Back to Journals » Journal of Pain Research » Volume 16
Effectiveness of Transcutaneous Neuromodulation on Abductor Muscles Electrical Activity in Subjects with Chronic Low Back Pain: A Randomized, Controlled, Crossover Clinical Trial
Authors Benítez-Martínez JC ![]() , García-Haba B, Fernández-Carnero S, Pecos-Martin D
, García-Haba B, Fernández-Carnero S, Pecos-Martin D ![]() , Sanchez Romero EA
, Sanchez Romero EA ![]() , Selva-Sarzo F
, Selva-Sarzo F ![]() , Cuenca-Zaldívar JN
, Cuenca-Zaldívar JN
Received 21 March 2023
Accepted for publication 5 July 2023
Published 24 July 2023 Volume 2023:16 Pages 2553—2566
DOI https://doi.org/10.2147/JPR.S409028
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Josep C Benítez-Martínez,1 Beatriz García-Haba,2 Samuel Fernández-Carnero,3,4 Daniel Pecos-Martin,3 Eleuterio A Sanchez Romero,4– 9 Francisco Selva-Sarzo,1,2 Juan Nicolás Cuenca-Zaldívar3,4,10,11
1Physiotherapy Faculty, University of Valencia, Valencia, 46010, Spain; 2Francisco Selva Physiotherapy Clinic, Valencia, 46008, Spain; 3Universidad de Alcalá, Facultad de Enfermería y Fisioterapia, Departamento de Fisioterapia, Grupo de Investigación en Fisioterapia y Dolor, Alcalá de Henares, 28801, Spain; 4Interdisciplinary Research Group on Musculoskeletal Disorders, Faculty of Sport Sciences, Universidad Europea deMadrid, Villaviciosa de Odón, 28670, Spain; 5Department of Physiotherapy, Faculty of Sport Sciences, Universidad Europea de Madrid, Villaviciosa de Odón, 28670, Spain; 6Musculoskeletal Pain and Motor Control Research Group, Faculty of Sport Sciences, Universidad Europea de Madrid, Madrid, 28670, Spain; 7Department of Physiotherapy, Faculty of Health Sciences, Universidad Europea de Canarias, Santa Cruz de Tenerife, 38300, Spain; 8Musculoskeletal Pain and Motor Control Research Group, Faculty of Health Sciences, Universidad Europea de Canarias, Santa Cruz de Tenerife, 38300, Spain; 9Physiotherapy and Orofacial Pain Working Group, Sociedad Española de Disfunción Craneomandibular y Dolor Orofacial (SEDCYDO), Madrid, 28009, Spain; 10Primary Health Center “El Abajón”, Las Rozas de Madrid, 28231, Spain; 11Research Group in Nursing and Health Care, Puerta de Hierro Health Research Institute - Segovia de Arana (IDIPHISA), Madrid, Spain
Correspondence: Eleuterio A Sanchez Romero; Francisco Selva-Sarzo, Email [email protected]; [email protected]
Introduction: Non-specific chronic low back pain (NSCLBP) is a major cause of functional impairment, resulting in consequences like job absenteeism and reduced quality of life. Risk factors such as muscle weakness and tightness have been implicated. Electromagnetic fields have therapeutic effects on human tissue, including pain relief and muscle relaxation. This study aimed to examine the impact of a tape with magnetic particles (MPT) applied to the lumbar area on abductor muscle strength and surface electromyography (sEMG) of the Gluteus Medius and Tensor of the Fascia Lata muscles in individuals with NSCLBP.
Methods: It was carried out a double-blind, randomized, controlled, crossover trial and with test retest, with 41 consecutive patients younger than 65 years who previously diagnosed with NSCLBP to assess the effect of a MPT over hip abductor muscle strength and activity. sEMG and force data were obtained during the Hip Stability Isometric Test (HipSIT). The HipSIT was used to assess the abduction strength using a hand-held dynamometer and sEMG. The HipSIT uses the maximum voluntary isometric contraction (MVIC). Four trials were recorded and the mean extracted for analysis. The tape was applied with either a MPT or a sham magnetic particle tape (SMPT) bilaterally without tension on from L1 to L5 paravertebral muscles.
Results: The significant increase in the recruitment of fibers and the significant increase in the maximum voluntary contraction by applying MPT with respect to the SMPT, correspond to the increases in the Peak Force and the decrease in the time to reach the maximum force (peak time) of both muscles.
Conclusion: Application of a MPT in patients with NSCLBP suggests an increase in muscle strength of the Gluteus Medius and Tensor Fascia Lata bilaterally during the HipSIT test. Lumbar metameric neuromodulation with MPT improves muscle activation of the hip musculature.
Keywords: transcutaneous nerve stimulation, electromyography, low back pain
Introduction
Non-specific chronic low back pain (NSCLBP) is one of the main reasons of loss of function that can have consequences such as job absenteeism and a decrease in the quality of life.1,2 Based in clinical findings and scientific studies, different risk factors have been stated as potential implication, such as muscle weakness3,4 and muscle tightness.5
The NSCLBP conservative treatment could include medication management and physical therapy.6 Several physical therapy interventions have been suggested, mainly exercise programs, manual therapy, education and electrotherapy.7 There is low-quality evidence that kinesiotaping has a beneficial role in pain reduction and disability improvement for patients with NSCLBP.8 However, elastic taping therapy in patients with lumbar radiculopathy has a positive effect on pain and functional status compared to rigid tape. Elastic taping can be recommended for clinical use because its effect is superior in some recovery parameters and its ease of use.9
Electromagnetic fields positively influence human tissue and have a number of therapeutic effects such as: pain relief, healing bone fracture, myorelaxation, myostimulation and joint mobilization. Gossling HR et al10 scientifically demonstrated in 1992 that the activation of body magnetic fields in different traumatic pathologies can be as effective compared to surgical interventions. Li Y et al11 reached the same conclusions in 2020. Magnetotherapy could provide a non-invasive, safe and easy method to directly treat the area of pain.12
The lumbopelvic and hip muscles’ dysfunction has been found in NSCLBP population.13 Gluteus medius and hip muscles are more likely to show altered recruitment and reduced strength.14,15 The superior gluteal nerve is found in the lower pelvis and arises from the dorsal divisions of the L4, L5, and S1 nerve roots of the sacral plexus. The superior gluteal nerve is responsible for innervation of the gluteus medius, gluteus minimus, and tensor fasciae latae muscles.16
Despite the inherent stability of the hip joint, active individuals often experience hip pain and injuries due to hip instability. One crucial muscle group that contributes to hip stability is the hip abductors, with the gluteus medius being the largest among them.17
Magnetic particle tape (MPT) is an elastic adhesive tape that incorporates magnetic particles with the ability to create low-power magnetic fields, which in a previous study provided preliminary results of blood flow and pain modulation in subjects with low back pain.18 It is unknown whether lumbar metameric neuromodulation would improve muscle activation of the hip musculature in patients with NSCLBP.
