Back to Journals » Journal of Pain Research » Volume 18
The Effect of Transcutaneous Electrical Acupuncture Stimulation on Postoperative Pain Control and Mobility in Patients Undergoing Percutaneous Endoscopic Lumbar Discectomy: Study Protocol for a Prospective Randomized Trial
Authors Hu CF, Meng FX, Luo X ![]() , Chen BY
, Chen BY
Received 6 August 2025
Accepted for publication 18 November 2025
Published 26 November 2025 Volume 2025:18 Pages 6345—6357
DOI https://doi.org/10.2147/JPR.S554528
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jinlei Li
Chen-Fu Hu,1 Fan-Xing Meng,1 Xin Luo,2,* Bing-Yao Chen1,*
1Department of Orthopedics, Beijing Daxing District People’s Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Department of Anesthesiology, Beijing Friendship Hospital, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xin Luo, Department of Anesthesiology, Beijing Friendship Hospital, Capital Medical University, Beijing, People’s Republic of China, Email [email protected] Bing-Yao Chen, Department of Orthopedics, Beijing Daxing District People’s Hospital, Capital Medical University, Beijing, People’s Republic of China, Email [email protected]
Purpose: Optimal perioperative analgesia and early ambulation are critical protocols of enhanced recovery after surgery (ERAS), which significantly impact patients’ clinical outcomes in spine surgery. Transcutaneous electrical acupoint stimulation (TEAS), a well-integrated technique combining the meridian-based protocols of conventional needle acupuncture with noninvasive modern electrotherapy, has been widely used to enhance perioperative recovery. Although several studies have confirmed the safety and feasibility of TEAS in various spinal procedures, clinical evidence supporting its application in percutaneous endoscopic lumbar discectomy (PELD) remains limited, prompting surgeons to evaluate its role within spine ERAS protocols. We hypothesized that, compared with placebo acupuncture, TEAS would provide superior pain relief and reduce analgesic requirements during the perioperative period, thereby decreasing opioid-related side effects, facilitating earlier ambulation, and improving short-term postoperative recovery quality after PELD.
Methods: This prospective, single-blind, randomized controlled clinical trial will enroll 86 patients scheduled to undergo PELD. Participants will be randomly assigned (1:1) to an active TEAS group (Group A) or a placebo TEAS group (Group P). In Group A, TEAS is applied bilaterally at Neiguan (PC6), Chengshan (BL57), Sanyinjiao (SP6), and Dachangshu (BL25) using alternating frequencies of 2/100 Hz and intensity ranging from 10 to 15 mA, adjusted to each patient’s maximum tolerable level. In Group P, electrodes are placed bilaterally at four non-acupoint sites (located 7 cun and 9 cun above and 1 cun outside HT7, and at 9 cun and 12 cun above BL60) and connected to the stimulator without activating electrical output, maintaining participant blinding. The treatment period includes 30 minutes prior to surgery, continuous stimulation throughout the procedure on the surgery day, and 30-minute interventions each morning on postoperative days 1 and 2 followed by 6 months of follow-up. The primary endpoint is time to postoperative ambulation. Secondary outcomes include pain-related indicators, scores on the 15-item Quality of Recovery scale (QoR-15), gastrointestinal function restoration, adverse events, patient satisfaction, and exploratory assessment of spinal function recovery indicators.
Discussion: TEAS offers an alternative for optimal perioperative pain management and promotion of early ambulation, congruent with alleviated ERAS protocols for endoscopic spine surgery.
Conclusion: This study aims to verify whether TEAS will benefit future patients and contribute to meaningful improvements in ERAS-based perioperative management for micro-spine surgery, ultimately supporting the establishment of a standardized PELD day-surgery model.
Trial Registration: The International Traditional Medicine Clinical Trial Registry (http://itmctr.ccebtcm.org.cn/); registered on April 17, 2025. Trial Registration Number: ITMCTR2025000779.
Plain Language Summary: Lumbar spine conditions like herniated discs and spinal narrowing are becoming more common, especially in middle-aged and older adults. These conditions often cause pain and limit mobility. Surgeons increasingly use a minimally invasive procedure called percutaneous endoscopic lumbar discectomy (PELD) to treat these problems. PELD allows for faster recovery, less tissue damage, and shorter hospital stays.
In this study, our research team explored whether a noninvasive therapy called transcutaneous electrical acupoint stimulation (TEAS) could influence postoperative recovery after PELD. TEAS works by sending mild electrical pulses to specific points on the skin, similar to acupuncture but without needles. Previous studies have shown that TEAS may have possible benefits in reducing perioperative adverse events.
We plan to enroll 86 patients undergoing PELD and randomly assign them to receive either real TEAS or a placebo version. Both groups will receive standard anesthesia and pain management. The study will assess postoperative recovery by measuring the time to first ambulation, pain levels, and the need for additional pain medications. The findings of this trial may provide clinical evidence on the feasibility and potential role of TEAS within perioperative ERAS management for PELD.
Keywords: percutaneous endoscopic lumbar discectomy, transcutaneous electrical acupoint stimulation, early ambulation time, perioperative pain, postoperative recovery
Introduction
Percutaneous endoscopic lumbar discectomy (PELD) is a well-established endoscopic surgical technique for treating lumbar degenerative lesions, offering the advantages of minimal invasiveness, reduced tissue trauma, decreased blood loss, and shorter hospitalization.1,2 Currently, with its growing prevalence and continued advancement, PELD has become a well-established surgical technique in China, with increasing annual case volumes. PELD is commonly performed as outpatient or short-stay procedures to optimize hospital resource utilization, promote patients’ post-hospitalization functional recovery, and facilitate early return to regular daily living across multiple health centers.3,4 Consequently, the implementation of modified enhanced recovery after surgery (ERAS) protocols aimed at promoting early postoperative movement, shortening hospital stays, and facilitating patients’ timely discharge has gained increasing attention from healthcare teams.5–7
Early ambulation, particularly same-day positive-mobilization, is an integral component of postoperative ERAS protocols and has been proven to produce favorable clinical outcomes and reduce hospital stays, aligning closely with the primary objectives of short-stay surgery.8–10 To minimize the adverse effects of perioperative pain on early ambulation and other recovery outcomes, ERAS protocols incorporate multimodal analgesic regimens that include potent, rapid-acting agents such as opioids, non-opioids, and adjuvants, which are typically prescribed to ensure satisfactory intraoperative and postoperative analgesia.11,12 However, these analgesics are associated with a high incidence of dose-dependent side effects,13 including over-sedation, postoperative nausea and vomiting (PONV), cardiovascular complications, respiratory depression, urinary retention, infection, opioid-induced hyperalgesia, and even chronic postoperative pain (CPSP).14 These adverse effects may not only delay initial ambulation and directly hinder postoperative rehabilitation but also negatively impact patients’ hospitalization and long-term outpatient outcomes.15,16 Reports indicate that 8.1–27.6% of patients experience CPSP after minimally invasive spine surgery (MISS), which is considered a surgical failure and impairs patients’ physical function, often necessitating additional outpatient treatments or hospital readmission.17,18 Overall, an urgent need exists to identify more effective, feasible, and safe non-pharmacologic interventions that can shorten time to ambulation and optimize short-stay PELD surgical protocols.
