Back to Journals » Clinical Ophthalmology » Volume 16
Glaucoma Drainage Device Erosions in Patients Receiving Anti-Vascular Endothelial Growth Factor Therapy for Diabetic Retinopathy
Authors Islam YFK ![]() , Vanner EA
, Vanner EA ![]() , Maharaj ASR, Schwartz SG
, Maharaj ASR, Schwartz SG ![]() , Kishor K
, Kishor K
Received 17 August 2022
Accepted for publication 2 November 2022
Published 9 November 2022 Volume 2022:16 Pages 3681—3687
DOI https://doi.org/10.2147/OPTH.S386033
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Yasmin Florence Khodeja Islam, Elizabeth A Vanner, Arindel SR Maharaj, Stephen G Schwartz, Krishna Kishor
Bascom Palmer Eye Institute, Department of Ophthalmology, University of Miami Miller School of Medicine, Miami, FL, USA
Correspondence: Krishna Kishor, Bascom Palmer Eye Institute, 7101 Fairway Drive, Palm Beach Gardens, Miami, FL, 33418, USA, Tel +1 561-515-1500, Fax +1 561-515-1588, Email [email protected]
Purpose: To determine if intravitreal anti-vascular endothelial growth factor (anti-VEGF) injections are associated with an increased risk of glaucoma drainage device (GDD) erosions.
Patients and Methods: A retrospective chart review was conducted including patients with diabetic retinopathy and had a GDD implanted at a large academic institution. The rate of GDD erosions was compared between eyes that did or did not receive intravitreal anti-VEGF injections. A subanalysis was also performed the relationship between diabetic macular edema (DME) and intravitreal steroid injections and GDD erosions.
Results: A total of 677 eyes from 608 patients was included. A total of 447 eyes received at least one anti-VEGF injection; 230 eyes never received such therapy. Twenty eyes (4.5%) receiving anti-VEGF had at least one erosion event, compared to 7 eyes (3.0%) of patients not receiving anti-VEGF therapy (OR 1.49, p=0.37). Diabetic macular edema was associated with a significantly increased rate of erosion in eyes not receiving anti-VEGF (71.4% versus 31.4%, p=0.034), but not in eyes receiving anti-VEGF (30.0% versus 40.7%, p=0.34). Receiving more than one specific anti-VEGF agent, an increased frequency or total number of anti-VEGF injections, or receiving intravitreal steroids were not associated with an increased risk of erosion (p> 0.05).
Conclusion: In patients with diabetic retinopathy, the use of anti-VEGF does not result in an increased rate of GDD erosions or recurrent erosions. Further research is needed over a longer follow-up period to determine if longer or more frequent anti-VEGF treatment is a risk factor for recurrent erosions.
Keywords: diabetic retinopathy, glaucoma drainage device, tube erosion, anti-vascular endothelial growth factor
Introduction
Glaucoma drainage devices (GDDs) are increasingly used to control glaucoma in patients with various diseases. Erosions, in which the GDD tube and/or plate become exposed, occur in approximately 5% of implants within the first five years after implantation;1 these GDDs need to be promptly revised or explanted to reduce the risk of endophthalmitis.2 Known risk factors for erosion include topical steroid use, uveitis, use of donor cornea or pericardium to cover the GDD during implantation, prior ocular surgery, female gender, older age, Caucasian race, and placing the GDD in an inferior quadrant of the eye.3–6 A history of diabetes mellitus has not been associated with an increased risk of GDD exposure.4,7,8 However, these studies did not specifically investigate diabetic retinopathy or treatment of diabetic retinopathy (intravitreal steroids and anti-vascular endothelial growth factor (anti-VEGF) agents) as risk factors for exposure.
