Back to Journals » Journal of Inflammation Research » Volume 16
Effect of Triglyceride-Glucose Indices and Circulating PCSK9-Associated Cardiovascular Risk in STEMI Patients with Primary Percutaneous Coronary Artery Disease: A Prospective Cohort Study
Authors Zhao X, Song L, Li J, Zhou J, Li N, Yan S, Chen R ![]() , Wang Y, Liu C, Zhou P, Sheng Z, Chen Y, Zhao H, Yan H
, Wang Y, Liu C, Zhou P, Sheng Z, Chen Y, Zhao H, Yan H ![]()
Received 13 September 2022
Accepted for publication 5 December 2022
Published 21 January 2023 Volume 2023:16 Pages 269—282
DOI https://doi.org/10.2147/JIR.S389778
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Xiaoxiao Zhao,1,* Li Song,1,* Jiannan Li,1 Jinying Zhou,1 Nan Li,1 Shaodi Yan,2 Runzhen Chen,1 Ying Wang,1 Chen Liu,1 Peng Zhou,1 Zhaoxue Sheng,1 Yi Chen,1 Hanjun Zhao,1 Hongbing Yan2
1Department of Cardiology, Fuwai Hospital, National Center for Cardiovascular Diseases, Peking Union Medical College & Chinese Academy of Medical Sciences, Beijing, People’s Republic of China; 2Fuwai Hospital Chinese Academy of Medical Sciences, Shenzhen, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hongbing Yan, Fuwai Hospital, Chinese Academy of Medical Sciences, 12 Langshan Road, Shenzhen, 518000, People’s Republic of China, Tel +86-13701339287, Email [email protected] Hanjun Zhao, Department of Cardiology, Fuwai Hospital, Chinese Academy of Medical Sciences, No. 167, Beijing, 100037, People’s Republic of China, Tel +86-15210020808, Email [email protected]
Background and Aims: This study aimed to determine whether convertase subtilisin/kexin type 9 (PCSK9)-associated cardiovascular risk is modulated by triglyceride-glucose (TyG) in ST-segment elevation myocardial infarction (STEMI) patients with primary percutaneous coronary disease (PCI).
Methods: A total of 1541 patients with STEMI (aged ≥ 18 years) undergoing primary PCI were consecutively enrolled between March 2017 and March 2019.
Outcomes: When stratifying the overall population according to TyG indices less than or greater than the median (TyG median = 9.07) as well as according to quartiles of PCSK9 levels, higher TyG index levels were significantly associated with all-cause mortality only when TyG levels were 9.07 or higher (ie, relative to quartile 1 [Q1], the adjusted HR for all-cause mortality was 3.20 [95% CI, 0.54– 18.80] for Q2, p = 0.199; 7.89 [95% CI, 1.56– 40.89] for Q3, p = 0.013; and 5.61 [95% CI, 1.04– 30.30] for Q4, p = 0.045. During a median follow-up period of 1.96 years, the HR for all-cause mortality was higher in the subset of patients with TyG ≥median and PCSK9 ≥median (p for trend = 0.023) among those with type 2 diabetes mellitus (T2DM). However, there were no statistically significant differences among the subgroups. Among T2DM patients with a TyG index greater than the median, the Kaplan-Meier curve showed that patients with the highest PCSK9 levels had an increased risk of all-cause mortality (log-rank p = 0.017) and cardiac-cause mortality (log-rank p = 0.037) compared with lower PCSK9 quartile levels.
Conclusion: Elevated PCSK9 levels are related to all-cause mortality and cardiac-related mortality when TyG levels are greater than the median, but not when levels are less than the median. This suggests a potential benefit of lowering circulating PCSK9 levels in STEMI patients with insulin resistance.
Keywords: triglyceride glucose index, proprotein convertase subtilisin/kexin type 9, mortality, type 2 diabetes, ST-segment elevation myocardial infarction, primary percutaneous coronary intervention
Introduction
Pro-protein convertase subtilisin/kexin type 9 (PCSK9) produced in the liver and intestines plays a critical role in cholesterol metabolism by mediating the degradation of hepatic low-density lipoprotein cholesterol receptors (LDLR) in lysosomes, thereby resulting in decreased LDL-C clearance from circulation and elevated plasma levels.1,2 PCSK9 levels are genetically mediated and are considered causal in the development of atherosclerotic cardiovascular disease (ASCVD).3–5 Recent studies have demonstrated that PCSK9 can directly or indirectly contribute to atherosclerosis, from initiation to progression, by leading to endothelial cell apoptosis, secretion of inflammatory cytokines, and inhibition of platelet activation, thereby inducing an increase in the migratory capacity of monocytes and platelet count/fibrinogen levels6,7 (Figure 1). Notably, PCSK9 has emerged as a therapeutic target for ASCVD, with PCSK9 monoclonal antibodies (mAbs) including evolocumab and alirocumab (which are clinically used to decrease circulating PCSK9 levels), providing substantial and proven benefits for those at very high risk of cardiovascular events.8,9
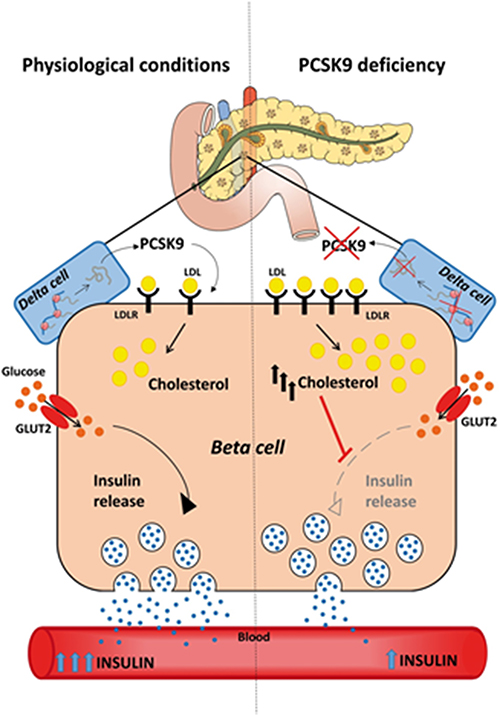 |
Figure 1 Influence of PCSK9 deficiency on β-cell function. Expression of low-density lipoprotein receptor (LDL-R) in β cells was controlled by the production of PCSK9. The deficiency of PCSK9 contribute to raised expression of LDL-R which result in increased accumulation of cholesterol esters and impact the glucose-stimulated insulin secretion and impaired glucose tolerance observed (referred from).6 Notes: Reproduced from Da Dalt L, Ruscica M, Bonacina F, et al. PCSK9 deficiency reduces insulin secretion and promotes glucose intolerance: the role of the low-density lipoprotein receptor. Eur Heart J. 2019;40(4):357–368, by permission of Oxford University Press.10 |
Despite these recent advances, the degree to which insulin resistance patient populations may benefit most from PCSK9 reduction remains unclear. It is likewise unclear whether there is an association between PCSK9 reduction and the incidence of cardiovascular endpoints among patients with insulin resistance. The triglyceride-glucose (TyG) index, derived from fasting blood glucose and fasting triglyceride (TG) levels, has been proposed as a surrogate biomarker for insulin resistance.11–14 Accordingly, in this study, we tested the hypothesis that PCSK-associated ASCVD risk would be statistically significantly modulated by levels of systemic insulin resistance in a large, contemporary STEMI population undergoing primary PCI. This study aimed to determine whether PCSK9-associated cardiovascular risk is modulated by TyG levels in ST-segment elevation myocardial infarction (STEMI) patients with primary percutaneous coronary disease (PCI). To our knowledge, the present study is the first study within a large cohort of STEMI patients undergoing primary PCI to demonstrate that PCSK9-associated ASCVD risk may be significantly mediated by concomitant levels of TyG.
