Back to Journals » Clinical Ophthalmology » Volume 16
Effects of COVID-19 on Intravitreal Injection Clinic After Lockdown
Authors Hsieh T, Gundlach BS, Ashrafzadeh S ![]() , Sarraf D, Tsui I
, Sarraf D, Tsui I
Received 22 February 2022
Accepted for publication 3 June 2022
Published 19 September 2022 Volume 2022:16 Pages 3089—3096
DOI https://doi.org/10.2147/OPTH.S358239
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Terry Hsieh,1 Bradley S Gundlach,2 Sahar Ashrafzadeh,2 David Sarraf,3,4 Irena Tsui3,5,6
1Stein Eye Institute, University of California, Los Angeles, CA, USA; 2David Geffen School of Medicine, University of California, Los Angeles, CA, USA; 3Ophthalmology Department, West Los Angeles Veterans Health Administration, Los Angeles, CA, USA; 4Retinal Disorders and Ophthalmic Genetics - Stein Eye Institute, University of California, Los Angeles, CA, USA; 5Retina Division - Stein Eye Institute, University of California, Los Angeles, CA, USA; 6Doheny Eye Institute, University of California, Los Angeles, CA, USA
Correspondence: Irena Tsui, Ophthalmology Department, West Los Angeles Veterans Health Administration, Los Angeles, CA, USA, Tel +1 310 825 7290, Fax +1 310 825 9946, Email [email protected]
Purpose: To examine the return of patients to intravitreal injection clinic after the COVID-19 lockdown.
Patients and Methods: The electronic medical records of all patients who received intravitreal injections at a tertiary care Veterans Health Administration (VHA) clinic 14 weeks post-lockdown (5/9/20-8/13/20) in Los Angeles County were reviewed. Reference groups included injection patients during the 7-week COVID-19 lockdown (3/19/20-5/8/20) and a 7-week pre-pandemic period in 2019 (3/19/19-5/8/19). Clinic volume was compared using a one-way ANOVA. Demographic data, medical and psychiatric co-morbidities, injection diagnoses, visual acuities, and clinic volumes were compared between the 3 periods using a generalized estimating equation multivariate analysis.
Results: The post-lockdown period group averaged 25.1 visits per week, compared with 12.3/week during lockdown and 25.4/week pre-COVID in intravitreal injection clinic. In the post-lockdown period, the VHA injection clinic returned closer to the pre-lockdown volume compared to the VHA comprehensive clinic (98.9% vs 57.4%, p < 0.001). Post-lockdown, COPD patients and organ transplant patients were less likely to receive injections compared to 2019 (OR 0.76 p = 0.008, OR 1.37 p < 0.0001, respectively). Patients with a diagnosis of cancer increased in proportion between the pre-pandemic and the post-lockdown periods (OR 1.31, p = 0.007). No differences were found, according to psychiatric co-morbidities. After lockdown, the proportion of patients receiving injections for diabetic macular edema (DME) increased (OR 1.11, p = 0.01).
Conclusion: Injection volume returned to pre-pandemic levels immediately after lockdown ended. However, patients with high-risk comorbidities did not return to intravitreal injection clinic post-lockdown. These results can inform medical organizations, which groups may need increased safety measures and targeted outreach to address their ophthalmic needs.
Keywords: age-related macular degeneration, anti-vascular endothelial growth factor, coronavirus, co-morbidities, diabetic retinopathy, retina
Introduction
The COVID-19 pandemic required physicians and patients to make difficult decisions about the urgency of ophthalmology care. Los Angeles County enforced a stay-at-home order (referred to as “lockdown”) early during the pandemic to minimize the spread of COVID-19.1 Clinics quickly adopted symptom screening algorithms, mask enforcement policies, and disinfection protocols.2,3 Many specialties pivoted into telemedicine visits to continue providing care; however, ophthalmology often requires in-person visits with an exam in close proximity.4,5 Intravitreal injection clinics add to that exposure risk as both the injection and the necessary retinal imaging, such as optical coherence tomography (OCT), must be performed within the recommended safe social distancing.6,7
Intravitreal injections are one of the most commonly performed ophthalmological procedure.8 Anti-vascular endothelial growth factor (anti-VEGF) injections are effective treatments for neovascular age-related macular degeneration (nvAMD) and diabetic macular edema (DME), two of the most common indications for injections. These conditions demand regular visits and often require consistent injection intervals to prevent permanent visual impairment.9,10 The high-risk medical comorbidities defined by the Centers for Disease Control and Prevention (CDC) for SARS CoV-2 infection overlap heavily with the patient population receiving intravitreal injections.11 During the lockdown, physicians were forced to triage vision-threatening conditions and allocate treatment based on the risk of permanent functional vision loss.12 On the other hand, patients also faced a difficult choice between losing vision versus risking serious COVID infection. COVID infections have also been linked to a broad range of ocular pathology, including posterior segment pathology. This wide array of uveal and retinal pathology has been reported to range from cotton wool spots and hemorrhages to optic neuritis, retinitis, panuveitis, and even vascular occlusions.13
We previously investigated both ophthalmic and non-ophthalmic factors during the COVID-19 lockdown period in Los Angeles County and found a decrease in patient volume by 50% along with an increased proportion of Hispanic patients, systemically healthier patients, and patients with a diagnosis of AMD compared with the year prior.14 In this current study, we sought to study similar factors in the intravitreal injection clinic in the period immediately after lockdown to identify ophthalmic trends in the post-lockdown era.
