Back to Journals » Journal of Inflammation Research » Volume 19
Effects of Transcutaneous Auricular Vagus Nerve Stimulation and Transcutaneous Electrical Acupoint Stimulation on Peripheral Inflammatory Factors in Patients with Negative Symptoms of Schizophrenia: A 2×2 Factorial Design Protocol
Authors Li W ![]() , Zhang S, Zhang B, Qian J, Lo V
, Zhang S, Zhang B, Qian J, Lo V ![]() , Su M, Li X, Chen Y, Li Y, Sun J
, Su M, Li X, Chen Y, Li Y, Sun J ![]() , Gong Y, Guo T
, Gong Y, Guo T ![]()
Received 1 May 2026
Accepted for publication 18 June 2026
Published 7 July 2026 Volume 2026:19 616229
DOI https://doi.org/10.2147/JIR.S616229
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Wenjun Li1,*, Shumin Zhang1,*, Bingkui Zhang2,*, Jun Qian3, Vanhao Lo1, Mingbing Su2, Xinghua Li2, Ying Chen2, Yan Li2, Jinbo Sun4,5, Yi Gong6, Taipin Guo1
1School of Second Clinical Medicine, Yunnan University of Chinese Medicine, Kunming, People’s Republic of China; 2Kunming Psychiatric Hospital, Kunming, People’s Republic of China; 3Department of Psychiatry, Anning First People’s Hospital Affiliated to Kunming University of Science and Technology, Kunming, People’s Republic of China; 4Wearable BCI and Intelligent Rehabilitation Innovation Lab, Guangzhou Institute of Technology, Xidian University, Xian, People’s Republic of China; 5Engineering Research Center of Molecular and Neuro Imaging of the Ministry of Education, School of Life Science and Technology, Xidian University, Xian, People’s Republic of China; 6Department of Encephalopathy, The First Affiliated Hospital of Yunnan University of Chinese Medicine, Kunming, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yi Gong; Taipin Guo, Email [email protected]; [email protected]
Background: Negative Symptoms of Schizophrenia (NSS) are the primary contributors to poor prognosis in schizophrenia (SCZ), and immune-inflammatory mechanisms play a pivotal role in their pathogenesis. As non-invasive neuromodulation techniques, transcutaneous auricular vagus nerve stimulation (taVNS), and transcutaneous electrical acupoint stimulation (TEAS) have been demonstrated to modulate peripheral inflammation levels in patients with SCZ.
Purpose: This study aims to investigate the independent and synergistic effects of taVNS and TEAS on modulating peripheral inflammatory factors and ameliorating negative symptoms in patients with NSS.
Patients and Methods: This study employs a single-blind, randomized, sham-controlled, 2×2 factorial design. A total of 108 participants will be randomly allocated in a 1:1:1:1 ratio to four groups: taVNS plus TEAS, active taVNS plus TEAS, sham taVNS plus TEAS, and sham taVNS plus sham TEAS. The interventions will be administered for 30 minutes per session on alternate days for 4 weeks, followed by a 4-week follow-up period. The primary outcome is the change from baseline in peripheral inflammatory cytokine levels at weeks 4 and 8.
Results: Recruitment is ongoing.
Conclusion: The study protocol aims to investigate the pre- and post-treatment changes in peripheral inflammatory cytokines among patients with NSS, with a specific focus on the correlation between symptom severity and alterations in inflammatory levels, thereby providing a biological rationale to guide clinical treatment.
Keywords: schizophrenia, negative symptoms, transcutaneous auricular vagus nerve stimulation, transcutaneous acupoint electrical stimulation, peripheral inflammatory cytokines, factorial design
Introduction
Schizophrenia (SCZ) is a severe psychiatric disorder. The negative symptoms of schizophrenia (NSS), centrally characterized by avolition, anhedonia, blunted affect, and social withdrawal, are critical factors leading to long-term disability and social marginalization1 and represent the primary cause of poor functional outcomes in SCZ.2,3 Epidemiological data indicate that up to 60% of patients experience prominent negative symptoms during the disease course. Notably, over half of these individuals require long-term clinical intervention due to the severity of these symptoms, imposing a substantial economic burden on their families and society.4,5
Currently, antipsychotics still primarily target the dopaminergic system, yet they offer limited improvement for negative symptoms.6 Furthermore, they are frequently associated with adverse effects such as extrapyramidal symptoms, weight gain, and abnormal glucose and lipid metabolism,7 which severely compromise patient medication adherence and long-term prognosis.
In the search for effective intervention targets for NSS, recent studies have revealed the significant role of immune-inflammatory mechanisms in the onset and development of these symptoms.8–10 Meta-analyses have demonstrated11 that among pro-inflammatory cytokines, interleukin-1β (IL-1β), interleukin-2 (IL-2), interleukin-6 (IL-6), and tumor necrosis factor-α (TNF-α) exhibit a moderate positive correlation with the severity of negative symptoms. Mechanistically, elevated peripheral inflammatory factors can trigger neuroinflammation, which subsequently disrupts dopaminergic reward circuits12 and impairs motivational integration,13 ultimately exacerbating negative symptoms.14 Therefore, exploring intervention strategies capable of effectively inhibiting peripheral inflammation is of significant importance.
Transcutaneous auricular vagus nerve stimulation (taVNS) and transcutaneous electrical acupoint stimulation (TEAS), as derivative non-invasive electrical stimulation techniques, have been demonstrated to modulate peripheral inflammation levels in SCZ. Previous studies have shown15 that taVNS can significantly reduce the levels of IL-2, IL-6, IL-1β, and TNF-α in patients with treatment-resistant SCZ, with the reduction in TNF-α being significantly correlated with the improvement of negative symptoms following treatment. The underlying mechanism may involve the activation of the cholinergic anti-inflammatory pathway, which inhibits the release of pro-inflammatory cytokines by central microglia and peripheral macrophages, thereby attenuating systemic inflammation15–17 and subsequently alleviating negative symptoms. Similarly, TEAS not only reduces IL-2 and IL-6 levels in patients with first-episode schizophrenia18 but also regulates cytokine expression in patients with late-pregnancy depression.19 It primarily exerts its anti-inflammatory effects by driving somato-autonomic reflexes, such as the vagal-adrenal axis.20,21 Although both taVNS and TEAS demonstrate promising therapeutic potential, their clinical efficacy remains limited, akin to other single neuromodulation modalities. Research indicates that combining taVNS with other neuromodulation techniques may yield greater therapeutic outcomes than standalone treatments. For instance, a mechanistic study by Sun et al16 revealed that the concurrent application of taVNS and transcranial direct current stimulation significantly enhanced the activation of central neural networks in healthy subjects. Furthermore, evidence shows that combined interventions integrating taVNS with electroacupuncture exhibit significant efficacy in alleviating depression comorbid with chronic pain.17 Therefore, it is reasonable to hypothesize that the combined use of taVNS and TEAS may generate complementary effects, thereby enhancing overall therapeutic efficacy.