Methods
Study Population
A total 1541 patients with STEMI aged≥18 years who undergoing primary PCI were consecutively enrolled between March 2017 and March 2019 and their baseline plasma PCSK9 levels were determined by ELISA (Flow chart was shown in Supplement Figure 1). The definition of STEMI followed the established criteria.15 The study protocol, approved by the Ethics Committee of Fuwai Hospital, Peking Union Medical College & Chinese Academy of Medical Sciences, was conducted in accordance with the principles outlined in the Declaration of Helsinki. Personal information related to the identities of the patients was concealed. Every patient signed the informed written consent before enrolled in the study.
Definition
Hypertension was defined as blood pressure (BP) ≥140/90 mmHg at rest over three measurements or a previous diagnosis of hypertension and current use of antihypertensive drugs.16 Patients were diagnosed with DM if they met one of the following criteria: (i) fasting plasma glucose level ≥7.0 mmol/L, (ii) 2-h plasma glucose value ≥11.1 mmol/L in the 75-g oral glucose tolerance test (OGTT), and (iii) casual plasma glucose level ≥11.1 mmol/L.17 Dyslipidaemia was defined by any of the following parameters:18 total cholesterol level ≥5.0 mmol/L, low-density lipoprotein cholesterol (LDL-C) level ≥3.0 mmol/L, triglyceride level ≥1.7 mmol/L, high-density lipoprotein cholesterol (HDL-C) level <1.2 mmol/L (in women) or <1.0 mmol/L (in men). Patients who did not meet the standards for never smokers (never smoked in their lifetime) or former light smokers (stopped smoking at least 15 years ago, with ≤10 total pack-years of smoking) were considered current smokers.19 Chronic kidney disease (CKD) was defined as abnormal kidney structure or function for more than 3 months, and end-stage renal disease (ESRD) was the final common pathway for CKD.20 MACEs were defined as a composite of all-cause death, myocardial infarction (MI) recurrence, and ischaemic stroke.
Laboratory Tests
Measurement of circulating PCSK9 levels Circulating levels of PCSK9 were measured using enzyme-linked immunosorbent assay (DY3888; R&D Systems, Catalog) according to the manufacturer’s instructions and compared with purified human PCSK9 standards.
Measurements
Baseline data, including patient clinical demographics such as age, sex, smoking status, history of disease (including hypertension, diabetes, hyperlipidemia and chronic kidney disease) and PCI, laboratory results, primary PCI procedures, and medical treatments, were obtained from hospital records. Serum levels of fasting plasma glucose and lipid profiles, including TG, total cholesterol (TC), lipase activator (LPA) and HDL-C, were determined by standard laboratory techniques at Fuwai Hospital. The TyG index was computed using the following formula: ln[fasting TG (mg/dL)×FPG (mg/dL)/2].12
Endpoints and Follow-Up
Recurrence MI was diagnosed as the symptom of typical chest pain or changes in typical serial electrocardiograms combined with positive cardiac troponins. Follow-up was performed by well-trained physicians routinely at 1, 6, and 12 months after the discharge via direct interviews, telephone calls and hospital discharge records or clinical notes, and well-trained physicians and nurses performed the clinical follow-up with the patients. The follow-up protocol was approved by obtaining permission from the Institutional Review Board of Chinese Academy of Medical Sciences Fuwai Hospital. Well-trained physicians in charge of the follow-up primary endpoints, including all-cause, death, cardiac death, recurrence MI, ischemic stroke, identified and extracted the primary endpoints from medical and hospital records, laboratory reports, clinical notes, and emergency records which required to be sent to our centers). There are two professional physicians blinded to the clinical and laboratory tests data confirmed the follow up endpoints.
Statistical Analysis
Continuous variables with normal or skewed distribution are shown as medians (interquartile range, IQR). Categorical variables are presented as frequencies (%). The subjects were divided into two groups according to the median level of TyG. For comparisons between groups, two-tailed independent-samples Student’s t-test for normally distributed variables and a Mann–Whitney U-test for variables with highly skewed distributions were performed. The chi-squared test was applied to compare the categorical variables. Univariate and multivariate Cox regression was carried out to determine the potential association between PCSK9 levels and the risk of endpoints events including all-cause mortality, cardiac death, recurrence MI and ischemic stroke. Hazard ratios (HRs) and 95% confidence intervals (CIs) for the relationship between PCSK9 combined with TyG and the incidence of endpoints events were generated with Cox regression models. Adjusted for the variables in model including age, gender, history of hypertension, history of diabetes mellitus, history of hyperlipidemia, history of coronary artery bypass graft, history of PCI, history of chronic kidney disease, current smoking, high-sensitivity C-reactive protein (hs-CRP), LDL-C, height, weight, heart rate at admission, systolic blood pressure, diastolic blood pressure, the use of statin, the TIMI flow prior and post-PCI, creatinine, lipase activator (lpa) and the use of intra-aortic balloon pump. PCSK9 categories depended on quartiles using the lowest quartile group as the reference. Subgroups were divided according to age (<65 years versus≥65 years), LDL-C (<70 mg/dL versus≥70 mg/dL)], and the status of T2DM (present versus absent). The areas under the receiver operating characteristic curve (ROC), sensitivity, specificity, Youden index and 95% CIs were calculated to evaluate the predictive ability of TyG combined with PCSK9 for mortality. Kaplan-Meier survival curves were constructed to evaluate the incidence rate of mortality according to the optimal quartile point of the PCSK9 among T2DM the groups divided by the median of TyG, and discrepancy rates of cumulative events were compared using the Log rank test.
All analyses were performed using SPSS (version 20.0; IBM Corp., Armonk, NY, USA), R Programming Language X64 4.0.4 (R Foundation for Statistical Computing, Vienna, Austria), and MedCalc version 18.2.1 (MedCalc Software, Ostend, Belgium). P values of<0.05 were considered statistically significant in all of the analyses, and all P values were two-tailed.
Results
Baseline Participant Characteristics
Table 1 describes the baseline clinical and biochemical characteristics of 1541 participants stratified according to achieved TyG levels at baseline (<median vs ≥median). The mean age of the participants was 61.0 years. Notably, 80.3% of the participants were men and 64.8% had hypertension. However, when baseline characteristics were evaluated according to median TyG levels, those with TyG levels of 9.07 or more (versus levels less than 9.07) had higher mean PCSK9 levels (means and interquartile ranges [IQRs]; 44.1 [23.7, 83.8] versus 49.0 [27.1, 92.7]) and a more frequent cluster of common cardiovascular risk factors (diabetes mellitus [DM], higher active greater low-density lipoprotein cholesterol levels, higher triglyceride levels, higher hs-CRP levels, and higher systolic and diastolic blood pressure levels). These participants were also more likely to be receiving beta-blockers. The prevalence of individual medical and demographic characteristics and the intersections of cardiovascular risk factors and endpoints are shown in Figure 2. The most frequently observed risk factor among participants with a TyG index less than the median was hyperlipidemia, followed by current smoking status, hypertension, and type 2 diabetes mellitus (T2DM). The prevalence of the risk factors mentioned above was similar among participants with TyG indices greater than the median. The most frequently observed intersection pattern was the simultaneous presence of all eight features.