The aim of this study was to investigate whether the effect of a MPT applied to the lumbar area in subjects with NSCLBP influences the strength of abductor muscle contraction and whether an immediate effect is obtained on surface electromyography (sEMG) of the Gluteus Medius and the Tensor of the Fascia Lata muscles.
Methods
Study Design
A double-blind randomized, controlled crossover trial was conducted between October 2021 and February 2022 to assess the effect of a MPT over lumbar region on hip abductor muscle strength and activity. All patients were informed about the study, they provided informed consent in accordance with the Helsinki Declaration and the study was approved for the Ethical Committee of University of Valencia by number 1622496 and registered in clinicaltrials.gov (NCT04893967). The recommendations of the “Consolidated Standards of Reporting Trials” (CONSORT) were followed19 (Figure 1).
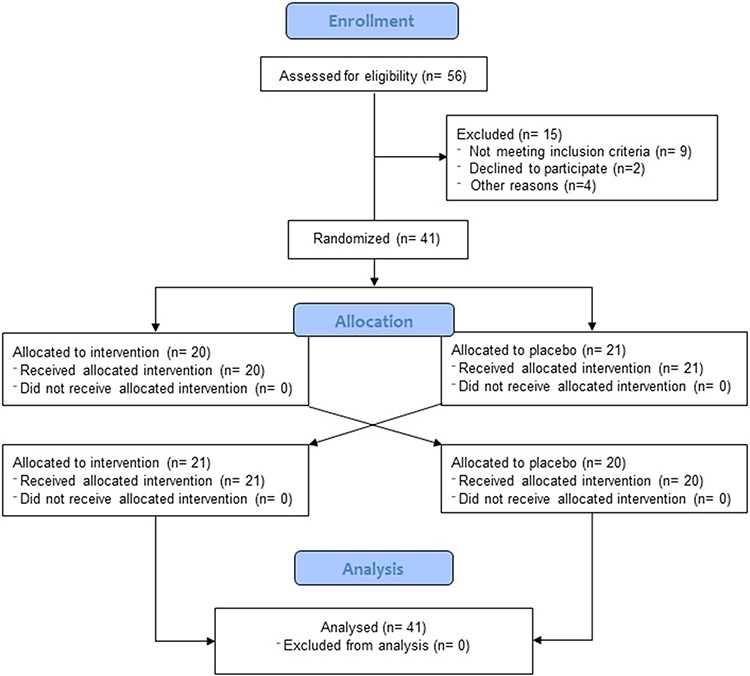 |
Figure 1 CONSORT Flow-diagram. |
Participants
Forty-one consecutive patients younger than 65 years who were previously diagnosed with NSCLBP by a physician were recruited to participate in the study from the following clinics from Valencia (Spain): Acuario Sports Clinic, Aston Clinic specializing in traumatology and sports physiotherapy, and Francisco Selva Physiotherapy Clinic. From an initial sample of 56 patients, 41 were finally included in the study, applying the following inclusion and exclusion criteria:
Inclusion criteria were as follows: (1) over 18 and less than 65 years of age and (2) having a medical diagnosis of NSCLBP. The exclusion criteria were as follows: (1) presence of malignant diseases such as cancer (2) neurological or degenerative diseases (3) pain duration less than three months (4) having conditions that would be a contraindication for the adhesive tape on the skin such as allergies (5) being pregnant (6) having a pacemaker (7) taking any medication that may interact with magnetic fields or contraindicated (8) metallic implant in lower limb (9) recent injury or trauma in spine or lower limbs.
The patients were assigned randomly into either magnetic particle tape group (MPT = 21) or sham magnetic particle tape group (SMPT = 21). Two conditions were applied in a crossover design for each condition with a washout period of 1 day between the trials.
Sample Size
The sample size was determined with the first 10 patients recruited in the study, using a t-test for paired data on the immediate post-treatment isometric testing values on the first and second day between both types of tape. Accepting a risk α of 0.05, a power of 80% and losses of 20%, a sample of 41 was estimated.
Tests and Measurements
The Hip Stability Isometric Test (HipSIT)20 was utilized to evaluate the strength of abduction. The HipSIT provides a comprehensive assessment of the strength of the entire hip musculature located in the back and sides, without the need to assess each muscle individually.21 The test required the subject to spread their knees apart while keeping their heels in contact, resulting in abduction of the upper hip.21 Maximum voluntary isometric contraction (MVIC) was employed for the HipSIT.
The patients were positioned on a treatment plinth in a side-lying position with the lower limbs flexed at 45° at the hip and 90° at the knee, and were requested to perform 4 MVIC using the Lafayette™ handheld dynamometer (HHD) (Lafayette Instrument Company, Lafayette, IN, USA). This device is frequently employed to assess muscle strength because of its exceptional reliability and validity compared to the gold standard isokinetic dynamometer.22
The intervention was administered by a female physiotherapist who was an expert in electromyography (EMG) and the use of a hand-held dynamometer (HHD). The physiotherapist had undergone training using the mDurance® system two years ago.
The HHD was placed between the femur and the strap, over a mark situated 5 cm proximal to the lateral knee joint line. Patients were instructed to push the tested leg upwards (abduction) at 20° of abduction.21 They were then instructed to push the dynamometer with maximum force for 5 seconds. Patients performed 1 practice trial, took a 30-second rest, and then performed the measured trials. Four trials were recorded and the mean was extracted for analysis.23
To avoid bias, a pre-defined script was employed to explain the tests. The hip abductor muscles’ peak force in kilograms (Kg), average force in kilograms (kg), and peak time in seconds (sec) over a five-second maximal voluntary isometric contraction were measured and recorded (Figure 2A).
 |
Figure 2 Electrode positioning for EMG evaluation (A). Dynamometry during Hip abduction (B). |
Muscle activity data were gathered using a validated21 sEMG system (mDurance® system; mDurance Solutions SL, Granada, Spain). This innovative system includes user-friendly software and a lightweight hardware, making it more accessible and cost-effective for clinicians and sports trainers. The skin was prepped by scrubbing the area using a cotton ball soaked in rubbing alcohol.
The sEMG electrodes were placed over the muscle bellies and in line with the muscle-fiber orientation of the Tensor Fascia Latae (TFL) and gluteus medius on both sides.24 The amplitude during the MVIC trials was collected. Gluteus medius and TFL RMS mean (μV), RMS mean/sec (μV/sec), and MVC mean (μV) were measured. We followed the guidelines established by SENIAM25 for equipment preparation, signal collection, and rectification (Figure 2B).
At the beginning of each session, a baseline measurement was taken to record the maximum voluntary isometric contraction (MVIC) and sEMG readings. This was done to serve as a control measure for the study. Four tests were conducted with a 30-second break between each trial. The average values were computed for each participant. In case any compensation was detected, the corresponding values were disregarded and a fresh assessment was done after a 20-second interval.21
Patients were advised to avoid engaging in any high-intensity exercise within 24 hours prior to the testing sessions.