Transcutaneous electrical acupoint stimulation (TEAS), a noninvasive alternative to conventional acupuncture, has been proposed as a preventive and adjuvant therapy to reduce perioperative complications and enhance patients’ postoperative physical recovery.19 Numerous clinical studies have demonstrated that TEAS possesses definite auxiliary analgesia for managing acute perioperative pain20–22 and may also have therapeutic potential in reducing CPSP following general surgery.23,24 Furthermore, TEAS has been associated with reduced postoperative pain intensity and a lower incidence of postoperative nausea and vomiting (PONV)25 and may lower the risk of postoperative cognitive dysfunction (POCD) in lumbar spine surgery,26 thereby contributing to accelerated safe discharge. Nevertheless, high-quality clinical evidence demonstrating that perioperative utilization of TEAS specifically reduces postoperative adverse events and promotes early rehabilitation after PELD remains lacking. Therefore, we designed this prospective, randomized, single-blind study to validate that TEAS, compared with non-acupoint stimulation, can provide adjunctive analgesic effects and enhance rapid movement in patients undergoing PELD post-surgery.
Methods and Analysis
Trial Design
This exploratory, prospective, single-blind, randomized controlled clinical trial will enroll patients scheduled to undergo PELD and randomly assign them in a 1:1 ratio to either the active TEAS group or the placebo TEAS group. This study will be conducted at Beijing Daxing District People’s Hospital of China, affiliated with Capital Medical University, following approval from the hospital’s ethics committee (Approval No: 20240719-1-15) and registration in the International Traditional Medicine Clinical Trial Registry (Trial Registry Number: ITMCTR2025000779). The study began on May 7, 2025, and will last for 12 months. Figure 1 illustrates the flowchart of the study progress.
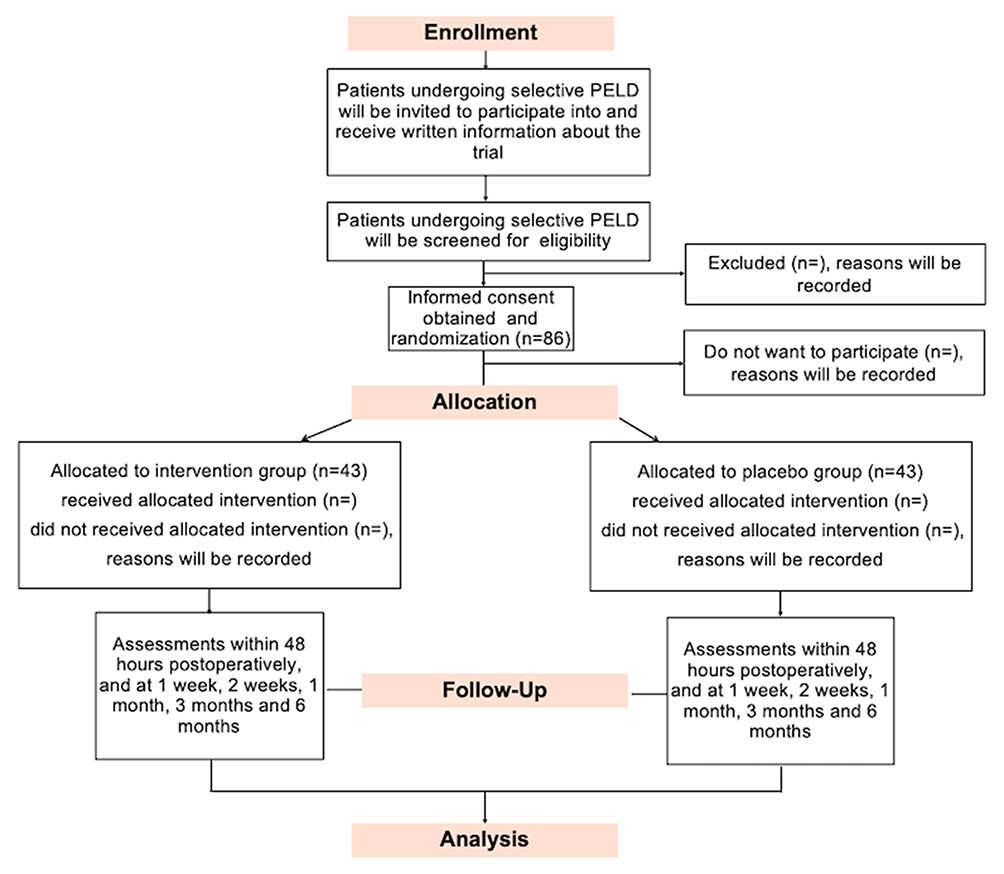 |
Figure 1 Flow chart of participant enrollment of TEAS and Control groups. Abbreviation: PELD, Percutaneous endoscopic lumbar discectomy. |
Study Participants and Recruitment
A total of 86 patients undergoing selective PELD at Beijing Daxing District People’s Hospital will be randomly assigned into two groups: the active TEAS group (Group A, n = 43) and the placebo TEAS group (Group P, n = 43). Eligible patients will be consecutively screened for enrolment according to predefined inclusion and exclusion criteria. All participants will provide written informed consent before enrolment. Participants may withdraw at any time because of unwillingness to provide detailed data, loss to follow-up, or withdrawal permitted by the investigators.
Inclusion criteria: (1) Aged 18–75 years, diagnosed with lumbar disc herniation (LDH) or lumbar spinal stenosis (LSS), and scheduled for PELD regardless of sex; (2) Body mass index (BMI) between 18 and 30 kg/m2 (BMI = weight in kilograms/height in meters squared); (3) American Society of Anesthesiologists (ASA) physical status classification I–III; and (4) Ability and willingness to provide informed consent and participate in the study.
Exclusion criteria: (1) Scarring or surgical incisions at acupoint meridians Neiguan (PC6), Chengshan (BL57), Sanyinjiao (SP6), and Dachangshu (BL25), or sham acupoints near Kunlun (BL60) and Shenmen (HT7); (2) Patients with skin infection above specified acupuncture points; (3) Nerve injuries affecting patients’ upper or lower limbs; (4) Participation in another clinical study within the past 4 weeks; (5) Inability to evaluate both the visual analog scale (VAS) score and the numeric rating scale (NRS) score; (6) Previous pacemaker placement; (7) Pregnancy or positive pregnancy test; (8) Use of central analgesics and opioid addiction; (9) Comorbidities before surgery, including severe mental disorders or neurological conditions; and (10) Any condition considered unsuitable for this study.
Withdrawal criteria: (1) Voluntary withdrawal from the trial; (2) Rejection of any standardized drug treatment throughout the surgery; (3) Occurrence of severe adverse events during the trial; (4) Lesions exceeding expectations intraoperatively and necessitating conversion to open surgery; and (5) Surgical duration exceeding 4 h.