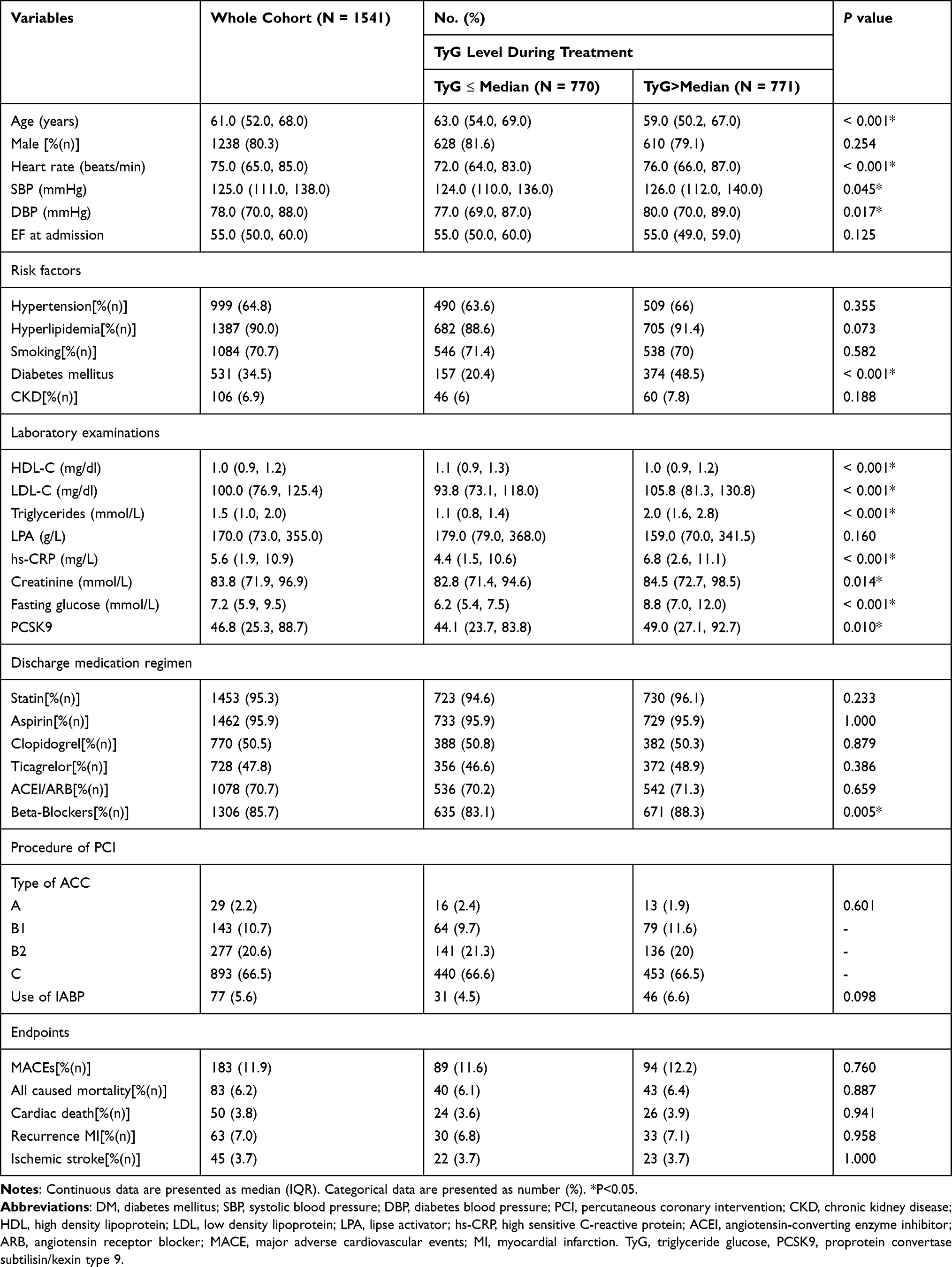 |
Table 1 Baseline Clinical and Optical Coherence Tomography Characteristics of the Study Population |
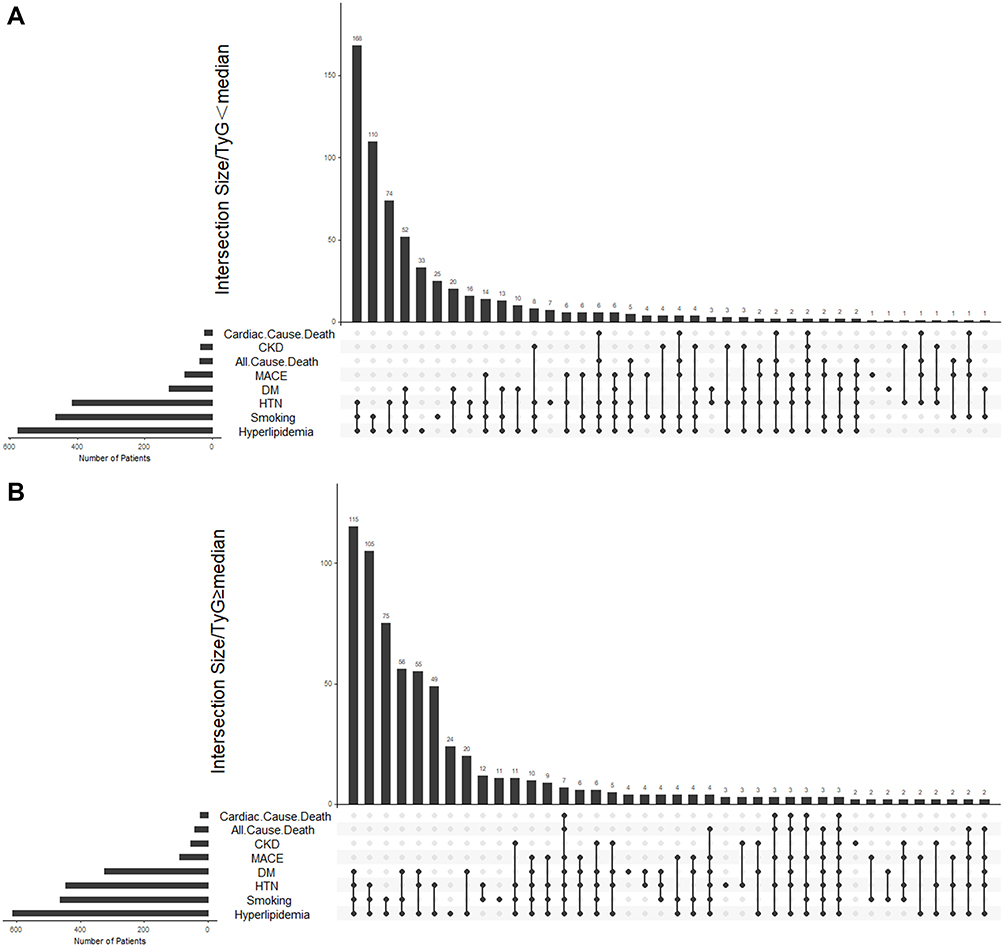 |
Figure 2 Upset plot of factors and intersections of cardiovascular risk characteristics (hyperlipidemia, status of smoking, hypertension, diabetes mellitus and chronic kidney disease) and endpoints during follow-up period (all cause death, cardiac cause death, major adverse cardiovascular events) of TyG <median (A) and TyG ≥median (B). Abbreviations: CKD, chronic kidney disease; HTN, hypertension, DM, diabetes mellitus; MACE, major adverse cardiovascular events; TyG, triglyceride glucose. |
Association Between Circulating PCSK9 Levels Combined with TyG and Incident of Endpoints
Table 2 describes univariable and fully adjusted multivariable associations between endpoints (including all-cause mortality, cardiac-cause mortality, recurrent myocardial infarction [MI], and ischemic stroke) stratified according to TyG and PCSK9 levels at baseline. When stratifying the overall population according to TyG indices (stratified at the median TyG level, 9.07) and quintiles of PCSK9 levels, higher TyG index levels were statistically significantly associated with all-cause mortality only when TyG levels were 9.07 or greater (relative to Q1, the adjusted HR for all-cause mortality was 3.20 [95% CI, 0.54–18.80] for Q2, p = 0.199; 7.89 [95% CI, 1.56–40.89] for Q3, p = 0.013; and 5.61 [95% CI, 1.04–30.30] for Q4, p = 0.045. The effect estimate for the trend test was 1.62 [95% CI, 1.07–2.45], p for trend = 0.023. In the setting of lower TyG levels (ie, less than the median), higher PCSK9 levels were not associated with a greater risk of clinical events. We observed a statistically significant interaction between PCSK9 and PCSK9 dichotomies in terms of all-cause mortality (p for interaction (crude) = 0.008, p for interaction (adjusted) = 0.033). Figure 3 shows the continuous hazard ratio across logarithmic PCSK9 levels for all-cause mortality according to crude and adjusted restricted cubic spline analyses among participants in all cohorts, as well as among diabetes mellitus (DM) and non-DM patients, stratified according to median levels of TyG. The RCS analysis showed that an increase in PCSK9 was consistently associated with a higher risk of all-cause mortality.
