Back to Journals » Journal of Hepatocellular Carcinoma » Volume 10
Effect of Different Liver Resection Modalities on the Prognosis of Patients with Hepatocellular Carcinoma on the Left Lateral Lobe
Authors Liu J ![]() , Sun M, Fang K, Wang J, Ma B, Song L, Liu T, Tang M, Wang K, Xia Y
, Sun M, Fang K, Wang J, Ma B, Song L, Liu T, Tang M, Wang K, Xia Y
Received 14 March 2023
Accepted for publication 20 June 2023
Published 28 June 2023 Volume 2023:10 Pages 997—1007
DOI https://doi.org/10.2147/JHC.S412554
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Mohamed Shaker
Jianwei Liu,1,* Minmin Sun,2,* Kunpeng Fang,3,* Jie Wang,1 Bowen Ma,1 Li Song,1 Ting Liu,1 Ming Tang,4 Kui Wang,1 Yong Xia4
1Department of Hepatic Surgery II, Third Affiliated Hospital of Naval Medical University (Eastern Hepatobiliary Surgery Hospital), Shanghai, 200438, People’s Republic of China; 2Department of Hepatic Surgery I, Third Affiliated Hospital of Naval Medical University (Eastern Hepatobiliary Surgery Hospital), Shanghai, 200438, People’s Republic of China; 3Department of Special Treatment I, Third Affiliated Hospital of Naval Medical University (Eastern Hepatobiliary Surgery Hospital), Shanghai, 200438, People’s Republic of China; 4Department of Hepatic Surgery IV, Third Affiliated Hospital of Naval Medical University (Eastern Hepatobiliary Surgery Hospital), Shanghai, 200438, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yong Xia, Department of Hepatic Surgery (IV), Third Affiliated Hospital of Naval Medical University (Eastern Hepatobiliary Surgery Hospital), #225 Changhai Road, Shanghai, 200438, People’s Republic of China, Tel +86-2181875005, Fax +86-2165562400, Email [email protected] Kui Wang, Department of Hepatic Surgery (II), Third Affiliated Hospital of Naval Medical University (Eastern Hepatobiliary Surgery Hospital), #225 Changhai Road, Shanghai, 200438, People’s Republic of China, Email [email protected]
Purpose: To investigate the effect of different liver resection modalities on the prognosis of left lateral lobe hepatocellular carcinoma (HCC) patients.
Methods: 315 patients with HCC on left lateral lobe were divided into open left lateral lobectomy (LLL) group (n=249) and open left hepatectomy (LH) group (n=66). The differences in long-term prognosis between two groups were compared.
Results: The results showed that narrow resection margin (Hazard Ratio (HR):1.457, 95% Confidential Interval (CI): 1.038– 2.047; HR:1.415, 95% CI: 1.061– 1.887), tumor diameter > 5 cm (1.645, 1.161– 2.330; 1.488, 1.123– 1.971), multiple tumors (2.021, 1.330– 3.073; 1.987, 1.380– 2.861), and microvascular invasion (MVI) (1.753, 1.253– 2.452; 1.438, 1.087– 1.902) are independent risk factors for overall survival (OS) and tumor recurrence (TR), while liver resection modality is not. After propensity score matching, liver resection modality is not an independent risk factor for OS and TR. Further analysis revealed that wide resection margins were achieved in all patients in the LH group but only 59.0% patients in the LLL group. The OS and TR rates were not significantly different between wide patients with resection margins in LLL group and LH group (P=0.766 and 0.919, respectively), but significantly different between patients with narrow resection margins in LLL group and LH group (P=0.012 and 0.017, respectively).
Conclusion: Liver resection modality is not an independent risk factor for the prognosis of patients with HCC on the left lateral lobe as long as wide margins are obtained. Nevertheless, with narrow margins, patients who underwent LH rather than LLL did better.
Keywords: hepatocellular carcinoma, left lateral hepatic lobe, left lateral lobectomy, left hepatectomy, prognosis
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Chen has been published for this article.