Data Processing
To process the isometric test data, a fourth order Butterworth bandpass filter was applied with a cut-off frequency between 20 and 450 Hz. Next, the signal was smoothed using a window size of 0.025 s root mean square (RMS) and overlapping of 0.0125 s between windows, for each system separately. Finally, the MVIC value was calculated by taking the average of the three highest RMS signal peaks over the 5 second isometric test, and used to normalize the RMS signal of each system. This procedure ensured that the data from both systems were comparable and accurate.24
Intervention
The researcher who applied the tape was unknown about what was being applied by using a black tape non identifiable. The therapist was given the tape to apply in each case. She did not know if it was the experimental tape or the placebo tape. The characteristics of both tapes were that they were composed of cotton fibers, with elastane producing a 50–60% elongation of the tape. The MPT had the same characteristics as the SMPT but also contained particles with magnetic properties.18 To find out whether the effect was produced by the physical ionization generated by the magnetic particles, the tape was applied with 0% elongation. In this way, no fascial tension was produced that could bias the results. In the study by Selva-Sarzo et al,18 a video was presented as supplementary material in which the two bandages were visually the same and when a strong magnet was approached, only one of the tapes adhered to it. The allocation of the patients for the tape application was randomized using the program Random Allocation Software26 and then was applied with either the MPT group or SMPT group bilaterally without tension on from L1 to L5 paravertebral muscles27 (Figure 3).
 |
Figure 3 Magnetic particle tape or sham magnetic particle tape application. |
In the first session, they completed the evaluation form and the informed consent form and conducted the HipSIT using dynamometer and sEMG for muscle strength assessments.
Statistical Analyses
For the statistical analysis, the R Ver. 4.1.3. program was used. (R Foundation for Statistical Computing, Institute for Statistics and Mathematics, Welthandelsplatz 1, 1020 Vienna, Austria) and the “refund”28 package.
A significance level of p < 0.05 was established. Quantitative variables were assessed for normal distribution using the Shapiro–Wilk test, while qualitative variables were presented as absolute values and relative frequencies, and quantitative variables were described as mean and standard deviation. As the variables were not normally distributed, a robust model of repeated measures with two factors, between (groups) and within (measurements), was used to analyze the outcome variables. The omnibus test reported an Anova-type pseudo-statistic obtained by bootstrap (ATSboot) and its level of significance. Post hoc tests were conducted using an exact permutation test between groups and the Wilcoxon Signed Rank test within groups, with the Bonferroni correction applied in both cases. Effect size was calculated using the statistic η2p (partial eta squared) obtained by bootstrap, with small (0.01–0.06), moderate (0.06–0.14), and large (>0.14) defined as the range for effect size magnitude. In post hoc tests, the non-parametric statistic r was used as the effect size, defined as 0.1–0.4 (small), 0.4–0.6 (moderate), and >0.6 (large).
The effect size was calculated with the statistic η2p (partial eta squared) obtained by bootstrap due to the non-normal distribution of the variables, defined as small (0.01–0.06), moderate (0.06–0.14) and large (>0.14). In the post hoc tests, the non-parametric statistic r was used as the effect size, defined as 0.1–0.4 (small), 0.4–0.6 (moderate) and >0.6 (large).
The raw sEMG signal was analyzed by applying a 5 Hz highpass filter and a 100 Hz lowpass filter and moving average smoothing. The first trial was selected using Bonato’s double-scheme threshold-based algorithm.29
Two variable-domain functional regression [scalar-on-function regression (SoFR)] models were applied between groups and measurement times using the processed sEMG data signal in Gluteus Medius and Tensor Fasciae Latae muscles.
A SoFR model is one in which the response variable takes scalar values, and the covariates take functional or scalar values. This type of model is an extension of the generalized additive models (GAM). In our case, since the sEMG data had a different number of data points between subjects, a VDFR model was applied that allows the functional coefficients to vary, smoothly, according to the domain width of each subject.30
Results
The study involved 41 patients balanced between men and women 19 males 22 females; age: 43.85 ± 12.89 years; height: 167.31 ± 27.95 cm; weight: 72.98 ± 14.92 kg, in whom the majority dominant leg was the right (90.2%) (Table 1).
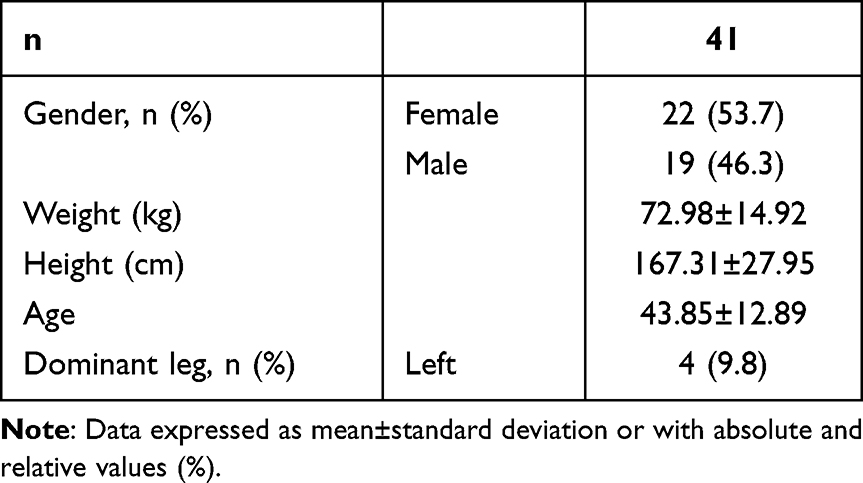 |
Table 1 Clinical and Demographic Characteristics of the Patients |
The existence of significant differences (p < 0.05) in the main effect of time it could be verified in all the quantitative result variables, except in the variables tensor fasciae latae RMS mean/sec (µV/sec), Dynamometry average force with small effect sizes and significant (Table 2).