Building upon these previous findings, the present study employs a 2×2 factorial design to investigate the independent and synergistic effects of two interventions, TEAS and taVNS, on peripheral inflammatory cytokine levels in patients with NSS. Furthermore, we aim to explore whether the severity of NSS correlates with changes in peripheral inflammatory cytokine levels, ultimately seeking to provide a biological basis for guiding clinical treatment.
Material and Methods
Study Design and Objectives
A randomized, sham-controlled 2×2 factorial design is adopted in this study, in which participants, outcome assessors, and statisticians are blinded to the group allocation. The proposed trial period is from January 30, 2026, to June 30, 2026. All participants will be randomly assigned in a 1:1:1:1 ratio to one of four groups: taVNS plus TEAS, taVNS plus sham TEAS, sham taVNS plus TEAS, or sham taVNS plus sham TEAS. Each participant will receive treatment every other day for 4 weeks, followed by a 4-week follow-up period. Clinical scale assessments will be conducted at baseline and at weeks 2, 4, 6, and 8. Blood samples will be collected at baseline, week 4, and week 8 (Table 1 and Figure 1).
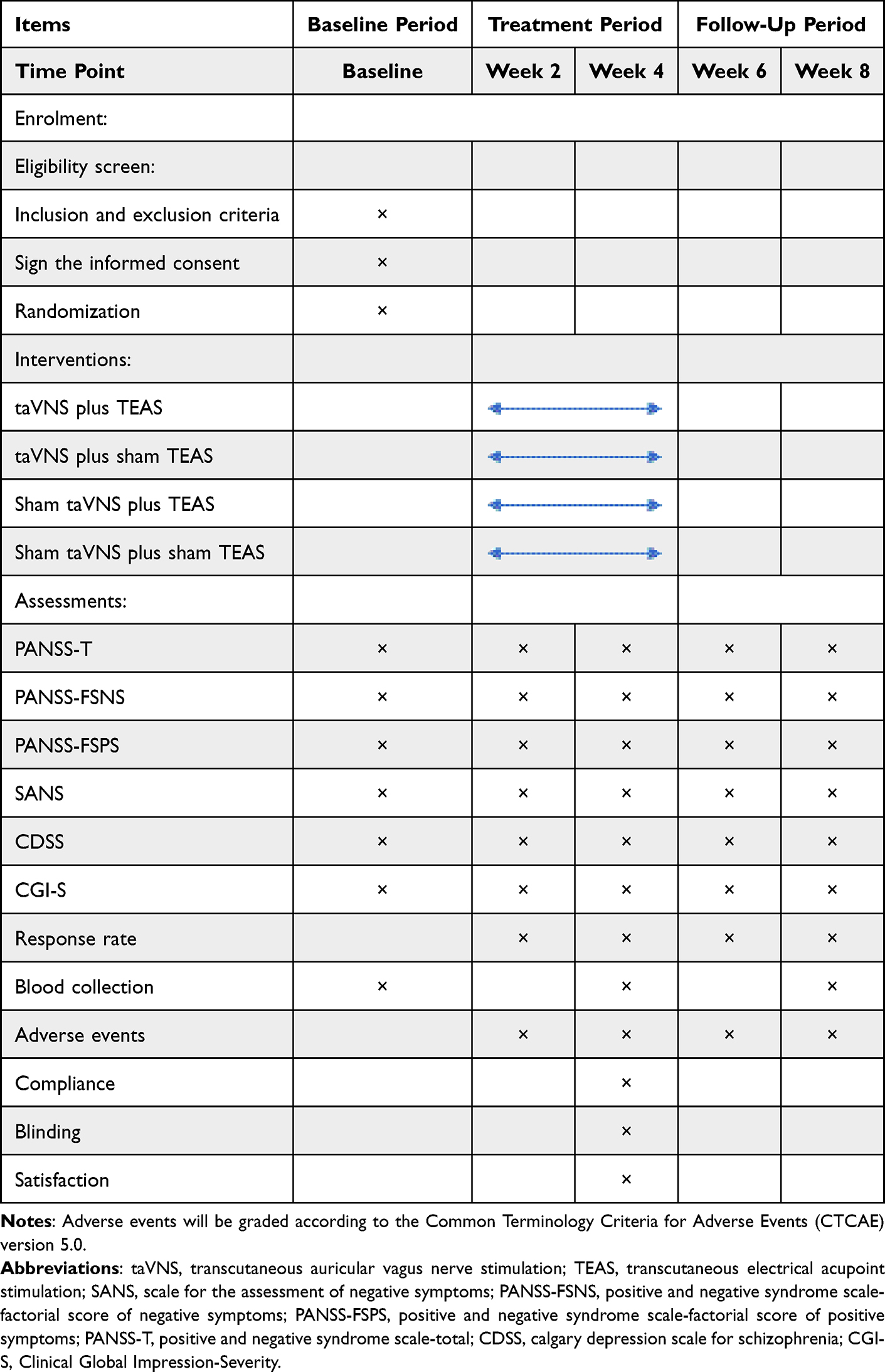 |
Table 1 Standard Protocol Items |
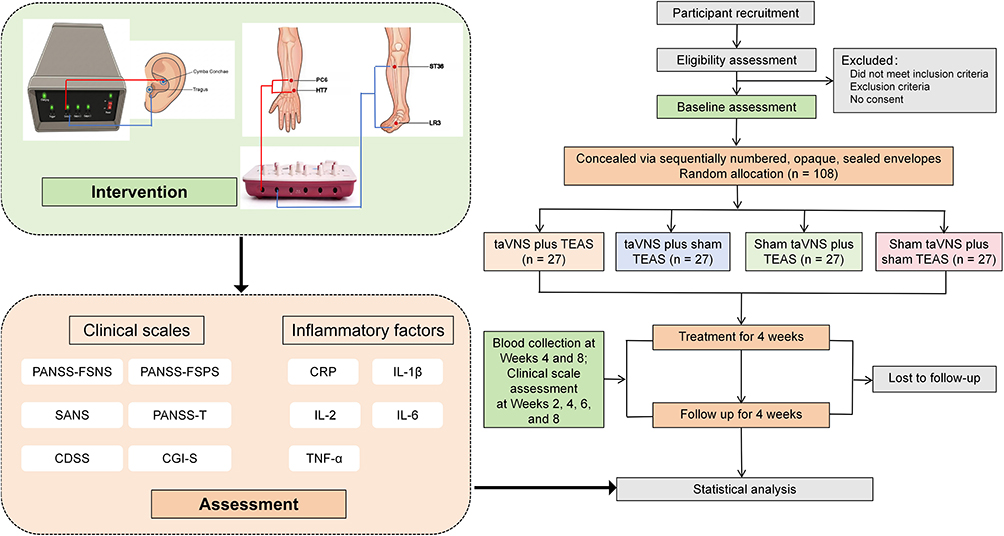 |
Figure 1 Study flowchart and intervention diagram. Following baseline assessments of clinical scales and inflammatory markers, 108 eligible patients will be randomized into four groups (n=27 per group). The study includes a 4-week treatment phase followed by a 4-week follow-up phase, with scheduled assessments to monitor clinical symptoms and peripheral inflammatory factors levels. Abbreviations: CDSS, Calgary Depression Scale for Schizophrenia; CGI-S, Clinical Global Impression-Severity; CRF, Case Report Forms; CRP, C-reactive protein; IL-1β, Interleukin-1β; IL-2, Interleukin-2; IL-6, Interleukin-6; PANSS-FSNS, Positive and Negative Symptom Scale-Factor Score for Negative Symptoms; PANSS-FSPS, Positive and Negative Syndrome Scale-Factorial Structure of Positive Symptoms; PANSS-T, Positive and Negative Syndrome Scale-Total; SANS, Scale for the Assessment of Negative Symptoms; taVNS, transcutaneous auricular vagus nerve stimulation; TEAS, transcutaneous electrical acupoint stimulation; TNF-α, Tumor necrosis factor-α. |
Recruitment
Participants will be recruited from the inpatient department of a psychiatric hospital. Trained psychiatrists will conduct rigorous screening of the participants. For those who meet the eligibility criteria, the psychiatrists will provide further explanations regarding the study procedures, objectives, potential benefits, and possible adverse events, while also informing them of their right to withdraw from the study at any time. Individuals who fully comprehend the trial details and agree to participate will sign a written informed consent form before randomization.
Inclusion and Exclusion Criteria
Inclusion criteria: (1) A diagnosis of schizophrenia as defined by the DSM-5; (2) Between 18 and 65 years of age;22(3) Clinically stable for at least 4 weeks before enrollment, and receiving a stable dose of antipsychotic medication (excluding patients taking antidepressants) for at least 4 weeks, with the dosage remaining unchanged throughout the intervention period; (4) A score of ≥ 24 on the Positive and Negative Syndrome Scale-Factor Score for Negative Symptoms (PANSS-FSNS) (N1: blunted affect, N2: emotional withdrawal, N3: poor rapport, N4: passive/apathetic social withdrawal, N6: lack of spontaneity and flow of conversation, G7: motor retardation, G16: active social avoidance), and a score of ≥ 4 on at least two of the three core negative symptom items (N1, N4, N6);23 (5) Written informed consent was obtained from the patient or their legally authorized representative.