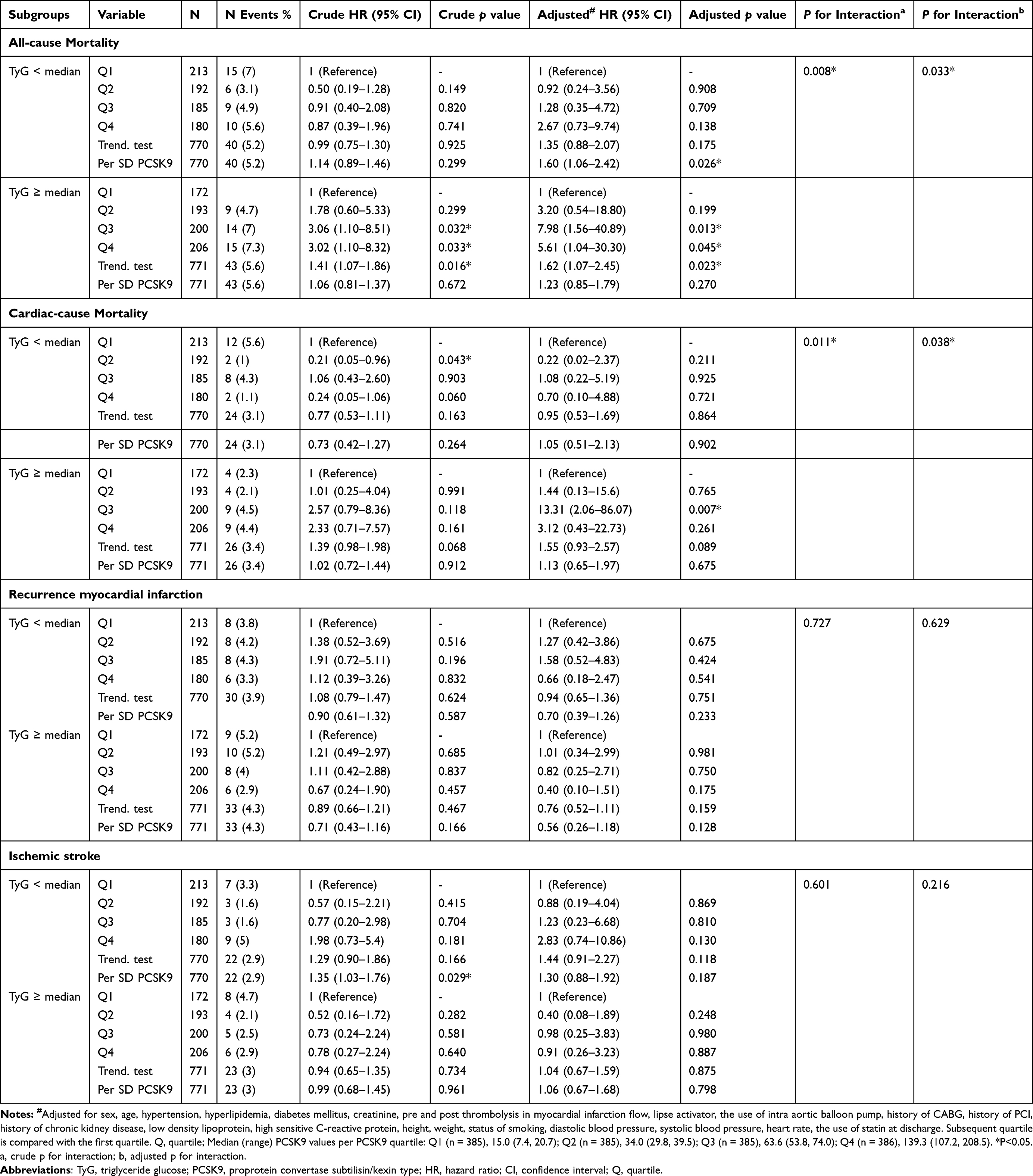 |
Table 2 Univariate and Multivariate Analyses of the Impact of TyG and PCSK9 on Endpoints |
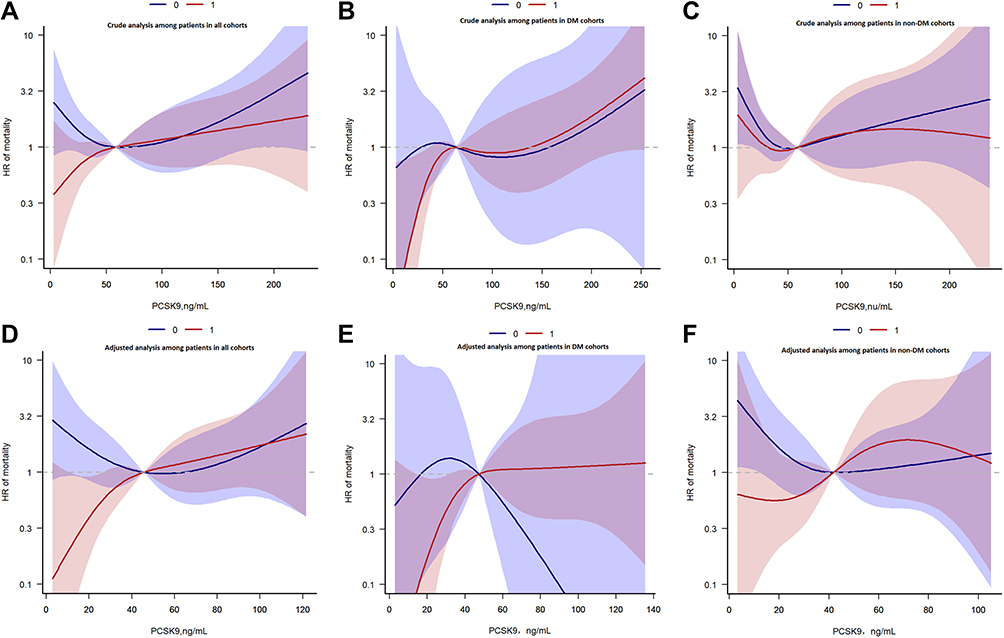 |
Figure 3 Continuous hazard ratio across logarithmic PCSK9 for all-cause mortality according to restricted cubic spline crude and adjusted analysis among patients in all cohorts, DM patients and non-DM patients stratified by TyG according to median. (A), Crude analysis among patients in all cohorts; (B), Crude analysis among patients in DM cohorts; (C), Crude analysis among patients in non-DM cohorts; (D), Adjusted analysis among patients in all cohorts; (E), Adjusted analysis among patients in DM cohorts; (F), Adjusted analysis among patients in non-DM cohorts. 0=TyG <median; 1=TyG≥median; HR, hazard ratio, line, predicted HR, dashed area, 95% confidence interval. Adjusted for age, gender, hypertension, hyperlipidemia, lipse activator, triglycerides, the use of intra-aortic balloon pump, history of CABG, history of PCI, high sensitive C-reactive protein, height, weight, low density lipoprotein, fasting glucose, diastolic blood pressure, systolic blood pressure, heart rate, the use of statin at discharge. |
Subgroup Analyses
During a median of 1.96 days of follow-up of, the hazard ratio for all-cause mortality was higher in the subset of participants with TyG ≥median and PCSK9 ≥median (p for trend = 0.023) among those with T2DM (Table 3). However, there were no statistically significant differences in the trend tests among subgroups divided by age (<65 vs ≥65 years) or LDL-C levels (<70 vs ≥70 mg/L).
