Back to Journals » Drug Design, Development and Therapy » Volume 19
Effects of Esketamine-Dexmedetomidine Combination on Immediate Postprocedural Oxygenation Index in Severe Pneumonia Patients Undergoing Bedside Fiberoptic Bronchoscopic Sputum Aspiration: A Prospective Randomised Controlled Trial
Authors Wang Y, Zhang R, Wu B, Han J, Li Y, Zhang L
Received 5 August 2025
Accepted for publication 21 November 2025
Published 4 December 2025 Volume 2025:19 Pages 10751—10764
DOI https://doi.org/10.2147/DDDT.S558206
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Leonidas Panos
Yongbin Wang,1 Rumeng Zhang,2 Bo Wu,2 Jueming Han,1 Yuzhen Li,1 Lu Zhang3
1Department of Respiratory and Critical Care Medicine, The Second Hospital, Cheeloo College of Medicine, Shandong University, Jinan, People’s Republic of China; 2Department of Anesthesiology, The Second Hospital, Cheeloo College of Medicine, Shandong University, Jinan, People’s Republic of China; 3Department of Intensive Care Unit, The Second Hospital, Cheeloo College of Medicine, Shandong University, Jinan, People’s Republic of China
Correspondence: Lu Zhang, Department of Intensive Care Unit, The Second Hospital, Cheeloo College of Medicine, Shandong University, 247 Bei Yuan Street, Jinan, 250033, People’s Republic of China, Tel +0086-17660081006, Email [email protected]
Purpose: The aim was to investigate the effect of esketamine-dexmedetomidine (ESK-DEX) combination on immediate postprocedural oxygenation index (OI) in severe pneumonia patients undergoing bedside fiberoptic bronchoscopic (FOB) sputum aspiration, and provide clinical reference.
Methods: A total of 90 patients diagnosed with severe pneumonia receiving non-invasive mechanical ventilation (NIV) who underwent bedside FOB were randomly and evenly divided into three groups: Group C (local anesthesia alone), Group D (DEX alone), Group ED (ESK-DEX). The primary outcome was the OI immediately after procedure (T1). The secondary outcomes: the OI was calculated at 6 h (T2), 12 h (T3), and 24 h (T4) after procedure; the mean arterial pressure (MAP) and heart rate (HR) were assessed at the following time points: FOB tip passage through nostril (t1), glottis (t2), 5 minutes after procedure (t3), and upon procedure completion (t4); Additionally, perioperative adverse events were also documented.
Results: The Group ED demonstrated significantly higher OI compared to Group C at T1 (mean difference, − 8.1; 95% CI, − 13.48, − 2.64; P=0.001). Similarly, the Group ED demonstrated significantly higher OI compared to Group C at each time point from T2 to T4, respectively (all P< 0.05). Regarding hemodynamic parameters, both Group ED and Group D exhibited significantly lower MAP and HR values compared to Group C from t1 to t4 time points, respectively (all P< 0.05). The total incidence of adverse events in Group ED was significantly reduced compared to Groups C (P=0.033).
Conclusion: Compared with conventional sedation protocols, the ESK-DEX combined regimen demonstrated superior OI preservation immediately after procedure, enhanced OI within 24 hours postoperatively, improved hemodynamic stability, and enhanced safety profile in severe pneumonia patients undergoing bedside FOB-guided suction therapy. This pharmacodynamic synergy addresses critical gaps in FOB sedation—simultaneously preventing hypoxemia, maintaining respiratory drive, and minimizing adverse events.
Keywords: esketamine, dexmedetomidine, oxygenation index, fiberoptic bronchoscopy, sputum aspiration
Introduction
Severe pneumonia remains a life-threatening condition in critical care medicine, with impaired respiratory function often exacerbated by retained airway secretions.1,2 Mechanical ventilation, while life-sustaining, further complicates mucus clearance due to suppressed cough reflexes and mucosal dehydration.3 Fiberoptic bronchoscopy (FOB) with bedside suctioning has emerged as a pivotal intervention for mechanically ventilated patients with refractory sputum retention, effectively mitigating airway obstruction and reducing ventilator-associated complications.4–6 However, procedural tolerance remains a significant challenge, as inadequate sedation during FOB may provoke agitation, incomplete secretion removal, and hemodynamic instability—particularly hazardous for patients with preexisting cardiocerebrovascular comorbidities.7,8 These limitations underscore the critical need for optimized sedation protocols that ensure procedural success while preserving physiological stability.
Conventional local anesthesia, though widely used, fails to suppress the intense cough reflex and psychological distress triggered by bronchoscopic instrumentation. Consequently, patients frequently experience hypoxemia, hypertension, and tachycardia during suctioning, which may precipitate myocardial ischemia or cerebral hypoperfusion in vulnerable populations.9,10 Supplemental sedation strategies—including opioids, benzodiazepines, and propofol—carry inherent risks of respiratory depression, hypotension, and delayed recovery, complicating their use in pulmonary compromised patients.11,12 This clinical dilemma necessitates innovative pharmacological approaches that synergize effective analgesia with hemodynamic preservation. Dexmedetomidine (DEX), a highly selective α2-adrenoceptor agonist, demonstrates unique advantages in procedural sedation through its anxiolytic, sympatholytic, and analgesic-sparing effects without significant respiratory depression.13,14 Its capacity to maintain patient cooperativeness during arousable sedation makes it theoretically ideal for FOB procedures.15 However, its propensity to induce dose-dependent bradycardia limits clinical utility, particularly in patients with conduction abnormalities or beta-blocker therapy.16 Esketamine (ESK), the S-enantiomer of ketamine, presents complementary pharmacological properties as an N-methyl-D-aspartate (NMDA) receptor antagonist with robust analgesic action, bronchodilatory effects, and cardiovascular stimulating properties through catecholamine reuptake inhibition.17,18 Emerging evidence suggests its potential to counteract DEX-induced bradycardia while synergistically enhancing sedation quality.19,20 Notably, evidence shows that ketamine is effective for the treatment of severe exacerbations of asthma, which also can inhibit inflammatory cascade, reduces inflammatory markers, and causes bronchodilation—may prove particularly advantageous in pneumonia patients experiencing bronchospasm during airway manipulation.21 The oxygenation index (OI, PaO2/FiO2 ratio), a sensitive marker of pulmonary gas exchange efficiency, serves as a critical prognostic indicator in acute respiratory failure.22 Current clinical observations reveal paradoxical post-FOB hypoxemia in small number of patients despite successful secretion clearance, potentially attributable to sedation-induced atelectasis, residual bronchospasm, or inflammatory mediator release during airway manipulation.23 This phenomenon underscores the intricate interplay between sedation quality, procedural stress response, and pulmonary pathophysiology. Physiological studies demonstrate that both DEX and ESK modulate systemic inflammatory responses through nuclear factor-kappa B (NF-κB) pathway inhibition and anti-cytokine effects.13,24–27 Their combined administration may theoretically attenuate procedure-related pulmonary inflammation while maintaining optimal ventilation-perfusion matching through preserved respiratory drive and bronchial smooth muscle relaxation. Crucially, ESK’s cardiovascular stimulating properties could counterbalance DEX’s negative chronotropic effects, potentially achieving superior hemodynamic stability compared to traditional sedation regimens.28,29
However, to date, the clinical application of ESK-DEX in bronchoscopy has been rarely reported in the medical literature. Interestingly, previous studies have nevertheless demonstrated the feasibility of implementing the ketamine-DEX combination during bronchoscopic examinations. Apostolos et al30 reported DEX-ketamine demonstrated a good safety profile (eg the rate of critical desaturation events, hemodynamic complications) in patients subjected to flexible bronchoscopy and achieved more profound sedation and better bronchoscopist satisfaction than the standard midazolam-fentanyl combination without increasing the rate of adverse events. El Sharkawy RA31 demonstrated that the concomitant administration of low dose of ketamine with DEX had better intubation time and sedation scores with higher patient satisfaction scores than the combination of propofol and low dose of ketamine in patients undergoing awake fiber-optic intubation. Sinha et al32 suggested that the use of DEX-ketamine combination in awake fiberoptic nasotracheal intubation provided better hemodynamic stability and sedation than DEX alone. From a pharmacodynamic perspective, ESK theoretically demonstrates distinct advantages over ketamine in airway procedures owing to its superior binding affinity for NMDA receptors, potentially conferring enhanced analgesic efficacy and a more favorable cardiovascular safety profile. These pharmacodynamic properties may offer clinical benefits for both diagnostic and therapeutic bronchoscopic interventions.18,33
Notably, there is an obvious knowledge gap persists regarding the synergistic effects of DEX-ESK coadministration in FOB procedures, particularly concerning postprocedural oxygenation dynamics and cardiocerebrovascular safety profiles. Hence, this study proposes a novel pharmacological strategy combining DEX’s stress-response modulation with ESK’s bronchodilatory and hemodynamic stabilizing properties. We hypothesize that this synergistic regimen will improve immediate postprocedural OI, maintain hemodynamic stability, and demonstrate lower incidence of adverse events. By correlating pharmacodynamic interactions with clinical outcomes, this investigation aims to establish an evidence-based framework for sedation optimization in critically ill patients requiring therapeutic bronchoscopy.
