Back to Journals » Open Access Emergency Medicine » Volume 17
Effect of an Educational Intervention on Nurses’ Knowledge Regarding Use of Modified Early Warning Score in Recognition of Critical Illness
Authors Olowo S, Luwaga R, Niyonzima V ![]()
Received 3 March 2025
Accepted for publication 15 August 2025
Published 21 August 2025 Volume 2025:17 Pages 215—232
DOI https://doi.org/10.2147/OAEM.S521517
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Amit Agrawal
Samuel Olowo,1,2 Rachel Luwaga,1 Vallence Niyonzima1
1Department of Nursing, Mbarara University of Science and Technology, Mbarara, Uganda; 2Department of Nursing, Busitema University, Mbale, Uganda
Correspondence: Vallence Niyonzima, Department of Nursing, Mbarara University of Science and Technology, Mbarara, P.O BOX 1410, Uganda, Tel +256777842830, Email [email protected]
Background: Nurses miss recognizingalterations in patients’ conditions despite charting. This is due to a lack of knowledge and understanding of deterioration. The modified early warning score (MEWS) aids nurses in early recognition of and response to clinical deterioration. However, utilization of MEWS remains a major challenge at Mulago Hospital, where approximately 63.2% of in-hospital cardiac arrests remain unrecognized. This has resulted in a significant burden of critical illness, with a prevalence of 11.7% and mortality rate of 5.5%. Mulago Hospital-medical and surgical wards showed limited documentation of nurses’ use of the MEWS. This study assessed the effect of an educational intervention on nurses’ knowledge of the use of MEWS to recognize critical illnesses at the Mulago Hospital.
Methods and Materials: A descriptive, quantitative, quasi-experimental one-group pretest-posttest design was employed. A convenience sample of 77 nurses from the Medical and Surgical units of Mulago National Referral Hospital participated. Nurses received face-to-face teaching on the Modified Early Warning Score (MEWS). Data were collected using a validated self-administered questionnaire, with pre-intervention data gathered two weeks before and post-intervention data one month after the training. The Wilcoxon signed-rank test was used to evaluate the effect of the intervention on nurses’ knowledge of MEWS, with significance set at p < 0.05 and a 95% confidence interval.
Results: The educational intervention led to a significant improvement in nurses’ knowledge of the Modified Early Warning Score (MEWS), as evidenced by a Wilcoxon signed-rank test result of Z = 7.631 (p < 0.0001). Prior to the intervention, the majority of participants (67.53%, n = 52) demonstrated a novice level of MEWS knowledge. The study sample consisted predominantly of female nurses (67.53%, n = 52), with most participants (75.32%, n = 58) aged over 30 years. The mean age was 36.78 ± 8.21 years.
Conclusion: Nurses’ baseline knowledge of the nurses towards MEWS was low. Educational interventions significantly improved nurses’ knowledge toward modified early warning scores in the recognition of critical illness.
Keywords: knowledge, nurse, modified early warning score, Mulago, Uganda
Background
Timely recognition of clinical deterioration among patients remains a major obstacle in the management of critical illnesses in resource-limited settings.1,2 Critical illness is defined as “a state of ill health with vital organ dysfunction, a high risk of imminent death if timely care is not provided, and the potential for reversibility”.3 Globally, the majority of clinical deterioration cases occur in hospital general wards.4 This has resulted in high mortality from critical illnesses, with over 80% of individuals residing in low- and middle-income countries.5 One of the major factors associated with this high mortality rate is the lack of early recognition of critical illness.2 Regarding the recognition of critical illness, nurses should have adequate knowledge and practice towards early detection and response to critical illness among patients under their care.6,7 Nurses’ ability of the nurses towards timely recognition and respond to signs of clinical deterioration plays a significant role in preventing or minimizing adverse events in patients.8 However, nurses miss alterations in patients’ conditions despite their charting.9 The most important factor associated with this is a lack of knowledge and understanding of deterioration.10,11 Fortunately, the modified early warning score (MEWS) aids nurses in early recognition of and response to clinical deteriorations.12–14 Considering logistic challenges and limited resource availability, for example, limited health workforce, the modified early warning score has proven to be a better tool for the early recognition of critical illness in resource-limited settings.15 In addition, the modified early warning score (MEWS) has been cited as the most validated among other early warning scores.16 The MEWS focuses on systolic blood pressure, pulse rate, temperature, respiratory rate, and level of consciousness using “Alert, Responsive to voice, Responsive to Pain and Unresponsive” (AVPU) approach to identify patients at risk of significant clinical deterioration.14 Implementation of MEWS has been associated with a significant decline in in-hospital cardiac arrest, early intensive care unit transfer, and a reduction in unexpected deaths among patients.17,18
However, utilization of MEWS remains a major challenge at Mulago Hospital, where approximately 63.2% of in-hospital cardiac arrests remain unrecognized.19 This has resulted in a significant burden of critical illness, with a prevalence of 11.7% and a 5.5% mortality.20 Furthermore, the researcher’s review of records from the Mulago Hospital-medical and surgical wards showed limited documentation to demonstrate nurses’ use of MEWS. Consequently, Kruisselbrink, Kwizera20 underscored the need to train nurses in MEWS at the Mulago Hospital. Saab, McCarthy21 highlighted the limitations of high-quality evidence in evaluating the effects of early warning score educational programs on nurses’ knowledge, confidence, and clinical performance. Therefore, this study sought to assess the effect of an educational intervention on nurses’ knowledge of the use of the MEWS to recognize critical illnesses at Mulago Hospital.
Materials and Methods
Study Setting
This study was conducted in identified units and wards at the Mulago National Referral Hospital in central Uganda. Mulago National Referral Hospital is a national referral hospitals.22 It also serves as a teaching hospital for the Makerere University College of Health Sciences.23 The Mulago National Referral Hospital is situated approximately three kilometers from Kampala, Uganda’s capital city, and is the largest metropolitan area. Mulago Hospital has a bed capacity of 150024 and offers both outpatient and inpatient specialized medical and surgical services for both pediatric and adults.23 The study was conducted in the following identified units and wards: intensive care unit, accident and emergency unit, medical emergency unit, medical high-dependency unit, medical wards, gastrointestinal ward, and trauma ward. Non-probability purposive sampling was employed to select study units and wards. These units were chosen because they are more likely to handle patients at a risk of significant clinical deterioration. The intensive care unit is a 16–18 bed adult general intensive care unit.25,26 The accident and emergency unit handles an estimated 300 patients daily with a catchment population of over 2 million people.24 It handles over 48,000 patients per year.27 The medical side of the accident and emergency unit is a 55 bed unit and serves as an entry point for adult medical patients.23 The medical emergency unit has a total bed capacity of 25 beds, handling over 30 patients daily and over 900 patients in one month.28 The medical ward has a bed capacity of 70 patients. The neurosurgery ward has a 24 bed capacity and houses a 2-bed high dependency unit.26 Infectious disease and gastrointestinal wards have a bed capacity of 54 each but can stretch up to 70–80 admissions.29 The trauma unit is among the orthopaedic units that generally has a bed capacity of 100–120 and receives over 10 cases per day.30
Study Design
A descriptive quantitative, quasi-experimental one-group pretest-posttest study design was used, in which “a single group of participants was used to measure the degree of change occurring as a result of treatments or interventions”.31–33 A quasi-experimental study design was defined as “an observational study with an exogenous explanatory variable (treatment or exposure) that the investigator does not control”.34 This design was suitable for this study because randomization was difficult.35 A control group was difficult to create because, at the participants’ level, the nurses would interact with each other, which would risk contamination of the intervention. At the unit level, there were a few wards to attempt cluster randomization. Second, the nurses were inherently different in the units in which they practiced. Therefore, this preexisting difference could be erroneously attributed to the intervention. Finally, it would be unethical to withhold this intervention, which would benefit patient care in the control group. Consequently, this design was suitable because it used individual nurses as their own controls.
Study Population
The study enrolled nurses working in the Mulago National Referral Hospital Medical and Surgical Ward and units. Mulago Hospital has over 800nurses.36 The study participants included nurses working in the intensive care unit, accident and emergency unit, medical emergency unit, medical high-dependency unit, medical ward, gastrointestinal ward, and trauma ward. The intensive care unit has 30 nurses,25,26 accident and emergency unit have a total of 27 nurses (enrolled nurses, assistant nursing officers, nursing officers, trauma nurses) and two nursing assistants. A medical emergency has a total of 15 nurses offering 24hour services,28 medical ward has over 30 nurses of all cadres. The neurosurgery ward had over 18 nurses providing 24hour coverage.26 Finally, the infectious disease ward had a minimum of 4 nurses working per shift.36 These units/wards were chosen because they were more likely to handle patients at a risk of significant clinical deterioration.