Liu et al examined the rate of GDD erosions in patients receiving anti-VEGF injections in the treatment of neovascular age-related macular degeneration (AMD). They reported that patients receiving anti-VEGF had similar total rates of GDD erosions, but there was a significantly higher rate of recurrent erosions among patients receiving anti-VEGF, with patients receiving anti-VEGF for neovascular AMD experiencing an average of 2.1 erosion events compared to 1.3 in patients with non-neovascular AMD not receiving anti-VEGF.9 Miraftabi et al also described two cases of combined subconjunctival anti-VEGF with GDD implantation that resulted in GDD exposure.10 The mechanism of GDD exposure after anti-VEGF is unclear but could be multifactorial. First, manipulation and trauma to the conjunctiva can result in conjunctival erosion and subsequent GDD exposure. Second, the anti-VEGF medication can alter wound healing and reduce scar formation, and thus use of anti-VEGF may make an erosion more likely. However, further studies in this field are necessary to elucidate the precise mechanism in which anti-VEGF intravitreal injections may increase the rate of GDD erosion.9,10
The present study compares the rates of GDD erosion between patients receiving intravitreal anti-VEGF and those not receiving anti-VEGF for the treatment of diabetic retinopathy. A subgroup analysis was performed for patients also receiving intravitreal steroids for the treatment of diabetic retinopathy. As prior studies have demonstrated that anti-VEGF for other indications increases the rate of GDD erosions, we hypothesize that the same will hold true for anti-VEGF treatment for diabetic retinopathy. Similarly, since topical steroids have been associated with an increased rate of GDD erosions in prior studies, we hypothesize that intravitreal steroids will also increase this risk.3–6,9,10
Methods
Retrospective Chart Review
A retrospective chart review was performed, identifying all patients who had a GDD placed and were treated for diabetic retinopathy at our institution between 2014–2021. To be included, patients must have had a GDD implanted at the University of Miami/Bascom Palmer Eye Institute and also been diagnosed with at least mild diabetic retinopathy, as determined by clinical examination. Patients must have been at least eighteen years old at the time of implantation; all genders were included. All models of GDD, including Ahmed, Molteno, and Baerveldt versions, were included. When treatment for diabetic retinopathy was indicated, patients were offered anti-VEGF injections and/or panretinal photocoagulation, when appropriate. Treatment decisions were made based on clinician and patient preference. Patients were excluded from this study if their GDD was placed outside of our institution, or the patient did not have any level of diabetic retinopathy.
Patient charts were reviewed for prior surgical history, number and type of anti-VEGF treatments, location and type of GDD, and whether an intravitreal steroid was administered. Not all physicians recorded the quadrant of anti-VEGF injection, so this was not analyzed. If it had been more than two years since the last anti-VEGF injection prior to the patient presenting for GDD exposure, they were analyzed in the group not receiving anti-VEGF injections. Visual acuity was measured using Snellen charts, and intraocular pressure was obtained via applanation except in cases of severe corneal disease resulting in unreliable applanation; in these cases, rebound tonometry was utilized.
Approval was obtained from the University of Miami Institutional Review Board (approval number 20100785) and this study adhered to the guidelines of the Declaration of Helsinki. The Institutional Review Board deemed that the study was exempt from requiring additional approval from study subjects due to the noninvasive and retrospective nature of the study. Patient records were de-identified prior to data analysis, and no potentially identifying information is released in this study.
Statistical Analysis
Descriptive statistics for categorical variables include counts and percentages and for continuous variables include means and ranges. Group differences for categorical variables were assessed with Pearson chi-square or Fisher exact tests, and the Mann–Whitney Wilcoxon two-sample test was used for the continuous variables (none of which was normally distributed). The odds ratio for erosion and anti-VEGF treatment was calculated using a generalized mixed model. A one-sample t-test and a one-sample binomial test were used to compare out results to those of a previous study. All analyses were done using SAS version 9.4 software (SAS Institute, Cary, NC, USA). A p-value < 0.05 was considered statistically significant.