Exclusion criteria: (1) A score of > 19 on the Positive and Negative Syndrome Scale-Factor Score for Positive Symptoms (PANSS-FSPS) (P1: delusions, P3: hallucinatory behavior, P5: grandiosity, P6: suspiciousness/persecution, G9: unusual thought content), and a score of ≥ 4 on two or more of the five PANSS-FSPS items;18 (2) A total score of > 6 on the Calgary Depression Scale for Schizophrenia (CDSS);24 (3) Comorbid psychiatric disorders such as depression, anxiety disorders, obsessive-compulsive disorder, and bipolar disorder, or neurological disorders such as epilepsy; (4) Severe medical conditions, including severe cardiovascular, hepatic, or renal diseases, or organic brain disease; (5) Alcohol or other substance dependence or addiction; (6) Suicidal tendencies or violent behavior; (7) Auricular deformities and other auricular disorders; (8) Treatment with antibiotics, anti-inflammatory drugs, or hormones within the past month; or having an acute infectious or acute inflammatory disease within the past 4 weeks; or concurrent chronic inflammatory diseases, autoimmune diseases, etc; (9) Presence of implanted electronic devices that may interfere with or be affected by TEAS/taVNS equipment, such as cardiac pacemakers, medication pumps, cochlear implants, or implanted brain stimulators; (10) A history of TEAS/taVNS treatment within the past 6 months; (11) Skin lesions, damage, or infection at the intended treatment site; (12) Females who are pregnant, lactating, planning to conceive, or within 6 months postpartum.
Withdrawal Criteria
(1) Participants mistakenly enrolled who do not meet the inclusion criteria; (2) Participants with poor compliance, or those who voluntarily withdraw during the treatment period; (3) Use of concomitant treatments prohibited by the study protocol.
Termination Criteria
(1) Participants who experience severe adverse reactions during the study and are deemed unsuitable for continued participation; (2) Participants whose condition deteriorates, necessitating an adjustment to the treatment regimen.
Random Allocation and Blinding
Eligible participants will be randomized in a 1:1:1:1 ratio into one of four groups: taVNS plus TEAS, taVNS plus sham TEAS, sham taVNS plus TEAS, or sham taVNS plus sham TEAS. The randomization sequence will be generated by an independent statistician using SPSS version 28.0 (IBM Corp., Chicago, IL, USA) and concealed in sequentially numbered, opaque, sealed envelopes. Following informed consent regarding the randomization procedure, an independent researcher—uninvolved in either data collection or intervention delivery—will draw an envelope to determine each participant’s group assignment. To further ensure methodological rigor, all treatments will be administered in separate rooms to prevent information exchange among participants. The participants, treating psychiatrists, outcome assessors, and statisticians, will be strictly blinded to the group allocation. Although the acupuncturists will be unblinded to the treatment assignments, they will not participate in any subsequent outcome assessments or data analysis. To optimize blinding efficacy, participants will be informed upon enrollment that they may not experience any overt sensation during the stimulation. Upon completion of the treatment phase, all participants will be asked to guess whether they received the taVNS or TEAS intervention, thereby assessing the success of the blinding procedure.
Intervention
Treatments will be administered by certified acupuncturists with at least 3 years of clinical experience. All acupuncturists will undergo standardized training to ensure complete familiarity with the study protocol. Participants will continue taking their pre-enrollment antipsychotic medication throughout the study period. taVNS and TEAS will be administered simultaneously every other day for 30 minutes per session over 4 weeks, followed by a 4-week follow-up period (Table 1 and Figure 1).
