Back to Journals » Clinical Ophthalmology » Volume 20
Effectiveness of Trabeculectomy in Primary Open-Angle Glaucoma with Low Preoperative Intraocular Pressure
Authors Katayama H, Tojo N, Toyoda N ![]() , Hayashi A
, Hayashi A ![]()
Received 2 December 2025
Accepted for publication 10 February 2026
Published 17 February 2026 Volume 2026:20 586125
DOI https://doi.org/10.2147/OPTH.S586125
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Hiroshi Katayama, Naoki Tojo, Naoki Toyoda, Atsushi Hayashi
Department of Ophthalmology, Graduate School of Medicine and Pharmaceutical Sciences, University of Toyama, Toyama, Japan
Correspondence: Atsushi Hayashi, Department of Ophthalmology, Graduate School of Medicine and Pharmaceutical Sciences, University of Toyama, 2630 Sugitani, Toyama, 930-0194, Japan, Tel +81-76-434-7363, Fax +81-76-434-5037, Email [email protected]
Purpose: The aim of this study was to evaluate the efficacy of trabeculectomy for primary open angle glaucoma (POAG) with low preoperative intraocular pressure (IOP).
Patients and Methods: This was a retrospective single facility, non-randomized study. We included POAG patients with preoperative IOP ≤ 12 mmHg who were taking maximally tolerance glaucoma medications. We enrolled 11 patients who underwent trabeculectomy and could be followed for ≥ 3 years. We used the value of inclination of the mean deviation (MD) slope (dB/year) as the speed of progression of visual field defects as an index of surgical efficacy. We compared the MD slope before and after trabeculectomy.
Results: The mean preoperative IOP was 11.1± 1.4 mmHg and the mean postoperative IOP was 6.5± 2.5, 8.6± 2.8 and 8.8± 2.1 mmHg at 1, 2, and 3 years respectively. The inclination value of MD slope significantly improved from − 1.19± 0.35 to − 0.13± 0.37 dB/year (p< 0.001). Trabeculectomy significantly decreased IOP and slowed the progression of visual field defects.
Conclusion: The results suggest that trabeculectomy might be effective even in patients with very low preoperative IOP.
Keywords: trabeculectomy, glaucoma, low IOP, NTG, MD slope
Introduction
Normal tension glaucoma accounts for more than 90% of all glaucoma cases in Japan.1 In Japan, there are many cases of glaucoma progressing despite low intraocular pressure (IOP) compared to other countries. In many low-IOP patients, glaucomatous damage to the visual field will progress if treatment is limited to eye drops. Although are multiple surgical treatments for glaucoma, the options for glaucoma patients with low preoperative IOP are limited. For example, while minimally invasive glaucoma surgery (MIGS) often reported that the post operative IOP results in mid-teen values of the mmHg range, and it is difficult to reduce below 12 mmHg.2 Tube shunt surgery is effective for glaucoma in general, but problematic for patients with low preoperative IOP because it is high risk of hypotony.3
On the other hand, trabeculectomy (Trab) has been reported to be effective at mitigating the visual field deterioration in patients with low-IOP glaucoma,4–7 and has become the most common surgery for such patients. During a Trab, a bleb is formed in the sub-tenon space to receive the outflow of aqueous humor, thereby further lowering the IOP. Following the Trab procedure in a patient with low-preoperative IOP glaucoma, the IOP must be strictly controlled by suture lysis, suturing, or needling.
In the special case of glaucomatous patients with very low preoperative IOP under 12 mmHg, it remains controversial whether surgical intervention is appropriate. However, we have encountered cases in which the visual fields are deteriorated despite very low IOP with tolerated eye drop treatment. The purpose of this study was to investigate whether trabeculectomy is effective for such patients. We included cases in which visual field defects progressed even when preoperative IOP was ≤12 mmHg. To our knowledge, this is the first study to examine the outcomes of trabeculectomy in patients with very low preoperative IOP of ≤12 mmHg. However, the question arises as to whether it is appropriate to evaluate the surgical outcomes based on IOP alone for such very low-IOP glaucoma patients. Indeed, Trab that targets very low IOP carries the risk of vision loss due to postoperative hypotony.8,9 Therefore, in addition to postoperative IOP, we compared the rate of deterioration of visual field defects before and after Trab, and postoperative visual acuity (VA).
Patients and Methods
Patients
This was a retrospective, single facility, non-randomized observational study. We included patients with primary open angle glaucoma (POAG) and preoperative IOP of 12 mmHg or less. We defined the preoperative IOP as the mean of the IOPs measured at the two visits prior to surgery while under treatment with glaucoma medication. Inclusion criteria were as follows: (1) POAG; (2) preoperative IOP ≤12 mmHg with glaucoma medications; (3) at least five visual field tests performed before surgery; (4) at least five visual field tests performed after surgery; (6) follow-up for more than 3 years after surgery; (7) best-corrected VA ≥0.1. We excluded patients who had undergone filtration glaucoma surgeries, or who had other eye disorders that affect vision or the visual field.