Results
A total of 677 eyes from 608 patients was included. The characteristics of patients included in the study are depicted in Table 1. A total of 447 eyes received at least one dose of anti-VEGF therapy; 230 eyes never received such therapy. One or more erosions occurred in 4.5% of patients receiving anti-VEGF therapy, compared to 3.0% of patients not receiving anti-VEGF therapy. The odds ratio for erosion for eyes receiving anti-VEGF was 1.49 (95% CI 0.65–3.85, p=0.37), but this was not statistically significant.
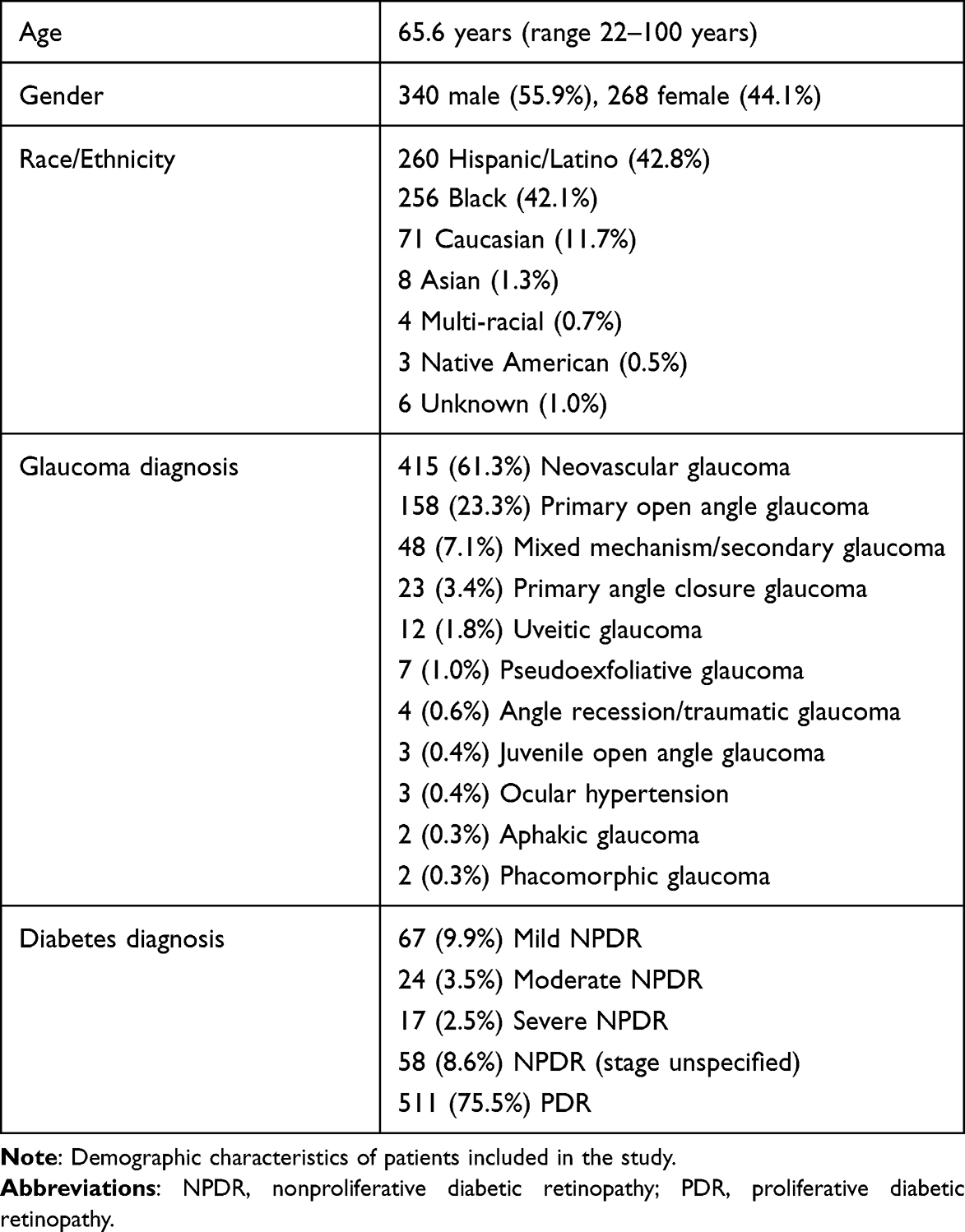 |
Table 1 Demographic Characteristics |
In patients who had GDD exposure, 44.4% underwent primary explanation, whereas the remaining 55.6% underwent revision upon the first exposure. Of the revisions, 33.3% used a scleral patch graft during revision surgery, 33.3% used a corneal patch graft, 6.7% used a pericardial patch graft, and 26.7% did not use a patch graft because the tube was tunneled through the sclera, effectively burying it. Twenty percent of those initially revised ultimately required removal due to re-exposure and/or endophthalmitis.