Sample Size Determination
The sample size for educational intervention research was determined using the McConnell, Monteiro37 formula for obtaining sample size for educational intervention research:

“Whereby, δ represents the anticipated difference between group means (eg, μ1-μ2), and σ represents the pooled standard deviation between the two groups. Zα/2 is the value associated with the significance criterion, and Zβ is the value associated with the statistical power of the study. For a type-1 error of 0.05 (two-tailed), the corresponding Z α/2 was 1.96, and for a statistical power of 0.8, the corresponding Zβ was 0.842. This formula represents the sample size required for each group. Because the values associated with the significance criterion (Zα/2) and statistical power are conventionally set at 0.05 and 0.8, respectively, the formula above can be simplified to  whereby “16” comes from the full formula as described by Lehr.38 However, in this present MEWS study, there was uncertainty about the “δ” which is anticipated difference between the pre-intervention and post-intervention means scores of the knowledge and practice toward Modified early warning score. Similarly, uncertainty exists on “σ” which is the anticipated pooled standard deviation between pre-intervention and post-intervention scores of the knowledge and practice towards MEWS. In situations where there is uncertainty of specific information on δ and σ, the authors have suggested that sample size calculations should be performed using standardized effect sizes.39–41 Therefore, for the two-group comparison, using the conventional α = 0.05 and β = 0.20, the final formulae after several steps in the calculation are summarized as follows: n = 16(1/(effect size) 2), where n is the required sample size. Therefore, we used a standard medium effect size of 0.5,39 n = 16(1/(0.5) 2) = 64 participants. However, considering an attrition of 20%, = 20/100 = 0.2 = (0.2x64) = 12.8 participants. Therefore, the total sample size required was (64+12.8) = 76.8, approximately 77 participants. In addition, for a planned paired t-test analysis, a prior power analysis provided a total sample size of 20 participants per group to detect a large effect.42 Therefore, the final sample size for this MEWS educational interventional project of 77 participants was adequate to measure the effect of the intervention since we used a single group for pre-intervention and post-intervention.
whereby “16” comes from the full formula as described by Lehr.38 However, in this present MEWS study, there was uncertainty about the “δ” which is anticipated difference between the pre-intervention and post-intervention means scores of the knowledge and practice toward Modified early warning score. Similarly, uncertainty exists on “σ” which is the anticipated pooled standard deviation between pre-intervention and post-intervention scores of the knowledge and practice towards MEWS. In situations where there is uncertainty of specific information on δ and σ, the authors have suggested that sample size calculations should be performed using standardized effect sizes.39–41 Therefore, for the two-group comparison, using the conventional α = 0.05 and β = 0.20, the final formulae after several steps in the calculation are summarized as follows: n = 16(1/(effect size) 2), where n is the required sample size. Therefore, we used a standard medium effect size of 0.5,39 n = 16(1/(0.5) 2) = 64 participants. However, considering an attrition of 20%, = 20/100 = 0.2 = (0.2x64) = 12.8 participants. Therefore, the total sample size required was (64+12.8) = 76.8, approximately 77 participants. In addition, for a planned paired t-test analysis, a prior power analysis provided a total sample size of 20 participants per group to detect a large effect.42 Therefore, the final sample size for this MEWS educational interventional project of 77 participants was adequate to measure the effect of the intervention since we used a single group for pre-intervention and post-intervention.
Eligibility Criteria
The inclusion criteria were as follows: nurses who worked and regularly assigned duties at Mulago National Referral Hospital at the time of the study. All Nurses who had completed a minimum of three months providing direct service to patients in the medical ward, medical emergency unit, accident and emergency unit, medical high-dependency unit trauma ward, and gastrointestinal ward (GIT ward).
Nurses on leave at the time of data collection were excluded. Intern nurses who were unavailable at the study hospital during the intervention and posttest phases were excluded. This decision was made in consultation with unit managers and based on the researcher’s experience as a former nurse intern at Mulago National Referral Hospital (2019–2020). Interns often rotate between Mulago, Kawempe (for midwifery), and Kiruddu (for hands-on experience). Since the posttest was conducted one month after the intervention, it was anticipated that some interns would have rotated to other hospitals, leading to missing data and potentially affecting the study’s accuracy. Nursing assistants were excluded from this study. This is because they are not directly involved in patient clinical care.
Sampling Technique
Given that the number of nurses working in the individual study units was small, a convenience sampling strategy was employed to recruit all eligible nurses working in intensive care units, accidents and emergency units, medical emergency units, medical high-dependency unit medical wards, gastrointestinal wards, infectious disease wards, and trauma wards.
Data Collection Tools
The questionnaire was divided into three sections: The section captured the sociodemographic characteristics of the nurses, including gender, level of nursing training, length of experience, prior training on MEWS, prior training on basic life support, prior training on advanced life support, experience initiating or responding to code blue situations, current area of practice, and duration of working in the current unit/ward. This section assessed nurses’ knowledge of toward MEWS. The details of the data collection tool are described below.
Quantitative data on nurses’ knowledge were collected using a validated, paper-based questionnaire consisting of 41 items. The tool was originally developed by liswati43 and demonstrated good validity and reliability. It has since been used in related studies, including by Olang, Manik,44 who assessed nurses’ knowledge of early warning systems in a private hospital in Indonesia. The instrument showed strong psychometric properties, with a Cronbach’s alpha of 0.75 and item-total correlations above 0.40.44
Permission to adapt this tool for the current study was obtained from Olang, Manik.44 Following a comprehensive literature review, the researcher made contextual modifications to focus on components of the Modified Early Warning Score (MEWS) as implemented at Mulago National Referral Hospital20 and Mbarara Regional Referral Hospital45 in Uganda. These modifications were informed by related studies,14,46–49 and the adapted tool was reviewed for content validity by experts in emergency and critical care.
Oxygen saturation and urine output were excluded from the questionnaire, as they were not part of the MEWS used in the current project. Items originally assessing scoring using oxygen saturation were replaced with equivalent alternatives to maintain the construct validity of the tool.
Additional guidance for modifying the tool was drawn from a study by Janakaraj,50 which evaluated the effectiveness of education on MEWS for nurses in the United States.
The final questionnaire consisted of 41 items assessing knowledge of MEWS. Of these, 28 were true/false statements, three were multiple-choice questions, and 10 were short-structured questions requiring brief written responses. The tool was administered as both a pre-test and a post-test, conducted four weeks after the completion of the educational intervention.
Data Collection Procedure
Upon the necessary approvals, from 20th July 2023 to 20th October 2023 the data collection then proceeded by the principal investigator and knowledgeable, trained and experienced research assistants. Data collection was done in three phases that is; pre-intervention phase, intervention, and post-intervention phases.
Pre-Intervention Phase
Pre-interventional data were collected by the researchers one week before the intervention. These pre-intervention findings facilitated the modification of the teaching plan based on participants’ baseline knowledge and practices regarding MEWS. Data were collected using a self-administered researcher-designed questionnaire issued to each respondent with explanations as necessary. The respondents answered the questionnaire in approximately 45 minutes, without referring to any resources, and handed it over to the researcher immediately upon completion.
Intervention Phase
The educational session aimed to enhance nurses’ knowledge of the use of a modified early warning score. This phase was performed two weeks after the pre-intervention phase.
This study used a face-to-face teaching strategy. The session included a group of 12–14 participants per session and was a one-time session per group for a period of one month for all eight study units/wards. The intervention was performed separately for each unit and ward. The study participants consisted of different cadres, given that different cadres were free during a particular period, which maximized participation. The teaching sessions were provided twice on the same day during the morning and afternoon after a discussion with the unit in charge of its possibility so that all nurses on different shifts could participate. Nurses who agreed to participate were requested to attend the changeover shift. For participants who felt tired after their duties, a special arrangement was made, particularly regarding their duties. The aim was to protect the participants from extra fatigue during their participation in this study. The teaching session was held for one hour daily per session.
A PowerPoint presentation on introduction to clinical deterioration and critical illness, the validated modified early warning score in the Ugandan setting,20,45 calculation of the MEWS score, identification of clinical deterioration, and escalation of care as stipulated in the MEWS flow algorithm was used during the teaching session. PowerPoint was made available as a handout of slides and printed as hard copies. These hard copies facilitated learning in the case of unstable electricity. Two short videos, each lasting 5 minutes, were adapted from YouTube academic channels and were shown to the participants after a thorough audit to reinforce the completion of the modified early warning score tool in clinical practice. In addition, a patient case scenario with vital signs designed by the researchers after a comprehensive literature review was used to further enhance the nurses’ understanding of the modified early warning score. Other materials, including an ink pen, the MEWS tool itself, and case study scenarios, were available to participants during the study period. The Modified early warning score flow sheet was checked to determine the accuracy of the MEWS scores calculated by the participants in response to the case scenarios provided. All these were used to ensure an efficient and comprehensive understanding of the material. It is important to emphasize that, at the end of the training, the participants were provided with a certificate indicating the knowledge attained on the modified early warning score.
