Back to Journals » Infection and Drug Resistance » Volume 19
Drug Resistance Patterns and Pathogen Distribution in Patients with Urinary Tract Infection in Suzhou, China: A Five-Year Retrospective Study (2020–2024)
Authors Gao J, Wu F, Zhang Y, Wu J, Li W, Su N, Wang Y
Received 27 September 2025
Accepted for publication 19 January 2026
Published 29 January 2026 Volume 2026:19 554982
DOI https://doi.org/10.2147/IDR.S554982
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Oliver Planz
Jingjing Gao,1,2 Fei Wu,3,4 Yuqiong Zhang,1,2 Jian Wu,1,2 Wenjing Li,1,2 Ning Su,1,2 Ya’nan Wang1,2
1Department of Clinical Laboratory, The Affiliated Suzhou Hospital of Nanjing Medical University, Suzhou Municipal Hospital, Gusu School, Nanjing Medical University, Suzhou, Jiangsu, People’s Republic of China; 2Suzhou Key Laboratory of Intelligent Critical Illness Biomarkers Translational Research, Suzhou, Jiangsu, People’s Republic of China; 3School of Medicine, Jiangsu University, Zhenjiang, Jiangsu, People’s Republic of China; 4Department of Clinical Laboratory, Xi’an Fengcheng Hospital, Xi’an, Shanxi, People’s Republic of China
Correspondence: Ya’nan Wang, Department of Clinical Laboratory, The Affiliated Suzhou Hospital of Nanjing Medical University, Suzhou Municipal Hospital, Gusu School, Nanjing Medical University, Suzhou, Jiangsu, 215104, People’s Republic of China, Tel +86-51262368419, Email [email protected]
Objective: To investigate the distribution of pathogens and their antimicrobial resistance profiles in urine cultures from patients with urinary tract infections (UTIs) in Suzhou, China, and to guide empirical treatment decisions.
Methods: We analyzed 9,249 non-duplicate, positive midstream urine cultures collected from January 2020 to December 2024. Bacterial and fungal identification was performed using matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS). Antimicrobial susceptibility testing (AST) was conducted following Clinical and Laboratory Standards Institute (CLSI) guidelines.
Results: Female patients (60.1%) and those aged > 65 years (64.3%) accounted for the majority of cases. Escherichia coli (33.3%) was the predominant pathogen followed by Enterococcus faecalis (8.6%), Klebsiella pneumoniae (8.4%), and Enterococcus faecium (8.0%). Its resistance to third/fourth-generation cephalosporins (eg, cefotaxime from 50.4% to 38.8%) decreased significantly (P < 0.05), while resistance to fluoroquinolones remained high (> 60%). Carbapenem resistance in Klebsiella pneumoniae exhibited alarming fluctuations, peaking at 40.6% in 2023. The prevalence of extended-spectrum β-lactamase (ESBL)-producing Escherichia coli decreased significantly. Enterococcus faecium displayed extreme resistance to ampicillin and fluoroquinolones (> 94%), whereas Enterococcus faecalis was more susceptible. Azole resistance in Candida albicans markedly declined but remained high in Candida tropicalis.
Conclusion: Escherichia coli was the main bacterial urinary pathogen in the Suzhou region. The dynamically high carbapenem resistance in Klebsiella pneumoniae and the severe, species-specific resistance profile of Enterococcus faecium critically limited treatment options. Significant temporal changes in pathogen distribution and resistance patterns underscored the necessity for ongoing local surveillance, tailored empirical therapy, and reinforced antimicrobial stewardship programs to guide effective UTI management in the region.
Keywords: urinary tract infection, pathogen distribution, antimicrobial resistance, carbapenem-resistant Klebsiella pneumoniae, empirical therapy
Introduction
Urinary tract infection (UTI) is one of the most common infections encountered in clinical practice worldwide, imposing a substantial burden on healthcare systems.1,2 Its recurrent nature significantly impacts patients’ quality of life.3 Common uropathogens include Escherichia coli, Klebsiella pneumoniae, Enterococcus faecalis, Enterococcus faecium, Streptococcus agalactiae, Proteus mirabilis, and fungal species such as Candida spp.4 Timely and appropriate antimicrobial therapy is crucial for the effective management of UTIs.5 However, recent epidemiological shifts have revealed an increasing prevalence of multidrug-resistant (MDR) bacteria, such as extended-spectrum β-lactamase (ESBL)-producing Enterobacteriaceae, carbapenem-resistant Klebsiella pneumoniae (CRKP) and vancomycin-resistant enterococci (VRE), which markedly complicate empirical therapeutic strategies.6–9
Previous studies have indicated considerable variation in the prevalence of uropathogens across different geographical regions and investigations.10 Therefore, data from other countries or regions can only serve as a reference. Furthermore, the prevalence of UTIs increases with age, affecting up to 20% of women over 65 years.11 Notably, antimicrobial resistance trends are dynamic and continuously evolve under influences including antimicrobial selection pressure, the emergence and spread of resistant clones, and changes in healthcare practices.12 Consequently, proactive and regular surveillance of local uropathogen distribution and associated resistance patterns is essential for promoting rational antimicrobial use and curbing the emergence of resistant strains.
Comprehensive longitudinal studies on uropathogen prevalence and the dynamic evolution of drug resistance profiles in the Suzhou region are currently lacking. While valuable, existing national or provincial surveillance data often lack the granularity required to provide precise, evidence-based guidance for empirical therapy across diverse healthcare settings.13 This need for actionable, local clinical data persists even as research frontiers expand. For instance, a recent systematic review by Palumbo et al synthesized advances in understanding the urobiome and innovative molecular diagnostics for urinary disorders.14 While such work is crucial for future diagnostic and therapeutic strategies, it also underscores the importance of local epidemiological surveillance. Data on pathogens and their antibiotic resistance profiles continued to provide the evidence required for empirical treatment decisions in current clinical practice. To address this gap, this study retrospectively analyzed clinical data from UTI patients in the Suzhou region from 2020 to 2024. We aimed to elucidate local pathogen distribution and changing trends in antimicrobial resistance, thereby providing valuable evidence-based insights to inform local UTI prevention, control strategies, and rational antibiotic utilization.
Materials and Methods
Study Design and Data Collection
This retrospective study was conducted at a Grade A tertiary general hospital with six campuses in Eastern China from January 2020 to December 2024. Patients who had received antimicrobial agents within two weeks prior to sample collection were excluded from this study. According to the standard clinical protocol, all urine samples (midstream clean catch, nappy pad, catheter aspirated) had been collected in sterile containers, properly labeled, and promptly transported to the clinical microbiology laboratory within two hours. To minimize contamination, a clean catch midstream method was employed wherever possible. In neonates and early infants, nappy pad method, described by Liaw et al was used.15 In case of catheterized patients, urine specimen were collected either through the catheter collection port or through puncture of the tubing with a sterile needle.16 For this analysis, only the first positive urine culture from each patient was included for analysis to avoid duplication. Demographic data (age, sex, ward) and collection dates were retrieved anonymously from the laboratory information system. The study was approved by the Ethics Committee of The Affiliated Suzhou Hospital of Nanjing Medical University (Approval No. K-2024-144-K01). The requirement for informed consent was waived due to the retrospective nature of the study.