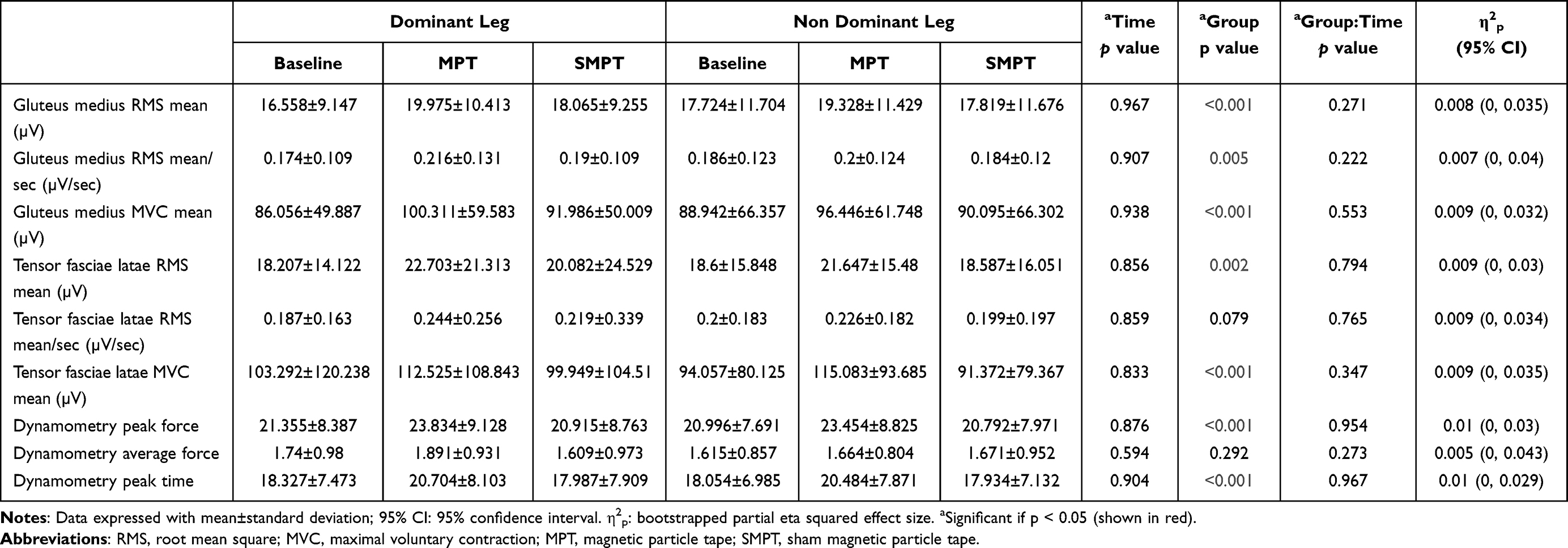 |
Table 2 Quantitative Outcome Variables |
In the post hoc tests between groups, no significant differences between the dominant and non-dominant leg were evident (Supplementary File. Table 1). However, in the intra-group pairwise comparisons, significant differences were evident in both the dominant and non-dominant legs in most of the outcome variables in the MPT–Baseline, SMPT–MPT comparisons, except for the variable Dynamometry peak force, with moderate to large significant effect sizes (Supplementary File. Table 2).
The trend graphs showed how the dynamometry and sEMG activation values were greater in the dominant leg compared to the non-dominant one, although these differences were not significant. These values increased with the application of the MPT in both groups, with significant differences compared to baseline values, and drastically decreased with the application of the SMPT with significant differences between both types of tape, with a return to values similar to those obtained baseline, which explained the absence of significant differences in the SMPT–Baseline comparison (Figure 4).
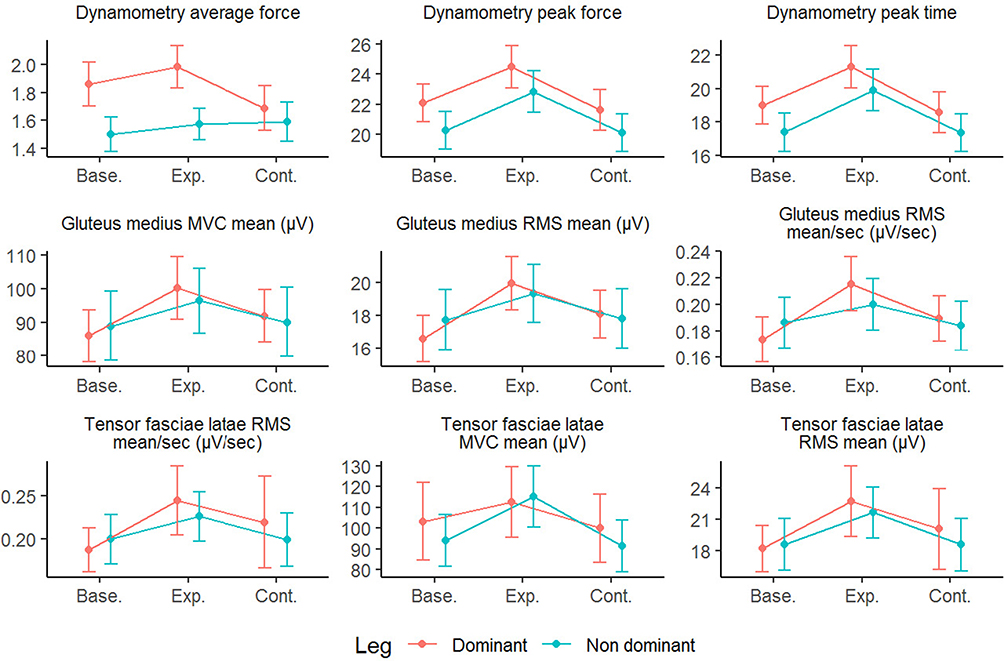 |
Figure 4 Outcome variables trend graphs. Abbreviations: Base, baseline; Exp., magnetic particle tape; Cont., sham magnetic particle tape. |
The sEMG recording of the gluteus medius and tensor fasciae latae raw and processed is shown in Figure 5.