Post-Intervention Phase
The post-intervention data were collected using the same questionnaire and checklist used in the pretest, one month after the educational interventions were completed. This period of data collection post-intervention was based on guidance from other related studies.26,51,52 The data collection procedure is illustrated in Figure 1.
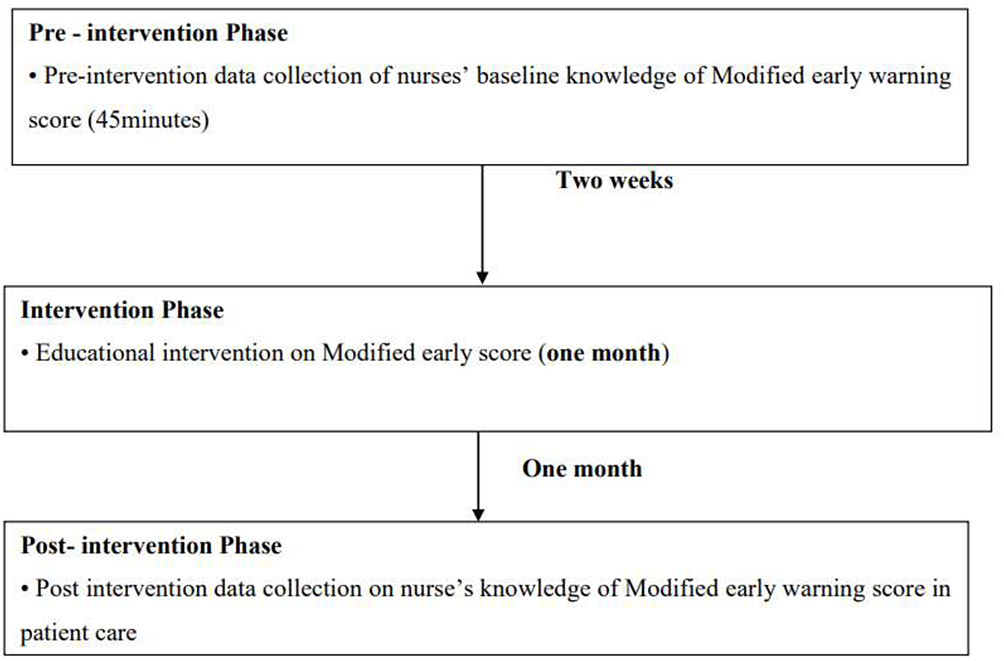 |
Figure 1 Study profile. |
Data Management Analysis and Presentation
After data collection, the data were entered into the EpiData software version 3.10, where they were cleaned, coded, and checked for completeness. Knowledge questions was coded “True = 1” for the correct response and “False = 0” for an incorrect response. For knowledge, a score was given “1” for questions answered correctly and “0” for questions answered wrongly. This facilitated obtaining the overall mean knowledge scores pre-intervention and post-intervention. The denominator for knowledge score was 41. The ranking of the nurses’ knowledge of the Modified early warning scores was based on Benners’ stages of competency53 as follows: A total knowledge score ≥ 90% was categorized as “Excellent” and the corresponding level of competency was “Expert”; 80% to 89% was categorized as “Very good” and the corresponding level of competency was “Proficient”; 70% to 79% was categorized as “good” and the corresponding level of competency was “competent”; 60% to 69% was categorized as “Fair” and the corresponding level of competency was “Advanced beginner”; <60% was categorized as “Fail” and the corresponding level of competency was “Novice.”
For data analysis and presentation, Data from EpiData were exported to STATA, version 17.0 for statistical analysis.
Descriptive statistics in terms of mean and standard deviation were performed for continuous variables and frequencies and percentages for categorical variables. These analyses were performed for demographic, pre-intervention, and post-intervention data. For knowledge scores pre- and post intervention, a test for assumption of normality was performed using statistical tests such as skewness and kurtosis tests. The statistical test of normality of the distribution of scores revealed that post-test knowledge scores (p = 0.00233) were not normally distributed.
The Mean, median, and standard deviation of the differences in knowledge scores for knowledge pre-intervention and post-intervention were obtained. The effects of the educational intervention were then assessed. However, since the post-test knowledge data were not normally distributed, the “Wilcoxon signed-rank test” was used to assess the effect of the educational intervention on nurses’ knowledge of the nurses toward modified early warning scores. For all analyses, the level of significance was set at a 95% confidence interval of 0.05. Statistical significance was set at p < 0.05. Data are presented as tables and graphs, where applicable.
Quality Control Measures
The study employed a validated tool to measure knowledge of the Modified Early warning score. The questionnaires were pretested with five nurses working in the medical ward of Mbarara Regional Referral Hospital to ensure consistency. Ambiguous questions were adjusted accordingly. Furthermore, both the questionnaire and teaching materials were given to the researchers and content experts for perusal, and corrections were made. The tests and instructions were given in the same manner in a similar situation for all nurses to increase the reliability of the tools. The data collection tool was tested using Cronbach’s alpha which was 0.85. The training of the research assistants was ensured. The research assistants included nurses with masters of nursing science in critical care nursing who were experienced in the management of deteriorating and critically ill patients.
Ethical Considerations
This study was approved by the Mbarara University of Science and Technology Research and Ethics Committee (Reference number: MUST-2023-844), and administrative clearance was obtained from Mulago National Referral Hospital. Additional permission was secured from the managers of the respective study units. Verbal and written informed consent was obtained from participants after a detailed explanation of the study’s aims and procedures. Participation was entirely voluntary, and individuals were informed that withdrawal would not affect their professional standing or care delivery. During all phases of the study, confidentiality was strictly upheld; participants were assigned unique identification numbers to ensure anonymity, and all information collected was accessible only to the research team. Strict Adherence to the “ethical principles for medical research involving human subjects” as stipulated in the “Declaration of Helsinki”54 and the “ethical principles of Belmont report of respect for persons, beneficence and justice”54 was ensured throughout the entire research process.
Results
Demographics of the Participants
A total of 77 nurses were recruited for the study. The majority of the participants (52 [67.53%]) were females. Most of the participants 58 (75.32%) were aged above 30 years with a mean aged of 36.78 ± 8.21 years and a medium age of 35 years. Regarding the Level of education, the majority of participants 43 (55.84%) were at the diploma level, followed by the bachelor’s level, 29 (37.66%). Regarding Ugandan employment, the majority 43 (55.84%) were assistant nursing officers. This was followed by 31 (40.26%) nursing officers. Regarding nursing experience, the majority of the participants 29 (37.66%) had worked between 6–10 years. The mean number of years worked in their current wards was 3.40 ± 2.13years. Table 1 presents the results.