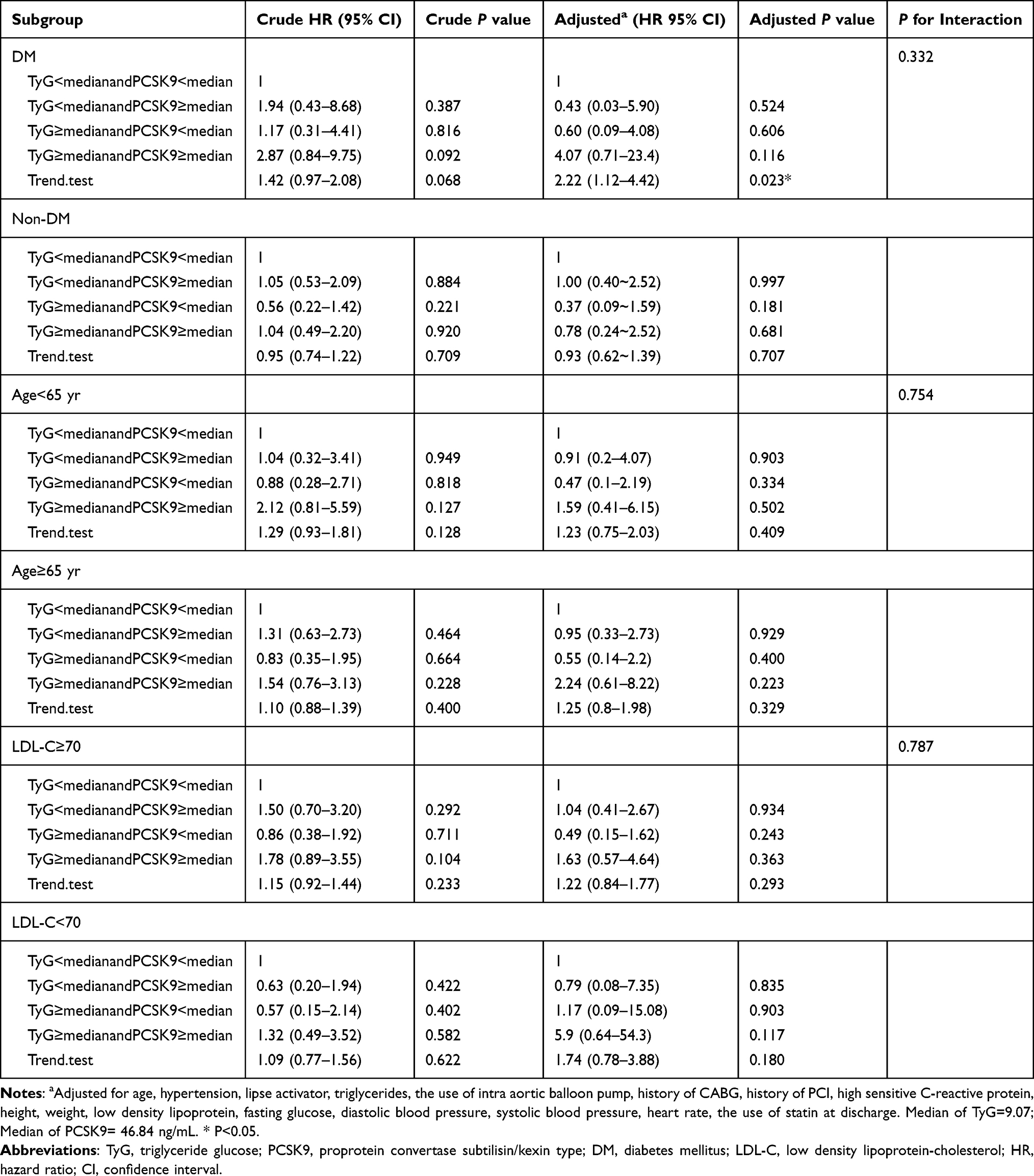 |
Table 3 Stratified Analyses of the Associations Between Risk for Incident All-Cause Mortality and the Groups According to PCSK9&TyG |
Figure 4 shows the Kaplan-Meier curves for the cumulative incidence of all-cause mortality up to a median of 1.96 years, stratified by quartiles of PCSK9 index levels among the T2DM subgroups, and divided by the median TyG level. Among T2DM participants with a TyG index greater than the median, the K-M curve showed that participants in the group with the highest PCSK9 levels had an increased risk of all-cause mortality (log-rank p = 0.017) (Figure 4A) and cardiac-cause mortality (log-rank p = 0.037) (Figure 4B) compared with the other quartiles of PCSK9 levels. However, there were no statistically significant differences between the four groups among T2DM patients with TyG indices less than the median (Figure 4C and 4D).
