Back to Journals » Psychology Research and Behavior Management » Volume 19
Dual Mediating and Moderating Roles of Hope in the Association Between Marital Satisfaction and Post-Traumatic Growth Among Chinese Breast Cancer Patients: A Latent Profile Analysis
Authors Gu ZH ![]() , Bao JX, Tan Y, Li MY
, Bao JX, Tan Y, Li MY ![]()
Received 30 March 2026
Accepted for publication 26 May 2026
Published 3 June 2026 Volume 2026:19 612295
DOI https://doi.org/10.2147/PRBM.S612295
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Zhi Hui Gu, Ji Xiang Bao, Yang Tan, Meng Yao Li
Department of Social Medicine, School of Health Management, China Medical University, Shenyang, People’s Republic of China
Correspondence: Meng Yao Li, Email [email protected]
Purpose: This study aimed to identify latent profiles of post-traumatic growth (PTG) among Chinese breast cancer patients and to explore the dual mediating and moderating roles of hope in the association between marital satisfaction (MS) and PTG, so as to clarify the psychological mechanism underlying marital relationship and positive psychological adaptation after cancer.
Patients and Methods: A cross-sectional survey was conducted on 421 breast cancer patients from the Breast Surgery Department of Anshan Cancer Hospital, Liaoning, China. Participants completed the Herth Hope Index, Marital Adjustment Scale, and Post-traumatic Growth Inventory. Latent profile analysis (LPA) was used to classify PTG sub-types; hierarchical regression, bootstrap resampling and simple slope tests were applied to examine the mediating and moderating effects. Statistical analyses were performed using Mplus 8.3 and IBM SPSS 26.0.
Results: Three latent PTG subgroups were identified: PTG-resistance (20.5%), PTG-slow growth (27.6%), and PTG-healthy growth (51.9%). Hope exerted a partial mediating effect on the relationship between MS and PTG, accounting for 29.5% of the total effect. Also, hope significantly moderated this association and served as a weakening moderator (ΔR2=0.139, P< 0.001). The positive linkage stronger among those with lower hope levels. Patients with high hope relied less on marital relationship quality to achieve positive psychological growth and maintained stable PTG independently.
Conclusion: Hope acts as both partial mediator and weakening moderator. Low-hope patients are more affected by MS, whereas high-hope patients maintain steady PTG via internal psychological resources. This PTG sub-type classification combined with hope-related psychological mechanisms facilitates targeted and individualized psychological intervention strategies for breast cancer patients.
Keywords: post-traumatic growth, marital satisfaction, hope, breast cancer, mediating and moderating role, latent profile analysis
Introduction
Breast cancer is the most commonly diagnosed cancer in women. Globally, there are 2.3 million new cases of female breast cancer, accounting for 23.8% of all new cancer cases in women.1 Breast cancer is also one of the most common cancer types in China.2 In 2022, there were approximately 357,200 newly diagnosed female breast cancer cases in China, accounting for 15.59% of the total new cancer cases.3 Post-traumatic growth (PTG) refers to profound positive psychological transformation attained through active struggle with traumatic events, manifesting as positive changes beyond pre-trauma levels.4 PTG serves as a core indicator of positive psychological adaptation in BC patients, with key manifestations including improved interpersonal relationships, enhanced appreciation for life, strengthened personal strength, elevated spiritual growth, and exploration of new life possibilities.5,6 PTG can effectively alleviate negative emotions such as anxiety and depression, reduce physical and mental distress, and enhance self-confidence and self-efficacy.4,6 High levels of PTG are closely associated with positive coping styles, resilience, and healthy lifestyle behaviors, which further improve long-term quality of life and mental health outcomes.5–7
Available evidence indicates that PTG is prevalent and nearly ubiquitous among BC patients.5 Most existing studies evaluate PTG in BC patients by comparing scale total and sub-scale scores and classifying PTG levels via score cut-offs, treating patients as a homogeneous group.8–10 However, PTG cannot be simply defined by scale scores alone, as it exhibits obvious intrinsic heterogeneity with a predominant moderate growth pattern.11,12 Latent Profile Analysis (LPA) can identify distinct PTG sub-types based on multidimensional responses and accurately reflect population heterogeneity.13 While several studies have examined PTG latent profiles in BC patients, relevant evidence remains scarce with no consensus on sub-type categorization, profile traits and mechanisms. However, most existing evidence is derived from Western populations, and studies focusing on Chinese breast cancer patients remain limited. In particular, few studies have adopted a localized perspective to explore PTG heterogeneity and its psychological mechanisms within Chinese cultural contexts, where family-centric values, marital relationships, and collective coping patterns play uniquely critical roles. Furthermore, the dynamic associations among MS, hope, and PTG have not been fully clarified, and the potential mediating and moderating mechanisms underlying these relationships remain under explored, leading to an insufficient understanding of how positive psychological resources function in Chinese patients. This study therefore employed LPA to identify PTG profiles, explore their distribution and heterogeneity, overcome the drawbacks of traditional score-based assessment, and inform targeted psychological interventions.
Marital satisfaction (MS) is a critical psychosocial protective factor for women with breast cancer. It promotes positive adaptation by relieving stress, improving supportive communication and illness acceptance, and mediates the relationship between dyadic coping and post-traumatic growth (PTG).14–16 Dyadic coping interventions can enhance PTG by increasing MS.17 Higher concordance in MS between patients and partners predicts fewer psychological problems, better decision-making satisfaction, optimized coping, and improved social and occupational functioning.18–22 Poor MS is an independent risk factor for cancer recurrence, metastasis, and mortality.23,24 Moreover, higher MS fosters positive PTG patterns and serves as a key protective factor for PTG.25,26 In conclusion, MS is essential for disease adaptation and serves as a core foundation for PTG in breast cancer patients. Improving marital quality effectively promotes positive psychological changes and long-term health adjustment.
Beyond social environmental factors, hope serves as a key positive psychological resource for PTG in patients with breast cancer. It can independently and positively predict PTG and acts as a core bridge linking traumatic experiences to positive psychological transformation.27,28 Hope is conceptualized as an intrinsic motivational force that guides life orientation, a source of optimistic confidence, and a resilient belief that drives individuals to pursue goal attainment with a positive mindset.29 Various psychological interventions, such as mindfulness-based cognitive therapy and psycho educational interventions, can effectively improve patients’ level of hope and further promote PTG.30,31 Hope plays an important mediating role between PTG and illness adaptation, and its positive correlation with PTG is stronger than that of resilience.32,33 PTG can also enhance hope in reverse, forming a mutually reinforcing positive cycle between the two; meanwhile, a high level of hope is a crucial protective factor facilitating the occurrence and development of PTG.34,35
Despite the above progress, critical research gaps remain. First, most studies ignore the cultural specificity of Chinese patients, lacking a localized perspective to explain how marital relationships and hope jointly influence PTG. Second, the integrated model of “MS - hope - PTG” has rarely been verified in Chinese breast cancer samples. Third, the potential moderating role of hope in the linkage between MS and PTG remains unclear under Chinese cultural contexts. Therefore, this study aims to fill these gaps by adopting a localized perspective, exploring PTG latent profiles, and clarifying the mediating and moderating roles of hope in the relationship between MS and PTG among Chinese breast cancer patients.