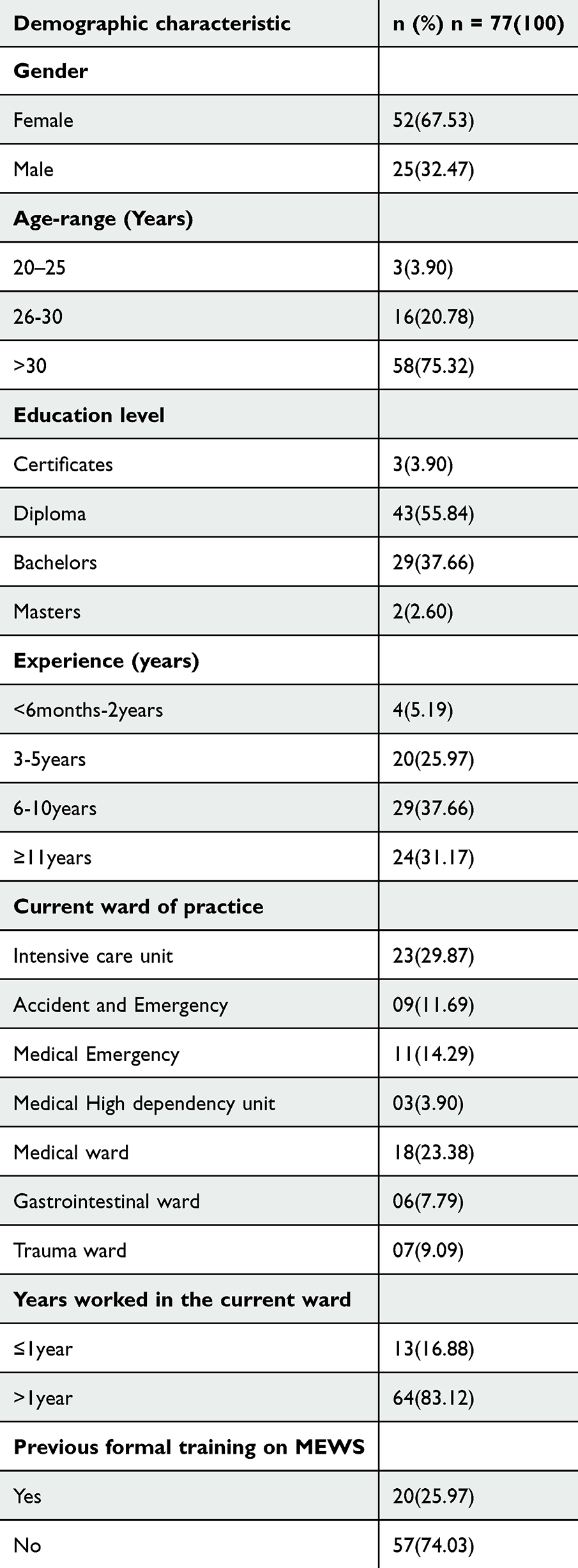 |
Table 1 Socio-Demographic Characteristics of the Participants |
Knowledge of Nurses on Modified Early Warning Score
The majority of the participants 73 (94.81%) in the pretest knew that it was true that the modified early warning score had five physiological parameters, while in the post-test, 77 (100%) knew that the MEWS had five physiological parameters, including systolic blood pressure, pulse rate, breathing frequency, temperature, and level of consciousness. Regarding the indication of MEWS, approximately 64 (83.12%) of the participants knew that MEWS was used for all patients who were hospitalized (hospital) in both internal medicine and surgery wards/units, while 73 (94.81%) knew this indication in the post-test. Table 2 presents the results.
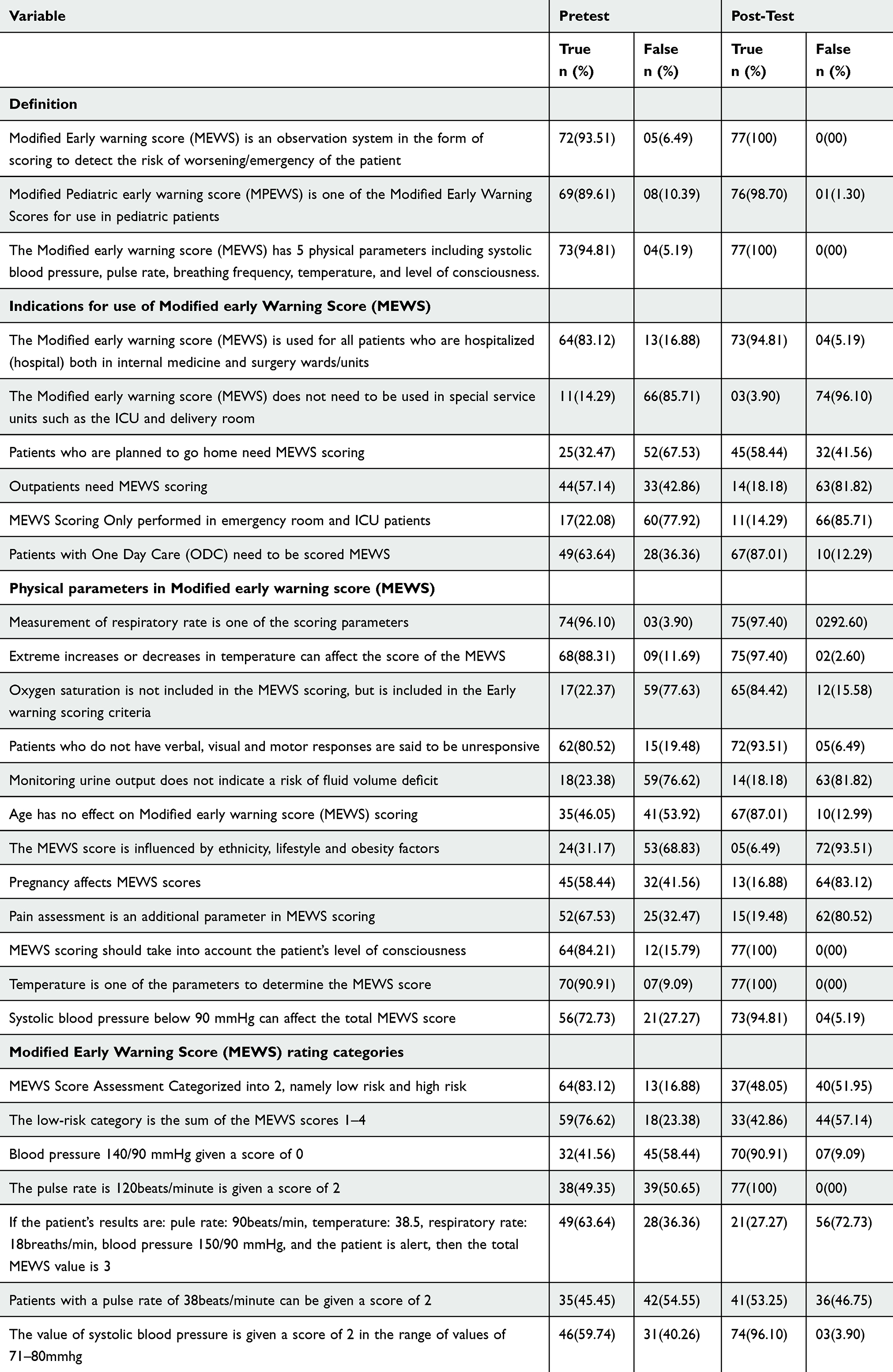 |
Table 2 Knowledge of the Nurses’ Pretest and Post-Test on Specific Items Under Definition, Indication, Parameter and Rating of Modified Early Warning Score |
Knowledge of the Nurses on the Actions/Intervention in Response to the Modified Early Warning Score
Approximately 13 (16.88%) participants knew how often the MEWS score was achieved. The majority (n = 62, 80.52%) did not know where to document the modified early warning score. The majority, 55 (71.43%), did not perform the actions for a patient, with a mean score of 0–2. The majority, 64 (83.12%), did not know the actions for an MEWS score of 3–4. About 64 (83.12%) participants did not take action to be undertaken for a MEWS score of 4, and the majority did not know the intervention to be done for a patient with a MEWS score of greater than 5. The results are summarized in Table 3.
