Back to Journals » Open Access Emergency Medicine » Volume 14
Assessment of Knowledge, Practice, and Associated Factors Towards Airway and Breathing Management Among Nurses Working in the Emergency Departments of Selected Public Hospitals in Addis Ababa, Ethiopia: A Cross-Sectional Study
Authors Nigatu M, Debebe F, Tuli W ![]()
Received 13 March 2022
Accepted for publication 23 May 2022
Published 27 May 2022 Volume 2022:14 Pages 235—247
DOI https://doi.org/10.2147/OAEM.S366218
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Mulachew Nigatu,1 Finot Debebe,2 Wagari Tuli2
1Department of Emergency, All Africa Leprosy, Tuberculosis, Rehabilitation, and Training Center Hospital, Addis Ababa, Ethiopia; 2Department of Emergency Medicine, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia
Correspondence: Wagari Tuli, Email [email protected]
Background: As airway issues or respiratory failures are the leading causes of death in the first hours after an injury, nurses’ understanding and practice of fundamental airway and breathing therapies remain “cornerstones” of competent emergency care. As a result, the goal of this study was to evaluate nurses’ airway and breathing management knowledge, practice, and associated factors in the emergency departments of selected governmental hospitals in Addis Ababa, Ethiopia.
Methods: During the study period of April 12 to April 30, 2021, a cross-sectional survey was conducted with a thorough enumeration of all respondents using the census method. The data were collected from the respondents using a self-administered and structured questionnaire. Data quality was ensured by pre-testing the tools and giving data collectors training. The data were analyzed using the SPSS version 25 program. The researchers used mean, frequency, bivariable, and multiple logistic regression analyses. Only P-values less than 0.05 were considered statistically significant.
Results: A total of 102 people took part in this study, with a 96.2% response rate. Females made up slightly more than half of the respondents 52.9%, and their ages ranged from 24 to 48 years old, with a mean age of 29.50 (SD ± 4.96). Only 45.1% of those polled were well versed in the emergency airway and breathing management. About 90.2% of the respondents had a BSc degree. At p< 0.05, having previously received airway and breathing management training was statistically correlated with knowledge.
Conclusion: Although many of the practice problems were correctly answered, the respondents in this study had insufficient knowledge of airway and breathing management. As a result, it is critical to give nursing training because it is strongly linked to the knowledge and practice of nurses.
Keywords: knowledge, practice, nurse, airway management, breathing management
Background
The airway connects the nose and mouth to the alveoli in the lungs, where oxygen (O2) and carbon dioxide (CO2) are exchanged naturally. Airway management is a technique, maneuver, or equipment used to maintain the patency of the airway so that normal physiological activities, such as gas exchange, can be accomplished.1 Manual ventilation may be required if a person’s O2 and CO2 exchange is inadequate. However, basic airway maneuvers to open the airway are typically enough to regulate or improve spontaneous air movements.2
As airway issues or respiratory failures are the leading causes of death in the first hours after an injury, the basic procedures remain the “cornerstones” of appropriate emergency care.3,4 Airway and breathing management require immediate attention, as patients may die if these actions are not taken. One of the most important emergency airway management procedures for keeping patients alive is airway maintenance without “endotracheal intubation”.5
Opening the airway with manual maneuvers such as head tilt - chin lift, jaw thrust, recovery positioning, keeping the airway open with devices such as oropharyngeal and nasopharyngeal airways, oxygen therapy, suctioning/removing secretion, and ventilation are all basic airway and breathing management. In the event of a foreign body obstruction, numerous treatments such as abdominal thrusts (Heimlich maneuver), chest thrusts, and back blows (slaps) can be used to manage the fundamental airway. The presence of arterial hypoxemia and tissue hypoxia is the most common reasons for supplementary oxygen. High-flow delivery systems (venture masks), low-flow delivery systems (nasal prong/cannula), basic masks, partial rebreathing masks, and Bag-Mask Ventilation are all options for delivering oxygen.2,5–9
In patients who are at risk of secretion, suctioning using large-bore suction catheters can help with emergency airway control. The bag valve mask, which was pioneered by anesthesiologists in the 1950s and 1960s and has saved many lives, takes first place in the revolution of airway management for substantial improvements in anesthesiology and resuscitation.7,8,10–13
In developed countries, well-organized Emergency Medical Service (EMS) systems have been shown to save lives that were previously at high risk of dying at the scene or while being transported to the hospital. However, in developing metropolitan cities such as Addis Ababa, Ethiopia, there is still a high rate of preventable morbidity and mortality. The main causes are a lack of a coordinated EMS system, a designated well-developed emergency center (EC), insufficient human and material resources to care for injured or acutely ill patients, insufficient medical training on triage and emergency management principles, and a lack of long-term funding for emergency care services.14,15
Previous studies have demonstrated inadequate fundamental airway and breathing management with wide variance between emergency departments, despite its clinical and research importance in the management of critically ill and injured patients.16–18 According to a Nepalese study, just 33% of health practitioners knew how to properly open the airway of an unresponsive injured victim. Similarly, an Egyptian study found that more than 85% of respondents could not name the first step in confirming a suspected airway obstruction.9,19
According to the authors’ knowledge, no study has been conducted specifically on nurses’ knowledge and practice of emergency airway and breathing management in our study areas, which is the most important in planning training for its use, differentiating, and preventing the factors linked to poor patient outcomes. As a result, the purpose of this study was to evaluate the knowledge, practice, and associated factors of airway and breathing management among nurses working in the emergency departments of selected public hospitals governed by the Addis Ababa Health Bureau (AAHB) in Addis Ababa, Ethiopia.
Objective
General Objective
To analyze nurses’ emergency airway and breathing management knowledge, practices, and associated factors in the emergency departments of selected public hospitals in Addis Ababa, Ethiopia.
Specific Objective
To assess knowledge of emergency airway and breathing management among nurses working in the emergency departments of selected public hospitals in Addis Ababa, Ethiopia.
To assess practice of emergency airway and breathing management among nurses working in the emergency departments of selected public hospitals in Addis Ababa, Ethiopia.
To find out what factors were linked to emergency airway and breathing management expertise among nurses working in the emergency departments of a few public hospitals in Addis Ababa, Ethiopia.