Introduction
Hepatocellular carcinoma (HCC) is a common malignant tumor with morbidity and mortality ranking top among all malignant tumors in China.1 More than 50% world’s new liver cancer cases are identified in China each year.2 Currently, resection is the most effective treatment for HCC,3,4 but the postoperative prognosis of HCC patients is still very poor.5,6 The surgical modality can be divided into anatomical liver resection and non-anatomical liver resection or local resection and extended resection. Previous studies have suggested that anatomical hepatectomy can lead to better long-term prognosis than non-anatomical hepatectomy.7,8 However, regardless of the resection modality, radical resection is the principle for all HCC patients. For patients with HCC on the left lateral lobe, left lateral lobectomy (LLL) and left hepatectomy (LH) are common surgical approaches.9,10 Both can be performed laparoscopically or openly. Studies have reported that laparoscopic LH may achieve better overall survival (OS) than open LLL.11 However, the effects of open LLL or LH on postoperative complications, OS, and tumor recurrence (TR) of patients with HCC on the left lateral lobe are still unclear. Therefore, this study systematically analyzed the effects of different liver resection modalities on postoperative complications, OS, and TR of patients with HCC on the left lateral lobe.
Patients and Methods
Patients
A total of 315 patients who had HCC on the left lateral lobe and underwent open LLL or open LH in our hospital from June 2011 to August 2013 were enrolled in the study. These patients were followed up until January 2018. All patients underwent routine preoperative laboratory tests to evaluate their surgical tolerance and tumor resectability. The inclusion criteria were: (1) all patients underwent open LLL or open LH; (2) preoperative liver function assessment indicated Child-Pugh grade A and Child-Pugh score ≤B7; (3) tumor located only in the left lateral lobe (hepatic segment II or III) but not in other liver segments; (4) single or multiple tumors did not invade the sagittal part of the portal vein; (5) tumor was not involved in large blood vessels, diaphragm and other surrounding organs and did not metastasize; (6) tumor was completely resected, and the surgical resection margin was R0; (7) HCC was pathologically confirmed after the operation; (8) the Clinicopathological and follow-up data are complete. The exclusion criteria were: (1) patients underwent laparoscopic LLL or laparoscopic LH; (2) tumor located on sites other than the left lateral lobe; (3) tumor was accompanied by diaphragmatic invasion or other metastases; (4) patients had received other antitumor therapy before surgery; (5) R0 resection was not achieved in the resection margin;12 (6) preoperative liver function assessment indicated Child-Pugh score > B7; and (7) patients had clinically significant portal hypertension.13 In this study, resection margins were divided into wide margins and narrow margins. The wide margins were defined as the distance of the resection margin to the tumor ≥1 cm, and the narrow margins were defined as the distance of the resection margin to the tumor < 1 cm.14
In accordance with the Declaration of Helsinki, this study was approved by the Institutional Ethics Committee of our hospital. All patients provided written informed consent before participating and allowed the use of their clinicopathological data during diagnosis and treatment for medical research.
Tumor Resection
Open Left Lateral Lobectomy
LLL was performed via bilateral subcostal arc incision or reverse L-shaped incision. First, the situation of the liver and the abdominal cavity was explored. Then the left lateral lobe of the liver was fully exposed. Along the left side of the sagittal portion of the portal vein, ultrasonic scalpels or vascular forceps were used to gradually cut off the liver tissues. After the left lateral hepatic lobe was completely sectioned, thorough hemostasis was performed at the liver resection surface.10 The hepatic portal was occluded during resection by the Pringle maneuver,15 which involved multiple cycles of 15-min clamping and 5-min release of the portal triad.
Open Left Hepatectomy
The left lateral hepatic lobe was fully exposed and the liver tissue was slowly separated along the left of the middle hepatic vein with ultrasonic scalpel and vascular clamp during the hepatic portal occlusion. After left hepatic lobe was completely sectioned, thorough hemostasis was performed at the liver resection surface.9 During liver resection, the hepatic portal was occluded using the Pringle maneuver. In this study, the caudate lobe was preserved during LH.