Theoretical Basis
Snyder’s Hope Theory posits that hope consists of two interrelated dimensions: agency thinking and pathways thinking.36 Agency thinking refers to an individual’s internal motivation and belief in pursuing goals, while pathways thinking reflects one’s perceived capacity to generate effective strategies for achieving those goals.36 Hope is a key positive psychological trait that can be enhanced by external environmental support, which in turn drives positive psychological behaviors and adaptive developmental outcomes. MS constitutes a critical form of positive external support within intimate relationships for patients; harmonious and satisfying marital interactions continuously foster both agency and pathways thinking, thereby elevating overall hope levels.37,38 In turn, higher hope motivates patients to confront their illness trauma, regulate negative emotions, and proactively seek positive changes, ultimately facilitating PTG.32–35
The Stress Buffering Theory suggests that external support resources exert a buffering effect on the impact of stressful events, with internal positive psychological resources acting as a “psychological buffer” that alters the strength and effectiveness of external factors on physical and mental health outcomes.39 Under varying levels of internal psychological resources, the positive benefits derived from the same external support differ significantly.39 A breast cancer diagnosis represents a major negative life stressor, and marital satisfaction serves as an intimate external support resource to mitigate illness-related stress; hope functions as an internal psychological buffer that moderates this relationship.37,39
Based on the above theoretical frameworks and empirical evidence, we propose the following hypotheses:
Hypothesis 1: Distinct latent profiles of PTG exist among Chinese breast cancer patients. Hypothesis 2: Hope mediates the association between MS and PTG among breast cancer patients. Specifically, higher MS is linked to greater hope, which in turn promotes higher levels of PTG. Hypothesis 3: Hope plays a significant moderating role in the relationship between MS and PTG, such that the positive association between MS and PTG differs significantly across levels of hope.
Methods
Study Design
A cross-sectional, observational, questionnaire-based study was conducted in the Department of Breast Surgery, Anshan Cancer Hospital, Liaoning, China, between January 2020 and December 2020. Convenience sampling was used to recruit participants. Eligible patients were informed about the purpose, procedure, and confidentiality of the study. All participants provided written informed consent prior to data collection. Data collection was performed via face-to-face interviews with assistance from trained investigators. Patients first completed the questionnaires independently; investigators remained on-site to provide explanations when needed and to check for missing or invalid responses immediately after completion. Any missing items were clarified and supplemented on the spot to ensure data quality.
Study Sample
A total of 500 questionnaires were distributed, and 421 valid questionnaires were included in the final analysis, yielding an effective response rate of 84.2%, which meets the recommended sample size requirements for LPA (≥300)40 and mediation/moderation analyses (≥250–300)41 according to prior methodological studies.
Inclusion Criteria: (1) female patients aged ≥18 years; (2) pathologically confirmed breast cancer at any disease stage; (3) had completed primary surgery and were currently receiving adjuvant radiotherapy or chemotherapy; (4) able to communicate clearly, comprehend the questionnaire, and complete all assessments independently with assistance.
Exclusion Criteria: (1) pre-existing severe mental disorders, cognitive impairment, or intellectual disability before cancer diagnosis; (2) severe comorbidities or other malignant tumors that would severely affect psychological assessment.
Measurements
Demographic and Clinical Characteristics
Demographic variables included age (“≤45”, “46–55”, and “≥56”), residence (“city” and “rural”), education level (“middle school or under”, “senior high school” and “undergraduate or above”), per capital monthly income (“≤3000”, “3001–5000” and “≥5001CNY”). Clinical variables included cancer stages (“0/I”, “II” and “III/IV”), tumor size (“<3cm” and “≥3cm”). Fertility status, recurrence status and contralateral mastectomy were categorized as “yes” and “no”.
Post-Traumatic Growth Inventory (PTGI)
PTG was measured using the 21-item Chinese version of the PTGI, which includes five sub-scales: Relating to Others, New Possibilities, Personal Strength, Appreciation of Life, and Spiritual Change.42 Items were rated on a 6-point Likert scale (0 = “not at all” to 5 = “extremely”). Total scores ranged from 0 to 105, with higher scores indicating greater PTG. The Cronbach’s α in this study was 0.959.
Marital Adjustment Scale (MAS)
Marital satisfaction was assessed using the 15-item MAS.43 Total scores range from 2 to 158; scores ≥100 indicate normal marital adjustment. Higher scores reflect better marital satisfaction. The reliability and validity of the scale in Chinese populations have been tested.40 The Cronbach’s α for MAS in this study was 0.692.
Herth Hope Index (HHI)
Hope level was measured using the 12-item HHI, covering three dimensions: positive attitude, positive action, and intimate connection with others.44 Items were scored on a 4-point Likert scale (1–4). Total scores range from 12 to 48, with higher scores representing higher hope. The Cronbach’s α was 0.813.
Statistical Analysis
LPA was performed using Mplus 8.3 to identify distinct PTG subgroups based on the 21 individual item scores of the PTGI. Model selection was based on: Akaike Information Criterion (AIC), Bayesian Information Criteria (BIC), and Adjusted Bayesian Information Criteria (aBIC) (lower values indicate better fit);45 Entropy (values closer to 1 indicate clearer classification);46 LMRT (Lo-Wendell-Rubin Test) and BLRT (Bootstrap Likelihood Ratio Test) (P<0.05 indicates better fit than the k-1 profile model);47 Posterior probabilities (>0.70 for each class) and theoretical interpretability. Class membership was determined using the maximum posterior probability rule.
IBM SPSS Statistics 26.0 is used for analyzing the mediating and moderating effects. First, hierarchical multiple regression was conducted to examine hope as a potential mediator or moderator. The conditional process model (Model 4 for mediation, Model 1 for moderation) was used to test the hypothesized effects in a unified analytical framework. Mediation effect: The indirect effect was tested using 5000 bootstrap samples. A significant mediation was confirmed if the BCa 95% CI did not include 0.48 Moderation effect: Simple slope analysis was performed to clarify the nature of the interaction.49 Two-tailed tests were used, and P< 0.05 was considered statistically significant.
Results
Latent Profile Analysis of PTG
The fitting indices of the five models are shown in Table 1. The P values of LMR in 4-profile and 5-profile pattern model are >0.05, indicating that it should be excluded. According to the judgment criteria, if a model has higher entropy and lower AIC, BIC, and aBIC and achieves significant LMR and BLRT, the model has a greater fit. Therefore, based on the above criteria, combined with the sample percentage and practical significance, the 3-profile model is selected as the optimal models in this study.
