Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Effects of Intraparietal Gastric Botulinum Toxin-A Injection on Weight Loss: A Retrospective Study of 500 Patients
Authors Bekin A ![]() , Sahutoglu T, Atay K
, Sahutoglu T, Atay K ![]()
Received 1 January 2025
Accepted for publication 22 September 2025
Published 4 October 2025 Volume 2025:18 Pages 3771—3779
DOI https://doi.org/10.2147/DMSO.S515242
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Liang Wang
Ahmet Bekin,1 Tuncay Sahutoglu,2 Kadri Atay3
1Dr.Nazif Bagricak Kadikoy Hospital, Department of General Surgery, Istanbul, Turkiye; 2Mehmet Akif Inan Research and Training Hospital, Department of Internal Medicine and Nephrology, Sanlıurfa, Turkiye; 3Mardin Research and Training Hospital, Department of Gastroenterology, Mardin, Turkiye
Correspondence: Kadri Atay, Mardin Research and Training Hospital, Department of Gastroenterology, Mardin, Turkiye, Email [email protected]
Introduction: Obesity is a serious and widespread health concern, and while there is no universally effective pharmacological treatment, endoscopic applications such as intraparietal gastric botulinum toxin-A injection have shown promise. This study aimed to investigate the effects of intragastric botulinum toxin-A injection on weight loss and to evaluate the ratio of weight loss achieved.
Methods: This was a retrospective cohort study conducted between 2020– 2022. 500 patients were included in this study who had undergone gastric botulinum toxin-A application and completed at least 6 months of regular follow-up. Patients were injected intramuscularly with 1000 U of botulinum toxin-A in the antrum and fundus regions of the stomach via endoscopy under sedation anesthesia (midazolam and propofol). Patients were monitored for 2 hours after the procedure and were then discharged. A low-calorie diet and active life support were provided under the guidance of a dietician for 6 months after the procedure.
Results: At the end of the third and sixth months, all subjects lost body weight, with mean weight loss of 10.54 ± 3.36 kg (13.9 ± 4.4%) (Group 1), 13.54 ± 4.57 kg (15.1 ± 4.9%) (Group 2), 16.76 ± 3.86 kg (16.0 ± 3.6%) (Group 3), and 20.6 ± 5.33 kg (16.4 ± 4.2%) (Group 4) at the third month; and 14.50 ± 4.95 kg (19.2 ± 6.6%) (Group 1), 18.39 ± 6.49 kg (20.5 ± 7.0%) (Group 2), 23.37 ± 5.51 kg (22.4 ± 5.2%) (Group 3), and 29.17 ± 7.96 kg (23.2 ± 6.3%) (Group 4) at the sixth month, respectively. The differences between the third and sixth months were statistically significant (p < 0.05). The body mass index values of the patients also showed significant reductions at the end of the third and sixth months (p < 0.05). These results were statistically significant and reflect the primary outcome of the study.
Conclusion: Intraparietal gastric botulinum toxin-A injection can lead to significant weight loss and may contribute to the development of effective, minimally invasive approaches for the management of obesity. Further studies with larger sample sizes and longer follow-up periods are needed to confirm these findings.
Keywords: body mass index, botulinum toxin-A injection, intraparietal gastric botulinum toxin-A, obesity, weight loss
Introduction
Obesity is a serious and widespread health concern with far-reaching consequences, including an increased risk of several diseases such as diabetes, coronary artery disease, hypertension, hyperlipidemia, sleep apnea syndrome, and cerebral stroke.1 According to the World Health Organization, obesity is one of the most pressing global health challenges, contributing to significant morbidity and mortality worldwide. The prevalence of obesity has been increasing steadily, with almost 40% of adults worldwide now considered overweight.2 While genetic, social, psychological, and behavioral factors all contribute to obesity, the underlying mechanisms are complex and multifaceted.2 Botulinum toxin, derived from the bacterium Clostridium botulinum, is a potent inhibitor of muscle contraction that works by blocking the release of acetylcholine in the neuromuscular area.3,4 Botulinum toxin type A (BTX-A) has been used successfully to treat a range of muscle contraction disorders, including strabismus, dystonia, and tremors.5,6 It has also been used to treat achalasia, a disorder of esophageal motility in the gastrointestinal tract.7 Recent research has shown that injecting BTX-A into the stomach can slow gastric motility and delay gastric emptying, leading to increased feelings of satiety and potentially resulting in weight loss.8 BTX-A inhibits acetylcholine release at neuromuscular junctions, resulting in temporary paralysis of targeted gastric smooth muscles. When injected into the antrum and/or fundus, this can slow gastric emptying and increase the sensation of fullness, thereby reducing caloric intake.9 There is currently no universally effective pharmacological treatment for obesity. Surgical interventions, while effective, carry risks such as nutritional deficiencies and other long-term complications.10 As a result, endoscopic applications, including intraparietal gastric Btx-A injection, have become an area of active research. The conflicting results in previous studies may be attributed to variations in sample size, BTX-A dose, injection site, and methodological differences in study design. In this study, we aimed to investigate the effects of intraparietal gastric Btx-A injection on weight loss in a patient population and to evaluate the ratio of weight loss achieved.