Bacterial Culture and Identification
Urine samples were inoculated onto 5% sheep blood agar and MacConkey agar (Autobio, China) using a calibrated 10-μL pipette and inoculating loop. Plates were incubated at 35°C under 5% CO2 for 24–48 hours. Significant growth was defined as ≥105 CFU/mL for gram-negative bacteria and ≥104 CFU/mL for gram-positive bacteria.17 Contaminated samples (containing >3 bacterial species) were excluded. Bacterial identification was performed using matrix-assisted laser desorption/ionization time-of-flight mass spectrometry (MALDI-TOF MS, Bruker Daltonics, Germany).
Antimicrobial Susceptibility Testing
Antimicrobial susceptibility testing (AST) was performed using the Phoenix automated system (BD, USA), the VITEK-2 compact system (bioMérieux, France), or the Kirby-Bauer disk diffusion method, following Clinical and Laboratory Standards Institute (CLSI) guidelines.18 The antibiotics tested included penicillin, ampicillin, piperacillin/tazobactam, ceftazidime, cefotaxime, cefuroxime, cefazolin, cefepime, cefoxitin, imipenem, meropenem, aztreonam, cefoperazone/sulbactam, ampicillin/sulbactam, nitrofurantoin, minocycline, tetracycline, ciprofloxacin, levofloxacin, amikacin, gentamicin, sulfamethoxazole/trimethoprim, vancomycin, teicoplanin, tigecycline, linezolid. Considering the use of multiple AST platforms, quality control was performed using reference strains: Escherichia coli ATCC25922, Klebsiella pneumoniae ATCC 700603, Pseudomonas aeruginosa ATCC 27853, Staphylococcus aureus ATCC 29213, Staphylococcus aureus ATCC 25923, and Enterococcus faecalis ATCC 29212. Results were interpreted as “susceptible” (S), “intermediate” (I), or “resistant” (R) according to CLSI breakpoints.
Antifungal Susceptibility Testing
Antifungal susceptibility testing for Candida isolates against flucytosine, amphotericin B, fluconazole, itraconazole, and voriconazole was performed using the ATB FUNGUS 3 kit (bioMérieux, France), with minimum inhibitory concentrations (MICs) determined according to the manufacturer’s instructions. Quality control was ensured using Candida parapsilosis ATCC 22019 and Candida krusei ATCC 6258. Susceptibility was interpreted according to CLSI M60 guidelines.19
Statistical Analysis
Data analysis was conducted using WHONET 5.6 (WHO, Switzerland) and SPSS Statistics 27.0 (IBMCorp., USA). Categorical variables (demographic characteristics, pathogen distribution, resistance rates) were presented as frequencies and percentages. The chi-square test was used to compare categorical variables between groups. To assess significant temporal trends over the five-year study period (2020–2024) for key outcomes such as pathogen distribution and antimicrobial resistance rates, the chi-square test for trend (Cochran-Armitage test) was employed. A two-tailed P-value of <0.05 was considered statistically significant.
Results
Demographic Characteristics of Patients
A total of 9,249 non-duplicate urine samples were included. Females consistently accounted for the majority (60.1%, 5,560/9,249), which was significantly higher than males (39.9%, 3,689/9,249). The gender distribution remained stable across the study years (Z = 0.867, P = 0.386). Patients aged over 65 years constituted the largest group (64.3%, 5,948/9,249), with their proportion increasing from 62.1% to 65.9% (Z = 2.659, P = 0.008). The age distribution varied significantly over the study period (χ2 = 84.799, P < 0.001). The age group of 45–65 years represented a stable second largest group (23.4%, 2,164/9,249) of the total. Younger age groups (15–44 years and <15 years) were less represented, constituting 10.3% and 2.0% of the cohort, respectively (Table 1).
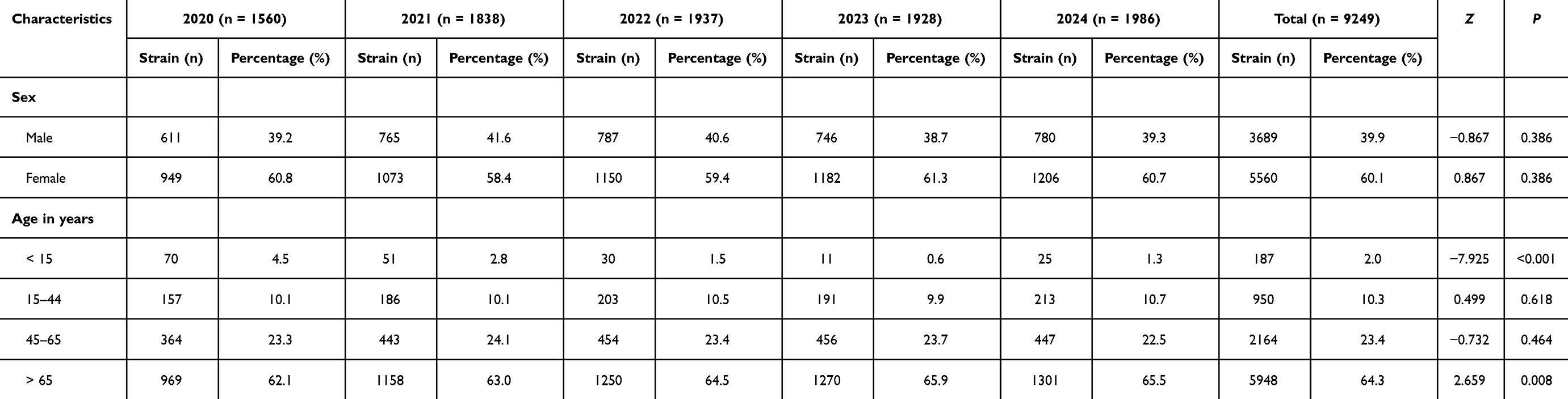 |
Table 1 The Characteristics of Patients According to Their Age and Gender |
Pathogens Distribution
A total of 9,249 non-duplicate pathogenic strains were isolated from urine samples from 2020 to 2024. Their distribution was shown in Table 2. Escherichia coli was the predominant pathogen, accounting for 33.3% of isolates, followed by Enterococcus faecalis (8.6%), Klebsiella pneumoniae (8.4%), and Enterococcus faecium (8.0%). The isolation rate of Escherichia coli increased significantly over time (from 32.4% to 38.1%; Z = 4.544, P < 0.001). In contrast, Enterococcus faecium showed a significant declining trend (from 10.4% to 6.5%; Z = −4.120, P < 0.001). Additionally, the isolation frequencies of Candida albicans also exhibited a significant change over time (from 2.1% to 5.2%; Z = 1.966, P = 0.049). No significant temporal variation was observed for Klebsiella pneumoniae (Z = 1.250, P = 0.211) or Enterococcus faecalis (Z = −0.664, P = 0.506). Other organisms, including Staphylococcus aureus and Citrobacter freundii, were less frequently isolated.