Materials and Methods
Study Area and Study Period
The research was conducted in Addis Ababa, Ethiopia’s capital city, at AAHB-managed public hospitals. AAHB was in charge of six public hospitals in Addis Ababa. Three of these hospitals were chosen at random for this investigation. Yekatit 12 Hospital, Zewditu Memorial Hospital, and Tirunesh Beijing Hospital are the hospitals in question. There are 44 nurses at Yekatit 12 Hospital; 45 nurses at Zewditu Memorial Hospital; and 17 nurses at Tirunesh Beijing Hospital. A total of 106 nurses were working in the emergency rooms of the three hospitals. The current research took place from April 12 to April 30, 2021.
Study Design
A cross-sectional survey study design was conducted to assess nurses´ knowledge, practice, and associated factors of airway and breathing management in the emergency departments of selected public hospitals in Addis Ababa, Ethiopia.
Population
Source Population
All nurses who were working at the emergency departments of government hospitals under the AAHB.
Study Population
All nurses who were working at the emergency departments of the three randomly selected governmental hospitals under AAHB.
Eligibility Criteria
Inclusion and Exclusion Criteria
Nurses working in the emergency departments of the participating hospitals who were available during the study period and had at least six months of experience had been included, while nurses who did not volunteer to participate in the study were omitted.
Sample Size Determination
There was no need to calculate the sample size because the total number of nurses working in the emergency departments of the three randomly selected hospitals was modest; therefore, all nurses who met the inclusion criteria were included in the study. A total of 102 people were included in the study.
Study Variables
Dependent Variables
Knowledge and practice of nurses toward emergency airway and breathing management were dependent variables of the study.
Independent Variables
Sociodemographic characteristics: age, sex, educational level, work experience, and previous emergency training were independent variables of the study.
Operational Definition
Airway and breathing management: Basic airway management knowledge and skills that include opening the airway, clearing secretion, O2 therapy, bag-mask ventilation, using devices to keep the airway open, and so on.6
Knowledge: The level of understanding of the different subjects regarding airway and breathing management. Good knowledge was defined as a score of greater or equal to the mean value of the knowledge questions, whereas poor knowledge was less than the mean value.
Practice: The necessary actions to be taken to help patients with emergency airway and breathing problems, like opening the airway for patients with trauma or non-trauma, applying maneuvers for choking patients, oxygen administration by bag valve masks for gasping patients, and so on.
Data Collection Tools and Procedures
After evaluating several studies, data was obtained from the study population using a standardized self-administered questionnaire15,20,21 based on the objectives intended for the study. The questionnaire is divided into three sections. Nurses’ sociodemographic features, knowledge of emergency airway and breathing management, and practice of emergency airway and breathing management were all examined. Age, sex, degree of schooling, work experience, and previous emergency-related training are among the sociodemographic questions. There are sixteen (16) multiple-choice questions in the knowledge section, each with one right answer. The correct answer received one point, while all other erroneous responses received zero points. The mean value for the knowledge questions was then determined, and respondents who scored greater or equal to the mean value were regarded to have strong knowledge of emergency airway and breathing management, while those who scored less than the mean value were judged to have poor knowledge. There are ten (10) multiple-choice questions in the practice questions about nurses’ emergency airway and breathing management skills. Descriptive statistics were used to summarize the data on nurse practice in the emergency airway and breathing management. Previous researchers examined the validity and reliability of the questionnaires, which were written in English. For this study, the questionnaire was pre-tested on 5% of nurses working in the emergency department of Menelik II hospital. Based on the results of the pretest, corrections were made to some of the questions by senior emergency physicians of Addis Ababa University. Three bachelors of science degree (BSC) nurses with prior expertise in data gathering were chosen and received a one-day training on the data collection process. For each hospital, a data collector was assigned, and all processes were done under the supervision of the lead investigator.
Data Quality Control
In addition to the training provided to data collectors, the primary investigator was reviewing how the data collectors were doing their jobs and supervising the activity on a daily basis during data collection. The lead investigator checked the completeness of questionnaires at the end of each data collection day.
Data Analysis
The information was double-checked for accuracy, coded, and entered into Epi Data version 3.1 before being transferred to the Statistical Package for Social Science (SPSS) version 25 for further analysis. For continuous variables, descriptive statistics such as mean and standard deviation were utilized, whereas, for categorical variables, frequency, and percentage distribution were used. The study’s findings were then arranged and presented, utilizing narratives, texts, tables, and graphs. The link between dependent and independent factors was demonstrated using bivariable and multivariable logistic regression models. To find variables associated with nurse knowledge and practice, all independent variables with p-values less than 0.25 in the bivariable logistic regression analysis were fitted into the multivariable logistic regression analysis. The strength of the connection was measured using the crude odds ratio (COR) and adjusted odds ratio (AOR) with corresponding 95% confidence intervals (CI). Finally, factors in the multivariable logistic regression were considered statistically significant if their P-values were less than 0.05.
Results
Socio-Demographic Characteristics of Respondents
A total of 102 nurses took part in the survey, with a 96.2% response rate, while four nurses were unavailable throughout data collection. More than half of the study participants (52.9%) were females, ranging in age from 24 to 48 years old, with a mean age of 29.50 (SD 4.96). The majority of the study participants, 92 (90.2%), had a BSc degree, and the majority of them, 74 (72.5%), had emergency job experience ranging from one to five years (Table 1). In terms of past emergency-related training, 53 (52%) of the respondents had had different training, while 49 (48%) had not received any emergency-related training, and 11.32% took other type of training lke infection prevention, and general training on covid (Figure 1).