Electrode Placement and Device Settings: Earbud-type electrodes (TES-M3-M-01; Wearable Brain–Computer Interface and Intelligent Rehabilitation Technology Innovation Laboratory, Xidian University, and Guangzhou Institute of Technology, China) will be applied to the left cymba conchae and tragus (Figure 1). The device will be programmed with a pulse frequency of 25 Hz, a 250 μs pulse width, and a 30-second on/off cycle. The current intensity will be adjustable from 0.1 to 3 mA in 0.1 mA increments. Through repeated measurements, the target stimulation intensity will be individually titrated to the exact midpoint between the participant’s sensory and pain thresholds.
taVNS: The current will be ramped up at a rate of 0.1 mA/s until reaching the target intensity within the initial 30 seconds. This stimulation level will be maintained for 29 minutes, followed by a gradual ramp-down to zero at the identical rate.
Sham taVNS: While electrodes will be positioned at the same anatomical sites, actual electrical delivery will be restricted to the beginning and the end of the treatment session. Utilizing the identical ramp-up and ramp-down rates, the current output will last for less than 1 minute at each of these two time points to ensure effective blinding.
Acupoint Selection and Preparation: Bilateral Neiguan (PC6), Shenmen (HT7), Zusanli (ST36), and Taichong (LR3) will be targeted (Table 2), located according to the WHO Standard Acupuncture Point Locations. Following routine disinfection, an SDZ-II electroacupuncture device (Suzhou, China) will be used, with anodes placed on PC6 and ST36, and cathodes on HT7 and LR3.
 |
Table 2 Location of Acupoint in the Trial |
TEAS: The device will be set to a 50 Hz frequency and a 0.2 ms ± 30% pulse width. Current intensity will be gradually increased until achieving a “strong but comfortable” level, which will be maintained for 30 minutes.
Sham TEAS: While using the same acupoints and 30-minute duration, the current will be quickly lowered to the minimal sensory threshold within 30 seconds, and then ramped down to 0 over the following 15 seconds. To ensure effective blinding, the device’s operational cues (flashing indicator lights and sounding buzzer) will continue functioning throughout the session without delivering any actual electrical stimulation.
To ensure the integrity of the blinding, the sham taVNS and sham TEAS interventions are identical to the active interventions regarding device appearance, electrode placement procedure, duration, and setting. These sham protocols have been well-validated in previous studies, demonstrating sensory similarity to active stimulation and high sham credibility.15,25 Furthermore, participants will be informed at enrollment that they may or may not experience sensations during the stimulation.
Sample Size
The sample size estimation was based on the primary biological outcome: the change in peripheral TNF-α levels from baseline to week 4. Referring to the variance parameters from a previous trial involving patients with treatment-resistant schizophrenia predominantly presenting with negative symptoms15 (where TNF-α levels decreased from 380.47 ± 52.74 to 306.28 ± 42.34 pg/mL after treatment), and considering that the non-TRS patients included in this study possess better neuroimmune plasticity and greater potential for downregulation, we set the expected effect size for the targeted main effect at a medium-to-large level (Cohen’s f = 0.30). The sample size calculation was performed using G*Power software based on a two-way analysis of variance. The parameters were set as follows: a two-tailed significance level of 0.05, a statistical power (1-β) of 0.80, a numerator degree of freedom of 1, and 4 groups. A minimum of 90 participants is required to effectively detect this effect. Accounting for an anticipated dropout rate of approximately 15%, at least 27 patients are required per group, resulting in a final planned recruitment of 108 patients.
Assessments
The primary outcome measure of this study is the change in serum concentrations of C-reactive protein (CRP) and inflammatory cytokines (IL-1β, IL-2, IL-6, and TNF-α) from baseline at weeks 4 and 8. Fasting venous blood samples (2 mL) will be drawn by a nurse. The samples will be allowed to stand at room temperature for 20 minutes, followed by centrifugation at 3000 rpm for 10 minutes at 4°C. The separated serum will then be immediately stored in a −80°C freezer.
The secondary outcomes include: (1) Score changes from baseline to weeks 2, 4, 6, and 8 on the PANSS-FSNS, PANSS-FSPS, Scale for the Assessment of Negative Symptoms (SANS), Positive and Negative Syndrome Scale total score (PANSS-T), Calgary Depression Scale for Schizophrenia (CDSS), and Clinical Global Impressions-Severity (CGI-S) scale, as well as the treatment response rates at these four time points; (2) Safety and compliance evaluations, encompassing the continuous recording of adverse events throughout the entire study period, the monitoring of participant treatment compliance, and treatment satisfaction surveys; (3) Trial quality assessment, evaluating the success rate of the blinding procedure at the conclusion of the study.
The PANSS is widely used to assess symptom severity in patients with schizophrenia. The scale consists of 30 items divided into three domains: positive symptoms, negative symptoms, and general psychopathology. Each item is rated on a 7-point scale ranging from 1 (absent) to 7 (extreme). Specifically, the PANSS-FSNS—which comprises items N1, N2, N3, N4, N6, G7, and G16—is utilized to comprehensively evaluate the patients’ negative symptoms of schizophrenia.26,27 The PANSS-FSPS—which comprises items P1, P3, P5, P6, and G9—is utilized to comprehensively evaluate the patients’ positive symptoms.28 The PANSS Total Score (PANSS-T) represents the sum of all item scores and is utilized to assess the overall symptom severity of the patients.29
The treatment response rate will be defined as the proportion of participants who achieve a ≥20% reduction in the PANSS-FSNS score from baseline.23
The SANS is widely utilized to assess negative symptoms in patients with schizophrenia. The scale encompasses a total of 24 items categorized into five distinct subscales: affective flattening/blunting, alogia, avolition, anhedonia/asociality, and attention impairment. Scoring for each item ranges from 0 (normal) to 5 (severe).30
Serving as a standardized instrument to assess current illness severity, the CGI-S evaluates the patient’s medical history, major symptoms, and functional impairment. This comprehensive assessment is quantified using a 7-point scale, ranging from 1 (normal, not at all ill) to 7 (extremely ill).31
Applicable across all stages of the disorder, the CDSS is specifically designed to isolate and evaluate depressive symptoms in patients with schizophrenia. The instrument comprises nine items: depression, hopelessness, self-depreciation, guilty ideas of reference, pathological guilt, morning depression, early wakening, suicide, and observed depression. Each item is rated from 0 (absent) to 3 (severe).32
To promote participant retention and complete follow-up, researchers will maintain regular communication with participants and their primary physicians. If a participant decides to discontinue the trial interventions (taVNS/TEAS) early, they will still be encouraged to attend the scheduled assessment visits (at weeks 6 and 8) to collect the primary and secondary outcome data (eg, blood samples and PANSS scores) for the intention-to-treat analysis, provided they have not withdrawn their consent.