 |
Table 2 Distribution of Main Pathogens Causing UTIs Among Patients |
Drug Resistance Patterns
Resistance of Escherichia coli to Common Antibiotics
Escherichia coli isolates exhibited significant temporal variations in resistance to several antibiotics (Table 3). Consistently high resistance was observed to ampicillin (75.8% overall), with no significant annual variation (P = 0.577). High resistance was also noted for fluoroquinolones: ciprofloxacin (63.2% overall) and levofloxacin (60.2% overall). Significant decreasing trends were observed for ceftazidime (from 22.5% to 14.4%, P = 0.001), cefotaxime (from 50.4% to 38.8%, P = 0.001), cefuroxime (from 52.6% to 41.7%, P = 0.025), cefepime (from 37.2% to 27.9%, P = 0.005), and cefoxitin (from 13.8% to 7.3%, P = 0.002). Resistance to sulfamethoxazole/trimethoprim remained high (43.8% overall). In contrast, carbapenems (imipenem 1.2%, meropenem 1.0%) maintained excellent activity, with both showing decreasing trends (P = 0.009 and P = 0.029, respectively). Similarly, amikacin (1.9% overall) and β-lactam/β-lactamase inhibitor combinations such as cefoperazone/sulbactam (3.9% overall) and piperacillin/tazobactam (3.7% overall) proved highly effective.
 |
Table 3 Resistance of Escherichia coli to Common Antibiotics |
Resistance of Klebsiella pneumoniae to Common Antibiotics
Klebsiella pneumoniae exhibited significant temporal variations in resistance to some antibiotics (Table 4). Alarmingly, carbapenem resistance showed marked fluctuations. Imipenem resistance rose from 20.2% in 2020 to a peak of 40.6% in 2023 before declining to 22.1% in 2024 (Z = 1.754, P = 0.079); meropenem resistance followed a nearly similar pattern (Z = 1.872, P = 0.061). Resistance to third- and fourth-generation cephalosporins was consistently high and variable: ceftazidime (39.7% overall), cefepime (41.4% overall), and cefotaxime (46.0% overall). High resistance was also noted for fluoroquinolones (ciprofloxacin 49.4%; levofloxacin 43.5%) and ampicillin/sulbactam (46.7% overall). Although lower, amikacin resistance (24.8% overall) showed a significant increasing trend (Z = 1.984, P = 0.047), peaking at 34.8% in 2023. Similarly, resistance to piperacillin/tazobactam also rose from 25.8% to 47.6% (Z = 2.099, P = 0.036). Resistance to β-lactam/β-lactamase inhibitor combinations, cefoperazone/sulbactam, was 32.3%, with no significant annual variation (P = 0.454).
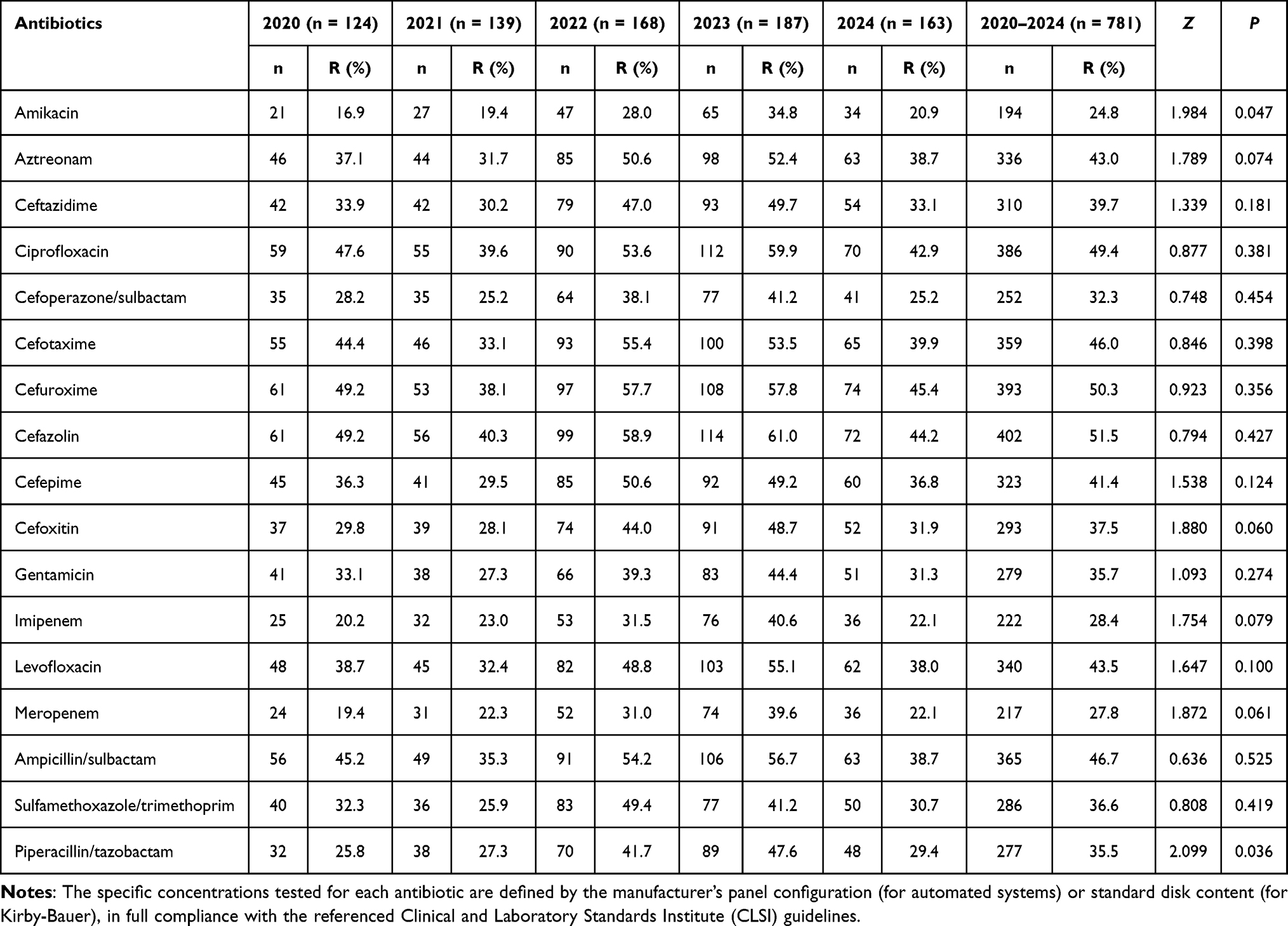 |
Table 4 Resistance of Klebsiella pneumoniae to Common Antibiotics |
ESBL and CRE Prevalence in Common Pathogens
From 2020 to 2024, the prevalence of ESBL-producing Escherichia coli significantly declined from 50.4% to 38.8% (Z = −3.376, P = 0.001). Carbapenem-resistant Escherichia coli showed a decreasing trend (from 2.8% to 0.7%; Z = −2.612, P = 0.009). ESBL rates in Klebsiella pneumoniae fluctuated between 33.1% and 55.4% (Z = 0.846, P = 0.398), peaking at 55.4% in 2022 before falling to 39.9% in 2024. The prevalence of CRKP also showed a fluctuation (Z = 1.754, P = 0.079), rising from 20.2% in 2020 to a peak of 40.6% in 2023, then declining to 22.1% in 2024 (Table 5).