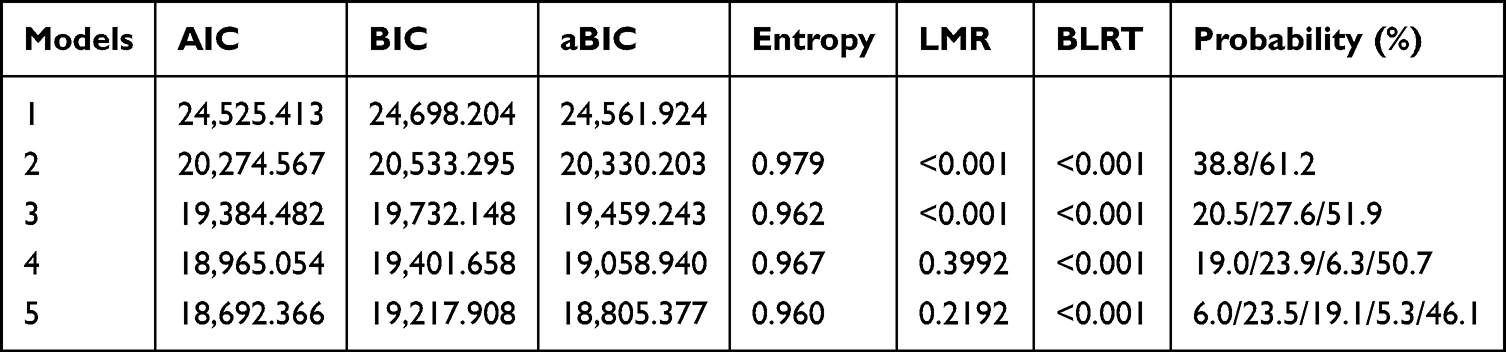 |
Table 1 Fit Indices of Each Model |
Naming of Latent Profiles of PTG
Figure 1 shows these three profiles of PTG. Low-level group means PTG scores are the lowest (mean=45.642) and maintain a stable level, hence it is named the “PTG-Resistance group” (n=86, 20.5%). Moderate-level group means PTG scores are moderate (mean=61.903) and show high fluctuation, hence it is named the “PTG-Slow growth group” (n=117, 27.6%). High-level group means PTG scores are the highest (mean=80.444) and show little fluctuation, hence it is named the “PTG-Health group” (n=218, 51.9%).
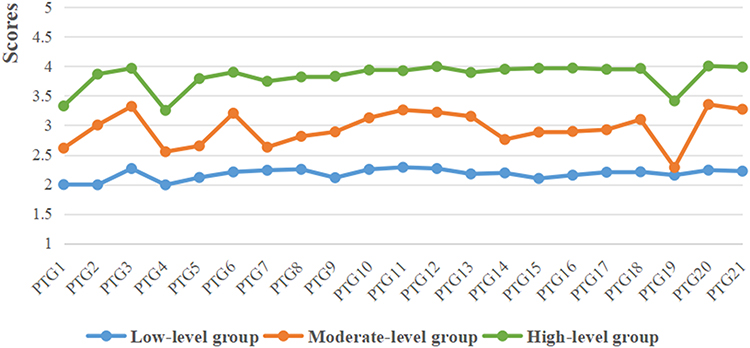 |
Figure 1 Latent profiles of PTG among BC patients. Notes: PTG1-PTG3 for appreciation of life; PTG4-PTG8 for new possibilities; PTG9-PTG12 for personal power; PTG13-PTG14 for spiritual change; PTG15-PTG21 for relating to others. |
Descriptive Analyses
Table 2 presented the demographic and clinical characteristics of the group differences in PTG. The mean age was 54.3±10.3. Patients who had children reported higher PTG scores than those who never had a child (P<0.05). Patients with an income of 3001–5000 (CNY) had higher PTG levels than others (P<0.05). No clinical characteristics were found to be significantly associated with PTG.
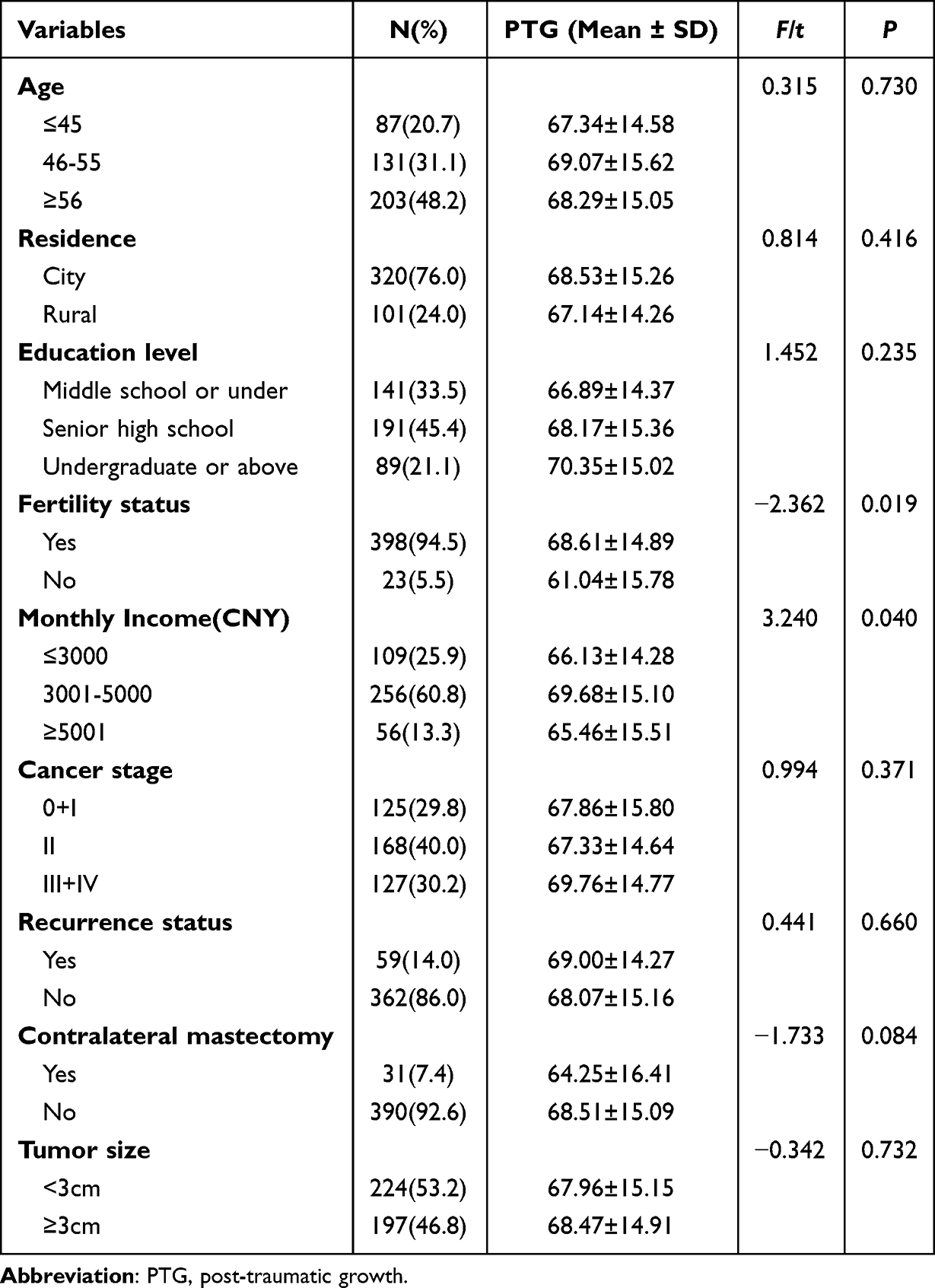 |
Table 2 Demographic and Clinical Characteristics of PTG Among BC Patients |
Correlations Between PTG, Hope and MS
Table 3 presented the correlation coefficients between variables. Hope (r=0.486, P<0.001) and MS (r =0.450, P<0.001) were positively correlated with PTG in our study.