Postoperative Follow-Up and Endpoints
All patients received routine post-operative re-examinations, including blood routine, liver and kidney function examinations, and tumor indicators, including serum alpha-fetoprotein (AFP), carcinoembryonic antigen (CEA), and cancer antigens (CA) 19–9. Additionally, abdominal B-ultrasound, abdominal contrast-enhanced magnetic resonance imaging (MRI), and computerized tomography (CT) were conducted. Patients were re-examined every two months within two years after surgery and every three months after two years of surgery. If recurrence was confirmed, the time when AFP was abnormally elevated or a new tumor appeared on imaging was defined as the time of recurrence. Patients with a high risk of tumor recurrence based on tumor size, tumor number, and microvascular invasion (MVI) after surgery were recommended to undergo prophylactic transcatheter arterial chemoembolization (TACE) one month after surgery.16,17 Postoperative complications were assessed according to the Clavien-Dindo criteria.18
The primary endpoints were OS and TR. OS was defined as the period from the day of hepatic resection until the patients died or loss to follow-up. TR was defined as the period from the day of hepatic resection until tumor recurrence or metastasis.
Statistical Analysis
Measurement data were described as median (range) and compared using the independent t-test or Mann–Whitney U-test. Count data were presented as numbers (percentages) and compared using the chi-square test or Fisher’s exact test. Survival and recurrence curves were plotted using the Kaplan-Meier method. Independent risk factors for postoperative OS and TR rates were analyzed using Cox regression analysis. OS was defined as the time from surgery to death or last follow-up, and tumor recurrence was defined as the time from surgery to the first postoperative diagnosis of recurrence or metastasis. The relative risk was presented as a hazard ratio (HR) and 95% confidence interval (CI). A P value less than 0.05 was considered statistically significant. All data were analyzed using SPSS version 19 (SPSS Inc, Chicago, IL, USA) and R software version 4.0.0 (http://www.R-project.org). In this article a one-to-two propensity score matching (PSM) was used to balance the differences in baseline clinicopathological features between the LLL and LH groups. Covariates included in the PSM analysis were PLT (> /≤ 100*109/L), CA 19-9 (> /≤ 39 U/mL), Hilar clamping (> /≤ 20 minutes), Tumor diameter (> /≤ 5cm) to calculate the propensity score by logistic regression.
Results
Clinicopathological Features
Figure 1 shows the patient selection flow chart for this study. A total of 315 patients diagnosed with HCC on the left lateral lobe were enrolled in the study and divided into the LLL group (n=249) and LH group (n=66) based on the resection modality.
 |
Figure 1 Flow chart for selecting patients in the LLL group and in the LH group. |
Supplement Table 1 lists the baseline characteristics of the 315 patients with HCC on the left lateral lobe. No significant differences were observed between the two groups in clinicopathological features. However, compared to the LH group, patients in the LLL group had lower platelet count (140.0 vs 157.0109/L, P=0.039), lower CA199 (17.3 vs 20.3 U/mL, P=0.040), a lower proportion of hilar clamping > 20 minutes (16.1% vs 30.3%, P=0.009), a higher proportion of narrow margins (41.0% vs 0, P<0.001), and smaller tumor diameter (4.1cm vs 4.7cm, P=0.017). After PSM, no significant differences were observed between the two groups in clinicopathological features (Table 1).
 |
Table 1 Baseline Characteristics of Patients After PSM |
OS and TR in the Whole Cohort and PSM Group
The median follow-up time for the 315 HCC patients was 58.9 months. The 1, 3, and 5-year OS rates were 91.1%, 70.1%, 53.3% and the TR rates were 15.6%, 48.6%, 68.0%, respectively. Supplement Table 2 lists the results of univariate analyses for postoperative OS and TR. Supplement Table 3 lists the results of multivariate analyses for postoperative OS and TR. The results of multivariate analyses showed that the liver resection modality was not an independent risk factor for patients’ postoperative OS and TR. The postoperative 1, 3, and 5-year OS rates were 90.7%, 68.2%, and 51.5% for patients in the LLL group and 92.4%, 77.3%, and 60.3% for patients in the LH group (P=0.176) (Figure 2A). The postoperative 1, 3, and 5-year TR rates were 16.5%, 49.8%, and 69.5% for patients in the LLL group and 12.1%, 49.9%, and 62.3% for patients in the LH group (P=0.257) (Figure 2B).