A total of 11 consecutive patients (11 eyes) who underwent Trab for the first time at Toyama University Hospital or Oyama Eye Clinic during the period from January 2017 to December 2021 met the inclusion criteria and were included in this analysis. Among them, 6 patients simultaneously underwent cataract surgery. One glaucoma specialist (N.T.) diagnosed the cases of POAG and performed Trab.
An experienced glaucoma specialist (N.T) diagnosed POAG using gonioscopy, fundus photography, optical coherent tomography (OCT) RS-3000 (Nidek; Aichi, Japan), and visual field testing (Humphrey visual field analyzer (HVF); Carl Zeiss Meditec, Dublin, CA). We measured IOP with Goldmann applanation tonometry (GAT). We did not predetermine the time of IOP measurement and did not consider the fluctuation of IOP.
Patients who have already received maximum glaucoma medication treatment but have not been found to be effective in preventing the progression of visual field damage were candidates for surgery. The surgical indication was determined by a single glaucoma specialist (N.T). This study adhered to the Declaration of Helsinki and was approved by the institutional review board of the University of Toyama (Approval No. R2024122). We provided a thorough explanation of possible consequences of the study to all patients before surgery and obtained written informed consent.
Surgical Techniques
All patients were performed by single surgeon (N.T.) with abundant experience in glaucoma filtration surgery. All patients underwent Trab as follows: Tenon’s capsule anesthesia and conjunctival marking were performed, followed by fornix-based conjunctival incision and dissection of Tenon’s capsule. After creating a 4x4mm square half-thickness scleral flap, a deep flap was created. Mitomycin C (MMC) 0.04% was applied for 4 minutes and then thoroughly irrigated with balanced salt solution. In the case of simultaneous cataract surgery, the cataract surgery was performed at this time. The surgical indication for simultaneous cataract surgery was determined by a single glaucoma specialist (N.T). The trabecular meshwork was removed, the peripheral iris was removed, and the scleral flap was sutured. The conjunctiva was sutured to prevent aqueous humor from leaking from the filtration bleb. Dexamethasone was injected in subconjunctiva, and antibiotic and steroid ointments were applied.
Evaluation of the Factors
The VF examinations were performed using a HVF with the standard 30–2 or 10–2 test pattern and the Swedish Interactive Threshold Algorithm (SITA) standard strategy. The 30–2 and 10–2 indications for visual field tests were determined by a glaucoma specialist (N.T). Visual field tests were performed preoperatively and postoperatively using the same visual field test pattern. We excluded cases that had not been examined more than five times with the same visual field test pattern. Progression of visual field defects was evaluated using analysis software HfaFiles ver.5 (Beeline Co., Tokyo). This software can display the slope of changes in mean deviation (MD) (dB) against time. We compared between preoperative and postoperative MD slopes (dB/year) and evaluate the effectiveness of Trab in decreasing the MD slope. We also used HVF data from contributing hospitals.
Definition of Success
We defined success as IOP reduction ratio ≥20% compared to the preoperative IOP. In this study, we did not use the absolute value of postoperative IOP for the definition of success due to very low preoperative IOP. We defined failure as following conditions: (1) IOP reduction ratio <20% on two consecutive visits after the first postoperative month; (2) IOP <5mmHg on two consecutive visits after the first postoperative month; (3) requiring additional glaucoma surgery; or (4) phthisis or loss of light perception. In this study, there was no failure criterion for IOP being too low. After Trab surgery, glaucoma medications were discontinued, and glaucoma medications treatment was added as need. The addition of glaucoma medication did not affect the definition of success or failure.
Postoperative Complications
We evaluated the postoperative complications as (1) choroidal detachment (CD), (2) shallow anterior chamber (subjectivity observed with a slit lamp), (3) hyphema (niveau formation) (4) hypotony maculopathy (vertical slices of OCT reveal folds on the macular area due to hypotony), (5) vitreous prolapse, (6) bullous keratopathy (the central corneal endothelial cell density could not be measured with the EM-3000 specular microscope (Tomey, Nagoya, Japan)) and (7) endophthalmitis.
Statistical Analysis
We used a Wilcoxon signed-rank test to compare pre- and post-operative outcomes. We used a Kaplan–Meier curve to estimate the survival rate of Trab surgery. All of the statistical analyses were performed with JMP Pro 14 software (SAS, Cary, NC). Significance was defined as a p-value <0.05.
Results
Ophthalmic Data
The surgeries were conducted without intraoperative complications such as expulsive hemorrhage. All cases were followed-up without additional glaucoma surgery within 3 years. The characteristics of the patients are summarized in Table 1.