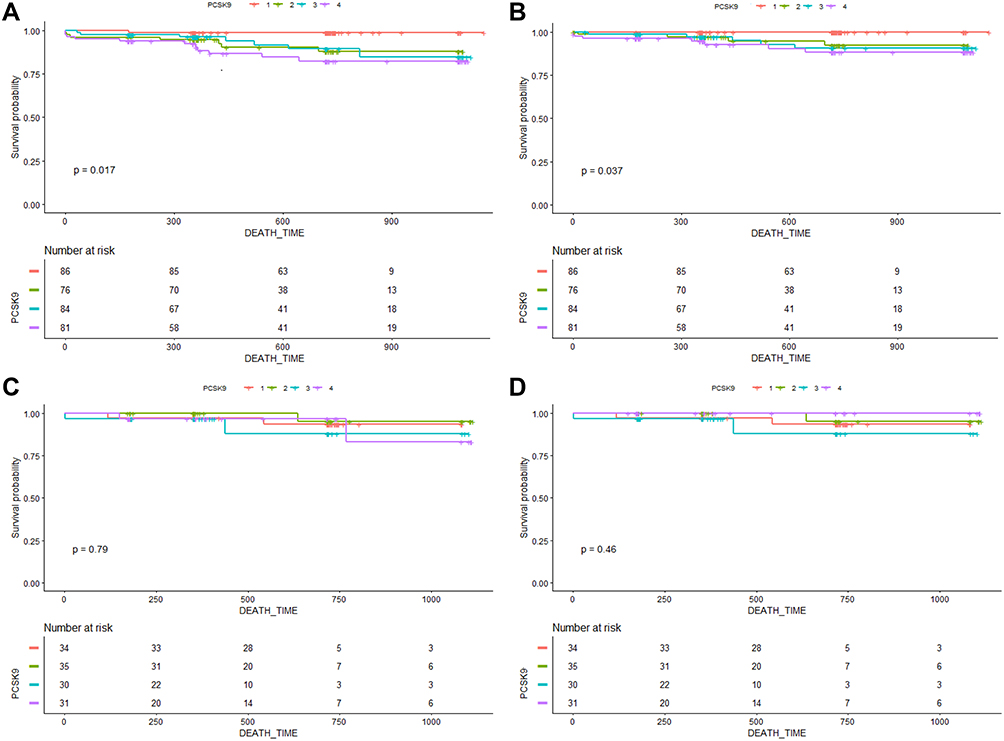 |
Figure 4 Kaplan-Meier Curves of all-cause mortality and cardiac cause mortality stratified by achieved proprotein convertase subtilisin/kexin type (PCSK9) quartiles in the setting of achieved triglyceride glucose (TyG) levels of less than median vs median or more among patients with diabetes mellitus. (A), Kaplan-Meier Curves of all-cause mortality stratified by PCSK9 quartiles in the setting of achieved TyG levels of median or more among patients with DM. Test of trend across quartiles: P = 0.017. (B), Kaplan-Meier Curves of cardiac-cause mortality stratified by PCSK9 quartiles in the setting of achieved TyG levels of median or more among patients with DM. Test of trend across quartiles: P = 0.037. (C), Kaplan-Meier Curves of all-cause mortality stratified by PCSK9 quartiles in the setting of achieved TyG levels of less than median among patients with DM. Test of trend across quartiles: P = 0.790. (D), Kaplan-Meier Curves of cardiac cause mortality stratified by PCSK9 quartiles in the setting of achieved TyG levels of less than median among patients with DM. Test of trend across quartiles: P = 0.460. Subsequent quartile is compared with the first quartile. Q, quartile; Median (range) PCSK9 values per PCSK9 quartile: Q1 (n = 385), 15.0 (7.4, 20.7); Q2 (n = 385), 34.0 (29.8, 39.5); Q3 (n = 385), 63.6 (53.8, 74.0); Q4 (n = 386), 139.3 (107.2, 208.5). *P<0.05. Abbreviations: PCSK9, proprotein convertase subtilisin/kexin type; TyG, triglyceride glucose; DM, diabetes mellitus. |
Discussion
We demonstrate for the first time, to our knowledge, that circulating PCSK9 level mediated ASCVD risk appears to be mediated by concomitant TyG levels in a large, contemporary, cohort with STEMI who undergoing the primary PCI. In fully adjusted analyses, we elucidated a stepwise association between PCSK9 levels and all-cause mortality only in individuals with greater degrees of systemic insulin resistance (ie, baseline TyG levels ≥median). No association between rising PCSK9 levels and all-cause mortality was noted when TyG levels were less than the median. These data shed new light on the apparent interdependence of two known mediators of primary and residual ASCVD risk: PCSK9 and systemic insulin resistance.
TyG Levels and PCSK9-Associated Cardiovascular Risk
The most striking finding in the current study was the positive association between circulating PCSK9 levels and an increased risk of all-cause mortality in patients with TyG index levels greater than the median (after both crude and full adjustment). Previous studies have demonstrated that individuals with lower plasma PCSK9 levels had a higher prevalence of DM, based on 539 stable coronary artery disease cohorts.21 Furthermore, a study at the cellular level22 found that liraglutide, a glucagon-like peptide-1 receptor agonist, can suppress blood glucose and decrease PCSK9 expression through an HNF1α-dependent mechanism. A population-based prospective study enrolling 4205 subjects with pre-diabetes concluded that elevated circulating PCSK9 levels were correlated with an increased incidence of type 2 diabetes during a median follow-up period of 3.1 years.23 Moreover, evidence from animal studies and at the cellular level has shown that downregulation of PCSK9 and inhibition of PCSK9 and the LDL receptor by polydatin ameliorates glucose metabolism.24 Higher levels of PCSK9 have been correlated with type 125 and type 2 diabetes,26 and this correlation increased substantially with worsening glycemic control.27 Longitudinal analyses by Ramin-Mangata et al28 showed that the presence of T2DM may modify the association between plasma PCSK9 and non-HDL cholesterol among DM patients. These findings suggest a possible role of PCSK9 in glucose metabolism.
We observed that elevated PCSK9 concentrations were positively related to all-cause mortality and cardiac-related mortality when TyG levels were higher than the median. Nevertheless, the exact molecular mechanisms of PCSK9 and insulin resistance remain unclear, and it is necessary to investigate the precise mechanisms underlying these associations in future studies. PCSK9 monoclonal antibodies (mAbs), including evolocumab and alirocumab, have been clinically used to decrease circulating PCSK9 levels, and are proven to provide substantial benefits for patients at very high risk of cardiovascular events.29 Although the present analysis outlines the utility of measuring TyG levels among a STEMI cohort undergoing primary PCI to better assess PCSK9-associated ASCVD risk, the data are also noteworthy for a lack of Lp(a)-associated ASCVD risk given TyG levels less than 9.07 (ie, the median level), irrespective of the magnitude of PCSK9 elevation. The present data are supported by the clinical prospective observations of Shi et al30 in a Chinese study, which demonstrated an association between circulating PCSK9 levels and the risk of T2DM. Similarly, a closer analysis of Table 2 within the present study suggests that, for individuals with TyG levels at the median or higher, each SD unit increase in PCSK9 level confers a 23% increased risk of all-cause mortality.