Materials and Methods
Data Collection and Subjects
This retrospective cohort study was approved by the Institutional Review Board of the Greater Los Angeles Veterans Health Administration (VHA). The veteran population is considered a vulnerable population due to increasing minority composition.15 Given the retrospective nature of this study, patient consent to review medical records was waived by the IRB. The IRB approval number is 2020–000187. Confidentiality of patient data was maintained, and this study was compliant with the Declaration of Helsinki.
Patient charts were reviewed using the VHA Computerized Patient Record System (CPRS). Data was collected from intravitreal injection clinic, comprehensive clinic, and retina clinic from the pre-lockdown (March 19th, 2019 to May 8th, 2019), lockdown (March 19th, 2020 to May 8th, 2020), and post-lockdown (May 9th, 2020 to August 13th, 2020) periods. Patient demographic information (eg age, gender, self-reported race, residential zip code, homeless status), ophthalmic status (eg visual acuity, diagnosis, indication for injection), and both medical and psychiatric co-morbidities [eg body mass index (BMI), hypertension, high-risk COVID-19 co-morbidities, mental health diagnoses] were collected. The medical conditions considered high-risk co-morbidities for COVID-19 disease by the Center for Disease Control and Prevention (CDC) were identified including cancer, chronic kidney disease, chronic obstructive pulmonary disease, heart conditions (defined as heart failure, coronary artery disease, cardiomyopathies, arrhythmias, or valvular insufficiencies), BMI (kg/m2), and type 2 diabetes.11 Associated psychiatric conditions, which have a higher prevalence among veterans than in the general population,16 including depression, anxiety, schizophrenia, schizoaffective disorder, post-traumatic stress disorder, psychosis, and others, were also recorded.
During the seven-week lockdown period of March 19th, 2020 to May 8th, 2020, patients were called one week in advance of their clinic appointments. Patients with decreased vision, any new vision complaints, or with a diagnosis of nvAMD or functional monocular status were encouraged to keep their appointments and come in for evaluation. Those with stable vision or other diagnoses [eg diabetic macular edema (DME), diabetic retinopathy (DR), retinal vein occlusion (RVO), or central serous retinopathy (CSR)] were encouraged to reschedule. Non-ophthalmic co-morbidities did not influence providers’ recommendations. Appointments were not canceled if the patient wanted to come in, regardless of diagnosis or vision. Patients in the same seven-week period from March 19th, 2019 to May 8th, 2019 served as a pre-pandemic control group. The 14-week period immediately following the lifting of the lockdown order from May 9th, 2020 to August 13th, 2020 served as the post-lockdown group.
Statistical Analysis
All patients who attended intravitreal injection clinic during the time periods listed above were included for statistical analysis. One-way Analysis of Variance (ANOVA) with Dunnett correction for multiple comparisons was performed to analyze the proportion of visits per week compared to pre-lockdown. A p-value <0.05 was considered to be statistically significant. Generalized Estimating Equations (GEE) routine was used for analysis to allow for inter-eye correlation and repeat measurements during each follow-up period. The GEE routine used a linear model to analyze the main effects between parameters using a robust estimator covariance matrix with an independent correlation structure. Parameter estimates (β) were used to calculate odds ratios (OR) with corresponding 95% confidence intervals (CI) and p-values. This routine was used to calculate ORs between two time periods, analyzing the rates of follow-up for each independent variable (demographic information, medical/psychiatric history, ophthalmic history) in a univariable model. This was repeated twice to calculate ORs for each combination of time periods. Bonferroni correction was applied to both analyses for two multiple comparisons: (1) pre- versus post-lockdown and (2) during versus post-lockdown. Thus, a p-value <0.025 was considered statistically significant due to multiple comparisons. A Pearson chi-square test between groups was used to compare the number of patients in each time period whose BMI > 30 or BMI > 40. Study data were managed using Research Electronic Data Capture (REDCap, Vanderbilt University, Nashville, TN). Matlab 2020a (Natick, MA, USA) was used for data handling and processing, and SPSS 27.0 (IBM Corp., Armonk, NY, USA) was used for statistical analysis.17,18
Results
The study sample included a total of 625 visits of 292 patients across all time periods. In the intravitreal injection clinic, the pre-, during, and post-lockdown period groups averaged 25.4, 12.3, and 25.1 visits per week, respectively. Table 1 shows the mean visits per week in the pre-, during, and post-lockdown periods for various clinics as well as percentage of volume in the post-lockdown period compared to the pre-lockdown period. The comprehensive clinic averaged 57.4% (95% CI 0.428–0.719), retina clinic 77.2% (95% CI 0.602–0.941), and injection clinic 98.8% (95% CI 0.857–1.12) of their “normal” volume in the post-lockdown period. In comparison to the injection clinic, the comprehensive clinic post-lockdown volume was significantly lower (p = 0.0003), while the retina clinic volume only trended towards significance (p = 0.0597). The mean ages of patients in the intravitreal injection clinic for the pre-, during, and post-lockdown periods were 74.3, 72.0, and 74.6 years, respectively. Demographic data for each time period are presented in Supplemental Table 1. No significant difference was found in the gender of the patients between the groups. The proportion of Hispanic patients trended toward more in the lockdown period than in post-lockdown (OR 1.13, p = 0.027). No other significant differences were found between groups for the proportion of those self-identified as White, Black, Asian, or Pacific Islander between each of the time periods (Figure 1).