Materials and Methods
Study Design and Ethics
This single-centre, prospective, randomized, controlled clinical study has been approved by the Research Ethics Committee of the Second Hospital of Shandong University (Approval No. KYLL2024460) and registered in the Chinese Clinical Trial Center (No. ChiCTR2400086719). This study was conducted in strict accordance with the ethical requirements set out in the Declaration of Helsinki and followed the Consolidated Standards of Reporting Trials (CONSORT) reporting guideline. Consent was obtained from the patients before surgery, and informed consent for anesthesia and the program was signed.
Inclusion and Exclusion Criteria
A total of 90 patients diagnosed with severe pneumonia receiving non-invasive mechanical ventilation (NIV) (aged 35–85 years; ASA grade III–IV), who failed to respond to conventional sputum suction therapy and presented with refractory hypoxemia (SpO2<90%) secondary to radiologically confirmed mucus plug-induced atelectasis, were enrolled in this study as candidates for FOB at the Second Hospital of Shandong University between August 2024 and May 2025 were enrolled in this study. The exclusion criteria included the following: (1) Preoperative cognitive impairment; (2) History of severe hypertension or heart disease; (3) There is severe liver and kidney dysfunction; (4) Recently taking antidepressants, sedatives, or analgesics; (5) Hypersensitivity or contraindications to the study drug; (6) Previous history of respiratory surgery, respiratory neoplasm, or anatomic abnormalities in the head, neck, face, nose, mouth or airway; (7) Patients receiving invasive mechanical ventilation or tracheotomy; (8) Contraindications for FOB; (9) Failed to complete intraoperative data collection and postoperative follow-up; (10) Patient withdrawal or other factors that may affect the experimental results (eg, the patient experiences restlessness and it difficult to complete the operation, procedural completion necessitates adjustment of the anesthetic protocol, the patient experiences requires tracheal intubation).
Randomization and Blinding
All participants were randomly and evenly assigned to three groups in a blinded fashion (with a sealed opaque envelope) by the administrator who did not take part in the treatment. Thirty minutes before surgery, an independent nurse anesthetist who was unaware of the randomization opened the envelopes and assigned eligible patients to three groups as follows: Group C (local anesthesia alone), Group D (DEX administration alone), and Group ED (DEX-ESK). The participants, chief anesthesiologists, FOB physician, and the outcome assessor were unaware of the group assignments. Only the independent anesthesia nurse was responsible for the group allocation and prepared the experimental drugs knew the group allocation, but they did not involve in the other parts of the study.
Study Interventions and Anesthesia Procedure
All patients were regularly monitored by electrocardiography (ECG), noninvasive blood pressure (NIBP), and peripheral oxygen saturation (SpO2). In addition, they received intramuscular administration of midazolam (0.05–0.075 mg/kg) for sedation and glycopyrrolate 0.5 mg to inhibit salivary secretions, along with intravenous dexamethasone (0.2 mg/kg) to prevent airway spasm or oedema as prophylactic measures 30 minutes prior to the procedure. All patients were positioned with the more patent nasal cavity selected. The nasal mucosal vasculature was pre-treated by topical application of 1% ephedrine solution for decongestion, followed by administration of 3 mL 2% lidocaine gel applied to both the nasal cavity and posterior nasal apertures to minimize mucosal injury during subsequent procedures.
Intervention protocols for each group: Group C: The mucosae of the hard palate, soft palate, tongue, base of the tongue, posterior pharyngeal wall, epiglottis, and glottic cleft were sprayed with 5% tetracaine. Additionally, 3 mL of 2% lidocaine was injected via the cricothyroid membrane to anesthetize the tracheal surface. Moreover, Group C received no additional systemic sedative infusion beyond the standardized premedication regimen (intramuscular midazolam, glycopyrrolate, and dexamethasone); Group D: DEX was administered as a loading dose of 1 μg/kg over 10 minutes, followed by a continuous infusion at 0.5 μg/kg/h; Group ED: DEX was administered as a loading dose of 1 μg/kg over 10 minutes, followed by a continuous infusion at 0.5 μg/kg/h. ESK was additionally administered as repeated bolus doses of 0.5–1.0 mg/kg when clinically necessary.34,35
FOB was performed by the same experienced physician who had completed at least 100 FOBs. All patients were positioned in a semi-recumbent posture (bed head elevated 30–45 degrees) and administered 100% fraction of inspired oxygen (FiO21.0) via a mask during the procedure. The surface of FOB was coated with sterile water-soluble lubricant. Procedures were initiated only after confirming SpO2≥90%. Under direct visualization, the bronchoscope was carefully advanced through the nasal passage into the targeted bronchus for secretion suction. Bronchoalveolar lavage was performed as clinically indicated. During slow instrument withdrawal, intermittent negative pressure suction was applied to maintain airway clearance.
In the event of intraoperative SpO2 < 85%, escalate respiratory support (eg, transition to NIV or invasive mechanical ventilation). If hemodynamic instability develops and fails to improve after pausing the procedure, administer vasoactive agents as clinically indicated. A reduction or elevation in the MAP by more than 20% of the baseline value was treated with intravenous 50 μg norepinephrine or 12.5 mg urapidil, respectively. Bradycardia, denoted by a heart rate of < 50 beats/min, was treated with intravenous atropine 0.25–0.5 mg. Tachycardia was treated with intravenous esmolol 20 mg. The above treatments were repeated, if needed. For localized bleeding, topical application of 1:10,000 epinephrine solution may be utilized. The total procedure duration should be strictly controlled within 15 minutes.
Outcomes
The primary outcome was the OI immediately after procedure (T1). The secondary outcomes: the OI was calculated at 6 h (T2), 12 h (T3), and 24 h (T4) after procedure; the mean arterial pressure (MAP) and heart rate (HR) were assessed at the following time points: FOB tip passage through nostril (t1), glottis (t2), 5 minutes after procedure (t3), and upon procedure completion (t4); the perioperative adverse reactions (during the procedure and within 24 hours post-procedure) including body movement, cough, respiratory depression, postoperative nausea and vomiting (PONV), hypertension, hypotension, tachycardia, bradycardia, bronchospasm / laryngospasm, and postoperative cognitive dysfunction (POCD).
Measurement method of OI:
Definition and Formula
The OI is calculated as: OI=PaO2/FiO2, where PaO2= arterial partial pressure of oxygen, and FiO2= fraction of inspired oxygen.
Measurement Protocol
Arterial Blood Gas (ABG) Sampling
(I) Sampling Site: Percutaneous puncture of radial, brachial, or femoral artery using a heparinized syringe. (II) Pre-analytical Requirements: Sample analyzed within 15 minutes (or placed on ice if delayed); Confirmation of adequate anticoagulation (visible syringe mixing). (III) Analytical Method: PaO2 measured via electrochemical sensor (ABG analyzer, GEM Premier 3000®), with daily calibration per CLSI guidelines.
FiO2 Determination
(I) NIV and High-flow nasal cannula (HFNC): FiO2 estimated via manufacturer’s flow- FiO2 nomogram. (II) Venturi masks: Preset FiO2 verified by external oxygen analyzer. (III) Standard masks/nasal cannula: FiO2 calculated using empirical equations (eg, FiO2=0.21+0.03×oxygen flow [L/min], with notation of inherent variability.