 |
Figure 2 Overall survival and tumor recurrence curves of patients with HCC on the left lateral lobe in the LH group and LLL group before and after propensity score matching. (A) Overall survival curve before propensity score matching; (B) Tumor recurrence curve before propensity score matching; (C) Overall survival curve after propensity score matching; (D) Tumor recurrence curve after propensity score matching. |
Table 2 and 3 show the results of univariate and multivariate analyses of postoperative OS and TR rates after PSM, respectively. The results of multivariate analyses showed that narrow margin (HR:1.838, 95% CI:1.038–3.257; HR:1.875, 95% CI:1.153–3.048), tumor diameter >5 cm (HR:1.829, 95% CI:1.100–3.041; HR:1.516, 95% CI:1.014–2.268), multiple tumors (HR:2.389, 95% CI:1.369–4.170; HR:2.440, 95% CI:1.516–3.928) and MVI (HR:1.575, 95% CI:1.004–2.471; HR:1.452, 95% CI:1.006–2.095) were independent risk factors for OS and TR, while liver resection modality was not an independent risk factor for OS and TR. The postoperative 1, 3, and 5-year OS rates after PSM were 88.5%, 67.2%, and 51.1% for patients in the LLL group and 93.4%, 80.3%, and 63.7% for patients in the LH group (P=0.079) (Figure 2C). The postoperative 1, 3, and 5-year TR rates were 18.0%, 50.0%, and 70.3% for patients in the LLL and 11.5%, 41.0%, and 60.9%, for patients in the LH group (P=0.163) (Figure 2D).
 |
Table 2 Univariate Analysis of OS and TR for HCC of Left Lateral Lobe After PSM |
 |
Table 3 Multivariate Analysis of OS and TR for HCC of Left Lateral Lobe After PSM |
The Differences in OS and TR Rates Between LLL Group and LH Group
The 1-, 3-, and 5-year OS rates were 87.3%, 58.8%, and 41.1%, respectively, for patients with narrow margins in the LLL group and 92.4%, 77.3%, and 60.3%, respectively, for patients in the LH group (P=0.012) (Figure 3A). The 1, 3, and 5-year TR rates were 22.5%, 59.8%, and 76.5%, respectively, for patients with narrow margins in the LLL group and 12.1%, 43.9%, and 62.3% for patients in the LH group (P=0.017) (Figure 3B). The 1-, 3-, and 5-year OS rates were 93.2%, 74.8%, and 58.7%, respectively, for patients with wide margins in the LLL group and 92.4%, 77.3%, and 60.3%, respectively, for patients in the LH group (P=0.766) (Figure 3C). The 1-, 3-, and 5-year TR rates were 12.2%, 42.9%, and 64.6%, respectively, for patients with wide margins in the LLL group and 12.1%, 43.9%, and 62.3%, respectively, for patients in the LH group (P=0.919) (Figure 3D).
 |
Figure 3 Overall survival and tumor recurrence of patients with HCC on the left lateral lobe who had wide resection margins and narrow resection margins in the LLL group and in the LH group. (A) Postoperative overall survival curve of patients with wide resection margin in the LLL and LH groups; (B) Postoperative tumor recurrence curve of patients with wide resection margin in the LLL and LH groups; (C) Postoperative overall survival curve of patients with narrow resection margin in the LLL and LH groups; (D) Postoperative tumor recurrence curve of patients with narrow resection margin in the LLL and LH groups. |
The Differences in Postoperative Complications and Liver Function Between LLL Group and LH Group
Of the 315 HCC patients, 55 patients had postoperative complications, 44 patients had one postoperative complication, and 8 patients had two different postoperative complications. The postoperative complication rate was 55/315 (17.5%).
The postoperative complication rate was 42/249 (16.8%) for patients in the LLL group and 13/66 (19.7%) for patients in the LH group (P=0.590). The rate of grade III/IV postoperative complications was 4/249 (1.6%) and 2/66 (3.0%) for patients in the LLL group and in the LH group, respectively (P=0.806) (Table 4).