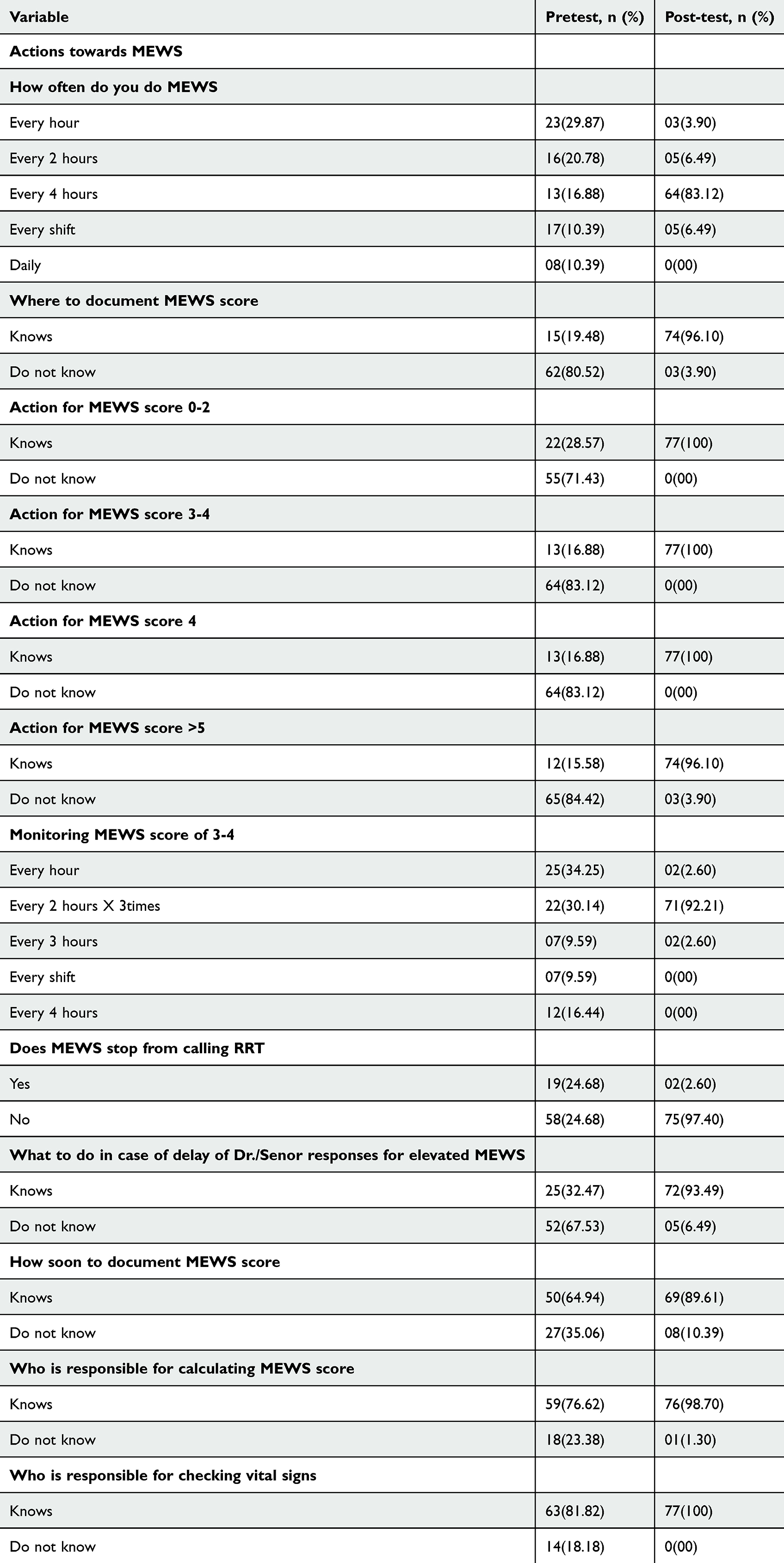 |
Table 3 Knowledge of the Nurses on the Actions/Intervention in Response to the Modified Early Warning Score |
Knowledge Rank of the Nurses Towards Modified Early Warning Score
The majority 52 (67.53%) demonstrated a novice level of knowledge, meaning that they scored less than 60% of the overall knowledge score according to Patricia-Benner’s ranking of the knowledge level of nurses. This was followed by about 18 (23.38%) of the nurses demonstrating an advanced beginner’s level of knowledge, meaning that they scored between 60–69% on the overall knowledge towards the modified early warning score. Further breaking down their knowledge of the different aspects of the Modified Early Warning score, the majority 66 (85.71%) of participants demonstrated an expert level of knowledge towards the definition of MEWS. The results are summarized in Table 4.
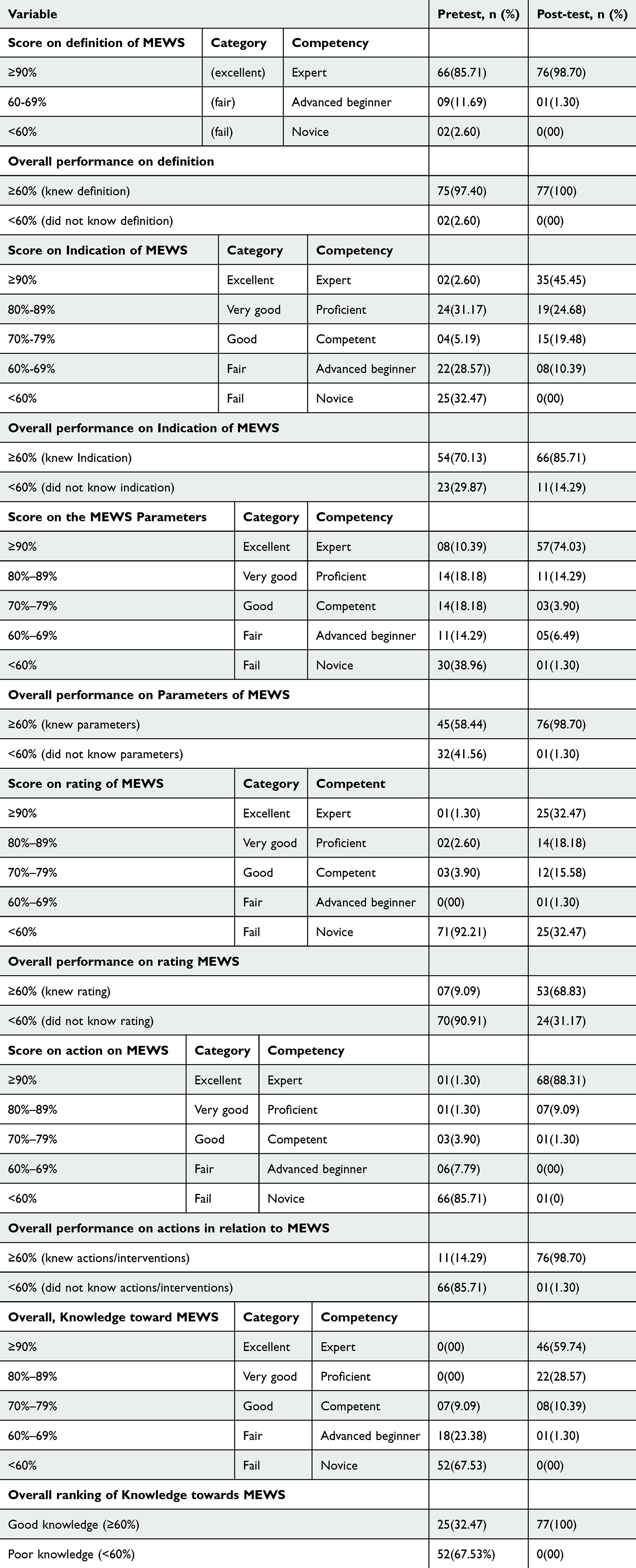 |
Table 4 Knowledge Rank of the Nurses Towards Modified Early Warning Score |
Effect of Educational Intervention on Nurses’ Knowledge on MEWS
The mean knowledge of the nurses towards the modified early warning score before the intervention was 22.06 ± 3.83 with a median knowledge of 21. The mean knowledge score of the nurses post-intervention was 40 ± 3.35 with a median knowledge score of 36. Because the knowledge post-intervention score was not normally distributed (p < 0.0001), a Wilcoxon signed-rank test was performed to determine the effect of the educational intervention on nurses’ knowledge towards modified early warning scores. The results showed that the educational intervention affected the nurses’ knowledge of the modified early warning score (Z = 7.631, p < 0.0001). The results are summarized in Table 5.
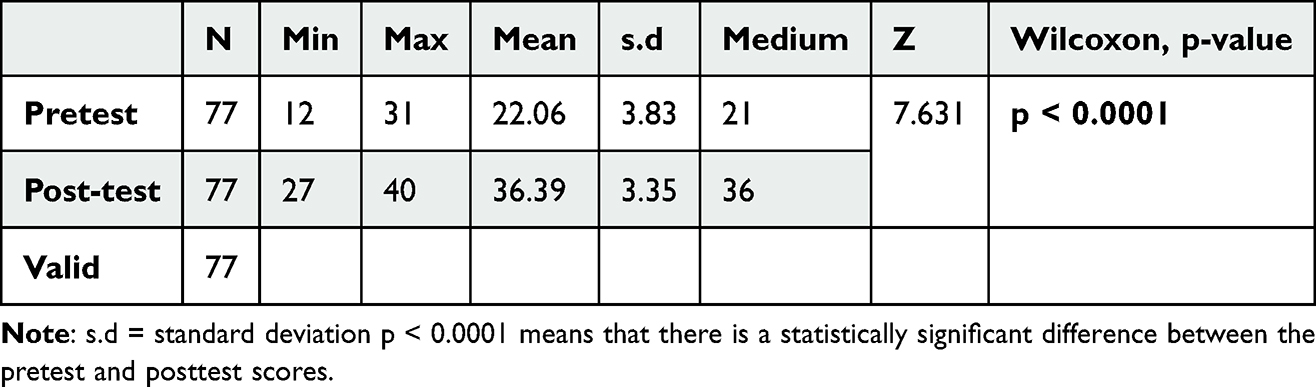 |
Table 5 Effect of Educational Intervention on Nurses’ Knowledge Towards MEWS |
Discussions
This study aimed to understand the effect of an educational intervention on nurses’ knowledge towards the use of the modified early warning score (MEWS) in the recognition of critical illness at the Mulago National Referral Hospital.