Sample Size Calculation
The sample size was estimated using PASS 11.0 (NCSS-PASS 11, USA). According to the results of a preparatory experiment, the OI representing a major endpoint immediately after procedure, was 306.2 ± 17.7 in Group C, 311.7 ± 16.2 in Group D, and 326.3 ± 19.5 in Group ED. The sample size was estimated using a one-way analysis of variance (ANOVA) power analysis with a significance level of 5% and power (1-β) of 0.90. The size of each group was estimated to be 24 cases. Considering a 20% dropout rate, a sample of size was N1=N2=N3=24/0.8=30 cases per group, for a total of 90 patients would be sufficient in this trial.
Statistical Analysis
Statistics were performed with SPSS Statistics 25.0 (IBM Corp, Armonk, NY, USA). Shapiro–Wilk test was used to test the normality of the data distribution. Levene’s test was used to test the homogeneity of variance. Data with normal distribution were presented as mean ± standard deviation (SD) and compared using one-way ANOVA, and subsequent pairwise comparisons were conducted using Bonferroni correction. Data with abnormal distribution were presented as median (IQR) and compared by Kruskal–Wallis test, and subsequent pairwise comparisons were performed by Nemenyi test. Categorical variables were described as n (%) and compared by Chi-square test or Fisher’s exact test (as expected cell counts were less than 5), and subsequent pairwise comparisons were performed using Bonferroni correction. For repeated-measures data that are normally distributed, repeated-measures ANOVA was utilized, and subsequent pairwise comparisons were conducted using Bonferroni correction. The assumption of sphericity was evaluated using Mauchly’s test. In cases where sphericity was violated (Mauchly’s test p < 0.05), Greenhouse–Geisser or Huynh–Feldt corrections were applied to adjust the degrees of freedom and corresponding p-values accordingly. If the data exhibited a skewed distribution, the Generalized Estimating Equations (GEE) method was recommended. P value < 0.05 was considered statistically significant.
Results
A total of 97 patients were enrolled in the study. Seven patients were excluded because they did not meet the inclusion criteria (n = 7). Two participants in Group C experienced severe coughing that necessitated modification of the anesthetic protocol to ensure successful procedure completion, and one participant in Group D developed acute heart failure 5 hours after suctioning, requiring emergent endotracheal intubation with invasive mechanical ventilation, leading to their withdrawal from the study. Ultimately, 87 participants successfully completed the study without complications (eg, local hemorrhage, hypoxemia, tracheal laceration, or cerebrovascular accident) and were included in the analysis (Figure 1). The intention-to-treat population comprised all 90 randomized patients; the per-protocol population comprised 87 patients (Group C: 28, Group D: 29, Group ED: 30).
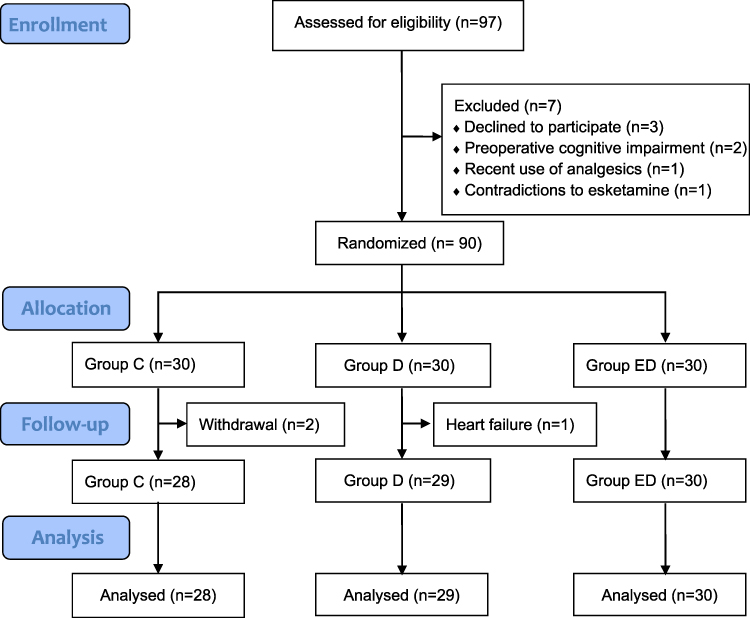 |
Figure 1 Flow chart of patient screening and selection process. Abbreviations: Group C, Local anesthesia; Group D, Dexmedetomidine; Group ED, Dexmedetomidine combined with esketamine. |
The patient characteristics at baseline were well balanced between the groups (Table 1). Based on one-way ANOVA: Group ED demonstrated significantly higher OI compared to Group C immediately after procedure (T1) (mean difference, −8.1; 95% CI, −13.48, −2.64; P=0.001), while no significant differences were observed between Groups D and C (mean difference, −4.2; 95% CI, −9.62, 1.31; P=0.201) or between Groups D and ED (mean difference, −3.9; 95% CI, −9.28, 1.46; P=0.237) (Figure 2 and Table 2). Similarly, based on repeated measures ANOVA: Group ED demonstrated significantly higher OI compared to Group C at each time point from T2 to T4, respectively (all P<0.05), while no significant differences were observed between Groups D and C or between Groups