Randomization and Blinding
General data will be collected until the end of the follow-up period (Table 1). Before trial initiation, a statistician generated a random allocation sequence based on the sample size using a random number generator. The study subject serial numbers are placed in separate sealed envelopes by an anesthesia nurse who remains blinded to the assignments and is excluded from trial implementation. Once eligible patients are enrolled, the nurse draws a well-prepared envelope for perioperative acupoint stimulation and delivers it to the acupuncturists. Patients are randomly assigned to Group A or Group P according to the randomization code concealed in the envelope. Acupuncturists, who are aware of the group assignments, will administer acupuncture from preoperative 30 min to the postoperative day 2. In this single-blind trial, the anesthesiologists responsible for anesthesia management and intraoperative data collection are unblinded. The surgeons and anesthesiologists are not involved in outcome assessment. The patients, postoperative follow-up assessors, and statisticians remain blinded to exact grouping status and are excluded from all intervention-related clinical procedures.
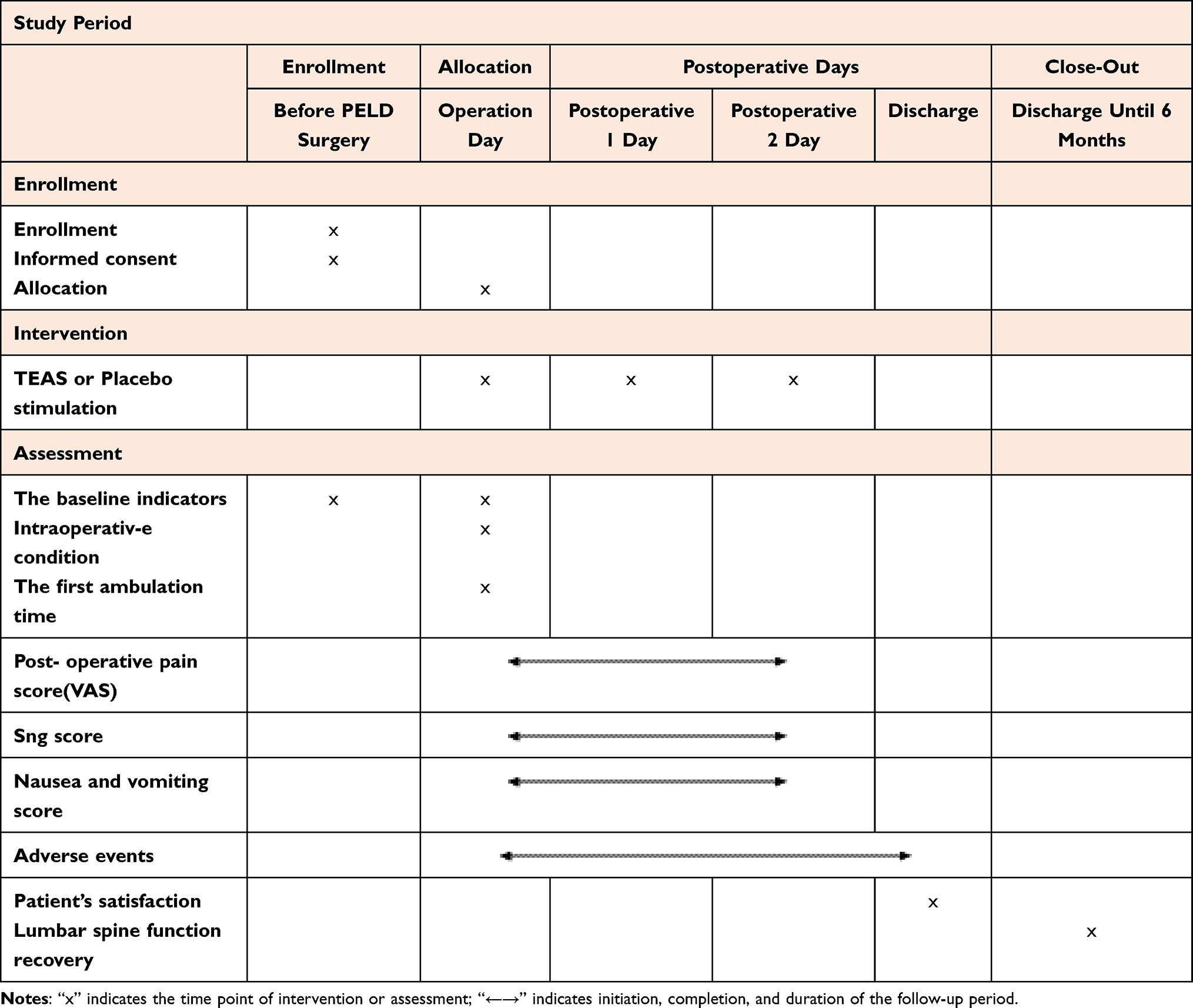 |
Table 1 Recommendations for Interventional Trials Schedule for Enrollment, Interventions, and Assessments |
Intervention
All participants will receive standardized perioperative ERAS management, anesthesia regimens, and procedures after being assigned to one of the following research groups:
Group A: Patients in the active TEAS group will receive stimulation at four bilateral acupoints (PC6, BL57, SP6, and BL25 as shown in Figure 2). PC6, which belongs to the sixth acupoint of the pericardium meridian, is located on the forearm’s palmar side, two cun from the wrist, between the tendons of the palmaris longus and the radial flexor carpi. BL57, situated on the foot taiyang bladder meridian, corresponds to the muscle-tendon junction of the lower medial gastrocnemius muscle belly. SP6 is positioned 3 cun superior to the prominence of the medial malleolus, posterior to the tibia. BL25 is situated on the lateral 1.5 cun below the spinous process of the fourth lumbar vertebra. PC6 offers significant antiemetic effects via vagal modulation, and together with SP6 regulates visceral and somatic pain pathways. BL57 and BL25 are associated with meridians of the lower back and lower limbs. Before treatment, the skin is routinely disinfected, and symmetric bilateral pairs of electrode patches will be attached to the above corresponding acupoints. Treatment will commence at a frequency of 2/100 Hz (disperse-dense wave alternating every 3 s), produced by Han’s acupoint nerve stimulator (HANS-200A, Nanjing Jisheng Medical Technology Co., Ltd., China), with a stimulation intensity ranging from 10 to 15 mA, titrated to each patient’s maximum tolerable threshold. Bilateral PC6, BL57 and SP6 will receive continuous stimulation from 30 minutes before surgery until surgery completion, which can not only activate endogenous analgesic pathways but also provide continuous analgesic input and stabilize hemodynamic responses during surgical stimulation and 30-min stimulations each morning between 9:00 and 11:00 a.m. on postoperative days 1 and 2. Each 30-minute intervention represents an effective therapeutic phase of TEAS, sufficient to induce and maintain therapeutic and neuro-modulatory effects. Due to intraoperative positioning constraints, BL25 will receive similar 30-min stimulations prior to surgery and on the mornings of postoperative days 1 and 2, but not during the surgery.