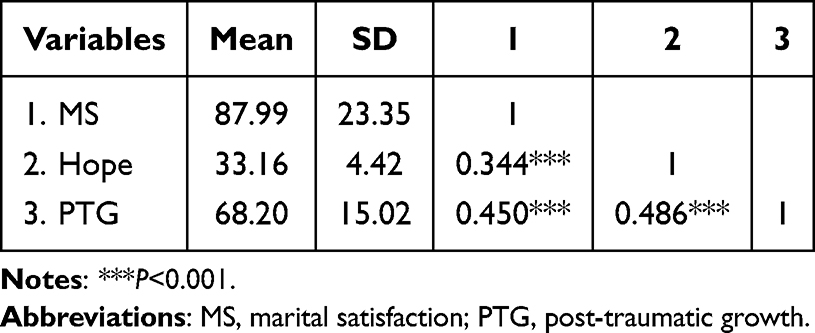 |
Table 3 Pearson Correlations Between the Study Variables |
Mediation Analysis
Table 4 presented the outcomes of the hierarchical linear multiple regression analysis. MS was positively correlated with PTG (β=0.448, P<0.001; Step 2), and hope was positively associated with PTG (β=0.380, P<0.001 Step 3).
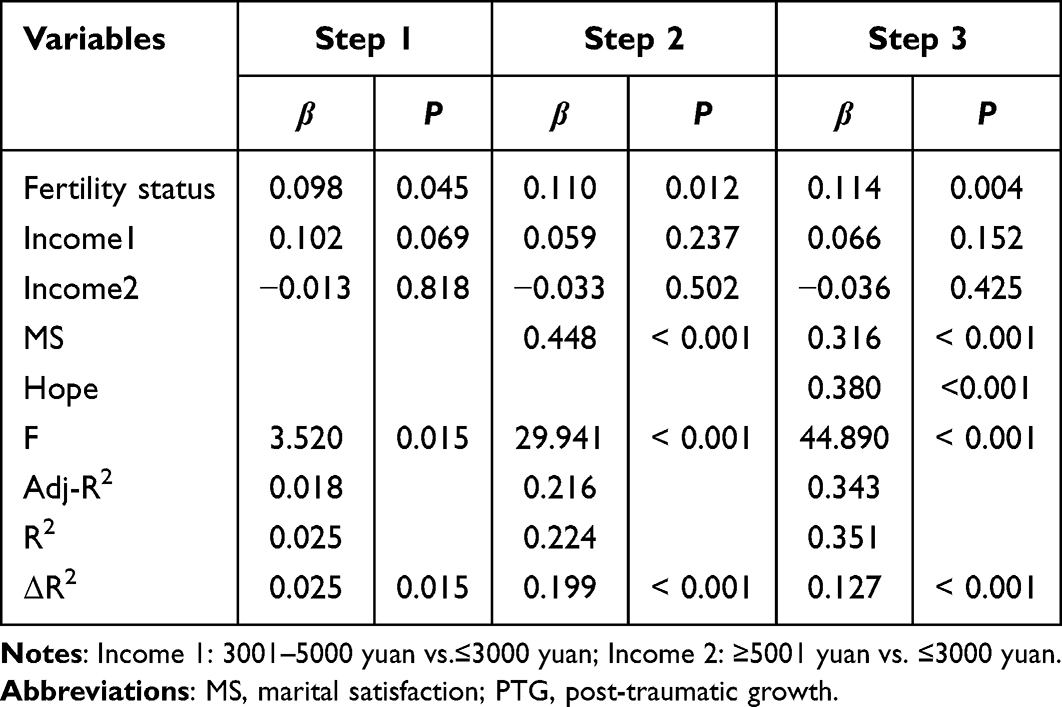 |
Table 4 The Result of Hierarchical Linear Multiple Regression Analysis of PTG |
The results of the mediation analysis were presented in Table 5. The total effect of MS on PTG (“c path”) was initially evaluated. MS was a positive association with PTG (c=0.288, P<0.001). Then, the path coefficient of indirect effect (a*b product) of MS on PTG via hope was 0.085 (BCa 95%CI: 0.059,0.115). The confidence interval for indirect effect did not contain zero, which suggested that hope played a mediating role between MS and PTG. The total effect of MS on PTG was 0.288 (P<0.001), and the direct effect was 0.204 (P<0.001), manifesting that hope had a partially mediating effect in the association between MS and PTG.
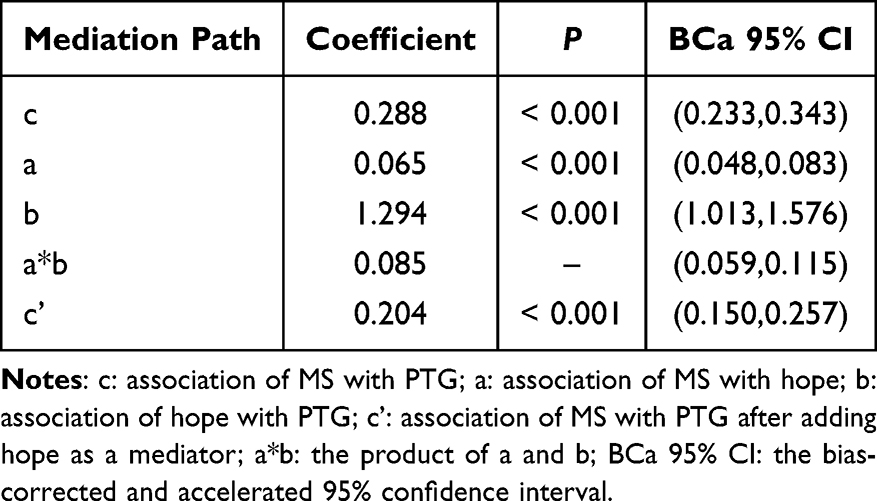 |
Table 5 The Results of the Mediation Analysis |
To understand the effect size of the mediating path, we applied the formula (a*b)/c to calculate the proportion of the total effect of the MS on PTG that was mediated by hope. The proportion of mediation of hope was 29.5%. The mediating model and path coefficients were shown in Figure 2.