Methods
Patient Selection and Ethical Considerations
Between 2020–2022, a total of 500 patients were included in this study, who had undergone gastric Btx-A application and completed at least 6 months of regular follow-up. Ethics committee approval was received for this study from Dr.Nazif Bağrıcak Kadıköy Hospital Ethics Committee (Approval No: 2020/045). Informed consent was obtained from all participants. This study was conducted in accordance with the principles of the Declaration of Helsinki. The inclusion criteria for the study were patients who could not effectively lose weight despite undergoing diet and exercise programs. The endoscopic procedure was performed on all patients using the same technique. Under sedation anesthesia, patients underwent endoscopy in the endoscopy unit. Sedation was achieved using intravenous midazolam (2.5–5 mg) and propofol (50–100 mg) administered under anesthesiologist supervision. A total of 1000 U of BTX-A (Dysport®, Ipsen Biopharm Ltd., Wrexham, United Kingdom) was diluted with 8 mL of 0.9% NaCl saline. The antrum region was injected intramuscularly with 750 U to 30 spots, and the fundus region was injected intramuscularly with 250 U to 10 spots, with 1 mL at each spot using a sclerotherapy needle (Boston Scientific 23-G 5 mm; Interject™, Boston Scientific, Marlborough, MA, USA). Starting from the pyloric region, patients were injected at 40 regions in the stomach. The same injection map was used in all patients. Patients were monitored for 2 hours after the procedure and were then discharged.
Follow-up and Inclusion-Exclusion Criteria
The low-calorie diet was personalized according to basal metabolic rate (calculated using the Harris–Benedict formula) with a target of 500–1000 kcal/day deficit. Macronutrient distribution was balanced (45% carbohydrate, 30% fat, 25% protein). Adherence to the standardized post-procedure low-calorie diet and physical activity recommendations was monitored through monthly in-person follow-up visits and direct interviews with the dietician. Patients were asked to self-report their daily food intake and physical activity patterns, and these reports were reviewed during each visit. In the 6th month, patients were evaluated in terms of appetite and feelings of satiety after meals. This was a retrospective cohort study conducted between 2020–2022. Patient data were recorded and analyzed retrospectively.
Inclusion Criteria
Patients aged 18–65 years who:
- Had no history of bariatric or major gastrointestinal surgery.
- Had failed to lose ≥5% of their baseline body weight despite at least 6 months of supervised diet and exercise programs.
- Had no prior medical or herbal weight-loss treatment in the past 3 months.
Exclusion Criteria
Patients were excluded if they had:
- Chronic, endocrine, or autoimmune diseases.
- Pathologies of the esophagus, stomach, or duodenum confirmed by endoscopy.
- Regular use of medications affecting weight or appetite.
- Pregnancy.
- Metabolic diseases preventing weight loss.
- History of gastrointestinal malignancy or alcohol abuse.
- Participation in any diet or medical/herbal weight-loss program within the past 3 months.
Failure to lose weight was defined as losing less than 10% of baseline body weight at the end of the 6-month follow-up period, despite undergoing the standardized post-procedure diet and activity program.
The primary outcome parameters were changes in body weight, BMI, and subjective appetite levels. For subgroup analysis, patients were divided into four groups based on baseline BMI:Group 1: <30 kg/m², Group 2: 30–34.9 kg/m², Group 3: 35–39.9 kg/m², and Group 4: ≥40 kg/m². Physical activity status was also recorded, and patients were stratified into two groups based on whether they reported regular exercise during the 6-month follow-up. Patients were followed clinically at 1st, 3rd, and 6th months, and instructed to report any gastrointestinal symptoms. Routine follow-up endoscopy was not performed unless symptoms such as epigastric pain, nausea, or vomiting occurred.