 |
Table 5 ESBL and CRE Prevalence in Common Pathogens |
Resistance of Enterococcus faecalis to Common Antibiotics
Enterococcus faecalis showed significant temporal variations in resistance to several antibiotics (Table 6). Resistance to ciprofloxacin increased significantly from 28.7% to 50.3% (Z = 2.861, P = 0.004). Levofloxacin resistance also showed an increasing trend (from 28.2% to 46.9%; Z = 2.258, P = 0.024). Although high, the resistance to tetracycline (from 89.4% to 78.7%; Z = −2.452, P = 0.014) and minocycline (from 84.8% to 65.0%; Z = −4.737, P < 0.001) showed a decreasing trend. However, no resistance was detected to high-level gentamicin, teicoplanin, or vancomycin during the study period. Notably, linezolid resistance showed a significant increasing trend (from 2.6% to 8.1%; Z = 2.401, P = 0.016). Resistance to ampicillin, nitrofurantoin, and penicillin showed no significant temporal variations.
 |
Table 6 Resistance of Enterococcus faecalis to Common Antibiotics |
Resistance of Enterococcus faecium to Common Antibiotics
Enterococcus faecium exhibited very high resistance to ciprofloxacin (97.3%), penicillin (97.2%), ampicillin (96.5%), and levofloxacin (94.5%) over the five-year period (Table 7). Significant temporal variations were observed in resistance to nitrofurantoin (70.2% overall, Z = 5.088, P < 0.001) and tetracycline (39.5% overall, Z = 3.329, P = 0.001). In contrast, resistance remained low for high-level of gentamicin, tigecycline, teicoplanin, vancomycin, and linezolid, suggesting their potential efficacy (Table 7).
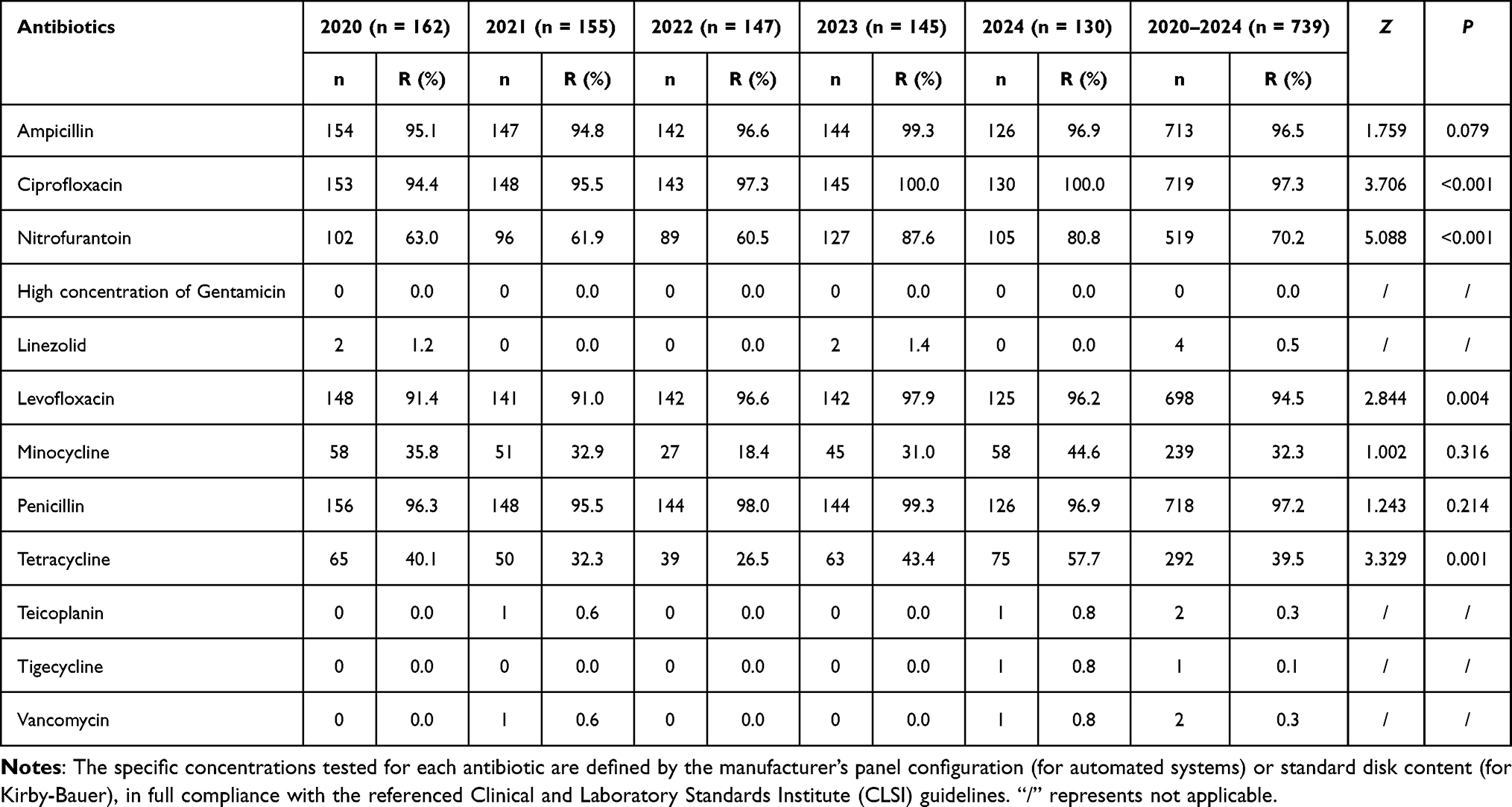 |
Table 7 Resistance of Enterococcus faecium to Common Antibiotics |
Resistance of Candida albicans to Common Antifungal Agents
As shown in Table 8, Candida albicans demonstrated consistently high susceptibility to amphotericin B, with no resistant isolates detected. Significant decreases in resistance were observed for fluconazole (from 33.3% to 5.7%, Z = −5.616, P < 0.001), itraconazole (from 28.4% to 2.3%, Z = −5.919, P < 0.001), and voriconazole (from 48.5% to 4.6%, Z = −6.541, P < 0.001). These trends suggested improved antifungal stewardship and possibly more appropriate triazole usage in recent years.
 |
Table 8 Resistance of Candida albicans to Common Antifungal Agents |
Resistance of Candida tropicalis to Common Antifungal Agents
In contrast, Candida tropicalis exhibited persistently higher resistance to azole antifungals (Table 9). Amphotericin B and flucytosine remained effective. Fluconazole resistance remained high (44.9% overall) and did not exhibit a statistically significant temporal trend over the study period (Z = −1.401, P = 0.161). Itraconazole resistance averaged 34.0% with fluctuations (Z = −0.536, P = 0.592). A non-significant numerical decrease in voriconazole resistance was observed (Z = −1.110, P = 0.267).
 |
Table 9 Resistance of Candida tropicalis to Common Antifungal Agents |
Discussion
UTIs represent a major clinical and public health challenge due to their high incidence, recurrence rate, and the growing threat of antimicrobial resistance.20,21 Empirical treatment of UTIs requires a thorough understanding of local pathogen epidemiology and resistance data.22 Our study provides a detailed five-year analysis of uropathogen distribution and evolving resistance patterns in a tertiary hospital with six campuses in Suzhou, China, revealing several notable trends with direct clinical implications.