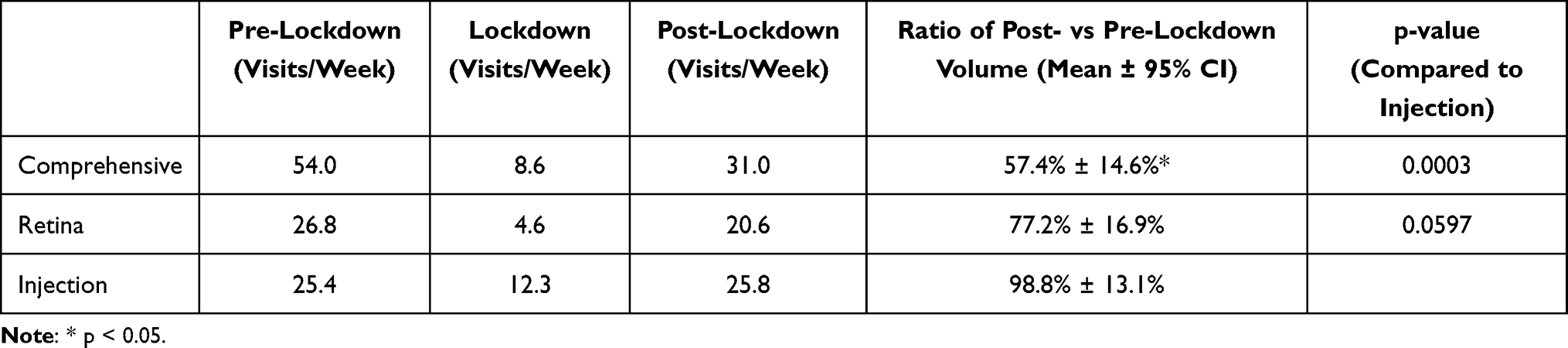 |
Table 1 Clinic Volume |
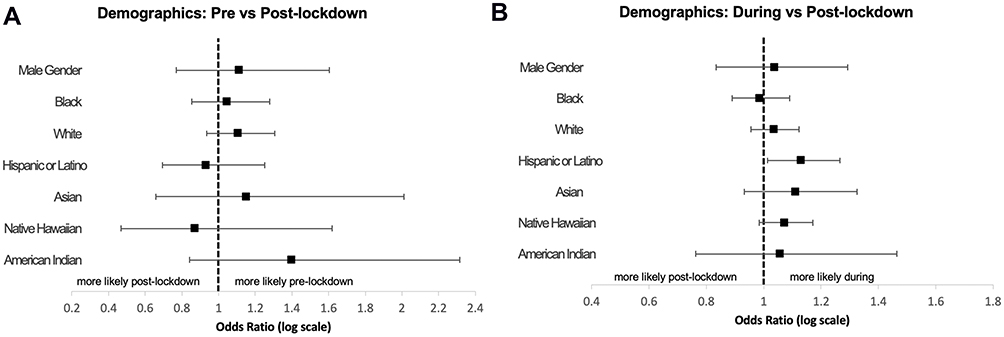 |
Figure 1 Odds ratios of demographic variables. No significant differences were found in demographics when comparing periods against the post-lockdown period (A). Demographic variables of pre- vs post-lockdown time periods (B). Demographic variables of during vs post-lockdown time periods. Significance set at p<0.025 to account for multiple comparisons. |
Medical and psychiatric co-morbidities of patients in each time period are provided in Supplemental Table 2. There was no significant difference in the mean BMI (Supplemental Table 2), presence of diabetes, or presence of chronic kidney disease in patients in each of the time periods (Figure 2). As the risk for COVID-19-related morbidity increases with BMI, a chi-square analysis was performed to compare the number of patients in each time period with obesity (BMI > 30) or severe obesity (BMI > 40). This analysis demonstrated no difference in the number of patients between each period (Supplemental Tables 3 and 4).11 Post-lockdown, COPD patients and organ transplant patients were less likely to receive injections compared to 2019 (OR post vs pre-lockdown 0.76 p = 0.008, OR 0.62 p < 0.0001, respectively) (Figure 2). In the pre-pandemic period, 11.2% of patients had a history of organ transplant, but during the lockdown period, zero patients with organ transplant history presented to clinic; after the lockdown, those patients comprised only 4.2% of the patient volume. Patients with cancer diagnoses comprised a lower proportion of pre-pandemic patients compared to post-lockdown patients (OR 0.77, p = 0.007).