Statistical Analysis
Statistical analyses will be conducted according to the intention-to-treat principle. Normally distributed continuous variables will be reported as means ± standard deviations (SD), whereas non-normally distributed data will be presented as medians and interquartile ranges (IQR). Categorical variables will be expressed as frequencies and percentages. For missing data, we will assume the data are missing at random and handle them using multiple imputation. To evaluate the robustness of our results against potential departures from the random and missing-not-at-random assumption, a sensitivity analysis will be performed under the assumption of missing not at random. For repeated measures data that meet the assumptions of normality and homogeneity of variance, mixed-effects models will be employed; if these assumptions are not met, generalized linear mixed models will be utilized. The models will include “Time”, “taVNS”, “TEAS”, and all their interaction terms as fixed effects. Baseline outcome values and the concurrent antipsychotic dosage (calculated as olanzapine equivalents33) will be included in the models as pre-specified covariates to adjust for potential pharmacological confounding. The three-way interaction will be tested first; if significant, simple main effects at weeks 4 and 8 will be further analyzed. If non-significant, the models will proceed to evaluate two-way interactions and ultimately assess the independent main effects of taVNS and TEAS. Post-hoc analyses will be performed based on the characteristics of the outcome data, with multiple comparisons corrected using either Dunnett’s or Tukey’s test. The correlations between inflammatory cytokines and clinical scale scores will be assessed using Pearson’s correlation or Spearman’s rank correlation, depending on the data distribution. All hypothesis tests will be two-sided, and a P-value < 0.05 will be considered statistically significant. Furthermore, blinding efficacy will be assessed by calculating the guess rate and Bang’s Blinding Index.
Data Management
To ensure the highest standards of accuracy, completeness, and authenticity, all research personnel will undergo standardized training before study initiation. All participant information will be maintained under strict confidentiality. Original data will be gathered by psychiatrists at pre-specified time points using validated questionnaires and clinical assessment tools, with all findings documented in Case Report Forms (CRF). To minimize entry errors, two independent research assistants, uninvolved in the clinical procedures, will perform double data entry for secure electronic storage. Following data collection, statistical analyses will be executed by professional statisticians. The Ethics Committee, which maintains no conflict of interest with the project, will conduct periodic reviews of trial progress and CRF integrity, reserving the right to modify or terminate the study if necessary. All primary clinical data will be archived for a minimum of five years following the publication of the study results.
Risk Management
Participants will continue their prescribed antipsychotic treatments under the supervision of their primary physicians. Safety will be closely monitored, with all adverse events encountered during the trial being thoroughly evaluated and recorded in the CRF. Specifically, the severity of all adverse events will be graded according to the Common Terminology Criteria for Adverse Events version 5.0, which classifies events on a 5-point scale: Grade 1 (Mild), Grade 2 (Moderate), Grade 3 (Severe), Grade 4 (Life-threatening), and Grade 5 (Death). In the event of an adverse event (typically Grade 3 or higher), appropriate medical intervention will be provided immediately and sustained until the condition is resolved or effectively managed. Furthermore, any adverse events will be promptly documented and reported to the Institutional Review Board within 24 hours.
Discussion
NSS constitutes a core symptom cluster of SCZ. The resulting social withdrawal and avolition severely impair patients’ self-care capacity and lead to a significant deterioration in their quality of life.1,34 In recent years, the peripheral inflammation hypothesis has gained considerable attention. Accumulating evidence suggests that chronic peripheral inflammation is closely associated with the pathogenesis of schizophrenia and is considered one of the core pathological mechanisms underlying negative symptoms.11,13 Clinical observations reveal that patients exhibit significantly elevated levels of systemic inflammatory markers (eg, CRP) and multiple pro-inflammatory cytokines (IL-1β, IL-2, IL-6, TNF-α) compared to healthy controls.35,36 Furthermore, the aberrant expression of the latter four demonstrates a moderate positive correlation with the severity of negative symptoms.11 At the pathophysiological level, excessive peripheral pro-inflammatory cytokines can compromise the integrity of the blood–brain barrier and infiltrate the central nervous system,37 thereby directly activating cerebral microglia. Once activated, microglia not only release massive amounts of cytokines (such as TNF-α and IL-1β) to induce an inflammatory cascade,38 but also trigger the aberrant activation of the complement system. This mediates inappropriate synaptic pruning, further exacerbating the disruption of neural circuits.39 Such central neuropathological damage, driven by peripheral inflammation, can ultimately lead to structural and functional impairments in key brain regions such as the prefrontal cortex, which manifest clinically as negative symptoms including apathy and alogia.40 Given the close correlation of CRP, IL-1β, IL-2, IL-6, and TNF-α with negative symptoms, as well as their roles as key effector molecules in the aforementioned immune cascade, this study selected these five peripheral inflammatory markers for measurement, aiming to evaluate their dynamic changes before and after the intervention.
As non-invasive neuromodulation techniques, taVNS and TEAS can effectively avoid medication-induced adverse effects while exerting targeted anti-inflammatory effects through neuro-immune axes such as the cholinergic anti-inflammatory pathway. The theoretical foundation of taVNS is based on the innervation of the auricle by the auricular branch of the vagus nerve; therefore, transcutaneous stimulation of this region can achieve effects comparable to those of implantable vagus nerve stimulation.41 The vagus nerve is not only central to autonomic regulation but also plays a pivotal role in immune modulation via the cholinergic anti-inflammatory pathway. Studies have demonstrated42–44 that acetylcholine released from vagal nerve terminals specifically binds to α7 nicotinic acetylcholine receptors on the surface of immune cells, thereby effectively inhibiting the activation of central microglia and peripheral macrophages. This process significantly downregulates the release of multiple pro-inflammatory cytokines, including TNF-α, IL-1β, and IL-6, thereby blocking the cascade amplification of the systemic inflammatory response at the molecular level. TEAS combines the advantages of traditional acupuncture and electrical nerve stimulation. By integrating the therapeutic effects of both without puncturing the skin, it effectively circumvents acupuncture-related risks of infection, bleeding, and pain, thereby generally yielding higher patient adherence.45 Research indicates that the stimulation of ST36 and LR3 can activate the vagal-adrenal axis via somatosensory afferent pathways, suppressing peripheral systemic inflammation and subsequently blocking the trans-barrier transmission of inflammatory signals to the central nervous system.46,47 Concurrently, the stimulation of PC6 and HT7 can modulate the vagus nerve and the hypothalamic–pituitary–adrenal axis, inhibiting central microglial activation as well as the levels of IL-1β and TNF-α, thus ameliorating the central neuroinflammatory microenvironment.48,49 Based on these mechanisms, we selected these four sets of acupoints—ST36, LR3, PC6, and HT7—for the intervention.