Statistical Analyses
Statistical analyses were performed using JASP version 0.17.1. The Shapiro–Wilk test was used to assess normality, and Levene’s test was applied to evaluate the homogeneity of variances. For normally distributed data, means and standard deviations (SD) were reported; for non-normally distributed data, medians and interquartile ranges (IQR) were presented. Comparisons between two independent groups (eg, diet vs non-diet) were made using the independent samples t-test for parametric data and the Mann–Whitney U-test for non-parametric data. Comparisons among more than two groups (eg, BMI-based subgroups) were performed using one-way ANOVA for normally distributed variables or the Kruskal–Wallis test for non-normally distributed variables. When ANOVA or Kruskal–Wallis tests indicated statistical significance, Bonferroni or Dunn’s post hoc tests were applied to adjust for multiple comparisons. For categorical variables, results were expressed as frequencies and percentages, and comparisons were made using the Chi-square test or Fisher’s exact test as appropriate. A post-hoc power calculation indicated that a sample size of 500 provided >90% power to detect between-group differences of ≥3% in weight loss at α = 0.05. A p-value of <0.05 was considered statistically significant.
Results
The study involved the application of gastric botulinum toxin-A (Btx-A) to 500 patients, comprising 413 females (82.6%) and 87 males (17.4%), with a mean age of 37.93 ± 10.11 years and a mean BMI of 34.59 ± 6.09 kg/m2. The initial weight and height of patients were 95.99 ± 19.29 kg and 166.23 ± 7.88 cm, respectively (Table 1).
 |
Table 1 Baseline Characteristics of the Study Population (n = 500) |
 |
Table 2 Weight Loss and BMI Reduction Data in Subgroups at the 3rd and 6th months After Intragastric Injection of Botulinum Toxin Type-A |
Tables 1–3 presented baseline BMI, baseline body weight, percentage of weight loss at the third- and sixth months following treatment, and weight and BMI at the end of the sixth month for all patients. At the end of the third and sixth months, all subjects lost body weight, with mean weight loss ratios of 13.9 ± 4.4%, 15.1 ± 4.9%, 16% ± 3.6% and 16.4 ±4.2 at the third month, and 19.2 ± 6.6%, 20.5 ± 7.0%, 22.4 ± 5.2%, and 23.2 ± 6.3% at the sixth month for Groups 1, 2, 3, and 4, respectively.
 |
Table 3 Mean Weight and BMI Reduction 6th Months Post Botox Treatment in All Patients (n = 500) |