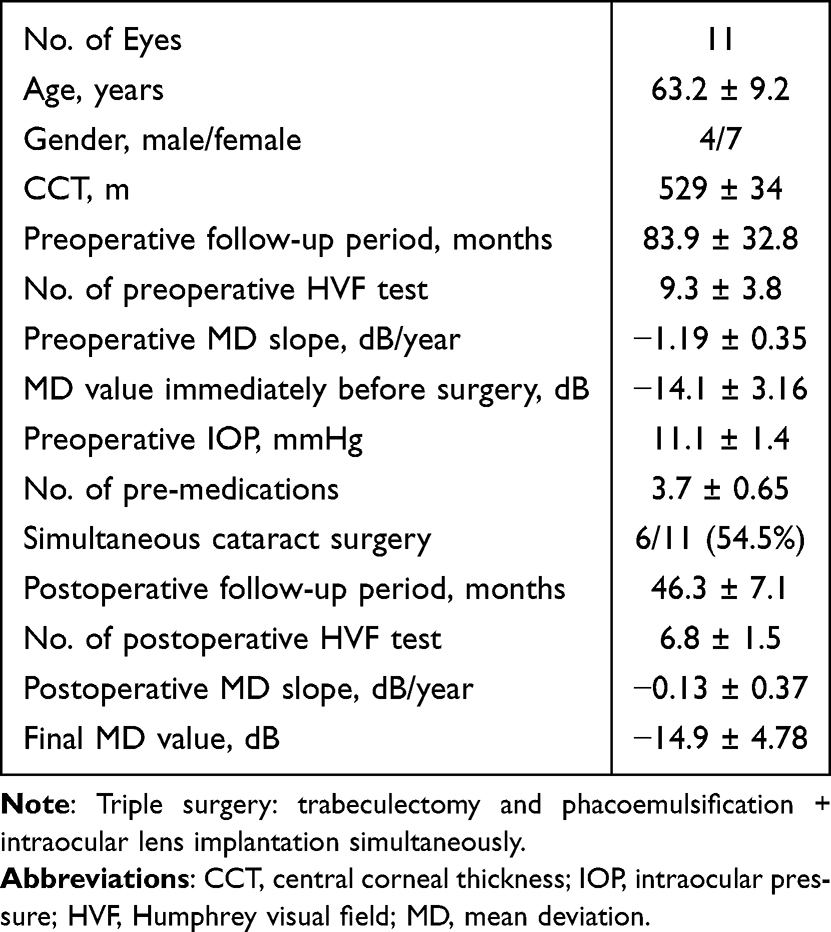 |
Table 1 Ophthalmic Data |
Postoperative IOP
The postoperative IOPs and the number of glaucoma medications are summarized in Table 2. The means of the postoperative IOPs at 6, 12, 18, 24, 30 and 36 months were significantly lower than the means of the preoperative IOPs. There was one case in which postoperative IOP at 3 years was higher than preoperative IOP. The results of the Kaplan-Meier analysis are illustrated in Figure 1. The success rates at 12, 24 and 36 months were 81.8%, 45.5% and 36.4%, respectively. As the reasons for failure, there were five cases due to IOP reduction ratio <20% and two cases due to IOP <5mmHg.
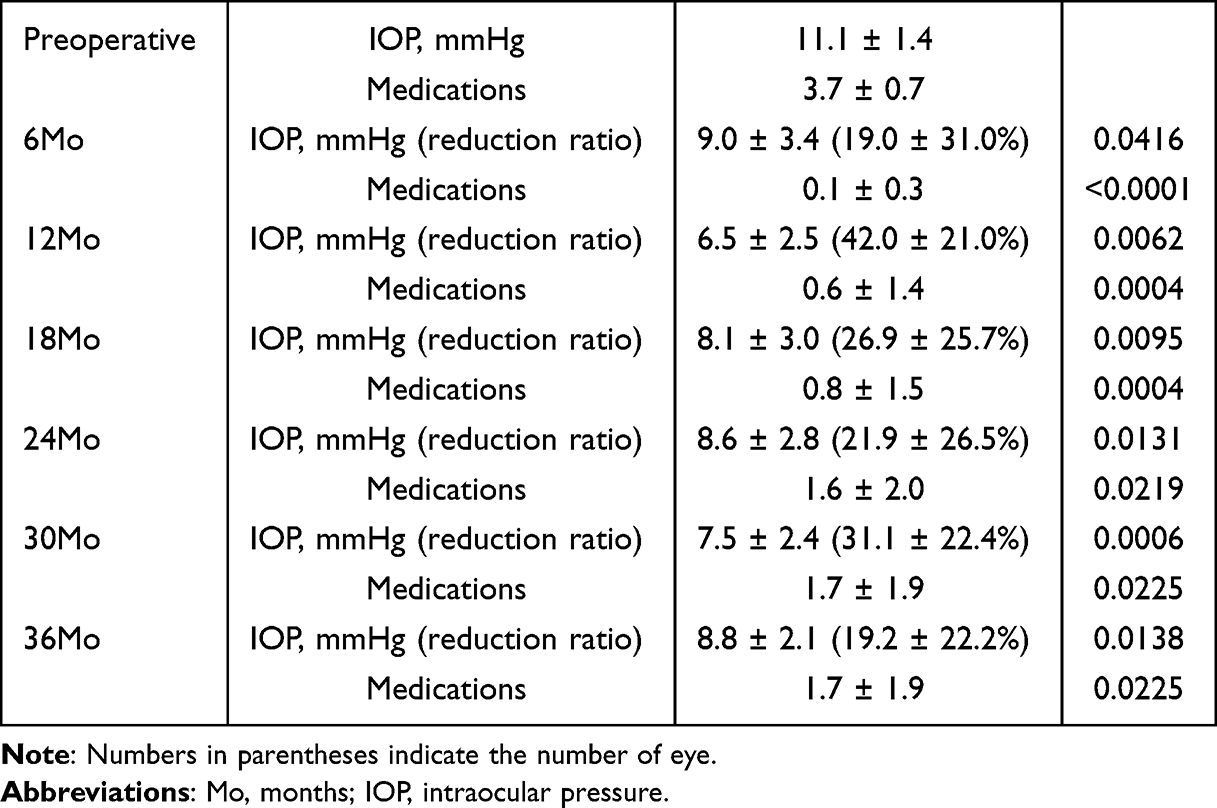 |
Table 2 Postoperative IOP and Number of Medications Numbers |
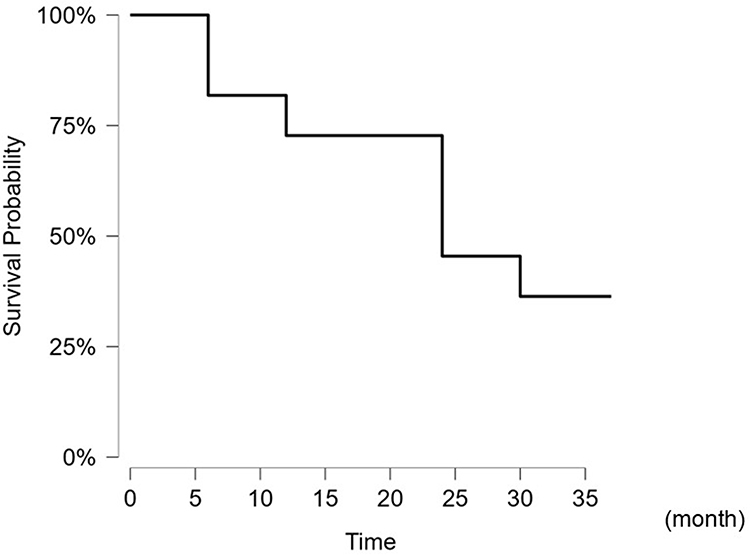 |
Figure 1 The Kaplan-Meier analysis of the 11 eyes. |
Visual Field
Nine cases were followed in the 30–2 mode, and 2 cases were followed in the 10–2 mode. Trab significantly improved the MD slope from −1.19 ± 0.35 to −0.13 ± 0.37 dB/year (p<0.001). There was no case in which the MD slope worsened compared with the preoperative MD slope. By extending the earlier progression of visual field defects across this same time period, we can estimate that a deterioration of 2.26 dB would have occurred without surgical intervention.
Visual Acuity
Table 3 provides the data of the mean VA and the difference from the preoperative VA to the postoperative VA. The decimal VA values were converted to logMAR. Even though 6 of the 11 studied cases underwent simultaneous cataract surgery, VA worsened after surgery. In particular, significant VA decline was observed at two years after surgery, however no significant VA decline was observed at three-year after surgery. In patients who underwent simultaneous cataract surgery, VA changed from 0.164 ± 0.426 to 0.185 ± 0.296 (p=0.786), while in patients who underwent Trab alone, VA changed from 0.177 ± 0.266 to 0.257 ± 0.311 (p=0.352) after 3 years. We did not observe any patients with postoperative wipe-out phenomenon.