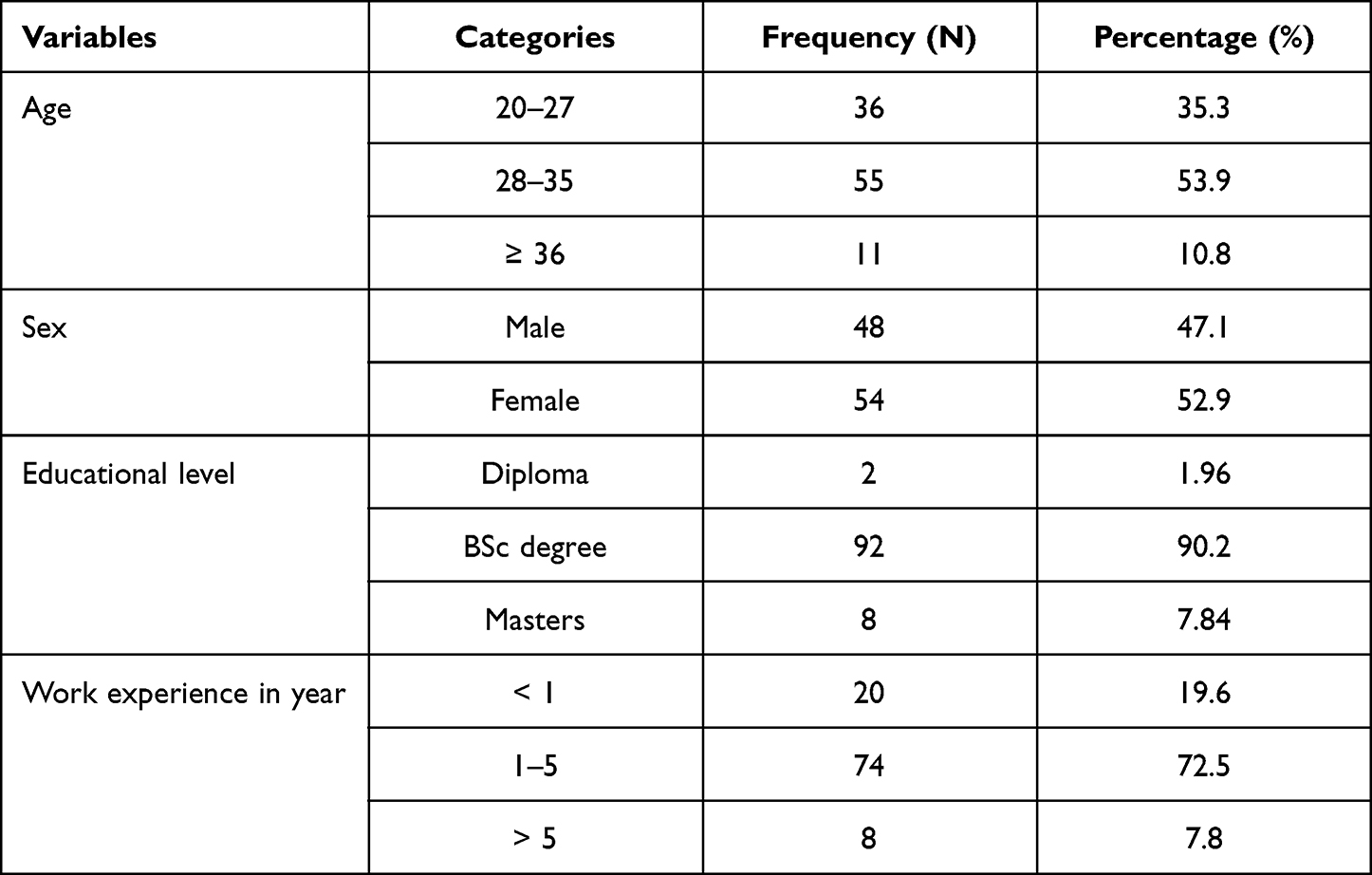 |
Table 1 Socio-Demographic Characteristics of Respondents, 2021 (N=102) |
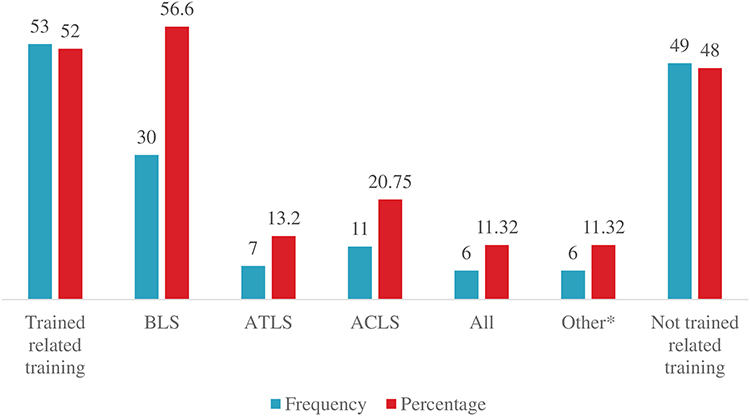 |
Figure 1 Status of the respondents on the emergency related training, 2021 (N=102). Abbreviations: BLS, basic life support; ATLS, advanced trauma life support; ACLS, advanced cardiac life support; Other*, training like infection prevention, general training on COVID-19, and soft ware training on patient data. |
Knowledge of Nurses on the Airway and Breathing Managements
To begin with, the mean value of knowledge questions was determined to be 9.44 (59%). Respondents who scored greater or equal to the mean value were considered knowledgeable about airway and breathing management. As a result, the participants’ overall knowledge of airway and breathing management was 46 (45.1%) (Figure 2). Respondent’s knowledge of the specific cases was variable. Seventy-five (73.5%) and 61 (59.8%) of respondents correctly identified the maneuvers used to open the airway with and without trauma suspicion (jaw thrust maneuver and head tilt-chin lift maneuver), respectively. Eighty-seven (85.3%) of the participants correctly identified difficulty speaking, breathing, or coughing as signs and symptoms of complete airway obstruction, and nearly all 98 (96.1%) of the participants correctly identified positioning a patient as a basic maneuver for airway and breathing management. Only 37 (36.3%) of the total respondents correctly identified endotracheal intubation as a non-basic airway device, and 37 (36.3%) correctly identified bag valve mask as a manual ventilation device that provides high oxygen concentration and artificial ventilation for someone with airway and breathing problems. The knowledge question with the fewest responses was “Not supraglottic airway,” which revealed that only 30.4% of the participants correctly answered that a bag valve mask is not a supraglottic airway (Table 2).