At the end of the sixth month, 319 (63.8%) of patients exercised regularly, while 281 (36.2%) did not. The proportion of patients who exercised regularly and lost weight in six months was significantly higher than those who did not exercise regularly (P = 0.05) (Table 4). Among patients who underwent a diet program, 433 (86.6%) did so regularly, while 67 did not. The mean weight and BMI reduction for six months post-Btx treatment in patients undergoing regular diet were significantly higher than those who did not undergo a regular diet program (Table 5). (P = 0.001 and 0.02, respectively).
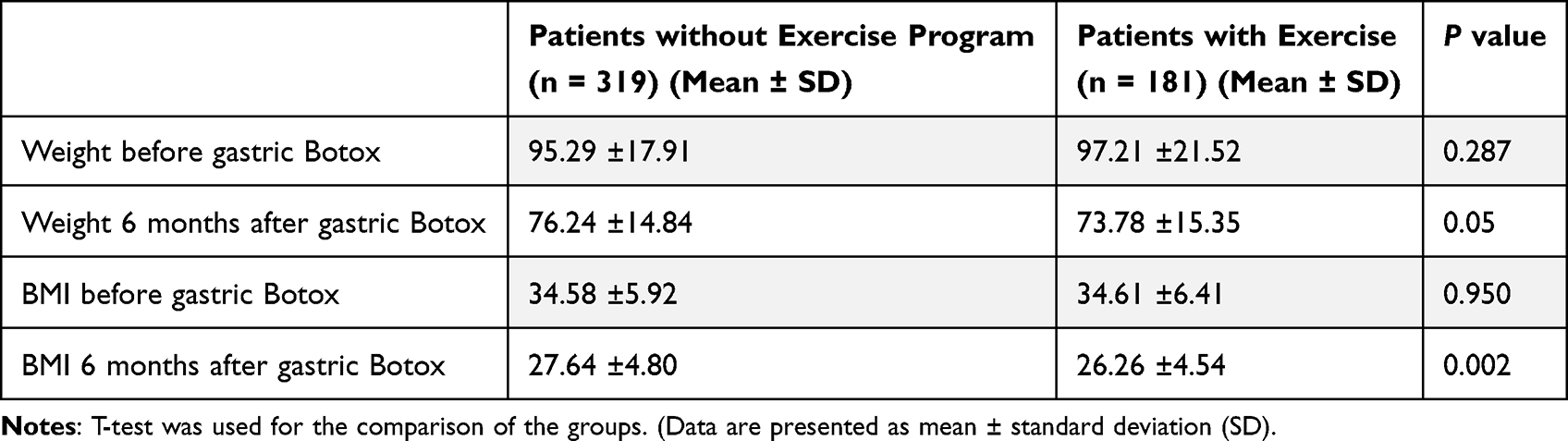 |
Table 4 Mean Weight and BMI Reduction for Patients with and without Exercise. Patients with Exercise Program (n = 181), Patients without Exercise (n = 319) |
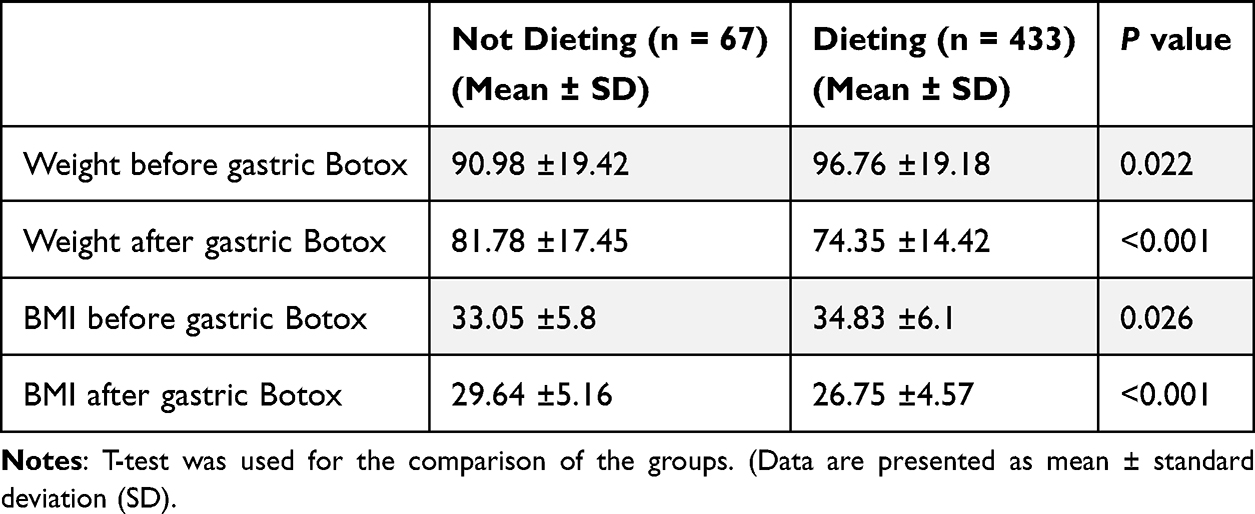 |
Table 5 Mean Weight and BMI Reduction 6th Months Post Botox Treatment for Patients Undergoing Diet vs Those Not Following a Diet (Dieting Group: n = 433, Non-Dieting Group: n = 67) |
The mean BMI and weight were significantly different from the baseline values at the end of the third and sixth months for Groups 1, 2, 3, and 4. Mean body weight loss percentages were significantly higher in Groups 3 and 4 when compared to Groups 1 and 2 at the second, third, and sixth-month time points. There was a decreasing trend in body weight until the end of the third and sixth months for all subjects. Nearly all subjects reported feeling early satiety in follow-up visits.
At the end of the six-month follow-up, the weight of patients decreased by a mean of 20.6 kg after Btx application (P = 0.001). When this comparison was made in terms of BMI, a mean decrease of 7.49 kg/m2 was detected in patients after six months (P = 0.001). Of the patients, 447 (94.8%) stated that their appetite decreased, and they felt satiated for six months, while the remaining 53 (5.2%) patients stated that there was no change in their appetite and duration of satiety (Table 3).
Out of the 500 patients who received gastric Btx-A treatment, 38 patients (7.6%) lost less than 10% of their body weight, which was considered an unsuccessful treatment. On the other hand, 462 patients (92.4%) lost more than 10% of their body weight, which was considered a successful treatment (P = 0.001). No acute side effects were observed immediately following the endoscopic procedure. However, eight patients reported experiencing nausea and vomiting, 23 patients experienced abdominal cramps, and 55 patients experienced constipation during the follow-up period. No serious adverse events or procedure-related mortality occurred (Table 6).