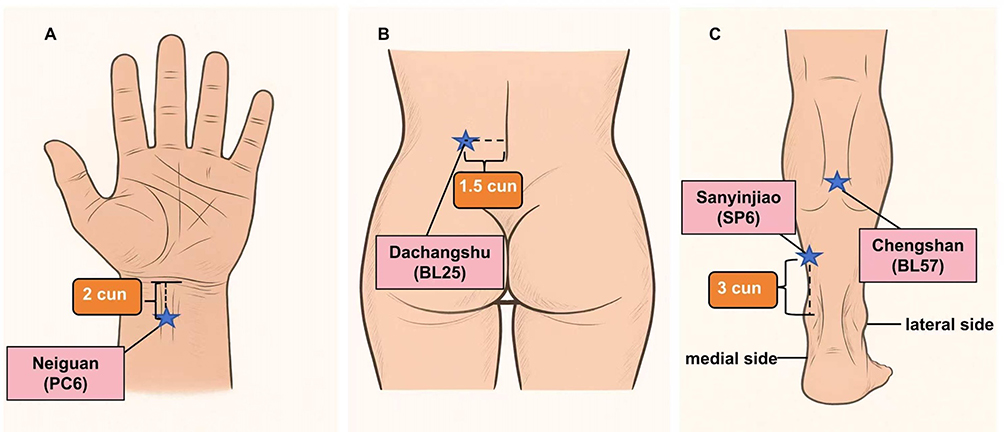 |
Figure 2 Anatomical locations of acupoints used for TEAS intervention. (A) Neiguan (PC6) is located on the palmar side of the forearm, 2 cun proximal to the transverse wrist crease, between the tendons of the palmaris longus and flexor carpi radialis. (B) Dachangshu (BL25) lies 1.5 cun lateral to the lower border of the spinous process of the fourth lumbar vertebra (L4). (C) Sanyinjiao (SP6) is situated 3 cun superior to the medial malleolus, posterior to the tibial border, and Chengshan (BL57) is positioned at the midpoint of the line connecting the popliteal crease and the heel, in the depression between the gastrocnemius heads. Notes: “Cun” is a traditional Chinese proportional unit of length used to locate acupoints, defined as the width of the patient’s thumb at the interphalangeal joint. |
Group P: In the placebo TEAS group, patients will be informed of possible electrical stimulation during the procedure and have electrode patches applied to four placebo points: (1) 7 cun and (2) 9 cun proximal to a point located 1 cun radial to HT7 (Shenmen), measured along the forearm from the palmar wrist crease; and (3) 9 cun and (4) 12 cun proximal to BL60 (Kunlun), measured vertically upward from the highest point of the lateral malleolus and located on the line connecting BL60 (Kunlun) and the popliteal fossa (as shown in Figure 3). However, the electrode patches are connected to the HANS acupoint nerve stimulator in full view of the patient, and no electrical stimulation will be administered thereby simulating the intervention without physiological effects. The intervention period for Group P also includes 30 min before surgery and continues until surgery completion, followed by 30-min interventions each morning on postoperative days 1 and 2. The intervention protocols for the two groups are illustrated in Figure 4.
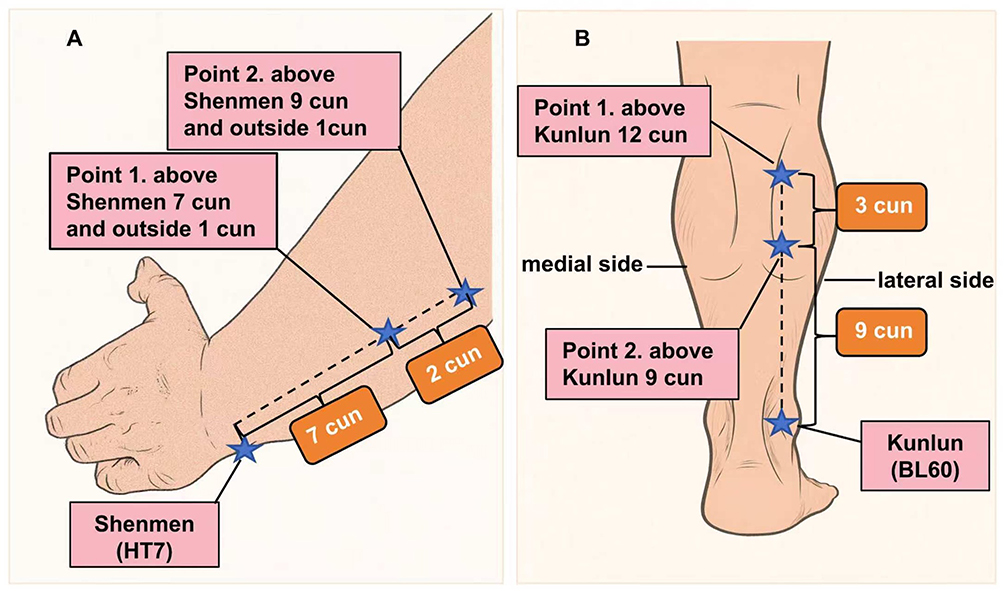 |
Figure 3 Surface localization of non-Meridian and non-acupoint sites used for sham TEAS stimulation. (A) Point 1 was located 7 cun proximal and 1 cun radial to Shenmen (HT7); Point 2 was 9 cun proximal and 1 cun radial to HT7, both measured along the anterior forearm from the palmar wrist crease. (B) Point 1 was positioned 12 cun superior to Kunlun (BL60); Point 2 was 9 cun superior to BL60. Both points were aligned vertically along the posterolateral aspect of the lower leg, referencing the line between BL60 and the popliteal fossa. Notes: “Cun” is a traditional Chinese proportional unit of length used to locate acupoints, defined as the width of the patient’s thumb at the interphalangeal joint. |
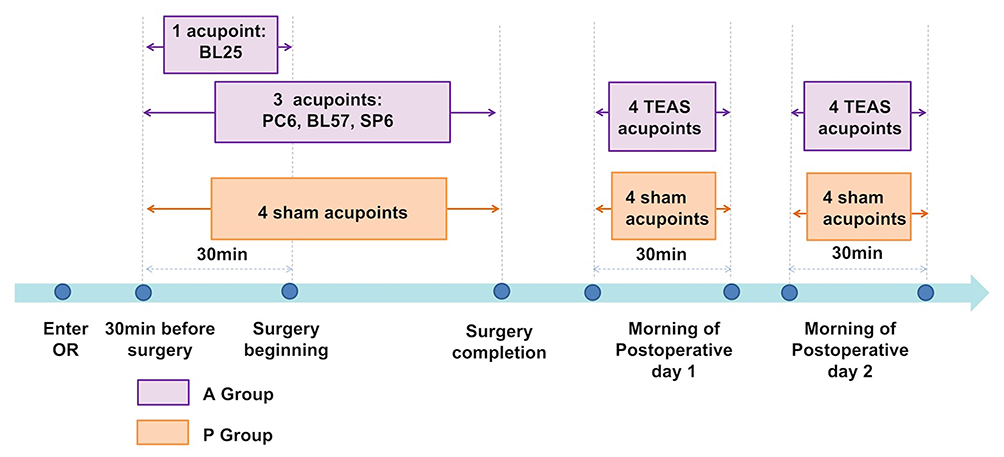 |
Figure 4 Perioperative intervention schedule for TEAS and sham stimulation. Abbreviation: OR, operating room. |
Standard Perioperative ERAS Management, Anesthesia Regimens, and Procedure
Preoperative period: After admission to the hospital, patients are informed about the surgical process and recovery expectations. Nutritional status of the patients is also assessed and optimized to foster effective postoperative healing. Two hours before surgery, 100 mg of celecoxib and 75 mg of pregabalin are administered orally. Patients’ preoperative fasting time is limited to 6 h for solids and 2 h for clear liquids. Upon arrival in the operating room, all patients are informed about the active TEAS or placebo intervention to reaffirm their voluntary participation. Standard monitoring, including heart rate (HR), electrocardiogram (ECG), pulse oxygen saturation (SpO2), and noninvasive blood pressure (NIBP), is applied. Acupuncturists will execute the corresponding stimulation in the different groups starting 30 min before PELD surgery and continue until the procedure’s completion.