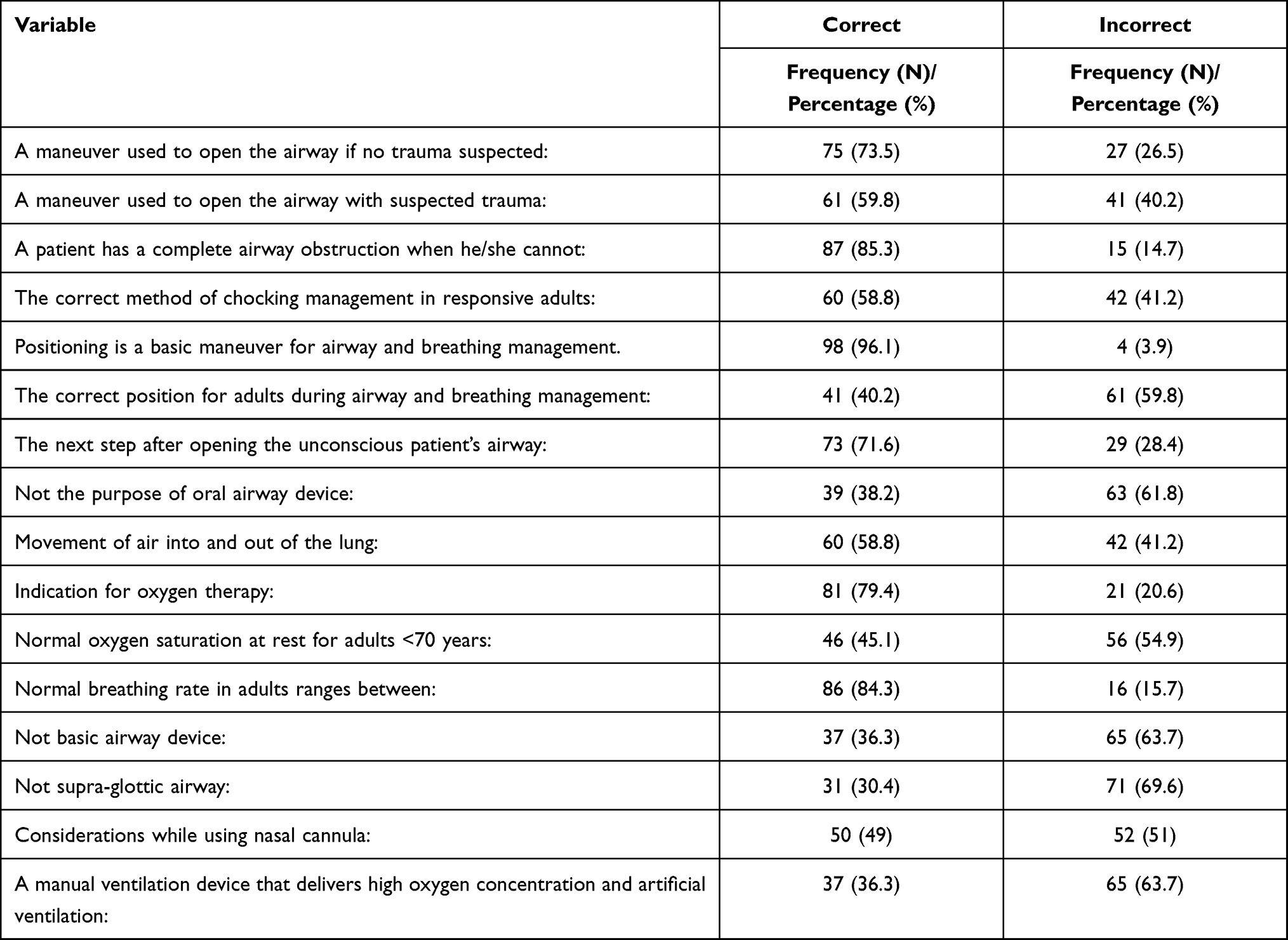 |
Table 2 Distribution of Responses on Knowledge Assessment of Airway and Breathing Management 2021 (N=102) |
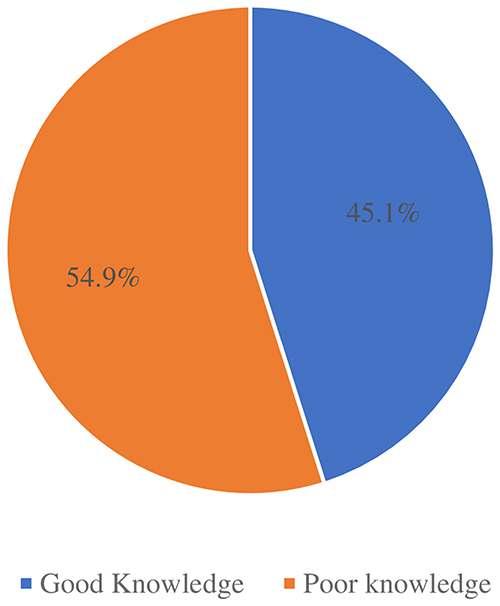 |
Figure 2 Overall level of knowledge of respondents, 2021 (N=102). |
Practice of Nurses on the Airway and Breathing Managements
As shown in Table 3, the proper action (jaw thrust) was chosen by 88 (86.3%) of the responders when opening the airway for a patient with a suspected neck injury. The activities to be done for a responsive patient displaying choking symptoms, before suctioning, and a comatose injured patient as a first action was properly answered by about 25 (24.5%), 49 (48.0%), and 74 (72.5%) of the respondents, respectively. When it came to appropriate nursing care during oxygen therapy, only 33 (32.4%) of the study participants were able to provide an accurate response. Only 30 (29.4%) of respondents correctly answered the question about using a face mask for a patient with airway and breathing problems, while the majority of 73 (71.6%) correctly answered the question about using an ambu bag for a patient with airway and breathing problems.