Baseline Knowledge of the Nurses Towards Modified Early Warning Score
The findings from the study revealed a generally low baseline knowledge of nurses towards modified early warning scores with the majority of the nurses; 52(67.53%) being classified as novices. The possible explanation for this observed low baseline knowledge of the participants towards MEWS could be lack of regular training on MEWS. This was demonstrated by the majority 57(74.03%) reporting to have had no formal previous training on MEWS. The findings of this study on the low baseline knowledge of the Modified Early Warning Score (MEWS), is consistent with findings from several studies across Africa, which have similarly reported limited knowledge and understanding of early warning systems among frontline healthcare providers. In South Africa, Burger, Jordan56 found that many nurses had never received formal training in MEWS or other early warning systems prior to study interventions. Their baseline assessments showed significant knowledge gaps, particularly in interpreting vital signs and recognizing early signs of clinical deterioration. This aligns with our findings at Mulago National Referral Hospital, suggesting that even in tertiary referral settings, knowledge about MEWS remains inadequate without targeted training. Similarly, in Uganda, Kruisselbrink, Kwizera20 evaluated the utility of MEWS in identifying critical illness among hospitalized patients but noted that the successful implementation of MEWS was challenged by limited awareness and training among nursing staff. This highlights a consistent theme that while MEWS may be a validated tool, its effectiveness is compromised by poor baseline knowledge among users particularly nurses who the first point of contact for patient are monitoring. Furthermore, Nakitende, Nabiryo15 reported that although MEWS and other scoring systems had predictive utility, their impact on patient outcomes was constrained by poor familiarity among healthcare providers. Their study emphasized the need for intensive education and contextual adaptation of scoring tools to improve their uptake and consistent use. However, the findings from this study on nurses’ knowledge of the nurses towards modified early warning scores are contrary to those of a study conducted by Olang, Manik44 in Indonesia, which revealed adequate knowledge of nurses towards early warning scores. A possible explanation for the differences in these study findings could be due to differences in the study design and setting. Expounding this further, Olang, Manik44 did not provide a theory to guide their investigation. Furthermore, nurses’ knowledge of the MEWS varied according to the practice setting. The setting usually differed in terms of factors such as local healthcare policies, the availability of educational resources, or nurse workload. Therefore, the present study provides an understanding of nurses’ knowledge of nurses towards MEWS from the perspective of developing countries, such as Uganda, and the results show that their knowledge was poor. A significant knowledge gap was observed regarding the indicators used in MEWS with only 2.6% demonstrating expert knowledge and 32.47% classified as novices. This could be attributed to inadequate training or lack of exposure to MEWS during both pre-service and in-service education. A substantial proportion (74.03%) of the study participants reported no prior formal training on MEWS, which likely contributed to their poor knowledge in regards to MEWS indicators. Training has been consistently associated with improved knowledge and confidence in using early warning scores.46 With regard to knowledge of the physiological parameters, including the respiratory rate, systolic blood pressure, level of consciousness, pulse rate, and temperature that make up the MEWS, the nurses’ knowledge was wanting in this aspect, as the majority 30(38.96%) were found to be novices. Regarding the rating (scoring) of the modified early warning score parameters, their knowledge was very poor, as the majority 71 (92.21%) demonstrated a novice level of knowledge in this aspect. The findings of this study on the knowledge of the physiological parameters that constitute the modified early warning score and their ratings are similar to those in related studies conducted by Eddahchouri, Koeneman57 in the Netherlands and Credland, Dyson58 in a narrative review. This was described in these related studies in terms of Nurses’ poor compliance with early warning scores in terms of early warning score calculation accuracy, monitoring frequency and clinical response and generally incomplete early warning scores assessments.57,58 This study also investigated nurses’ knowledge of actions towards the actions/intervention in relation to their MEWS. Nurses reported a lack of knowledge regarding this aspect. This was shown by the majority of 66 (85.71) who did not know what interventions to be done in response to the total scores obtained upon calculation of the MEWS score. Although the nurses generally had limited overall knowledge of MEWS, knowledge of some aspects, such as the definition of the modified early warning score, was good. This was demonstrated by 66 (85.71) participants with expert knowledge regarding the definition of MEWS.
Effect of Education on Nurses’ Knowledge on Modified Early Warning Score
The findings of this study demonstrated that the educational intervention had an effect on nurses’ knowledge toward the modified early warning scores using the Wilcoxon signed-rank test (Z = 7.631, p < 0.0001). The possible explanation for the improvement of the nurses’ knowledge with the educational intervention could as a result adhering to the Knowles’s principles of adult learning. These findings are in agreement with those from related studies in Africa. For example, Nadr Ebraheim, Karawan Sayed Sallam59 in Egypt found a significant improvement of studied nurses’ performance regarding identification and response to clinical deterioration due to positive effect of EWS educational program intervention. Similar findings are in line with those from other related studies across the globe21,50,60,61 in which an educational intervention for nurses was associated with a significant increase in nurses’ knowledge towards modified early warning scores. While our finding (Z = 7.631, p < 0.0001) aligns with the broader literature indicating knowledge gain from nurse education on MEWS, nuanced differences exist.21,50,60,61 Janakaraj50 in the United States used a paired t-test under normal distribution assumptions, whereas our data violated normality, prompting choice of the Wilcoxon test to maintain validity. Damayanti, Trisyani60 strengthened causal claims by including a control group and between-group analyses, whereas our single-group pre-post design limits causal inference despite showing within-group improvement. Finally, our adoption of Knowles’ adult learning theory parallels Mussa, Al-Raimi61 in Midwestern United States who employed of Technology acceptance model (TAM), although they focused on attitudes and behavioral intention toward MEWS technology, extending beyond pure knowledge gain. Further findings from a systematic review by Saab, McCarthy21 found that and educational interventions significantly improved nurses knowledge in regard to MEWS.
Study Strengths and Limitations
The first notable limitation of this study was the absence of an independent control group (noninterventional group). The variations in the characteristics of the study units at Mulago National Referral Hospital made it difficult to select non-intervention units that could be compared to the experimental wards/units. This limitation weakens the internal validity of the study and poses challenges to confidently attributing the observed improvements in nurses’ knowledge of the Modified Early Warning Score (MEWS) solely to the educational intervention. Without a control group, it becomes difficult to rule out alternative explanations for the observed changes. Factors such as increased awareness of MEWS from other informal sources (eg, peer discussions, hospital policy updates, or concurrent trainings), the Hawthorne effect (participants altering behavior due to being observed), or maturation (natural improvement over time) could have contributed to the post-intervention improvement in knowledge. The design does not allow for distinguishing whether the knowledge gains were a direct result of the structured training or influenced by these external variables. Additionally, the one-group design limits the ability to generalize findings. A control group receiving no intervention or receiving an alternative form of training would have provided a benchmark to compare the effectiveness of the intervention against usual practices. Such comparison would strengthen causal inferences and provide more robust evidence of the intervention’s true impact. However, despite the absence of a control group, the pre- and post-test design and follow-up after one month of intervention increased the robustness of the results. The second limitation of this study is that it was a single-center study conducted in a national referral hospital. Therefore, this may limit the generalizability of the findings to lower-centered facilities such as regional referral and district hospitals. However, Mulago National Referral Hospital has the largest number of nurses among all cadres in Uganda. With the transfer system in Uganda that allows the transfer of nurses from one facility, for example, a regional referral hospital to a national referral hospital, the nurses will therefore be representative of all nurses in Uganda and reduce the threat to the generalizability of the findings. Finally, the potential biases from convenience sampling was minimized by ensuring a diverse representation across different wards and roles.
Implication for Practice
The study generated information about the use of the Modified Early Warning score in the recognition of critical illness and proved that educational intervention improves the knowledge and practice of nurses towards the use of the Modified Early Score in the recognition of critical illness. This information will help nurses easily adopt a validated modified early warning score for Uganda to use for monitoring patients both in the wards and in emergency and critical care units, which will improve clinical practice.
It will serve as an eye-opener for nurses in education to put more emphasis on the use of the modified early warning score in monitoring patients, while training students in both theoretical and clinical areas. To maintain and enhance MEWS-related knowledge, it is critical to integrate regular refresher sessions into existing in-service education schedules. These could be offered quarterly or biannually and should focus on reinforcing key concepts, updating staff on any protocol changes, and using clinical scenarios or simulations to sharpen decision-making skills. Refresher trainings should also address common challenges nurses face in MEWS implementation and emphasize real-time application. Establishing a mentorship system where experienced nurses or clinical educators offer ongoing guidance can bridge the gap between theory and practice. Unit-based champions or MEWS “super-users” can support their peers in interpreting scores correctly and responding to deterioration promptly. Supervisors can also periodically assess MEWS charts and provide Given that many nurses demonstrated novice-level knowledge, incorporating MEWS into pre-service nursing curricula and mandatory orientation programs for new hires will ensure foundational competence before practice begins. This early exposure builds familiarity and confidence in recognizing patient deterioration.