Tables 2 and 3 list the various ocular characteristics and risk factors for erosion between eyes that received anti-VEGF but did not have an erosion, those that did not receive anti-VEGF and did not have an erosion, those that received anti-VEGF and had at least one erosion event, and those that did not receive anti-VEGF but had at least one erosion event. The most common glaucoma diagnosis in both groups receiving anti-VEGF was neovascular glaucoma, while primary open angle glaucoma was the most common diagnosis in those not receiving anti-VEGF. The vast majority of GDDs were placed superotemporally (85–95% in all groups), but the type of patch graft used varied between groups. Most patients in all groups were pseudophakic. On average, the mean (range) time from last anti-VEGF injection to GDD erosion was 4.4 (range 0.25 to 25) months.
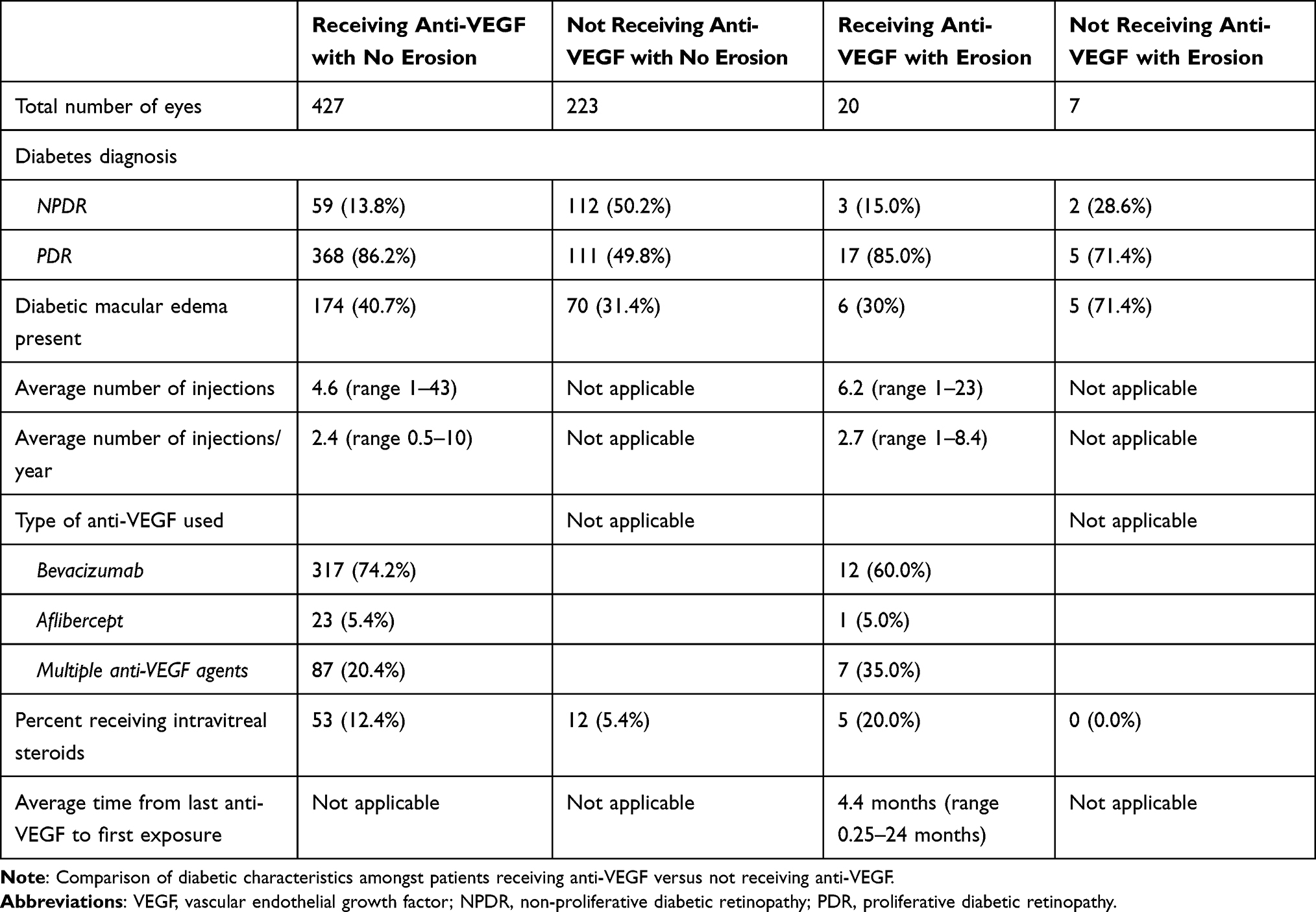 |
Table 2 Comparison of Diabetic Characteristics Amongst Patients with Receiving Anti-Vascular Endothelial Growth Factor (Anti-VEGF) versus Not Receiving Anti-VEGF |