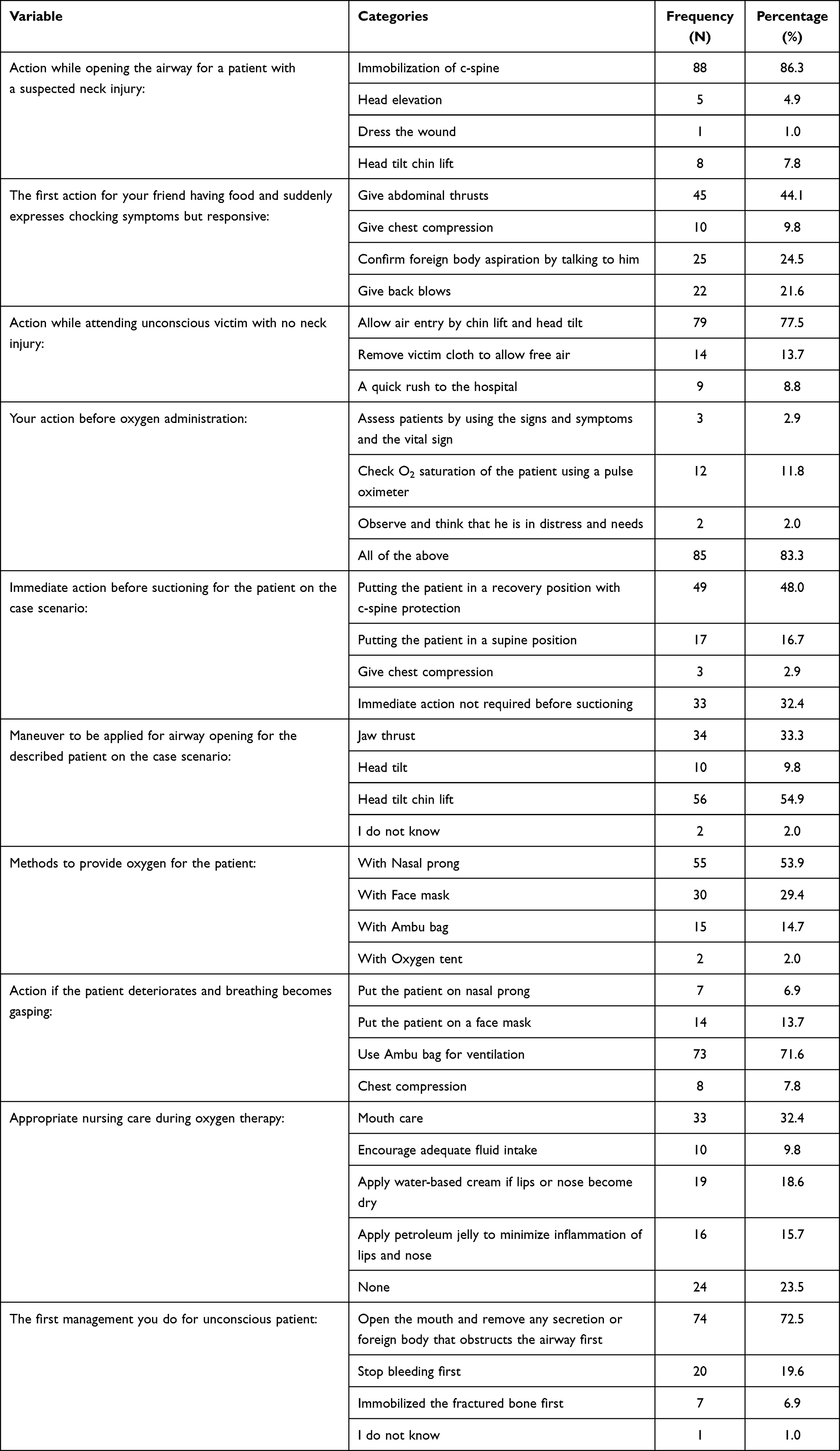 |
Table 3 Distribution of Responses on the Practice Assessment of Airway and Breathing Management, 2021 (N=102) |
Factors Affecting Knowledge of the Respondents
Bivariable logistic regression was used to establish the crude odds ratio of nurses’ strong understanding of airway and breathing management based on socio-demographic parameters such as age, sex, having received related training, emergency work experience, and educational level (Table 4). In bivariable logistic regression, only being trained in related training and job experience were significantly correlated with knowledge of airway and breathing management, with P = 0.029 and P = 0.075, respectively. Nurses who had been trained were 2.72 times more likely to be knowledgeable [COR = 2.72, 95% CI (1.11–6.67)] than those who had not been trained, and nurses with one to five years of emergency work experience were 2.54 times more likely to be knowledgeable [COR = 2.54, 95% CI (0.91–7.12)] than those with less than one year of work experience. Then, with a p-value, less than 0.25, the two variables of being trained in related training and having emergency job experience were included in multivariable logistic regression. In multivariate logistic regression, only individuals who had received related training were significantly correlated with knowledge of airway and breathing management with a p-value less than 0.05. As a result, nurses who had received relevant training were 2.78 times more likely to be informed than nurses who had not [AOR = 2.78, 95% CI (1.01–7.64)].
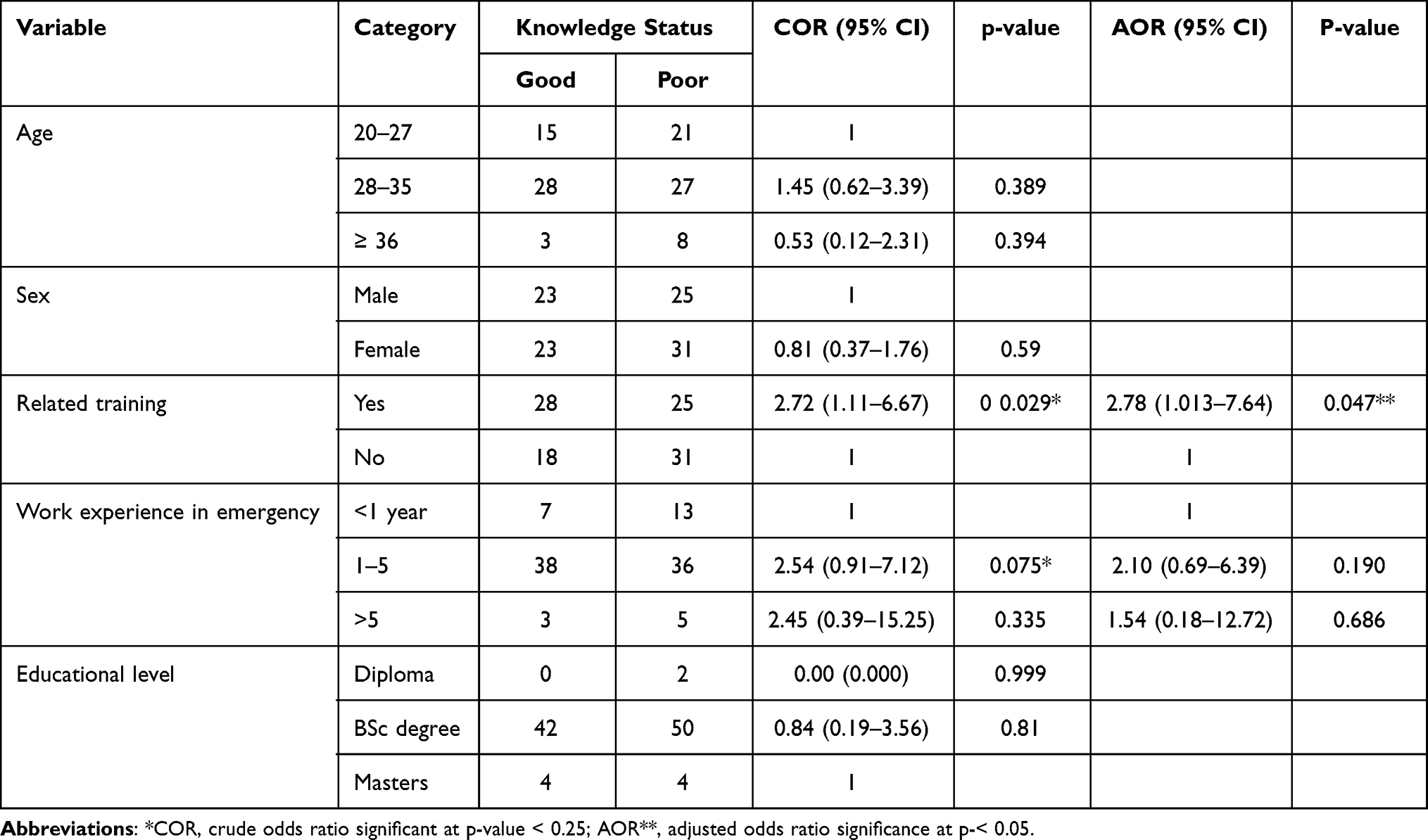 |
Table 4 Bivariable and Multivariable Analysis of Factors Affecting the Knowledge Towards Airway and Breathing Management 2021 (N=102) |
Discussion
Nurses are the frontline workers in emergency rooms, dealing with a variety of patients with a variety of issues, particularly those with airway and breathing problems that require immediate attention. Nurses’ knowledge and experience are critical in dealing with such issues. As a result, the goal of this study was to analyze nurses’ knowledge, practice, and associated factors related to emergency airway and breathing treatment in public hospitals in Addis Ababa, Ethiopia.
With a score of ≥ mean value of 59% on the knowledge questions, only 45.1% of the respondents had an overall good understanding of airway and breathing management. The findings were consistent with a study conducted across several departments at Jazan University in Saudi Arabia, which found that the majority of students lacked fundamental knowledge of airway and breathing management. However, the current study’s findings were lower than those of a study conducted in India, which revealed a 63% success rate. The writers, on the other hand, described this as an insufficient level of expertise. The disparity could be owing to the study participants, who in the Indian study were undergraduate dental students learning about airway-related diseases and their managements in their courses, whereas in our study, the participants were nurses working in hospitals.22,23
More than half of the study’s participants (52.0%) had received airway and breathing management training. This was in contrast to research conducted at Jazan University in Saudi Arabia, which revealed that 52.3% of the participants had received no training on airway and breathing management. The difference could be due to the fact that the participants in the Jazan University study came from a variety of departments, including health sciences and non-health departments such as engineering, computer science, and business administration, so they were not trained in specific emergency training.22,24