Mechanisms of PCSK9 Combined with TyG in Atherosclerosis and Cardiovascular Risk
Within the current literature, Mendelian randomization studies have recently proven that genetic variants of PCSK9 are associated with higher circulating fasting glucose concentrations as well as an increased risk of T2DM.31,32 Lorenzo et al have shown that PCSK9 critically controls LDLR expression in the pancreas and may contribute to the maintenance of proper physiological balance in order to limit cholesterol overload in beta cells, as described in experimental models; a possible mechanism underlying this causal association may be the identification of LDLR in the pancreatic islets as a potential target for locally produced PCSK9.10 Furthermore, these observations suggest that PCSK9 decreases plasma insulin levels, which is paralleled by cholesterol ester accumulation and increased insulin content. More interestingly, insulin secretion and cellular toxicity have been associated with the accumulation of cholesterol in pancreatic islets, indicating a critical role of cholesterol metabolism in the pancreas.33,34 Consequently, genetic and acquired that increase LDL-R expression should be closely related to altered glucose metabolism. Notably, the deficiency of selective β cells favors cholesterol accumulation in β cells, which is closely related to impaired insulin secretion under hypercholesterolemic conditions.6,35 An increase in cholesterol esters reduced by PCSK9 may weaken the intracellular response, which is designed to mitigate free cholesterol cell toxicity and could result in long-term cell apoptosis.34,36,37 However, it is important to stress that the differences in lipid and lipoprotein metabolism in mice as compared with humans suggest the need to further address the crosstalk among these pathways. Based on our findings, this observation could be a result of the synergistic effects of systemic insulin resistance and PCSK9-related pro-atherosclerotic or pro-thrombotic mechanisms, lowering the PCSK9 cut-off point for mediating secondary ASCVD-related events.
Limitation
This study has some limitations that must be given consideration. First, the use of a single baseline PCSK9 measurement (ie, the absence of evaluating effects of longitudinal changes in the incidence of cardiovascular events during the follow-up period to predict outcomes) did not allow us to assess the causal risk for incident cardiovascular endpoints. Thus, further studies are necessary to clarify the mechanisms underlying the association between PCSK9 levels and insulin resistance. Third, it is unclear whether our findings in STEMI individuals in China can be generalized to other diseases or other ethnicities. Therefore, further prospective investigations among diverse populations, larger sample sizes, and studies with long-term follow-up should be undertaken. Lastly, loss or gain of function PCSK9 gene mutations may have had an impact on the statistical results of the current study.38 However, due to the study design, we did not analyze PCSK9 mutations.
Conclusions
To our knowledge, the present study is the first study within a large cohort of STEMI patients undergoing primary PCI to demonstrate that PCSK9-associated ASCVD risk may be significantly mediated by concomitant levels of insulin resistance which represented by TyG. Elevated PCSK9 levels are related to all-cause mortality and cardiac-related mortality when TyG levels are greater than the median, but not when these levels are less than the median. These findings shed further insight into the mechanisms underlying PCSK9-associated ASCVD risk and might prove useful for identifying individuals who would benefit the most from novel PCSK9-lowering therapies. These findings likewise suggest a potential benefit of lowering the circulation levels of PCSK9 in STEMI patients with insulin resistance.
Data Sharing Statement
The datasets used and/or analyzed during this study are available from the corresponding author on reasonable request.
Ethics Approval
It is from the ethics committee of the department of Cardiology, Fuwai Hospital, National Center for Cardiovascular Diseases, Peking Union Medical College, China.
Consent for Publication
Written informed consent for publication was obtained from all participants.
Acknowledgments
The authors gratefully acknowledge all individuals who participated in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences (2016-I2M-1–009), National Natural Science Funds (number: 81970308), the Fund of “Sanming” Project of Medicine in Shenzhen (number: SZSM201911017) and Shenzhen Key Medical Discipline Construction Fund (number: SZXK001).
Disclosure
No conflicts of interest, financial or otherwise, are declared by the authors.
References
1. Zhang D-W, Lagace TA, Garuti R, et al. Binding of proprotein convertase subtilisin/kexin type 9 to epider- mal growth factor-like repeat A of low density lipoprotein receptor decreases receptor recycling and increases degradation. J Biol Chem. 2007;282:18602–18612. doi:10.1074/jbc.M702027200
2. Li C, Lin L, Zhang W, et al. Efficiency and safety of proprotein convertase subtilisin/kexin 9 monoclonal antibody on hypercholesterolemia: a meta-analysis of 20 randomized controlled trials. J Am Heart Assoc. 2015;4:e001937. doi:10.1161/JAHA.115.001937
3. Sabatine MS, Giugliano RP, Keech AC, et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med. 2017;376(18):1713–1722. doi:10.1056/NEJMoa1615664
4. Schwartz GG, Steg PG, Szarek M, et al. Alirocumab and cardiovascular outcomes after acute coronary syndrome. N Engl J Med. 2018;379(22):2097–2107. doi:10.1056/NEJMoa1801174
5. Sabatine MS, Leiter LA, Wiviott SD, et al. Cardiovascular safety and efficacy of the PCSK9 inhibitor evolocumab in patients with and without diabetes and the effect of evolocumab on glycaemia and risk of new-onset diabetes: a prespecified analysis of the Fourier randomised controlled trial. Lancet Diabetes Endocrinol. 2017;5(12):941–950. doi:10.1016/S2213-8587(17)30313-3
6. Tang Y, Li SL, Hu JH, Sun KJ, Liu LL, Xu DY. Research progress on alternative non-classical mechanisms of PCSK9 in atherosclerosis in patients with and without diabetes. Cardiovasc Diabetol. 2020;19(1):33. doi:10.1186/s12933-020-01009-4
7. Ferri N, Marchianò S, Tibolla G, et al. PCSK9 knock-out mice are protected from neoin- timal formation in response to perivascular carotid collar placement. Atherosclerosis. 2016;253:214–224. doi:10.1016/j.atherosclerosis.2016.07.910
8. Camera M, Rossetti L, Barbieri SS, et al. PCSK9 as a positive modulator of platelet activation. J Am Coll Cardiol. 2018;71(8):952–954. doi:10.1016/j.jacc.2017.11.069
9. Gencer B, Mach F, Murphy SA, et al. Efficacy of evolocumab on cardiovascular outcomes in patients with recent myocardial infarction: a prespecified secondary analysis from the Fourier trial. JAMA Cardiol. 2020;5(8):952–957. doi:10.1001/jamacardio.2020.0882
10. Da Dalt L, Ruscica M, Bonacina F, et al. PCSK9 deficiency reduces insulin secretion and promotes glucose intolerance: the role of the low-density lipoprotein receptor. Eur Heart J. 2019;40(4):357–368. doi:10.1093/eurheartj/ehy357
11. Cannon CP, Blazing MA, Giugliano RP, et al.; IMPROVE-IT Investigators. Ezetimibe added to statin therapy after acute coronary syndromes. N Engl J Med. 2015;372(25):2387–2397. doi:10.1056/NEJMoa1410489