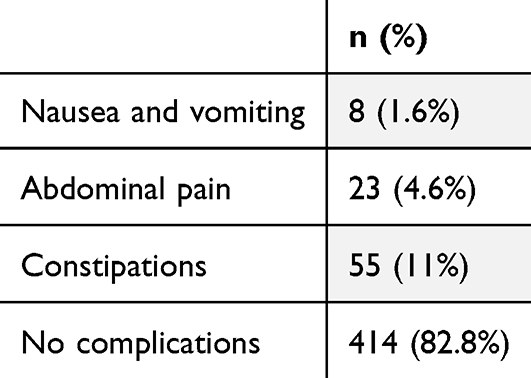 |
Table 6 Complications Following Endoscopic Procedures in Patients (n = 500) |
Discussion
In this study, we investigated the effectiveness of intraparietal gastric Botox application in obese patient groups. According to our study results, we found that 92.4% of our patients had a weight loss of more than 10% after intraparietal gastric botox application, which we considered a success. In the subgroup analysis of our patient groups, we observed significantly higher weight loss rates in patients who adhered to diet and exercise programs. Additionally, we found that 94.8% of our patient population had a decrease in appetite as one of the goals of the Botox treatment.
Botulinum toxin is now being used safely in almost all medical specialties, especially in the field of aesthetics.11 Gastric BTX-A reduces acetylcholine-mediated smooth muscle contractions in the antrum/pylorus, slows gastric motility and emptying, and increases postprandial satiation, thereby lowering caloric intake. Randomized data show BTX-A can delay gastric emptying, although weight-loss efficacy has been inconsistent across trials.9 The physiological effect of gastric BTX-A depends on the injection site: intramural injections into the antrum and/or fundus can reduce antral contractility and delay gastric emptying, thereby increasing satiation, whereas intrapyloric injections are intended to relax the pyloric sphincter and may facilitate gastric emptying in selected contexts; randomized human data on pyloric injection remain mixed.9 Accordingly, our protocol targeted the antrum and fundus rather than the pylorus.
The increasing prevalence of obesity and related complications, including mortality and morbidity, has made it imperative to find new treatment options for obesity. Endoscopic BTX-A therapy may be a suitable option for obese patients who are either not eligible for bariatric surgery due to high surgical risk, or who wish to lose weight prior to undergoing bariatric surgery, given its potential reversibility and low intraoperative and postoperative risks. It also helps to lose weight before surgery and control additional diseases such as type 2 diabetes, dyslipidemia, and hepatic steatosis, reducing the risks that may occur post surgery.12–15
There are conflicting results in the literature regarding the use of intraparietal gastric Btx-A injection in the treatment of obesity. A randomized controlled trial conducted by Park et al, which is one of the studies that demonstrated the effectiveness of Btx, clearly showed that gastric Btx-A injections are effective in reducing body weight and preventing gastric emptying. It was shown that body weight in the Btx-A group decreased significantly compared to the saline and control groups.16 In another study by Rollnik et al, patients showed a significant decrease in food intake and an average weight loss of 9 kg during a 4-month follow-up period after endoscopic intraparietal gastric Botox injection.17 In contrast, Bustamante et al conducted a meta-analysis of randomized clinical trials and concluded that BTX-A was not superior to placebo in achieving significant weight loss.18 Likewise, Topazian et al found that although antral BTX-A injections delayed gastric emptying, they did not result in a significant reduction in body weight compared to placebo.9 These discrepancies may be related to variations in patient selection, injection sites, dosages, and concurrent dietary interventions across studies. In our study, we observed a significant decrease in weight and BMI indices in our patients compared to their initial weights, which is consistent with the studies conducted by Park and Rollnik in the literature. Based on our results, we believe that gastric Botox application is effective in weight loss for obese patients.
In humans, lifestyle caloric restriction typically yields 5–10% total body weight loss (TBWL) by 6 months, with variable longer-term maintenance.19 By contrast, evidence from randomized and meta-analytic studies for intragastric BTX-A is mixed: several RCTs show no superiority over placebo, while some protocols (antrum+fundus, higher dose/multi-site) report signals of benefit.20
Metabolic/bariatric surgery provides the largest and most durable weight loss: contemporary guidelines and cohorts report ≈22–26% TBWL at 5 years for sleeve gastrectomy/Roux-en-Y, and >60% excess weight loss maintained long-term.21 Various publications demonstrate that Btx-A injected into the antrum and fundus of the stomach slows gastric emptying and changes gastric motility, leading to weight loss. Furthermore, studies on both animals and humans have shown that Btx-A injections into the stomach wall decrease food intake and body weight.22–28
Studies examining the effect of Btx-A injection at different doses on gastric emptying are available.9,29,30 Topazian et al compared the effects of different doses of Btx-A injection on gastric antral muscularis propria and found that low doses were not associated with early satiety, changes in eating behavior, or weight loss, but higher doses (300 units) resulted in delayed gastric emptying.9 Similarly, Gracis et al suggested that the effect of Btx-A on the stomach could be related to the width and number of areas injected into the organ.31 The dose and distribution of BTX-A within the stomach may represent critical determinants of treatment efficacy. Notably, we found no published data on weight-adjusted dosing of gastric BTX-A, and dose calculation based on body weight is also uncommon in other therapeutic indications of BTX-A. In our study, all patients received a relatively high total dose of 1000 units, distributed across an extensive treatment area involving 40 intramuscular injection sites in the antrum and fundus. We hypothesize that this combination of higher dose and broader gastric coverage contributed to the greater weight loss observed in our cohort. Importantly, patients also reported a marked decrease in hunger and an increase in satiety, which may further support the potential value of optimized dosing and application area in enhancing clinical outcomes.