According to the findings of the current study, the vast majority of participants (85.3%) were aware of the symptoms of complete airway obstruction. Our findings compare favorably to those of research conducted in Ethiopia by Legese Mebrahtu (58.9%) and Tiruneh Tafere (22.65%).25,26 Furthermore, a study conducted in Gondar, Ethiopia, differed from this one in that 79.6% of study participants were aware of the signs of airway blockage.27 The discrepancy could be related to the study’s utilization of a variety of health providers, as well as the study’s setting and study period. However, the current study’s findings are remarkably identical to those of Gangadevi Nandasena’s study, which found that 84.3% of the study subjects had knowledge of blocked airway care.28,29
A small but vocal majority in this study, 73.5% of participants correctly identified the procedure performed to open the airway for a patient who has no worry of neck damage. Our findings are similar to those reported in studies by Gondar Comprehensive Hospital in Ethiopia and Ali M. Alabdali, who found that 71.7% and 69.4% of respondents, respectively, were aware of airway opening maneuvers.27,30
When a patient’s airway cannot be protected, airway and breathing management equipment must be employed.25 According to the current study, just 36.3% of respondents recognized the use of an Ambu bag. This was refuted by research conducted in Rwanda, which found that 92.2% of study participants correctly answered questions on how to use the device.15 The discrepancy might be due to the fact that every health professional in our country Ethiopia are un familiar with airway and breathing management because the emergency department was newly emerged in our country. So, many of our study participants were unable to recognize the use of Ambu bag during airway and breathing management. Another prospective study conducted at Nikoukari hospital, a teaching hospital located in Tabriz, Iran showed that most residents who took traditional instructions regarding airway management faced difficult ventilation and intubation; but they improved this gap after rotating of anesthesiology rotation.31 This could also be supported by another study conducted at Nikoukari hospital.32
Only 38.2% of the participants in this study were able to correctly answer the question about why they needed to use an oral airway device. This contrasted with a study conducted in Rwanda, which found that 86.3% of study participants were aware of the objective of using an oral airway device.15 According to a Turkish study, only 7.7% of respondents were able to correctly attach nasal airway devices while regulating their airways and breathing.33 The explanation, in our opinion, could be due to the low value placed on such critical emergency medical equipment.
In multivariable logistic regression, the socio-demographic information being trained on related training on airway and breathing management was statistically connected with the respondents’ knowledge at a p-value less than 0.05, with p = 0.047 and [AOR = 2.783, 95% CI (1.013–7.645)]. The findings of this study are consistent with those of a study conducted in Gondar, Ethiopia, and Rwanda, which found that training improved respondents’ understanding of emergency treatment [AOR: 2.76, 95% CI (1.40–5.42)] and (Chi2 = 12.632, P = 0.006), respectively.15,24,27
The current study’s 86.3% finding is nearly identical to findings from studies conducted in Ethiopia and Rwanda, which revealed that a large majority of respondents, 88.3% and 96.1%, respectively, gave the correct response to the question, “What action should be taken while opening the airway for a patient with a suspected neck injury?” immobilizing the cervical spine by using the jaw thrust maneuver during airway and breathing management.15,26 In contrast to this study, another one conducted in Nepal found that just 33% of volunteers were able to open the injured patient’s airway.33 The explanation for the disparity could be attributed to the fact that the Nepalese study used volunteers who did not all work in the same field.