The study found that female patients accounted for 60.1% of cases, significantly outnumbering males (39.9%). This finding was consistent with the observations of Herbawi A et al, who reported a higher proportion of UTIs in females (59.1%) compared to males (40.9%).23 In Romania, the proportion of UTIs in females was 73%, considerably higher than that of males (27%).24 Numerous factors, including female anatomical and physiological characteristics, menopause, pregnancy, and pelvic organ prolapse, contribute to their higher risk of UTIs.25 Previous studies have indicated that the incidence of UTIs increases with patient age.26 The majority of cases occurred in individuals aged >65 years (64.3%), a finding aligned with other studies and likely reflecting age-associated factors such as comorbidities, urinary incontinence, catheter use, prolonged antimicrobial exposure, and declined immune function.27,28 However, the proportion of pediatric cases (<15 years) declined significantly across the study period (Z = −7.925, P < 0.001). This trend could be attributed to improvements in community hygiene education, early intervention for congenital urological anomalies, and reduced unnecessary antimicrobial use in pediatric settings. Such targeted interventions highlighted the potential impact of public health strategies on reducing UTI burden in vulnerable pediatric populations, a point that warranted further prospective evaluation.
Escherichia coli (33.3%) was the predominant uropathogen in this study, confirming its leading role in both community and healthcare settings worldwide.29 Its remarkable adaptability in the urinary tract environment is facilitated by various virulence factors, including adhesins, toxins, and iron acquisition systems.30 Enterococcus faecalis was the second most frequently isolated bacterial pathogen, followed by Klebsiella pneumoniae, Enterococcus faecium, Pseudomonas aeruginosa, and Candida albicans. However, some studies have ranked Klebsiella pneumoniae as the second most common uropathogen.31 A survey in India reported that Escherichia coli accounted for 39.7% of isolates, while Klebsiella pneumoniae constituted 20.7%.32 This discrepancy might stem from differences in patient demographics and local antimicrobial use policies. Nevertheless, the most prevalent uropathogens remain consistent, albeit with regional variations in their rankings.
In this study, Escherichia coli exhibited high resistance rates to several commonly used antibiotics. Resistance to first- and second-generation cephalosporins and sulfamethoxazole/trimethoprim reached 40–50%, while resistance to ampicillin, ciprofloxacin, and levofloxacin was as high as 60–76%. These resistance rates significantly compromise the effectiveness of empirical therapeutic regimens. Similar findings were reported by Niu X et al, who noted resistance rates exceeding 50% to ampicillin and quinolones in Escherichia coli.33 This trend, consistent with observations in other countries,34 was primarily driven by plasmid-mediated quinolone resistance (PMQR) genes and chromosomal mutations in target enzymes.35 Notably, we observed a significant decline in Escherichia coli resistance to third-generation cephalosporins (ceftazidime: 22.5% to 14.4%, P = 0.001; cefotaxime: 50.4% to 38.8%, P = 0.001) over the study period. This reduction correlates with the implementation of our hospital’s antimicrobial stewardship program (ASP), which restricted the empirical use of third-generation cephalosporins for uncomplicated UTIs and mandated pre-prescription culture testing for complicated cases. The ASP also promoted the use of narrow-spectrum agents, which likely reduced selection pressure on cephalosporin-resistant strains. In contrast, Escherichia coli demonstrated low resistance to aminoglycosides (amikacin, 1.9%) and β-lactam/β-lactamase inhibitor combinations (piperacillin/tazobactam, 3.7%; cefoperazone/sulbactam, 3.9%), providing valuable options for targeted therapy. The low resistance to aminoglycosides and β-lactam/β-lactamase inhibitors was comparable to the reports by Siriphap A et al.36 However, a study from Malawi reported a resistance rate of 88.1% to sulfamethoxazole/trimethoprim in Escherichia coli, indicating considerable regional and national variation in antibiotic resistance patterns.37 Furthermore, carbapenems (imipenem, 1.2%; meropenem, 1.0%) maintained excellent and consistent activity against Escherichia coli isolates throughout the study period, a finding largely consistent with Bayaba S et al.38 This sustained susceptibility made carbapenems reliable alternatives for treating multidrug-resistant Escherichia coli infections. However, the use of carbapenems should remain restricted to confirmed MDR infections to prevent resistance emergence.
The resistance profile of Klebsiella pneumoniae was particularly concerning. The high and fluctuating resistance to cephalosporins, fluoroquinolones, and especially carbapenems (peaking at 40.6% in 2023) drastically limited treatment options. Maraki S et al reported high resistance rates in Klebsiella pneumoniae to ciprofloxacin (47.8%), amoxicillin/clavulanic acid (34.2%), and sulfamethoxazole-trimethoprim (42.8%).31 Another study indicated resistance rates of 4% to amikacin, 21% to meropenem, and 36% to cefuroxime axetil.39 The disparities in resistance rates among uropathogenic bacteria across these studies may be attributed to various factors, such as differences in study populations and geographic regions. The most striking finding was the sharp increase in carbapenem resistance in Klebsiella pneumoniae, rising from 20.2% in 2020 to 40.6% in 2023 before declining to 22.1% in 2024. While the precise cause remained to be fully elucidated, this peak was highly suggestive of a localized clonal outbreak within our hospital network, potentially exacerbated by high antimicrobial selection pressure. The subsequent decline in 2024 likely reflected the effectiveness of intensified infection control measures, including enhanced hand hygiene monitoring, contact precautions for CRKP-positive patients, and environmental decontamination of high-touch surfaces in urology and geriatric wards. This trend underscored the volatile and rapidly evolving nature of carbapenem resistance and the critical need for real-time surveillance to trigger immediate intervention strategies.40 For empirical therapy, this trend also implied that carbapenems should no longer be considered first-line agents for Klebsiella pneumoniae UTIs in our region, especially in high-risk settings. Instead, newer β-lactam/β-lactamase inhibitor combinations (eg, ceftazidime/avibactam) or polymyxins might be more appropriate, though their use requires careful consideration of local susceptibility data.
ESBL-producing Enterobacteriaceae often exhibit cross-resistance to multiple antibiotics, severely limiting treatment options.41 From 2020 to 2024, the rate of MDR in ESBL-positive Escherichia coli declined (from 50.4% to 38.8%), while the proportion of ESBL-positive Klebsiella pneumoniae fluctuated (peaking at 55.4% in 2022). This regional variation likely reflects differences in antimicrobial use intensity. The five-year ESBL-positive detection rate was similar to previous findings.42 However, the Yartey SN reported a lower ESBL-positive rate (16.8%).43 The high proportions of ESBL-producing strains among Escherichia coli (42.6%) and Klebsiella pneumoniae (46.0%) isolates meant that first-line use of cephalosporins was no longer justified; instead, β-lactam/β-lactamase inhibitor combinations (eg, piperacillin/tazobactam) should be prioritized, especially in patients with risk factors for ESBL infection. Fluctuations in the annual prevalence of ESBL-producing strains suggested complex dynamics involving clonal dissemination, infection control measures, and antibiotic selective pressure.