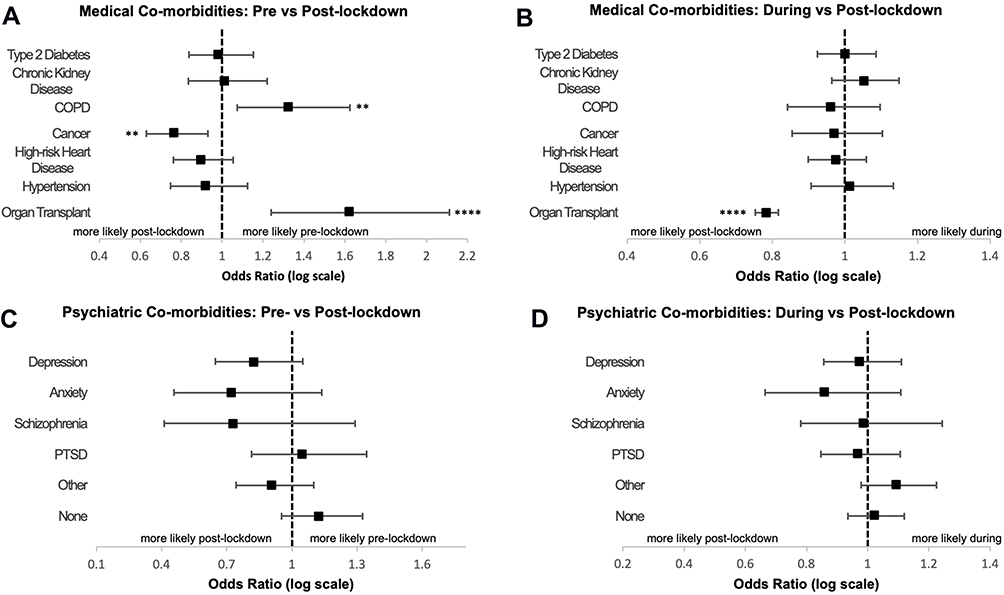 |
Figure 2 Odds ratios of medical and psychiatric co-morbidities. In the pre-lockdown period compared to the post-lockdown period, significantly more patients with COPD or organ transplants received intravitreal injections. Comparison of during vs post-lockdown periods showed significantly decreased patients with solid organ transplants. Patients with cancer were significantly increased in the post-lockdown period in comparison to pre-lockdown. No significant differences were found in the proportion of patients with psychiatric co-morbidities in either of the time period comparisons. (A) Medical co-morbidities of pre- vs post-lockdown time periods (B). Medical co-morbidities of during vs post-lockdown time periods (C). Psychiatric co-morbidities of pre- vs post-lockdown time periods (D). Psychiatric co-morbidities of during vs post-lockdown time periods. Significance set at p<0.025 to account for multiple comparisons. **p < 0.01. ****p < 0.0001. |
Our data showed no significant differences in the proportion of patients with psychiatric co-morbidities between the time periods, except for psychosis and schizoaffective disorder though there were very few patients in each group (n ≤ 3). The proportion of patients with depression trended toward a decrease from 20.2% in 2019 to 16.3% during lockdown to 14.1% in the post-lockdown period, but these differences were not significant. Similarly, patients with anxiety decreased from 7.3% to 5.8% to 4.2%, but these differences were not statistically significant.
Figure 3 and Supplemental Table 5 contain the proportion by indication for which patients received intravitreal injections during each time period. This analysis demonstrated no significant differences in patients receiving injections for nvAMD when comparing the pre- and post-lockdown periods or the during and post-lockdown periods (OR 0.98 and 0.91, respectively). After lockdown, the proportion of patients receiving injections for diabetic macular edema (DME) increased in the post-lockdown versus the lockdown period (OR for during vs post-lockdown 0.90 with reciprocal OR 1.11, p = 0.01) and was not significantly different from the “pre-pandemic” period (OR 0.95, p = 0.58). There were no other significant differences found among other indications for injections (eg RVO, CSR or pachychoroid, and other) between the time periods.