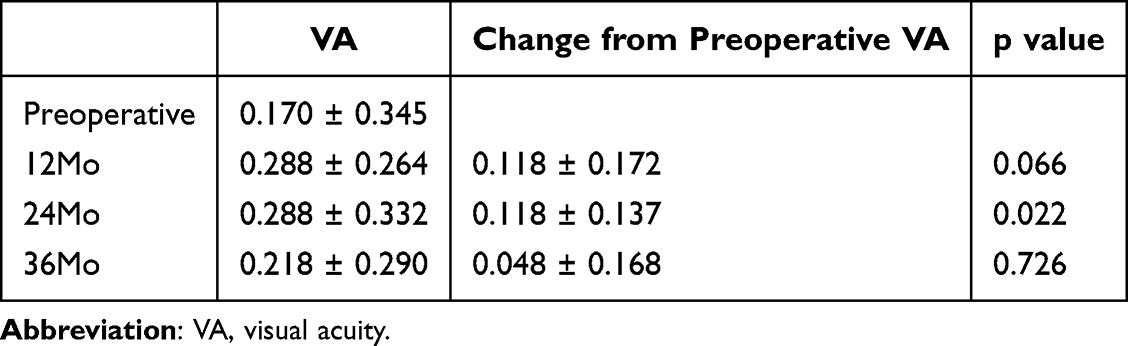 |
Table 3 Change of Visual Acuity |
Complications
The postoperative complications are summarized in Table 4. There were no cases with hypotony maculopathy, vitreous prolapse, bullous keratopathy or endophthalmitis.
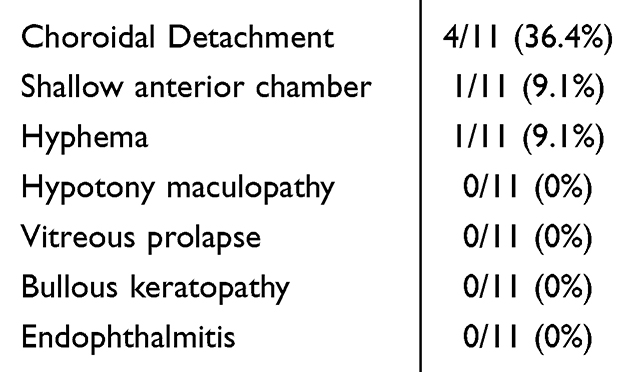 |
Table 4 Complications |
Discussion
NTG is defined as a POAG case with an untreated IOP of 21 mmHg or less.9 In this study, we could not confirm their untreated IOP. However, all included patients might NTG, we considered it impossible to define NTG and therefore referred to it as POAG. We believe that referring to the literature on NTG (low-IOP POAG) is not a problem.
Several studies have shown that trabeculectomy is also effective for NTG.5–7,10,11 It has been reported that trabeculectomy for NTG is associated with a high risk of complications.8,12 If visual field impairment persists despite low IOP, it is difficult to decide whether to recommend surgery or monitor the progress with eye drops treatment. Glaucoma is a multifactorial disease, and it is difficult to grasp the pathology based on just one factor, ie, IOP.13 Therefore, in order to confirm that the IOP is truly low and that visual field impairment is progressing, it is necessary to repeatedly perform visual field tests and measure IOP over several years. In this study, the mean of the follow-up period before surgery was extremely long at 83.9 months. During that time, visual field tests were performed an average of 9.3 times. It has been reported that visual field tests are more reliable when performed 10 times.14 Therefore, several years are required to obtain a reliable set of visual field test results, and glaucoma may worsen over that period. Indeed, in this study, the mean MD value had progressed to −14.1 dB immediately before surgery.
At present, reduction of the IOP is the only treatment reliably shown to improve glaucoma.14 Our results showed that the Trab could reduce IOP from 11.1 to 8.8 mmHg. Previous studies reported that Trab for NTG reduced IOP from 13.9 to 9.0 mmHg,15 from 13.9 to 8.1 mmHg,10 and from 16.2 to 11.0 mmHg.4 Another study estimated that a reduction of 30% or more in IOP is desirable for NTG.16 In this study, a reduction of approximately 20% in IOP was achieved. However, even with a 20% reduction in IOP, the progression of visual field defect was somewhat mitigated. Trab was suggested to be effective for glaucoma characterized by progression of the visual field impairment despite low preoperative IOP. It has been reported that either a 20% reduction from preoperative IOP or holding the IOP to single digits is effective in preventing the progression of NTG.17–19 However, the postoperative IOP needs to be about 6 to 9 mmHg, and very strict postoperative IOP control is required. In addition, it is expected that the risk of complications due to low IOP will inevitably increase. In this study, the number of patients who occurred CD was high compared to previous studies.8,10
Naito et al reported that when IOP us lowered below 7 mmHg, there is a high risk of deterioration of VA.10 Our results showed that VA was poor for up to two years after surgery, and gradually improved over the third year. Shoji et al reported that the risk factors of deterioration in VA after Trab were CD and shallow anterior chamber.20 These facts underscore that postoperative management should be performed by a doctor with extensive experience in Trab surgery.