Carbapenems are often used as first-line drugs for infections caused by MDR bacteria such as Klebsiella pneumoniae.44 The molecular mechanisms typically involve the production of carbapenemases, such as Klebsiella pneumoniae carbapenemases (KPC) and new delhi metallo‑β‑lactamase (NDM), along with porin mutations and efflux pump overexpression.45 In this study, the resistance rate to imipenem in Klebsiella pneumoniae rose from 20.2% in 2020 to a peak of 40.6% in 2023, representing one of the most significant threats to effective UTI treatment in this region. This trend necessitated a critical re-evaluation of empirical carbapenem use for severe UTIs in our hospital, using them in combination with rapid diagnostic tests when CRKP risk was high. This trend also mirrored the spread of CRE, often facilitated by healthcare transmission.46 This alarming rise in CRKP might warrant the use of newer β-lactam/β-lactamase inhibitor combinations as preferred empirical choices in high-risk settings.47 Furthermore, while tracking dominant pathogens is vital, the emergence of rare, MDR organisms, as illustrated by a recent case of Cedecea lapagei UTI, reminded us that continuous laboratory vigilance and tailored susceptibility testing remain irreplaceable for optimal patient management, especially among the elderly and immunocompromised.48
Enterococcus faecium isolates exhibited extremely high resistance rates to ampicillin (96.5%), penicillin (97.2%), ciprofloxacin (97.3%), and levofloxacin (94.5%), rendering these traditional anti-enterococcal agents largely ineffective. Fluoroquinolones are a critical class of antibiotics, as they have traditionally been highly effective against complicated UTIs.49 The increasing rate of resistance to these drugs should be a cause for concern. In contrast, Enterococcus faecalis demonstrated significantly lower resistance to the aforementioned drugs, underscoring the importance of species identification in guiding appropriate therapy. The difference in resistance patterns between the two enterococcal species reflects their distinct inherent and acquired resistance mechanisms. Conversely, glycopeptides (vancomycin, 0.3%; teicoplanin, 0.3%) as well as agents such as tigecycline (0.1%) and linezolid (0.5%) remained highly active against Enterococcus faecium, providing reliable options for severe infections. The absence of high-level aminoglycoside resistance (HLAR) suggests that combination synergistic therapy remains viable. It is noteworthy that linezolid resistance in enterococci is typically associated with mutations in the 23S rRNA gene or acquisition of the transferable cfr gene.50 Although the proportion of linezolid-resistant enterococci was low in this study (Enterococcus faecalis, 5.2%; Enterococcus faecium, 0.5%), its emergence warranted vigilant monitoring and further investigation through molecular characterization of resistance mechanisms.
Candida albicans was the predominant fungal isolate, consistent with its status as the most common cause of fungal UTIs globally.51 Antifungal susceptibility analysis revealed a significant declining trend in azole resistance among Candida albicans isolates, with fluconazole resistance decreasing from 33.3% to 5.7% over the study period. This encouraging trend coincided with broader institutional efforts in antifungal stewardship and might reflect improved adherence to appropriate dosing regimens. In contrast, Candida tropicalis maintained high fluconazole resistance (44.9% overall), emphasizing the need for species-specific testing. Consistent with other reports, the susceptibility to amphotericin B remained nearly universal.52,53 It is important to note that the smaller sample size for some Candida species may contribute to variation in resistance rates when compared to larger studies. A key limitation of our analysis was the lack of detailed clinical data on prior azole exposure, diabetes mellitus status, or immunosuppressive therapy, which restricted our ability to investigate specific risk factors for azole-resistant candiduria. Future prospective studies incorporating these variables were needed. Collectively, these fluctuating and species-dependent patterns underscore the dynamic nature of antifungal resistance and reinforce the imperative for continuous local surveillance to inform empirical therapy decisions.
Study Limitations
This study has several limitations. First, as a single-center study, its findings may not be fully generalizable to other regions. Second, the retrospective design limited the availability of detailed clinical data (eg, prior antibiotics, catheter use, outcomes) for risk factor analysis and further stratification of the patient population. Third, by including only symptomatic patients with positive urine cultures, the true UTI prevalence, particularly in outpatients or culture-negative cases, may be underestimated. Future multicenter prospective studies should integrate clinical and molecular data to address these limitations and provide more actionable insights for empirical therapy.
Conclusion
Our study highlighted dynamic trends in UTI pathogens and resistance in Suzhou, with key implications for clinical practice. Escherichia coli, while predominant, showed high resistance to fluoroquinolones, advising against their empirical first-line use. The fluctuating but high carbapenem resistance in Klebsiella pneumoniae necessitated restricting empirical carbapenem use, especially in severe cases. The high rates of ESBL-production in Escherichia coli and Klebsiella pneumoniae, often associated with MDR profiles, severely limit therapeutic options. Furthermore, species-specific MDR patterns were evident among enterococci, with Enterococcus faecium demonstrating extremely high resistance to ampicillin and fluoroquinolones, unlike Enterococcus faecalis. The significant decline in ESBL-producing Escherichia coli and azole resistance in Candida albicans reflected successful stewardship. These data, derived from a predominantly female and elderly (> 65 year) patient population, underscored the necessity of continuous local surveillance. The high and evolving MDR rates, particularly of CRKP and Enterococcus faecium, highlighted the urgent need for tailored empirical therapy and enhanced antimicrobial stewardship to guide effective UTI management.
Abbreviations
UTIs, Urinary tract infections; ESBL, Extended-spectrum beta-lactamases; CRE, Carbapenem-resistant Enterobacteriaceae; CRKP, Carbapenem-resistant Klebsiella pneumoniae; VRE, Vancomycin-resistant enterococci; MDR, Multidrug-resistant; MALDI-TOF MS, Matrix-assisted laser desorption/ionization time-of-flight mass spectrometry; AST, Antimicrobial susceptibility testing; CLSI, Clinical and Laboratory Standards Institute; MIC, Minimal inhibitory concentration; HLAR, High-level aminoglycoside resistance; KPC, Klebsiella pneumoniae carbapenemases; NDM, New Delhi metallo‑β‑lactamase; PMQR, Plasmid-mediated quinolone resistance; ASP, Antimicrobial stewardship program.
Ethics Approval
This study was approved by the Ethics Committee of The Affiliated Suzhou Hospital of Nanjing Medical University (Approval No. K-2024-144-K01). As a retrospective analysis, the requirement for obtaining informed consent was exempted by the same ethics committee. De-identified patient data were obtained from the hospital microbiology laboratory, where the bacterial strains were isolated. All procedures were carried out in strict conformity with the principles of the Declaration of Helsinki.