Given that both taVNS and TEAS may possess antidepressant effects, the CDSS is employed for monitoring during the screening and intervention phases to control for potential confounding factors. Regarding the stimulation frequency, an every-other-day protocol was adopted. This approach minimizes the risk of adverse reactions and ensures patient adherence while avoiding over-stimulation, thereby guaranteeing the safety and stability of the study procedures. In summary, this study represents the first randomized controlled trial to explore the peripheral inflammatory mechanisms underlying the combined use of taVNS and TEAS in patients with NSS. This combined intervention strategy holds promise for overcoming the limitations of monotherapy, thereby providing novel theoretical and clinical evidence for the treatment of NSS. Notably, this combined therapy is characterized by its user-friendly operation, compact equipment, and minimal adverse reactions. These features confer significant advantages for mobile applications, making them suitable for inpatient, outpatient, and even community settings. Consequently, it can significantly enhance clinical flexibility and patient adherence, demonstrating broad prospects for clinical application.
However, this study protocol has several limitations. First, the therapists are not blinded, which may affect the objectivity of the treatment outcomes. To minimize potential bias, strict blinding will be implemented for both the clinical assessors and data analysts, thereby maximizing the objectivity of the efficacy evaluations. Second, as a single-center trial conducted in China, the external validity and generalizability of our findings are inherently limited by cultural and clinical practice variability. Specifically, the high cultural familiarity and acceptance of acupoint-based therapies (such as TEAS) among the Chinese population may elevate treatment expectations, which could substantially amplify the placebo response in both the active and sham intervention groups. Therefore, future validation through multi-center, cross-cultural cohorts is fundamentally warranted. Finally, our exploration of inflammatory mechanisms has certain limitations. First, the assay panel primarily focuses on specific pro-inflammatory cytokines (eg, CRP, IL-1β, IL-2, IL-6, and TNF-α), which cannot fully capture the complex immune-inflammatory network. Second, to minimize patient burden and prevent high dropout rates in this vulnerable NSS population, blood sampling is restricted to baseline, Week 4, and Week 8. This infrequent sampling precludes the capture of early biological response dynamics. Future in-depth investigations should incorporate multi-dimensional neuroimmune markers and more frequent sampling time points.
Conclusions
In summary, guided by the role of peripheral inflammation, this study protocol outlines a non-invasive combined intervention strategy for NSS. By dynamically monitoring inflammatory markers before and after the intervention, we aim to further elucidate the potential correlation between peripheral inflammatory cytokine levels and the severity of negative symptoms. Ultimately, this approach seeks to provide a reliable biological rationale for the objective clinical assessment of disease status and the guidance of individualized treatment.
Dissemination Policy
The results of this trial will be completely and transparently reported in peer-reviewed academic journals and presented at relevant domestic and international scientific conferences.
Abbreviations
CDSS, Calgary Depression Scale for Schizophrenia; CGI-S, Clinical Global Impression-Severity; CRF, Case Report Forms; CRP, C-reactive protein; IL-1β, Interleukin-1β; IL-2, Interleukin-2; IL-6, Interleukin-6; NSS, Negative Symptoms of Schizophrenia; PANSS-FSNS, Positive and Negative Symptom Scale-Factor Score for Negative Symptoms; PANSS-FSPS, Positive and Negative Syndrome Scale-Factorial Structure of Positive Symptoms; PANSS-T, Positive and Negative Syndrome Scale-Total; SANS, Scale for the Assessment of Negative Symptoms; SCZ, Schizophrenia; taVNS, Transcutaneous Auricular Vagus Nerve Stimulation; TEAS, Transcutaneous Electrical Acupoint Stimulation; TNF-α, Tumor necrosis factor-α.
Data Sharing Statement
The data for this study will be available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2013. All procedures involving human subjects/patients were approved by the Ethics Committee of Kunming Psychiatric Hospital (Approval No.: 2025-LLSC004). The study protocol adheres to the SPIRIT guidelines and was registered with the International Traditional Medicine Clinical Trial Registry (registration number: ITMCTR2026000212) on January 28, 2026. Written informed consent is obtained from all participants before any study-related procedures. The consent process will be conducted face-to-face by trained psychiatrists. Data confidentiality and participant privacy are maintained throughout the study in accordance with the General Data Protection Regulation. Any important modifications to the study protocol (e.g., changes to eligibility criteria, outcome measures, or statistical analyses) will be formally submitted to the Ethics Committee of Kunming Psychiatric Hospital for approval before implementation. Subsequently, these amendments will be updated on the International Traditional Medicine Clinical Trial Registry, and all relevant trial investigators and participants will be informed accordingly.
Author Contributions
Wenjun Li: Conceptualization, writing – original draft preparation; Shumin Zhang: Conceptualization, writing – original draft preparation; Bingkui Zhang: Conceptualization, methodology, writing original draft preparation; Jun Qian: methodology, writing – original draft preparation; Vanhao Lo: methodology, writing – review and editing; Mingbin Su: investigation, writing – review and editing; Xinghua Li: investigation, writing – review and editing; Ying Chen: investigation, writing – review and editing; Yan Li: investigation, writing – review and editing; Jinbo Sun: investigation, writing – review and editing, supervision; Yi Gong: methodology, writing – review and editing, supervision, project administration; Taipin Guo: methodology, writing – review and editing, supervision, project administration. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study is supported by the Yunnan Province Traditional Chinese Medicine Joint Special General Project (202301AZ070001-179); the Yunnan High-level Talents in Traditional Chinese Medicine Discipline Leader (Chinese Medicine Acupuncture): Taipin Guo; the Xidian University Specially Funded Project for Interdisciplinary Exploration (TZJH2024014); the “Liang Fanrong Expert Workstation” of Yunnan Province-Yunnan Science and Technology Programme (202305AF150072). These funding sources had no role in the design, execution, analysis, or interpretation of this study, and will not influence the submission of results.
Disclosure
The authors declare no competing interests.