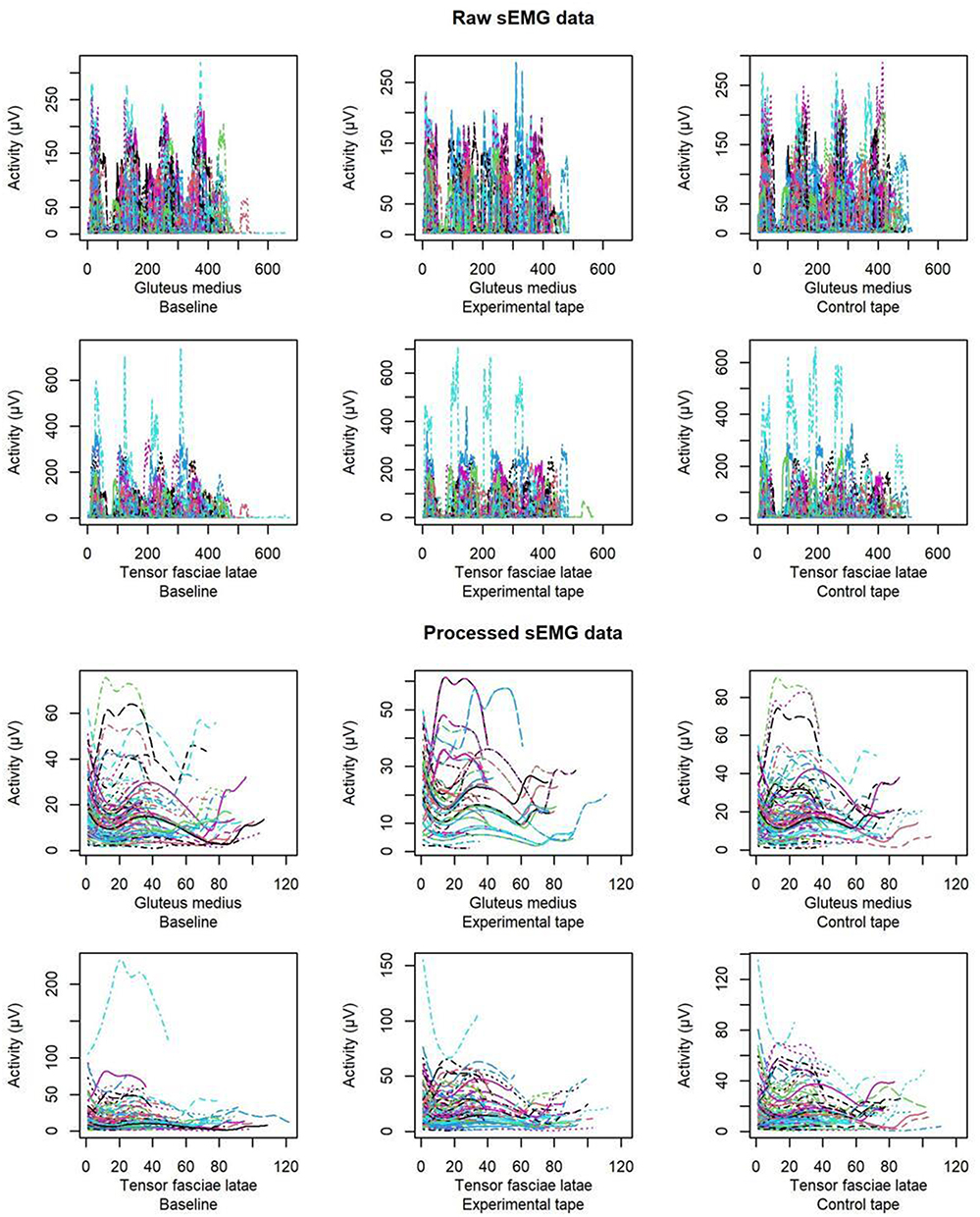 |
Figure 5 sEMG recording of the gluteus medius and tensor fasciae latae raw and processed. |
The SoFR regression model showed no significant difference between the dominant and non-dominant leg (Supplementary File. Table 3). sEMG recording in gluteus medius was found to significantly predict (F = 13.71, p = 0.013) the type of tape (MPT or SMPT) applied (Table 3).
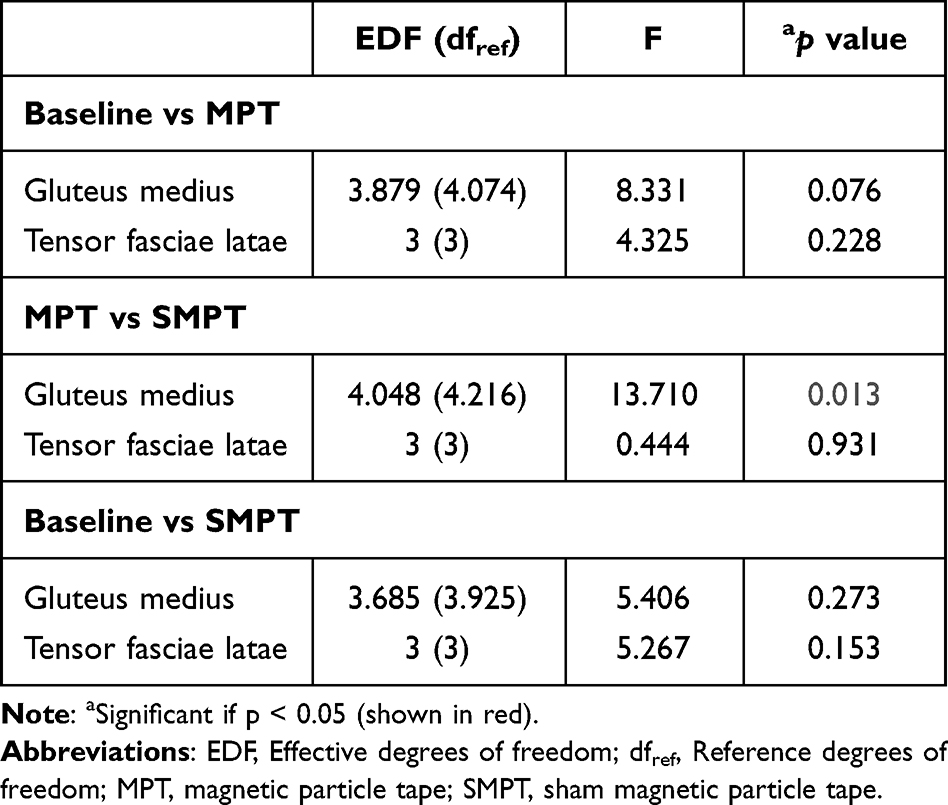 |
Table 3 sEMG Raw Smoothed Models Between Measurement Times |
The contour graph showed how a greater activation of the gluteus medius was associated with the application of the MPT (Figure 6).
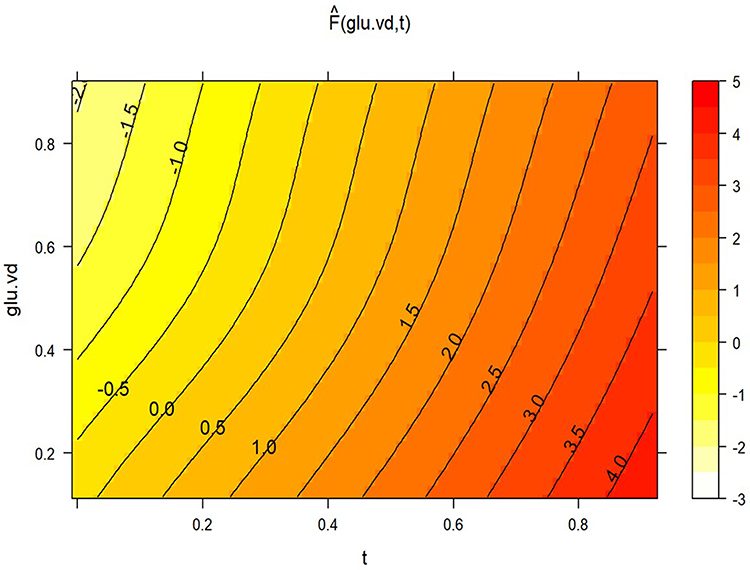 |
Figure 6 Contour plot of pseudo t-statistic. |
Discussion
The primary aim of this study was to investigate whether the effect of a tape with magnetic particles applied to the lumbar area in patients with NSCLBP has an effect on MVIC of the hip abduction by the HipSIT. The secondary aim was to determine if there were differences on the Gluteus Medius and Tensor Fascia Latae activation.