D and ED, respectively (all P>0.05) (Figure 2 and Table 2); Regarding hemodynamic parameters, both the Group ED and Group D exhibited significantly lower MAP and HR values compared to the Group C from t1 to t4 time points, respectively (all P<0.05). Notably, however, there was no statistically significant difference between the Group ED and Group D in these parameters, respectively (all P>0.05) (Figure 3A, B and Table 2). In terms of perioperative safety, the total incidence of adverse events in the Group ED was significantly reduced compared to Groups C (P=0.033). However, no statistically significant difference was observed between Group D and Group C or Group D and Group ED regarding the adverse event occurrence, respectively (all P>0.05) (Table 3). These findings suggest that the combined regimen provides superior clinical outcomes in maintaining oxygenation stability while improving hemodynamic profiles and safety parameters in this patient population.
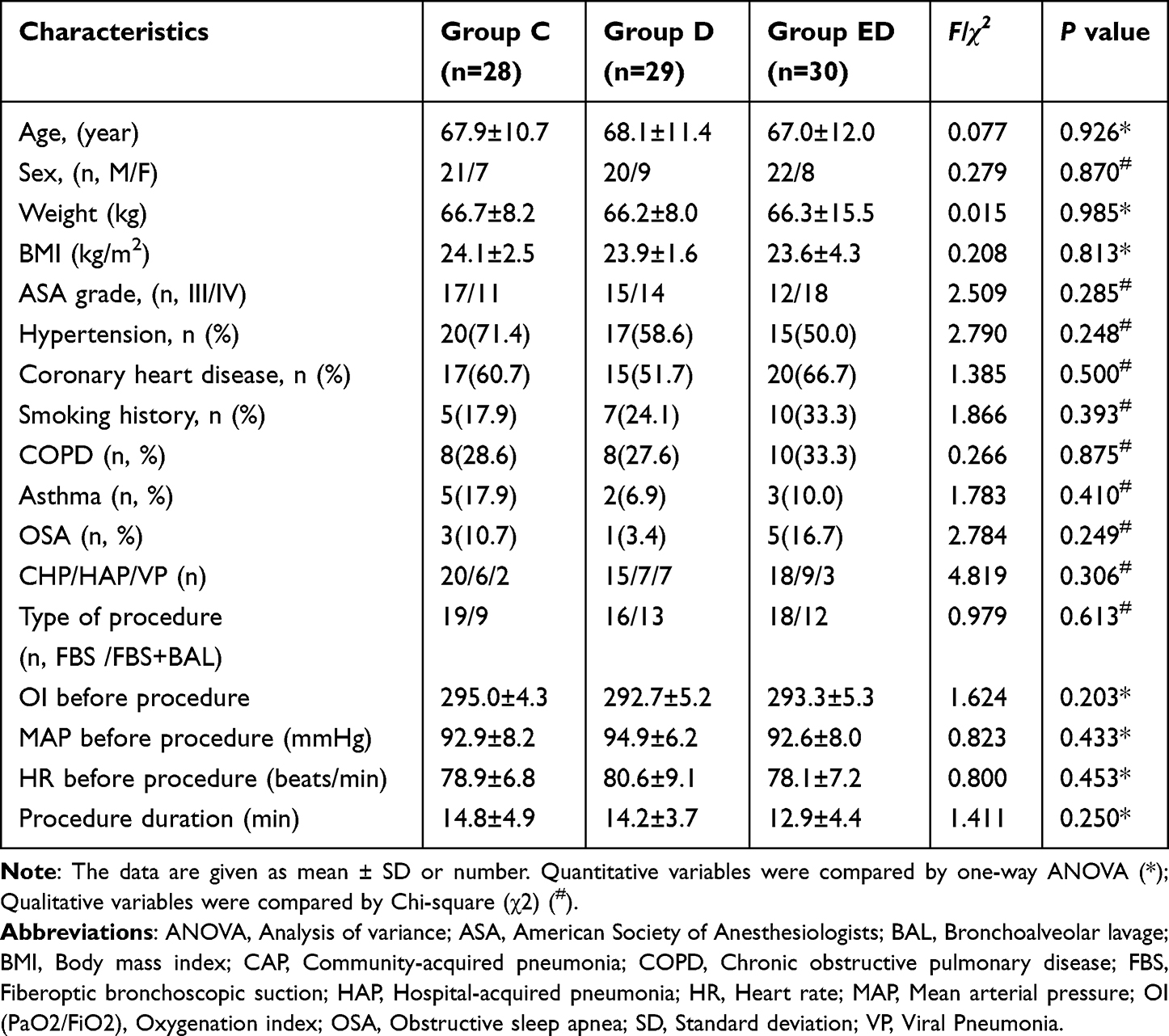 |
Table 1 Comparison of Demographic Data and Characteristics in the Groups |
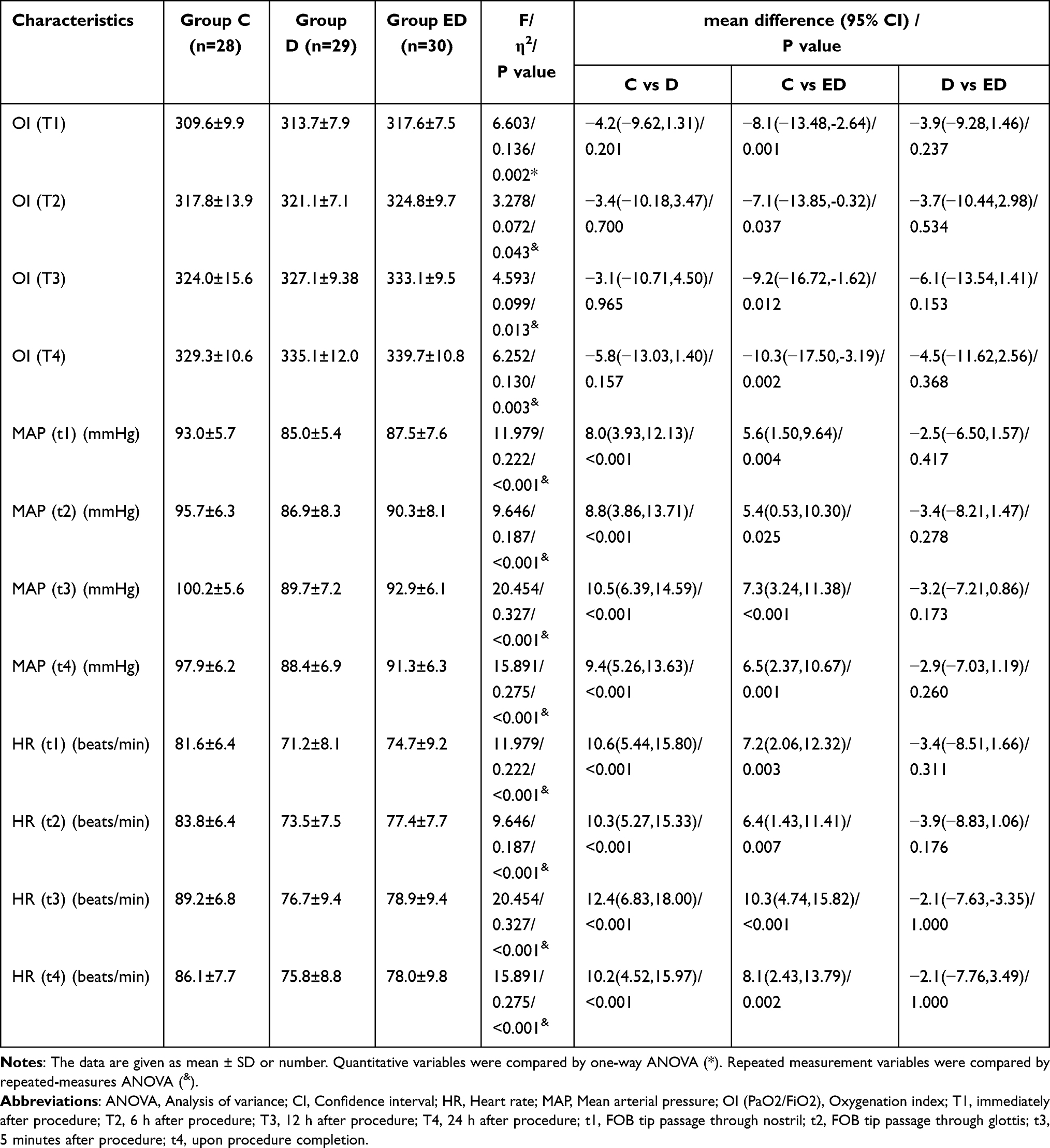 |
Table 2 Comparison of Primary and Secondary Outcomes |
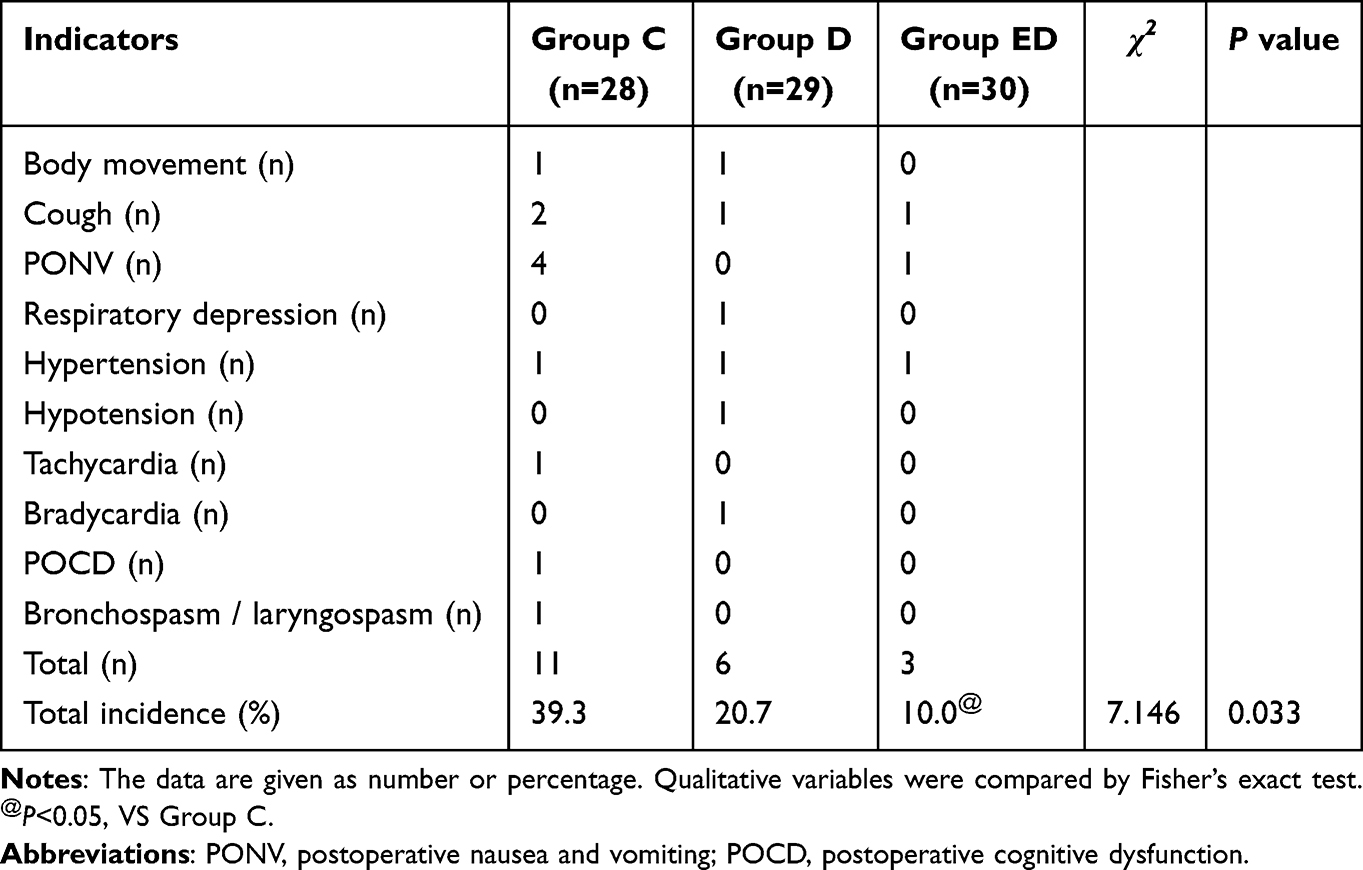 |
Table 3 Comparison of Perioperative Adverse Reactions |
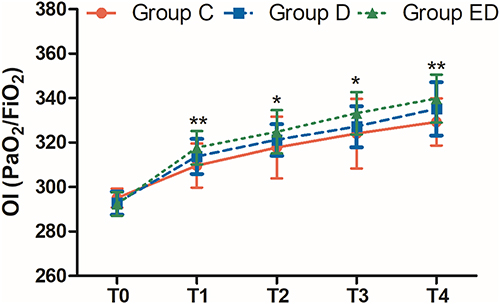 |
Figure 2 Comparison of the OI after procedure (T0), immediately after procedure (T1), and at 6 h (T2), 12 h (T3), and 24 h (T4) after procedure. (28 patients in Group C, 29 patients in Group D and 30 patients in group ED). The data are expressed as mean ± SD. Compared with Group C, *p<0.05, **p<0.01. Abbreviations: Group C, Local anesthesia; Group D, Dexmedetomidine; Group ED, Dexmedetomidine combined with esketamine; SD, Standard deviation; OI, Oxygenation index (PaO2/FiO2). |
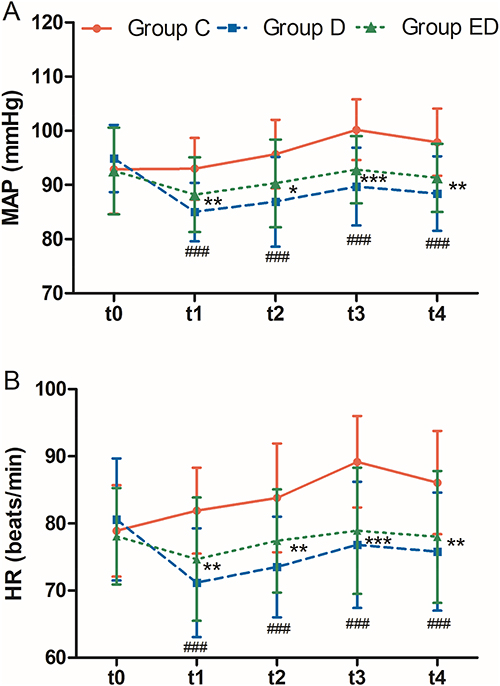 |
Figure 3 Comparison of the MAP (A) and HR (B) before procedure (t0), at FOB tip passage through nostril (t1), glottis (t2), 5 minutes after procedure (t3), and upon procedure completion (t4). (28 patients in Group C, 29 patients in Group D and 30 patients in group ED). The data are expressed as mean ± standard deviation. Compared with Group C, *p<0.05, **p<0.01, ***p<0.001. Compared with Group D, ###p<0.001. Abbreviations: Group C, Local anesthesia; Group D, Dexmedetomidine; Group ED, Dexmedetomidine combined with esketamine; HR, Heart rate; MAP, Mean arterial pressure; SD, Standard deviation; FOB, Fiberoptic bronchoscopic. |
Discussion
The present study demonstrates that the co-administration of ESK-DEX combination during bedside FOB for sputum suction significantly improves postoperative OI while maintaining perioperative hemodynamic stability and reducing adverse events compared to DEX alone or local anesthesia care. These findings highlight the potential clinical advantages of this novel combination regimen in optimizing perioperative outcomes for patients undergoing invasive respiratory procedures.
Compared to Group C, the Group ED demonstrated a superior OI at T1, as well as consistently higher indices from T2 to T4, potentially due to synergistic pharmacological effects. ESK, a potent NMDA receptor antagonist, has demonstrated anti-inflammatory properties and bronchodilatory effects via β2-adrenergic receptor activation, potentially reducing airway resistance and alveolar collapse during bronchoscopy.36 DEX, a highly selective α2-adrenoreceptor agonist, exerts lung-protective effects by attenuating systemic inflammatory responses and oxidative stress, as evidenced in ARDS models.37,38 The combination likely mitigates procedure-induced hypoxia through dual mechanisms: ESK’s preservation of respiratory drive counterbalances DEX’s mild respiratory depressant effects, while their combined anti-inflammatory action may reduce post-procedural alveolar-capillary membrane injury.26,39,40 Ishibashi et al41 reported that DEX was safe and effective in spontaneously