Only 24.5% of survey participants were aware of the first action that should be taken for a victim who suddenly displayed a sign of choking while eating. The majority of trial participants (71.6%) were able to provide ventilation using an Ambu bag. This is a significant difference from a study conducted in Botswana, which found that 48.2% of respondents were unable to deliver ventilation using an Ambu bag.34 The reason for this could be due to the fact that the study subjects in Botswana were district hospital nurses, and during the management of any emergency situations, the focus should be given to breathing before taking time for any system adjustments. Because oxygen treatment is one of the most important and fundamental abilities in the management of breathing, nurses should be familiar with indications, safe delivery techniques, and the amount of oxygen to be provided during the procedure. If oxygen therapy is chosen, the appropriate delivery device should be employed.20,28,34
This study has its own strength and limitations. As strength, the study tried to find the gaps in knowledge and practice towards airway and breathing management among nurses working in the emergency department which will serve as a source of information for further study. The limitations of this study were: the study used a cross-sectional study design which does not show the cause and effect association; the attitude aspect of respondents towards airway and breathing management was not included in this study even though it is very important for exercise, and the study did not use observation for practical assessment questions rather it used only theoretical information.
Conclusion
Finally, the goal of this research was to assess the nurses’ knowledge and practice in the three hospitals’ emergency departments, as well as the factors that influence airway and breathing care. According to the findings of this study, nurses working in emergency rooms lacked a basic understanding of airway and breathing treatment. Participation in related training was found to be strongly linked to nurses’ expertise. As a result, all nurses working in emergency departments of hospitals in Addis Ababa, Ethiopia, should get in-service training on basic life support.
Abbreviations
AAHB, Addis Ababa Health Bureau; ACLS, advanced cardiac life support; AOR, adjusted odds ratio; ATLS, advanced trauma life support; BLS, basic life support; BSC, bachelor of science degree; CI, confidence interval; CO2, carbondioxide; COR, crude odds ratio; EC, emergency center; EMS, emergency medical service; IRB, institutional review board; O2, oxygen, SD, standard deviation; SPSS, statistical package for social science.
Data Sharing Statement
All the data used to support the findings of this study are found in the hands of the corresponding author.
Ethical Considerations
Ethical clearance was obtained from both Addis Ababa University, College of Health Sciences, Department of Emergency Medicine, and the AAHB Institutional Review Board (IRB). The cooperative letter was written to each hospital’s administration for the activity. The purpose and data collection procedure of the study were communicated with the concerned body of the institutions. Permission was obtained from the relevant personnel in charge of the hospitals. Formal permission was secured from each hospital before distribution of the questionnaires and respondents were informed verbally to identify their willingness to respond to the questionnaires. Finally, written consent was obtained from the respondents who had participated in the study, and the confidentiality of the participants was kept throughout the study by not writing their names on the questionnaire.
Acknowledgments
First and foremost, we would like to express our gratitude to Addis Ababa University, College of Health Sciences, Department of Emergency Medicine, and Addis Ababa Health Bureau for their assistance in obtaining approval. Second, we praised the leadership of each institution, as well as the data collectors and participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was funded by Addis Ababa University, College of Health Sciences.
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. Elkarta E, Eldegwy M. Airway management in critical settings. In: Special Considerations in Human Airway Managements. IntechOpen; 2020.
2. Davies JD, Costa BK, Asciutto AJ. Approaches to manual ventilation Discussion. Respir Care. 2014;59(6):810–824. doi:10.4187/respcare.03060
3. Getahun N. Assessment of Knowledge, Attitude and Practices of First Aid Service Provision Associated with Road Traffic Accidents Among Taxi Drivers in Addis Ababa. Ethiopia: Addis Ababa University; 2015.
4. Teshale AA, Alemu ZA. Knowledge, attitude and practice of first aid and factors associated with practice among taxi drivers in Addis Ababa, Ethiopia. Ethiop J Health Dev. 2017;31(3):200–207.
5. Roberts JR, Hedges JR. Roberts and Hedges’ Clinical Procedures in Emergency Medicine E-Book. Elsevier Health Sciences; 2013.
6. Reardon R, Mason P, Clinton J. Basic airway management and decision making. Clin Procedures Emerg Med. 2014;6:39–61.
7. Srinivasan AP, Albalawe MA, Issrani R, Patil SR, Prabhu N, Siddanna S. Awareness, knowledge, and attitude of Saudi students towards basic life support: a Cross-Sectional Study. Pesquisa Brasileira em Odontopediatria e Clínica Integrada. 2021;21:45.
8. Veronese J-PT. An assessment of theoretical knowledge and psychomotor skills of basic life support cardio-pulmonary resuscitation provision by emergency medical services in a province in South Africa. University of Cape Town; 2015.
9. Roshana S, Batajoo K, Piryani R, Sharma M. Basic life support: knowledge and attitude of medical/paramedical professionals. World J Emerg Med. 2012;3(2):141. doi:10.5847/wjem.j.issn.1920-8642.2012.02.011
10. Matioc AA. An Anesthesiologist’s perspective on the history of basic airway management: the “modern” era, 1960 to present. Anesthesiology. 2019;130(5):686–711. doi:10.1097/ALN.0000000000002646
11. Alfakey M, Alkarani A. Students’ knowledge and attitudes toward basic life support. Int J Eval Res Educ. 2021;10(3):871–877.
12. Azlan NZ, Noor NHM, Othman N. Knowledge, attitude and awareness of basic life support among health sciences university students. Int J Care Scholars. 2021;4(Supplementary1):4–12.
13. Khedher YZ, Shawwa L, Alamri AA, Farraj MM, Bayoumi ME. Knowledge and attitude of basic life support among medical students at King Abdul-Aziz University. Egypt J Hosp Med. 2017;69(8):3066–3076. doi:10.12816/0042857
14. Germa F, Bayleyegn T, Kebede T, Ducharme J, Bartolomeos K. Emergency medicine development in Ethiopia: challenges, progress and possibilities. African J Emerg Med. 2013;3(1):3–9. doi:10.1016/j.afjem.2012.08.005
15. Nshutiyukuri C. Assessment of nurse’s knowledge, attitude and practice in emergency care of road traffic accidents victims at three selected Rwanda Hospitals. University of Rwanda; 2017.
16. Kelkay M, Kassa H, Birhanu Z, Amsalu S. A cross sectional study on knowledge, practice and associated factors towards basic life support among nurses working in Amhara region referral hospitals, northwest Ethiopia. Hos Pal Med Int J. 2018;2(2):123–130.