Intraoperative period: All PELD procedures will be performed under local anesthesia (mixture of 10 mL 1% ropivacaine, 15 mL 2% lidocaine, and 20 mL saline injected with 18-G needles), combined with conscious sedation using intravenous sufentanil (5 µg) administered by anesthesiologists. Additionally, patients will receive repeated single doses of 5 µg sufentanil if severe intraoperative pain (VAS scores ≥ 4) recurs. After marking the puncture point with the C‐arm, skin preparation and draping will be performed, followed by the insertion of the puncture needle to the target position and placement of the working cannula. The endoscopic surgical system will be placed in the final position, reconfirmed using the C-arm. Under endoscopic visualization, nucleus pulposus removal, nerve root and dural sac exploration, and nerve root decompression will be conducted. Upon completion of these core steps, betamethasone (4 mg) will be administered to the local nerves, and incisions will be closed with surgical sutures, marking the end of the entire procedure. Before leaving the operating room, patients will receive flurbiprofen axetil (50 mg) and tropisetron hydrochloride (5 mg) to reduce postoperative pain and PONV.
Postoperative period: Patients are encouraged to move (including standing and walking) within 6 h postoperatively while wearing a lumbar support brace. On the first and second postoperative days, patients will receive 30 min of TEAS stimulation according to group assignment. On the second postoperative day, patients are instructed to wear the lumbar support brace and perform ambulation exercises. For acute postoperative pain management, morphine (1 mg) will be administered as a single dose, with repeated dosing provided if patients report postoperative pain or if VAS scores ≥4 occur during the 2-day follow-up period.
Outcome Measures
All clinical data and outcomes will be collected and recorded by a blinded medical monitor from the Data Monitoring Committee (DMC).
Primary Outcome Measure
The primary outcome is the time to first ambulation, defined as the ability to stand and walk independently after PELD.9
Secondary Outcomes Measures
- Preoperative indicators: General demographic data, comorbidities, and baseline Quality of Recovery-15 (QoR-15) score.
- Intraoperative indicators: HR, blood pressure, instability of hemodynamic parameters and vasoactive drug dosage, frequency of moderate-to-severe intraoperative pain and analgesic requirements, surgery duration, surgical complications, and related treatments.
- Postoperative indicators: QoR-15 score at ambulation and 24 h post-surgery, Sng27 and VAS scores at 1, 4, 6, 18, 24, and 48 h postoperatively, postoperative analgesic consumption, appetite recovery time, anesthesia- and surgery-related adverse events, patient satisfaction at 48 h post-surgery, and Oswestry disability index (ODI) and Japanese Orthopedic Association (JOA) scores at postoperative weeks 1 and 2, and months 1, 3, and 6.
Safety Monitoring
Although the noninvasive characteristics of TEAS ensure patient safety, anesthesia- or surgery-related adverse events may still occur and will require appropriate treatment from physicians. Adverse events (AEs) will be monitored and documented throughout the perioperative period. TEAS-associated AEs may include localized skin reactions (such as erythema, pruritus, or rash), discomfort at the stimulation sites, or hypersensitivity to the electrode materials. Hemodynamic instability is characterized by any of the following: hypotension, defined as a mean arterial pressure (MAP) below 65 mmHg persisting for more than 3 minutes; hypertension, indicated by a systolic blood pressure exceeding 180 mmHg or diastolic pressure over 100 mmHg; bradycardia, with a heart rate under 50 bpm; or tachycardia, with a heart rate above 100 bpm. These conditions will be managed using intravenous fluid administration and vasoactive agents. Oxygen desaturation, defined as a drop in SpO2 below 90% lasting at least 10 seconds, will be managed through airway repositioning or supplemental oxygen. Additional postoperative events such as nausea, vomiting, or surgery-related complications (including hemorrhage, wound infection, or nerve injury) will also be recorded. Once any adverse event occurs, the investigator will promptly assess its severity, followed by proper treatment and documentation. Patients will be constantly monitored and managed until clinical safety is ensured.
Statistical Analysis and Sample Size Calculation
All detailed data will be promptly collected using paper case report forms (CRFs) by trained data collectors and systematically organized by statisticians. Statistical analyses will be performed using SPSS version 22.0 (IBM Corp., Armonk, NY, USA). The Shapiro–Wilk test will be applied to assess the normality of continuous variables. Measurement data will be expressed as mean ± standard deviation for normally distributed variables or as median (interquartile range, IQR) for non-normally distributed variables. Between-group comparisons will be conducted using the independent Student’s t-test or the Mann–Whitney U-test, as appropriate. The enumeration data will be presented as percentages and analyzed using the Chi-square test or Fisher’s exact test. Based on our pre-experimental outcomes, the average time to first ambulation was 6 ± 2 h and 8 ± 4 h post-surgery in Group A and Group P, respectively. The PASS software (version 21.0; NCSS, LLC, USA) was used for sample size estimation, with equal sample sizes for both groups. Assuming α = 0.05 (two-sided), β = 0.1, and power = 0.8, a minimum of 41 patients per group was required. Allowing a 5% loss to follow-up rate, a total of 86 patients (43 per group) was deemed necessary. For graphical presentation, Kaplan–Meier survival curves will be used to illustrate time-to-ambulation, and bar charts will be generated to visualize between-group differences in QoR-15 scores across postoperative time points. A fragility index (FI) analysis was conducted to assess the robustness of the dichotomous primary outcome, defined as early ambulation within 6 hours after surgery according to ERAS recommendations and the pre-specified protocol.
Ethical Considerations, Amendments, and Dissemination
This trial was approved by the Institutional Review Board of Beijing Daxing District People’s Hospital of China, affiliated with Capital Medical University, and conducted in adherence to the Declaration of Helsinki and its subsequent amendments. Any significant modifications or administrative changes to the study protocol will be submitted to the local medical ethics committee for approval and will require a formal protocol amendment. The privacy and confidentiality of patient data will be strictly protected by the investigators, and anonymized data will be utilized in publications or reports to prevent potential information leaks. If data sharing is required, all shared data will be properly desensitized, and personal identifiers will be replaced with coded numbers. All participants will be notified of any updates, and any amendments will be posted on the trial registry website to ensure transparency. The final manuscript reporting the study results will be publicly available and submitted to scientific journals.