breathing patients after endoscopic submucosal dissection. Ding et al42 demonstrated that the protective role of ESK against lung injury, inflammation, oxidative stress, and apoptosis in mice with ARDS and revealed the reaction mechanism related to mitophagy in a basic study. Similarly, Song et al43 revealed that in elderly patients undergoing thoracoscopic radical surgery for lung cancer, treatment with ESK combined with distal limb ischemic can alleviate acute lung injury by enhancing anti-inflammatory response to reduce lung complications and promote the patients’ recovery. In addition, Yang et al44 showed that patients undergoing same-visit bidirectional endoscopy, the administration of low-dose ESK resulted in an approximately 61% reduction in the incidence of desaturation and hypotension, accompanied by decreased propofol requirements in a randomized clinical trial. Furthermore, Zhou et al45 showed that the combination of ESK and DEX had minimal impact on respiration during percutaneous endoscopic transforaminal discectomy. Nie et al7 exhibited that compared with remifentanil, the combination of ESK with propofol leaded to more stable intraoperative hemodynamics, lower transient hypoxia rate, and fewer incidence of adverse events in FOB.
The findings of these reports are consistent with our research results, demonstrating that ESK and DEX exhibit pulmonary protective effects and deserve further clinical promotion. In addition to the synergistic organ-protective effects of these two medications, multiple contributing factors were identified to collectively enhance OI improvement, which include optimized analgesia-sedation management, stabilized respiratory function, attenuated stress response, uneventful procedural execution, thorough airway secretion clearance, and reduced incidence of adverse events.
The MAP and HR in Group ED measured at four critical time points (t1-t4) were significantly lower than those in Group C. Similarly, compared to the Group C, the Group D also exhibited a significant reduction in both MAP and HR. Furthermore, though no statistically significant differences were observed between Group ED and Group D, these parameters demonstrated visually smoother fluctuations in Group ED compared to Group D, with consistently higher mean values across observation intervals. The MAP and HR displayed minimal fluctuations and remained relatively stable across the four time points, accompanied by a reduced stress response. Notably, this attenuated hemodynamic response with diminished fluctuations may confer protective benefits in critically ill patients by maintaining physiologically appropriate MAP and HR levels during intense surgical stimulation, thereby reducing the risk of cardiovascular/cerebrovascular adverse events and associated complications. The absence of sustained tachycardia or hypertension perioperative in Group ED suggests DEX’s α2-mediated central sympatholytic effects effectively modulate ESK’s acute adrenergic surge.46 This dynamic balance warrants particular consideration in patients with cardiovascular comorbidities, where individualized hemodynamic monitoring remains essential.
Our results are consistent with the previous outcomes conducted by Zhou et al45 revealed that the ESK-DEX had minimal impact on circulation during percutaneous endoscopic transforaminal discectomy. In a randomized double-blind clinical trial, Lin et al47 reported that low-dose ESK combined with DEX has fewer hemodynamic effects on patients, milder respiratory depression, and shorter recovery time because of its better controllability of sedation depth in lung tumor percutaneous radiofrequency ablation. Additionally, in a retrospective analysis, Lin et al48 showed that compared with DEX alone, the ESK-DEX during spinal tumor surgery can demonstrated superior sedation, pain control and lower MAP and HR, making it a viable alternative for spinal tumor surgery anesthesia.