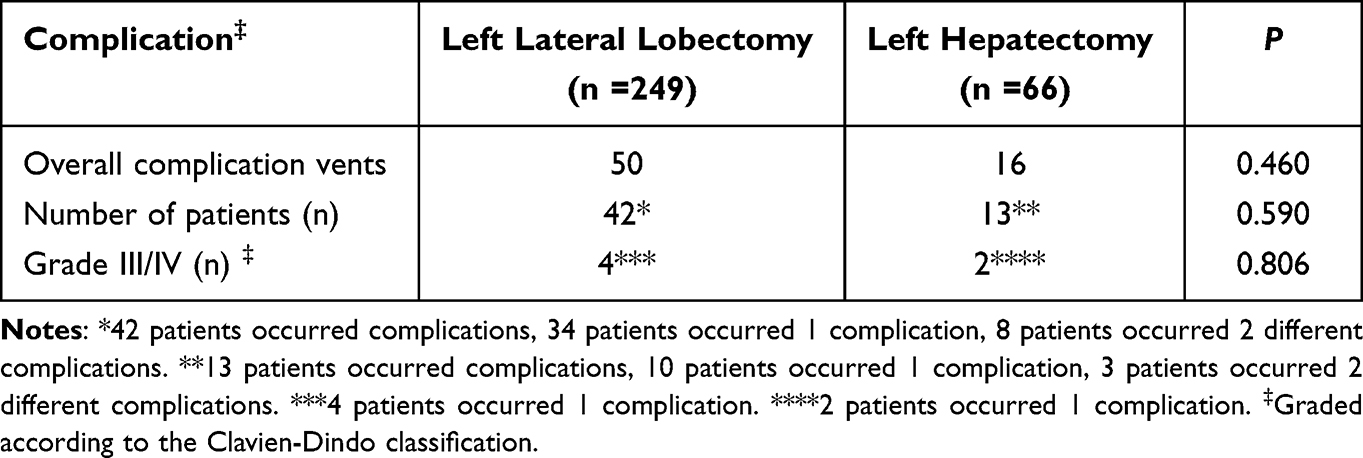 |
Table 4 Complication of Patients Underwent Hepatectomy |
In terms of postoperative liver function, the TBIL levels and ALT levels on the first postoperative day were 34.9 μmol/L and 35.1 μmol/L, 289.2 IU/L and 319.6 IU/L, respectively, for patients in the LLL group and LH group, which showed no significant differences (P=0.965 and P=0.665, respectively). The TBIL and ALT levels on postoperative day 3 were 27.7 μmol/L and 126.9 IU/L, respectively, for patients in the LLL group and 31.3 μmol/L and 105.9 IU/L, respectively, for patients in the LH group, showing no significant differences (P=0.155 and P=0.087, respectively). The TBIL and ALT levels on postoperative day 5 were 15.2 μmol/L and 60.1 IU/L, respectively, for patients in the LLL group and 14.9 μmol/L and 59.1 IU/L, respectively, for patients in the LH group, showing no significant differences (P=0.155 and P=0.818, respectively). (Supplement Table 1).
Discussion
The common surgical modality for patients with HCC on the left lateral hepatic lobe is LLL and LH.9,10 The LLL involves cutting off liver tissues sequentially along the left side of the sagittal portion of the portal vein, while the LH involves cutting off the liver tissues gradually along the line 0.5 cm away from the left side of the middle hepatic vein to the first hepatic hilum. Due to the anatomical limits of the LLL, wide resection margins cannot be obtained for some patients whose tumors are adjacent to the sagittal portion of the portal vein. Comparing with LLL, LH involves more liver tissues and could lead to greater damage to the liver. However, wide resection margins can be obtained for some HCC patients, resulting in more thorough treatment.
Our results firstly compared the difference of open LLL and open LH. The results showed that the resection margin can affect patients’ postoperative OS and TR. Wide resection margins can improve patients’ prognosis, consistent with the results of previous studies.14,19–21 The liver resection modality is not an independent risk factor for prognosis. In other words, LH is not a protective factor for prognosis compared with LLL. The reason may be the high proportion (59.0%) of wide margins in the LLL group in this study. A high proportion of wide margins results in a better long-term prognosis of patients in the LLL group. Therefore, no significant difference in prognosis was found between the LH group and the LLL group. We further divided these patients in the LLL group into the wide resection margin group and the narrow resection margin group and compared them with patients with LH. The results showed that the prognosis of patients with wide resection margin in the LLL group is similar to that of patients in the LH group. In other words, the liver resection modality has no significant effect on the prognosis of these patients. However, patients with narrow resection margins in the LLL group have a significantly worse prognosis than patients in the LH group. The underlying reason may be that only narrow margin can be obtained for left lateral lobe HCC patients with the tumors adjacent to the sagittal portion of the portal vein during LLL due to the anatomical limits. To obtain wide margins, these patients must undergo LH. Therefore, LH can improve their prognosis. That is, the liver resection modality has an impact on the prognosis of these patients. This may be related to paracancerous foci and MVI, which are collectively referred to as peritumoral micrometastasis and are important factors for postoperative recurrence of HCC, especially early recurrence.22,23 Studies have shown that pericancerous micrometastasis is also associated with tumor metastasis, recurrence, and poor prognosis.24,25 Our results also showed that MVI is an independent risk factor for postoperative OS and TR, consistent with previous studies.22,23 A study showed that micrometastasis could also occur in in the liver tissues adjacent to the tumor HCC patient with small tumors, while the probability of micrometastasis was significantly higher in HCC patients with larger tumors.26 Our results showed that patients in the LH group had a significantly larger tumor diameter than patients in the LLL group (4.7 vs 4.1 cm, P=0.016). In addition, more patients in the LH group were MVI positive, which may be related to the larger tumor diameter, consistent with the findings of a previous study.26 Moreover, studies have found that patients with multiple tumors have a poor prognosis,27–29 which may be related to tumor origin and MVI rate.