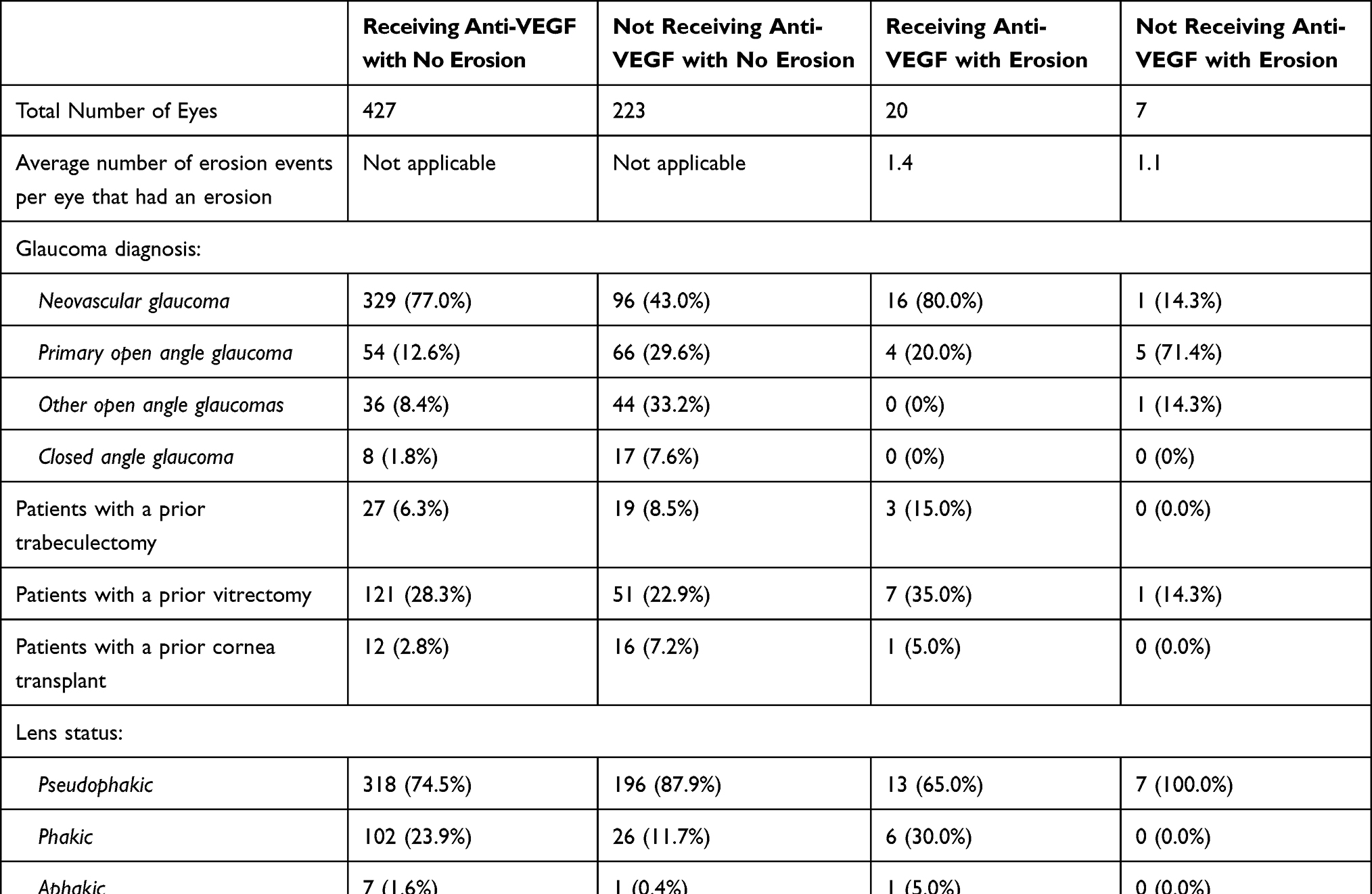 |
Table 3 Comparison of Glaucoma and Surgical Characteristics Amongst Patients with Receiving Anti-Vascular Endothelial Growth Factor (Anti-VEGF) versus Not Receiving Anti-VEGF |
The average number of intravitreal injections per year was similar between eyes receiving anti-VEGF who did not develop an erosion compared to those who did (2.4 versus 2.7, p=0.45), and the average total number of injections was similar (4.6 versus 6.2, p=0.87). There was no statistically significant difference between the number of erosion events per eye between eyes that received anti-VEGF and had at least one erosion compared to the eyes that did not receive anti-VEGF and had at least one erosion (1.5 versus 1.1, p=0.57).
The rates of diabetic macular edema (DME), as defined by fluid noted on clinical examination and/or macular optical coherence tomography, were significantly different between eyes that did not receive anti-VEGF and did not have an erosion compared to those that did have an erosion (70 eyes out of 223, or 31.4%, versus 5 eyes out of 7, or 71.4%, p=0.034). However, DME rates were similar between eyes that received anti-VEGF that did not have an erosion compared to those that did (40.7% versus 30.0%, p=0.34). Receiving more than one type of anti-VEGF was not a risk factor for erosion (20.4% in eyes that did not have an erosion versus 35.0% in eyes that did have an erosion, p=0.25).
Intravitreal steroid use was not associated with an increased risk of erosion; the rates of intravitreal steroid use in eyes that received anti-VEGF and did not have an erosion was 12.4% compared to 20.0% in eyes receiving anti-VEGF that did have an erosion (p=0.30). Similarly, the rate of intravitreal steroid use was 5.4% in eyes that did not receive anti-VEGF and did not have an erosion compared to 0.0% in eyes that did not receive anti-VEGF and did have an erosion (p=1.0). The timing of intravitreal steroid administration varied between patients; some received them concomitantly with anti-VEGF treatment, some in-between anti-VEGF treatments, and others without any anti-VEGF treatment.