References
1. Kalisova L, Michalec J, Dechterenko F. et al. Impact of cognitive performance and negative symptoms on psychosocial functioning in Czech schizophrenia patients. Schizophrenia. 2023;9(1):43. doi:10.1038/s41537-023-00374-9
2. Marder SR, Umbricht D. Negative symptoms in schizophrenia: newly emerging measurements, pathways, and treatments. Schizophr Res. 2023;258:71–12. doi:10.1016/j.schres.2023.07.010
3. Howes O, Fusar-Poli P, Osugo M. Treating negative symptoms of schizophrenia: current approaches and future perspectives. Br J Psychiatry J Ment Sci. 2023;223(1):332–335. doi:10.1192/bjp.2023.57
4. Lyne J, O’Donoghue B, Owens E, et al. Prevalence of item level negative symptoms in first episode psychosis diagnoses. Schizophr Res. 2012;135(1–3):128–133. doi:10.1016/j.schres.2012.01.004
5. Galderisi S, Mucci A, Dollfus S, et al. EPA guidance on assessment of negative symptoms in schizophrenia. Eur Psychiatry. 2021;64(1):e23. doi:10.1192/j.eurpsy.2021.11
6. Grace AA, Uliana DL. Insights into the mechanism of action of antipsychotic drugs derived from animal models: standard of care versus novel targets. Int J Mol Sci. 2023;24(15):12374. doi:10.3390/ijms241512374
7. De Hert M, Yu W, Detraux J, Sweers K, van Winkel R, Correll CU. Body weight and metabolic adverse effects of asenapine, iloperidone, lurasidone and paliperidone in the treatment of schizophrenia and bipolar disorder: a systematic review and exploratory meta-analysis. CNS Drugs. 2012;26(9):733–759. doi:10.2165/11634500-000000000-00000
8. Goldsmith DR, Haroon E, Miller AH, Strauss GP, Buckley PF, Miller BJ. TNF-α and IL-6 are associated with the deficit syndrome and negative symptoms in patients with chronic schizophrenia. Schizophr Res. 2018;199:281–284. doi:10.1016/j.schres.2018.02.048
9. Goldsmith DR, Haroon E, Miller AH, et al. Association of baseline inflammatory markers and the development of negative symptoms in individuals at clinical high risk for psychosis. Brain Behav Immun. 2019;76:268–274. doi:10.1016/j.bbi.2018.11.315
10. Perry BI, Zammit S, Jones PB, Khandaker GM. Childhood inflammatory markers and risks for psychosis and depression at age 24: examination of temporality and specificity of association in a population-based prospective birth cohort. Schizophr Res. 2021;230:69–76. doi:10.1016/j.schres.2021.02.008
11. Dunleavy C, Elsworthy RJ, Upthegrove R, Wood SJ, Aldred S. Inflammation in first-episode psychosis: the contribution of inflammatory biomarkers to the emergence of negative symptoms, a systematic review and meta-analysis. Acta Psychiatr Scand. 2022;146(1):6–20. doi:10.1111/acps.13416
12. Treadway MT, Cooper JA, Miller AH. Can’t or won’t? Immunometabolic constraints on dopaminergic drive. Trends Cognit Sci. 2019;23(5):435–448. doi:10.1016/j.tics.2019.03.003
13. Dr G, Mh R. Inflammation and negative symptoms of schizophrenia: implications for reward processing and motivational deficits. Front Psychiatry. 2020;11:46.
14. Nayak U, Manikkath J, Arora D, Mudgal J. Impact of neuroinflammation on brain glutamate and dopamine signalling in schizophrenia: an update. Metab Brain Dis. 2025;40(2):119. doi:10.1007/s11011-025-01548-3
15. Cui Y, Sun J, Zhang B, et al. Efficacy and safety of transcutaneous auricular vagus nerve stimulation for patients with treatment-resistant schizophrenia with predominantly negative symptoms: a randomized clinical trial and efficacy sensitivity biomarkers. Mol Psychiatry. 2025;30(11):5437–5447. doi:10.1038/s41380-025-03132-8
16. Sun JB, Tian QQ, Yang XJ, et al. Synergistic effects of simultaneous transcranial direct current stimulation (tDCS) and transcutaneous auricular vagus nerve stimulation (taVNS) on the brain responses. Brain Stimul. 2021;14(2):417–419. doi:10.1016/j.brs.2021.02.010
17. Li S, Zhang Z, Jiao Y, et al. An assessor-blinded, randomized comparative trial of transcutaneous auricular vagus nerve stimulation (taVNS) combined with cranial electroacupuncture vs. citalopram for depression with chronic pain. Front Psychiatry. 2022;13:902450. doi:10.3389/fpsyt.2022.902450
18. Li Q, Gong Y, Cui Y, et al. Efficacy of transcutaneous electrical acupoint stimulation for patients with first-episode schizophrenia: an 8-week, preliminary, randomized controlled trial. Psychiatry Res. 2023;325:115255. doi:10.1016/j.psychres.2023.115255
19. Chen WY, Li L, Wang HY, Jiang N. Effects of Transcutaneous Electrical Acupoint Stimulation for Depression in Late Pregnancy and Impacts on Inflammatory Cytokines. Zhen Ci Yan Jiu. 2018;43(1):44–48. doi:10.13702/j.1000-0607.160781
20. Js H. Acupuncture: neuropeptide release produced by electrical stimulation of different frequencies. Trends Neurosci. 2003;26(1):17–22.
21. L S, W Z, S Y, et al. A neuroanatomical basis for electroacupuncture to drive the vagal-adrenal axis. Nature. 2021;598(7882):641–645.
22. Marder SR, Alphs L, Anghelescu IG, et al. Issues and perspectives in designing clinical trials for negative symptoms in schizophrenia. Schizophr Res. 2013;150(2–3):328–333. doi:10.1016/j.schres.2013.07.058
23. Leucht S, Barabássy Á, Laszlovszky I, et al. Linking PANSS negative symptom scores with the Clinical Global Impressions Scale: understanding negative symptom scores in schizophrenia. Neuropsychopharmacology. 2019;44(9):1589–1596. doi:10.1038/s41386-019-0363-2
24. Addington D, Addington J, Schissel B. A depression rating scale for schizophrenics. Schizophr Res. 1990;3(4):247–251. doi:10.1016/0920-9964(90)90005-R
25. Rakel B, Cooper N, Adams HJ, et al. A new transient sham TENS device allows for investigator blinding while delivering a true placebo treatment. J Pain. 2010;11(3):230–238. doi:10.1016/j.jpain.2009.07.007
26. Marder SR, Daniel DG, Alphs L, Awad AG, Keefe RSE. Methodological issues in negative symptom trials. Schizophr Bull. 2011;37(2):251–254. doi:10.1093/schbul/sbq161
27. Hopkins SC, Ogirala A, Loebel A, Koblan KS. Understanding antipsychotic drug treatment effects: a novel method to reduce pseudospecificity of the Positive and Negative Syndrome Scale (PANSS) factors. Innov Clin Neurosci. 2017;14(11–12):54–58.