In other clinical applications, such as pharyngeal swallowing disorders, botulinum toxin typically has a limited duration of action, often requiring repeat injections within 3–4 months.32 In our cohort, sustained weight loss and appetite reduction were observed up to 6 months without re-injection. We hypothesize that this prolonged effect may be due to the higher total dose administered (1000 U Dysport®), the extensive injection mapping covering both the antrum (30 sites) and fundus (10 sites), and the combined implementation of a low-calorie diet. These differences suggest that both the injection protocol and adjunctive lifestyle interventions may influence the duration of clinical benefit.
Although a wide range of side effects such as fatigue, headache, and gastrointestinal symptoms have been reported after Btx-A injection,33 we observed gastrointestinal symptoms such as nausea and vomiting in 8 patients (1.6%), abdominal pain in 23 (4.6%), and constipation in 55 (11%) of our patients in our study. Overall, no side effects were observed in 82.8% of our patients. Based on these results, we can say that intraparietal gastric Botox injection is a reliable method for treating obesity.
Diet is one of the most important issues in weight loss during obesity treatment.34 In our study, all our patients were enrolled in a low-calorie diet program after the procedure. We found a statistically significant difference in weight loss between patients who followed the diet and those who did not (P < 0.01). The importance of appetite decrease in weight loss is well known. One of the most interesting aspects of this study was the effect of Botox on appetite. After intraparietal gastric Botox treatment, 447 out of 500 patients (94.8%) reported a decrease in appetite.
What sets our study apart from previous ones on intraparietal gastric BTX-A injection is that most prior studies were conducted with small sample sizes, typically ranging from 13 to 24 patients,17,35 whereas our study represents one of the largest case series in the literature, including 500 patients.
Our study has some limitations, including the absence of a placebo group, the relatively short follow-up period of six months, and the inability to monitor ghrelin levels in patients who received gastric Btx-A injection. However, our results suggest that gastric Btx-A injection is significantly effective for obese patients and may be a promising option for those who cannot undergo surgery. Therefore, further prospective, placebo-controlled studies with longer follow-up periods should be conducted to assess the long-term effectiveness and safety of gastric Btx-A injection therapy.
In conclusion, our study supports the effectiveness and safety of intraparietal gastric Botox injection for weight loss in obese patients. Further studies are needed to establish optimal dosing strategies and to identify the patient population that would benefit the most from this treatment.
Abbreviations
BTX-A, Botulinum Toxin-A; BMI, Body Mass Index.
Disclosure
Tuncay Sahutoglu has received speaker honorariums from AstraZeneca, Amgen, Sanofi, Nobel Ilac, Baxter, Boehringer Ingelheim, Abdi Ibrahim-Otsuka, Alexion, and Astellas none of which are associated with this work. The authors report no other conflicts of interest in this work.
References
1. Mokdad AH, Serdula MK, Dietz WH, Bowman BA, Marks JS, Koplan JP. The spread of the obesity epidemic in the United States, 1991–1998. JAMA. 1999;282(16):1519–1522. doi:10.1001/jama.282.16.1519
2. World Health Organization. Obesity and overweight: key facts. World Health Organization. Available from: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
3. DasGupta BR. Structure and biological activity of botulinum neurotoxin. J Physiol. 1990;84(3):220–228.
4. Montecucco C. Clostridial Neurotoxins: The Molecular Pathogenesis of Tetanus and Botulism. Vol 195. Current Topics in Microbiology and Immunology. Springer; 1995.