MVI rate is significantly higher in patients with multiple tumors than in patients with a single tumor.30 A wide resection margin can increase the probability of resecting potential peritumoral micro-metastasis, thereby reducing the possibility of postoperative recurrence of intrahepatic metastasis31 and improving patients’ prognosis. In addition, liver function assessment is an important factor affecting the choice of surgical modality.32 For patients with severe liver cirrhosis, if preoperative evaluation suggests severe liver function damage after surgery, even if the tumor is adjacent to the sagittal portal vein, more clinicians will consider performing LLL. In addition, the risk of postoperative complications also affects surgical modality selections. Our results showed that LH does not increase the incidence of postoperative complications compared with LLL. That is, although LH involves more liver tissue, it does not significantly increase the probability of postoperative complications compared with LLL, which is consistent with previous studies.11 In terms of postoperative liver function, our results showed that no significant difference in the levels of TBIL and ALT on the postoperative day 1, 3, and 5 between the LLL group and the LH group, indicating no significant difference in postoperative liver function between the two groups. This may be benefited from stricter preoperative screening in patients in the LH group.
Our study has some limitations. First, the size of patients included in this study is relatively small. Second, the study is a single-center retrospective study. Although it is a real-world study, the results need to be further validated in multi-center prospective studies with larger sample sizes.
Conclusion
The modality of liver resection is not an independent prognostic risk factor for patients with HCC on the left lateral lobe. As long as the wide surgical margins are ensured, the choice of surgical modality has no significant effect on their long-term prognosis. However, for left lateral lobe HCC patients with tumors adjacent to the sagittal portion of the portal vein, it is crucial to ensure adequate margins, and LH is recommended to achieve a better prognosis.
Data Sharing Statement
The data supporting the findings of this study are available upon request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Ethics Statements
This study was approved by the Ethics Committee of Eastern Hepatobiliary Surgery Hospital. All patients provided written informed consent before participating and allowed the use of their clinicopathological data during diagnosis and treatment for medical research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded in full by the Program of Science and Technology Commission of Shanghai Municipality (grant number 21Y11912700 to Yong Xia).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
2. Feng RM, Zong YN, Cao SM, Xu RH. Current cancer situation in China: good or bad news from the 2018 Global Cancer Statistics? Cancer Commun. 2019;39(1):22. doi:10.1186/s40880-019-0368-6
3. Zaydfudim VM, Vachharajani N, Klintmalm GB, et al. Liver resection and transplantation for patients with hepatocellular carcinoma beyond Milan criteria. Ann Surg. 2016;264(4):650–658. doi:10.1097/SLA.0000000000001866
4. Forner A, Reig M, Bruix J. Hepatocellular carcinoma. Lancet. 2018;391(10127):1301–1314. doi:10.1016/S0140-6736(18)30010-2
5. European Association for the Study of The Liver; European Organisation for Research and Treatment of Cancer. EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2012;56(4):908–943. doi:10.1016/j.jhep.2011.12.001