Our results showed that Trab was effective in slowing the rate of visual field deterioration, from −1.19 to −0.13 dB/year. There have been several reports comparing the rate of progression of visual field defects between before and after Trab for NTG. Previous groups reported MD slope improvements of −0.70 to −0.25 dB/year,7 −0.91 to −0.31 dB/year,9 and −1.05 to −0.25 dB/year.19 Our results were similar to these previous reports.
Factors that have been reported to contribute to the progression of visual field defects include a thin CCT, large fluctuation of IOP, ocular perfusion pressure and advanced age.21–25 Although our study had a small number of patients and limited statistical power, we believe that it would be desirable to increase the number of patients and investigate risk factors in the future.
The success of glaucoma surgery is generally determined by the value of postoperative IOP. However, when preoperative IOP is already very low, the use of postoperative IOP as the sole criterion of surgical success can be misleading. In this study, five cases resulted in failure due to insufficient IOP reduction, however further reduction in IOP might increase the risk of failure due to < 5mmHg and the risk of VA aggravation. Maintaining long-term visual function is also an important factor for surgical success. It is thus necessary to consider not only IOP but also visual field and VA. However, visual field tests are subjective and not always reliable. Including VA as an index of surgical success could help to compensate for this limitation of visual field tests. Finally, we note that Trab has been reported to worsen VA, albeit not significantly.26 Patients should be fully apprised of the possibility of a decrease in VA.
It is unclear why there was a correlation between VA and MD slope in our analysis. VA and visual field do not necessarily correlate.27 In general, VA is often preserved until the end stage of glaucoma, and it is difficult to predict the visual field from VA. When damage occurs from the nerve fiber in the macula, the MD value may be in the acceptable range, but VA may be poor. Regarding the correlation between the progression of myopia and visual field defects, reports have described that patients with shorter axial length are more likely to have progression of visual field defects and that myopia is not a factor in the progression of visual field defects.28,29 Since one of our patients had high myopia (22.93–30.04 mm), the progression of visual field damage may also have been influenced by myopia in this analysis. In a study with only 11 cases, we cannot rule out that the inclusion of this highly myopic patient affected the accuracy of our results.
Several other study limitations bear mention. This research contained special cases, and there are many points that differ from the concept of normal glaucoma surgery. This was a retrospective analysis. Prospective studies would be preferable. Since the preoperative IOP was very low, the laser suture-lysis was intentionally performed earlier to achieve a lower target IOP than usual. There is a risk that the results would vary greatly depending on the preoperative IOP values. It has been reported that factors that contribute to progression of NTG include the presence of history of disc hemorrhage, high baseline IOP, long-term IOP fluctuation, significantly greater vertical cup-to-disc ratio, ocular perfusion pressure and blood pressure.30–33 We did not consider these factors. In addition, we did not analyze the results of visual field testing by segmented subfield. We were unable to compare the Visual Field Index before and after surgery. We included cases who underwent simultaneous cataract surgery. It has been reported that simultaneous cataract surgery affects the outcomes of glaucoma surgical.34 We did not define the indications for glaucoma surgery, cataract surgery, or additional glaucoma medications. The number of patients and times of visual field test were small and the follow-up period was short.
Although many glaucoma surgical devices have been developed, surgical methods for cases with very low preoperative IOP might be limited. Trab has the advantage of being able to adjust IOP after surgery and to achieve very low postoperative IOP. Trab was could significantly lower IOP and suppress the progression of visual field defects even in patients with low preoperative IOP.
Data Sharing Statement
The datasets in our study are available from the corresponding author on reasonable request.
Consent for Publication
We consent for publication.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received.
Disclosure
No potential conflict of interest was reported by the authors.