Discussion
In this series, intravitreal anti-VEGF therapy was not associated with an increased risk of GDD erosion. Similarly, the number of GDD erosions per eye was not higher in eyes that had an erosion between eyes receiving anti-VEGF and not receiving anti-VEGF therapy. There is only one other study evaluating GDD erosions in patients receiving anti-VEGF; Liu et al reported that anti-VEGF therapy for neovascular AMD was associated with a higher rate of recurrent erosions. However, they also reported that the overall rate of erosions was similar between eyes receiving anti-VEGF and those that did not.9
It is unclear why anti-VEGF treatment for AMD would be associated with an increased risk of recurrent erosion, but anti-VEGF therapy for diabetic retinopathy was not. In terms of demographics, the present study contained fewer Caucasian patients (11.7%) than Liu et al’s study (78%, p < 0.001). Caucasian race is associated with a higher rate of GDD erosions,9,11 so this difference may have affected the results. Additionally, the present cohort was younger, with an average of 66 years compared to over 75 years (p < 0.001) in the Liu et al study; older age is also a reported risk factor for GDD erosions.11 Patients in the prior study received anti-VEGF therapy on average every six weeks, whereas in the present study, patients received an injection on average every twenty-two weeks. Similarly, the average time from last anti-VEGF injection to GDD exposure was 1.5 months in the prior study, compared to 4.4 months in the current study.9 Nonetheless, this study further supports their finding that anti-VEGF therapy itself is not associated with an increased rate of overall GDD erosions.
The presence of DME was associated with an increased rate of GDD erosions in patients not receiving anti-VEGF in this study, but not in those receiving anti-VEGF. However, this subgroup analysis was relatively small compared to the entire cohort, and thus further dedicated studies would be needed to confirm this observation. Imazeki et al reported that anti-VEGF therapy for DME decreases the inflammatory effects of DME;12 this may explain why DME was associated with an increased rate of GDD erosions in patients receiving anti-VEGF therapy.
Topical steroid use has previously been associated with an increased risk of GDD exposure;4,13 however, prior studies have not evaluated the effect of intravitreal steroids on the rate of GDD exposure. To our knowledge, this is the first study that evaluates the risk of GDD exposure amongst patients receiving intravitreal steroids; interestingly, unlike topical steroid use, intravitreal steroid use is not associated with an increased risk of erosion. This suggests that the risk of erosion from steroid use may be related to local conjunctival effects.13,14 However, like the DME subanalysis, the number of patients in this group was relatively small, and thus this observation needs to be confirmed.
Limitations of this study include the relatively small number of eyes with GDD erosions as compared to the number of eyes that did not have GDD erosions; this reflects the relatively low rate of GDD erosions. This is also related to the relatively short follow-up after GDD placement; the average length of time since the GDD was placed was approximately three years in all groups. Many studies on GDD outcomes rates have longer follow-up, although the prior study evaluating GDD erosions after anti-VEGF treatment did not have a minimum follow-up length.1,9,15 Longer follow-up may identify additional erosion events and thus may be able to elucidate trends that are currently not statistically significant. Additionally, as this study was conducted at a large academic center with surgeons at varying levels of experience and techniques, there is a possibility that different surgical methods between surgeons can confound the results.
Conclusion
In conclusion, anti-VEGF therapy was not associated with an increased rate of GDD erosions or an increased number of GDD erosions in eyes that experienced at least one erosion event. However, the presence of DME was associated with a higher risk of GDD erosion in eyes not receiving anti-VEGF therapy. Further studies with longer follow-up and larger cohorts will be important to determine if these trends persist with longer anti-VEGF therapy.
Brief Summary
Anti-vascular endothelial growth factor (anti-VEGF) intravitreal injections for diabetic retinopathy are not associated with an increased rate of glaucoma drainage device erosions.