Trial Status
This trial was approved by the Institutional Review Board of Beijing Daxing District People’s Hospital of China, affiliated with Capital Medical University. Patient recruitment began on May 7, 2025, following registration with the International Traditional Medicine Clinical Trial Registry.
Discussion
With the accelerated aging of the population and reduced physical activity in daily life, lumbar degenerative diseases, including LDH and LSS, have become leading causes of morbidity in China, resulting in a growing demand for surgical treatments.28–30 Since its introduction in China in the 1990s, PELD has gained widespread acceptance and has been widely used for treating lumbar degenerative diseases.31,32 With its efficacy confirmed in multiple clinical trials, PELD has become a well-established technique that experienced spinal endoscopic surgeons can perform at an increasingly rapid rate. Simultaneously, alleviated ERAS pathways, including preoperative health education, nutritional optimization, sustainable pain management, and early mobilization, are comprehensively applied in PELD for surgical care to expedite postoperative recovery and support short-stay or day-surgery models.11,33
Day-surgery, because of its advantages of “short and fast”, is defined in China as a planned procedure where the patient is discharged within 24 h or hospitalized for no more than 48 h.34 Two retrospective clinical studies have analyzed the safety and surgical effectiveness of PELD in the day-surgery model for treating LDH. One study conducted by Kou’s team35 evaluated 275 patients with LDH and found that PELD performance during day-surgery significantly shortened hospital stays and reduced general anesthesia-related complications. Similarly, Yu’s team9 reported that patient ambulation within 2 h postoperatively and same-day discharge yielded successful clinical therapeutic efficacy without increasing the risk of re-herniation, while facilitating earlier return to normal activities. Although PELD is widely available for treating patients with LSS, ambulation time in elderly patients remains significantly delayed. Li’s research team31 observed first ambulation times of 4.9 ± 1.82 h in patients aged 65–74 and 5.2 ± 1.73 h in those over 75, which is considerably longer than those reported in Yu’s team study.9 The first ambulation time on the day of surgery is a critical indicator for achieving day-surgery discharge, and patient recovery quality at hospital discharge is a strong predictor of postoperative rehabilitation in daily life.9 PELD performance within an ambulation surgery model is limited in elderly patients, with few innovative ERAS protocols designed to facilitate early mobilization and support the day-surgery model. As key members of the ERAS team, anesthesiologists have focused on perioperative ERAS management by transitioning from intubated general anesthesia to local anesthesia accompanied by monitored anesthesia care.36 Under local anesthesia, surgeons can assess nerve injury through intraoperative feedback, while anesthesiologists can promptly identify patient discomfort and detect sudden life-threatening adverse events. Remarkably, local anesthetic agents used alone have been reported to cause terrible surgical experiences, mainly because of unexpected intraoperative pain. A retrospective study conducted by Ru’s research team,37 involving 1100 patients with LDH undergoing PELD, found that moderate-to-severe pain frequently occurred under local anesthesia because of traction from different endoscopic instruments, which was commonly relieved with potent intravenous analgesics. Additionally, acute postoperative pain is a major factor contributing to prolonged ambulation time and is strongly associated with an increased risk of developing CPSP.38 Consequently, opioids remain irreplaceable agents involved in analgesic regimens for perioperative pain treatment. However, their side effects should not be overlooked, especially nausea and vomiting, respiratory depression, and ileus, which delay the first ambulation time, prolong patient hospitalization, and impede the development of short-stay surgery models.14 CPSP, partially induced by opioid usage and derived from acute post-surgical pain, is more prevalent among elderly patients, who are more susceptible to severe pain, physical function decline, and even depression.17
To minimize opioid-related side effects, ERAS protocols incorporate preemptive and multimodal analgesia strategies that combine various analgesics to reduce the effects of painful stimulation and perioperative opioid consumption. Nonsteroidal anti‐inflammatory drugs (NSAIDs), acetaminophen, gabapentinoids, and tramadol are mostly used in opioid-balanced analgesia schemes for spine surgery and have been proven to effectively reduce perioperative opioid requirements.11 However, despite their opioid-sparing effects, NSAIDs carry gastrointestinal and cardiovascular risks, and tramadol is associated with a higher incidence of PONV, both of which can delay hospital discharge and compromise patient safety.39 Intraoperative dexmedetomidine is also used for exerting opioid-sparing effects and reducing analgesic consumption, with advantages of minimal respiratory depression but notable side effects such as bradycardia and hypotension, which are fatal for elderly patients during perioperative period.40 According to standardized ERAS discharge criteria, patients are eligible for discharge once they can ambulate independently, and the intensity of postoperative pain has decreased to a mild level (VAS ≤ 3) and is manageable with oral analgesics without any other complications.41 An arduous decision must be made between pain control and patient safety because of the risks associated with complex, multi-dose analgesic regimens, highlighting the need for continued investigation into personalized and safer analgesic interventions for patients undergoing PELD.
TEAS provides noninvasive analgesia that can be combined with opioids to reduce opioid consumption in both vulnerable and non-vulnerable populations. Studies have demonstrated that the perioperative analgesic effects of TEAS are effective not only in children but also in elderly and frail patients.21,42 Multiple mechanisms have been proposed to explain how TEAS exerts inhibitory effects on pain, including facilitating endogenous opioid peptide release, inhibiting the product of intrinsic pain-inducing substances, interfering with the MAPK signal pathway, and downregulating TRPV1 phosphorylation.21 Additionally, TEAS reduces the incidence of PONV and promotes gastrointestinal motility by activating 5-HT and norepinephrine fibers,43 while attenuating cognitive deficits by inhibiting neuronal peroxide reactions in hippocampal tissue and preventing central and peripheral nervous systems inflammation.44 These beneficial effects highlight TEAS’s broad potential for integration into perioperative ERAS management.
Therefore, this study represents a significant effort to evaluate the effects of TEAS on early ambulation and postoperative pain in patients undergoing PELD. Positive findings would provide strong evidence supporting TEAS’s role in reducing opioid-related side effects, promoting early rehabilitation, decreasing hospitalization complications, enhancing patient satisfaction, and optimizing ERAS protocols for PELD. In the study, although ODI and JOA scores will be followed up for six months, this trial mainly focuses on perioperative and early recovery outcomes. The long-term functional data are exploratory and intended to provide descriptive insights for future confirmatory studies. Moreover, several limitations still remain. First, as a single-center clinical trial, the results may not be widely applicable across different institutions, particularly those with distinct patient demographics or perioperative care protocols. Second, the study did not assess inflammatory biomarkers or stress-related hormones, which limits the ability to explore the physiological pathways through which TEAS may influence perioperative outcomes. Future research should consider incorporating objective biological indicators, such as proinflammatory cytokines and cellular regulatory mediators, to investigate potential shifts in systemic inflammation and stress responses. Such data could help elucidate the mechanistic underpinnings of TEAS during the perioperative period of PELD and potentially expand its clinical applicability through a deeper understanding of its therapeutic effects.
Conclusion
This study aims to verify whether TEAS will benefit future patients and contribute to meaningful improvements in ERAS-based perioperative management for micro-spine surgery, ultimately supporting the establishment of a standardized PELD day-surgery model.