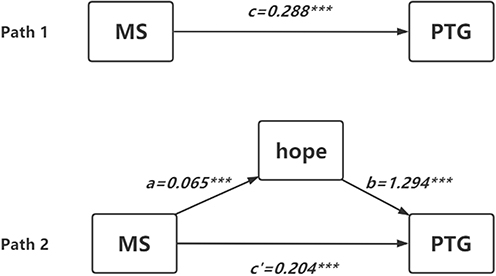 |
Figure 2 Model of mediating role of hope in the relationship between MS and PTG. Abbreviations: MS: marital satisfaction; PTG: post-traumatic growth. Notes: c: association of MS with PTG; a: association of MS with hope; b: association of hope with PTG; c’: association of MS with PTG after adding hope as a mediator.***P<0.001. |
Moderation Model
Table 6 presented the results of hierarchical linear multiple regression analysis which was applied to test the effect of moderation, that is, to test the existence of interactions. The first layer controlled two general demographic data of fertility status and income (CNY), the second layer added centralized MS, and the third layer added centralized hope and interactions of MS and hope. The results indicated that the hope had a significant moderating effect on the association between MS and PTG among BC patients after controlling covariates (β=-0.108, P=0.008).
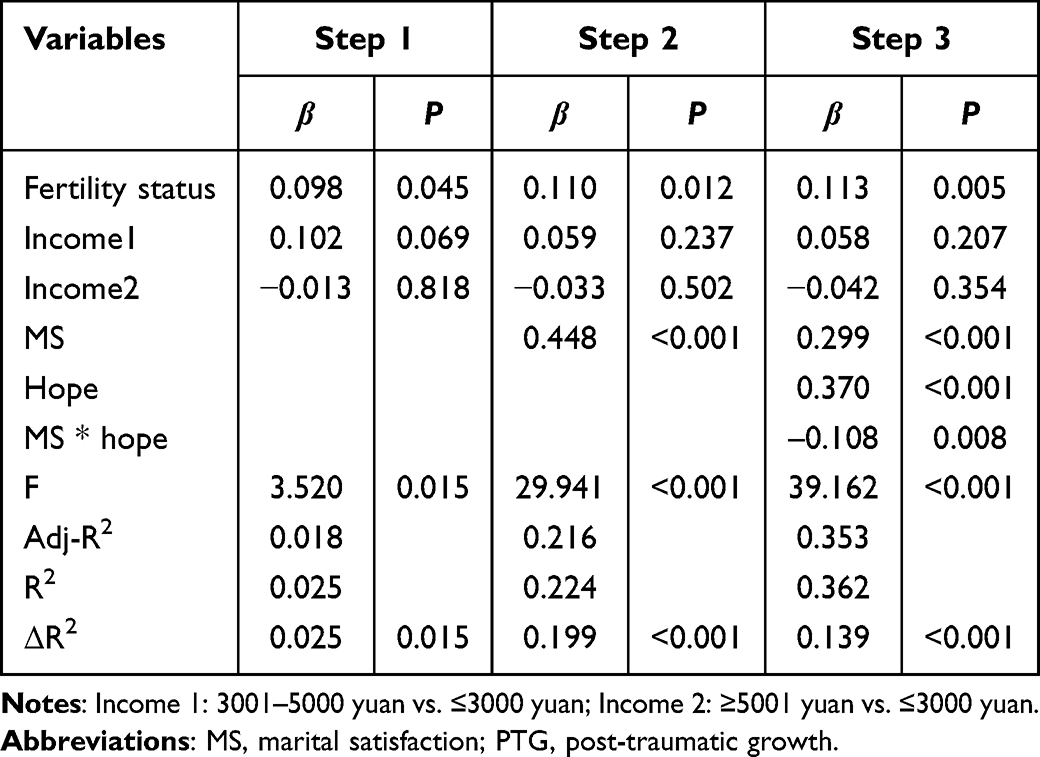 |
Table 6 The Moderating Effects of Hope on the Relationship Between PTG and MS |
Figure 3 shows the simple slopes plot illustrating how hope level moderates the link between MS and PTG among breast cancer patients. The findings confirmed hope level exerts a significant moderating influence on the correlation between MS and PTG. Subsequent simple slope analyses demonstrated that MS is positively correlated with PTG across all hope levels. In patients with low hope, the positive association between MS and PTG is more prominent, with a steeper simple slope of 12.252. In those with high hope, this positive association is relatively milder, with a gentler simple slope of 5.883. Given identical MS levels, patients with higher hope always attain higher PTG scores than those with lower hope. In addition, rising MS contributes to a more notable elevation in PTG among patients low in hope.
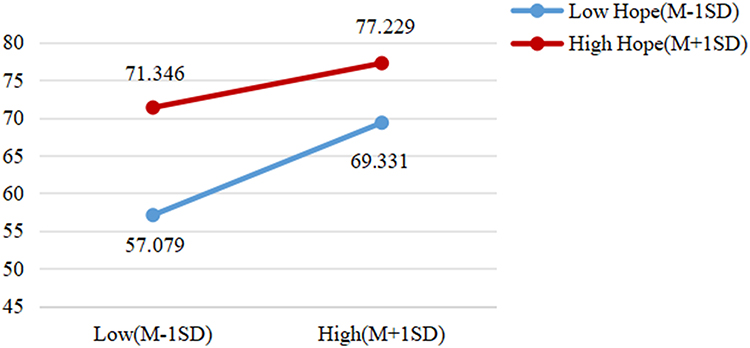 |
Figure 3 Moderating effect of hope on the relationship between MS and PTG in BC patients. Abbreviations: MS, marital satisfaction; PTG, post-traumatic growth. |
Discussion
Latent Profiles of PTG in Breast Cancer Patients
In this study, PTG among breast cancer patients was classified into three distinct sub-types: PTG-Health group, PTG-Slow growth group, and PTG-Resistance group, which was consistent with previous research.12 The PTG-Health group accounted for the largest proportion. Patients in this subgroup typically exhibited strong psychological adaptability and achieved substantial positive changes during their struggle with the disease, such as a greater appreciation for life and enhanced inner personal growth.50 The PTG-Slow growth group represented a transitional stage of psychological transformation. Although these patients displayed a certain degree of positive growth, their psychological status remained unstable. Since no obvious negative psychological symptoms were observed, clinical staff should provide targeted psychological support to consolidate and further elevate their level of positive growth. Patients in the PTG-Resistance group struggled to achieve positive psychological changes and showed obvious stagnation in personal growth. With greater psychological vulnerability, this group urgently requires systematic and professional psychological interventions to break through barriers to growth and achieve positive psychological transformation.6,51 The identification of such heterogeneous patterns in PTG fully highlights the critical practical significance of implementing individualized psychological intervention strategies in clinical oncology practice.