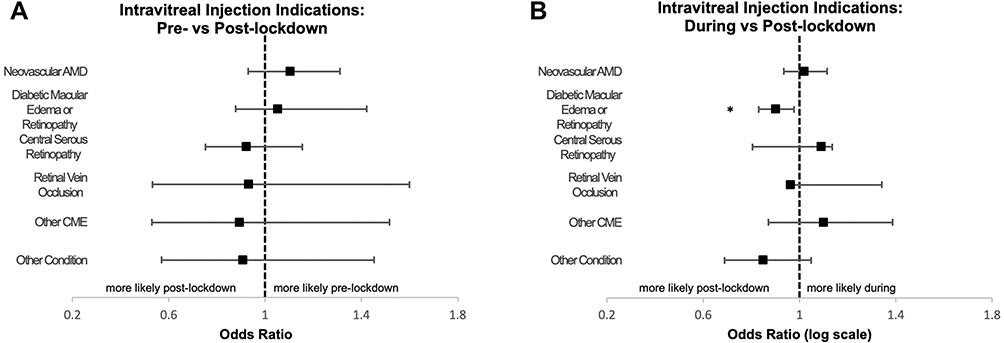 |
Figure 3 Odds ratios of indications for intravitreal injections. Comparison of during vs post-lockdown period showed a significant decrease in the proportion of patients receiving intravitreal injections for diabetic indications during lockdown. There were no significant differences found in the indications for intravitreal injections between pre- and post-lockdown time periods (A). Indications for injections of pre- vs post-lockdown time periods (B). Indications for injections of during vs post-lockdown time periods. Significance set at p<0.025 to account for multiple comparisons. *p < 0.025. |
Discussion
The COVID-19 lockdown, an unprecedented event, was unsustainable, as businesses and healthcare institutions suffered remarkable financial losses and in some cases, operational insolvency.19,20 Despite the lockdown ending in May of 2020, COVID-19 was still a palpable threat without the availability of a vaccine at that time. Physicians and patients had little guidance on how to proceed in the post-lockdown era while still needing to maintain precautionary measures. This study showed that immediately after lockdown, the VHA intravitreal injection clinic returned to its pre-COVID-19 volume but was comprised of systemically healthier patients seeking treatment. Furthermore, there was a rebound in the number and proportion of diabetic patients who had delayed injections during lockdown.
Interestingly, our previous study demonstrated a significant rise in the Latino/Hispanic proportion of patients in injection clinic during the lockdown, which was not true after restrictions were lifted.14 Our previous theory was that Hispanic patients tend to live in multigenerational housing and have a higher proportion of essential workers, which would increase the exposure risk to COVID-19. Though we cannot exactly determine why there was such a difference, we speculate that much higher COVID-19 infection and death rates in the Latino/Hispanic population during March and April21 may have caused this vulnerable population to take more precautions and stay at home in May and June even after the lockdown was lifted.
Our data demonstrate that although overall injection clinic volume returned to baseline after lockdown, even faster than other ophthalmology clinics, patients with COPD and solid organ transplants, both high-risk co-morbidities, were less likely to return to clinic post-lockdown. It makes sense that these groups chose to limit their exposure given the significantly increased mortality and hospitalization risk if infected with COVID-19. It is important for ophthalmologists to be aware of this trend to identify patients with high-risk systemic co-morbidities and accommodate their safe return to intravitreal injection clinic for continued vision care.22 Our data contained a significant proportion of diabetic patients in the intravitreal injection clinic during each period. As diabetes causes widespread microangiopathy, other studies have demonstrated that diabetic retinopathy and nephropathy can be frequently associated and correlate in severity.23–26 Attendance in injection clinic by diabetics and patients with chronic kidney disease was not significantly different between periods in our study. Since our data suggest that these patients are likely to continue physician visits even during lockdown measures, it is important that these patients be referred for multifactorial diabetes management to reduce their cardiovascular and overall mortality, especially with emerging data demonstrating long-term elevated cardiovascular risk.25,27
Veterans have a higher incidence of psychiatric co-morbidities and that the pandemic may represent a factor destabilizing mental health, we hypothesized that these patients would be most affected during the pandemic.16 Other studies have shown that the pandemic increased anxiety and depression, as well as creating difficulties in accessing mental health care.28,29 There were statistical differences in those diagnosed with psychosis or schizoaffective, but we caution limited extrapolation given the very small number of patients. Our data showed that there were no significant differences in intravitreal clinic visits among those with a diagnosis of depression or anxiety. This may reflect the accessibility and high quality of mental healthcare within the Veteran healthcare system.
Injection and clinic volumes fell both nationally and worldwide as lockdown measures were enforced.30–34 While the VHA injection clinic returned to pre-pandemic volumes in the post-lockdown period, comprehensive and retina clinics at the same site continued to have a decreased volume of about 50%. Our facility opened the standard scheduling grids for these clinics in the post-lockdown period. This demonstrates the priority that both physicians and patients placed on continuing intravitreal injections as a delay in injections can lead to permanent vision loss. Other studies have demonstrated that pandemic-induced delays in care are associated with worse visual outcomes in patients who need injections for treatment across all types of diagnoses.35–38 Furthermore, one center reported a significant rise in large submacular hemorrhages as a result of the lockdown.39 Therefore, we are encouraged that injection clinic was able to rebound back to pre-lockdown volumes so quickly.