Furthermore, Ye et al49 demonstrated that DEX-ESK in patients undergoing total laparoscopic hysterectomy under general anesthesia was effective in reducing stress response and maintaining stable hemodynamics in a randomized clinical trial. Interestingly, El-Rouby et al50 reported both DEX-KET combination and DEX alone are effective in providing hemodynamic stability, as well as DEX-KET combination significantly improved the behavior of sedated children compared to DEX alone.
The significantly lower incidence of adverse events in the Group ED (eg, notably less cough and PONV) underscores the therapeutic synergy between these agents. DEX’s anxiolytic properties likely mitigate ESK’s psychotomimetic effects,51 while ESK’s bronchodilation counteracts potential α2-mediated bronchoconstriction.52 Importantly, the combination appears to reduce the mutual dosage, potentially lowering related complications. This safety advantage holds particular relevance for ICU critically ill patients. Qiao et al53 revealed that the less gastrointestinal events were observed in Group DEX-ESK compared with Group ESK in pediatric patients undergoing strabismus surgery. Ye et al54 reported that patients in Group DEX-ESK had less risks of PONV and bradycardia in geriatric patients undergoing hip surgery. Xie et al19 showed that the findings suggest that low-dose ESK and DEX can reduce the incidence of emergence delirium in children undergoing fiber bronchoscopy. Similarly, Huang et al55 demonstrated that DEX plus ESK decreased the incidence of bradycardia and partly improved postoperative recovery quality. Lu et al56 reported that the incidence of emergence agitation and the paediatric anaesthesia emergence delirium (PAED) score in the ED group were lower than those in the DEX and ESK groups. Conversely, Zhou et al45 reported that the ESK-DEX combination is associated with increased incidences of postoperative dizziness and psychiatric side effects in percutaneous endoscopic transforaminal discectomy, which potentially attributable to the combination of prolonged operative duration and elevated dosages of dual pharmacological agents administered during the procedure.
These findings suggest that ESK-DEX combination therapy may offer potential advantages in sedation protocols for FOB procedures in critical care settings. However, further validation through multicenter randomized controlled trials is warranted before these results can be broadly applied in clinical practice. The improved OI support its use in patients with acute respiratory failure requiring frequent sputum clearance, where maintaining adequate OI is prognostic. Furthermore, the hemodynamic profile makes this regimen particularly suitable for critical patients with cardiovascular and cerebrovascular diseases. Future protocols should consider intraoperative bispectral index monitoring to optimize dosing, given the narrow therapeutic window in critically ill populations.
While this study provides robust preliminary evidence, several limitations warrant acknowledgment. Firstly, the single-center design and relatively small sample size may limit generalizability, and the results of this study require a multi-center and large sample for further confirmation. However, from another perspective, the single-center implementation ensured strict standardization of FOB suction procedures, sedation protocols, and OI measurement techniques—critical for minimizing heterogeneity in this proof-of-concept study. Secondly, we did not account for potential confounding factors including disease duration, variations in antibiotic regimens, and corticosteroid administration, which may have influenced the findings. Thirdly, the inclusion criteria were limited to pneumonia patients receiving non-invasive ventilation, thereby the conclusions may not be generalizable to populations requiring tracheal intubation or high-flow oxygen therapy. Fourthly, due to limitations in finite human resources and funding allocation, the absence of long-term outcome data (eg, ventilator-free days, ICU mortality) precludes assessment of clinical significance beyond immediate physiological parameters. Fifthly, in our study design, patients with preexisting COPD and chronic smoking history were not excluded, as this would have substantially limited the generalizability of our findings to real-world surgical populations. Moreover, statistical analyses revealed no significant intergroup differences in either COPD prevalence (p=0.875) or smoking exposure levels (p=0.393). However, the residual confounding from these factors could theoretically persist. In future, we will develop some studies which employ stratified analyses or adjusted multivariate models to explicitly quantify these interactions. Sixthly, it should be noted that the per-protocol approach used in this study, while methodologically appropriate for assessing efficacy under ideal conditions, may limit the generalizability of our findings to more clinically complex populations. Finally, the fixed dosing regimen may not account for interpatient variability in drug metabolism, particularly in renal/hepatic impairment. Furthermore, future multicenter trials should incorporate pharmacokinetic modeling, biomarker analysis (eg, inflammatory cytokines), and extended follow-up to validate these findings.
Conclusion
Compared with conventional sedation protocols, the ESK-DEX combined regimen demonstrated superior OI preservation immediately after procedure, enhanced OI within 24 hours postoperatively, improved hemodynamic stability, and enhanced safety profile in critically severe pneumonia patients undergoing bedside FOB-guided suction therapy. This pharmacodynamic synergy addresses critical gaps in FOB sedation—simultaneously preventing hypoxemia, maintaining respiratory drive, and minimizing adverse events. While further research is needed to establish dosing optimization and long-term benefits, these findings may inform the optimization of sedation protocols for similar procedures and warrant further investigation in larger, multicentre settings.
Abbreviations
ANOVA, analysis of variance; ARDS, acute respiratory distress syndrome; ASA, American Society of Anesthesiologists; BAL, bronchoalveolar lavage; BMI, body mass index; CAP, community-acquired pneumonia; CI, confidence interval; COPD, chronic obstructive pulmonary disease; DEX, dexmedetomidine; D, diabetes mellitus; ESK, esketamine; FBS, fiberoptic bronchoscopic suction; FiO2, fraction of inspired oxygen; HAP, hospital-acquired pneumonia; HR, heart rate; MAP, mean arterial pressure; NMDA, N-methyl-D-aspartate; NIV, non-invasive mechanical ventilation; IQR, interquartile range-range; OI (PaO2/FiO2), oxygenation index; OSA, obstructive sleep apnea; P, probability; PaCO2, partial pressure of arterial dioxide; PAED, paediatric anaesthesia emergence delirium; PaO2, partial pressure of arterial oxygen; POCD, postoperative cognitive dysfunction; PONV, postoperative nausea and vomiting; SpO2, pulse oximetry saturation; SD, standard deviation; α2AR, α2 adrenergic receptor; VP, viral pneumonia.
Data Sharing Statement
The datasets used in this study were obtained from the corresponding authors based on reasonable requirements.