Acknowledgments
The authors are grateful to all the anonymous reviewers for their constructive comments and suggestions to this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The work was funded by the Suzhou Science and Technology Research Program for Medical and Healthcare Innovation (SYWD2025145), the Suzhou Key Laboratory of Intelligent Critical Illness Biomarkers Translational Research (SZS2024029), the Suzhou Medical and Health Technology Innovation Project (SYWD2024326), the Suzhou Strengthening Health through Science and Education Project (MSXM2025033), and the Nanjing Medical University - Qilu Clinical Research Fund Project (2024KF0258).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Li L, Li Y, Chen Y, et al. Global, regional, and national lifetime probabilities of urinary tract infections and interstitial nephritis from 1990 to 2021. J Health Popul Nutr. 2025;44(1):231. doi:10.1186/s41043-025-00950-y
2. Yang X, Chen H, Zheng Y, et al. Disease burden and long-term trends of urinary tract infections: a worldwide report. Front Public Health. 2022;10:888205. doi:10.3389/fpubh.2022.888205
3. Maxwell K, Roberts L, Kramer M, et al. Psychosocial burden and healthcare disillusionment in recurrent UTI: a large-scale international survey of patient perspectives. Front Urol. 2023;3:1264299. doi:10.3389/fruro.2023.1264299
4. Timm MR, Russell SK, Hultgren SJ. Urinary tract infections: pathogenesis, host susceptibility and emerging therapeutics. Nat Rev Microbiol. 2025;23(2):72–15. doi:10.1038/s41579-024-01092-4
5. Bavanandan S, Keita N. Urinary Tract Infection Prevention and Treatment. Semin Nephrol. 2023;43(5):151468. doi:10.1016/j.semnephrol.2023.151468
6. Jiang J, Long T, Porter AR, et al. Carbapenem-Resistant, Virulence Plasmid-Harboring Klebsiella pneumoniae, United States. Emerg Infect Dis. 2025;31(4):761–771. doi:10.3201/eid3104.241396
7. Zollner-Schwetz I, König E. Treatment options for multidrug-resistant Gram-negatives in urinary tract infections. Curr Opin Urol. 2023;33(3):173–179. doi:10.1097/mou.0000000000001084
8. Aththanayaka A, Weerasinghe G, Weerakkody NS, et al. Effectiveness of selective antibiotics use in ESBL-related UTIs. BMC Microbiol. 2024;24(1):360. doi:10.1186/s12866-024-03495-y
9. Hota S, Patil SR, Mane PM. Enterococcus: understanding Their Resistance Mechanisms, Therapeutic Challenges, and Emerging Threats. Cureus. 2025;17(2):e79628. doi:10.7759/cureus.79628
10. Zeng Z, Zhan J, Zhang K, et al. Global, regional, and national burden of urinary tract infections from 1990 to 2019: an analysis of the global burden of disease study 2019. World J Urol. 2022;40(3):755–763. doi:10.1007/s00345-021-03913-0
11. Gajdács M, Ábrók M, Lázár A, Burián K. Urinary Tract Infections in Elderly Patients: a 10-Year Study on Their Epidemiology and Antibiotic Resistance Based on the WHO Access, Watch, Reserve (AWaRe) Classification. Antibiotics. 2021;10(9):1098. doi:10.3390/antibiotics10091098
12. Tang KWK, Millar BC, Moore JE. Antimicrobial Resistance (AMR). Br J Biomed Sci. 2023;80:11387. doi:10.3389/bjbs.2023.11387
13. Qin X, Ding L, Hao M, et al. Antimicrobial resistance of clinical bacterial isolates in China: current status and trends. JAC Antimicrob Resist. 2024;6(2):dlae052. doi:10.1093/jacamr/dlae052
14. Palumbo S, Lucarelli G, Lasorsa F, et al. Urobiome and Inflammation: a Systematic Review on Microbial Imbalances and Diagnostic Tools for Urinary Disorders. Urology. 2025;200:206–215. doi:10.1016/j.urology.2025.03.050
15. Liaw LC, Nayar DM, Pedler SJ, Coulthard MG. Home collection of urine for culture from infants by three methods: survey of parents’ preferences and bacterial contamination rates. BMJ. 2000;320(7245):1312–1313. doi:10.1136/bmj.320.7245.1312
16. Hooton TM, Bradley SF, Cardenas DD, et al. Diagnosis, prevention, and treatment of catheter-associated urinary tract infection in adults: 2009 International Clinical Practice Guidelines from the Infectious Diseases Society of America. Clin Infect Dis. 2010;50(5):625–663. doi:10.1086/650482
17. Shang H, Wang Y, Shen Z. National Clinical Laboratory Procedures[M].
18. CLSI. Performance standards for antimicrobial susceptibility testing. In: CLSI Guideline M100. Wayne, Pennsylvania, USA: Clinical and Laboratory Standards Institute; 2024.
19. CLSI. Performance standards for antifungal susceptibility testing of yeasts. In: CLSI Guideline M60. Wayne, Pennsylvania, USA: Clinical and Laboratory Standards Institute; 2020.
20. He Y, Zhao J, Wang L, et al. Epidemiological trends and predictions of urinary tract infections in the global burden of disease study 2021. Sci Rep. 2025;15(1):4702. doi:10.1038/s41598-025-89240-5
21. Von Vietinghoff S, Shevchuk O, Dobrindt U, et al. The global burden of antimicrobial resistance - urinary tract infections. Nephrol Dial Transplant. 2024;39(4):581–588. doi:10.1093/ndt/gfad233
22. Nelson Z, Aslan AT, Beahm NP, et al. Guidelines for the Prevention, Diagnosis, and Management of Urinary Tract Infections in Pediatrics and Adults: a WikiGuidelines Group Consensus Statement. JAMA Netw Open. 2024;7(11):e2444495. doi:10.1001/jamanetworkopen.2024.44495
23. Herbawi A, Abu Taha A, Aiesh BM, et al. Spectrum and antibiotic resistance in community- and hospital-acquired urinary tract infections among adults: experience from a large tertiary care center in a developing country. Urologia. 2024;91(2):394–402. doi:10.1177/03915603241236361
24. Borcan AM, Radu G, Simoiu M, et al. A Five-Year Analysis of Antibiotic Resistance Trends among Bacteria Identified in Positive Urine Samples in a Tertiary Care Hospital from Bucharest, Romania. Antibiotics. 2024;13(2):160. doi:10.3390/antibiotics13020160
25. Bonkat G, Wagenlehner F, Cai T, et al. Classification of Urinary Tract Infections in 2025: moving Beyond Uncomplicated and Complicated. Eur Urol Open Sci. 2025;75:44–47. doi:10.1016/j.euros.2025.03.010
26. Ligon MM, Joshi CS, Fashemi BE, et al. Effects of aging on urinary tract epithelial homeostasis and immunity. Dev Biol. 2023;493:29–39. doi:10.1016/j.ydbio.2022.11.003
27. Hu Y, Ma W, Tang K, et al. Global burden of urinary tract infections in older women from 1990 to 2021 with projections to 2040: a trend analysis of the Global Burden of Disease Study 2021. Front Cell Infect Microbiol. 2025;15:1577777. doi:10.3389/fcimb.2025.1577777
28. Bausch K, Stangl FP, Prieto J, et al. Urinary Infection Management in Frail or Comorbid Older Individuals. Eur Urol Focus. 2024;10(5):731–733. doi:10.1016/j.euf.2024.08.007
29. Bernaitis L, Bharathi P, Ezhilarasu A, Revathi PS. Isolation and molecular characterization of multi-drug resistant uropathogenic Escherichia coli from urine samples: insights into urinary tract infection management. The Microbe. 2024;5:100185. doi:10.1016/j.microb.2024.100185