Implication for Future Research
Exploratory descriptive research with a larger sample should be conducted by examining nurses’ knowledge and practice regarding the use of the modified early warning score in the recognition of critical illness.
A randomized controlled trial should be conducted to assess whether educational intervention improves nurses’ knowledge and practices regarding the use of the Modified Early Warning Score in the recognition of critical illness among patients.
The same study can be conducted with a mixed design, especially with an intervention and a control group, where observation can be included to ascertain whether the nurses actually implement the modified early warning score in a real practice environment.
The study findings will act as a baseline for future studies on the use of modified early warning scores in the recognition of critical illnesses by nurses in the research and clinical fields.
Conclusion
The study established an insight into the local perspective on the knowledge of nurses towards the Modified Early Warning score and later examined the effect of an educational intervention on nurses’ knowledge towards the Modified Early Warning score.
It has been demonstrated that nurses’ baseline knowledge of the nurses toward the modified early warning score at Mulago National Referral Hospital falls short of the recommended guidelines.
In addition, this study showed that educational intervention significantly improved nurses’ knowledge (p < 0.0001) toward the use of modified early warning scores in recognition of critical illness.
Recommendations
Based on the outcome of this study, hospital administration should regularly arrange refresher continuous in-service education or out-of-hospital nurse training for nurses regarding the use of modified early warning scores in early recognition of critical illness. This will equip the staff with the knowledge and skills needed to advance quality care for patients.
The Ministry of Health and Hospital Administration should provide guidelines for Modified Early Warning scores in strategic places, especially on the walls of different units, to guide nurses in the assessment of patients.
Modified early warning scores should be included in the nursing curricula at different levels of nursing training.
Nurses in the wards, ICU, Emergency, and high-dependence units should always monitor patients using the Modified Early Warning Score and use a tool that has been tested to be effective at Mulago National Referral Hospital. This will help in the early recognition of clinical deterioration, and therefore, in early interventions to mitigate preventable deaths.
Data Sharing Statement
Data from this study will be freely made available by the corresponding author.
Acknowledgment
We are grateful to the study participants and the Adminstration of Mulago National Referral Hospital for their clearance for this study to be conducted.
Author Contributions
All authors made a significant contribution to the work reported, that is in the conception, study design, execution, and acquisition of data, analysis and interpretation. All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Schell CO, Gerdin Wärnberg M, Hvarfner A, et al. The global need for essential emergency and critical care. Critical Care. 2018;22(1):1–5. doi:10.1186/s13054-018-2219-2
2. Diaz JV, et al. Global critical care: moving forward in resource-limited settings. Annal global health. 2019;85(1).
3. Kayambankadzanja RK, Schell CO, Gerdin Wärnberg M, et al. Towards definitions of critical illness and critical care using concept analysis. BMJ Open. 2022;12(9):e060972. doi:10.1136/bmjopen-2022-060972
4. Kellett J, Sebat F. Make vital signs great again–A call for action. Eur J Internal Med. 2017;45:13–19. doi:10.1016/j.ejim.2017.09.018
5. Hopkinson D, Akuamoah-Boateng K, Banguti P, et al. The impact of the fundamental critical course on knowledge acquisition in Rwanda. Southern African J Critical Care. 2022;38(1):14–19. doi:10.7196/SAJCC.2022.v38i1.491
6. Liyew B, Tilahun AD, Kassew T. Knowledge, attitude, and associated factors towards physical assessment among nurses working in intensive care units: a multicenter cross-sectional study. Critical Care Res Practice. 2020;2020.
7. Bliss M, Aitken LM. Does simulation enhance nurses’ ability to assess deteriorating patients? Nurse education in practice. Nurs Edu Practice. 2018;28:20–26. doi:10.1016/j.nepr.2017.09.009
8. Massey D, Chaboyer W, Anderson V. What factors influence ward nurses’ recognition of and response to patient deterioration? An integrative review of the literature. Nurs Open. 2017;4(1):6–23. doi:10.1002/nop2.53
9. Al-Moteri M, Plummer V, Cooper S, et al. Clinical deterioration of ward patients in the presence of antecedents: a systematic review and narrative synthesis. Aust Crit Care. 2019;32(5):411–420. doi:10.1016/j.aucc.2018.06.004
10. Treacy M, Stayt LC. To identify the factors that influence the recognizing and responding to adult patient deterioration in acute hospitals. J Adv Nurs. 2019;75(12):3272–3285. doi:10.1111/jan.14138
11. Posthuma LM, Visscher MJ, Hollmann MW, et al. Monitoring of high-and intermediate-risk surgical patients. Anesthesia Analg. 2019;129(4):1185–1190. doi:10.1213/ANE.0000000000004345
12. Jensen JK, Skår R, Tveit B. The impact of early warning score and rapid response systems on nurses’ competence: an integrative literature review and synthesis. J Clin Nurs. 2018;27(7–8):e1256–e1274. doi:10.1111/jocn.14239
13. Al-Kalaldeh M, Suleiman K, Abu-Shahroor L, et al. The impact of introducing the modified early warning score’MEWS’on emergency nurses’ perceived role and self-efficacy: a quasi-experimental study. Int Emerg Nurs. 2019;45:25–30. doi:10.1016/j.ienj.2019.03.005
14. Warren T, Moore LC, Roberts S, et al. Impact of a modified early warning score on nurses’ recognition and response to clinical deterioration. J Nurs Manag. 2021;29(5):1141–1148. doi:10.1111/jonm.13252
15. Nakitende I, Nabiryo J, Namujwiga T, et al. Do different patient populations need different early warning scores? The performance of nine different early warning scores used on acutely ill patients admitted to a low-resource hospital in sub-Saharan Africa. Clin Med. 2020;20(1):67. doi:10.7861/clinmed.2019-0196
16. Gerry S, et al. Early warning scores for detecting deterioration in adult hospital patients: systematic review and critical appraisal of methodology. BMJ. 2020;369.
17. Bunkenborg G, Poulsen I, Samuelson K, et al. Mandatory early warning scoring—implementation evaluated with a mixed-methods approach. Appl Nurs Res. 2016;29:168–176. doi:10.1016/j.apnr.2015.06.012
18. Zografakis‐Sfakianakis M, De Bree E, Linardakis M, et al. The value of the Modified Early Warning Score for unplanned Intensive Care Unit admissions of patients treated in hospital general wards. Int J Nurs Practice. 2018;24(3):e12632. doi:10.1111/ijn.12632
19. Ocen D, et al. Prevalence, outcomes and factors associated with adult in hospital cardiac arrests in a low-income country tertiary hospital: a prospective observational study. BMC Emerg Med. 2015;15(1):1–6. doi:10.1186/s12873-015-0047-0
20. Kruisselbrink R, Kwizera A, Crowther M, et al. Modified early warning score (MEWS) identifies critical illness among ward patients in a resource restricted setting in Kampala, Uganda: a prospective observational study. PLoS One. 2016;11(3):e0151408. doi:10.1371/journal.pone.0151408
21. Saab MM, McCarthy B, Andrews T, et al. The effect of adult Early Warning Systems education on nurses’ knowledge, confidence and clinical performance: a systematic review. J Adv Nurs. 2017;73(11):2506–2521. doi:10.1111/jan.13322
22. Kwizera A, Sendagire C, Kamuntu Y, et al. Building Critical Care Capacity in a Low-Income Country. Critic Care Clin. 2022;38(4):747–759. doi:10.1016/j.ccc.2022.07.003
23. Nakalema I, Kaddumukasa M, Nakibuuka J, et al. Prevalence, patterns and factors associated with hypertensive crises in Mulago hospital emergency department; a cross-sectional study. Afr Health Sci. 2019;19(1):1757–1767. doi:10.4314/ahs.v19i1.52
24. Wangoda R, et al. Animal bite injuries in the accident and emergency unit at Mulago Hospital in Kampala. Uganda Pan African Med J. 2019;33.
25. Atumanya P, Sendagire C, Wabule A, et al. Assessment of the current capacity of intensive care units in Uganda; A descriptive study. J Crit Care. 2020;55:95–99. doi:10.1016/j.jcrc.2019.10.019
26. Nakiganda C, et al. Improving nurses’ knowledge on sepsis identification and management at mulago national referral hospital: a quasi experimental study. Nurs Res Rev. 2022;12:169–176.