The Mediating Role of Hope Between MS and PTG
Mediation analysis revealed a significant total effect of MS on PTG, which was consistent with extensive previous evidence.52 This finding indicates that positive marital support has direct correlation with the development of PTG among patients with breast cancer.52 Further analyses indicated that hope played a partial mediating role in this relationship. A harmonious and stable marital relationship creates a safe and supportive emotional atmosphere, helps patients build confidence in recovery, and thereby enhances their level of hope.53 As a core positive psychological resource, hope enables individuals to engage in cognitive reappraisal of traumatic events, reframe negative experiences caused by the disease, and reconstruct their cognitive schema. These psychological processes represent key mechanisms underlying the development of PTG.28 Taken together, a high-quality marital relationship not only fosters PTG directly but also exerts an indirect effect by elevating hope. These findings clearly elucidate the internal psychological pathway through which marital emotional support helps patients cultivate psychological resilience and achieve positive psychological growth.
The Moderating Role of Hope Between MS and PTG
Hope exerted a significant negative moderating effect on the association between MS and PTG in patients with breast cancer. Specifically, MS showed a stronger positive association with PTG among patients with lower levels of hope, whereas the facilitative effect of MS gradually weakened as hope increased. These findings suggest an obvious compensatory effect of marital support on PTG: when patients lack sufficient internal positive psychological resources and struggle to cope with disease-related trauma on their own, a high-quality marital relationship and spousal support become the most central and irreplaceable external emotional foundation for promoting positive psychological transformation.54,55 Previous studies have also confirmed that social support and intimate relationships exert stronger protective effects on PTG among individuals with insufficient internal psychological resources, greater psychological stress, and more prominent negative emotions. Conversely, the beneficial effect of external support becomes relatively weaker when individuals possess abundant internal positive resources.6,56 For breast cancer patients, hope serves as a vital internal psychological resource and interacts with spousal support in relation to PTG. When hope is deficient, the compensatory value of spousal support becomes particularly prominent, as it effectively compensates for the lack of internal psychological resources, helps patients complete cognitive reconstruction and psychological adaptation, and ultimately facilitates the emergence and development of PTG.
Further analyses showed that the strength of the positive association between MS and PTG was attenuated among patients with high levels of hope. Although MS still exerted a positive influence, its effect size was significantly reduced. Patients with high hope possess mature and stable internal cognitive and emotional regulation capacities, allowing them to accomplish trauma adaptation and psychological growth through their own internal resources, thereby reducing their dependence on the quality of marital relationships.57,58 Even at the same level of MS, patients with high hope consistently achieved higher PTG scores than those with low hope. This result further confirms that hope is an independent protective factor for mental health that can directly enhance positive psychological growth without relying on marital status.
In summary, hope functioned as a weakening moderator in this study: as hope increased, the impact of MS on PTG gradually decreased. The psychological status of patients with low hope is more susceptible to changes in marital relationships, whereas patients with high hope can maintain stable positive psychological growth even under poor marital conditions.
Clinical Implications
Based on the three heterogeneous sub-types of PTG in breast cancer patients in this study: The PTG-Health group requires only regular follow-up to maintain positive mental status. The PTG-Slow growth group needs routine psychological support, cognitive guidance, and couple communication interventions to consolidate growth. The PTG-Resistance group urgently needs targeted interventions focusing on hope promotion, meaning reconstruction, and improved marital support. This classification enables rapid psychological screening and risk stratification, supporting differentiated interventions and improving precision and resource efficiency. Combined with the dual mediating and moderating role of hope, interventions can be optimized: enhancing marital support for low-hope patients, and maintaining internal psychological resources for high-hope patients. The sub-types based and mechanism-targeted precise intervention model provides a new practical reference for individualized psychosocial care in breast cancer.
Limitations
First, this was a cross-sectional study, unable to infer causality. Participants had inconsistent time since diagnosis and surgery, and we did not collect data on surgical type, breast reconstruction status and marriage duration. These unadjusted confounding factors may introduce potential bias to the results. Second, the Cronbach’s α of the Marital Adjustment Scale was 0.692, slightly below the conventional standard. Though acceptable, the relatively low internal consistency may affect measurement stability and relevant result interpretation. Third, single-center convenience sampling may cause selection bias and restrict the generalizability of findings.
Conclusion
This study confirmed that hope exerts both partial mediating effect and buffering moderating effect on the relationship between MS and PTG among Chinese breast cancer patients. Meanwhile, obvious individual heterogeneity in PTG was verified via LPA. The findings suggest that comprehensive psychological interventions focusing on enhancing hope level and improving marital support can effectively facilitate positive psychological adjustment and improve overall psychological adaptation among breast cancer patients.
Data Sharing Statement
The datasets generated and/or analysed during the current study are not publicly available due the data also forms part of an ongoing study but are available from the corresponding author on reasonable request.
Ethics Approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of China Medical University. Personal privacy was protected when handling personal data, and we kept individual records completely secret. Informed consent was obtained from all individual participants included in the study.
Acknowledgment
The authors would acknowledge the services of staffs in the Department of Breast Surgery, Anshan Cancer Hospital, Liaoning, China, who helped to get the written informed consent about the conduct of this survey and distribute the questionnaires to the patients with breast cancer.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the [National Natural Science Foundation of China] under Grant [number 71904204].
