrical acupoint stimulation or tropisetron for prevention of postoperative nausea and vomiting in gynaecological patients undergoing laparoscopic surgery. Br J Anaesth. 2015;115(6):883–889. doi:10.1093/bja/aev352
15. In CB, Lee SJ, Sung TY, Cho CK, Jee YS. Effects of chlorpheniramine maleate on catheter-related bladder discomfort in patients undergoing ureteroscopic stone removal: a randomized double-blind study. Int J Med Sci. 2021;18(4):1075–1081. doi:10.7150/ijms.53043
16. Gao F, Zhang Q, Li Y, et al. Transcutaneous electrical acupoint stimulation for prevention of postoperative delirium in geriatric patients with silent lacunar infarction: a preliminary study. Clin Interv Aging. 2018;13:2127–2134. doi:10.2147/CIA.S183698
17. Ni CY, Wang ZH, Huang ZP, et al. Early enforced mobilization after liver resection: a prospective randomized controlled trial. Int J Surg. 2018;54(Pt A):254–258. doi:10.1016/j.ijsu.2018.04.060
18. Donmez T, Erdem VM, Uzman S, et al. Laparoscopic cholecystectomy under spinal-epidural anesthesia vs. general anaesthesia: a prospective randomised study. Ann Surg Treat Res. 2017;92(3):136–142. doi:10.4174/astr.2017.92.3.136
19. Han J, Oh AY, Jeon YT, et al. Quality of recovery after laparoscopic cholecystectomy following neuromuscular blockade reversal with neostigmine or sugammadex: a prospective, randomized, controlled trial. J Clin Med. 2021;10(5):938. doi:10.3390/jcm10050938
20. Kowalik U, Plante MK. Urinary retention in surgical patients. Surg Clin North Am. 2016;96(3):453–467. doi:10.1016/j.suc.2016.02.004
21. Rowe TA, Juthani-Mehta M. Diagnosis and management of urinary tract infection in older adults. Infect Dis Clin North Am. 2014;28(1):75–89. doi:10.1016/j.idc.2013.10.004
22. Zhao X, Wang L, Wei N, et al. Epidemiological and clinical characteristics of healthcare-associated infection in elderly patients in a large Chinese tertiary hospital: a 3-year surveillance study. BMC Infect Dis. 2020;20(1):121. doi:10.1186/s12879-020-4840-3
23. Andersson KE, Arner A. Urinary bladder contraction and relaxation: physiology and pathophysiology. Physiol Rev. 2004;84(3):935–986. doi:10.1152/physrev.00038.2003
24. Hokanson JA, Langdale CL, Sridhar A, Milliken P, Grill WM. State-dependent bioelectronic interface to control bladder function. Sci Rep. 2021;11(1):314. doi:10.1038/s41598-020-79493-7
25. Reiter PD, Clevenger AC. Nalbuphine reduces opioid-associated urinary retention in pediatric patients. Pediatr Crit Care Med. 2019;20(5):e240–e244. doi:10.1097/PCC.0000000000001920
26. Verhamme KM, Sturkenboom MC, Stricker BH, Bosch R. Drug-induced urinary retention: incidence, management and prevention. Drug Saf. 2008;31(5):373–388. doi:10.2165/00002018-200831050-00002
27. Merrill L, Gonzalez EJ, Girard BM, Vizzard MA. Receptors, channels, and signalling in the urothelial sensory system in the bladder. Nat Rev Urol. 2016;13(4):193–204. doi:10.1038/nrurol.2016.13
28. Yu Y, de Groat WC. Sensitization of pelvic afferent nerves in the in vitro rat urinary bladder-pelvic nerve preparation by purinergic agonists and cyclophosphamide pretreatment. Am J Physiol Renal Physiol. 2008;294(5):F1146–F1156. doi:10.1152/ajprenal.00592.2007
29. Ohmasa F, Saito M, Oiwa H, et al. Pharmacological preconditioning of ATP-sensitive potassium channel openers on acute urinary retention-induced bladder dysfunction in the rat. BJU Int. 2012;110(6Pt B):E245–E252. doi:10.1111/j.1464-410X.2012.10965.x
30. Pfisterer MH, Griffiths DJ, Schaefer W, Resnick NM. The effect of age on lower urinary tract function: a study in women. J Am Geriatr Soc. 2006;54(3):405–412. doi:10.1111/j.1532-5415.2005.00613.x
31. Collins VM, Daly DM, Liaskos M, et al. OnabotulinumtoxinA significantly attenuates bladder afferent nerve firing and inhibits ATP release from the urothelium. BJU Int. 2013;112(7):1018–1026. doi:10.1111/bju.12266
32. Wang JH, Chen BG, Yin J, Wang G, Zou WG, Luo XJ. 不同穴位电针对脊髓损伤所致尿潴留大鼠逼尿肌兴奋性及BDNF和TrkB表达的影响 [Effect of electroacupuncture of different acupoints on the excitability of detrusor muscle and the expression of BDNF and TrkB in the spinal cord of rats with urinary retention due to spinal cord injury]. Zhen Ci Yan Jiu. 2009;34(6):387–392. Chinese.
33. Tanaka Y, Koyama Y, Jodo E, et al. Effects of acupuncture to the sacral segment on the bladder activity and electroencephalogram. Psychiatry Clin Neurosci. 2002;56(3):249–250. doi:10.1046/j.1440-1819.2002.00976.x
34. Goldman N, Chen M, Fujita T, et al. Adenosine A1 receptors mediate local anti-nociceptive effects of acupuncture. Nat Neurosci. 2010;13(7):883–888. doi:10.1038/nn.2562
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effects of Transcutaneous Electrical Acupoint Stimulation on Recovery After Gynecological Laparoscopic Surgery: A Randomized, Single-Blind, Controlled Trial
Zheng J, Zhou H, Diao Y, Song P, Yi Z, Guo X, Li L
Journal of Pain Research 2025, 18:6449-6462
Published Date: 3 December 2025