Abbreviations
ERAS, Enhanced recovery after surgery; TEAS, Transcutaneous electrical acupoint stimulation; PELD, Percutaneous endoscopic lumbar discectomy; QoR-15, 15-item Quality of Recovery scale; PONV, Postoperative nausea and vomiting; CPSP, Chronic postoperative pain; MISS, Minimally invasive spine surgery; POCD, Postoperative cognitive dysfunction; NRS, Numeric rating scale; VAS, Visual analog scale; BMI, Body mass index; ASA, American Society of Anesthesiologists; HR, Heart rate; ECG, Electrocardiogram; SpO2, Oxygen saturation; MAP, Mean arterial pressure; DMC, Data Monitoring Committee; CRFs, Case report forms; ODI, Oswestry disability index; JOA, Japanese Orthopedic Association score.
Data Sharing Statement
The data supporting the findings of this study will be available from the corresponding authors upon reasonable request. Interested researchers may obtain the datasets by contacting Dr. Xin Luo ([email protected]) or Dr. Bing-Yao Chen ([email protected]) via email.
Ethics and Dissemination
This study was approved by the Ethics Committee of Beijing Daxing District People’s Hospital, Capital Medical University, China. Patients were enrolled after registration in the International Traditional Medicine Clinical Trial Registry.
Acknowledgments
We thank the orthopedic surgeons at Beijing Daxing District People’s Hospital, Capital Medical University, and all team members involved in this study for their valuable contributions.
Author Contributions
All authors made substantial contributions to the conception and design of the study, as well as to data collection, execution, analysis, and interpretation. They were all involved in drafting or revising the manuscript critically for important intellectual content, approved the final version for publication, agreed on the journal for submission, and take responsibility for the integrity and accuracy of all aspects of the work.
Funding
This study was supported solely by the research funding program of our institute with no additional external grant support. The authors declare no financial or personal affiliations with Nanjing Jisheng Medical Technology Co., Ltd., the manufacturer of the Han’s acupoint nerve stimulator used in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tang J, Liang Z, He J, et al. Percutaneous endoscopic lumbar discectomy for lumbar disc herniation using an endoscopic staining: a technical note. Orthop Surg. 2021;13(4):1430–1436. doi:10.1111/os.12907
2. Mao L, Shen Z, Zhu W, et al. Comparison of the efficacy of microendoscopic discectomy and percutaneous endoscopic lumbar discectomy for treating adolescent lumbar disc herniation. Sci Rep. 2025;15(1):10185. doi:10.1038/s41598-025-94635-5
3. Liu C, Chu HL, Li G, et al. The 20 most important questions for novices of full-endoscopic spinal surgery in China: a mixed-method study protocol. BMJ Open. 2021;11(8):e049902. doi:10.1136/bmjopen-2021-049902
4. Du C, Song K, Hai B, Wang X. Retrospective study of minimal three-year follow-up of transforaminal endoscopic discectomy for lumbar disc herniation: 5000 multicenter cases. Cureus. 2023;15(12):e50993. doi:10.7759/cureus.50993
5. Luo J, Tang Y, Cao J, Li W, Zheng L, Lin H. Application of an enhanced recovery after surgery care protocol in patients undergoing lumbar interbody fusion surgery: a meta-analysis. J Orthop Surg Res. 2025;20(1):154. doi:10.1186/s13018-025-05523-7
6. Huang J, Shi Z, Duan FF, et al. Benefits of early ambulation in elderly patients undergoing lumbar decompression and fusion surgery: a prospective cohort study. Orthop Surg. 2021;13(4):1319–1326. doi:10.1111/os.12953
7. Duojun W, Hui Z, Zaijun L, Yuxiang G, Haihong C. Enhanced recovery after surgery pathway reduces the length of hospital stay without additional complications in lumbar disc herniation treated by percutaneous endoscopic transforaminal discectomy. J Orthop Surg Res. 2021;16(1):461. doi:10.1186/s13018-021-02606-z
8. Soffin EM, Wetmore DS, Barber LA, et al. An enhanced recovery after surgery pathway: association with rapid discharge and minimal complications after anterior cervical spine surgery. Neurosurg Focus. 2019;46(4):E9. doi:10.3171/2019.1.FOCUS18643
9. Yu L, Zhu B, Dong H, et al. Does immediate postoperative early ambulation affect clinical results of full-endoscopic lumbar discectomy? A historical control study of daytime operation with a 8-hour hospital stay versus inpatient operation. Orthop Surg. 2023;15(9):2354–2362. doi:10.1111/os.13814
10. Zakaria HM, Bazydlo M, Schultz L, et al. Ambulation on postoperative Day #0 is associated with decreased morbidity and adverse events after elective lumbar spine surgery: analysis from the Michigan spine surgery improvement collaborative (MSSIC). Neurosurgery. 2020;87(2):320–328. doi:10.1093/neuros/nyz501
11. Muthu S, Jeyaraman M, Jeyaraman N, Ramasubramanian S. Optimizing outcomes: implementing enhanced recovery after surgery in orthopedic surgery. World J Methodol. 2024;14(4):95558. doi:10.5662/wjm.v14.i4.95558
12. Choi YS, Kim TW, Chang MJ, Kang SB, Chang CB. Enhanced recovery after surgery for major orthopedic surgery: a narrative review. Knee Surg Relat Res. 2022;34(1):8. doi:10.1186/s43019-022-00137-3
13. Yoo JS, Ahn J, Buvanendran A, Singh K. Multimodal analgesia in pain management after spine surgery. J Spine Surg. 2019;5(suppl 2):S154–S159. doi:10.21037/jss.2019.05.04
14. Wheeler M, Oderda GM, Ashburn MA, Lipman AG. Adverse events associated with postoperative opioid analgesia: a systematic review. J Pain. 2002;3(3):159–180. doi:10.1054/jpai.2002.123652
15. Colvin LA, Bull F, Hales TG. Perioperative opioid analgesia-when is enough too much? A review of opioid-induced tolerance and hyperalgesia. Lancet. 2019;393(10180):1558–1568. doi:10.1016/S0140-6736(19)30430-1
16. Fiore JF, El-Kefraoui C, Chay MA, et al. Opioid versus opioid-free analgesia after surgical discharge: a systematic review and meta-analysis of randomised trials. Lancet. 2022;399(10343):2280–2293. doi:10.1016/S0140-6736(22)00582-7
17. Alshammari HS, Alshammari AS, Alshammari SA, Ahamed SS. Prevalence of chronic pain after spinal surgery: a systematic review and meta-analysis. Cureus. 2023;15(7):e41841. doi:10.7759/cureus.41841
18. Chen Z, He L, Di J, et al. Lumbar facet joint osteoarthritis as the underlying reason for persistent low back pain after minimally invasive discectomy. Arch Orthop Trauma Surg. 2023;143(7):3811–3821. doi:10.1007/s00402-022-04595-y