Disclosure
The authors reported no conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–12. doi:10.3322/caac.21834
2. Han B, Zheng R, Zeng H, et al. Cancer incidence and mortality in China, 2022. J Natl Cancer Cent. 2024;4(1):47–53. doi:10.1016/j.jncc.2024.01.006
3. Sun K, Zhang B, Lei S, et al. Incidence, mortality, and disability-adjusted life years of female breast cancer in China, 2022. Chin Med J. 2024;137(20):2429–2436. doi:10.1097/CM9.0000000000003278
4. Duan X, Yang X, Duan Y, et al. Post-traumatic growth experiences of breast cancer patients and spouses: a dyadic qualitative study. Support Care Cancer. 2025;33(7):643. doi:10.1007/s00520-025-09704-2
5. Gahane V, Deshpande Y, Goyal A. Correlates of post-traumatic growth for patients with breast cancer: a systematic review and meta-analysis. J Health Psychol. 2026;31(6):2203–2224. doi:10.1177/13591053251375310
6. Nisiraiou A, Bozas A, Kyrou D, et al. Post-Traumatic Growth in Adult Cancer Survivors: a Scoping Review of Psychological Factors, Predictors, and Interventions. Int J Psychol. 2025;60(5):e70097. doi:10.1002/ijop.70097
7. Cheng L, Gao H, Zhou Z, et al. Perceived stress and post-traumatic growth in breast cancer patients: a moderated mediation model. BMC Psychol. 2026;14(1):220. doi:10.1186/s40359-026-03971-2
8. Song D, Bai Y, Liu Y, et al. Patterns and predictors of symptom burden and posttraumatic growth among patients with cancer: a latent profile analysis. Support Care Cancer. 2024;32(6):363. doi:10.1007/s00520-024-08577-1
9. Liu J, Griva K, Mahendran R. Latent profiles of fear of cancer recurrence and associations with physical and mental health outcomes. Ann Behav Med. 2023;57(9):743–752. doi:10.1093/abm/kaad023
10. He C, Wu C, He Y, et al. Characteristics and influencing factors of social isolation in patients with breast cancer: a latent profile analysis. Support Care Cancer. 2023;31(6):363. doi:10.1007/s00520-023-07798-0
11. Arefian M, Yang X, Duan Y, et al. A latent profile analysis of post-traumatic growth in spouses of breast cancer patients. Front Public Health. 2025;13:1634910. doi:10.3389/fpubh.2025.1634910
12. Guo K, Li H, Du W, et al. Patterns and predictors of post-traumatic growth and fear of disease progression in breast cancer patients: a latent profile analysis. Front Psychiatry. 2025;16:1604787. doi:10.3389/fpsyt.2025.1604787
13. Wang Y, Kim E, Yi Z. Robustness of latent profile analysis to measurement noninvariance between profiles. Educ Psychol Meas. 2022;82(1):5–28. doi:10.1177/0013164421997896
14. Shrout MR, Renna ME, Leonard MJ, et al. Couples in breast cancer survivorship: Daily associations in relationship satisfaction, stress, and health. Compr Psychoneuroendocrinol. 2024;20:100261. doi:10.1016/j.cpnec.2024.100261
15. Krok D, Telka E, Moroń M. Marital satisfaction, partner communication, and illness acceptance among couples coping with breast cancer: a dyadic approach. Psychooncology. 2023;32(8):1240–1247. doi:10.1002/pon.6174
16. Suo R, Zhang L, Tao H, et al. The effects of dyadic coping and marital satisfaction on posttraumatic growth among breast cancer couples. Support Care Cancer. 2021;29(9):5425–5433. doi:10.1007/s00520-021-06121-z
17. Wang Y, Zhang J, Wang S, et al. Feasibility and preliminary efficacy of a systematic transaction model-guided dyadic coping nursing intervention for patients with breast cancer and their spousal caregivers: a pilot study. Asia Pac J Oncol Nurs. 2024;12:100621. doi:10.1016/j.apjon.2024.100621
18. Sohn KJ, Kim SH, Lee H, et al. Factors affecting return to work in breast cancer survivors in Korea: a cross-sectional study. Womens Health Nurs. 2024;30(4):277–287. doi:10.4069/whn.2024.12.10
19. Vachon EA, Krueger E, Haggstrom DA, et al. The association between relationship satisfaction concordance and breast cancer survivors’ physical and psychosocial well-being. Healthcare. 2024;12(2):134. doi:10.3390/healthcare12020134
20. Seng MM, Adarkwah yiadom S, Otto-Dobos LD, et al. The role of oxytocin in mediating the relationships between social factors and chemotherapy-associated cognitive decline in female patients with breast cancer. Psychoneuroendocrinology. 2025;176:107428. doi:10.1016/j.psyneuen.2025.107428
21. Wang Y, Zhang Q, Wang X, et al. Current status and influencing factors of participating satisfaction during surgical treatment decision-making among breast cancer patients with immediate breast reconstruction. Eur J Oncol Nurs. 2023;66:102402. doi:10.1016/j.ejon.2023.102402
22. Wypych-ślusarska A, Ociepka S, Krupa-Kotara K, et al. Ways of coping with stress in women diagnosed with breast cancer: a preliminary study. Healthcare. 2025;13(6):609. doi:10.3390/healthcare13060609
23. Yuan L, Cai H, An W, et al. Associations between marital quality and the prognosis of breast cancer in young Chinese women: 10.3-year median follow-up. Chin Clin Oncol. 2023;12(5):51. doi:10.21037/cco-23-63
24. Shrout MR, Madison AA, Renna ME, et al. The gut connection: intestinal permeability as a pathway from breast cancer survivors’ relationship satisfaction to inflammation across treatment. Brain Behav Immun. 2022;100:145–154. doi:10.1016/j.bbi.2021.11.012
25. Kokou-Kpolou CK, Adansikou K, Park S, et al. Prolonged grief and posttraumatic growth among middle-aged and older widowed persons: a latent class analysis and testing for the role of social support. Death Stud. 2022;46(6):1401–1413. doi:10.1080/07481187.2021.1978115
26. Benedetti MG, Tarricone I, Monti M, et al. Psychological well-being, self-esteem, quality of life and gender differences as determinants of post-traumatic growth in long-term knee rotationplasty survivors: a cohort study. Children. 2023;10(5):867. doi:10.3390/children10050867
27. Ofei SD, Teye-Kwadjo E, Amankwah-Poku M, et al. Determinants of post-traumatic growth and quality of life in Ghanaian breast cancer survivors. Cancer Invest. 2023;41(4):379–393. doi:10.1080/07357907.2023.2181636
28. Corn BW, Feldman DB. Hope as a bridge to post-traumatic growth. Support Care Cancer. 2024;33(1):10. doi:10.1007/s00520-024-09063-4
29. Richardson AL, Long LJ, Gallagher MW. Hope and anxiety: a meta-analytic review. J Clin Psychol. 2026;82(3):227–247. doi:10.1002/jclp.70068
30. Arefian M, Asgari-Mobarake K. Mindfulness-integrated cognitive behavioral therapy reduces pain and psychological distress, and improves equanimity, hope and post-traumatic growth during breast cancer treatment: a pilot randomized controlled trial. Eur J Oncol Nurs. 2025;76:102881. doi:10.1016/j.ejon.2025.102881