12. Guerrero-Romero F, Simental-Mendia LE, Gonzalez-Ortiz M, et al. The product of triglycerides and glucose, a simple measure of insulin sensitivity. Com- parison with the euglycemic-hyperinsulinemic clamp. J Clin Endocrinol Metab. 2010;95(7):3347–3351. doi:10.1210/jc.2010-0288
13. Mazidi M, Kengne AP, Katsiki N, Mikhailidis DP, Banach M. Lipid accumula- tion product and triglycerides/glucose index are useful predictors of insulin resistance. J Diabetes Complicat. 2018;32(3):266–270. doi:10.1016/j.jdiacomp.2017.10.007
14. Du T, Yuan G, Zhang M, Zhou X, Sun X, Yu X. Clinical usefulness of lipid ratios, visceral adiposity indicators, and the triglycerides and glu- cose index as risk markers of insulin resistance. Cardiovasc Diabetol. 2014;13:146. doi:10.1186/s12933-014-0146-3
15. Ibanez B, James S, Agewall S, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39:119–177. doi:10.1093/eurheartj/ehx393
16. Aronow WS. Hypertension guidelines. Hypertension. 2011;58(3):347–348. doi:10.1161/HYPERTENSIONAHA.111.177147
17. Rubino F, Nathan DM, Eckel RH, et al. Metabolic surgery in the treatment algorithm for type 2 diabetes: a joint statement by international diabetes organizations. Diabetes Care. 2016;39(6):861–877. doi:10.2337/dc16-0236
18. Shrank WH, Barlow JF, Brennan TA. New therapies in the treatment of high cholesterol: an argument to return to goal-based lipid guidelines. JAMA J Am Med Assoc. 2015;314(14):1443–1444. doi:10.1001/jama.2015.10017
19. Lin L, Zhao J, Hu J, et al. Current smoking has a detrimental effect on survival for Epidermal Growth Factor Receptor (EGFR) and Anaplastic Lymphoma Kinase (ALK) negative Advanced non-squamous Non-small Cell Lung Cancer (NSCLC) patients treated with pemetrexed continuation maintenance. J Cancer. 2018;9(12):2140–2146. doi:10.7150/jca.24872
20. Stevens PE, Levin A; Kidney disease: improving global outcomes chronic kidney disease guideline development work group, M. Evaluation and management of chronic kidney disease: synopsis of the kidney disease: improving global outcomes 2012 clinical practice guideline. Ann Intern Med. 2013;158(11):825–830. doi:10.7326/0003-4819-158-11-201306040-00007
21. Caselli C, Del Turco S, Ragusa R, et al. Association of PCSK9 plasma levels with metabolic patterns and coronary atherosclerosis in patients with stable angina. Cardiovasc Diabetol. 2019;18(1):144. doi:10.1186/s12933-019-0949-3
22. Yang SH, Xu RX, Cui CJ, et al. Liraglutide downregulates hepatic LDL receptor and PCSK9 expression in HepG2 cells and db/db mice through a HNF-1a dependent mechanism. Cardiovasc Diabetol. 2018;17(1):48. doi:10.1186/s12933-018-0689-9
23. Peng J, Liu MM, Jin JL, et al. Association of circulating PCSK9 concentration with cardiovascular metabolic markers and outcomes in stable coronary artery disease patients with or without diabetes: a prospective, observational cohort study. Cardiovasc Diabetol. 2020;19(1):167. doi:10.1186/s12933-020-01142-0
24. Wang Y, Ye J, Li J, et al. Polydatin ameliorates lipid and glucose metabolism in type 2 diabetes mellitus by downregulating proprotein convertase subtilisin/kexin type 9 (PCSK9). Cardiovasc Diabetol. 2016;15:19. doi:10.1186/s12933-015-0325-x
25. Levenson AE, Wadwa RP, Shah AS, et al. PCSK9 is increased in youth with type 1 diabetes. Diabetes Care. 2017;40(7):e85–7. doi:10.2337/dc16-2563
26. Levenson AE, Shah AS, Khoury PR, Kimball TR, Urbina EM, de Ferranti SD. Obesity and type 2 diabetes are associated with elevated PCSK9 levels in young women. Pediatr Diabetes. 2017;18(8):755–760. doi:10.1111/pedi.12490
27. Bojanin D, Vekic J, Milenkovic T, et al. Association between proprotein convertase subtilisin/kexin 9 (PCSK9) and lipoprotein subclasses in children with type 1 diabetes mellitus: effects of glycemic control. Atherosclerosis. 2019;280:14–20. doi:10.1016/j.atherosclerosis.2018.11.020
28. Ramin-Mangata S, Wargny M, Pichelin M, et al. Circulating PCSK9 levels are not associated with the conversion to type 2 diabetes. Atherosclerosis. 2019;293:49–56. doi:10.1016/j.atherosclerosis.2019.11.027
29. Reyes-Sofer G, Pavlyha M, Ngai C, et al. Effects of PCSK9 inhibition with alirocumab on lipoprotein metabolism in healthy humans. Circulation. 2017;135(4):352–362. doi:10.1161/CIRCULATIONAHA.116.025253
30. Shi J, Zhang W, Niu Y, et al. Association of circulating proprotein convertase subtilisin/kexin type 9 levels and the risk of incident type 2 diabetes in subjects with prediabetes: a population-based cohort study. Cardiovasc Diabetol. 2020;19(1):209. doi:10.1186/s12933-020-01185-3
31. Schmidt AF, Swerdlow DI, Holmes MV, et al. PCSK9 genetic variants and risk of type 2 diabetes: a Mendelian randomisation study. Lancet Diabetes Endocrinol. 2017;5:97–105. doi:10.1016/S2213-8587(16)30396-5
32. Lotta LA, Sharp SJ, Burgess S, et al. Association between low-density lipoprotein cholesterol-lowering genetic variants and risk of type 2 diabetes: a meta-analysis. JAMA. 2016;316:1383–1391. doi:10.1001/jama.2016.14568
33. Hao M, Head WS, Gunawardana SC, Hasty AH, Piston DW. Direct effect of cholesterol on insulin secretion: a novel mechanism for pancreatic beta-cell dysfunction. Diabetes. 2007;56:2328–2338. doi:10.2337/db07-0056
34. Paul R, Choudhury A, Choudhury S, Mazumder MK, Borah A. Cholesterol in pancreatic beta-cell death and dysfunction: underlying mechanisms and pathological implications. Pancreas. 2016;45:317–324. doi:10.1097/MPA.0000000000000486
35. Brunham LR, Kruit JK, Pape TD, et al. Beta-cell ABCA1 influences insulin secretion, glucose homeostasis and response to thiazolidinedione treatment. Nat Med. 2007;13:340–347. doi:10.1038/nm1546
36. Brunham LR, Kruit JK, Verchere CB, Hayden MR. Cholesterol in islet dysfunction and type 2 diabetes. J Clin Invest. 2008;118:403–408. doi:10.1172/JCI33296
37. Cochran BJ, Hou L, Manavalan AP, et al. Impact of perturbed pancreatic beta-cell cholesterol homeostasis on adipose tissue and skeletal muscle metabolism. Diabetes. 2016;65:3610–3620. doi:10.2337/db16-0668
38. Hopkins PN, Krempf M, Bruckert E, et al. Pharmacokinetic and pharmacodynamic assessment of alirocumab in patients with familial hypercholesterolemia associated with proprotein convertase subtilisin/kexin type 9 gain-of-function or apolipoprotein B loss-of-function mutations. J Clin Lipidol. 2019;13(6):970–978. doi:10.1016/j.jacl.2019.10.007
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prognostic Value of Pentraxin-3 Change After Primary Percutaneous Coronary Intervention in Patients with ST-Segment Elevation Myocardial Infarction
Li SY, Liu L, Wang DK, Ding XS, Li WP, Li HW
Journal of Inflammation Research 2023, 16:1255-1266
Published Date: 22 March 2023
Mortality Outcomes in People with Lung Cancer with and without Type2 Diabetes: A Cohort Study in England
Igbinosa EG, Dharmasekara B, Quint JK, Popat S, Bhaskaran K, Morganstein D, Cook S
Clinical Epidemiology 2025, 17:681-692
Published Date: 17 July 2025
The Association Between Estimated Glomerular Filtration Rate and All-Cause Mortality in Patients with Dysglycemia in Northeastern Thailand

Sribenjalak D, Charoensri S, Kritmetapak K, Pongchaiyakul C
Diabetes, Metabolic Syndrome and Obesity 2025, 18:4733-4739
Published Date: 22 December 2025