The significant increase in the recruitment of fibers and the significant increase in the maximum voluntary contraction by applying MPT with respect to the SMPT correspond to the increases in the Peak Force and the decrease in the time to reach the maximum force (Peak Time) of both muscles.
Our data agree with prior studies showing the effects of MPT in the population with NSCLBP results with immediate effects of pain relief and an increase in the parameters of blood flow analyzed, postulating it to be a plausible therapy for pain and systemic neuromodulation.18 In our case, it was in the muscle force production and muscle electrophysiology. We found higher activation in gluteus medius and tensor fascia latae muscles in MPT group in dominant and in non-dominant leg compared against SMPT group and baseline.
Hypothesis of MPT’s Mechanism of Action
Our findings are in line with the results of previous studies in the biomedical magnetizing effects.10,11,28–37 Our hypothesis and interpretation about the action of the MPT would be oriented to the development of similar properties used in the biomedical magnetic field, so they do not show any magnetization unless they encounter magnetic fields like those of the epidermis, presenting a rapid change of magnetic state.
Perhaps, if pain is reduced, the pain-producing mechanisms may no longer negatively influence the electrical signals of the lumbar nerves, especially the superior gluteal nerve that innervates the tested musculature.18
Just recently was assumed that sensory neurons were the main and, in some cases, the only transducers of innocuous and noxious stimuli in the skin.38 However, this dogma has been essentially denied by recent work demonstrating how non-neuronal cells, including keratinocytes, are required for normal detection and encoding of somatosensory stimuli in the peripheral nervous system.38
The epidermis is the most superficial layer of the skin and is part of the Central Nervous System. The epidermis contains intraepidermal free nerve endings (FNE) corresponding to Aδ and C fibers as well as Aβ fibers associated with Merkel cells.39 Two distinct groups of nerve fibers are found in the epidermis, the cutaneous sensory nerve fibers and the autonomic nerve fibers. The epidermis contains a variety of different cells.40 The most relevant cells of the epidermis are keratinocytes and Merkel cells, which together with the dendrites of Aβ-type afferent sensory neurons, whose cell bodies are located in the dorsal root ganglia, form the “Tactile Dome”. Together, these structures can be considered the mechanosensory organs of the epidermis.40
Keratinocytes are activated by electromagnetic wave radiation such as ultraviolet B light (UVB). In a mouse model of sunburn pain, exposure to UVB light resulted in profound mechanical and thermal allodynia, effects that were entirely dependent on UVB-induced activation and sensitization of TRPV4-expressing keratinocytes.41 Once the epidermal ion flow has been created, the mechanism of electrical and magnetic stimulation at the neural level could be the same, which are the depolarization of the axon and the initiation of the action potential.39 The identification of keratinocytes as the primary transducers of damaging stimuli is a paradigm shift in the field of cutaneous sensory transduction.39
The low electromagnetic intensity that can be generated with MPT as it does not adhere or repel like magnets suggests that it acts superficially. Activation of keratinocytes, which make up more than 95% of epidermal cells, could release a wide range of neuroactive factors in addition to forming tight “synapse-like” connections with intraepidermal nerve fibers,38 inducing action potential activation in sensory neurons.38
Effect of MPT on Strength
In the present study, the value of peak force in dynamometry was statistically significant when control and experimental group were compared in dominant and non-dominant leg. The effect of the MPT on peak force (see Table 2) is comparable with Chilibeck et al42 when application of spinal manipulation reported an increase (104 ± 43 to 116 ± 43 Nm) compared to placebo (84 ± 24 to 85 ± 31 Nm) (p = 0.03).
The increase in the recruitment of fibers obtained with the sEMG and the increase in maximum voluntary contraction by applying MPT correspond to the increases in Peak force and the decrease in the time to reach maximum force (peak time) of both muscles. Therefore, MPT looks to be helpful to recruit more fibers and increase voluntary force, reaching it in less time in patients with NSCLBP.
This translates into better muscle tone and, when doing sports, less risk of injury by activating the muscles earlier and with more force. In people with NSCLBP, dysfunction of muscles such as the gluteus medius has been demonstrated to increase spinal loading and reduce spinal stability.43
This finding is complementary to the one made by Selva et al18 for being able to reduce the perceived low back pain when applying MPT. Therefore, when the pain decreases, nerve activity could be activated, modulating the nervous information that reaches the musculature, influencing the tone.
Gluteus medius muscle weakness is a common presentation in people with NSCLBP.44 The musculature of the hip and ankle are coactivated, so surely in people with NSCLBP there will be neural dysfunction in both joints.45 The assessment of ankle dorsiflexion is used to prevent and treat injuries in the lower extremities, so it would be interesting to assess the influence of NSCLBP on ankle joint mobility. Cooper et al44 concluded that focusing on assessment and treatment of gluteus medius muscle dysfunction may allow for better clinical decision-making and better treatment outcomes for people with LBP, and then the application of MPT could help this kind of patient groups. If the metameric application of Magnetic Tape achieves a significant and immediate increase in muscle strength, perhaps it means that the dysfunction or lack of strength is not due to the musculature itself, but to incorrect nerve activation.
We believe that patients with NSCLBP presenting with gluteus medius weakness and associated tenderness may represent a treatment subgroup that could benefit from first achieving correct muscle activation of the TFL and gluteus medius, followed by appropriate therapeutic exercise.
To the best our knowledge, this is the first study to observe the effects of magnetic particles in a tape on an epidermis and the effect in the force and activation of hip abduction muscles. On the other hand, only the acute effects of the MPT on force and activation were studied. Then, we must be careful to generalize the results and middle and long-term effect in greater sample should be studied. As well as the implication of the effects of magnetic tape on the autonomic nervous system.46 Further research should answer these questions.
The results of application of MPT in people with NSCLBP suggested an increase in muscle strength of the Gluteus Medius and Tensor Fascia Lata bilaterally during the HipSIT test. MPT could be involved in recruitment of more fibers and increase voluntary force, reaching it in less time in patients with NSCLBP.
The application of MPT reported an immediate improvement in NSCLBP, so the improvement in strength observed in this study may have helped to decrease or eliminate inhibitory reflexes, allowing neuromodulation of muscle electrical activity.
By placing MPT bilaterally, no differences were found between the dominant and non-dominant side, although fiber recruitment, maximum voluntary contraction, Peak Force were significantly increased on both sides, and the time to reach peak time of recovery was decreased in both muscles compared to SMPT tape and basal state.
Limitations and Future Directions
As limitations, pain in the paravertebral back muscles could have been recorded in addition to the irritated bone element. Also, the referred pain to lower limbs or loss of function. This may be the cause of the contradictory results in activation and differences between dominant and non-dominant in some cases. Finally, the visceral or abdominal and pelvic viscero-somatic relations neither were considered.