27. Luggya TS, Alenyo Ngabirano A, Sarah R, et al. Trauma unit admissions at the Ugandan National Referral Hospital: a descriptive study. Afr Health Sci. 2022;22(1):404–409. doi:10.4314/ahs.v22i1.49
28. Kisuule I, Seremba E, Kagimu M. Prevalence of gastrointestinal bleeding and frequency of selected predictors of mortality on the medical emergency ward at mulago hospital. 2020.
29. Kiguba R, Karamagi C, Bird SM. Extensive antibiotic prescription rate among hospitalized patients in Uganda: but with frequent missed-dose days. J Antimicrob Chemother. 2016;71(6):1697–1706. doi:10.1093/jac/dkw025
30. Bizimana J, et al. Colonization of patients hospitalized at orthopedic department of tertiary hospital in uganda with extended-spectrum beta-lactamase-producing enterobacteriaceae. 2022.
31. White H, Sabarwal S. Quasi-experimental design and methods. Methodological briefs: impact evaluation. 2014;8(2014):1–16.
32. Flannelly KJ, Flannelly LT, Jankowski KRB. Threats to the internal validity of experimental and quasi-experimental research in healthcare. J Health Care Chaplaincy. 2018;24(3):107–130. doi:10.1080/08854726.2017.1421019
33. Siedlecki SL. Quasi-experimental research designs. Clinic Nurs Special. 2020;34(5):198–202. doi:10.1097/NUR.0000000000000540
34. Bärnighausen T, Tugwell P, Røttingen J-A, et al. Quasi-experimental study designs series—paper 4: uses and value. J Clin Epidemiol. 2017;89:21–29. doi:10.1016/j.jclinepi.2017.03.012
35. Miller CJ, Smith SN, Pugatch M. Experimental and quasi-experimental designs in implementation research. Psychiatry Res. 2020;283:112452. doi:10.1016/j.psychres.2019.06.027
36. Erkki L, Hedlund J. nurses’ experiences and perceptions of caring for patients with HIV/AIDS in Uganda. 2013.
37. McConnell MM, Monteiro S, Bryson GL. Sample size calculations for educational interventions: principles and methods. Can J Anaesth. 2019;66(8):864–873. doi:10.1007/s12630-019-01405-9
38. Lehr R. Sixteen S‐squared over D‐squared: a relation for crude sample size estimates. Stat Med. 1992;11(8):1099–1102. doi:10.1002/sim.4780110811
39. Cohen J. Statistical Power Analysis for the Behavioral Sciences Lawrence Earlbaum Associates. 20th–. Lawrence Earlbaum Associates; 1988.
40. Allen JC. Sample size calculation for two independent groups: a useful rule of thumb.
41. Norman G, Monteiro S, Salama S. Sample size calculations: should the emperor’s clothes be off the peg or made to measure? BMJ. 2012;345.
42. Buchner A, et al. G* power (version 3.1. 2)[computer program]. 2009.
43. liswati RMMKTH. Gambaran tingkat pengetahuan perawat tentang early warning score di RSKB cinta kasih tzu chi cengkareng. Jakarta Univesitas Indonesia. 2015.
44. Olang J, Manik MJ, Simamora O. Nurses’knowledge of early warning score At A Private Hospital In Eastern Indonesia. Nurs Curr. 2019;7(1):9–15.
45. Tumwesigye R. Use of Modified Early Warning Score to Detect Critical Illness in Medical Ward Mbarara Regional Referral Hospital. Mbarara University of science and technology: University Libraray. in Nursing. 2021.
46. Subbe CP, et al. Validation of a modified Early Warning Score in medical admissions. Qjm. 2001;94(10):521–526. doi:10.1093/qjmed/94.10.521
47. Abd Al Mohsen AH, Shehata MA. Value of modified early warning score among critically ill patients. Med J Cairo Univ. 2010;78(1).
48. Reini K, Fredrikson M, Oscarsson A. The prognostic value of the Modified Early Warning Score in critically ill patients: a prospective, observational study. Eur J AnaesthesioL. 2012;29(3):152–157. doi:10.1097/EJA.0b013e32835032d8
49. Montenegro SMSL, Miranda CH. Evaluation of the performance of the modified early warning score in a Brazilian public hospital. Revista Brasileira de Enfermagem. 2019;72:1428–1434. doi:10.1590/0034-7167-2017-0537
50. Janakaraj S. Effectiveness of education on modified early warning system for nurses. 2020.
51. Lainscak M, Blue L, Clark AL, et al. Self‐care management of heart failure: practical recommendations from the patient care committee of the heart failure association of the european society of cardiology. Eur J Heart Fail. 2011;13(2):115–126. doi:10.1093/eurjhf/hfq219
52. Khademian Z, Mohebi N, Khademian MH. Effects of training on knowledge and attitudes of coronary care unit nurses in relation to teamwork: a quasi-experimental study. J Vascular Nurs. 2020;38(3):132–136. doi:10.1016/j.jvn.2020.05.004
53. Brenner P. From Novice to Expert: Excellence and Power in Clinical Nursing Practice. River, NJ: Prentice Hall Upper Saddle; 2001.
54. Rickham P. Human experimentation. Code of ethics of the world medical association. Declaration Helsinki British Med J. 1964;2(5402):177.
55. National Commission for the Protection of Human Subjects. of B, Behavioral R. United States, the Belmont Report: Ethical Principles and Guidelines for the Protection of Human Subjects of Research. Vol. 2. Department of Health, Education, and Welfare, National Commission for the …; 1978.
56. Burger D, Jordan S, Kyriacos U. Validation of a modified early warning score‐linked Situation‐Background‐Assessment‐Recommendation communication tool: a mixed methods study. J Clin Nurs. 2017;26(17–18):2794–2806. doi:10.1111/jocn.13852
57. Eddahchouri Y, Koeneman M, Plokker M, et al. Low compliance to a vital sign safety protocol on general hospital wards: a retrospective cohort study. Int J Nurs Studies. 2021;115:103849. doi:10.1016/j.ijnurstu.2020.103849
58. Credland N, Dyson J, Johnson MJ. What are the patterns of compliance with Early Warning Track and Trigger Tools: a narrative review. Appl Nurs Res. 2018;44:39–47. doi:10.1016/j.apnr.2018.09.002
59. Nadr Ebraheim M, Karawan Sayed Sallam G, Samir AbdelHamid Ghait S, et al. Early Warning Score (EWS) Education: its effect on nurses’ performance regarding identification and response to clinical deterioration. Egy J Health Care. 2023;14(3):1140–1158. doi:10.21608/ejhc.2023.338898
60. Damayanti R, Trisyani Y, Nuraeni A. Effects of Early Warning Score (EWS) tutorial simulation on nurses. Knowledge Clin Performance Nurse Media J Nurs. 2019;9(2):231–241. doi:10.14710/nmjn.v9i2.24821
61. Mussa CC, Al-Raimi A, Becker EA. Predicting respiratory therapists’ intentions to use the modified early warning score by using an enhanced technology acceptance model. Respiratory Care. 2019;64(4):416–424. doi:10.4187/respcare.06428
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Assessment of Knowledge, Practice, and Associated Factors Towards Airway and Breathing Management Among Nurses Working in the Emergency Departments of Selected Public Hospitals in Addis Ababa, Ethiopia: A Cross-Sectional Study
Nigatu M, Debebe F, Tuli W
Open Access Emergency Medicine 2022, 14:235-247
Published Date: 27 May 2022
Improving Nurses Knowledge and Practices of Delirium Assessment at Mbarara Regional Referral Hospital: A Quasi Experimental Study
Baluku Murungi E, Niyonzima V, Atuhaire E, Nantume S, Beebwa E
Advances in Medical Education and Practice 2023, 14:313-322
Published Date: 30 March 2023
Knowledge, Attitude, and Practice of Insulin Pump Among Non-Endocrinology Nurses in South China

Mo C, Huang X, Lu X, Zhou Y, Su Y, Zhang H
Diabetes, Metabolic Syndrome and Obesity 2023, 16:3417-3423
Published Date: 30 October 2023
Knowledge and Practice Level of Nurses Towards Geriatric Care and Its Associated Factors in Selected Public Hospitals in Wolaita Zone, Southern Ethiopia 2022
Kebede C, Anjulo F, Meleku M, Dessalegn L, Geta T, Merkine M, Nigussie GB
Nursing: Research and Reviews 2024, 14:33-43
Published Date: 8 February 2024
Development and Effectiveness of a Central Venous Catheter Management Education Program for Nurses in Hematology-Oncology Wards
Park S, Kim J
Nursing: Research and Reviews 2026, 16:546043
Published Date: 5 February 2026