6. Grazi GL, Ercolani G, Pierangeli F, et al. Improved results of liver resection for hepatocellular carcinoma on cirrhosis give the procedure added value. Ann Surg. 2001;234(1):71–78. doi:10.1097/00000658-200107000-00011
7. Xu H, Liu F, Hao X, et al. Laparoscopically anatomical versus non-anatomical liver resection for large hepatocellular carcinoma. HPB. 2020;22(1):136–143. doi:10.1016/j.hpb.2019.06.008
8. Liu Y, Dai Y, Zhang XX, Li SM, Liu RJ, Fan H. Comparative analysis of anatomic and non-anatomic hepatectomy for single small hepatocellular carcinoma with microvascular invasion. Zhonghua Yi Xue Za Zhi. 2018;98(24):1937–1940. Chinese. doi:10.3760/cma.j.issn.0376-2491.2018.24.009
9. Kobayashi A, Miyagawa S. Left hepatectomy. J Hepatobiliary Pancreat Sci. 2012;19(1):38–43. doi:10.1007/s00534-011-0452-z
10. Belli G, Fantini C, D’Agostino A, Belli A, Cioffi L, Russolillo N. Laparoscopic left lateral hepatic lobectomy: a safer and faster technique. J Hepatobiliary Pancreat Surg. 2006;13(2):149–154. doi:10.1007/s00534-005-1023-y
11. Zou J, Li S, Wang Q, et al. Surgical strategies for hepatocellular carcinoma located in the left lateral lobe: a propensity score-matched and prognostic nomogram study. Cancer Med. 2021;10(10):3274–3287. doi:10.1002/cam4.3894
12. Yang T, Lu JH, Lau WY, et al. Perioperative blood transfusion does not influence recurrence-free and overall survivals after curative resection for hepatocellular carcinoma: a propensity score matching analysis. J Hepatol. 2016;64(3):583–593. doi:10.1016/j.jhep.2015.10.012
13. de Franchis R; Baveno V Faculty. Revising consensus in portal hypertension: report of the Baveno V consensus workshop on methodology of diagnosis and therapy in portal hypertension. J Hepatol. 2010;53(4):762–768. doi:10.1016/j.jhep.2010.06.004
14. Aoki T, Kubota K, Hasegawa K, et al. Significance of the surgical hepatic resection margin in patients with a single hepatocellular carcinoma. Br J Surg. 2020;107(1):113–120. doi:10.1002/bjs.11329
15. Pringle JH. Notes on the arrest of hepatic hemorrhage due to trauma. Ann Surg. 1908;48(4):541–549. doi:10.1097/00000658-190810000-00005
16. Chen MY, Juengpanich S, Hu JH, et al. Prognostic factors and predictors of postoperative adjuvant transcatheter arterial chemoembolization benefit in patients with resected hepatocellular carcinoma. World J Gastroenterol. 2020;26(10):1042–1055. doi:10.3748/wjg.v26.i10.1042
17. Wang H, Yu H, Qian YW, Cao ZY, Wu MC, Cong WM. Postoperative adjuvant transcatheter arterial chemoembolization improves the prognosis of patients with huge hepatocellular carcinoma. Hepatobiliary Pancreat Dis Int. 2021;20(3):232–239. doi:10.1016/j.hbpd.2020.12.018
18. Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205–213. doi:10.1097/01.sla.0000133083.54934.ae
19. Shi M, Guo RP, Lin XJ, et al. Partial hepatectomy with wide versus narrow resection margin for solitary hepatocellular carcinoma: a prospective randomized trial. Ann Surg. 2007;245(1):36–43. doi:10.1097/01.sla.0000231758.07868.71
20. Yang P, Si A, Yang J, et al. A wide-margin liver resection improves long-term outcomes for patients with HBV-related hepatocellular carcinoma with microvascular invasion. Surgery. 2019;165(4):721–730. doi:10.1016/j.surg.2018.09.016
21. Laurent C, Blanc JF, Nobili S, et al. Prognostic factors and longterm survival after hepatic resection for hepatocellular carcinoma originating from noncirrhotic liver. J Am Coll Surg. 2005;201(5):656–662. doi:10.1016/j.jamcollsurg.2005.05.027
22. Erstad DJ, Tanabe KK. Prognostic and therapeutic implications of microvascular invasion in hepatocellular carcinoma. Ann Surg Oncol. 2019;26(5):1474–1493. doi:10.1245/s10434-019-07227-9