References
1. Iwase A, Suzuki Y, Araie M, et al. The prevalence of primary open-angle glaucoma in Japanese: the Tajimi study. Ophthalmology. 2004;111(9):1641–8. doi:10.1016/j.ophtha.2004.03.029
2. Lavia C, Dallorto L, Maule M, Ceccarelli M, Fea AM. Minimally-invasive glaucoma surgeries (MIGS) for open angle glaucoma: a systematic review and meta-analysis. PLoS One. 2017;12(8):e0183142. doi:10.1371/journal.pone.0183142
3. Coleman AL, Hill R, Wilson MR, et al. Initial clinical experience with the ahmed glaucoma valve implant. Am J Ophthalmol. 1995;120(1):23–31. doi:10.1016/S0002-9394(14)73755-9
4. Shigeeda T, Tomidokoro A, Araie M, Koseki N, Yamamoto S. Long-term follow-up of visual field progression after trabeculectomy in progressive normal-tension glaucoma. Ophthalmology. 2002;109(4):766–770. doi:10.1016/S0161-6420(01)01009-0
5. Koseki N, Araie M, Shirato S, Yamamoto S. Effect of trabeculectomy on visual field performance in central 30 degrees field in progressive normal-tension glaucoma. Ophthalmology. 1997;104(2):197–201. doi:10.1016/S0161-6420(97)30334-0
6. Hashimoto Y, Michihata N, Matsui H, Fushimi K, Yasunaga H, Aihara M. Reoperation rates after Ex-PRESS versus trabeculectomy for primary open-angle or normal-tension glaucoma: a national database study in Japan. Eye. 2020;34(6):1069–1076. doi:10.1038/s41433-019-0641-6
7. Mataki N, Murata H, Sawada A, Yamamoto T, Shigeeda T, Araie M. Visual field progressive rate in normal tension glaucoma before and after trabeculectomy: a subfield-based analysis. Asia-Pac J Ophthalmol. 2014;3(5):263–266. doi:10.1097/APO.0000000000000020
8. Jongsareejit B, Tomidokoro A, Mimura T, Tomita G, Shirato S, Araie M. Efficacy and complications after trabeculectomy with mitomycin C in normal-tension glaucoma. Japanese J Ophthalmol. 2005;49(3):223–227. doi:10.1007/s10384-004-0181-9
9. Lee BL, Bathija R, Weinreb RN. The definition of normal-tension glaucoma. J Glaucoma. 1998;7(6):366–371. doi:10.1097/00061198-199812000-00003
10. Naito T, Fujiwara M, Miki T, et al. Effect of trabeculectomy on visual field progression in Japanese progressive normal-tension glaucoma with intraocular pressure < 15 mmHg. PLoS One. 2017;12(8):e0184096. doi:10.1371/journal.pone.0184096
11. Lai C, Shao SC, Chen YH, Kuo YK, Lai CC, Chuang LH. Trabeculectomy with antimetabolite agents for normal tension glaucoma: a systematic review and meta-analysis. Front Med. 2022;9:932232. doi:10.3389/fmed.2022.932232
12. Hagiwara Y, Yamamoto T, Kitazawa Y. The effect of mitomycin C trabeculectomy on the progression of visual field defect in normal-tension glaucoma. Graefes Arch Clin Exp Ophthalmol. 2000;238(3):232–236. doi:10.1007/s004170050349
13. Vasile P, Valeria C, Speranta S, et al. Sympathetic context of the disease - a new era in glaucoma management. Romanian J Ophthalmol. 2021;65(1):15–19. doi:10.22336/rjo.2021.4
14. Taketani Y, Murata H, Fujino Y, Mayama C, Asaoka R. How many visual fields are required to precisely predict future test results in glaucoma patients when using different trend analyses? Invest Ophthalmol Visual Sci. 2015;56(6):4076–4082. doi:10.1167/iovs.14-16341
15. Nakajima K, Sakata R, Ueda K, et al. Central visual field change after fornix-based trabeculectomy in Japanese normal-tension glaucoma patients managed under 15 mmHg. Graefes Arch Clin Exp Ophthalmol. 2021;259(8):2309–2316. doi:10.1007/s00417-021-05215-y
16. Collaborative Normal-Tension Glaucoma Study Group. The effectiveness of intraocular pressure reduction in the treatment of normal-tension glaucoma. Am J Ophthalmol. 1998;126(4):498–505. doi:10.1016/S0002-9394(98)00272-4
17. Schultz SK, Iverson SM, Shi W, Greenfield DS. Safety and efficacy of achieving single-digit intraocular pressure targets with filtration surgery in wyes with progressive normal-tension glaucoma. J Glaucoma. 2016;25(2):217–222. doi:10.1097/IJG.0000000000000145
18. Aoyama A, Ishida K, Sawada A, Yamamoto T. Target intraocular pressure for stability of visual field loss progression in normal-tension glaucoma. Japanese J Ophthalmol. 2010;54(2):117–123. doi:10.1007/s10384-009-0779-z
19. Iverson SM, Schultz SK, Shi W, Feuer WJ, Greenfield DS. Effectiveness of single-digit IOP targets on decreasing global and localized visual field progression after filtration surgery in eyes with progressive normal-tension glaucoma. J Glaucoma. 2016;25(5):408–414. doi:10.1097/IJG.0000000000000240