Acknowledgments
We thank the participants enrolled in this study and the study team for their essential contributions.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas, took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This work was supported by the clinical medical projects of Jinan science and technology bureau under Grant No. 202019198.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cillóniz C, Torres A, Niederman MS. Management of pneumonia in critically ill patients. BMJ. 2021;375:e065871. doi:10.1136/bmj-2021-065871
2. Chen Z, Zhong M, Jiang L, et al. Effects of the lower airway secretions on airway opening pressures and suction pressures in critically ill COVID-19 patients: a computational simulation. Ann Biomed Eng. 2020;48(12):3003–3013. doi:10.1007/s10439-020-02648-0
3. Goetz RL, Vijaykumar K, Solomon GM. Mucus clearance strategies in mechanically ventilated patients. Front Physiol. 2022;13:834716. doi:10.3389/fphys.2022.834716
4. Tang H, Yuan Z, Li J, Wang Q, Fan W. Fiberoptic bronchoscopy for the prevention of ventilator-associated pneumonia: a meta-analysis of randomized controlled trials. J Infect Dev Ctries. 2024;18(9):1413–1420. doi:10.3855/jidc.17866
5. Shi Z, Qin Y, Zhu Y, et al. Effect of bronchoalveolar lavage with fiberoptic bronchoscopy combined with vibration sputum drainage on mechanically ventilated patients with severe pneumonia: a prospective randomized controlled trial in 286 patients. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2017;29(1):66–70. doi:10.3760/cma.j.issn.2095-4352.2017.01.014
6. Zhao Y, Dai X, Ji J, Cheng P. Bronchial lavage under fiberoptic bronchoscopy in the treatment of severe pulmonary infection. Pak J Med Sci. 2020;36(3):396–401. doi:10.12669/pjms.36.3.1539
7. Nie J, Chen W, Jia Y, Zhang Y, Wang H. Comparison of remifentanil and esketamine in combination with propofol for patient sedation during fiberoptic bronchoscopy. BMC Pulm Med. 2023;23(1):254. doi:10.1186/s12890-023-02517-1
8. Wu B, Zhu W, Wang Q, et al. Efficacy and safety of ciprofol-remifentanil versus propofol-remifentanil during fiberoptic bronchoscopy: a prospective, randomized, double-blind, non-inferiority trial. Front Pharmacol. 2022;13:1091579. doi:10.3389/fphar.2022.1091579
9. Yanik F, Sagiroglu G, Karamustafaoglu YA. Sublingual vs. intranasal dexmedetomidine sedation for flexible fiberoptic bronchoscopy procedure: a retrospective comparative study. Eur Rev Med Pharmaco. 2023;27(23):11351–11360. doi:10.26355/eurrev_202312_34574
10. Chai B, Guo J, Xu Z, et al. Comparison of the efficacy and safety of remimazolam and propofol for fiberoptic bronchoscopy in older patients: a prospective, randomized controlled study. BMC Geriatr. 2025;25(1):337. doi:10.1186/s12877-025-05984-9
11. Luo Z, Tu H, Zhang X, et al. Efficacy and safety of HSK3486 for anesthesia/sedation in patients undergoing fiberoptic bronchoscopy: a multicenter, double-blind, propofol-controlled, randomized, phase 3 study. CNS Drugs. 2022;36(3):301–313. doi:10.1007/s40263-021-00890-1
12. Chen W, Bao W, Shi J, Shi L, Cui J. Investigation into the application of remimazolam in conjunction with low-dose propofol for pediatric fiberoptic bronchoscopy. Sci Rep. 2024;14(1):11671. doi:10.1038/s41598-024-62181-1
13. Li F, Ma L, Yan S, Liu D. Effects of dexmedetomidine or propofol on postoperative oxygenation index during invasive ventilation in patients after off-pump coronary artery bypass grafting: a single-center retrospective study. Int J Gen Med. 2025;18:3463–3476. doi:10.2147/IJGM.S524691
14. Li N, Zhang Y, Yang F, et al. Effects of dexmedetomidine on oxygenation and inflammatory factors in patients undergoing uvulopalatopharyngoplasty: a prospective, randomized, placebo-controlled trial. Sleep Breath. 2023;27(3):1099–1106. doi:10.1007/s11325-022-02711-1
15. Yang T, Mudabbar MS, Chen T, et al. Dexmedetomidine dosage in critically ill patients undergoing intraoperative wake-up test: a randomized controlled trial. Medicine. 2022;101(10):e28993. doi:10.1097/MD.0000000000028993
16. Abosheaishaa H, Abdallfatah A, Abdelghany A, et al. Dexmedetomidine as an adjunctive sedative in patients undergoing endoscopic submucosal dissection: a systematic review and meta-analysis. ASIDE Gastroenterol. 2025;1(1):7–14. doi:10.71079/aside.gi.0109257
17. Huang X, Li X, Sun Y, Wu A, Ai P. Comparison of esketamine/propofol and sufentanil/propofol on intraoperative hypoxemia during bronchoscopy: a randomized trial. Drug Des Devel Ther. 2025;19:4429–4436. doi:10.2147/DDDT.S490423
18. Suleiman A, Wongtangman K, Eikermann M, Stucke AG. Neuroanatomical and pharmaco-physiological effects of hypoxia and esketamine on breathing, the sympathetic nerve system, and cortical function. Br J Anaesth. 2025;134(2):277–280. doi:10.1016/j.bja.2024.11.011
19. Xie W, Wang L, Peng Z, et al. The impact of preoperative low-dose esketamine and dexmedetomidine nasal administration on the emergence delirium in children undergoing fiber bronchoscopy: a prospective randomized controlled trial. Clin Neuropharmacol. 2025;48(3):97–103. doi:10.1097/WNF.0000000000000637
20. Xu SX, Shan XS, Gao JM, et al. Effect of esketamine vs dexmedetomidine adjunct to propofol sedation for pediatric 3Tesla magnetic resonance imaging: a randomized, double-blind, controlled trial. Eur J Med Res. 2022;27(1):258. doi:10.1186/s40001-022-00890-x
21. Gautam CS, Mahajan SS, Sharma J, Singh H, Singh J. Repurposing Potential of Ketamine: opportunities and Challenges. Indian J Psychol Med. 2020;42(1):22–29. doi:10.4103/IJPSYM.IJPSYM_228_19
22. Shah N, Sarangi BU, Shankar GH, Walimbe A. Comparison of PaO2/FiO2 (PF ratio) to SpO2/FiO2 (SF ratio) and OI to OSI for predicting short term outcomes in children with acute hypoxemic respiratory distress: a prospective observational study. Indian J Pediatr. 2025;92(8):823–829. doi:10.1007/s12098-024-05134-w
23. Uluç K, Akkütük Öngel E, Köylü Ilkaya N, et al. Analysis of 332 fiberoptic bronchoscopies performed in a respiratory intensive care unit: a retrospective study. Eur Rev Med Pharmaco. 2024;28(4):1433–1438. doi:10.26355/eurrev_202402_35465
24. Zhi J, Duan Q, Wang Q, Du X, Yang D. Dexmedetomidine reduces IL-4 and IgE expression through downregulation of the TLR4/NF-κB signaling pathway to alleviate airway hyperresponsiveness in OVA mice. Pulm Pharmacol Ther. 2022;75:102147. doi:10.1016/j.pupt.2022.102147
25. Xu L, Li T, Chen Q, et al. The α2AR/Caveolin-1/p38MAPK/NF-κB axis explains dexmedetomidine protection against lung injury following intestinal ischaemia-reperfusion. J Cell Mol Med. 2021;25(13):6361–6372. doi:10.1111/jcmm.16614
26. Cai SY, Liu A, Xie WX, et al. Esketamine mitigates mechanical ventilation-induced lung injury in chronic obstructive pulmonary disease rats via inhibition of the MAPK/NF-κB signaling pathway and reduction of oxidative stress. Int Immunopharmacol. 2024;139:112725. doi:10.1016/j.intimp.2024.112725
27. Fu M, Xu R, Chen G, et al. Postoperative esketamine improves ventilation after video-assisted thoracoscopic lung resection: a double-blinded randomized controlled trial. Heliyon. 2024;10(3):e25100. doi:10.1016/j.heliyon.2024.e25100
28. Pei D, Xiao T, Zeng L, et al. Optimal doses of intranasal esketamine plus dexmedetomidine for sedating toddlers during transthoracic echocardiography: a prospective, double-blind, randomized trial. Ann Med. 2025;57(1):2453087. doi:10.1080/07853890.2025.2453087
29. Zou H, Wang LX, Wang M, et al. MTOR –mediated allergy is involved in the protective effect of ketamine on allergic airway inflammation. J Immunol Res. 2019;2019:5879714. doi:10.1155/2019/5879714
30. Apostolos F, Nikolaos Z, Charalampos M, et al. Dexmedetomidine-ketamine combination versus fentanyl-midazolam for patient sedation during flexible bronchoscopy: a prospective, single-blind, randomized controlled trial. BMC Pulm Med. 2024;24(1):301. doi:10.1186/s12890-024-02988-w
31. El Sharkawy RA. Efficacy of adding low-dose ketamine to dexmedetomidine versus low-dose ketamine and propofol for conscious sedation in patients undergoing awake fiber-optic intubation. Anesth Essays Res. 2019;13(1):73–78. doi:10.4103/aer.AER_181_18