Funding
This study was supported by the NIH Center Core Grant P30EY014801 and an unrestricted grant to the University of Miami from the Research to Prevent Blindness.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gedde SJ, Herndon LW, Brandt JD, Budenz DL, Feuer WJ, Schiffman JC. Postoperative complications in the tube versus trabeculectomy (TVT) study during five years of follow-up. Am J Ophthalmol. 2012;153(5):804–814.e1. doi:10.1016/j.ajo.2011.10.024
2. Gedde SJ, Scott IU, Tabandeh H, et al. Late endophthalmitis associated with glaucoma drainage implants. Ophthalmology. 2001;108(7):1323–1327. doi:10.1016/s0161-6420(01)00598-x
3. Al-Beishri AS, Malik R, Freidi A, Ahmad S. Risk factors for glaucoma drainage device exposure in a Middle-Eastern population. J Glaucoma. 2019;28(6):529–534. doi:10.1097/IJG.0000000000001220
4. Netland P, Chaku M, Ishida K, Rhee D. Risk factors for tube exposure as a late complication of glaucoma drainage implant surgery. OPTH. 2016;547. doi:10.2147/OPTH.S104029
5. Trubnik V, Zangalli C, Moster MR, et al. Evaluation of risk factors for glaucoma drainage device–related erosions: a retrospective case-control study. J Glaucoma. 2015;24(7):498–502. doi:10.1097/IJG.0000000000000034
6. Levinson JD, Giangiacomo AL, Beck AD, et al. Glaucoma drainage devices: risk of exposure and infection. Am J Ophthalmol. 2015;160(3):516–521.e2. doi:10.1016/j.ajo.2015.05.025
7. Byun YS, Lee NY, Park CK. Risk factors of implant exposure outside the conjunctiva after Ahmed glaucoma valve implantation. Jpn J Ophthalmol. 2009;53(2):114–119. doi:10.1007/s10384-008-0630-y
8. Geffen N, Buys YM, Smith M, et al. Conjunctival complications related to Ahmed glaucoma valve insertion. J Glaucoma. 2014;23(2):109–114. doi:10.1097/IJG.0b013e31826ab693
9. Liu KC, Gomez-Caraballo M, Challa P, Asrani SG. Recurrent tube erosions with anti-vascular endothelial growth factor therapy in patients with age-related macular degeneration. Ophthalmol Glaucoma. 2020;3(4):295–300. doi:10.1016/j.ogla.2020.04.005
10. Miraftabi A, Nilforushan N. Wound dehiscence and device migration after subconjuntival bevacizumab injection with Ahmed glaucoma valve implantation. J Ophthalmic Vis Res. 2016;11(1):112. doi:10.4103/2008-322X.180703
11. Muir KW, Lim A, Stinnett S, Kuo A, Tseng H, Walsh MM. Risk factors for exposure of glaucoma drainage devices: a retrospective observational study. BMJ Open. 2014;4(5):e004560. doi:10.1136/bmjopen-2013-004560
12. Imazeki M, Noma H, Yasuda K, Motohashi R, Goto H, Shimura M. Anti-VEGF therapy reduces inflammation in diabetic macular edema. Ophthalmic Res. 2020;64:43–49. doi:10.1159/000508953
13. Ragan AM, Docherty G, Crichton A. Are topical steroids a risk factor for tube exposure in glaucoma drainage devices? OPTH. 2021;15:1759–1761. doi:10.2147/OPTH.S281384
14. Chang L, Crowston JG, Cordeiro MF, Akbar AN, Khaw PT. The role of the immune system in conjunctival wound healing after glaucoma surgery. Surv Ophthalmol. 2000;45(1):49–68. doi:10.1016/S0039-6257(00)00135-1
15. Budenz DL, Barton K, Gedde SJ, et al. Five-year treatment outcomes in the Ahmed Baerveldt Comparison Study. Ophthalmology. 2015;122(2):308–316. doi:10.1016/j.ophtha.2014.08.043
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effects of COVID-19 on Intravitreal Injection Clinic After Lockdown
Hsieh T, Gundlach BS, Ashrafzadeh S, Sarraf D, Tsui I
Clinical Ophthalmology 2022, 16:3089-3096
Published Date: 19 September 2022
Non-Linear Relationship Between Fasting C-Peptide and Retinopathy in Patients with Type 2 Diabetes Mellitus - A Retrospective Study
Ma J, Han C, Lv Y, Cai H
Diabetes, Metabolic Syndrome and Obesity 2025, 18:1035-1045
Published Date: 7 April 2025