As with many other groups, we prioritized those with nvAMD over RVO and diabetic indications for injection during the lockdown period.12,33,40 Our results support that nvAMD patients are continuing their treatments during and after the lockdown. Previous randomized trials of patients with DME show that treatment can be delayed in eyes with good visual acuity.41 Telemedicine has been shown to be efficacious in the diagnosis and management of diabetic retinopathy.26,42 Spurred on by the pandemic, telemedicine could offer increased access to care and decentralized monitoring of diabetic retinopathy or macular edema patients via physician review of images instead of face-to-face visits during lockdown times.43 However, post-pandemic studies have demonstrated delays in care resulted in worse short-term visual outcomes for diabetic retinopathy.37,44 Therefore, we view it favorably that immediately after we stopped the triage process post-lockdown, there was a rebound increase in patients receiving injections for diabetic indications, and we expect more to have returned in the post-vaccine area.
Strengths and Limitations
This study examined a racially diverse and often underserved, urban population with a high prevalence of medical and psychiatric co-morbidities from a composite EMR. Other studies have examined the visual acuity outcomes, clinic volumes, or indications for injection during the pandemic period, but to our knowledge, this study is the first to analyze and report on the co-morbidities of the patients in the post-lockdown era. A major limitation of this study may be related to ascertainment bias due to the retrospective nature of the study. The cohort studied was predominantly male, as this was a VHA-based study, which may not be representative of the general population. While this was a single-institution study, the West Los Angeles Veterans Affairs ophthalmology clinic is a tertiary care center providing intravitreal injections for a large catchment area and multiple satellite clinics across Southern California.
Future Directions
This study can be expanded into the post-vaccine era along with COVID variant-induced spikes to see whether repeated COVID surges continue to affect patient and physician decision-making on intravitreal injection clinics. Furthermore, during future pandemics, this study and its framework can be used as a starting point to identify at-risk patients when access to ophthalmological care becomes limited.
Conclusion
Intravitreal injection clinic volume rebounded to pre-pandemic levels immediately following the state-mandated COVID-19 lockdown period in the spring of 2020, while other clinics continued at half of their pre-COVID-19 volume. However, patients with high-risk medical co-morbidities were less likely to return to the post-lockdown injection clinic, increasing their risk of permanent vision loss. These results can be used to appropriately allocate clinic resources towards injection clinic and determine which groups may need increased safety measures and targeted outreach to address their fears about returning to clinic and their ophthalmic needs.
Disclosure
Dr David Sarraf reports grants, personal fees from Amgen, personal fees from Bayer, grants from Boehringer, grants from Genentech, non-financial support from Heidelberg, personal fees from Iveric Bio, personal fees from Novartis, grants, personal fees, non-financial support from Optovue, grants from Regeneron, non-financial support from Topcon, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. COVID-19 Orders. Los Angeles mayor website for COVID-19 orders. Available from: https://www.lamayor.org/COVID19Orders.
2. Syed AAO, Jahan S, Aldahlawi AA, Alghazzawi EA. Preventive practices of ophthalmologists during COVID-19 pandemic. Clin Ophthalmol. 2021;15:1267–1275. doi:10.2147/OPTH.S295730
3. Safadi K, Kruger JM, Chowers I, et al. Ophthalmology practice during the COVID-19 pandemic. BMJ Open Ophthalmol. 2020;5(1):e000487. doi:10.1136/bmjophth-2020-000487
4. Chao GF, Li KY, Zhu Z, et al. Use of telehealth by surgical specialties during the COVID-19 pandemic. JAMA Surg. 2021;156(7):620–626. doi:10.1001/jamasurg.2021.0979
5. Johnson C, Taff K, Lee BR, Montalbano A. The rapid increase in telemedicine visits during COVID-19. Patient Exp J. 2020;7(2):72–79. doi:10.35680/2372-0247.1475
6. Shabto JM, De Moraes CG, Cioffi GA, Liebmann JM. Review of hygiene and disinfection recommendations for outpatient glaucoma care: a COVID era update. J Glaucoma. 2020;29(6):409–416. doi:10.1097/IJG.0000000000001540
7. American Academy of Ophthalmology. Coronavirus (COVID-19) American Academy of Ophthalmology Update. Coronavirus (COVID-19); 2021. Available from: https://eyewiki.aao.org/Coronavirus_(COVID-19)#Non-essential_imaging.2Ftesting_should_be_deferred.2C_and_equipment_use_should_be_kept_at_a_minimum.
8. Williams GA. IVT injections: health policy implications. Available from: https://www.reviewofophthalmology.com/article/ivt-injections-health-policy-implications.
9. Ramakrishnan MS, Yu Y, VanderBeek BL. Visit adherence and visual acuity outcomes in patients with diabetic macular edema: a secondary analysis of DRCRnet Protocol T. Graefes Arch Clin Exp Ophthalmol. 2021;259(6):1419–1425. doi:10.1007/s00417-020-04944-w
10. Framme C, Eter N, Hamacher T, et al. Aflibercept for patients with neovascular age-related macular degeneration in routine clinical practice in Germany: twelve-month outcomes of PERSEUS. Ophthalmol Retina. 2018;2(6):539–549. doi:10.1016/j.oret.2017.09.017
11. Centers for Disease Control and Prevention. People at increased risk: people with certain medical conditions. Available from: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.html.