32. Sinha SK, Joshiraj B, Chaudhary L, et al. A comparison of dexmedetomidine plus ketamine combination with dexmedetomidine alone for awake fiberoptic nasotracheal intubation: a randomized controlled study. J Anaesth Clin Pharm. 2014;30(4):514–519. doi:10.4103/0970-9185.142846
33. Mion G, Himmelseher S. Esketamine: less drowsiness, more analgesia. Anesth Analg. 2024;139(1):78–91. doi:10.1213/ANE.0000000000006851
34. Wang Y, Feng C, Fu J, Liu D. Clinical application of ultrasound-guided internal branch of superior laryngeal nerve block in patients with severe COPD undergoing awake fibreoptic nasotracheal intubation: a randomized controlled clinical trial. Int J Chron Obstruct Pulmon Dis. 2023;18:521–532. doi:10.2147/COPD.S399513
35. Korkmaz Ekren P, Basarik Aydogan B, Gurgun A, et al. Can fiberoptic bronchoscopy be applied to critically ill patients treated with noninvasive ventilation for acute respiratory distress syndrome? Prospective observational study. BMC Pulm Med. 2016;16(1):89. doi:10.1186/s12890-016-0236-y
36. Shi J, Song S, Wang Y, et al. Esketamine alleviates ferroptosis-mediated acute lung injury by modulating the HIF-1α/HO-1 pathway. Int Immunopharmacol. 2024;142(Pt A):113065. doi:10.1016/j.intimp.2024.113065
37. Bai YX, Zhang JH, Zhao BC, Liu KX, Bai YW. Dexmedetomidine attenuates one-lung ventilation associated lung injury by suppressing inflammatory responses: a systematic review and meta-analysis. Clin Exp Pharmacol Physiol. 2021;48(9):1203–1214. doi:10.1111/1440-1681.13525
38. Chen Q, Qin Z, Sun Y, et al. Dexmedetomidine activates Akt, STAT6 and IRF4 modulating cytoprotection and macrophage anti-inflammatory phenotype against acute lung injury in vivo and in vitro. J Inflamm Res. 2022;15:2707–2720. doi:10.2147/JIR.S357012
39. Liu A, Gao XH, Mao Y, et al. Esketamine mitigates lung injury in COPD rat models under mechanical ventilation: an RNA-sequencing and bioinformatics analysis of serum exosome miRNA profiles. Gene. 2025;962:149571. doi:10.1016/j.gene.2025.149571
40. Hong X, Xu S, Sun G, et al. Efficacy and safety of esketamine for smoking cessation among patients diagnosed with lung cancer and major depression disorder: a randomized, placebo-controlled clinical trial. J Affect Disord. 2025;383:1–10. doi:10.1016/j.jad.2025.04.077
41. Ishibashi C, Hayashida M, Sugasawa Y, et al. Effects of dexmedetomidine on hemodynamics and respiration in intubated, spontaneously breathing patients after endoscopic submucosal dissection for cervical esophageal or pharyngeal cancer. J Anesth. 2016;30(4):628–636. doi:10.1007/s00540-016-2175-4
42. Ding M, Pei P, Liu W, et al. Esketamine regulates mitophagy through ULK1/FUNDC1 signaling pathway to improve LPS-induced acute respiratory distress syndrome. Curr Pharm Design. 2025;31(34):2774–2782. doi:10.2174/0113816128361112250221065359
43. Song N, Yang Y, Zheng Z, et al. Effect of esketamine added to propofol sedation on desaturation and hypotension in bidirectional endoscopy: a randomized clinical trial. JAMA Network Open. 2023;6(12):e2347886. doi:10.1001/jamanetworkopen.2023.47886
44. Yang Y, Liu G, Ou Y, Lu W. Lung-protective effect of esketamine combined with distal limb ischemic preconditioning in elderly patients undergoing thoracoscopic radical surgery for lung cancer: a randomized controlled trial in 160 cases. Nan Fang Yi Ke Da Xue Xue Bao. 2024;44(3):484–490. doi:10.12122/j.issn.1673-4254.2024.03.09
45. Zhou JS, Chen Z, Liu YY, et al. Observation on the analgesic effect of different doses of a combination of esketamine and dexmedetomidine administered for percutaneous endoscopic transforaminal discectomy: a randomized, double-blind controlled trial. Cns Drugs. 2024;38(7):547–558. doi:10.1007/s40263-024-01083-2
46. Lee S. Dexmedetomidine: present and future directions. Korean J Anesthesiol. 2019;72(4):323–330. doi:10.4097/kja.19259
47. Lin Z, Li S, Zhou Y, et al. A comparative study of esketamine-dexmedetomidine and sufentanil-dexmedetomidine for sedation and analgesia in lung tumor percutaneous radiofrequency ablation (PRFA): a randomized double-blind clinical trial. BMC Anesthesiol. 2023;23(1):304. doi:10.1186/s12871-023-02266-y
48. Lin C, Yan L, Shi J, et al. Comparative sedative effects of esketamine and dexmedetomidine versus dexmedetomidine alone in patients undergoing spinal tumor surgery. Ther Clin Risk Manag. 2025;21:747–755. doi:10.2147/TCRM.S515869
49. Ye X, Xie B, Li Y, Zhong R, Li Y. Effect of dexmedetomidine-assisted esketamine on hemodynamics and stress level in patients undergoing total laparoscopic hysterectomy under general anesthesia. J Formos Med Assoc. 2025;S0929-6646(25):00336. Online ahead of print. doi:10.1016/j.jfma.2025.06.045
50. El-Rouby SH, Crystal YO, Elshafie AM, Wahba NA, El-Tekeya MM. The effect of dexmedetomidine-ketamine combination versus dexmedetomidine on behavior of uncooperative pediatric dental patients: a randomized controlled clinical trial. J Appl Oral Sci. 2024;32:e20240057. doi:10.1590/1678-7757-2024-0057
51. Chu Q, Zhu K, Bai Y, et al. A single low dose of dexmedetomidine efficiently attenuates esketamine-induced overactive behaviors and neuronal hyperactivities in mice. Front Hum Neurosci. 2021;15:735569. doi:10.3389/fnhum.2021.735569
52. Qiao D, Liu W, Xue H, et al. Comparison of the effects of esketamine/midazolam and remifentanil/midazolam on respiratory mechanics in mechanically ventilated patients with acute respiratory distress syndrome. BMC Anesthesiol. 2025;25(1):339. doi:10.1186/s12871-025-03211-x
53. Qiao H, Zhuang Y, Lv P, et al. Intranasal esketamine versus esketamine-dexmedetomidine combination for premedication in pediatric patients undergoing strabismus surgery: a randomized controlled trial.Transl Pediatr. Translational Pediatrics. 2024;13(8):1327–1335. doi:10.21037/tp-24-45
54. Ye Q, Hu Y, Xing Q, et al. The effects of opioid-free anesthesia with dexmedetomidine and esketamine on postoperative anesthetic-related complications for hip surgery in the elderly. Int J Gen Med. 2024;17:6291–6302. doi:10.2147/IJGM.S492771
55. Huang Z, Liu N, Hu S, et al. Effect of dexmedetomidine and two different doses of esketamine combined infusion on the quality of recovery in patients undergoing modified radical mastectomy for breast cancer - a randomised controlled study. Drug Des Devel Ther. 2023;17:2613–2621. doi:10.2147/DDDT.S422896
56. Lu X, Tang L, Lan H, Li C, Lin H. A comparison of intranasal dexmedetomidine, esketamine or a dexmedetomidine-esketamine combination for induction of anaesthesia in children: a randomized controlled double-blind trial. Front Pharmacol. 2021;12:808930. doi:10.3389/fphar.2021.808930
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Dexmedetomidine and Two Different Doses of Esketamine Combined Infusion on the Quality of Recovery in Patients Undergoing Modified Radical Mastectomy for Breast Cancer - A Randomised Controlled Study
Huang Z, Liu N, Hu S, Ju X, Xu S, Wang S
Drug Design, Development and Therapy 2023, 17:2613-2621
Published Date: 28 August 2023
Opioid-Free Anesthesia for Pain Relief After Laparoscopic Cholecystectomy: A Prospective Randomized Controlled Trial
Yu JM, Tao QY, He Y, Liu D, Niu JY, Zhang Y
Journal of Pain Research 2023, 16:3625-3632
Published Date: 30 October 2023
Intranasal Dexmedetomidine-Esketamine Combination Premedication versus Monotherapy for Reducing Emergence Delirium and Postoperative Behavioral Changes in Pediatric Tonsillectomy and/or Adenoidectomy: A Randomized Controlled Trial

Liao Y, Xie S, Zhuo Y, Chen S, Luo Y, Wei Y, Yao Y
Drug Design, Development and Therapy 2024, 18:4693-4703
Published Date: 23 October 2024
The Effects of Opioid-Free Anesthesia with Dexmedetomidine and Esketamine on Postoperative Anesthetic-Related Complications for Hip Surgery in the Elderly
Ye Q, Hu Y, Xing Q, Wu Y, Zhang Y
International Journal of General Medicine 2024, 17:6291-6302
Published Date: 17 December 2024
Effect of Intraoperative Intravenous Infusion of Esketamine Combined with Dexmedetomidine on Postoperative Sleep Disturbance in Patients Undergoing Radical Mastectomy
Geng X, Pu Y, Hu Z, Zhang H, Wang M, Fang C, Lv G, Li W, Zhang X, Fan X, Liu S, Chen X, Wu J
Drug Design, Development and Therapy 2025, 19:4629-4640
Published Date: 31 May 2025