30. Zhou Y, Zhou Z, Zheng L, et al. Urinary Tract Infections Caused by Uropathogenic Escherichia coli: mechanisms of Infection and Treatment Options. Int J Mol Sci. 2023;24(13):10537. doi:10.3390/ijms241310537
31. Maraki S, Mavromanolaki VE, Stafylaki D, et al. Antimicrobial resistance trends among Klebsiella pneumoniae associated with urinary tract infections in Crete, Greece, 2017–2022. Acta Microbiol Immunol Hung. 2024;71(2):121–126. doi:10.1556/030.2024.02297
32. Pathi BK, Mohapatra S, Sharma V, et al. Antimicrobial Sensitivity Patterns of Bacteria Causing Urinary Tract Infections: a Retrospective Study of Elderly Patients Admitted to a Tertiary Care Hospital in Bhubaneswar, India. Cureus. 2025;17(1):e77399. doi:10.7759/cureus.77399
33. Niu X, Hou B, Yang L, et al. Patterns of Drug Resistance and Bacterial Pathogen Distribution in Patients with Urinary Tract Infections in the Jiaxing Region from 2020 to 2022. Infect Drug Resist. 2023;16:5911–5921. doi:10.2147/IDR.S424158
34. Jalil MB, Al Atbee MYN. The prevalence of multiple drug resistance Escherichia coli and Klebsiella pneumoniae isolated from patients with urinary tract infections. J Clin Lab Anal. 2022;36(9):e24619. doi:10.1002/jcla.24619
35. Marquez-Salazar DA, Delgadillo-Valles R, Hernandez-Acevedo GN, et al. Coexistence of PMQR and ESBL genes among clinical Escherichia coli isolates from community-acquired UTI in Mexicali, on the US-Mexico border. Braz J Infect Dis. 2025;29(4):104554. doi:10.1016/j.bjid.2025.104554
36. Siriphap A, Kitti T, Khuekankaew A, et al. High prevalence of extended-spectrum beta-lactamase-producing Escherichia coli and Klebsiella pneumoniae isolates: a 5-year retrospective study at a Tertiary Hospital in Northern Thailand. Front Cell Infect Microbiol. 2022;12:955774. doi:10.3389/fcimb.2022.955774
37. Bwanali AN, Lubanga AF, Kondowe S, et al. Trends and patterns of antimicrobial resistance among common pathogens isolated from adult bloodstream and urinary tract infections in public health facilities in Malawi, 2020–2024. BMC Infect Dis. 2025;25(1):946. doi:10.1186/s12879-025-11335-1
38. Bayaba S, Founou RC, Tchouangueu FT, et al. High prevalence of multidrug resistant and extended-spectrum β-lactamase-producing Escherichia coli and Klebsiella pneumoniae isolated from urinary tract infections in the West region, Cameroon. BMC Infect Dis. 2025;25(1):115. doi:10.1186/s12879-025-10483-8
39. Neelambike Sumana M, Maheshwarappa YD, K G, et al. A retrospective study of the antimicrobial susceptibility patterns of Klebsiella pneumoniae isolated from urine samples over a decade in South India. Front Microbiol. 2025;16:1553943. doi:10.3389/fmicb.2025.1553943
40. Lei TY, Liao BB, Yang LR, et al. Hypervirulent and carbapenem-resistant Klebsiella pneumoniae: a global public health threat. Microbiol Res. 2024;288:127839. doi:10.1016/j.micres.2024.127839
41. Nguyen MN, Gladstone BP, De Angelis G, et al. Tracing carriage, acquisition, and transmission of ESBL-producing Escherichia coli over two years in a tertiary care hospital. Genome Med. 2024;16(1):151. doi:10.1186/s13073-024-01424-2
42. Azzam A, Khaled H, Samer D, Nageeb WM. Prevalence and molecular characterization of ESBL-producing Enterobacteriaceae in Egypt: a systematic review and meta-analysis of hospital and community-acquired infections. Antimicrob Resist Infect Control. 2024;13(1):145. doi:10.1186/s13756-024-01497-z
43. Yartey SN, Kungu F, Asantewaa AA, Donkor ES. Extended Spectrum Beta-Lactamase-Producing Bacterial Clones in West Africa: a Systematic Review and Meta-Analysis from a One Health Perspective. Sci Rep. 2025;15(1):29625. doi:10.1038/s41598-025-10695-7
44. Macesic N, Uhlemann AC, Peleg AY. Multidrug-resistant Gram-negative bacterial infections. Lancet. 2025;405(10474):257–272. doi:10.1016/s0140-6736(24)02081-6
45. Bush K, Bradford PA. Epidemiology of β-Lactamase-Producing Pathogens. Clin Microbiol Rev. 2020;33(2):e00047–19. doi:10.1128/cmr.00047-19
46. Ma J, Song X, Li M, et al. Global spread of carbapenem-resistant Enterobacteriaceae: epidemiological features, resistance mechanisms, detection and therapy. Microbiol Res. 2023;266:127249. doi:10.1016/j.micres.2022.127249
47. Mackow NA, van Duin D. Reviewing novel treatment options for carbapenem-resistant Enterobacterales. Expert Rev Anti Infect Ther. 2024;22(1–3):71–85. doi:10.1080/14787210.2024.2303028
48. Aveta A, Napodano G, Spena G, et al. Rare case of urinary tract infection caused by Cedecea lapagei in a 93-year-old patient in southern Italy. Infez Med. 2025;33(2):221–225. doi:10.53854/liim-3302-8
49. Thompson D, Xu J, Ischia J, Bolton D. Fluoroquinolone resistance in urinary tract infections: epidemiology, mechanisms of action and management strategies. BJUI Compass. 2024;5(1):5–11. doi:10.1002/bco2.286
50. Beh JQ, Daniel DS, Judd LM, et al. Genomics to understand the global landscape of linezolid resistance in Enterococcus faecium and Enterococcus faecalis. Microb Genom. 2025;11(6):001432. doi:10.1099/mgen.0.001432
51. Ahmad S, Boekhout T, Al-Hatmi AMS, et al. Epidemiology of Candidemia, Candiduria and Emerging Candidozyma (Candida) auris Across Gulf Cooperative Council Countries and Yemen in the Arabian Peninsula. Mycoses. 2025;68(6):e70073. doi:10.1111/myc.70073
52. Kilbas I, Kahraman Kilbas EP, Horhat FG, Ciftci IH. Twenty-Year Course of Antifungal Resistance in Candida albicans in Türkiye: a Systematic Review and Meta-Analysis. J Fungi. 2025;11(8):603. doi:10.3390/jof11080603
53. Ahmady L, Gothwal M, Mukkoli MM, Bari VK. Antifungal drug resistance in Candida: a special emphasis on amphotericin B. Apmis. 2024;132(5):291–316. doi:10.1111/apm.13389
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Analysis of Antimicrobial Use and Bacterial Susceptibility in Patients with Urinary Tract Infections at a Certain Hospital From 2021 to 2023: A Retrospective Cohort Study
Li K, Li X, Jiang J
International Journal of General Medicine 2026, 19:562925
Published Date: 24 February 2026
Phenotypic Detection of Extended-Spectrum β-Lactamase and Antimicrobial Resistance Patterns in Multidrug-Resistant Uropathogenic Enterobacterales at a Tertiary-Care Hospital in Bangladesh
Biswas P, Setu SK, Sattar ANI, Avi AD
Infection and Drug Resistance 2026, 19:615697
Published Date: 30 June 2026
Fosfomycin Trometamol in the Management of Urinary Tract Infection: A Focus on Antimicrobial Susceptibility and Resistance
Stefani S, Tascini C
Infection and Drug Resistance 2026, 19:589847
Published Date: 15 July 2026