17. Irfan B, Zahid I, Khan MS, et al. Current state of knowledge of basic life support in health professionals of the largest city in Pakistan: a cross-sectional study. BMC Health Serv Res. 2019;19(1):1–7. doi:10.1186/s12913-019-4676-y
18. Kassa C, Bilale A. Basic life support knowledge and its associated factors among a non-medical population in Gondar Town, Ethiopia. Open Access Emerg Med. 2020;2:323.
19. Ghanem E, Elgazar M, Oweda K, et al. Awareness of basic life support among Egyptian medical students; a cross-sectional study. Emergency. 2018;6:1.
20. Rutto J, Chepchirchir A, Odero T. Nurse’s knowledge, attitude and practice on the initial management of acute poisoning among adult casualties: study at Kenyatta National Hospital, Kenya; 2012.
21. Tenaw Z, Siyoum M, Tsegaye B, Werba TB, Bitew ZW. Health professionals job satisfaction and associated factors in Ethiopia: a systematic review and meta-analysis. Health Services Res Manage Epidemiol. 2021;8:23333928211046484. doi:10.1177/23333928211046484
22. Ahmad A, Akhter N, Mandal RK, et al. Knowledge of basic life support among the students of Jazan University, Saudi Arabia: is it adequate to save a life? Alexandria J Med. 2018;54(4):555–559. doi:10.1016/j.ajme.2018.04.001
23. Shree Y, Kumar K, Ganapathy D. Awareness of basic life support among dental students. researchgate. net; 2019. Available from: https://www.researchgate.net/profile/KiranPandurangan2/publication/339873903Awarenessofbasiclifesupportamongdentalstudents/links/5e69b30e458515c5de628420/Awarenessofbasiclifesupportamongdentalstudents.pdf.
24. Yunus M, Mishra A, Karim HMR, Raphael V. Knowledge, attitude and practice of basic life support among junior doctors and students in a tertiary care medical institute. Int J Res Med Sci. 2015;3644–3650. doi:10.18203/2320-6012.ijrms20151416
25. Mebrahtu L. Assessment of knowledge attitude and practices of military personnel regarding first aid measures in northern command 21st division. Addis Ababa University; 2014.
26. Taye TT. Assessment of knowledge, attitude and practice of first aid associated with fighting accidents among community police officers in Addis Ababa City, Ethiopia. Addis Ababa University; 2017.
27. Mersha AT, Egzi AHKG, Tawuye HY, Endalew NS. Factors associated with knowledge and attitude towards adult cardiopulmonary resuscitation among healthcare professionals at the University of Gondar comprehensive specialized hospital, Northwest Ethiopia: an institutional-based cross-sectional study. BMJ Open. 2020;10(9):e037416. doi:10.1136/bmjopen-2020-037416
28. Nandasena G, Abeysena C. Knowledge, attitudes and skills of doctors, nurses and emergency medical technicians in pre-hospital care and emergency medicine who accompany patients in ambulances which arrive at the National Hospital of Sri Lanka; 2018.
29. Alsayil SN, Alzahran S, Alhawiti W. Awareness of basic life support among medical and nursing students at Tabuk University. Basic Res J Med Clin Sci. 2016;5(3):53–57.
30. Alqurashi AI. Attitude and awareness toward heart attack symptoms and lifesaving actions among population of western region, KSA. Middle East J Fam Med. 2020;7(10):42.
31. Soleimanpour H, Gholipouri C, Panahi JR, Afhami MR, Ghafouri RR, Golzari SE. Role of anesthesiology curriculum in improving bag-mask ventilation and intubation success rates of emergency medicine residents: a prospective descriptive study. BMC Emerg Med. 2011;11:8. doi:10.1186/1471-227X-11-8
32. Soleimanpour H, Panahi JR, Mahmoodpoor A. Digital intubation training in residency program, as an alternative method in airway management. Pak J Med Sci. 2011;27:401–404.
33. Gok F, Kılıcaslan A, Topal A, Yavsan D, Yosunkaya A. An assessment of the current knowledge of nurses, staffed in intensive care units, about airway management and basic life support. J Chest Dis Crit Care Med. 2014;1:56–60. doi:10.15197/sabad.4.1.09
34. Uwineza Didi V. Knowledge, attitudes and practice among nurses toward oxygen administration to the critically ill patients at UTHK. University of Rwanda; 2017.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Knowledge and Practice of Wound Care and Associated Factors among Nurses Working in South Wollo Zone Government Hospitals, Ethiopia
Tegegne B, Yimam F, Mengesha Yalew Z, Wuhib M, Mekonnen L, Asmamaw Yitayew Y, Ademe S, Tsegaye D, Eshetie Y, Chanie M
Chronic Wound Care Management and Research 2022, 9:1-11
Published Date: 20 July 2022
Improving Nurses Knowledge and Practices of Delirium Assessment at Mbarara Regional Referral Hospital: A Quasi Experimental Study
Baluku Murungi E, Niyonzima V, Atuhaire E, Nantume S, Beebwa E
Advances in Medical Education and Practice 2023, 14:313-322
Published Date: 30 March 2023
Knowledge, Attitude, and Practice of Insulin Pump Among Non-Endocrinology Nurses in South China

Mo C, Huang X, Lu X, Zhou Y, Su Y, Zhang H
Diabetes, Metabolic Syndrome and Obesity 2023, 16:3417-3423
Published Date: 30 October 2023
Knowledge and Practice Level of Nurses Towards Geriatric Care and Its Associated Factors in Selected Public Hospitals in Wolaita Zone, Southern Ethiopia 2022
Kebede C, Anjulo F, Meleku M, Dessalegn L, Geta T, Merkine M, Nigussie GB
Nursing: Research and Reviews 2024, 14:33-43
Published Date: 8 February 2024
Current Perspectives, Practices, and Barriers Faced by Community Pharmacists Regarding Pharmaceutical Care Services for Diabetes Mellitus in the United Arab Emirates
Jairoun AA, Al-Hemyari SS, Shahwan M, Jairoun SA, Alorfi NM, Zyoud SH, Suliman AA, Shahwan MK, Alnuaimi G, Shahwan M, Al-Qirim T, El-Dahiyat F
Journal of Multidisciplinary Healthcare 2024, 17:2563-2576
Published Date: 23 May 2024