20. Sato N, Kasahara M, Kono Y, et al. Early postoperative visual acuity changes after trabeculectomy and factors affecting visual acuity. Graefes Arch Clin Exp Ophthalmol. 2023;261(9):2611–2623. doi:10.1007/s00417-023-06076-3
21. Viswanathan D, Goldberg I, Graham SL. Relationship of change in central corneal thickness to visual field progression in eyes with glaucoma. Graefes Arch Clin Exp Ophthalmol. 2013;251(6):1593–1599. doi:10.1007/s00417-013-2295-6
22. Coleman-Belin J, Harris A, Chen B, et al. Aging effects on optic nerve neurodegeneration. Int J Mol Sci. 2023;24(3):2573. doi:10.3390/ijms24032573
23. Kim JS, Choi HJ, Park KH. Glaucoma conversion of the contralateral eye in unilateral normal-tension glaucoma patients: a 5-year follow-up study. Br J Ophthalmol. 2021;105(10):1383–1389. doi:10.1136/bjophthalmol-2020-316371
24. Ishida K, Yamamoto T, Kitazawa Y. Clinical factors associated with progression of normal-tension glaucoma. J Glaucoma. 1998;7(6):372–377. doi:10.1097/00061198-199812000-00004
25. Choi J, Kim KH, Jeong J, et al. Circadian fluctuation of mean ocular perfusion pressure is a consistent risk factor for normal-tension glaucoma. Invest Ophthalmol Vis Sci. 2007;48(1):104–111. doi:10.1167/iovs.06-0615
26. Costa VP, Smith M, Spaeth GL, Gandham S, Markovitz B. Loss of visual acuity after trabeculectomy. Ophthalmology. 1993;100(5):599–612. doi:10.1016/S0161-6420(93)31597-6
27. Ernest PJ, Schouten JS, Beckers HJ, Hendrikse F, Prins MH, Webers CA. An evidence-based review of prognostic factors for glaucomatous visual field progression. Ophthalmology. 2013;120(3):512–519. doi:10.1016/j.ophtha.2012.09.005
28. Chen DF, Wang C, Si Y, et al. Natural history and risk factors for glaucoma progression in Chinese patients with normal-tension glaucoma. Invest Ophthalmol Visual Sci. 2024;65(3):28. doi:10.1167/iovs.65.3.28
29. Han JC, Han SH, Park DY, Lee EJ, Kee C. Clinical course and risk factors for visual field progression in normal-tension glaucoma with myopia without glaucoma medications. Am J Ophthalmol. 2020;209:77–87. doi:10.1016/j.ajo.2019.08.023
30. Sakata R, Yoshitomi T, Iwase A, et al. Factors associated with progression of Japanese open-angle glaucoma with lower normal intraocular pressure. Ophthalmology. 2019;126(8):1107–1116. doi:10.1016/j.ophtha.2018.12.029
31. Lee JM, Caprioli J, Nouri-Mahdavi K, et al. Baseline prognostic factors predict rapid visual field deterioration in glaucoma. Invest Ophthalmol Visual Sci. 2014;55(4):2228–2236. doi:10.1167/iovs.13-12261
32. Lee K, Yang H, Kim JY, Seong GJ, Kim CY, Bae HW. Risk factors associated with structural progression in normal-tension glaucoma: intraocular pressure, systemic blood pressure, and myopia. Invest Ophthalmol Visual Sci. 2020;61(8):35. doi:10.1167/iovs.61.8.35
33. Leung DYL, Tham CC. Normal-tension glaucoma: current concepts and approaches-A review. Clin Exp Ophthalmol. 2022;50(2):247–259. doi:10.1111/ceo.14043
34. Ogata-Iwao M, Inatani M, Takihara Y, Inoue T, Iwao K, Tanihara H. A prospective comparison between trabeculectomy with mitomycin C and phacotrabeculectomy with mitomycin C. Acta ophthalmologica. 2013;91(6):e500–1. doi:10.1111/aos.12133
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Statistical Analysis of Factors Affecting Surgically Induced Astigmatism Following Trabeculectomy
Shiratori N, Nakamoto K, Nishio Y, Takano Y, Arima T, Kunishige T, Suzuki H, Igarashi T, Takahashi H
Clinical Ophthalmology 2022, 16:3833-3839
Published Date: 21 November 2022
Glaucoma Surgery and Ocular Blood Flow in Colour Doppler Imaging: Is There a Link?
Zarzecki M, Obuchowska I, Ustymowicz A, Konopińska J
Clinical Ophthalmology 2024, 18:49-60
Published Date: 6 January 2024
Compared to Trabeculectomy, Ex-Press® Surgery Significantly Decreased the Loss of Corneal Endothelial Cell Density in Low-Intraocular-Pressure Glaucoma: 3-Year Follow-Up
Otsuka M, Tojo N, Yamazaki H, Ueda-Consolvo T, Hayashi A
Clinical Ophthalmology 2024, 18:3009-3015
Published Date: 22 October 2024
Trends in Glaucoma Fellowship Surgical Experience
Creagmile J, Chen N, Yee P, Lin K, Fox A, Smith A, Kwan C, Mosaed S
Clinical Ophthalmology 2025, 19:2719-2727
Published Date: 12 August 2025
Optimizing Filtration Surgery Procedures in African-Derived Populations: Trabeculectomy and Preserflo
Gazzard G, Kailani O, Muntasser H, Lim KS, Vig N, Yu J
Clinical Ophthalmology 2026, 20:570347
Published Date: 10 March 2026