12. Korobelnik JF, Loewenstein A, Eldem B, et al. Anti-VEGF intravitreal injections in the era of COVID-19: responding to different levels of epidemic pressure. Graefes Arch Clin Exp Ophthalmol. 2021;259(3):567–574. doi:10.1007/s00417-021-05097-0
13. Sanjay S, Agrawal S, Jayadev C, et al. Posterior segment manifestations and imaging features post-COVID-19. Med Hypthesis Discov Innov Ophthalmol. 2021;10(3):95–106. doi:10.51329/mehdiophthal1427
14. Ashrafzadeh S, Gundlach BS, Tsui I. The impact of non-ophthalmic factors on intravitreal injections during the COVID-19 lockdown. Clin Ophthalmol. 2021;15:3661–3668. doi:10.2147/OPTH.S314840
15. Health Equity. Veterans affairs office of research & development. Available from: https://www.research.va.gov/topics/health_equity.cfm.
16. Hoerster KD, Lehavot K, Simpson T, McFall M, Reiber G, Nelson KM. Health and health behavior differences: u.S. Military, veteran, and civilian men. Am J Prev Med. 2012;43(5):483–489. doi:10.1016/j.amepre.2012.07.029
17. MATLAB Mathworks Version R2021a
18. IBM SPSS statistics for Windows. Version 27.0; 2020.
19. Barnett ML, Mehrotra A, Landon BE. Covid-19 and the upcoming financial crisis in health care. NEJM Catalyst Innov Care Delivery; 2020;1(2):45.
20. Coibion O, Gorodnichenko Y, Weber M. The cost of the Covid-19 crisis: lockdowns, macroeconomic expectations, and consumer spending. Nat Bur Econ Res. 2020. doi:10.3386/w27141
21. County of Los Angeles Department of Public Health. COVID-19 surveillance dashboard. Available from: http://dashboard.publichealth.lacounty.gov/covid19_surveillance_dashboard/.
22. Centers for Disease Control and Prevention. When you’ve been fully vaccinated. Available from: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/fully-vaccinated.html.
23. Minutolo R, Gabbai FB, Provenzano M, et al. Cardiorenal prognosis by residual proteinuria level in diabetic chronic kidney disease: pooled analysis of four cohort studies. Nephrol Dial Transpl. 2018;33(11):1942–1949. doi:10.1093/ndt/gfy032
24. Minutolo R, Sasso FC, Chiodini P, et al. Management of cardiovascular risk factors in advanced type 2 diabetic nephropathy: a comparative analysis in nephrology, diabetology and primary care settings. J Hypertens. 2006;24(8):1655–1661. doi:10.1097/01.hjh.0000239303.93872.31
25. Sasso FC, Chiodini P, Carbonara O, et al. High cardiovascular risk in patients with Type 2 diabetic nephropathy: the predictive role of albuminuria and glomerular filtration rate. The NID-2 Prospective Cohort Study. Nephrol Dial Transplant. 2012;27(6):2269–2274. doi:10.1093/ndt/gfr644
26. Sasso FC, Pafundi PC, Gelso A, et al. Relationship between albuminuric CKD and diabetic retinopathy in a real-world setting of type 2 diabetes: findings from No blind study. Nutr Metab Cardiovasc Dis. 2019;29(9):923–930. doi:10.1016/j.numecd.2019.05.065
27. Xie Y, Xu E, Bowe B, Al-Aly Z. Long-term cardiovascular outcomes of COVID-19. Nat Med. 2022;28(3):583–590. doi:10.1038/s41591-022-01689-3
28. Xiong J, Lipsitz O, Nasri F, et al. Impact of COVID-19 pandemic on mental health in the general population: a systematic review. J Affect Disord. 2020;277:55–64. doi:10.1016/j.jad.2020.08.001
29. Sarraf D, Sarraf DR, Sadda S. Is virtual existence our new reality? Graefes Arch Clin Exp Ophthalmol. 2020;258(7):1357–1358. doi:10.1007/s00417-020-04750-4
30. Xu D, Starr MR, Boucher N, et al. Real-world vitreoretinal practice patterns during the 2020 COVID-19 pandemic: a nationwide, aggregated health record analysis. Curr Opin Ophthalmol. 2020;31(5):427–434. doi:10.1097/ICU.0000000000000692
31. Leng T, Gallivan MD, Kras A, et al. Ophthalmology and COVID-19: the impact of the pandemic on patient care and outcomes—An IRIS® registry study. Ophthalmology. 2021;128:1782–1784. doi:10.1016/j.ophtha.2021.06.011
32. El Hamichi S, Gold A, Heier J, Kiss S, Murray TG. Impact of the COVID-19 pandemic on essential vitreoretinal care with three epicenters in the United States. Clin Ophthalmol. 2020;14:2593–2598. doi:10.2147/OPTH.S267950