31. Arefian M, Asgari-Mobarakeh K. Psychoeducational intervention for pain, psychological distress, hope, and post-traumatic growth among breast cancer patients during chemotherapy: a pilot randomized controlled trial. Pain Manag Nurs. 2024;25(5):e355–e366. doi:10.1016/j.pmn.2024.04.012
32. Wang Y, Song Z, Wei L, et al. The mediating role of psychological capital between post-traumatic growth and uncertainty in illness among patients with Parkinson’s disease. Geriatr Nurs. 2023;50:194–202. doi:10.1016/j.gerinurse.2023.01.014
33. Senger AR, McGrew SJ, Gallagher MW, et al. Associations of resilience and hope with mental and physical health among firefighters. J Clin Psychol. 2023;79(9):2124–2136. doi:10.1002/jclp.23534
34. Karaaslan Eser A, Avci Isik S, Ercivan S. The chain mediating effect of illness acceptance, body compassion, and post-traumatic growth on hope in cancer patients: a multicenter serial mediation analysis. Eur J Oncol Nurs. 2026;81:103151. doi:10.1016/j.ejon.2026.103151
35. Baník G, Dědová M, Vargová L. Cancer-related posttraumatic growth and posttraumatic stress: how are they connected and what are their correlates? Support Care Cancer. 2022;30(10):8183–8192. doi:10.1007/s00520-022-07252-7
36. Jing Y, Hu H. Effect of Snyder’s hope theory-based nursing intervention on patients with breast cancer. Rev Esc Enferm USP. 2025;59:e20240305. doi:10.1590/1980-220X-REEUSP-2024-0305en
37. Rock EE, Steiner JL, Rand KL, et al. Dyadic influence of hope and optimism on patient marital satisfaction among couples with advanced breast cancer. Support Care Cancer. 2014;22(9):2351–2359. doi:10.1007/s00520-014-2209-0
38. Sun Y. Psychological capital and subjective well-being: a multi-mediator analysis among rural older adults. BMC Psychol. 2025;13(1):315. doi:10.1186/s40359-025-02407-7
39. Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psychol Bull. 1985;98(2):310–357. doi:10.1037/0033-2909.98.2.310
40. Tein JY, Coxe S, Cham H. Statistical power to detect the correct number of classes in latent profile analysis. Struct Equation Model. 2013;20(4):640–657. doi:10.1080/10705511.2013.824781
41. Fritz MS, Mackinnon DP. Required sample size to detect the mediated effect. Psychol Sci. 2007;18(3):233–239. doi:10.1111/j.1467-9280.2007.01882.x
42. Dong L, Hu Y, Xu GH. Reliability and validity of the Chinese version of post-traumatic growth inventory scale in breast cancer survivors. J Nurs Sci. 2013;28:21–23. doi:10.3870/hlxzz.2013.22.021
43. Locke H, Wallace K. General marital satisfaction and adjustment scales. In: Fredman N, Sherman R, editors. The Handbook of Measurements for Marriage and Family Therapy. New York: Brunner-Mazel; 1997.
44. Herth K. Abbreviated instrument to measure hope: development and psychometric evaluation. J Adv Nurs. 1992;17(10):1251–1259. doi:10.1111/j.1365-2648.1992.tb01843.x
45. Liu Q, Charleston MA, Richards SA, et al. Performance of akaike information criterion and Bayesian information criterion in selecting partition models and mixture models. Syst Biol. 2023;72(1):92–105. doi:10.1093/sysbio/syac081
46. Larose C, Harel O, Kordas K, et al. Latent class analysis of incomplete data via an entropy-based criterion. Stat Methodol. 2016;32:107–121. doi:10.1016/j.stamet.2016.04.004
47. Kim SY. Determining the number of latent classes in single- and multi-phase growth mixture models. Struct Equation Model. 2014;21(2):263–279. doi:10.1080/10705511.2014.882690
48. Preacher KJ, Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Meth. 2008;40(3):879–891. doi:10.3758/BRM.40.3.879
49. Igartua JJ, Mediation HAF. Moderation, and conditional process analysis: concepts, computations, and some common confusions. Span J Psychol. 2021;24:e49. doi:10.1017/SJP.2021.46
50. Huang S, Huang M, Long F, et al. Post-traumatic growth experience of breast cancer patients: a qualitative systematic review and meta-synthesis. PLoS One. 2025;20(1):e0316108. doi:10.1371/journal.pone.0316108
51. Bayraktar S, Ozkan M. Unchanging dynamics in posttraumatic growth in cancer patients: ways of coping and illness perception. Front Psychol. 2023;14:1223131. doi:10.3389/fpsyg.2023.1223131
52. Suo R, Ye F, Xie M, et al. The relationship of marital adjustment and posttraumatic growth in female breast cancer patients and their husbands. Psychol Health Med. 2023;28(2):401–407. doi:10.1080/13548506.2022.2067339
53. Ni Y, Huang L, Tong C, et al. Analysis of the levels of hope and influencing factors in infertile women with first-time and repeated IVF-ET cycles. Reprod Health. 2021;18(1):200. doi:10.1186/s12978-021-01248-y
54. Orovou E, Tzitiridou-Chatzopoulou M, Rigas N, et al. Mapping the relationship between post-traumatic stress and post-traumatic growth and the mediating role of resilience. Clin Psychol Psychother. 2026;33(2):e70249. doi:10.1002/cpp.70249
55. Nik Jaafar NR, Abd Hamid N, Hamdan NA, et al. Posttraumatic growth, positive psychology, perceived spousal support, and psychological complications in head and neck cancer: evaluating their association in a longitudinal study. Front Psychol. 2022;13:920691. doi:10.3389/fpsyg.2022.920691
56. Aliche CJ, Idemudia ES, Uche PN. Social support protects against the negative psychological impacts of death anxiety, and depression on posttraumatic growth in cancer patients. Omega. 2024;302228241302195. doi:10.1177/00302228241302195
57. Soria-Reyes LM, Cerezo MV, Polak AT, et al. The stress process and well-being in breast cancer: the mediating role of hope and zest. Integr Cancer Ther. 2025;24:15347354251396665. doi:10.1177/15347354251396665
58. Stanton AL, Danoff-Burg S, Huggins ME. The first year after breast cancer diagnosis: hope and coping strategies as predictors of adjustment. Psychooncology. 2002;11(2):93–102. doi:10.1002/pon.574
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Latent Profile Analysis and Determinants of Marital Adjustment in Patients with Breast Cancer
Chen XF, Shen C, Gu ZF, Dong C, Zhuang Y, Lu LH, Lu P, Li YJ
Journal of Multidisciplinary Healthcare 2024, 17:5799-5809
Published Date: 5 December 2024
Unveiling Psychological Capital Profiles and Their Impact on Quality of Life in Breast Cancer Patients: A Latent Profile Analysis
Cui C, Liu H, Wang L
Cancer Management and Research 2025, 17:2429-2440
Published Date: 22 October 2025