5. Jankovic J, Brin MF. Therapeutic uses of botulinum toxin. N Engl J Med. 1991;324(17):1186–1194. doi:10.1056/NEJM199104253241707
6. Jankovic J, Hallett M. Therapy with Botulinum Toxin.
7. Pasricha PJ, Ravich WJ, Hendrix TR, Sostre S, Jones B, Kalloo AN. Intrasphincteric botulinum toxin for the treatment of achalasia. N Engl J Med. 1995;332(12):774–778. doi:10.1056/NEJM199503233321203
8. James AN, Ryan JP, Parkman HP. Inhibitory effects of botulinum toxin on pyloric and antral smooth muscle. Am J Physiol Gastrointest Liver Physiol. 2003;285(2):G291–7. doi:10.1152/ajpgi.00296.2002
9. Topazian M, Camilleri M, Enders FT, et al. Gastric antral injections of botulinum toxin delay gastric emptying but do not reduce body weight. Clin Gastroenterol Hepatol. 2013;11(2):145–50e1. doi:10.1016/j.cgh.2012.09.029
10. Swidnicka-Siergiejko A, Wroblewski E, Andrzej D. Endoscopic treatment of obesity. Can J Gastroenterol. 2011;25(11):627–633. doi:10.1155/2011/174163
11. Bach K, Simman R. The multispecialty toxin: a literature review of botulinum toxin. Plast Reconstr Surg Glob Open. 2022;10(4):e4228. doi:10.1097/GOX.0000000000004228
12. Madruga-Neto AC, Bernardo WM, de Moura DTH, et al. The effectiveness of endoscopic gastroplasty for obesity treatment according to FDA thresholds: systematic review and meta-analysis based on randomized controlled trials. Obes Surg. 2018;28(9):2932–2940. doi:10.1007/s11695-018-3335-4
13. Forlano R, Ippolito AM, Iacobellis A, et al. Effect of the BioEnterics intragastric balloon on weight, insulin resistance, and liver steatosis in obese patients. Gastrointest Endosc. 2010;71(6):927–933. doi:10.1016/j.gie.2009.06.036
14. Herve J, Wahlen CH, Schaeken A, et al. What becomes of patients one year after the intragastric balloon has been removed? Obes Surg. 2005;15(6):864–870. doi:10.1381/0960892054222894
15. de Moura EG, Martins BC, Lopes GS, et al. Metabolic improvements in obese type 2 diabetes subjects implanted for 1 year with an endoscopically deployed duodenal-jejunal bypass liner. Diabetes Technol Ther. 2012;14(2):183–189. doi:10.1089/dia.2011.0152
16. Park JS, Zheng HM, Kim JM, Kim CS, Jeong S, Lee DH. The effect of intragastric administration of botulinum toxin type A on reducing adiposity in a rat model of obesity using micro-CT and histological examinations. Gut Liver. 2017;11(6):798–806. doi:10.5009/gnl16557
17. Rollnik JD, Meier PN, Manns MP, Goke M. Antral injections of botulinum a toxin for the treatment of obesity. Ann Intern Med. 2003;138(4):359–360. doi:10.7326/0003-4819-138-4-200302180-00026
18. Bustamante F, Brunaldi VO, Bernardo WM, et al. Obesity treatment with botulinum toxin-A is not effective: a systematic review and meta-analysis. Obes Surg. 2017;27(10):2716–2723. doi:10.1007/s11695-017-2857-5
19. Chao AM, Paul A, Hodgkins JV, Wadden TA. A guideline-directed approach to obesity treatment. Diabetes Spectr. 2024;37(4):281–295. doi:10.2337/dsi24-0001
20. Arabpour E, Golmoradi H, Tape PMK, et al. Intragastric botulinum toxin injection for weight loss: current trends, shortcomings and future perspective. Clin Endosc. 2025;58(1):10–24. doi:10.5946/ce.2024.153
21. Biter LU, t Hart JW, Noordman BJ, et al. Long-term effect of sleeve gastrectomy vs Roux-en-Y gastric bypass in people living with severe obesity: a Phase III multicentre randomised controlled trial (SleeveBypass). Lancet Reg Health Eur. 2024;38:100836. doi:10.1016/j.lanepe.2024.100836
22. Gui D, De Gaetano A, Spada PL, Viggiano A, Cassetta E, Albanese A. Botulinum toxin injected in the gastric wall reduces body weight and food intake in rats. Aliment Pharmacol Ther. 2000;14(6):829–834. doi:10.1046/j.1365-2036.2000.00765.x
23. Coskun H, Duran Y, Dilege E, Mihmanli M, Seymen H, Demirkol MO. Effect on gastric emptying and weight reduction of botulinum toxin-A injection into the gastric antral layer: an experimental study in the obese rat model. Obes Surg. 2005;15(8):1137–1143. doi:10.1381/0960892055002275