28. Mohr PE, Cheng CM, Claxton K, et al. The heterogeneity of schizophrenia in disease states. Schizophr Res. 2004;71(1):83–95. doi:10.1016/j.schres.2003.11.008
29. Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. 1987;13(2):261–276. doi:10.1093/schbul/13.2.261
30. Andreasen NC. Negative symptoms in schizophrenia. Definition and reliability. Arch Gen Psychiatry. 1982;39(7):784–788. doi:10.1001/archpsyc.1982.04290070020005
31. Busner J, Targum SD. The clinical global impressions scale: applying a research tool in clinical practice. Psychiatry. 2007;4(7):28–37.
32. Addington D, Addington J, Maticka-Tyndale E. Assessing depression in schizophrenia: the Calgary Depression Scale. Br J Psychiatry Suppl. 1993;22(S22):39–44. doi:10.1192/S0007125000292581
33. Leucht S, Samara M, Heres S, et al. Dose Equivalents for Second-Generation Antipsychotic Drugs: the Classical Mean Dose Method. Schizophr Bull. 2015;41(6):1397–1402. doi:10.1093/schbul/sbv037
34. H Y, C Y, B Y, T W. Cognitive-behavioral therapy for the improvement of negative symptoms and functioning in schizophrenia: a systematic review and meta-analysis of randomized controlled trials. PLoS One. 2025;20(5):e0324685.
35. Goldsmith DR, Rapaport MH, Miller BJ. A meta-analysis of blood cytokine network alterations in psychiatric patients: comparisons between schizophrenia, bipolar disorder and depression. Mol Psychiatry. 2016;21(12):1696–1709. doi:10.1038/mp.2016.3
36. Müller N. Inflammation in schizophrenia: pathogenetic aspects and therapeutic considerations. Schizophr Bull. 2018;44(5):973–982. doi:10.1093/schbul/sby024
37. H X, H B, C J. Peripheral inflammation and blood-brain barrier disruption: effects and mechanisms. CNS Neurosci Ther. 2021;27(1):36–47.
38. Kempuraj D, Thangavel R, Selvakumar GP, et al. Brain and Peripheral Atypical Inflammatory Mediators Potentiate Neuroinflammation and Neurodegeneration. Front Cell Neurosci. 2017;11:216. doi:10.3389/fncel.2017.00216
39. Warwick CA, Keyes AL, Woodruff TM, Usachev YM. The complement cascade in the regulation of neuroinflammation, nociceptive sensitization, and pain. J Biol Chem. 2021;297(3):101085. doi:10.1016/j.jbc.2021.101085
40. Howes OD, McCutcheon R. Inflammation and the neural diathesis-stress hypothesis of schizophrenia: a reconceptualization. Transl Psychiatry. 2017;7(2):e1024. doi:10.1038/tp.2016.278
41. Rong P, Liu J, Wang L, et al. Effect of transcutaneous auricular vagus nerve stimulation on major depressive disorder: a nonrandomized controlled pilot study. J Affect Disord. 2016;195:172–179. doi:10.1016/j.jad.2016.02.031
42. Borovikova LV, Ivanova S, Zhang M, et al. Vagus nerve stimulation attenuates the systemic inflammatory response to endotoxin. Nature. 2000;405(6785):458–462. doi:10.1038/35013070
43. Andersson U, Tracey KJ. Neural reflexes in inflammation and immunity. J Exp Med. 2012;209(6):1057–1068. doi:10.1084/jem.20120571
44. Li L, Liu Z, Jiang YY, Shen WX, Peng YP, Qiu YH. Acetylcholine suppresses microglial inflammatory response via α7nAChR to protect hippocampal neurons. J Integr Neurosci. 2019;18(1):51–56. doi:10.31083/j.jin.2019.01.114
45. Yildiz M, Kozanhan B. Transcutaneous electric acupoint stimulation reduces rocuronium injection-related pain: a prospective randomized controlled study. Eur Rev Med Pharmacol Sci. 2022;26(17):6215–6220. doi:10.26355/eurrev_202209_29639
46. Torres-Rosas R, G Yehia, G Peña, et al. Dopamine mediates vagal modulation of the immune system by electroacupuncture. Nat Med. 2014;20(3):291–295.
47. Wu X, Hu R, Jiang S, et al. Electroacupuncture attenuates LPS-induced depression-like behavior through kynurenine pathway. Front Behav Neurosci. 2022;16:1052032. doi:10.3389/fnbeh.2022.1052032
48. Cao F, Xu Y, Zhang M, et al. Baihui (DU20), shenmen (HT7) and sanyinjiao (SP6) target the cAMP/CREB/BDNF and PI3K/akt pathways to reduce central nervous system apoptosis in rats with insomnia. Heliyon. 2022;8(12):e12574. doi:10.1016/j.heliyon.2022.e12574
49. Zhao W, Zou W. Effects of electroacupuncture on postoperative cognitive dysfunction and its underlying mechanisms: a literature review of rodent studies. Front Aging Neurosci. 2024;16:1384075. doi:10.3389/fnagi.2024.1384075
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Predictive Role of Aberrant Metabolic Parameters and Negative Automatic Thinking on the Cognitive Impairments Among Schizophrenia Patients with Metabolic Syndrome
Zhang X, He C, Ju P, Xia Q, Gao J, Zhang L, Chen X, Yuan H, Gao H, Zhang Y, Yan J, Xie W, Zhu C
Neuropsychiatric Disease and Treatment 2022, 18:1087-1097
Published Date: 7 June 2022
Automatic Thoughts, Self-Stigma, and Resilience Among Schizophrenia Patients with Metabolic Syndrome: A Cross-Sectional Study
Ma S, Ju P, Xia Q, Pan Z, Gao J, Zhang L, Gao H, Yan J, Zhang J, Wang K, Li C, Xie W, Zhu C
Neuropsychiatric Disease and Treatment 2023, 19:1195-1206
Published Date: 17 May 2023
Systematic Literature Review of Studies Reporting Measures of Functional Outcome or Quality of Life in People with Negative Symptoms of Schizophrenia
Hadzi Boskovic D, Smith-Palmer J, Pöhlmann J, Pollock RF, Hwang S, Bruhn D
Patient Related Outcome Measures 2024, 15:199-217
Published Date: 17 June 2024
A Clinically Oriented Review of New Antipsychotics for Schizophrenia
Luca M, Luca A, Serretti A
Neuropsychiatric Disease and Treatment 2024, 20:2637-2649
Published Date: 27 December 2024
Factors Affecting Negative Symptoms in Schizophrenia and Their Relationship with Anxiety and Depression
Zeng G, Liang R, Xiao L, Cao W, Zhou W, Wang W, Liu C, Zhou H, Shi X, Chen B, Chen W
Neuropsychiatric Disease and Treatment 2025, 21:229-240
Published Date: 4 February 2025