19. Szmit M, Krajewski R, Rudnicki J, Agrawal S. Application and efficacy of transcutaneous electrical acupoint stimulation (TEAS) in clinical practice: a systematic review. Adv Clin Exp Med. 2023;32(9):1063–1074. doi:10.17219/acem/159703
20. Tahmasbi F, Sanaie S, Eslami S, Rahimi-Mamaghani A. Application of transcutaneous electrical acupoint stimulation (TEAS) for management of postoperative pain after gynecological surgeries: a meta-analysis. Pain Manag Nurs. 2025;26(1):111–124. doi:10.1016/j.pmn.2024.12.005
21. Wang D, Shi H, Yang Z, et al. Efficacy and safety of transcutaneous electrical acupoint stimulation for postoperative pain: a meta-analysis of randomized controlled trials. Pain Res Manag. 2022;2022:7570533. doi:10.1155/2022/7570533
22. Liu LY, Su Y, Wang RR, et al. Transcutaneous electrical acupoint stimulation benefits postoperative pain relief of oocyte retrieval: a randomized controlled trial. J Integr Med. 2024;22(1):32–38. doi:10.1016/j.joim.2024.01.005
23. Hou Y, Kang F, Liu H, et al. Perioperative transcutaneous electrical acupoint stimulations as part of an enhanced recovery after surgery protocol for living donors undergoing nephrectomy: a randomized, controlled clinical trial. Heliyon. 2023;9(3):e14423. doi:10.1016/j.heliyon.2023.e14423
24. Lu Z, Wang Q, Sun X, et al. Transcutaneous electrical acupoint stimulation before surgery reduces chronic pain after mastectomy: a randomized clinical trial. J Clin Anesth. 2021;74:110453. doi:10.1016/j.jclinane.2021.110453
25. Wu X, Huang J, Zhang Y, et al. Perioperative transcutaneous electrical acupoint stimulation (pTEAS) in pain management in major spinal surgery patients. BMC Anesthesiol. 2022;22(1):342. doi:10.1186/s12871-022-01875-3
26. Wang LF, Liang WD, Wang BY, et al. Transcutaneous electrical acupoint stimulation for reducing cognitive dysfunction in lumbar spine surgery: a randomized, controlled trail. Front Aging Neurosci. 2022;14:1034998. doi:10.3389/fnagi.2022.1034998
27. Chiu HY, Su IW, Yu YW, Chen YC, Chen CC, Lin JH. Soreness or sng: a common symptom with differential clinical impact from pain in degenerative lumbar spine diseases. BMJ Open Qual. 2023;12(1):e001982. doi:10.1136/bmjoq-2022-001982
28. Xiu P, Zhang X. Endoscopic spine surgery in China: its evolution, flourishment, and future opportunity for advances. J Spine Surg. 2020;6(suppl 1):S49–S53. doi:10.21037/jss.2019.07.01
29. Parenteau CS, Lau EC, Campbell IC, Courtney A. Prevalence of spine degeneration diagnosis by type, age, gender, and obesity using Medicare data. Sci Rep. 2021;11(1):5389. doi:10.1038/s41598-021-84724-6
30. Li H, Ou Y, Xie F, Liang W, Tian G, Li H. Linical efficacy of percutaneous endoscopic lumbar discectomy for the treatment of lumbar spinal stenosis in elderly patients: a retrospective study. J Orthop Surg Res. 2020;15(1):441. doi:10.1186/s13018-020-01968-0
31. Xie P, Feng F, Chen Z, et al. Percutaneous transforaminal full endoscopic decompression for the treatment of lumbar spinal stenosis. BMC Musculoskelet Disord. 2020;21(1):546. doi:10.1186/s12891-020-03566-x
32. Ahn Y. Percutaneous endoscopic decompression for lumbar spinal stenosis. Expert Rev Med Devices. 2014;11(6):605–616. doi:10.1586/17434440.2014.940314
33. Kamson S, Trescot AM, Sampson PD, Zhang Y. Full-endoscopic assisted lumbar decompressive surgery performed in an outpatient, ambulatory facility: report of 5 years of complications and risk factors. Pain Physician. 2017;20(2):E221–E231.
34. Jiang L, Houston R, Li C, et al. Day surgery program at West China Hospital: exploring the initial experience. Cureus. 2020;12(7):e8961. doi:10.7759/cureus.8961
35. Kou L, Wan W, Chen C, et al. Can the full-percutaneous endoscopic lumbar discectomy in day surgery mode achieve better outcomes following enhanced recovery after surgery protocol? A retrospective comparative study. Front Surg. 2022;9:914986. doi:10.3389/fsurg.2022.914986
36. Zheng B, Yu P, Liang Y, Liu H. Comparison of safety and efficacy of anesthesia methods in percutaneous endoscopic lumbar discectomy: a network meta-analysis. Pain Res Manag. 2024;2024:8022643. doi:10.1155/prm/8022643
37. Ru N, Su C, Li J, et al. Varied low back pain induced by different spinal tissues in percutaneous endoscopic lumbar discectomy: a retrospective study. Pain Physician. 2022;25(2):E331–E339.
38. Tazreean R, Nelson G, Twomey R. Early mobilization in enhanced recovery after surgery pathways: current evidence and recent advancements. J Comp Eff Res. 2022;11(2):121–129. doi:10.2217/cer-2021-0258
39. Grossi P. Enhanced recovery after surgery (ERAS) protocols in orthopaedic surgery: opioids or not opioids? J Pain Res. 2025;18:1683–1695. doi:10.2147/JPR.S496891
40. Shuai Y, Chen Z, Wan Q, Wu J, Wang X. Dexmedetomidine: a real-world safety analysis based on FDA adverse event reporting system database. Front Pharmacol. 2024;15:1419196. doi:10.3389/fphar.2024.1419196
41. Gatam AR, Gatam L, Phedy, Mahadhipta H, Ajiantoro, Aprilya D. Full endoscopic lumbar stenosis decompression: a future gold standard in managing degenerative lumbar canal stenosis. Int J Spine Surg. 2022;16(5):821–830. doi:10.14444/8338
42. Li Y, Ma Y, Guo W, et al. Effect of transcutaneous electrical acupoint stimulation on postoperative pain in pediatric orthopedic surgery with the enhanced recovery after surgery protocol: a prospective, randomized controlled trial. Anaesth Crit Care Pain Med. 2023;42(6):101273. doi:10.1016/j.accpm.2023.101273
43. Chen J, Tu Q, Miao S, Zhou Z, Hu S. Transcutaneous electrical acupoint stimulation for preventing postoperative nausea and vomiting after general anesthesia: a meta-analysis of randomized controlled trials. Int J Surg. 2020;73:57–64. doi:10.1016/j.ijsu.2019.10.036
44. Zhang Y, Jiang Y, Glielmi CB, et al. Long-duration transcutaneous electric acupoint stimulation alters small-world brain functional networks. Magn Reson Imaging. 2013;31(7):1105–1111. doi:10.1016/j.mri.2013.01.006
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effects of Transcutaneous Electrical Acupoint Stimulation on Recovery After Gynecological Laparoscopic Surgery: A Randomized, Single-Blind, Controlled Trial
Zheng J, Zhou H, Diao Y, Song P, Yi Z, Guo X, Li L
Journal of Pain Research 2025, 18:6449-6462
Published Date: 3 December 2025