The results demonstrate physiological baselines states changes. Future research is needed to explore the possible mechanisms of action and the possible benefits for other conditions and locations using MPT, given that to date, we can only establish hypotheses, in the light of the results obtained, and based on neuroscience.
The impact of patients’ treatment expectations can also be examined, as research suggests that certain expectations, such as tailored treatment with regular monitoring, a positive outlook on outcomes, acceptance or acknowledgement of pain relief limitations, effective communication, individualized care, and explanation of pain may be associated with improved recovery outcomes for those with low back pain.47
Conclusions
MPT applied to the lumbar area in subjects with NSCLBP was effective in increasing abductor muscle contraction strength compared to the SMPT group.
Greater activation of the gluteus medius and TFL was found in the MPT group in the dominant and non-dominant leg compared to the SMPT group.
Impact Statement
The findings of this study will provide data on the effectiveness of a MPT for people with NSCLBP for health care policy makers, physicians, and insurers. Data from this study will also inform future pragmatic trials for non-pharmacological interventions and chronic musculoskeletal pain conditions.
Author Contributions
Conceptualization: BGH, SFC, FSS, JNCZ; Data curation: SFC, JNCZ; Formal analysis: JNCZ; Funding acquisition: JNCZ; Investigation: JCBM, BGH; Methodology: JCBM, BGH, SFC, DPM, FSS, JNCZ; EASR Project administration: JCBM, BGH, SFC, DPM, FSS, JNCZ; Resources: BGH, FSS; Software: JNCZ; Supervision: SFC, FSS; EASR Validation: JCBM, BGH, SFC, DPM; EASR; Visualization: JCBM, BGH, SFC, DPM, FSS, JNCZ; EASR Writing-original draft: BGH, SFC, FSS, JNCZ; Writing-review and editing: JCBM, BGH, SFC, DPM, FSS, JNCZ, EASR. All authors have read and agreed to the published version of the manuscript. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Data Sharing Statement
The data presented in this study are available on request from the corresponding authors – Dr Eleuterio A. Sánchez-Romero. The data are not publicly available due to ethical restrictions.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki and approved for the Ethical Committee of University of Valencia by number 1622496 and registered on 20/05/2021 at clinicaltrials.gov (NCT04893967). Informed consent was obtained from all subjects involved in the study.
Consent for Publication
Patients gave their consent to publish the results of the study, and their anonymity was always respected.
Acknowledgments
To the patients for their participation.
Funding
The authors completed the manuscript without the aid of any type of funding.
Disclosure
The authors report a potential conflict of interest in the fact that FSS is the developer of the magnetic tape. The authors do not present any relationship of any kind with the Brand. Francisco Selva-Sarzo reports an European patent for adhesive fascial tape (no 3479804). The authors report no other conflicts of interest in this work.
References
1. Vos T, Allen C, Arora M, Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the global burden of disease study 2015. Lancet. 2016;388:1545–1602. doi:10.1016/S0140-6736(16)31678-6
2. Buchbinder R, van Tulder M, Öberg B, et al. Low back pain: a call for action. Lancet. 2018;391:2384–2388. doi:10.1016/S0140-6736(18)30488-4
3. Cho KH, Beom JW, Lee TS, et al. Trunk muscles strength as a risk factor for nonspecific low back pain: a pilot study. Ann Rehabil Med. 2014;38:234–240. doi:10.5535/arm.2014.38.2.234
4. Sánchez Romero EA, Alonso Pérez JL, Muñoz Fernández AC, et al. Reliability of sonography measures of the lumbar multifidus and transversus abdominis during static and dynamic activities in subjects with non-specific chronic low back pain. Diagnostics. 2021;11:632. doi:10.3390/diagnostics11040632
5. Halbertsma JPK, Göeken LNH, Hof AL, Groothoff JW, Eisma WH. Extensibility and stiffness of the hamstrings in patients with nonspecific low back pain. Arch Phys Med Rehabil. 2001;82:232–238. doi:10.1053/apmr.2001.19786
6. Dias LV, Cordeiro MA, Schmidt de Sales R, et al. Immediate analgesic effect of transcutaneous electrical nerve stimulation (TENS) and interferential current (IFC) on chronic low back pain: randomised placebo-controlled trial. J Bodyw Mov Ther. 2021;27:181–190. doi:10.1016/j.jbmt.2021.03.005
7. Hayden JA, Ellis J, Ogilvie R, Malmivaara A, van Tulder MW. Exercise therapy for chronic low back pain. Cochrane Database Syst Rev. 2021;9:CD009790. doi:10.1002/14651858.CD009790.pub2
8. Lin S, Zhu B, Huang G, et al. Short-term effect of kinesiotaping on chronic nonspecific low back pain and disability: a meta-analysis of randomized controlled trials. Phys Ther. 2020;100:238–254. doi:10.1093/ptj/pzz163
9. Bozkurt T, Kilic RT, Yosmaoglu HB. The effect of elastic therapeutic taping and rigid taping on pain, functionality, and tissue temperature in lumbar radiculopathy: a randomized controlled study. Somatosens Mot Res. 2021;38:1–8. doi:10.1080/08990220.2021.1986381
10. Gossling HR, Bernstein RA, Abbott J. Treatment of ununited tibial fractures: a comparison of surgery and pulsed electromagnetic fields (PEMF). Orthopedics. 1992;15:711–719. doi:10.3928/0147-7447-19920601-08
11. Li Y, Pan Q, Zhang N, et al. A novel pulsed electromagnetic field promotes distraction osteogenesis via enhancing osteogenesis and angiogenesis in a rat model. J Orthop Transl. 2020;25:87–95.
12. Alfano AP, Taylor AG, Foresman PA, et al. Static magnetic fields for treatment of fibromyalgia: a randomized controlled trial. J Altern Complement Med. 2001;7:53–64. doi:10.1089/107555301300004538
13. Nourbakhsh MR, Arab AM. Relationship between mechanical factors and incidence of low back pain. J Orthop Sports Phys Ther. 2002;32:447–460. doi:10.2519/jospt.2002.32.9.447
14. Arab AM, Nourbakhsh MR. The relationship between Hip abductor muscle strength and iliotibial band tightness in individuals with low back pain. Chiropr Osteopat. 2010;18. doi:10.1186/1746-1340-18-1
15. Nelson-Wong E, Poupore K, Ingvalson S, et al. Neuromuscular strategies for lumbopelvic control during frontal and sagittal plane movement challenges differ between people with and without low back pain. J Electromyogr Kinesiol Off J Int Soc Electrophysiol Kinesiol. 2013;23:1317–1324. doi:10.1016/j.jelekin.2013.08.011