33. Borrelli E, Grosso D, Vella G, et al. Impact of COVID-19 on outpatient visits and intravitreal treatments in a referral retina unit: let’s be ready for a plausible “rebound effect.”. Graefes Arch Clin Exp Ophthalmol. 2020;258(12):2655–2660. doi:10.1007/s00417-020-04858-7
34. Dulger SC, Citirik M, Camgoz EB, Teke MY. Intravitreal injections during the COVID-19 pandemic era. Med Hypothesis, Discov Innov Opt. 2021;2(2):50–55. doi:10.51329/mehdioptometry125
35. Borrelli E, Grosso D, Vella G, et al. Short-term outcomes of patients with neovascular exudative AMD: the effect of COVID-19 pandemic. Graefes Arch Clin Exp Ophthalmol. 2020;258(12):2621–2628. doi:10.1007/s00417-020-04955-7
36. Elfalah M, AlRyalat SA, Toro MD, et al. Delayed intravitreal anti-VEGF therapy for patients during the COVID-19 lockdown: an ethical endeavor. OPTH. 2021;15:661–669. doi:10.2147/OPTH.S289068
37. Naravane AV, Mundae R, Zhou Y, et al. Short term visual and structural outcomes of anti-vascular endothelial growth factor (anti-VEGF) treatment delay during the first COVID-19 wave: a pilot study. PLoS One. 2021;16(2):e0247161. doi:10.1371/journal.pone.0247161
38. Yeter DY, Dursun D, Bozali E, Ozec AV, Erdogan H. Effects of the COVID-19 pandemic on neovascular age-related macular degeneration and response to delayed Anti-VEGF treatment. J Fr Ophtalmol. 2021;44(3):299–306. doi:10.1016/j.jfo.2021.02.001
39. Romano F, Monteduro D, Airaldi M, et al. Increased number of submacular hemorrhages as a consequence of coronavirus disease 2019 lockdown. Ophthalmol Retina. 2020;4(12):1209–1210. doi:10.1016/j.oret.2020.06.027
40. Carnevali A, Giannaccare G, Gatti V, Scuteri G, Randazzo G, Scorcia V. Intravitreal injections during COVID-19 outbreak: real-world experience from an Italian tertiary referral center. Eur J Ophthalmol. 2021;31(1):10–12. doi:10.1177/1120672120962032
41. Baker CW, Glassman AR, Beaulieu WT, et al. Effect of initial management with aflibercept vs laser photocoagulation vs observation on vision loss among patients with diabetic macular edema involving the center of the macula and good visual acuity: a randomized clinical trial. JAMA. 2019;321(19):1880–1894. doi:10.1001/jama.2019.5790
42. Sasso FC, Pafundi PC, Gelso A, et al. High HDL cholesterol: a risk factor for diabetic retinopathy? Findings from NO BLIND study. Diabetes Res Clin Pract. 2019;150:236–244. doi:10.1016/j.diabres.2019.03.028
43. Galiero R, Pafundi PC, Nevola R, et al. The importance of telemedicine during COVID-19 pandemic: a focus on diabetic retinopathy. J Diabetes Res. 2020;2020:e9036847. doi:10.1155/2020/9036847
44. Ashkenazy N, Goduni L, Smiddy WE. Short-term effects of COVID-19-related deferral of intravitreal injection visits. OPTH. 2021;15:413–417. doi:10.2147/OPTH.S296345
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Towards a Device Agnostic AI for Diabetic Retinopathy Screening: An External Validation Study
Rao DP, Sindal MD, Sengupta S, Baskaran P, Venkatesh R, Sivaraman A, Savoy FM
Clinical Ophthalmology 2022, 16:2659-2667
Published Date: 17 August 2022
Glaucoma Drainage Device Erosions in Patients Receiving Anti-Vascular Endothelial Growth Factor Therapy for Diabetic Retinopathy
Islam YFK, Vanner EA, Maharaj ASR, Schwartz SG, Kishor K
Clinical Ophthalmology 2022, 16:3681-3687
Published Date: 9 November 2022
Considerations for the Identification and Management of Geographic Atrophy: Recommendations from an Expert Panel
Regillo CD, Nijm LM, Shechtman DL, Kaiser PK, Karpecki PM, Ryan EH, Ip MS, Yeu E, Kim T, Rafieetary MR, Donnenfeld ED
Clinical Ophthalmology 2024, 18:325-335
Published Date: 2 February 2024
Non-Linear Relationship Between Fasting C-Peptide and Retinopathy in Patients with Type 2 Diabetes Mellitus - A Retrospective Study
Ma J, Han C, Lv Y, Cai H
Diabetes, Metabolic Syndrome and Obesity 2025, 18:1035-1045
Published Date: 7 April 2025
Targeting Senescence, Oxidative Stress, and Inflammation: Quercetin-Based Strategies for Ocular Diseases in Older Adults
Medoro A, Davinelli S, Scuderi L, Scuderi G, Scapagnini G, Fragiotta S
Clinical Interventions in Aging 2025, 20:791-813
Published Date: 7 June 2025