24. Foschi D, Lazzaroni M, Sangaletti O, Corsi F, Trabucchi E, Bianchi Porro G. Effects of intramural administration of botulinum toxin A on gastric emptying and eating capacity in obese patients. Dig Liver Dis. 2008;40(8):667–672. doi:10.1016/j.dld.2008.02.040
25. Antakyalioglu B, Ozturan YA, Parlatir Y, Akin I, Ural K. Intragastric botulinum toxin-A injection: a novel approach to successfully manage feline obesity as an alternative technique to conventional treatment. Vet Rec Case Rep. 2024;13(1):e1030. doi:10.1002/vrc2.1030
26. Elshakh H, El-Ejji K, Taheri S. The role of endoscopic intra-gastric botulinum toxin-A for obesity treatment. Obes Surg. 2017;27(9):2471–2478. doi:10.1007/s11695-017-2806-3
27. Pirazzini M, Rossetto O, Eleopra R, Montecucco C. Botulinum neurotoxins: biology, pharmacology, and toxicology. Pharmacol Rev. 2017;69(2):200–235. doi:10.1124/pr.116.012658
28. Choi HS, Chun HJ. Recent trends in endoscopic bariatric therapies. Clin Endosc. 2017;50(1):11–16. doi:10.5946/ce.2017.007
29. Garcia-Compean D, Mendoza-Fuerte E, Martinez JA, Villarreal I, Maldonado H. Endoscopic injection of botulinum toxin in the gastric antrum for the treatment of obesity. Results of a pilot study. Gastroenterol Clin Biol. 2005;29(8–9):789–791. doi:10.1016/s0399-8320(05)86349-3
30. Junior AC, Savassi-Rocha PR, Coelho LG, et al. Botulinum A toxin injected into the gastric wall for the treatment of class III obesity: a pilot study. Obes Surg. 2006;16(3):335–343. doi:10.1381/096089206776116408
31. Gracies JM, Simpson DM. Botulinum toxin therapy. Neurologist. 2000;6:98–100.
32. Restivo DA, Casabona A, Nicotra A, et al. ALS dysphagia pathophysiology: differential botulinum toxin response. Neurology. 2013;80(7):616–620. doi:10.1212/WNL.0b013e318281cc1b
33. Ahmad SS, Sherpa G, Ahmed AR, Ahmad S. Intragastric botolinum toxin-A injection as a treatment for obesity in comparison to gastric balloon. Obes Surg. 2016;26(9):2235–2236. doi:10.1007/s11695-016-2305-y
34. World Health Organization. Obesity: preventing and managing the global epidemic. vol 894. WHO technical report series. World Health Organization; 2022.
35. Topazian M, Camilleri M, De La Mora-Levy J, et al. Endoscopic ultrasound-guided gastric botulinum toxin injections in obese subjects: a pilot study. Obes Surg. 2008;18(4):401–407. doi:10.1007/s11695-008-9442-x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Microbiome-Targeted Therapies as an Adjunct to Traditional Weight Loss Interventions: A Systematic Review and Meta-Analysis
Peckmezian T, Garcia-Larsen V, Wilkins K, Mosli RH, BinDhim NF, John GK, Yasir M, Azhar EI, Mullin GE, Alqahtani SA
Diabetes, Metabolic Syndrome and Obesity 2022, 15:3777-3798
Published Date: 11 December 2022
Clinical Insight on Semaglutide for Chronic Weight Management in Adults: Patient Selection and Special Considerations
Chao AM, Tronieri JS, Amaro A, Wadden TA
Drug Design, Development and Therapy 2022, 16:4449-4461
Published Date: 29 December 2022
Baseline Serum BCAAs are Related to the Improvement in Insulin Resistance in Obese People After a Weight Loss Intervention
Zhang C, Wang S, Wu Y, Guo Y, Wang X
Diabetes, Metabolic Syndrome and Obesity 2023, 16:179-186
Published Date: 19 January 2023
Effect of Weight Loss on the Apnea Hypopnea Index is Related to Waist Circumference in Chinese Adults with Overweight and Obesity
Ren Y, Cui X, Zhu X, Guo H, Zhou Q, Yuan P, Cheng H, Wu W
Diabetes, Metabolic Syndrome and Obesity 2024, 17:453-463
Published Date: 27 January 2024
Assessing the Impact of Bariatric Surgery on Quality of Life in the Saudi Population: A Systematic Review
Alqhtani H
Diabetes, Metabolic Syndrome and Obesity 2026, 19:572545
Published Date: 13 February 2026