16. Lung K, Lui F. Anatomy Abdomen and Pelvis, Superior Gluteal Nerve; 2022.
17. Tsutsumi M, Nimura A, Akita K. Clinical anatomy of the musculoskeletal system in the Hip region. Anat Sci Int. 2022;97:157–164. doi:10.1007/s12565-021-00638-3
18. Selva-Sarzo F, Fernández-Carnero S, Sillevis R, et al. The direct effect of magnetic tape® on pain and lower-extremity blood flow in subjects with low-back pain: a randomized clinical trial. Sensors. 2021;21:6517. doi:10.3390/s21196517
19. Schulz KF, Altman DG, Moher D. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ. 2010;340:c332. doi:10.1136/bmj.c332
20. Almeida GPL, Rodrigues HLDN, De Freitas BW, De paula lima PO. Reliability and validity of the Hip Stability Isometric Test (HipSIT): a new method to assess hip posterolateral muscle strength. J Orthop Sports Phys Ther. 2017;47:906–913. doi:10.2519/jospt.2017.7274
21. Molina-Molina A, Ruiz-Malagón EJ, Carrillo-Pérez F, et al. Validation of mDurance, A wearable surface electromyography system for muscle activity assessment. Front Physiol. 2020;11. doi: 10.3389/fphys.2020.606287
22. Mentiplay BF, Perraton LG, Bower KJ, et al. Assessment of lower limb muscle strength and power using hand-held and fixed dynamometry: a reliability and validity study. PLoS One. 2015;10:e0140822. doi:10.1371/journal.pone.0140822
23. Thorborg K, Bandholm T, Hölmich P. Hip- and knee-strength assessments using a hand-held dynamometer with external belt-fixation are inter-tester reliable. Knee Surg Sports Traumatol Arthrosc. 2013;21:550–555. doi:10.1007/s00167-012-2115-2
24. Konrad P. Noraxon: the ABC of EMG. Signal Processing; 2005. Available from: http://demotu.org/aulas/controle/ABCofEMG.pdf.
25. Freriks B, Hermens H. European recommendations for surface electromyography: results of the SENIAM project; 1999.
26. Saghaei M. Random allocation software for parallel group randomized trials. BMC Med Res Methodol. 2004;4:26. doi:10.1186/1471-2288-4-26
27. Selva-Sarzo F. Neuromodulación Superficial. Sistema de Valoración y tratamiento. Phyos Stability ed; 2022.
28. Goldsmith J, Scheipl F, Huang L, et al. Refund: regression with functional data. R Package Version; 2021.
29. Bonato P, D’Alessio T, Knaflitz M. A statistical method for the measurement of muscle activation intervals from surface myoelectric signal during gait. IEEE Trans Biomed Eng. 1988;45(3):287–299. doi:10.1109/10.661154
30. Gellar JE, Colantuoni E, Needham DM, Crainiceanu CM. Variable-domain functional regression for modeling ICU data. J Am Stat Assoc. 2014;109(508):1425–1439. doi:10.1080/01621459.2014.940044
31. Brown CS, Ling FW, Wan JY, Pilla AA. Efficacy of static magnetic field therapy in chronic pelvic pain: a double-blind pilot study. Am J Obstet Gynecol. 2002;187:1581–1587. doi:10.1067/mob.2002.128026
32. McKay JC, Prato FS, Thomas AW. A literature review: the effects of magnetic field exposure on blood flow and blood vessels in the microvasculature. Bioelectromagnetics. 2007;28:81–98. doi:10.1002/bem.20284
33. Cardoso VF, Francesko A, Ribeiro C, et al. Advances in magnetic nanoparticles for biomedical applications. Adv Healthc Mater. 2018;7:1.
34. Yang J, Zhang J, Ding C, Dong D, Shang P. Regulation of osteoblast differentiation and iron content in MC3T3-E1 cells by static magnetic field with different intensities. Biol Trace Elem Res. 2018;184:214–225. doi:10.1007/s12011-017-1161-5
35. Ortolani A, Bianchi M, Mosca M, et al. The prospective opportunities offered by magnetic scaffolds for bone tissue engineering: a review. Joints. 2016;4:228–235. doi:10.11138/jts/2016.4.4.228
36. Liu Z, Huang L, Liu L, et al. Activation of Schwann cells in vitro by magnetic nanocomposites via applied magnetic field. Int J Nanomedicine. 2015;10:43–61. doi:10.2147/IJN.S74332
37. Xu H-Y, Gu N. Magnetic responsive scaffolds and magnetic fields in bone repair and regeneration. Front Mater Sci. 2014;81(8):20–31. doi:10.1007/s11706-014-0232-1
38. Mikesell AR, Isaeva O, Moehring F, et al. Keratinocyte PIEZO1 modulates cutaneous mechanosensation. Elife. 2022;11. doi: 10.7554/eLife.65987
39. Talagas M, Lebonvallet N, Berthod F, Misery L. Cutaneous nociception: role of keratinocytes. Exp Dermatol. 2019;28:1466–1469. doi:10.1111/exd.13975
40. Boulais N, Misery L. The epidermis: a sensory tissue. Eur J Dermatol. 2008;18:119–127. doi:10.1684/ejd.2008.0348
41. Moore C, Cevikbas F, Pasolli HA, et al. UVB radiation generates sunburn pain and affects skin by activating epidermal TRPV4 ion channels and triggering endothelin-1 signaling. Proc Natl Acad Sci USA. 2013;110:E3225–34. doi:10.1073/pnas.1312933110
42. Chilibeck PD, Cornish SM, Schulte A, et al. The effect of spinal manipulation on imbalances in leg strength. J Can Chiropr Assoc. 2011;55:183.
43. Sadler S, Cassidy S, Peterson B, Spink M, Chuter V. Gluteus medius muscle function in people with and without low back pain: a systematic review. BMC Musculoskelet Disord. 2019;20:463. doi:10.1186/s12891-019-2833-4
44. Cooper NA, Scavo KM, Strickland KJ, et al. Prevalence of gluteus medius weakness in people with chronic low back pain compared to healthy controls. Eur Spine J. 2016;25:1258–1265. doi:10.1007/s00586-015-4027-6
45. Sadeghi H, Sadeghi S, Prince F, et al. Functional roles of ankle and Hip sagittal muscle moments in able-bodied gait. Clin Biomech. 2001;16:688–695. doi:10.1016/S0268-0033(01)00058-4
46. Sillevis R, Cuenca-Zaldívar JN, Fernández-Carnero S, García-Haba B, Sanchez-Romero EA, Selva-Sarzo F. Neuromodulation of the Autonomic Nervous System in Chronic Low Back Pain: A Randomized, Controlled, Crossover Clinical Trial Biomedicines. 2023;11(6):1551. doi:10.3390/biomedicines11061551
47. Ballestra E, Battaglino A, Cotella D, Rossettini G, Sanchez-Romero EA, Villafane JH. ¿Influyen las expectativas de los pacientes en el tratamiento conservador de la lumbalgia crónica? Una revisión narrativa (Do patients’ expectations influence conservative treatment in Chronic Low Back Pain? A Narrative Review). Retos. 2022;46:395–403. doi:10.47197/retos.v46.93950
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.