23. Subbotin VM. Privileged portal metastasis of hepatocellular carcinoma in light of the coevolution of a visceral portal system and liver in the chordate lineage: a search for therapeutic targets. Drug Discov Today. 2018;23(3):548–564. doi:10.1016/j.drudis.2018.01.020
24. Mansi J, Morden J, Bliss JM, Neville M, Coombes RC. Bone marrow micrometastases in early breast cancer-30-year outcome. Br J Cancer. 2016;114(3):243–247. doi:10.1038/bjc.2015.447
25. Sasaki E, Nagino M, Ebata T, et al. Immunohistochemically demonstrated lymph node micrometastasis and prognosis in patients with gallbladder carcinoma. Ann Surg. 2006;244(1):99–105. doi:10.1097/01.sla.0000217675.22495.6f
26. Cheng Z, Yang P, Qu S, et al. Risk factors and management for early and late intrahepatic recurrence of solitary hepatocellular carcinoma after curative resection. HPB. 2015;17(5):422–427. doi:10.1111/hpb.12367
27. Bruix J, Han KH, Gores G, Llovet JM, Mazzaferro V. Liver cancer: approaching a personalized care. J Hepatol. 2015;62(1 Suppl):S144–S156. doi:10.1016/j.jhep.2015.02.007
28. Wang YY, Zhong JH, Xu HF, et al. A modified staging of early and intermediate hepatocellular carcinoma based on single tumour >7 cm and multiple tumours beyond up-to-seven criteria. Aliment Pharmacol Ther. 2019;49(2):202–210. doi:10.1111/apt.15074
29. Wada H, Eguchi H, Noda T, et al. Selection criteria for hepatic resection in intermediate-stage (BCLC stage B) multiple hepatocellular carcinomas. Surgery. 2016;160(5):1227–1235. doi:10.1016/j.surg.2016.05.023
30. Lei Z, Li J, Wu D, et al. Nomogram for preoperative estimation of microvascular invasion risk in hepatitis b virus-related hepatocellular carcinoma within the Milan criteria. JAMA Surg. 2016;151(4):356–363. doi:10.1001/jamasurg.2015.4257
31. Shi C, Zhao Q, Liao B, et al. Anatomic resection and wide resection margin play an important role in hepatectomy for hepatocellular carcinoma with peritumoural micrometastasis. ANZ J Surg. 2019;89(11):E482–E486. doi:10.1111/ans.15396
32. Kokudo T, Hasegawa K, Shirata C, et al. Assessment of preoperative liver function for surgical decision making in patients with hepatocellular carcinoma. Liver Cancer. 2019;8(6):447–456. doi:10.1159/000501368
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Decaprenyl Diphosphate Synthase Subunit 1 (PDSS1): A Potential Prognostic Biomarker and Immunotherapy-Target for Hepatocellular Carcinoma
Yang Y, Li J, Tang M, Nie B, Huang W
Cancer Management and Research 2022, 14:1627-1639
Published Date: 3 May 2022
Identification of KRBA1 as a Potential Prognostic Biomarker Associated with Immune Infiltration and m6A Modification in Hepatocellular Carcinoma
Liu Y, Fu B, Yu Z, Song G, Zeng H, Gong Y, Ding Y, Huang D
Journal of Hepatocellular Carcinoma 2022, 9:497-516
Published Date: 31 May 2022
Low MARCO Expression is Associated with Poor Survival in Patients with Hepatocellular Carcinoma Following Liver Transplantation
Zhang Q, Wei Y, Li Y, Jiao X
Cancer Management and Research 2022, 14:1935-1944
Published Date: 11 June 2022
Histological Severity of Cirrhosis Influences Surgical Outcomes of Hepatocellular Carcinoma After Curative Hepatectomy
Liang BY, Gu J, Xiong M, Zhang EL, Zhang ZY, Lau WY, Wang SF, Guan Y, Chen XP, Huang ZY
Journal of Hepatocellular Carcinoma 2022, 9:633-647
Published Date: 23 July 2022
Nomogram for the Preoperative Prediction of the Macrotrabecular-Massive Subtype of Hepatocellular Carcinoma
Shan Y, Yu X, Yang Y, Sun J, Wu S, Mao S, Lu C
Journal of Hepatocellular Carcinoma 2022, 9:717-728
Published Date: 10 August 2022